TB Intensive San Antonio, Texas November 11 14, 2014
|
|
|
- Darlene Cobb
- 5 years ago
- Views:
Transcription
1 TB Intensive San Antonio, Texas November 11 14, 2014 Extrapulmonary TB Linda Dooley, MD November 13, 2014 Linda Dooley, MD has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1
2 Generalizations about Extrapulmonary TB Treated the same as pulmonary TB: same meds, DOT May be harder to diagnose; AFB culture often negative Can be (almost) anywhere Some patients have unsuspected pulmonary disease and may be infectious More generalizations Treat longer for 3 types: bone and joint, meningitis, miliary More common in immune suppressed patients (HIV, TNF blockers) More common in Asian patients 2
3 Pulmonary vs Extrapulmonary Pulmonary Extrapulmonary Distribution of Extrapulmonary TB Lymphatic Pleural Meningitis GI Bone and joint Miliary Genitourinary Other 3

4 DISTRIBUTION Patient with extrapulmonary TB may also have pulmonary involvement, even with a normal chest x ray ALWAYS GET SPUTUM FOR AFB EVEN IF THE CHEST X RAY IS NORMAL 4


5 Pleural Tuberculosis 2nd most common form of extra pulmonary TB (15 20%) In most of the world, TB is the most common cause of pleural effusions Higher incidence in HIV+ patients Commonly a manifestation of primary TB May progress from an exudative effusion to an empyema or bronchopleural fistula Pleural TB 5

6 TB Empyema Diagnosis Thoracentesis with pleural biopsy 30% yield for MTB from pleural fluid Exudative fluid with lymphocyte predominance, protein more than 4 g/l ; glucose varies Pleural biopsy and culture may double yield of + culture 6
7 Tuberculous pleural effusions often resolve without treatment but high risk for later pulmonary disease: treat as case anyway Treatment Same as pulmonary TB 6 months adequate if no drug resistance or immune problems Drop PZA at 2 months and leave EMB in regimen if cultures negative 7

8 Surgical/ Specialist Involvement For initial diagnosis: thoracentesis and pleural biopsy More rarely for repeat thoracentesis if pleural fluid re accumulates For chest tube placement and possible decortication if empyema develops Lymphatic TB 8
 Treat like pulmonary TB Immune reconstitution may occur even with HIV negative")
9 Most common form of extra-pulmonary TB (30-40%) Most common sites are cervical (scrofula) or mediastinal but can affect any node Diagnosis and Treatment Fine needle aspirate or open biopsy Culture for AFB Don t forget CXR and sputum More common in women, Asian population, immune suppression (HIV, TNF blockers) Treat like pulmonary TB Immune reconstitution may occur even with HIV negative patients 9
10 Surgical/Specialist Involvement ENT if cervical; site determines who does biopsy Initial diagnosis by fine needle aspirate or biopsy Repeat I&D if swelling worsens Site of disease determines need for surgical involvement: immune reconstitution can cause obstruction TB Meningitis cases annually in US 1% of TB disease Even with effective treatment, case fatality high: 15 40% Early diagnosis both difficult and critical 10

11 Pathogenesis TB granuloma spills into subarachnoid space producing inflammation, proliferative arachnoiditis, vasculitis and communicating hydrocephalus Localized initially to base of brain Necrotizing granulomatous changes in arachnoid and blood vessels Basilar meningitis 11
12 Diagnosis Presentation may mimic bacterial meningitis: acute, rapidly progressive May be a slowly progressive dementia over months with personality change, social withdrawal or memory deficits Lumbar puncture: AFB stain and culture, PCR, NAAT, low CSF glucose, high protein, lymphocyte predominance Negative results do NOT exclude the diagnosis CSF examination Serial examination of the CSF by AFB stain and culture is the best diagnostic approach Use last fluid obtained; higher yield for larger volume CSF (10 15cc) Typically elevated protein, low glucose, and lymphocyte predominance Early CSF may be relatively acellular or PMN predominant Smears and cultures may yield positive results days to weeks after therapy has been initiated or may be negative 12



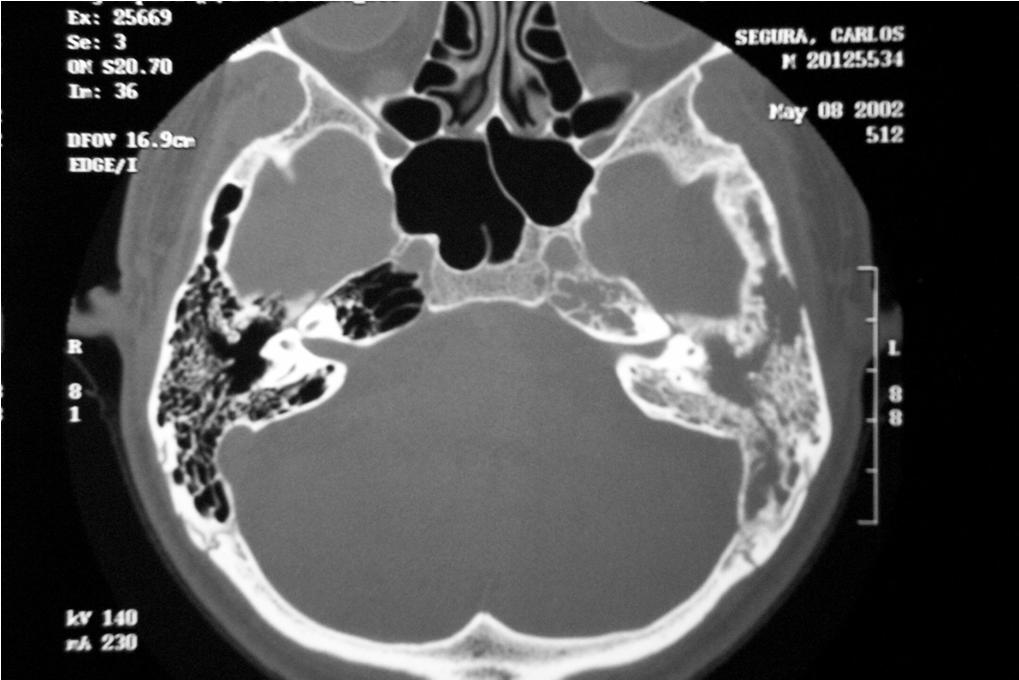
13 CT and MRI helpful in diagnosis Multiple tuberculomas along enhanced dural reflections Nov Basilar enhancement and hydrocephalus 13

14 Treatment Treat if meningitis suspected Early treatment essential Treatment 12 months for drug sensitive disease 18 months if no PZA Extend to months for severe illness, slow clinical response, or immune suppression No guidelines for length of treatment for MDR or XDR TB: expert consult essential 14
15 CSF Penetration of TB Meds GOOD FAIR POOR Isoniazid * Rifampin * Streptomycin * Pyrazimamide Ethambutol Capreomycin * Ethionamide Quinolones * Amikacin * Cycloserine * Can Be Given IV Kanamycin * Linezolid * Steroids Adjunctive corticosteroids may be beneficial and are recommended for all children and adults being treated for TB meningitis Doses Children: 2 4 mg/kg prednisone tapered over 4 weeks Adults: 60 mg/d prednisone tapered over 6 weeks or.4 mg/kg/day dexamethasone IV tapered to.1 mg/kg/day May need longer slower taper 15
16 Surgery Hydrocephalus may require urgent shunting. Serial LP and steroid therapy may suffice for Stage I patients awaiting response to antibiotics. Shunting should not be delayed in patients with stupor, coma or progressive neurologic signs. Nov 2009 Surgical/Specialist Involvement ER doc, radiologist or hospital doc for initial LP for diagnosis Neurosurgeon for shunt placement if needed later: surgery need can be urgent 16


17 Case: HIV+ man with abnormal MRI MRI done after fall Extensive work-up all negative except +QFT Empiric Rx for TB meningitis tried without reporting and drug induced hepatitis DOT begun: pt. able to tolerate TB Rx without PZA 17
18 Case: 20 yo Pakistani woman with severe headache and swollen neck nodes Fine needle aspirate: granulomatous tissue Normal CXR Consultant recommended LN biopsy for better chance MTB and sensitivities Pt declined: did not have $8000 required down payment Abnormal CT head; no LP done Observed induced sputum collection done by NCM had positive NAAT Drug sensitive MTB from sputum One month later also grew TB from neck aspirate Headache resolved on TB therapy 18

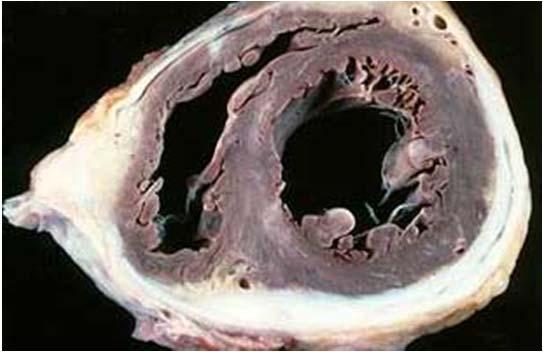
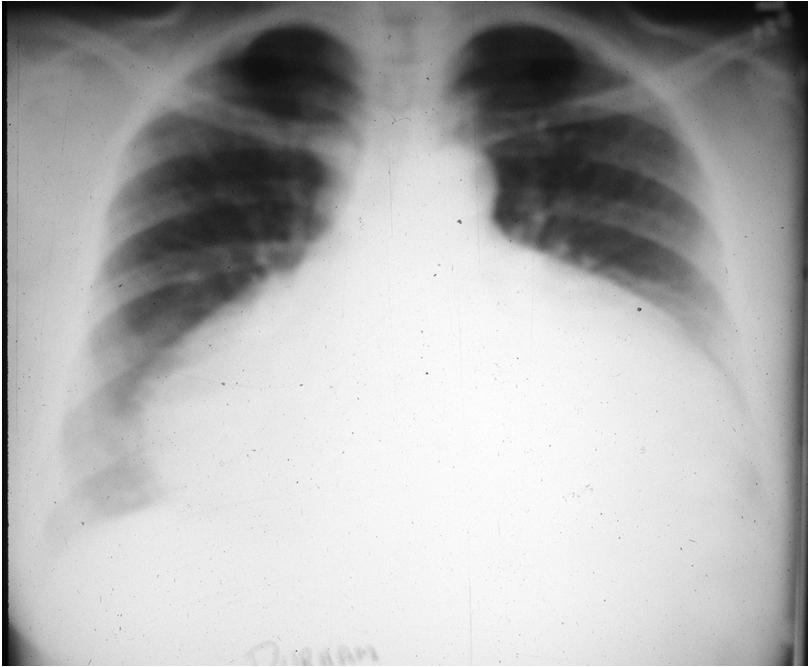
19 Pericardial TB Pericardial TB 19
20 Pericardial TB Uncommon and difficult diagnosis Presents with acute or insidious onset; nonspecific symptoms Ultrasound helpful; acid fast studies may not be positive Surgery for progressive tamponnade or recurrent effusions on TB Rx Steroids reduce mortality and need for surgery or repeat pericardiocentesis: start at 60 mg/d 1st month and reduce over 11 weeks Surgical/Specialist Involvement Cardiothoracic surgeon essential for initial diagnosis as well as for management of recurrent effusion or tamponnade May require urgent management Pericardial stripping may be needed 20
 Can be anywhere Frequently delayed diagnosis X ray not helpful in distinguishing other infectious destructive")
21 Bone and Joint TB Skeletal TB Spinal TB (Pott s disease) most common location: 40% Next most common: hip (40%) and knee (10%) Can be anywhere Frequently delayed diagnosis X ray not helpful in distinguishing other infectious destructive etiology 21
22 Diagnosis Joint aspiration: WBC may be granulocytes or lymphocytes WBC count varies widely Protein 4 6 g/dl; glucose may be low Acid fast culture yield high (up to 80%) Presence of positive smear much lower (20%) Treatment Standard TB therapy with extended treatment 12 months minimum but extend for slow or uncertain response 22
 Effective treatment may preclude need for surgery Soft Tissue TB")
23 Surgical/Specialist Involvement Orthopedist, primary care, or rheumatologist may do initial arthrocentesis for diagnosis Surgery may be needed if bone/joint stabilization required or if prosthesis needs to be removed With spinal TB, neurosurgery or spine surgeon involvement essential for spine stabilization (external or surgical) Effective treatment may preclude need for surgery Soft Tissue TB 23
24 Soft Tissue TB Often adjacent to bony and may be direct spread from bony structure or may erode into bone: can be difficult to know if bone involved If not sure if bone involved, treat like skeletal TB (longer duration) I&D of abscess will only be diagnostic if acid fast cultures done Surgical involvement for diagnosis and management of large abscesses Gastrointestinal and Peritoneal TB Peritoneal TB 10% extra pulmonary GI tract: any site possible but more common terminal ileum and cecum then rest of colon Often delayed diagnosis TB bacilli may be ingested rather than inspired: consider early if patient drank or ate unpasteurized milk products Acid fast cultures frequently negative: pathology caseating necrotizing granulomas 24


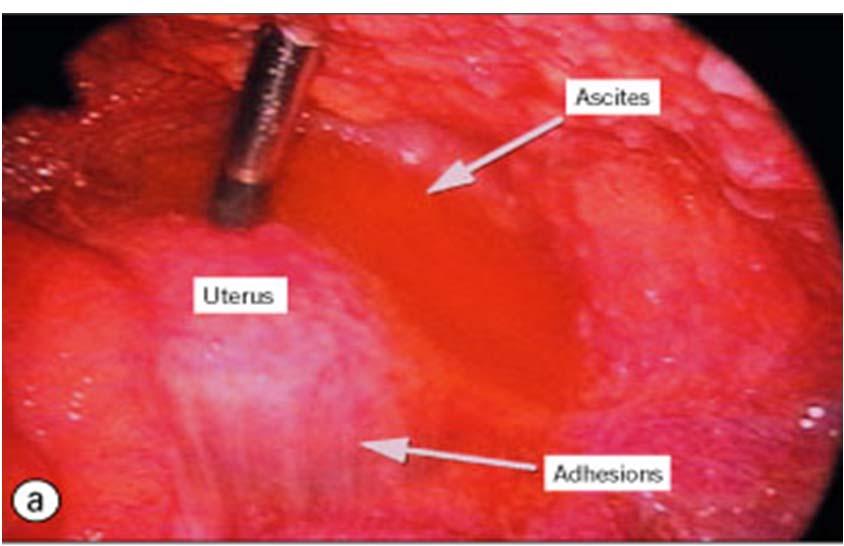
25 Peritoneal TB Laparoscopic view of peritoneal granulomas Peritoneal TB: laparoscopic view of spiderweb adhesions 25



26 Treatment If cultures negative or pending, assume PZA resistance Esophageal TB Duodenal TB Consider the age of your patient and possible childhood exposure to M. bovis 84 yo man with normal CXR 26

27 Surgical/Specialist Involvement Gastroenterologist or general surgery may make initial diagnosis Patient may need paracentesis for initial diagnosis or management of recalcitrant ascites Urogenital TB 27
; may be virtually diagnostic of renal")
28 Genitourinary TB 10 15% extrapulmonary TB Often insidious onset, subtle nonspecific symptoms, delay in diagnosis Hematogenous spread from primary site, often years after infection Any part of GU tract may be affected Ureteral abnormalities (multiple beading strictures); may be virtually diagnostic of renal TB 28

29 Renal TB May have pyuria or hematuria or both Acid fast cultures of urine for sterile pyuria May need more than 3 specimens of first morning urine collection Urine AFB studies not always positive NAAT testing may be helpful but negative result does not preclude diagnosis Surgery or stenting for obstruction Prostatic TB 29
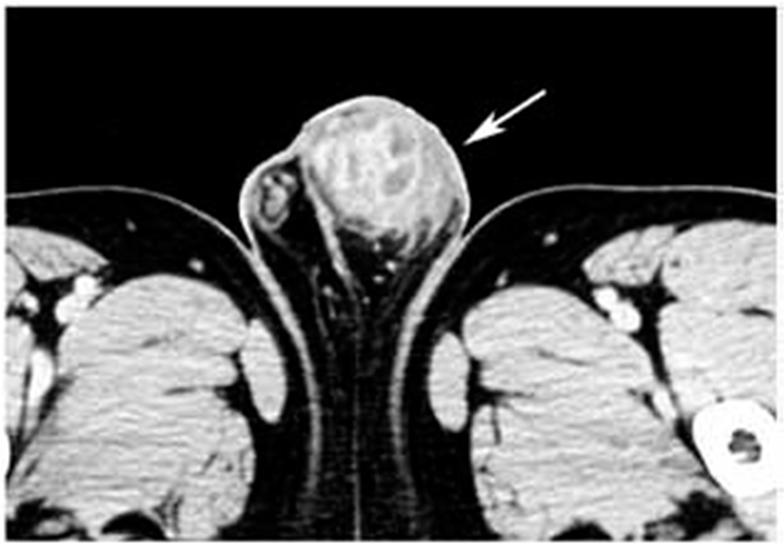
30 Testicular TB Uterine TB 30
31 Female Genital TB With Fallopian tube involvement, unlikely that preservation of fertility possible since usual scarring Often diagnosed by pathology after hysterectomy: treat even if involved organ removed Surgical/Specialist Involvement Urology or gynecology involved in initial diagnosis Urologist essential if renal obstruction develops for ureteral stent placement and removal Obstruction may develop after therapy underway: immune reconstitution 31


32 Other TB Laryngeal TB Tuberculous Otitis Media 32

33 TB Mastoiditis XXXXXXXXXX Adrenal TB 33

34 Adrenal insufficiency and TB May have unsuspected adrenal involvement alone or with disseminated TB Assessment of adrenal function if slow response or hypokalemia, hyponatremia, hypotension Don t forget adrenal insufficiency possiblity if steroids were stopped after long use Ocular TB 34

35 Ocular TB Diagnosis made by ophthalmologist Diagnosis of exclusion: patient should be followed by ophthalmology during TB treatment No cultures available Treat same as pulmonary TB TB of the Skin 35

36 Dermatologic TB May be hematogenous or direct spread May be injection: accidents in pathology or microbiology lab Treatment same as pulmonary TB What s left?? 36


37 TB Everywhere Miliary or Disseminated TB Tiny lesions spread throughout the body Distinctive pattern on CXR or CT 37
38 Miliary TB Pulmonary involvement may not be present Frequently subacute presentation with fever and weight loss More rarely can be a fulminant sepsis like presentation with acute onset and rapid deterioration (usually fatal) Liver biopsy may be helpful Blood cultures may be positive if acid fast studies done All AFB may be negative Treatment of Disseminated TB Prolonged treatment needed: 12 months or more Cultures may be negative: paucibacillary disease Don t let negative cultures or normal CXR tempt you to shorten therapy 38
39 Thank you Don t forget to get sputum AFB even if you think only extrapulmonary TB 39
Extra pulmonary Tuberculosis
 Extra pulmonary Tuberculosis SHANNON KASPERBAUER, MD NATIONAL JEWISH HEALTH DENVER TB COURSE APRIL 2019 Disclosures Insmed: speaker, advisory board, investigator No relevant disclosures for this talk Objectives
Extra pulmonary Tuberculosis SHANNON KASPERBAUER, MD NATIONAL JEWISH HEALTH DENVER TB COURSE APRIL 2019 Disclosures Insmed: speaker, advisory board, investigator No relevant disclosures for this talk Objectives
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Extrapulmonary Tuberculosis XPTB
 Extrapulmonary Tuberculosis XPTB Shannon Kasperbauer, MD National Jewish Health Denver TB Course April 2018 The Kings Evil strangely visited people all swol n and ulcerous, pitiful to the eye, the mere
Extrapulmonary Tuberculosis XPTB Shannon Kasperbauer, MD National Jewish Health Denver TB Course April 2018 The Kings Evil strangely visited people all swol n and ulcerous, pitiful to the eye, the mere
Extra Pulmonary Tuberculosis
 TB Intensive San Antonio, Texas December 1-3, 2010 Extrapulmonary TB Robert Longfield, MD, FACP; TCID December 3, 2010 Extra Pulmonary Tuberculosis TB Intensive Course December 2010 Robert N. Longfield,
TB Intensive San Antonio, Texas December 1-3, 2010 Extrapulmonary TB Robert Longfield, MD, FACP; TCID December 3, 2010 Extra Pulmonary Tuberculosis TB Intensive Course December 2010 Robert N. Longfield,
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Extra Pulmonary Tuberculosis:
 TB Intensive Tyler, Texas December 4-6, 2007 Extrapulmonary Tuberculosis Robert N. Longfield, MD, FACP December 6, 2007 Extra Pulmonary Tuberculosis: TB Intensive Course December, 2007 Robert N. Longfield,
TB Intensive Tyler, Texas December 4-6, 2007 Extrapulmonary Tuberculosis Robert N. Longfield, MD, FACP December 6, 2007 Extra Pulmonary Tuberculosis: TB Intensive Course December, 2007 Robert N. Longfield,
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Extrapulmonary Tuberculosis
 Extrapulmonary Tuberculosis Timothy H. Dellit, MD Professor, UW Allergy & Infectious Diseases Associate Medical Director Harborview Medical Center No financial conflicts Tuberculosis in King County1995-2014
Extrapulmonary Tuberculosis Timothy H. Dellit, MD Professor, UW Allergy & Infectious Diseases Associate Medical Director Harborview Medical Center No financial conflicts Tuberculosis in King County1995-2014
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Objectives. Highlight typical feature of TB pericarditis. How to make a diagnosis. How to treat TB pericarditis
 Dr. Conteh Objectives Highlight typical feature of TB pericarditis How to make a diagnosis How to treat TB pericarditis New evidence for adjunctive corticosteroid Introduction TB pericarditis occurs in
Dr. Conteh Objectives Highlight typical feature of TB pericarditis How to make a diagnosis How to treat TB pericarditis New evidence for adjunctive corticosteroid Introduction TB pericarditis occurs in
CNS Infections in the Pediatric Age Group
 CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Treatment of Tuberculosis Disease. Treatment of Tuberculosis. Decision to Treat Initiation of Therapy 1
 Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
SWABCHA Fact Sheet: Tuberculosis (TB)
") SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
Tuberculosis: update 2013
 Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Pediatric Drug-Resistant TB in China
 Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Extrapulmonary TB James B. McAuley MD MPH November 13, 2009 PEDIATRIC TB EXTRAPULMONARY DISEASE James B. McAuley MD MPH Rush University Medical Center
Pediatric TB Intensive Houston, Texas November 13, 2009 Extrapulmonary TB James B. McAuley MD MPH November 13, 2009 PEDIATRIC TB EXTRAPULMONARY DISEASE James B. McAuley MD MPH Rush University Medical Center
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
In Canada, there was a 25% reduction in incidence of genitourinary TB in the period compared with An interesting speculation
 Renal T B EPIDEMIOLOGY Young to middle age usually affected, rare in children Male : female ratio = 2:1 True prevalence and incidence not known as patients are usually asymptomatic With HIV pandemic, there
Renal T B EPIDEMIOLOGY Young to middle age usually affected, rare in children Male : female ratio = 2:1 True prevalence and incidence not known as patients are usually asymptomatic With HIV pandemic, there
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Enlarging TB Lymph Node Improving or Deteriorating? History. History. Physical examination. Distribution of lymph nodes
 Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Cryptococcal Meningitis
 Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Extrapulmonary Tuberculosis
 Extrapulmonary Tuberculosis Randall Reves, MD, Colorado University Denver, volunteer TB Clinician Denver Metro TB Control Program Slides adapted from originals by Timothy H. Dellit, MD, Harborview Medical
Extrapulmonary Tuberculosis Randall Reves, MD, Colorado University Denver, volunteer TB Clinician Denver Metro TB Control Program Slides adapted from originals by Timothy H. Dellit, MD, Harborview Medical
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
Improved diagnosis of extrapulmonary tuberculosis by antigen detection using immunochemistry-based assay. Tehmina Mustafa
 Improved diagnosis of extrapulmonary tuberculosis by antigen detection using immunochemistry-based assay Tehmina Mustafa Overview Introduction: extrapulmonary tuberculosis (TB) & diagnostic challenges
Improved diagnosis of extrapulmonary tuberculosis by antigen detection using immunochemistry-based assay Tehmina Mustafa Overview Introduction: extrapulmonary tuberculosis (TB) & diagnostic challenges
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
Role of imaging (images) in my practice. Dr P Senthur Nambi Consultant Infectious Diseases
 in my practice. Dr P Senthur Nambi Consultant Infectious Diseases") Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Managing meningitis not just antibiotics. Helena White December 2013
 Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Bilateral multiple choroidal granulomas and systemic vasculitis as presenting features of tuberculosis in an immunocompetent patient
 Kumar et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:40 DOI 10.1186/s12348-016-0109-9 Journal of Ophthalmic Inflammation and Infection BRIEF REPORT Open Access Bilateral multiple choroidal
Kumar et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:40 DOI 10.1186/s12348-016-0109-9 Journal of Ophthalmic Inflammation and Infection BRIEF REPORT Open Access Bilateral multiple choroidal
Property of Presenter. Not for Reproduction DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS
 DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
ANNEXURE A: EXPLANATORY NOTES ON THE DMR 164 REPORTING ON HIV AND TB FORM
 ANNEXURE A: EXPLANATORY NOTES ON THE DMR 164 REPORTING ON HIV AND TB FORM The form and content of the explanatory note is to: Inform those responsible for completing the DMR 164 Reporting Form - as to
ANNEXURE A: EXPLANATORY NOTES ON THE DMR 164 REPORTING ON HIV AND TB FORM The form and content of the explanatory note is to: Inform those responsible for completing the DMR 164 Reporting Form - as to
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Clinical Response to Treatment of Central Nervous System Tuberculosis in Non-Human Immunodeficiency Virus-Infected Adolescents and Adults
 Journal of Tuberculosis Research, 2016, 4, 173-182 http://www.scirp.org/journal/jtr ISSN Online: 2329-8448 ISSN Print: 2329-843X Clinical Response to Treatment of Central Nervous System Tuberculosis in
Journal of Tuberculosis Research, 2016, 4, 173-182 http://www.scirp.org/journal/jtr ISSN Online: 2329-8448 ISSN Print: 2329-843X Clinical Response to Treatment of Central Nervous System Tuberculosis in
TB/HIV 2 sides of the same coin. Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai
 TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
Difficult Diagnosis: Case History. 7 months prior, she happened to have undergone a C-spine MRI after a car accident
 Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant