Drug selection in Rheumatoid Arthritis
|
|
|
- Kory French
- 5 years ago
- Views:
Transcription
1 Drug selection in Rheumatoid Arthritis PROFESSOR KHAN ABUL KALAM AZAD PROFESSOR, DEPARTMENT OF MEDICINE DHAKA MEDICAL COLLEGE
2 Rheumatoid arthritis Autoimmune disease Onset generally occurs between 30 and 55 years of age Women are affected more often than men.
3 Disease hallmarks Inflammation of the synovium Progressive bone erosion Joint malalignment and destruction, and Weakness of surrounding tissues and muscles.
4 Presentations range from mild to severe Progressive course leading to functional limitations.
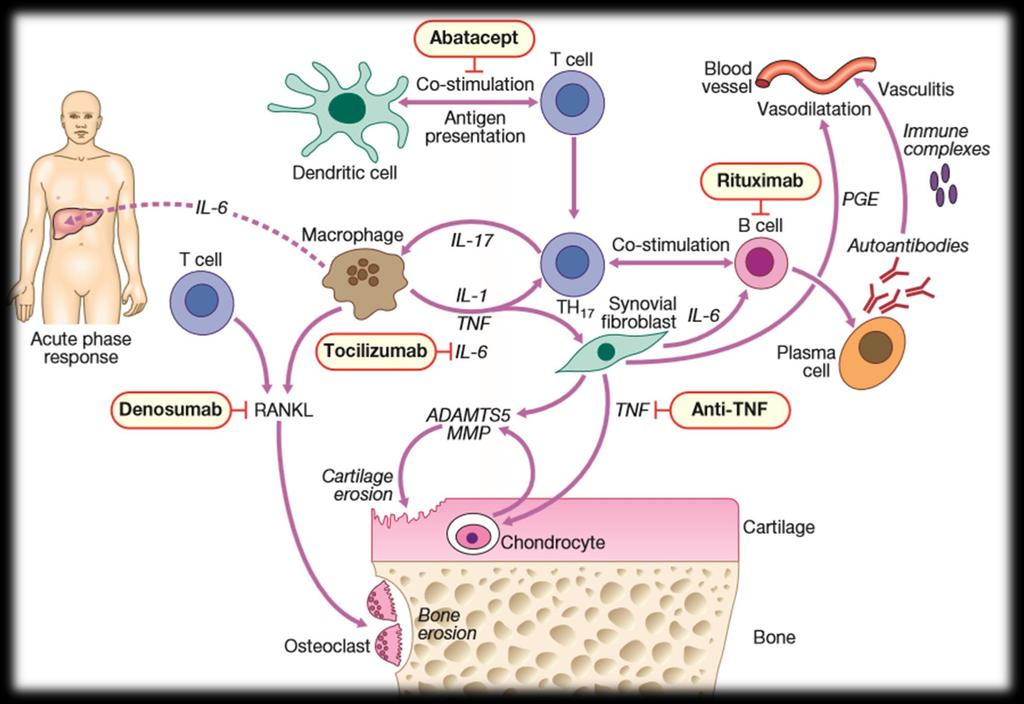
5 RA-Pathophysiology
6 Principles of treatment of RA Early diagnosis and commencement with DMARD treatment Alleviating or minimising pain Stopping the disease process Preventing deformity Minimising functional loss Regular monitoring for drug efficacy and toxicity Active patient participation in management of the condition. The Rheumatology Expert Group 2006

7 Treatment options in RA
8 Drug treatment in RA NSAIDS & Analgesics Corticosteroids DMARDs Synthetic DMARDs 1. Methotrexate 2. Hydroxychloroquine 3. Sulfasalazine 4. Leflunomide 5. Minocycline Biologic DMARDs Non-TNF 1. Abatacept 2. Rituximab 3. Tocilizumab Anti-TNF 4. Adalimumab 5. Etanercept 6. Infliximab 7. Certolizumab pegol 8. Golimumab
9 Indications for starting, resuming, adding, or switching DMARDs or biologic agents Target low disease activity or remission
10 Patient Activity Scale (PAS) or PAS-II (range 0 10) Remission: Low activity: Moderate activity: 3.71 to 8.0 High activity: 8.0 Routine Assessment of Patient Index Data 3 (range 0 10) Remission: Low activity: 1.0 to 2.0 Moderate activity: 2.0 to 4.0 High activity: 4.0 to 10 Clinical Disease Activity Index (range ) Remission: 2.8 Low activity: 2.8 to 10.0 Moderate activity: 10.0 to 22.0 High activity: 22 Disease Activity Score in 28 joints (range 0 9.4) Remission: 2.6 Low activity: 2.6 to 3.2 Moderate activity: 3.2 to 5.1 High activity: 5.1 Simplified Disease Activity Index (range ) Remission: 3.3 Low activity: 3.3 to 11.0 Moderate activity: 11.0 to 26 High activity: 26
11 Early RA (disease duration 6 months) DMARD monotherapy DMARD combination therapy (including double and triple therapy) Anti-TNF biologic with or without methotrexate
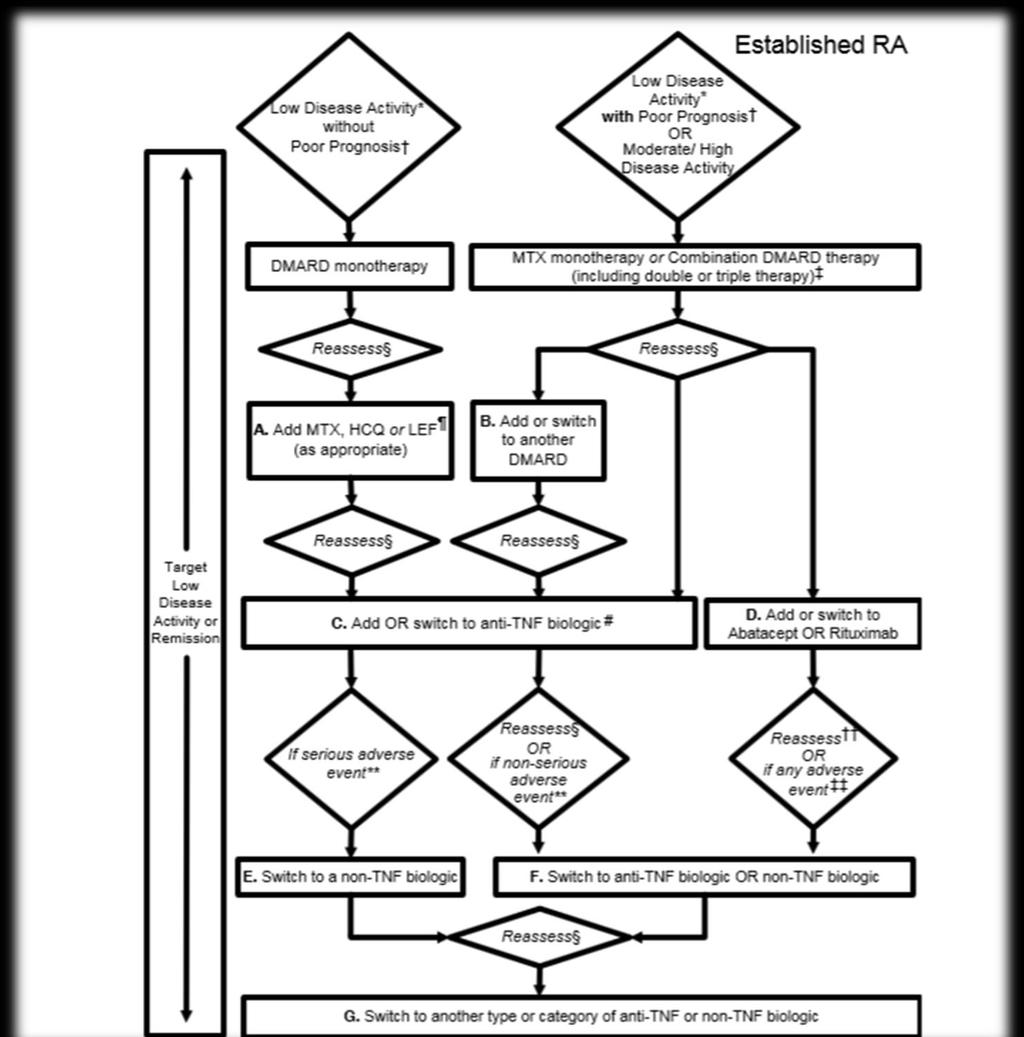
12 Established RA (disease duration 6 months or meeting the 1987 ACR RA classification criteria) Initiating and switching among DMARDs. Switching from DMARDs to biologic agents. Switching among biologic agents due to lack of benefit or loss of benefit Switching among biologic agents due to harms/adverse events
13 Early RA (disease duration 6 months) DMARD monotherapy Low disease activity Moderate or high disease activity with the absence of poor prognostic features
14 Poor prognostic factors Presence of 1 or more of the following features: Functional limitation (e.g., HAQ DI or similar valid tools), Extraarticular disease o Rheumatoid nodules, o RA vasculitis, o Felty s syndrome Positive rheumatoid factor or anti-ccp antibodies, or Bony erosions by radiograph
15 DMARD combination therapy (including double and triple therapy) Moderate or high disease activity plus poor prognostic features
16 Anti-TNF biologic with or without methotrexate High disease activity with poor prognostic features Infliximab is the only exception and the recommendation is to use it in combination with methotrexate, but not as monotherapy.
17 Established RA (disease duration 6 months or meeting the 1987 ACR RA classification criteria) Initiating and switching among DMARDs. After 3 months of DMARD monotherapy (in patients without poor prognostic features), deteriorates from low to moderate/high disease activity, then MTX, hydroxychloroquine, or leflunomide should be added After 3 months of treatment with MTX or MTX/ DMARD combination, moderate or high disease activity, add another non- MTX DMARD or switch to a different non-mtx DMARD.
18 Switching from DMARDs to biologic agents. Moderate or high disease activity after 3 months of MTX monotherapy or DMARD combination therapy switch to an anti-tnf biologic, abatacept, or rituximab After 3 months of intensified DMARD combination therapy or after a second DMARD, still has moderate or high disease activity, add or switch to an anti-tnf biologic
19 Switching among biologic agents due to lack of benefit or loss of benefit Moderate or high disease activity after 3 months of anti-tnf biologic therapy switch to another anti-tnf biologic or a non-tnf biologic Moderate or high disease activity after 6 months of a non-tnf biologic switch to another non-tnf biologic or an anti-tnf biologic
20 Switching among biologic agents due to harms/adverse events High disease activity after failing an anti-tnf biologic due to serious adverse event, switch to a non-tnf biologic Moderate or high disease activity after failing an anti-tnf biologic because of a nonserious adverse event, switch to another anti-tnf biologic or a non- TNF biologic Moderate or high disease activity after failing a non-tnf biologic because of an adverse event (serious or nonserious), switch to another non-tnf biologic or an anti-tnf biologic
21 Treatment of RA in Special situation
22 Use of biologic agents in RA patients with hepatitis, malignancy, or CHF, qualifying for more aggressive treatment Hepatitis B or C Etanercept can be used in RA patients with hepatitis C requiring RA treatment Biologic agent contraindicated in untreated chronic hepatitis B (disease not treated due to contraindications to treatment or intolerable adverse events) and RA patients with treated chronic hepatitis B with Child-Pugh class B and higher
23 Malignancies Can start or resume any biologic agent Patients who have been treated for solid malignancies or non melanoma skin cancer more than 5 years ago or Rituximab can only be used in RA patients with: previously treated solid malignancy within the last 5 years, previously treated nonmelanoma skin cancer within the last 5 years, previously treated melanoma skin cancer, or previously treated lymphoproliferative malignancys
24 CHF Anti-TNF biologic should not be used in RA patients with CHF with New York Heart Association (NYHA) class III or IV and who have an ejection fraction of 50% or less
25 TB screening for biologic agents Screening should be done to identify Latent TB Infection in all RA patients being considered for therapy with biologic agents
26 Vaccination in patients starting or currently receiving DMARDs or biologic agents Before starting a DMARD or a biologic agent patient should be vaccinated against with oall killed (pneumococcal, influenza intramuscular, and hepatitis B) orecombinant (human papillomavirus [HPV] vaccine for cervical cancer), and olive attenuated (herpes zoster) if not previously done vaccination is recommended as soon as possible
27 Pregnancy and RA In most patients with RA go into remission during pregnancy. Conception: methotrexate and leflunomide should be discontinued for at least 3 months before trying to conceive. Paracetamol: the oral analgesic of choice during pregnancy. Oral NSAIDs and selective COX-2 inhibitors: can be used after implantation up until the last trimester. Corticosteroids:to control disease flares; risk are hypertension, glucose intolerance and osteoporosis. Safe DMARDs : sulfasalazine, hydroxychloroquine, azathioprine or ciclosporin if required to control inflammation. Avoid DMARDs: methotrexate, leflunomide, cyclophosphamide, gold and penicillamine. Biological therapies: safety unclear. Breastfeeding: methotrexate, leflunomide, cyclophosphamide, ciclosporin, azathioprine, sulfasalazine and hydroxychloroquine are contraindicated.
28 ACR recommendation 2012
29 ACR recommendation 2012
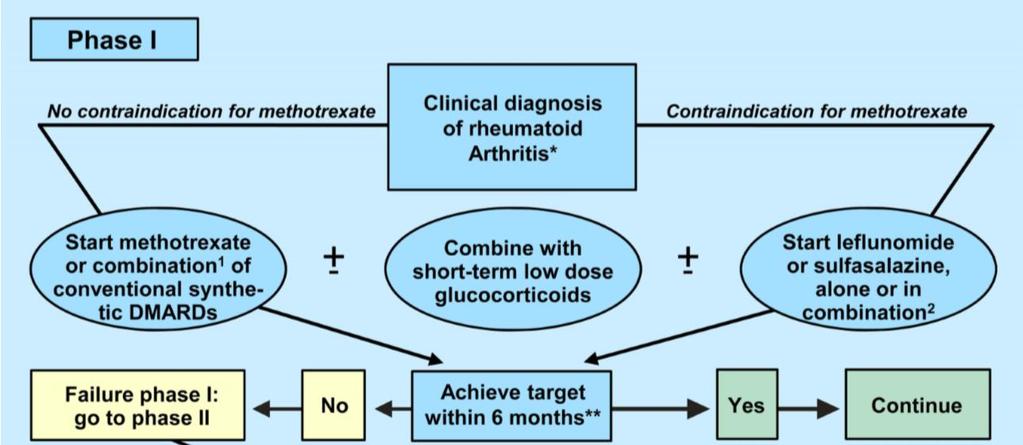
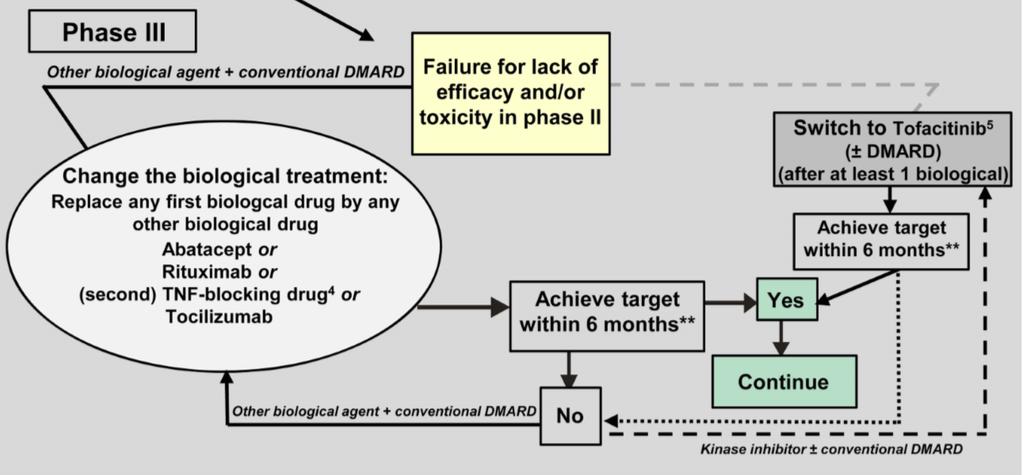
30 EULAR recommendations 2013


31 EULAR recommendations 2013
32 EULAR recommendations 2013
33 Low-dose glucocorticoids Should be considered as part of the initial treatment strategy (in combination with one or more csdmards) for up to 6 months, but should be tapered as rapidly as clinically feasible. Low dose refers primarily to a dose of 7.5 mg prednisone or equivalent per day
34 Proven capacity to increase clinical, functional and structural efficacy when combined with csdmards Combination has similar efficacy when compared with TNF inhibitors plus MTX (COBRA) Lower doses extended over a year or two, may increase DMARD activity and are even effective in this regard as monotherapy
35 Monotherapy is not specifically recommended and should only be used in exceptional cases when all other DMARDs have contraindications Task Force suggests using them only as bridging therapy and limiting their use to a maximum of 6 months then ideally tapering them
36 IMPROVED trial Very high rate of good outcomes using MTX plus low-dose glucocorticoids within a few months SAVE (Stop Arthritis Very Early) trial No efficacy of a single GC injection irrespective of added csdmards. Initial treatment of RA with low-dose prednisone plus MTX showed higher rates of remission and lower Health Assessment Questionnaire (HAQ) scores CAMERA II The MTX plus prednisone (10 mg/day) strategy was more effective than MTX plus placebo in reducing the progression of erosive joint damage MTX plus prednisone attained sustained remission at an earlier time point than MTX alone. Need for additional treatment was significantly lower in the MTX plus prednisone group than in the MTX monotherapy group There were no new safety concerns over 2 years beyond those previously reported.
37 Nonsteroidal anti-inflammatory drugs NSAIDs interfere with prostaglandin synthesis through inhibition of the enzyme cyclooxygenase (COX) Reduce swelling and pain Do not retard joint destruction Not sufficient to treat RA when used alone
38 6 placebo-controlled trials comparing celecoxib with placebo Risk of cardiovascular death, myocardial infarction, stroke, heart failure, or thromboembolic events increased after celecoxib treatment in a dose-dependent fashion
39 Analgesics Acetaminophen, tramadol, codeine, opiates, and various other analgesic can be used to reduce pain. These agents do not affect swelling or joint destruction.
40 Commonly used NSAIDs Ibuprofen Naproxen Ketoprofen, Piroxicam Indomethacine Diclofenac, and Selective COX 2 inhibitor- Celecoxib
41 SYNTHETIC DMARDs Methotrexate (MTX ) Sulfasalazine(SSZ) Hydroxychloroquine(HCQ) Leflunomide(LEF) Minocycline
42 MTX First treatment strategy in patients with active RA. Highly effective as monotherapy and in combination with glucocorticoids, other csdmards and bdmards Anchor drug in RA
43 As monotherapy with or without glucocorticoids leads to low disease activity states or 70% improvement in 25-50% of patients with early RA within 6-12 months. Some patients with low disease activity (defined as CDAI 10, DAS28<3.2, SDAI 11) may not need MTX and can do well on alternative csdmard therapies; Patients previously treated with other csdmards who should receive MTX at a sufficient dose and for sufficient time before progressing to potentially more intensive therapies.
44 Necessary steps when using MTX Dose optimization Optimal use of folic acid Recognition that the maximum effect of MTX is attained only after 4 6 months The optimal dose of mg a week with folate substitution, should be maintained for at least 8 weeks
45 When MTX is contraindicated (or early intolerance) Leflunomide or sulfasalazine should be considered as part of the (first) treatment strategy
46 Sulfasalazine SSZ monotherapy is recommended for patients with all disease durations without poor prognostic features and with all degrees of disease activity Dougados M et al. Combination therapy in early rheumatoid arthritis: a randomised, controlled, double blind 52 week clinical trial of sulphasalazine and methotrexate compared with the single components. Ann Rheum Dis 1999;58: Haagsma CJ et al.combination of sulphasalazine and methotrexate versus the single components in early rheumatoid arthritis: a randomized, controlled, double-blind, 52 week clinical trial. Br J Rheumatol 1997;36:
47 Meta-analysis of 15 randomized clinical trials support the effectiveness of SSZ as a treatment for RA Sulfasalazine treatment for rheumatoid arthritis: a meta analysis of 15 randomized trials. J Rheumatol Oct;26(10): Reduction in erosions has been reported with SZZ Van der Heijde D, Van Riel P, Nuver Swart I, GribnauF, Van de Putte L. Effects of Hydroxychloroquine and sulphasalazine on progression of joint damage in Rheumatoid arthritis. Lancet 1989;i: No teratogenicity is reported from over 2000 reports of pregnancy on the drug The drug be should be discontinued in pregnancy unless considered essential because of severe disease. The drug is considered safe in lactation, with little SSZ in the milk Esbjorner E, Jarnerot G, Wranne L. Sulphasalazine and sulphapyridine serum levels in children to mothers treated with sulphasalazine in pregnancy and lactation. Acta Paediatr Scand 76: ,1987 Mogadam M, Dobbins WO, Korelitz BI et al: pregnancy in inflammatory bowel disease: Effect of sulphasalazine and corticosteroid on fetal outcome. Gastroenterology 80: Day RO. Rheumatology. Klippel and Dieppe. Mosby publishers SAARDS
48 Comparison between HCQ & SSZ Variable SSZ HCQ P value lack of efficacy dropouts 5% 15% p = ESR 43% 26% p = 0.10 Morning stiffness 59% 40% p =0.09
49 Hydroxychloroquine Milder drugs Chloroquine is generally used for milder disease or in combination therapy It takes about three to six months to demonstrate efficacy Double blind studies show efficacy in percent of patients Regular 6-12 monthly eye checks for field-testing. Decrease disease activity of at least 30% has been described in up to 63% of patients. Bell C Y N. Hydroxychloroquine sulphate in rheumatoid arthritis: long term response rate and predictive parameters. Am J Med 1983; 75: Husain Z, Runge L A. Treatment complications of rheumatoid arthritis with gold, hydroxychloroquine, D-penicillamine and levamisole. J Rheumatol 1980; 7:
50 There is no influence on erosion progression compared to SSZ Van der Heijde D, Van Riel P, Nuver Swart I, GribnauF, Van de Putte L. Effects of Hydroxychloroquine and sulphasalazine on progression of joint damage in Rheumatoid arthritis. Lancet 1989;i: Felson DT, Anderson JA, Meenan RF. The comparative efficacy and toxicity of second line drugs in rheumatoid arthritis. Results of 2 meta-analyses Arthritis Rheum;33;10, reports exist of pregnancy in rheumatoid arthritis patients on anti-malarials. No reports of adverse fetal effect Nelson JL, Ostensen M. Pregnancy and rheumatoid arthritis. Rheum Dis Clin N Am. 1997;23,1: Parke AL. Antimalarial drugs, systemic lupus erythematosus and pregnancy. J Rheumatol 25: ,1988
51 The combination of MTX and HQ was the most popular DMARDs prescribed in the US and Canada Manathip Osiri, Pirom Kamolratanakul, Andreas Maetzel, Peter Tugwell. Cost effectiveness analysis of disease modifying antirheumatic drugs in rheumatoid arthritis. Rheumatol Int (2007)27:
52 Leflunomide 1. Reduction of signs and symptoms 2. Inhibition of structural damage 3. Improvement in physical function
53 Comparisons 95%Confidence Interval p Value US301 LEF vs. PL (12, 32) < MTX vs. PL (8, 30) < LEF vs. MTX (-4, 16) NS MN301 LEF vs. PL (7, 33) SSZ vs. PL (4, 29) LEF vs. SSZ (-8, 16) NS MN302 LEF vs. MTX (-19, -7) <0.0001
54 No consistent differences were demonstrated between LEF and MTX or between LEF and SSZ.
55 Inhibition of structural damage Sharp, JT. Scoring Radiographic Abnormalities in Rheumatoid Arthritis, Radiologic Clinics of North America, 1996; vol. 34, pp. 233 to 241
56 LEF was statistically significantly superior to placebo in inhibiting the progression of disease by the Sharp Score. No consistent differences were demonstrated between LEF and MTX or between LEF and SSZ.

57 Improvement in physical function
58 The combination of LEF and MTX was effective and well tolerated in the treatment of active RA patients. This combination may be a useful option as an initial treatment for active RA before starting biological agents.
59 Biologic DMARDs: Anti-TNF Etanercept Infliximab Adalimumab Certolizumab Golimumab Non TNF Rituximab Anakinra Abatacept Tocilizumab Tofacitinib
60
61 Consensus statements do not recommend their use until at least one nonbiologic DMARD, usually MTX, has been administered without sufficient success Severe adverse events generation of antibodies against these compounds emergence of antinuclear antibodies (ANAs) drug-induced lupus-like syndromes, and infections (including tuberculosis) Immunogenicity has been shown to occur in adalimumab and infliximab reducing their efficacy
62

63 Adalimumab
64 Tofacitinib Oral Biologic RA Treatment Approved in November of 2012 New class of drugs called Janus Kinase (JAK) inhibitors For moderate-to-severe RA who have had an inadequate response to methotrexate. Can be used alone or with nonbiologic DMARDs such as methotrexate Side effects such as infections, cancer, and stomach or intestinal tears.
65 Efficacy of Tofacitinib on ACR20 response criteria at 24 weeks
66 Biological DMARD±conventional synthetic DMARD versus conventional synthetic DMARD Biological DMARD+MTX combination versus conventional synthetic DMARD HIT HARD study ADA+MTX more effective than moderate dose MTX IMAGE study bdmard+mtx were superior to placebo+mtx in MTX-naive RA (RR (95% CI) 1.68 (1.54 to 1.84) for ACR 70 responses) bdmard+mtx were superior to placebo+mtx in MTX-IR (RR (95% CI) 4.07 (3.21 to 5.17)) bdmard+csdmard more effective than csdmard in mixed DMARD IR (RR (95% CI) 4.74 (2.63 to 8.56)
67 Biological DMARD monotherapy versus conventional synthetic DMARD FUNCTION study Efficacy and safety of TCZ 8 mg/kg monotherapy vs MTX monotherapy TCZ 8 mg/kg monotherapy group met its primary endpoint (DAS28 ESR remission at 6 months) 38.7% vs 15% in MTX monotherapy group, respectively, p Radiographic progression at 12 months was lower in those receiving TCZ than MTX, and lowest in the TCZ 8 mg/kg+mtx combination group.
68 Biological DMARD+MTX combination versus biological DMARD monotherapy Open-label JESMR study ETN+MTX was superior to ETN monotherapy for clinical outcomes SURPRISE study and ACT-RAY study TCZ with MTX (combination) with switching from MTX to TCZ monotherapy (MTX-withdrawal). Similar ACR 70 responses were seen for both groups at 6months 12-month data from the ACT-RAY study showed higher proportions of DAS28 remission (DAS28 remission37% vs 46%, p=0.03) and radiographic non-progression( 86% vs 92%, p=0.007 ) in the TCZ monotherapy and TCZ +MTX groups, respectively)
69 Head-to-head biological DMARD studies The ADACTA study evaluated bdmard monotherapy, comparing TCZ versus ADA. Significantly greater change in DAS28 from baseline to 6 months in the TCZ 8 mg/kg monotherapy versus ADA 40mg SC monotherapy group (95% CI): 1.5 ( 1.8 to 1.1), p<0.0001).
70 Conventional combination treatment versus biological treatment in methotrexate-refractory early rheumatoid arthritis Ronald F van Vollenhoven, Pierre Geborek et al. Conventional combination treatment versus biological treatment in methotrexate-refractory early rheumatoid arthritis: 2 year follow-up of the randomised, non-blinded, parallel-group Swefot trial. Lancet 2012; 379:
71 TAKE HOME MESSAGES Drug selection should be based on Early vs established disease Presence or absence of poor prognostic factors Efficacy Adverse events and Cost-benefit and Evidenced based trials MTX remains in the corner stone in the treatment of RA Biologic DMARDs can be used when situation permits. Combination treatment of MTX with other DMARDs showed better efficacy

72 Thank You
Treatment of Rheumatoid Arthritis: The Past, the Present and the Future
 Treatment of Rheumatoid Arthritis: The Past, the Present and the Future Lai-Ling Winchow FCP(SA) Cert Rheum(SA) Chris Hani Baragwanath Academic Hospital University of the Witwatersrand Outline of presentation
Treatment of Rheumatoid Arthritis: The Past, the Present and the Future Lai-Ling Winchow FCP(SA) Cert Rheum(SA) Chris Hani Baragwanath Academic Hospital University of the Witwatersrand Outline of presentation
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Update on the Treatment of Rheumatoid Arthritis Sabrina Fallavollita MDCM McGill University Canadian Society of Internal Medicine
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Update on the Treatment of Rheumatoid Arthritis Sabrina Fallavollita MDCM McGill University Canadian Society of Internal Medicine
James R. O Dell, M.D. University of Nebraska Medical Center
 Not everyone in the world needs a biologic: Lessons from TEAR and RACAT James R. O Dell, M.D. University of Nebraska Medical Center Disclosure Declaration James O Dell, MD Advisory Board for Crescendo,
Not everyone in the world needs a biologic: Lessons from TEAR and RACAT James R. O Dell, M.D. University of Nebraska Medical Center Disclosure Declaration James O Dell, MD Advisory Board for Crescendo,
Fml Limits. Azathioprine (Imuran) 50mg, 75mg, 100mg - $26.85 Cyclosporine, 25mg, 100mg. $ Leflunomide (Arava) 10mg Tablet - $144.
 50mg, 75mg, 100mg - $26.85 Cyclosporine, 25mg, 100mg. $ Leflunomide (Arava) 10mg Tablet - $144.") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Rheumatoid Arthritis (RA) P&T DATE: 2/15/2017 CLASS: Rheumatology/Anti-inflammatory Disorders REVIEW HISTORY 2/16, 5/15,
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Rheumatoid Arthritis (RA) P&T DATE: 2/15/2017 CLASS: Rheumatology/Anti-inflammatory Disorders REVIEW HISTORY 2/16, 5/15,
New Evidence reports on presentations given at EULAR Tocilizumab for the Treatment of Rheumatoid Arthritis
 New Evidence reports on presentations given at EULAR 2012 Tocilizumab for the Treatment of Rheumatoid Arthritis Report on EULAR 2012 presentations Tocilizumab monotherapy is superior to adalimumab monotherapy
New Evidence reports on presentations given at EULAR 2012 Tocilizumab for the Treatment of Rheumatoid Arthritis Report on EULAR 2012 presentations Tocilizumab monotherapy is superior to adalimumab monotherapy
Recommendations for RA management: what has changed?
 The 2016 Update of the EULAR Recommendations for RA management: what has changed? Baltics Rheumatology Conference Vilnius, September 21-22 Prof. Diego Kyburz University Hospital of Basel Switzerland Multiple
The 2016 Update of the EULAR Recommendations for RA management: what has changed? Baltics Rheumatology Conference Vilnius, September 21-22 Prof. Diego Kyburz University Hospital of Basel Switzerland Multiple
Rheumatoid arthritis
 Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Practical RA Treatment: James R. O Dell, M.D. University of Nebraska Medical Center May 24, 2014
 Practical RA Treatment: 2014 James R. O Dell, M.D. University of Nebraska Medical Center May 24, 2014 Disclosures James R. O Dell PI of Multinational RA trial supported by VA and NIH (NIAMS) that receives
Practical RA Treatment: 2014 James R. O Dell, M.D. University of Nebraska Medical Center May 24, 2014 Disclosures James R. O Dell PI of Multinational RA trial supported by VA and NIH (NIAMS) that receives
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Comparative Effectiveness Studies of Biologics Learning Objectives Understand the motivation for comparative effectiveness research
Annual Rheumatology & Therapeutics Review for Organizations & Societies Comparative Effectiveness Studies of Biologics Learning Objectives Understand the motivation for comparative effectiveness research
Rheumatoid Arthritis. By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University
 Department of Clinical Pharmacy, Shahid Beheshti Medical University") Rheumatoid Arthritis By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University Introduction RA is a Chronic, Systemic, Inflammatory disorder of unknown etiology
Rheumatoid Arthritis By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University Introduction RA is a Chronic, Systemic, Inflammatory disorder of unknown etiology
Rheumatoid arthritis 2010: Treatment and monitoring
 October 12, 2010 By Yusuf Yazici, MD [1] The significant changes in the way rheumatoid arthritis has been managed include earlier, more aggressive treatment with combination therapy. Significant changes
October 12, 2010 By Yusuf Yazici, MD [1] The significant changes in the way rheumatoid arthritis has been managed include earlier, more aggressive treatment with combination therapy. Significant changes
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0043I Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0043I Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 284.9 T2 Effective Date: June 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 284.9 T2 Effective Date: June 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") UnitedHealthcare Community Plan Medical Benefit Drug Policy ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION Policy Number: CS2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Community Plan Medical Benefit Drug Policy ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION Policy Number: CS2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
DMARD s in Clinical Practice
 DMARD s in Clinical Practice Professor Md. Mahabubul Islam Majumder Professor & Head, Department of Medicine Comilla Medical College, Comilla Bangladesh Disease-modifying antirheumatic drugs (DMARDs) A
DMARD s in Clinical Practice Professor Md. Mahabubul Islam Majumder Professor & Head, Department of Medicine Comilla Medical College, Comilla Bangladesh Disease-modifying antirheumatic drugs (DMARDs) A
Coverage Criteria: Express Scripts, Inc. monograph dated 12/15/ months or as otherwise noted by indication
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
Figure 1. Study flow diagram. Reasons for withdrawal during the extension phase are included in the flow diagram. 508 patients enrolled and randomized
 508 patients enrolled and randomized 126 assigned to sequential monotherapy (group 1) 121 assigned to step-up combination therapy (group 2) 133 assigned to initial combination therapy with prednisone (group
508 patients enrolled and randomized 126 assigned to sequential monotherapy (group 1) 121 assigned to step-up combination therapy (group 2) 133 assigned to initial combination therapy with prednisone (group
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Rheumatoid Arthritis. Improving Outcomes in RA: Three Pillars. RA: Chronic Joint Destruction and Disability What We Try to Prevent
 Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") UnitedHealthcare Commercial Medical Benefit Drug Policy SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION Policy Number: PHA031 Effective Date: March 1, 2019 Table of Contents Page COVERAGE RATIONALE...
UnitedHealthcare Commercial Medical Benefit Drug Policy SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION Policy Number: PHA031 Effective Date: March 1, 2019 Table of Contents Page COVERAGE RATIONALE...
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
Rheumatoid Arthritis Update
 Rheumatoid Arthritis Update Beth Valashinas, DO, FACOI, FACR Disclosures Speaker for AbbVie Pharmaceuticals Learning Objectives Upon completion of this session, participants should be able to discuss:
Rheumatoid Arthritis Update Beth Valashinas, DO, FACOI, FACR Disclosures Speaker for AbbVie Pharmaceuticals Learning Objectives Upon completion of this session, participants should be able to discuss:
Relative effect (95% CI) RR LOW 2,3 due to indirectness, imprecision. RR 1.45 (0.43 to 4.84) due to indirectness, imprecision. (0.18 to 20.
 RR LOW 2,3 due to indirectness, imprecision. RR 1.45 (0.43 to 4.84) due to indirectness, imprecision. (0.18 to 20.") Appendix: Evidence Reports Question In patients with early RA with moderate or high disease activity, who are DMARD-naive, what is the impact of combination double DMARD therapy vs. mono-dmard therapy
Appendix: Evidence Reports Question In patients with early RA with moderate or high disease activity, who are DMARD-naive, what is the impact of combination double DMARD therapy vs. mono-dmard therapy
ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
CDEC FINAL RECOMMENDATION
 CDEC FINAL RECOMMENDATION TOFACITINIB (Xeljanz Pfizer Canada Inc.) Indication: Rheumatoid Arthritis Recommendation: The Canadian Drug Expert Committee (CDEC) recommends that tofacitinib be listed, in combination
CDEC FINAL RECOMMENDATION TOFACITINIB (Xeljanz Pfizer Canada Inc.) Indication: Rheumatoid Arthritis Recommendation: The Canadian Drug Expert Committee (CDEC) recommends that tofacitinib be listed, in combination
Rheumatoid arthritis in adults: diagnosis and management
 National Institute for Health and Care Excellence Consultation Rheumatoid arthritis in adults: diagnosis and management Evidence review F DMARDs NICE guideline CG79 Intervention evidence review January
National Institute for Health and Care Excellence Consultation Rheumatoid arthritis in adults: diagnosis and management Evidence review F DMARDs NICE guideline CG79 Intervention evidence review January
What I Have Learned Over the Years - Keystone s Top 10 -
 What I Have Learned Over the Years - Keystone s Top 10 - Edward Keystone, MD FRCP(C) Professor of Medicine University of Toronto, CANADA Ontario Rheumatology Association Meeting Muskoka, Canada Sunday,
What I Have Learned Over the Years - Keystone s Top 10 - Edward Keystone, MD FRCP(C) Professor of Medicine University of Toronto, CANADA Ontario Rheumatology Association Meeting Muskoka, Canada Sunday,
Biologic therapy for Rheumatoid arthritis. Paul Etau Ekwom Physician and Rheumatologist
 Biologic therapy for Rheumatoid arthritis Paul Etau Ekwom Physician and Rheumatologist Objectives Case presentation of patient with rheumatoid arthritis on a biologic therapy. Discuss biologic therapy
Biologic therapy for Rheumatoid arthritis Paul Etau Ekwom Physician and Rheumatologist Objectives Case presentation of patient with rheumatoid arthritis on a biologic therapy. Discuss biologic therapy
Introduction. Rheumatoid Arthritis. Rheumatoid Arthritis. Arthritis vs Rheumatoid Arthritis
 Rheumatoid Arthritis Stuart Weisman, MD Boulder Medical Center, P.C. 303-622-3724 Introduction What is rheumatoid arthritis? How is it different than arthritis? What are the symptoms? How is it diagnosed?
Rheumatoid Arthritis Stuart Weisman, MD Boulder Medical Center, P.C. 303-622-3724 Introduction What is rheumatoid arthritis? How is it different than arthritis? What are the symptoms? How is it diagnosed?
Helpline No:
 ARTHRITIS FOUNDATION Registered Nonprofit Organisation - No. 002-847 NPO Helpline No: 0861 30 30 30 DRUGS AND ARTHRITIS This information leaflet is published by the Arthritis Foundation as part of our
ARTHRITIS FOUNDATION Registered Nonprofit Organisation - No. 002-847 NPO Helpline No: 0861 30 30 30 DRUGS AND ARTHRITIS This information leaflet is published by the Arthritis Foundation as part of our
Evaluating Newer Targeted Therapies for Patients with Rheumatoid Arthritis: Addressing Unmet Needs in the Primary Care Practice
 Evaluating Newer Targeted Therapies for Patients with Rheumatoid Arthritis: Addressing Unmet Needs in the Primary Care Practice Provided by Integrity Continuing Education, Inc. Supported by an educational
Evaluating Newer Targeted Therapies for Patients with Rheumatoid Arthritis: Addressing Unmet Needs in the Primary Care Practice Provided by Integrity Continuing Education, Inc. Supported by an educational
Rheumatoid Arthritis: Challenges and Opportunities in the Evolving Treatment Landscape ReachMD Page 1 of 9
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
The Hospital for Sick Children Technology Assessment at SickKids (TASK)
") The Hospital for Sick Children Technology Assessment at SickKids (TASK) THE USE OF BIOLOGIC RESPONSE MODIFIERS IN POLYARTICULAR-COURSE JUVENILE IDIOPATHIC ARTHRITIS Report No. 2010-01 Date: January 11,
The Hospital for Sick Children Technology Assessment at SickKids (TASK) THE USE OF BIOLOGIC RESPONSE MODIFIERS IN POLYARTICULAR-COURSE JUVENILE IDIOPATHIC ARTHRITIS Report No. 2010-01 Date: January 11,
Abatacept (Orencia) for active rheumatoid arthritis. August 2009
 for active rheumatoid arthritis. August 2009") Abatacept (Orencia) for active rheumatoid arthritis August 2009 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Abatacept (Orencia) for active rheumatoid arthritis August 2009 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
NIHR Innovation Observatory Evidence Briefing: November 2017
 NIHR Innovation Observatory Evidence Briefing: November 2017 Upadacitinib for adults with moderate to severe active rheumatoid arthritis after conventional synthetic disease-modifying anti-rheumatic drugs
NIHR Innovation Observatory Evidence Briefing: November 2017 Upadacitinib for adults with moderate to severe active rheumatoid arthritis after conventional synthetic disease-modifying anti-rheumatic drugs
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
MMS Pharmacology Lecture 2. Antirheumatic drugs. Dr Sura Al Zoubi
 MMS Pharmacology Lecture 2 Antirheumatic drugs Dr Sura Al Zoubi Revision Rheumatoid Arthritis Definition (RA): is the most common systemic inflammatory disease characterized by symmetrical inflammation
MMS Pharmacology Lecture 2 Antirheumatic drugs Dr Sura Al Zoubi Revision Rheumatoid Arthritis Definition (RA): is the most common systemic inflammatory disease characterized by symmetrical inflammation
Medication Policy Manual. Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013
 Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
Rheumatoid Arthritis: When to Start and when to Stop anti-tnf Therapy
 Rheumatoid Arthritis: When to Start and when to Stop anti-tnf Therapy [ Cuando iniciar o detener la tx anti-tnf?] Asociacion Costatarricense Medicina Interna August 7, 2015 Arthur Weinstein, MD, FACP,
Rheumatoid Arthritis: When to Start and when to Stop anti-tnf Therapy [ Cuando iniciar o detener la tx anti-tnf?] Asociacion Costatarricense Medicina Interna August 7, 2015 Arthur Weinstein, MD, FACP,
Comments from Wyeth on the Assessment Report for the appraisal of Enbrel in RA General Comments
 General Comments The TAR economic model is a complex model that attempts to reflect the multiple treatment options and pathways an RA patient can follow. This model demonstrates that it would be cost effective
General Comments The TAR economic model is a complex model that attempts to reflect the multiple treatment options and pathways an RA patient can follow. This model demonstrates that it would be cost effective
- Clinical Background, Motivation and my Experience at F2F meeting
 Predicting randomized clinical trial results with realworld evidence: A case study in the comparative safety of tofacitinib, adalimumab and etanercept in patients with rheumatoid arthritis - Clinical Background,
Predicting randomized clinical trial results with realworld evidence: A case study in the comparative safety of tofacitinib, adalimumab and etanercept in patients with rheumatoid arthritis - Clinical Background,
Review. One year in review 2017: novelties in the treatment of rheumatoid arthritis
 Review One year in review 2017: novelties in the treatment of rheumatoid arthritis F. Ferro 1, E. Elefante 1, N. Luciano 1, R. Talarico 1, M. Todoerti 2 1 Rheumatology Unit, Department of Clinical and
Review One year in review 2017: novelties in the treatment of rheumatoid arthritis F. Ferro 1, E. Elefante 1, N. Luciano 1, R. Talarico 1, M. Todoerti 2 1 Rheumatology Unit, Department of Clinical and
New Evidence reports on presentations given at EULAR Tocilizumab for the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis
 New Evidence reports on presentations given at EULAR 2011 Tocilizumab for the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2011 presentations Benefit of continuing
New Evidence reports on presentations given at EULAR 2011 Tocilizumab for the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2011 presentations Benefit of continuing
Assessment group response to Wyeth commentary on assessment report
 Assessment group response to Wyeth commentary on assessment report Subject & Wyeth s comments related section/page Model patient The TAR economic model is a complex model that attempts to reflect the population
Assessment group response to Wyeth commentary on assessment report Subject & Wyeth s comments related section/page Model patient The TAR economic model is a complex model that attempts to reflect the population
Alabama Medicaid Pharmacist
 Published Quarterly by Health Information Designs, LLC, Fall 2013 edition A Service of Alabama Medicaid PDL Update Effective October 1, 2013, the Alabama Medicaid Agency will update the Preferred Drug
Published Quarterly by Health Information Designs, LLC, Fall 2013 edition A Service of Alabama Medicaid PDL Update Effective October 1, 2013, the Alabama Medicaid Agency will update the Preferred Drug
2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients
 2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients Dr Alberta Hoi Rheumatologist MBBS, FRACP, PhD NEW ERA IN MUSCULOSKELETAL MEDICINE New drugs - Biologics,
2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients Dr Alberta Hoi Rheumatologist MBBS, FRACP, PhD NEW ERA IN MUSCULOSKELETAL MEDICINE New drugs - Biologics,
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies RA: Update on Biologic Therapy and Step-Up or Step-Down Therapeutic Options Learning Objectives Describe the importance of remission
Annual Rheumatology & Therapeutics Review for Organizations & Societies RA: Update on Biologic Therapy and Step-Up or Step-Down Therapeutic Options Learning Objectives Describe the importance of remission
SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") UnitedHealthcare Oxford Clinical Policy SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION Policy Number: PHARMACY 292.4 T2 Effective Date: April 1, 2018 Table of Contents Page INSTRUCTIONS FOR
UnitedHealthcare Oxford Clinical Policy SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION Policy Number: PHARMACY 292.4 T2 Effective Date: April 1, 2018 Table of Contents Page INSTRUCTIONS FOR
(tofacitinib) are met.
 are met.") Xeljanz (tofacitinib) Policy Number: 5.01. 560 Origination: 3/2014 Last Review: 3/2014 Next Review: 3/2015 Policy BCBSKC will provide coverage for Xeljanz (tofacitinib) when it is determined to be medically
Xeljanz (tofacitinib) Policy Number: 5.01. 560 Origination: 3/2014 Last Review: 3/2014 Next Review: 3/2015 Policy BCBSKC will provide coverage for Xeljanz (tofacitinib) when it is determined to be medically
Treat to a Target The New Paradigm in the Management of RA. Boulos Haraoui, MD FRCPC Université de Montréal Institut de rhumatologie de Montréal
 Treat to a Target The New Paradigm in the Management of RA Boulos Haraoui, MD FRCPC Université de Montréal Institut de rhumatologie de Montréal Disclosure Dr Boulos Haraoui Advisor/Research Grants/Speakers
Treat to a Target The New Paradigm in the Management of RA Boulos Haraoui, MD FRCPC Université de Montréal Institut de rhumatologie de Montréal Disclosure Dr Boulos Haraoui Advisor/Research Grants/Speakers
Effective Health Care Program
 Comparative Effectiveness Review Number 28 Effective Health Care Program Disease-Modifying Antirheumatic Drugs (DMARDs) in Children With Juvenile Idiopathic Arthritis (JIA) Executive Summary Background
Comparative Effectiveness Review Number 28 Effective Health Care Program Disease-Modifying Antirheumatic Drugs (DMARDs) in Children With Juvenile Idiopathic Arthritis (JIA) Executive Summary Background
Pain or stiffness in joints after periods of inactivity or excessive use
 Arthritis Awareness* Some older adults call it Arthur ; others refer to it as their constant compassion, but most describe it as extremely painful Arthritis is a chronic joint disease It is commonly believed
Arthritis Awareness* Some older adults call it Arthur ; others refer to it as their constant compassion, but most describe it as extremely painful Arthritis is a chronic joint disease It is commonly believed
Dr. Lyubomir Marinchev Chief of Rheumatology Department, MHAT SOFIAMED, Sofia, Bulgaria
 Dr. Lyubomir Marinchev Chief of Rheumatology Department, MHAT SOFIAMED, Sofia, Bulgaria Inter-Balkan meeting Open the frontiers and exchange of experiences, 27 th April 2013, Rhodes, Greece Patients with
Dr. Lyubomir Marinchev Chief of Rheumatology Department, MHAT SOFIAMED, Sofia, Bulgaria Inter-Balkan meeting Open the frontiers and exchange of experiences, 27 th April 2013, Rhodes, Greece Patients with
Rheumatoid Arthritis. Update in Rheumatoid Arthritis Diagnosis and Therapy. RA: Chronic Joint Destruction and Disability What We Try to Prevent
 Rheumatoid Arthritis Update in Rheumatoid Arthritis Diagnosis and Therapy Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid Arthritis Clinic
Rheumatoid Arthritis Update in Rheumatoid Arthritis Diagnosis and Therapy Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid Arthritis Clinic
Clinical Guideline. Rheumatoid Arthritis Drug Treatment Pathway
 Clinical Guideline Rheumatoid Arthritis Drug Treatment Pathway Guideline Summary This clinical guideline outlines the biologic treatment pathway for adult patients with rheumatoid arthritis. Bexley/Bromley/Greenwich/Lambeth/Lewisham
Clinical Guideline Rheumatoid Arthritis Drug Treatment Pathway Guideline Summary This clinical guideline outlines the biologic treatment pathway for adult patients with rheumatoid arthritis. Bexley/Bromley/Greenwich/Lambeth/Lewisham
ORENCIA (abatacept) Demonstrates Comparable Efficacy to Humira ( adalimumab
 Demonstrates Comparable Efficacy to Humira ( adalimumab") ORENCIA (abatacept) Demonstrates Comparable Efficacy to Humira (adalimumab) in Patients with Moderate to Severe Rheumatoid Arthritis in First Head-to-Head Study of These Agents ORENCIA demonstrated comparable
ORENCIA (abatacept) Demonstrates Comparable Efficacy to Humira (adalimumab) in Patients with Moderate to Severe Rheumatoid Arthritis in First Head-to-Head Study of These Agents ORENCIA demonstrated comparable
Horizon Scanning Centre November Secukinumab for active and progressive psoriatic arthritis. SUMMARY NIHR HSC ID: 5330
 Horizon Scanning Centre November 2012 Secukinumab for active and progressive psoriatic arthritis. SUMMARY NIHR HSC ID: 5330 Secukinumab is a high-affinity fully human monoclonal antibody that antagonises
Horizon Scanning Centre November 2012 Secukinumab for active and progressive psoriatic arthritis. SUMMARY NIHR HSC ID: 5330 Secukinumab is a high-affinity fully human monoclonal antibody that antagonises
New Evidence reports on presentations given at ACR Improving Radiographic, Clinical, and Patient-Reported Outcomes with Rituximab
 New Evidence reports on presentations given at ACR 2009 Improving Radiographic, Clinical, and Patient-Reported Outcomes with Rituximab From ACR 2009: Rituximab Rituximab in combination with methotrexate
New Evidence reports on presentations given at ACR 2009 Improving Radiographic, Clinical, and Patient-Reported Outcomes with Rituximab From ACR 2009: Rituximab Rituximab in combination with methotrexate
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of:
 blockers indicated for the treatment of:") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Rheumatology Therapeutics: Perioperative DMARD Management, Infection and Malignancy Risks, Vaccination Considerations. Heather Hansen, MD
 Rheumatology Therapeutics: Perioperative DMARD Management, Infection and Malignancy Risks, Vaccination Considerations Heather Hansen, MD Objectives Know Broad Categories of Rheumatoid Arthritis Medications
Rheumatology Therapeutics: Perioperative DMARD Management, Infection and Malignancy Risks, Vaccination Considerations Heather Hansen, MD Objectives Know Broad Categories of Rheumatoid Arthritis Medications
Reminder. Faculty Affiliation. Complete Session Pre- and Post-Test Complete Online Session Evaluation at End of Session. **Links found in Event App
 Overcoming Barriers to the Early Recognition and Diagnosis of Rheumatoid Arthritis in Real-world Practice: Strategies to Expedite Treatment to Remission Provided by Integrity Continuing Education, Inc.
Overcoming Barriers to the Early Recognition and Diagnosis of Rheumatoid Arthritis in Real-world Practice: Strategies to Expedite Treatment to Remission Provided by Integrity Continuing Education, Inc.
RHEUMATOID ARTHRITIS DRUGS
 Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
Xeljanz. Xeljanz, Xeljanz XR (tofacitinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 6 Last Review Date: March 16, 2018 Xeljanz Description Xeljanz, Xeljanz
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 6 Last Review Date: March 16, 2018 Xeljanz Description Xeljanz, Xeljanz
CIMZIA (certolizumab pegol)
") Pre - PA Allowance None Prior-Approval Requirements Age Diagnoses 18 years of age or older Patient must have ONE of the following: 1. Moderate to severe Crohn s Disease (CD) a. Inadequate response, intolerance
Pre - PA Allowance None Prior-Approval Requirements Age Diagnoses 18 years of age or older Patient must have ONE of the following: 1. Moderate to severe Crohn s Disease (CD) a. Inadequate response, intolerance
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta480
 Tofacitinib for moderate to severeere rheumatoid arthritis Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta480 NICE 2018. All rights reserved. Subject to Notice of rights
Tofacitinib for moderate to severeere rheumatoid arthritis Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta480 NICE 2018. All rights reserved. Subject to Notice of rights
ACTEMRA (tocilizumab)
") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Lecture: Rheumatology Update on DMARDs in Common Rheumatologic Diseases for the Family Physician. Sco Jay Harris, DO, FACFR
 Lecture: Rheumatology Update on DMARDs in Common Rheumatologic Diseases for the Family Physician Sco Jay Harris, DO, FACFR UPDATE ON DMARDS, BIOLOGICALS, CYTOKINE INHIBITORS/B CELL DEPLETIONS/CO-STIMULATION
Lecture: Rheumatology Update on DMARDs in Common Rheumatologic Diseases for the Family Physician Sco Jay Harris, DO, FACFR UPDATE ON DMARDS, BIOLOGICALS, CYTOKINE INHIBITORS/B CELL DEPLETIONS/CO-STIMULATION
THERAPY in RHEUMATOLOGY
 THERAPY in RHEUMATOLOGY RA OA AS Systemic diseases SLE Dermatomyositis Scleroderma Gout Rheumatic fever Lyme disease RHEUMATOID ARTRHRITIS Education Build a cooperative long-term relationship Use materials
THERAPY in RHEUMATOLOGY RA OA AS Systemic diseases SLE Dermatomyositis Scleroderma Gout Rheumatic fever Lyme disease RHEUMATOID ARTRHRITIS Education Build a cooperative long-term relationship Use materials
Perioperative Medicine:
 Perioperative Medicine: Management of rheumatologic agents Divya Gollapudi, MD May 2016 Medical Operative Consult Clinic Harborview Medical Center Your patient Ms. L is a 55 year-old F w/ h/o RA who presents
Perioperative Medicine: Management of rheumatologic agents Divya Gollapudi, MD May 2016 Medical Operative Consult Clinic Harborview Medical Center Your patient Ms. L is a 55 year-old F w/ h/o RA who presents
Dr Daniel Ching. Rheumatology Therapeutic Clinical Trials Centre Timaru
 Dr Daniel Ching Rheumatology Therapeutic Clinical Trials Centre Timaru Therapeutic Advances in Rheumatology GP CME Meeting, Dunedin, 18.08.2013 Dr Daniel Ching, MB FRCP FRACP Consultant Rheumatologist,
Dr Daniel Ching Rheumatology Therapeutic Clinical Trials Centre Timaru Therapeutic Advances in Rheumatology GP CME Meeting, Dunedin, 18.08.2013 Dr Daniel Ching, MB FRCP FRACP Consultant Rheumatologist,
Inflammatory arthritis Shared Decision Making
 Inflammatory arthritis Shared Decision Making DMARDs El Miedany et al. Ann Rheum Dis 74(Suppl2): 1002 DOI: 10.1136/annrheumdis-2015-eular.1410 www.rheumatology4u.com Copyrights reserved Contents 1 2 3
Inflammatory arthritis Shared Decision Making DMARDs El Miedany et al. Ann Rheum Dis 74(Suppl2): 1002 DOI: 10.1136/annrheumdis-2015-eular.1410 www.rheumatology4u.com Copyrights reserved Contents 1 2 3
Technology appraisal guidance Published: 26 January 2016 nice.org.uk/guidance/ta375
 Adalimumab, etanercept, infliximab, certolizumab pegol, golimumab, tocilizumab and abatacept for rheumatoid arthritis not previously treated with DMARDs or after conventional DMARDs only have failed Technology
Adalimumab, etanercept, infliximab, certolizumab pegol, golimumab, tocilizumab and abatacept for rheumatoid arthritis not previously treated with DMARDs or after conventional DMARDs only have failed Technology
Is it Autoimmune or NOT! Presented to AONP! October 2015!
 Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release)
, Xeljanz XR (tofacitinib extended-release)") Market DC Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release) Override(s) Prior Authorization Quantity Limit Medications Xeljanz (tofacitinib) Approval Duration 1 year Quantity Limit May be
Market DC Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release) Override(s) Prior Authorization Quantity Limit Medications Xeljanz (tofacitinib) Approval Duration 1 year Quantity Limit May be
Efficacy and Safety of Rituximab in the Treatment of Rheumatoid Arthritis and ANCA-associated Vasculitis
 New Evidence reports on presentations given at ACR/ARHP 2010 Efficacy and Safety of Rituximab in the Treatment of Rheumatoid Arthritis and ANCA-associated Vasculitis Report on ACR/ARHP 2010 presentations
New Evidence reports on presentations given at ACR/ARHP 2010 Efficacy and Safety of Rituximab in the Treatment of Rheumatoid Arthritis and ANCA-associated Vasculitis Report on ACR/ARHP 2010 presentations
Rheumatoid Arthritis. Module III
 Rheumatoid Arthritis Module III Management: Biological disease modifying anti-rheumatic drugs, glucocorticoids and special situations (pregnancy & lactation) Dr Ved Chaturvedi MD, DM Senior Consultant
Rheumatoid Arthritis Module III Management: Biological disease modifying anti-rheumatic drugs, glucocorticoids and special situations (pregnancy & lactation) Dr Ved Chaturvedi MD, DM Senior Consultant
Stelara. Stelara (ustekinumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 9 Last Review Date: September 20, 2018 Stelara Description Stelara
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 9 Last Review Date: September 20, 2018 Stelara Description Stelara
Efficacy and Safety of Tocilizumab in the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis
 New Evidence reports on presentations given at EULAR 2010 Efficacy and Safety of Tocilizumab in the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2010 presentations
New Evidence reports on presentations given at EULAR 2010 Efficacy and Safety of Tocilizumab in the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2010 presentations
Clinical Guideline. Rheumatoid Arthritis Drug Treatment Pathway
 Clinical Guideline Rheumatoid Arthritis Drug Treatment Pathway Guideline Summary This clinical guideline outlines the biologic treatment pathway for adult patients with rheumatoid arthritis. Bexley/Bromley/Greenwich/Lambeth/Lewisham
Clinical Guideline Rheumatoid Arthritis Drug Treatment Pathway Guideline Summary This clinical guideline outlines the biologic treatment pathway for adult patients with rheumatoid arthritis. Bexley/Bromley/Greenwich/Lambeth/Lewisham
certolizumab pegol (Cimzia )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
BRIEFING DOCUMENT. human, recombinant fusion protein: extracellular domain of CTLA-4 and Fc domain of human IgG1
 BRIEFING DOCUMENT Application Type BLA Submission Number 125118/0 Reviewer Name Team Leader Division Director Established Name (Proposed) Trade Name Applicant Formulation Dosing Regimen Indication Intended
BRIEFING DOCUMENT Application Type BLA Submission Number 125118/0 Reviewer Name Team Leader Division Director Established Name (Proposed) Trade Name Applicant Formulation Dosing Regimen Indication Intended
Meta-analysis of long-term joint structural deterioration in minimally treated patients with rheumatoid arthritis
 Jansen et al. BMC Musculoskeletal Disorders (2016) 17:348 DOI 10.1186/s12891-016-1195-4 RESEARCH ARTICLE Open Access Meta-analysis of long-term joint structural deterioration in minimally treated patients
Jansen et al. BMC Musculoskeletal Disorders (2016) 17:348 DOI 10.1186/s12891-016-1195-4 RESEARCH ARTICLE Open Access Meta-analysis of long-term joint structural deterioration in minimally treated patients
1 Executive summary. Background
 1 Executive summary Background Rheumatoid Arthritis (RA) is the most common inflammatory polyarthropathy in the UK affecting between.5% and 1% of the population. The mainstay of RA treatment interventions
1 Executive summary Background Rheumatoid Arthritis (RA) is the most common inflammatory polyarthropathy in the UK affecting between.5% and 1% of the population. The mainstay of RA treatment interventions
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC)
") DERBYSHIRE JOINT AREA PRERIBING COMMITTEE (JAPC) Derbyshire commissioning guidance on biologic drugs f the treatment of Rheumatoid arthritis with methotrexate This algithm is a tool to aid the implementation
DERBYSHIRE JOINT AREA PRERIBING COMMITTEE (JAPC) Derbyshire commissioning guidance on biologic drugs f the treatment of Rheumatoid arthritis with methotrexate This algithm is a tool to aid the implementation
Medication Policy Manual. Topic: Otezla, apremilast Date of Origin: May 9, 2014
 Medication Policy Manual Policy No: dru342 Topic: Otezla, apremilast Date of Origin: May 9, 2014 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1, 2015 IMPORTANT
Medication Policy Manual Policy No: dru342 Topic: Otezla, apremilast Date of Origin: May 9, 2014 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1, 2015 IMPORTANT
Effective Health Care Program
 Comparative Effectiveness Review Number 55 Effective Health Care Program Drug Therapy for Rheumatoid Arthritis in Adults: An Update Executive Summary Background Rheumatoid arthritis (RA), which affects
Comparative Effectiveness Review Number 55 Effective Health Care Program Drug Therapy for Rheumatoid Arthritis in Adults: An Update Executive Summary Background Rheumatoid arthritis (RA), which affects
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Subject: Cimzia Page: 1 of 5 Last Review Date: December 8, 2017 Cimzia Description Cimzia (certolizumab
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Subject: Cimzia Page: 1 of 5 Last Review Date: December 8, 2017 Cimzia Description Cimzia (certolizumab
EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update
 ARD Online First, published on October 25, 2013 as 10.1136/annrheumdis-2013-204573 Recommendation EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying
ARD Online First, published on October 25, 2013 as 10.1136/annrheumdis-2013-204573 Recommendation EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/20644 holds various files of this Leiden University dissertation. Author: Klarenbeek, Naomi Bertine Title: Targeted treatment in early rheumatoid arthritis
Cover Page The handle http://hdl.handle.net/1887/20644 holds various files of this Leiden University dissertation. Author: Klarenbeek, Naomi Bertine Title: Targeted treatment in early rheumatoid arthritis
Regulatory Status FDA-approved indication: Orencia is a selective T cell co-stimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
SIMPONI Solution for Injection in a pre-filled syringe Solution for Injection in a pre-filled pen, SmartJect
 SIMPONI Solution for Injection in a pre-filled syringe Solution for Injection in a pre-filled pen, SmartJect PRODUCT INFORMATION NAME OF THE MEDICINE Golimumab (rmc) CAS Registry Number: 476181-74-5 DESCRIPTION
SIMPONI Solution for Injection in a pre-filled syringe Solution for Injection in a pre-filled pen, SmartJect PRODUCT INFORMATION NAME OF THE MEDICINE Golimumab (rmc) CAS Registry Number: 476181-74-5 DESCRIPTION
Medical Management of Rheumatoid Arthritis (RA)
") Medical Management of Rheumatoid Arthritis (RA) Dr Lee-Suan Teh Rheumatologist Royal Blackburn Hospital Educational objectives ABC Appreciate the epidemiology of RA Be able to diagnosis of RA Competent
Medical Management of Rheumatoid Arthritis (RA) Dr Lee-Suan Teh Rheumatologist Royal Blackburn Hospital Educational objectives ABC Appreciate the epidemiology of RA Be able to diagnosis of RA Competent
Integrating Quality Measures for RA into Your Practice: Optimizing Patient Care Using Your Own Data
 Integrating Quality Measures for RA into Your Practice: Optimizing Patient Care Using Your Own Data Robin K. Dore, MD Clinical Professor of Medicine David Geffen School of Medicine at UCLA Los Angeles,
Integrating Quality Measures for RA into Your Practice: Optimizing Patient Care Using Your Own Data Robin K. Dore, MD Clinical Professor of Medicine David Geffen School of Medicine at UCLA Los Angeles,
Characteristics Associated with Biologic Monotherapy Use in Biologic-Naive Patients with Rheumatoid Arthritis in a US Registry Population
 Rheumatol Ther (2015) 2:85 96 DOI 10.1007/s40744-015-0008-9 ORIGINAL RESEARCH Characteristics Associated with Biologic Monotherapy Use in Biologic-Naive Patients with Rheumatoid Arthritis in a US Registry
Rheumatol Ther (2015) 2:85 96 DOI 10.1007/s40744-015-0008-9 ORIGINAL RESEARCH Characteristics Associated with Biologic Monotherapy Use in Biologic-Naive Patients with Rheumatoid Arthritis in a US Registry
Orencia (abatacept) for Rheumatoid Arthritis. Media backgrounder
 for Rheumatoid Arthritis. Media backgrounder") Orencia (abatacept) for Rheumatoid Arthritis Media backgrounder What is Orencia (abatacept)? Orencia (abatacept) is the first biologic agent to be available in both an intravenous (IV) and a self-injectable,
Orencia (abatacept) for Rheumatoid Arthritis Media backgrounder What is Orencia (abatacept)? Orencia (abatacept) is the first biologic agent to be available in both an intravenous (IV) and a self-injectable,
1.0 Abstract. Title. Keywords. Adalimumab, Rheumatoid Arthritis, Effectiveness, Safety. Rationale and Background
 1.0 Abstract Title Assessment of the safety of adalimumab in rheumatoid arthritis (RA) patients showing rapid progression of structural damage of the joints, who have no prior history of treatment with
1.0 Abstract Title Assessment of the safety of adalimumab in rheumatoid arthritis (RA) patients showing rapid progression of structural damage of the joints, who have no prior history of treatment with