New Zealand Organisation for Rare Disorders (NZORD) July 2017
|
|
|
- Betty Fitzgerald
- 5 years ago
- Views:
Transcription
 July 2017 Introduction to Hypermobility This New Zealand-based review is to help clinicians to recognise joint hypermobility and to consider possible diagnoses and management")
1 HYPERMOBILITY AND EHLERS-DANLOS SYNDROMES (EDS) A NEW ZEALAND OVERVIEW Includes Generalised Joint Hypermobility (GJH) and Hypermobility Spectrum Disorders (HSD) New Zealand Organisation for Rare Disorders (NZORD) July 2017 Introduction to Hypermobility This New Zealand-based review is to help clinicians to recognise joint hypermobility and to consider possible diagnoses and management approaches when in day-to-day practice they see patients with one or more of the following: Joint hypermobility (double-jointed), especially when associated with musculoskeletal pain Recurrent subluxations/dislocations Unusual skin especially skin fragility or hyperextensible skin Unusual bruising or bleeding The spectrum of Hypermobility disorders includes GJH (Generalised Joint Hypermobility), HSD (Hypermobility Spectrum Disorder), heds (Hypermobile Ehlers-Danlos Syndrome) and the other EDS (Ehlers-Danlos Syndromes) types. They are considered together here for simplicity and because of potential diagnostic overlap at first sight. This broad-based overview sets out to provide the clinician with tools to place patients in a presumptive diagnostic category based on clinical features and to develop an initial management plan. Hypermobility Spectrum Disorder (HSD) EDS (Main feature in heds but present in all types) HYPERMOBILITY OTHER (Trauma, neurological deficit, muscle disorders, etc.) HCTD (Heritable connective tissue disorders -Marfan's, osteogenesis imperfecta, etc.) RED FLAGS veds Vascular EDS 1,2,10 Arterial rupture or unusual bleeding in a child or young adult. Aorta, other large vessels and small vessels can be involved. See How to Save a Life 1,2 and veds reference article 10 All EDS Anaesthetics and Surgery Local anaesthetic local, regional or epidural has less effect and slower onset in EDS 27,28 o May need more anaesthetic and longer wait before beginning procedure Surgical issues o Prone to bleeding Ver /07/17 Page 1 of 15
2 o Problems with tourniquet compartment syndrome o Potential for tissue damage and subluxation with positioning issues Any clinician planning surgery or anaesthesia in a patient with hypermobility or EDS should carefully read Wiesmann et al: Recommendations for anaesthesia and perioperative management in patients with Ehlers-Danlos Syndrome(s) 26 Assessment History History of hypermobility (double-jointed) now or historically at any stage of life Hyperextensible (stretchy) skin Musculoskeletal pain (joint and muscle pain) History of one or more of these this list is not exhaustive o Enquire about family history all EDS has a genetic component o Repeated dislocations (often of more than one joint) - often spontaneous with less than usual trauma o Easy bruising especially in children where the history is of no trauma but there are obvious bruises. Is in the differential for non-accidental injury. o Vessel rupture or unusual internal bleeding in a young person o Unusual or severe prolapses and hernias or bowel perforation in younger people o Associated symptoms that may be present (but are not diagnostic) include (but not limited to): fatigue, headaches, sleep disturbance, autonomic dysfunction (especially POTS Postural Orthostatic Tachycardia Syndrome), irritable bowel, and Mast Cell Activation Syndrome Examination See Aids to Diagnosis Usual basic clinical examination Check for hypermobility - Check Beighton Score 3 o If 4/9, hypermobility is present (depends on age 3 ) o If positive, look for other EDS features to differentiate GJH, HSD and EDS o In adults, if too stiff or painful to do Beighton Score, use Five Point Questionnaire - see Aids to Diagnosis o Look for other causes of hypermobility e.g. neurological, trauma etc. Check skin for hyperextensibility especially in ceds. See Aids to Diagnosis o 3cm stretch at neck, elbow, and knee. 1.5cm forearm. 1 cm palm (thenar eminence). Check skin for atrophic scarring - see Aids to Diagnosis Assess joints and tender areas typical inflammatory signs absent in face of significant pain Investigations There are no specific or suggestive laboratory findings There are specific known genetic mutations/abnormalities for ceds and veds (and most of the rare types) but not for heds. Clinical diagnosis is made first using criteria outlined in 7 followed by genetic confirmation wherever possible and practical. Differential diagnosis a few suggestions (not exhaustive) Other causes of hypermobility such as constitutional, Marfan s Syndrome, Trisomy 21, previous injury, neuropathic joints, osteogenesis imperfecta Vessel rupture all other congenital and acquired causes including trauma Joint and muscle pain Ver /07/17 Page 2 of 15
 other vasculopathies and clotting")
3 o Other arthropathies usually are typically inflammatory in nature, have more swelling and often have suggestive radiology or laboratory o Fibromyalgia Bruising (esp. in children) other vasculopathies and clotting defects, e.g. von Willerbrands Stretchy skin - there may be other causes but in the context of hypermobility think of ceds Indications for transfer or initial specialised assessment Acute vascular rupture is a medical emergency consult vascular surgeons All others a clinician well versed in EDS if available Support services as this can be a chronic, debilitating and painful condition, a multidisciplinary approach over the long term is important AIDS TO DIAGNOSIS BEIGHTON SCORE Assessment tool for hypermobility point for each side for 1-4 and 1 point for 5. Total 9. If 4/9, hypermobility is present (From 7). See 3 for video. THE FIVE-POINT QUESTIONNAIRE Use in cases where it is not possible to do Beighton Score or where superimposed pain and stiffness in an adult will give a falsely low Beighton Score See 7 1. Can you now (or could you ever) place your hands flat on the floor without bending your knees? 2. Can you now (or could you ever) bend your thumb to touch your forearm? 3. As a child, did you amuse your friends by contorting your body into strange shapes or could you do the splits? 4. As a child or teenager, did your shoulder or kneecap dislocate on more than one occasion? 5. Do you consider yourself double-jointed? A yes answer to 2/5 questions suggests joint hypermobility with 80 85% SKIN - HYPEREXTENSIBILITY Ver /07/17 Page 3 of 15
 FACIAL")

4 SKIN - SCARRING (From 7 ) FACIAL FEATURES IN veds Ver /07/17 Page 4 of 15
5 Management ACUTE EMERGENCIES Vascular rupture appropriate vascular surgery or interventional radiology referral Dislocations appropriate orthopaedic referral Acute pain usual principles DIAGNOSIS Give a tentative clinical diagnosis. Assure the patient you don t think it s all in their head this is often what they have been told for a long time. Offer patient information on Ehlers-Danlos.com website and support groups See References REFERRAL If available refer to a clinician with experience in EDS geneticist, rheumatologist, etc. A multidisciplinary team best leads care. Practically this often means the primary care doctor will refer to the appropriate specialist as and when needed, e.g. orthopaedic surgeon, neurosurgeon. PAIN INITIAL (ACUTE) Usual principles for initial management of acute or chronic pain o Usually start with paracetamol and work up as needed o There are no specific analgesics proven to have significant advantage in HSD/EDS Bracing or splinting can be helpful INJURIES INSTABILITY, SUBLUXATIONS, DISLOCATIONS, TENDON & LIGAMENT INJURIES INITIAL EMERGENCY AND ACUTE (SHORT TERM) STRATEGIES Each individual injury episode (dislocation) should be treated as a new trauma on its own merits and not just passed off as part of your condition. Aim is to return to the pre-injury state. Even though a dislocation may be due to less force than in someone without EDS, the associated tissue effects and damage will likely be no less severe, e.g. Bankart lesion in shoulder. Dislocation - initial reduction o Because those with EDS may have severe pain, instability or injury elsewhere in the same region, some typical traction and twisting movements used for reduction may need to be modified to prevent injury elsewhere from the procedure itself, e.g. with shoulder dislocation pulling from the wrist or forearm may injure wrist or elbow. May need to modify hand position and grip. The force needed to reduce may be less than that needed for non-eds. Some patients can spontaneously reduce. o Protect skin it may be fragile. Use padding if needed. o Ligament and tendon injuries may take longer to heal and may recur after relatively less trauma after the first episode Subluxations may respond well to gentle manipulation rather than actual reduction Splinting and bracing are important after reduction Immediate post-trauma physiotherapy is used it is important to take into account the somewhat different approach needed in EDS. Appropriate rehabilitation is aimed at return to independent living Ver /07/17 Page 5 of 15
6 JOINT INSTABILITY AND PAIN LONG TERM STRATEGIES TO STABILISE After an initial injury some of the joints may become prone to repeat injury from relatively minor trauma Physiotherapy see below External bracing o Braces and splints can be useful to prevent or after dislocation/subluxation as well as for comfort o In the first instance splinting is best discussed with and accessed through a local physiotherapy department. o Specific hypermobility-focused splint types can improve function and reduce pain even in the absence of current or recent subluxation/dislocation. As an example, finger splints along the lines of ring splints 30 can be very helpful to prevent finger hyperextension to improve overall finger stability. o Neoprene or elastic supports and compressive clothing are also used and can be useful as they allow proprioceptive feedback as well as support and pain relief. Discuss options with physical therapist or occupational therapist. o Orthotic referral where appropriate Surgery may have a sub-optimal outcome but may be important in critical areas, e.g. craniocervical instability. When referring to or discussing with an orthopaedic surgeon, neurosurgeon, etc., be clear that the patient has EDS where issues may include slow healing, early recurrence and poor response to local anaesthetic agents. Non-surgical approaches to joint stabilisation such as prolotherapy offer some hope and may be appropriate in selected circumstances in adults. Materials (chemical/sclerosant) injected into ligaments are thought to induce healing with scarring and shortening which in turn may increase joint stability and thereby reduce pain and subluxation. Not yet widely available. PHYSIOTHERAPY 29 As there are limited management options, physiotherapy is key Traditional techniques of physiotherapy often need adapting for EDS and always require taking a wider view of the patient Physiotherapy should be aimed at empowering the patient towards self-management Aim for social rehabilitation training for independence with help of occupational therapists where needed Appropriate strategies: o Education and reassurance o Most patients will benefit from an individualised, carefully graduated exercise and activity programme o Physiotherapists can also advise on posture correction, proprioception training, splints/supports/taping, relaxation techniques, hydrotherapy, gentle manual techniques, including Myofascial release and pain management strategies o For dislocation and subluxation management, see I m popping out for a while 35 o The Muldowney Protocol 30 is an EDS specific programme that can take over a year to work through with a musculoskeletal therapist (6-9 months in younger patients). Not all patients can tolerate this and there are few physiotherapy departments that are likely to be able to provide a service over this length of time at this stage. Currently there is no evidence to show this is more beneficial than physiotherapy strategies listed above, but it may be worth investigating. Ver /07/17 Page 6 of 15
7 SURGERY AND ANAESTHESIA 26,27,28 Surgical complications may be increased due to slow healing and potential for bleeding. Appropriate strategies should be planned and discussed in EDS context. Recurrence after surgery may occur because of the inherently abnormal ligaments. Some issues with anaesthesia: o Unstable neck may be an issue with positioning o Slow and suboptimal response to local anaesthetic incl. epidurals o Tourniquet can cause bruising and compartment syndrome o Positioning can cause unexpected subluxations including temporomandibular joint during anaesthesia Any clinician planning surgery or anaesthesia in a patient with hypermobility or EDS should carefully read Wiesmann et al: Recommendations for anaesthesia and perioperative management in patients with Ehlers-Danlos Syndrome(s) 26 GENERAL SUPPORT Support groups offer advice on how to cope with day-to-day living with a painful chronic disease that may significantly disrupt life Chronic pain teams may help to design an overall pain management strategy Psychology support can be helpful Request Help A NOTE ON COORDINATING CARE Many patients can be managed by their GP and physiotherapist with occasional input from an EDS specialist Some with complex or severe issues will need a truly multidisciplinary team that may include orthopaedics, neurosurgery, gastroenterology, etc. Appropriate referrals for specific interventions, e.g. hand therapist, prolotherapy ADVICE Best all-round web advice: Ehlers-Danlos Society 12,13 Some geneticists, rheumatologists and musculoskeletal specialists have experience in diagnosing and managing EDS. Local availability will likely be variable. The New Zealand EDS Working Group that is part of NZORD (New Zealand Organisation for Rare Disorders) may be able to offer some resources in the near future. This may include a list of Health Professionals with EDS knowledge and experience. See NZORD. 33 GENERALISED JOINT HYPERMOBILITY (GJH) There is a spectrum of GJH 1. Asymptomatic (non-syndromic) GJH hypermobility without other symptoms. Other causes, e.g. neurological deficit must be excluded. 2. Symptomatic GJH that doesn t meet criteria for heds HSD 3. A well-defined syndrome - heds Ver /07/17 Page 7 of 15


8 Joint hypermobility can lead to micro and macro trauma, which in the long run can be a leading cause of pain and in adulthood degenerative changes. This can range from hyperextension injury to mild subluxation through to frank dislocation. Each event leads to surrounding collateral damage. HSD HYPERMOBILITY SPECTRUM DISORDER 4,5 Common Hypermobility and significant additional symptoms are typically limited to the musculoskeletal system Pain may be significant and debilitating Types o Generalised HSD G-HSD GJH Musculoskeletal manifestations Similar to heds o Peripheral HSD P-HSD Hypermobility in hands and feet only Musculoskeletal manifestations Similar to heds o Localised HSD L-HSD Hypermobility in a single joint Musculoskeletal manifestations Similar to heds o Historical history of one of the above usually with 5-Point Questionnaire EDS EHLERS-DANLOS SYNDROMES EDS (Ehlers-Danlos Syndromes) are a group of inherited disorders characterised by defects in collagen mainly affecting the ligaments and soft tissues Relatively rare about 1:5000. F>M Basis is abnormal collagen different types of collagen in each of the EDS types The commonest (>80-90%) is heds genetic basis currently not known ceds and veds are uncommon have a known genetic basis (see Table below) o All the rest are very rare but genetic basis is clear There are 13 types of EDS with significant overlap in features 5,6 Hypermobile - heds (Most common) Classical - ceds (Common) EDS Vascular - veds (Rare -Most risk) 10 Others (Very rare) CLINICAL CLASSIFICATION OF EDS EDS SUBTYPE ABBREV INHERITANCE GENETICS COLLAGEN Classical ceds AD COL5A1, COL5A2 Type 5 Vascular veds AD COL3A1 Type 3 Hypermobile heds AD Unknown Unknown 10 other types See Ref 6,7 Ver /07/17 Page 8 of 15
9 heds HYPERMOBILE EDS 7,8,9 Most common See heds Diagnostic Checklist for details and how to apply criteria - includes a downloadable pdf 8 o Criterion 1 - Main feature (must be present) Generalised Joint Hypermobility (Beighton Score 4/9 over age 50; 5/9 in young adults; 6/9 in children and adolescents) 3 o Criterion 2 (at least 2 features) Feature A Generalised connective tissue disorder (at least 5/12 present) Soft, velvety skin Mild skin hyperextensibility (not as much as ceds) Unexplained striae Piezogenic papules (nodules on side of feet) Recurrent/multiple hernias Atrophic scarring Arachnodactyly Arm span-height ratio: 1.05 Pelvic floor prolapse Dental crowding Mitral valve prolapse Aortic root dilatation Feature B Family history (autosomal dominant but can appear to skip) Feature C (at least 1) - see details in checklist Musculoskeletal pain Chronic widespread pain 3 months Recurrent joint dislocations/instability in absence of significant trauma (may also occur with trauma) o Criterion 3 All must be present No skin fragility Reasonable exclusion of other connective tissue disorders e.g. Marfan s Exclusion of other disorders that could cause GJH To diagnose heds all 3 criteria must be satisfied. Other features that can occur (not an exhaustive list) o Sleep disturbance, chronic fatigue, POTS, functional GIT disorders, unusual hernias, internal hernias, dysautonomia, Raynaud s, MCAS, some cardiac features, osteoarthritis secondary to joint instability, headaches, TMJ dysfunction, increased gynaecological presentations, pelvic floor dysfunction, anxiety, depression. Multiple other features that affect quality of life may be part of the spectrum. Overall effect on life may range from severe (bed-ridden) to relatively minor ceds CLASSICAL EDS 7,11 Relatively common Major criteria o Skin features - hyperextensible skin, atrophic scarring (esp. knees & elbows) o Generalised Joint Hypermobility Minor criteria Ver /07/17 Page 9 of 15
10 o Easy bruising o Soft, doughy skin o Skin fragility o Molluscoid pseudotumours o Subcutaneous spheroids o Hernia or history of o Epicanthal folds o Complications of GJH o Family history of 1 st degree relative To diagnose ceds: Criterion 1 Skin features Plus Criterion 2 GJH &/or at least 3 minor criteria Needs confirmation with genetic testing if possible. veds VASCULAR EDS 7,10 Rare and dangerous Major criteria o Family history proven veds o Arterial rupture at young age o Spontaneous colon perforation in absence of other disease o Uterine rupture without predisposing cause o Carotid-cavernous sinus fistula without trauma Minor criteria o Bruising not related to trauma or in unusual sites o Thin, translucent skin with easily visible veins o Characteristic facial appearance o Spontaneous pneumothorax o Acrogenic o Talipes equinovarus o Congenital hip dislocation o Hypermobility of small joints o Tendon and muscle rupture o Keratoconus o Gingival recession and fragility o Early onset varicose veins To diagnose need a family history with arterial rupture or dissection younger than 40 or any of the other major features Genetic testing is important ALL OTHER TYPES See Ref 7 Ver /07/17 Page 10 of 15
11 UNUSUAL SYMPTOMS THAT CAN BE ASSOCIATED WITH EDS esp. heds Dysautonomia (autonomic dysfunction) such as POTS (postural orthostatic tachycardia syndrome) MCAS (mast cell activation syndrome) masquerading as unusual allergies GIT symptoms including constipation Raynaud s A Note on Genetics Of the three most common forms of EDS, veds and ceds have an established genetic basis. Determining the exact molecular basis for these conditions can be useful for diagnosis, management and reproductive decision-making. It is, however, not mandatory that every person with a clinical diagnosis of EDS undergoes molecular analysis. To arrange for an assessment of the genetic basis for a person with a veds or ceds phenotype, a referral can be made to Genetic Health Services NZ through any one of their three hubs centered in Christchurch, Wellington or Auckland. See the GHSNZ website for details on how to lodge a referral and request for assessment at Rarer forms of EDS can also be assessed in a similar manner on a case-by-case basis. For heds (by far the most common), although there are clear familial (autosomal dominant) components underpinning the disorder, a defined molecular basis has not been discovered. A referral of such individuals can still be made to GHSNZ, but beyond a confirmation of the clinical diagnosis little specific laboratory investigation can be offered." Note that genetic services criteria for acceptance are such that assessment is not guaranteed, especially for heds. This document has been edited by Matthew Preston (Radiologist) for New Zealand EDS Working Group July matpre@gmail.com Ver /07/17 Page 11 of 15
12 Important Clinical Tools & References 1. HOW TO SAVE A LIFE - a condensed list of life-saving surgical and post-operative suggestions for patients with Vascular Ehlers-Danlos Syndrome (a bit dated but succinct) 2. HOW TO SAVE A LIFE downloadable booklet at 3. The Ehlers-Danlos Society. Beighton Score - How to assess Joint Hypermobility. Includes video and downloadable printable version at 4. What is HSD? - The Ehlers Danlos Society Online at 5. Castori M, Tinkle B, Levy H, Grahame R, Malfait F, Hakim A. A framework for the classification of joint hypermobility and related conditions. Am J Med Genet Part C Semin Med Genet C: Online at 6. EDS Types - The Ehlers Danlos Society Online 7. Malfait F, Francomano C, Byers P, et al. The 2017 international classification of the Ehlers Danlos syndromes. Am J Med Genet Part C Semin Med Genet C:8 26. Online 8. The International Consortium on Ehlers-Danlos Syndromes & Related Disorders. Diagnostic Criteria for Hypermobile Ehlers-Danlos Syndrome (heds). Online 9. Tinkle B, Castori M, Berglund B, Cohen H, Grahame R, Kazkaz H, Levy H. Hypermobile Ehlers Danlos syndrome (a.k.a. Ehlers Danlos syndrome Type III and Ehlers Danlos syndrome hypermobility type): Clinical description and natural history. Am J Med Gen. Online at Byers PH, Belmont J, Black J, De Backer J, Frank M, Jeunemaitre X, Johnson D, Pepin M, Robert L, Sanders L, Wheeldon N Diagnosis, natural history, and management in vascular Ehlers Danlos syndrome. Am J Med Genet Part C Semin Med Genet 175C: Online Bowen JM, Sobey GJ, Burrows NP, Colombi M, Lavallee ME, Malfait F, Francomano CA Ehlers Danlos syndrome, classical type. Am J Med Genet Part C Semin Med Genet175C: Online General References 12. Ehlers Danlos Society multiple resources for patients and doctors at Ehlers-Danlos Society collection of important articles for doctors at American Journal of Medical Genetics Part C: Seminars in Medical Genetics. Special Issue: The Ehlers-Danlos Syndromes: Reports from the International Consortium on the Ehlers-Danlos Syndromes March Volume 175, Issue 1. Pages i i, Online at Brady AF, Demirdas S, Fournel-Gigleux S, Ghali N, Giunta C, Kapferer-Seebacher I, Kosho T, Mendoza-Londono R, Pope MF, Rohrbach M, Van Damme T, Vandersteen A, van Mourik C, Voermans N, Zschocke J, Malfait F The Ehlers Danlos syndromes, rare types. Am J Med Genet Part C Semin Med Genet 175C: Online at Hakim A, O'Callaghan C, De Wandele I, Stiles L, Pocinki A, Rowe P Cardiovascular autonomic dysfunction in Ehlers Danlos syndrome Hypermobile type. Am J Med Genet Part C Semin Med Genet 175C: Online at Hakim A, De Wandele I, O'Callaghan C, Pocinki A, Rowe P Chronic fatigue in Ehlers Danlos syndrome Hypermobile type. Am J Med Genet Part C Semin Med Genet175C: Online Fikree A, Chelimsky G, Collins H, Kovacic K, Aziz Q Gastrointestinal involvement in the Ehlers Danlos syndromes. Am J Med Genet Part C Semin Med Genet 175C: Online Ver /07/17 Page 12 of 15
13 19. EricsonJr. WB, Wolman R Orthopaedic management of the Ehlers Danlos syndromes. Am J Med Genet Part C Semin Med Genet 175C: Online HendersonSr. FC, Austin C, Benzel E, Bolognese P, Ellenbogen R, Francomano CA, Ireton C, Klinge P, Koby M, Long D, Patel S, Singman EL, Voermans NC Neurological and spinal manifestations of the Ehlers Danlos syndromes. Am J Med Genet Part C Semin Med Genet175C: Online Chopra P, Tinkle B, Hamonet C, Brock I, Gompel A, Bulbena A, Francomano C Pain management in the Ehlers Danlos syndromes. Am J Med Genet Part C Semin Med Genet175C: Online Mitakides J, Tinkle BT Oral and mandibular manifestations in the Ehlers Danlos syndromes. Am J Med Genet Part C Semin Med Genet 175C: Online Seneviratne SL, Maitland A, Afrin L Mast cell disorders in Ehlers Danlos syndrome. Am J Med Genet Part C Semin Med Genet 175C: Online Bulbena A, Baeza-Velasco C, Bulbena-Cabré A, Pailhez G, Critchley H, Chopra P, Mallorquí-Bagué N, Frank C, Porges S Psychiatric and psychological aspects in the Ehlers Danlos syndromes. Am J Med Genet Part C Semin Med Genet 175C: Online onlinelibrary.wiley.com/doi/ /ajmg.c.31544/full 25. Recommendations for anaesthesia in EDS Wiesmann et al. Orphanet Journal of Rare Diseases 2014, 9:109. Online Local anaesthetic failure in EDS Downloadable brochures - For Physiotherapists 29. Engelbert RH, Juul-Kristensen B, Pacey V, de Wandele I, Smeenk S, Woinarosky N, Sabo S, Scheper MC, Russek L, Simmonds JV The evidence-based rationale for physical therapy treatment of children, adolescents, and adults diagnosed with joint hypermobility syndrome/hypermobile Ehlers Danlos syndrome. Am J Med Genet Part C Semin Med Genet175C: Online at The Muldowney Protocol the book is a How To for patients and physiotherapists to work through together. Available as hard copy Ring splints - For Patients 31,32,33,34,35,36 and Doctors 33 Seeking Advice 32. Ehlers-Danlos Society Patient Support Loosely speaking New Zealand support Facebook page type Loosely Speaking into the Facebook search box. This is a closed group so ask to join. Link is %20ehlers%20danlos%20nz%20support%20group 34. NZORD New Zealand Organisation for Rare Disorders at - includes Specialist Directory 35. Dislocation/subluxation management or I m just popping out for a while! - Jason Parry Genetic and Rare Diseases Information Centre at Myths and facts - for patients - at Ver /07/17 Page 13 of 15

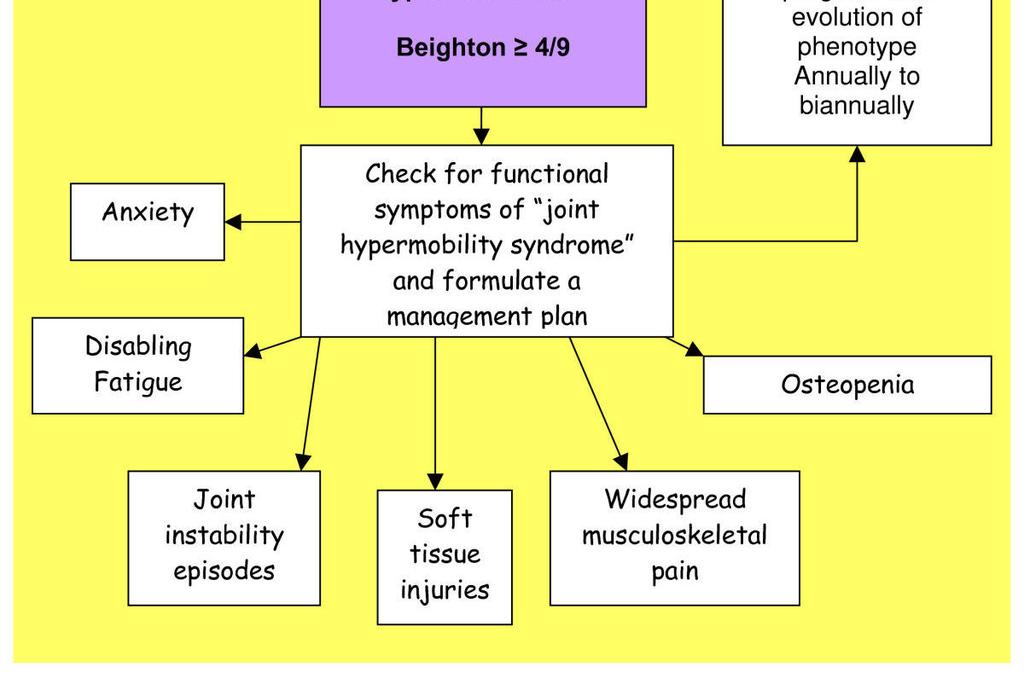

14 Appendix 1 Flowcharts Ver /07/17 Page 14 of 15
15 APPENDIX 2 WORKING GROUP MEMBERS (Alphabetical) NAME ORGANISATION ROLE BURLING; Rheumatologist Auckland Rheumatologist backtolife@iconz.co.nz Fraser CALLEAR; Rachel Hutt Valley DHB Paediatric Rheumatologist Rachel.Callear@huttvalleyd hb.org.nz CAMPBELL- STOKES; Priscilla CRAWFORD; Lisa PRESTON; Matthew ROBERTSON; Stephen TAYLOR; Will Hutt Valley DHB NZORD BOPDHB; Eastbay Radiology Department of Women s and Children s Health Dunedin School of Medicine University of Otago Physiotherapist Paediatric Rheumatologist Hutt Valley DHB Priscilla.Campbell- Stokes@huttvalleydhb.org.n z Relationship Manager Lisa.crawford@nzord.org.nz Medical - Radiologist matpre@gmail.com Curekids Professor of Paediatric Genetics Stephen.robertson@otago. ac.nz P: F: web: /clinical-genetics HYPERMOBILITY AND EDS PATHWAY DOCUMENT LIST To follow This current document is an overview of Hypermobility and EDS. Several of the areas covered require more detailed information to guide management in more detail. As they become available the additional documents will be added alongside this one. # TITLE PURPOSE STATUS CONTACT 1 Hypermobility And Ehlers- Overview and basic Current this Matthew Preston Danlos Syndromes - New Zealand Overview management guidelines with document extensive references 2 Physiotherapy in Hypermobility and EDS Detailed physiotherapy discussion To follow 3 Paediatric aspects of Paediatric specific matters To follow Hypermobility and EDS 4 Genetics in Hypermobility Details of genetics and To follow and EDS 5 Hypermobility and EDS Specific Therapies 6 Hypermobility And Ehlers- Danlos Syndromes - New Zealand Overview Patient Version genetic testing Discussion of therapies including some developing and trial therapies This document written for patients to use. Includes patient-friendly references and support resources. To follow To follow Ver /07/17 Page 15 of 15
Hypermobile Ehlers-Danlos syndrome (heds) vs. Hypermobility Spectrum Disorders (HSD): What s the Difference?
 vs. Hypermobility Spectrum Disorders (HSD): What s the Difference?") Hypermobile Ehlers-Danlos syndrome (heds) vs. Hypermobility Spectrum Disorders (HSD): What s the Difference? There has been a major revision in the approach to joint hypermobility (JH) as a whole. To recognize
Hypermobile Ehlers-Danlos syndrome (heds) vs. Hypermobility Spectrum Disorders (HSD): What s the Difference? There has been a major revision in the approach to joint hypermobility (JH) as a whole. To recognize
ICD-10-CM ICD-10-CM
 Summary: There is currently one ICD-10-CM code for Ehlers-Danlos Syndrome (Q79.6). A new classification of EDS was published in March 2017, defining 13 types of EDS. Physicians providing care for and persons
Summary: There is currently one ICD-10-CM code for Ehlers-Danlos Syndrome (Q79.6). A new classification of EDS was published in March 2017, defining 13 types of EDS. Physicians providing care for and persons
Welcome! Capital Area Ehlers-Danlos Syndrome Support Group
 Welcome! Capital Area Ehlers-Danlos Syndrome Support Group Ehlers-Danlos Syndrome A N O V E R V I E W G A Y L E Y A N K E E, M S N, N P ( R E T. ) J U N E 1 4, 2 0 1 8 What is Ehlers-Danlos Syndrome (EDS)?
Welcome! Capital Area Ehlers-Danlos Syndrome Support Group Ehlers-Danlos Syndrome A N O V E R V I E W G A Y L E Y A N K E E, M S N, N P ( R E T. ) J U N E 1 4, 2 0 1 8 What is Ehlers-Danlos Syndrome (EDS)?
9/7/2017. Ehlers-Danlos Syndrome Hypermobility Type (heds) 5-Point Questionnaire for JHM. Joint Hypermobility Beighton Score
 5-Point Questionnaire for JHM. Joint Hypermobility Beighton Score") http://medicalpicturesinfo.com/wp-content/uploads/2011/08/arachnodactyly-3.jpg 9/7/2017 Ehlers-Danlos Syndrome Hypermobility Type (heds) David Tilstra, MD MBA CentraCare Clinic No Disclosures Objectives:
http://medicalpicturesinfo.com/wp-content/uploads/2011/08/arachnodactyly-3.jpg 9/7/2017 Ehlers-Danlos Syndrome Hypermobility Type (heds) David Tilstra, MD MBA CentraCare Clinic No Disclosures Objectives:
Joint Hypermobility: Diagnosis for Non-Specialists
 Joint Hypermobility: Diagnosis for Non-Specialists This article describes how physician generalists can make useful working diagnoses of most patients with hypermobility syndromes, and proceed with effective
Joint Hypermobility: Diagnosis for Non-Specialists This article describes how physician generalists can make useful working diagnoses of most patients with hypermobility syndromes, and proceed with effective
EDNF Center for Clinical Care & Research at GBMC PHYSICIANS CONFERENCE September 15, 2014
 EDNF Center for Clinical Care & Research at GBMC 2014 PHYSICIANS CONFERENCE September 15, 2014 Pain in Ehlers-Danlos Syndrome Clair A. Francomano, M.D. Director, EDNF Center for Clinical Care and Research
EDNF Center for Clinical Care & Research at GBMC 2014 PHYSICIANS CONFERENCE September 15, 2014 Pain in Ehlers-Danlos Syndrome Clair A. Francomano, M.D. Director, EDNF Center for Clinical Care and Research
Common Questions about Hypermobility Conditions
 Common Questions about Hypermobility Conditions Below is a list of common questions asked by people who have learned they have hypermobile-type Ehlers Danlos Syndrome (heds), and Hypermobility Spectrum
Common Questions about Hypermobility Conditions Below is a list of common questions asked by people who have learned they have hypermobile-type Ehlers Danlos Syndrome (heds), and Hypermobility Spectrum
2017 International Criteria for the Ehlers-Danlos syndromes
 2017 International Criteria for the Ehlers-Danlos syndromes HMSA Statement of Position 20 th February 2017 The Hypermobility Syndromes Association (HMSA) wishes to respond to its Members concerns following
2017 International Criteria for the Ehlers-Danlos syndromes HMSA Statement of Position 20 th February 2017 The Hypermobility Syndromes Association (HMSA) wishes to respond to its Members concerns following
Ehlers-Danlos Syndromes Overview for primary care providers
 Ehlers-Danlos Syndromes Overview for primary care providers Roberto Mendoza-Londono MD, MSc, FCCMG, FRCPC Medical Director-EDS service, Hospital for Sick Children/UHN Interim Division Head, Genetics, HSC
Ehlers-Danlos Syndromes Overview for primary care providers Roberto Mendoza-Londono MD, MSc, FCCMG, FRCPC Medical Director-EDS service, Hospital for Sick Children/UHN Interim Division Head, Genetics, HSC
HYPERLAXITY SYNDROME Symptoms Questions to the patient Signs Acute or Traumatic Chronic or Nontraumatic
 A 30 year old project manager, who is new to your general practice, presents with right anterior knee pain after slipping and landing on his knee three months ago. Imaging shows no abnormality, but he
A 30 year old project manager, who is new to your general practice, presents with right anterior knee pain after slipping and landing on his knee three months ago. Imaging shows no abnormality, but he
The 2017 EDS/HSD Classification. May 3, 2017
 The 2017 Interntional Classification papers were published after peer review on March 17, 2017 in the American Journal of Human Genetics. They were written by the International Consortium on Ehlers-Danlos
The 2017 Interntional Classification papers were published after peer review on March 17, 2017 in the American Journal of Human Genetics. They were written by the International Consortium on Ehlers-Danlos
Currently at Cincinnati Children s Hospital As of 9/1/12, will be at Lutheran General Hospital in Chicago
 EDS and TOMORROW NO financial disclosures Currently at Cincinnati Children s Hospital As of 9/1/12, will be at Lutheran General Hospital in Chicago Also serve on the Board of Directors of the Ehlers-Danlos
EDS and TOMORROW NO financial disclosures Currently at Cincinnati Children s Hospital As of 9/1/12, will be at Lutheran General Hospital in Chicago Also serve on the Board of Directors of the Ehlers-Danlos
Coverage Guidelines. Genetic Testing and Counseling for Ehlers-Danlos Syndrome (EDS)
") Coverage Guidelines Genetic Testing and Counseling for Ehlers-Danlos Syndrome (EDS) Disclaimer: Please note that Baptist Health Plan Coverage Guidelines may be updated throughout the year. A printed version
Coverage Guidelines Genetic Testing and Counseling for Ehlers-Danlos Syndrome (EDS) Disclaimer: Please note that Baptist Health Plan Coverage Guidelines may be updated throughout the year. A printed version
EHLERS DANLOS SYNDROME. Fransiska Malfait, MD PhD Centre for Medical Genetics Ghent University Hospital Ghent, Belgium
 EHLERS DANLOS SYNDROME Fransiska Malfait, MD PhD Centre for Medical Genetics Ghent University Hospital Ghent, Belgium EDS is a heritable collagen disorder Heterogeneous group of diseases with: - Multi-systemic
EHLERS DANLOS SYNDROME Fransiska Malfait, MD PhD Centre for Medical Genetics Ghent University Hospital Ghent, Belgium EDS is a heritable collagen disorder Heterogeneous group of diseases with: - Multi-systemic
EHLERS-DANLOS SYNDROME (EDS) ADULT PROGRAM REFERRAL PACKAGE
 ADULT PROGRAM REFERRAL PACKAGE") EHLERS-DANLOS SYNDROME (EDS) ADULT PROGRAM REFERRAL PACKAGE In order to request assessment for adults at the EDS Program at Toronto General Hospital, please complete the form below and append the requested
EHLERS-DANLOS SYNDROME (EDS) ADULT PROGRAM REFERRAL PACKAGE In order to request assessment for adults at the EDS Program at Toronto General Hospital, please complete the form below and append the requested
Hypermobile type Ehlers-Danlos syndrome (heds) is the. Hypermobile Ehlers-Danlos Syndrome: Clinical Description and Natural History FOR NON-EXPERTS
 is the. Hypermobile Ehlers-Danlos Syndrome: Clinical Description and Natural History FOR NON-EXPERTS") The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers Danlos syndromes (EDS) are a mixed group of. Neurological and Spinal Manifestations of the Ehlers-Danlos Syndromes FOR NON-EXPERTS
 are a mixed group of. Neurological and Spinal Manifestations of the Ehlers-Danlos Syndromes FOR NON-EXPERTS") The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
Joining The Dots - EDS
 Joining The Dots - EDS Ehlers-Danlos Syndrome (EDS) named after physicians Ehlers and Danlos turn of 20th Century What is EDS? 2017 new classification -up to date encompasses 14 different individual genetic
Joining The Dots - EDS Ehlers-Danlos Syndrome (EDS) named after physicians Ehlers and Danlos turn of 20th Century What is EDS? 2017 new classification -up to date encompasses 14 different individual genetic
Joint hypermobility is a feature commonly encountered in
 The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The role of orthopedic surgery in the Ehlers-Danlos syndromes
 The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
Evidence suggests a link between connective tissue disorders
 The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
Ehlers-Danlos Syndrome
 OFFICE OF MEDICAL CANNABIS Ehlers-Danlos Syndrome SEPTEMBER 2016 Introduction Briefings such as this one are prepared in response to petitions to add new conditions to the list of qualifying conditions
OFFICE OF MEDICAL CANNABIS Ehlers-Danlos Syndrome SEPTEMBER 2016 Introduction Briefings such as this one are prepared in response to petitions to add new conditions to the list of qualifying conditions
Definitions of joint hypermobility: o Joint hypermobility (JH): Capability for a joint to move beyond normal physiological limits.
: Capability for a joint to move beyond normal physiological limits.") Definitions of joint hypermobility: o Joint hypermobility (JH): Capability for a joint to move beyond normal physiological limits. Descriptor, not diagnosis Also known as joint laxity, double-jointedness,
Definitions of joint hypermobility: o Joint hypermobility (JH): Capability for a joint to move beyond normal physiological limits. Descriptor, not diagnosis Also known as joint laxity, double-jointedness,
Vascular Ehlers- Danlos in the pediatric population
 Vascular Ehlers- Danlos in the pediatric population Shaine A. Morris, MD, MPH Pediatric Cardiology Texas Children s Hospital, Baylor College of Medicine Objectives Learn what Vascular EDS is, and how it
Vascular Ehlers- Danlos in the pediatric population Shaine A. Morris, MD, MPH Pediatric Cardiology Texas Children s Hospital, Baylor College of Medicine Objectives Learn what Vascular EDS is, and how it
TEACHERS GUIDE. For students with Ehlers Danlos Syndrome/EDS INFORMATION IN THIS GUIDE WAS GATHERED AND EDITED BY
 TEACHERS GUIDE For students with Ehlers Danlos Syndrome/EDS INFORMATION IN THIS GUIDE WAS GATHERED AND EDITED BY Andrea D Julian ACE CPT, Patient, Parent, Advocate Special thanks to: Sheila Roush PT NCS
TEACHERS GUIDE For students with Ehlers Danlos Syndrome/EDS INFORMATION IN THIS GUIDE WAS GATHERED AND EDITED BY Andrea D Julian ACE CPT, Patient, Parent, Advocate Special thanks to: Sheila Roush PT NCS
Inheritable Connective Tissue Diseases: Or It s Probably Not Marfan s. RJ Willes 4/23/2018
 Inheritable Connective Tissue Diseases: Or It s Probably Not Marfan s RJ Willes 4/23/2018 This pretty much sums it up. Inheritable Connective tissues diseases A homogenous collection of varied syndromes
Inheritable Connective Tissue Diseases: Or It s Probably Not Marfan s RJ Willes 4/23/2018 This pretty much sums it up. Inheritable Connective tissues diseases A homogenous collection of varied syndromes
Alison Middleditch MCSP MMACP Director of Surrey Physiotherapy and is based in Coulsdon, Surrey
 Alison Middleditch MCSP MMACP Director of Surrey Physiotherapy and is based in Coulsdon, Surrey Alison qualified from Kings College Hospital and has worked in both the NHS and Private Practice. She held
Alison Middleditch MCSP MMACP Director of Surrey Physiotherapy and is based in Coulsdon, Surrey Alison qualified from Kings College Hospital and has worked in both the NHS and Private Practice. She held
Postural Tachycardia Syndrome and Hypermobility Syndrome
 Postural Tachycardia Syndrome and Hypermobility Syndrome Blair P. Grubb MD FACC Departments of Medicine and Pediatrics Health Science Campus University of Toledo Toledo, Ohio USA Over the years it became
Postural Tachycardia Syndrome and Hypermobility Syndrome Blair P. Grubb MD FACC Departments of Medicine and Pediatrics Health Science Campus University of Toledo Toledo, Ohio USA Over the years it became
EDS my first 50 years!
 EDS my first 50 years! Rodney Grahame Honorary Professor UCL Unit for Rheumatology & Connective Tissue Disease, University College London and the London International Hypermobility Clinic MARS AND VENUS
EDS my first 50 years! Rodney Grahame Honorary Professor UCL Unit for Rheumatology & Connective Tissue Disease, University College London and the London International Hypermobility Clinic MARS AND VENUS
Classical Ehlers-Danlos Syndrome
 Classical Ehlers-Danlos Syndrome Clair A. Francomano, MD EDS Center for Clinical Care and Research Harvey Ins>tute for Human Gene>cs Greater Bal>more Medical Center Commi5ee Members Jessica M. Bowen Glenda
Classical Ehlers-Danlos Syndrome Clair A. Francomano, MD EDS Center for Clinical Care and Research Harvey Ins>tute for Human Gene>cs Greater Bal>more Medical Center Commi5ee Members Jessica M. Bowen Glenda
Ehlers-Danlos Syndrome (EDS) at a Glance
 at a Glance") Ehlers-Danlos Syndrome (EDS) at a Glance The Ehlers Danlos Syndromes (EDS) is a group of hereditary connective tissue disorders that primarily affect the skin and joints. Connective tissue provides support
Ehlers-Danlos Syndrome (EDS) at a Glance The Ehlers Danlos Syndromes (EDS) is a group of hereditary connective tissue disorders that primarily affect the skin and joints. Connective tissue provides support
PROFESSOR RODNEY GRAHAME THE HYPERMOBILITY UNIT, LONDON & UNIVERSITY COLLEGE LONDON
 PROFESSOR RODNEY GRAHAME THE HYPERMOBILITY UNIT, LONDON & UNIVERSITY COLLEGE LONDON EDS EDS 1 FREDERICK PARKES-WEBER (1863-1962) 1200 medical articles + 23 books over 50 years; 7 eponymous diseases including
PROFESSOR RODNEY GRAHAME THE HYPERMOBILITY UNIT, LONDON & UNIVERSITY COLLEGE LONDON EDS EDS 1 FREDERICK PARKES-WEBER (1863-1962) 1200 medical articles + 23 books over 50 years; 7 eponymous diseases including
The 2017 EDS International Classification. Your Questions Answered
 The 2017 EDS International Classification Your Questions Answered New Terminology 2017 EDS International Classification: Your Questions Answered 1 This is an exciting time in the history of the Ehlers-Danlos
The 2017 EDS International Classification Your Questions Answered New Terminology 2017 EDS International Classification: Your Questions Answered 1 This is an exciting time in the history of the Ehlers-Danlos
Pain. No Energy. Trouble Doing Things. Other Problems
 Self-Care for Kids & Teens with Hypermobility Spectrum Disorder Dr. Leslie Russek, PT, DPT, PhD, OCS Clarkson University What bothers you the most? Hips, knees, feet Shoulders, elbows Low back Neck, etc.
Self-Care for Kids & Teens with Hypermobility Spectrum Disorder Dr. Leslie Russek, PT, DPT, PhD, OCS Clarkson University What bothers you the most? Hips, knees, feet Shoulders, elbows Low back Neck, etc.
Hypermobility Syndromes. Middlesbrough Masterclass Nov 2013
 Hypermobility Syndromes Middlesbrough Masterclass Nov 2013 Speakers Dr Alan Hakim - Physician & Rheumatologist Dr Jane Simmonds- Physiotherapist They work at a specialist HM Unit for the diagnosis & management
Hypermobility Syndromes Middlesbrough Masterclass Nov 2013 Speakers Dr Alan Hakim - Physician & Rheumatologist Dr Jane Simmonds- Physiotherapist They work at a specialist HM Unit for the diagnosis & management
When a headache never goes away - Chronic daily headache in a teenager
 PBLD Table #6 When a headache never goes away - Chronic daily headache in a teenager Moderators: Taran Sangari M.D., Shailesh Shah M.D. Institution: Valley Children s Hospital, Madera, CA Objectives: Discuss
PBLD Table #6 When a headache never goes away - Chronic daily headache in a teenager Moderators: Taran Sangari M.D., Shailesh Shah M.D. Institution: Valley Children s Hospital, Madera, CA Objectives: Discuss
Instability due to disorders of collagen metabolism and inflammation
 Instability due to disorders of collagen metabolism and inflammation Chris Holroyd Consultant Rheumatologist University Hospital Southampton NHS Foundation Trust Outline Overview of hypermobility Genetic
Instability due to disorders of collagen metabolism and inflammation Chris Holroyd Consultant Rheumatologist University Hospital Southampton NHS Foundation Trust Outline Overview of hypermobility Genetic
Inherited Connective Tissue Disorders
 Inherited Connective Tissue Disorders Staci Kallish, DO Hospital of the University of Pennsylvania Perelman School of Medicine Department of Medicine Division of Translational Medicine and Human Genetics
Inherited Connective Tissue Disorders Staci Kallish, DO Hospital of the University of Pennsylvania Perelman School of Medicine Department of Medicine Division of Translational Medicine and Human Genetics
Carpal Tunnel Syndrome
 Patient information Carpal Tunnel Syndrome i Important information for all patients having Carpal Tunnel surgery. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
Patient information Carpal Tunnel Syndrome i Important information for all patients having Carpal Tunnel surgery. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging
 Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
Shoulder distension. Orthopaedic department. yeovilhospital.nhs.uk
 Shoulder distension Orthopaedic department 01935 384 159 yeovilhospital.nhs.uk This information booklet has been produced to help you gain the maximum benefit after your operation. It is not a substitute
Shoulder distension Orthopaedic department 01935 384 159 yeovilhospital.nhs.uk This information booklet has been produced to help you gain the maximum benefit after your operation. It is not a substitute
Wisconsin Integrative Pain Specialists
 Patient Information Today s Date: Patient s Name: DOB: Age: Gender: Marital Status: M S D What would you like us to call you? Address: City, State, Zip: Home Phone: Cell Phone: Work Phone: Email: Preferred
Patient Information Today s Date: Patient s Name: DOB: Age: Gender: Marital Status: M S D What would you like us to call you? Address: City, State, Zip: Home Phone: Cell Phone: Work Phone: Email: Preferred
Chapter 30 - Musculoskeletal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Exclude referred pain from the neck, diaphragm, heart, lungs, & polymyalgia rheumatica YES. NSAIDs/analgesics as required
 Shoulder Pain Clinical Presentation info for GPs who refer into PAH more info History and Examination Exclude referred pain from the neck, diaphragm, heart, lungs, & polymyalgia rheumatica more info for
Shoulder Pain Clinical Presentation info for GPs who refer into PAH more info History and Examination Exclude referred pain from the neck, diaphragm, heart, lungs, & polymyalgia rheumatica more info for
WRIST SPRAIN. Description
 WRIST SPRAIN Description Other sports, such as skiing, bowling, pole vaulting Wrist sprain is a violent overstretching and tearing of one Poor physical conditioning (strength and flexibility) or more ligaments
WRIST SPRAIN Description Other sports, such as skiing, bowling, pole vaulting Wrist sprain is a violent overstretching and tearing of one Poor physical conditioning (strength and flexibility) or more ligaments
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health
 T M J D I S O R D E R S U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health CONTENTS 2 4 6 7 8 9 14 WHAT IS THE TEMPOROMANDIBULAR JOINT? WHAT ARE TMJ DISORDERS? WHAT CAUSES TMJ DISORDERS?
T M J D I S O R D E R S U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health CONTENTS 2 4 6 7 8 9 14 WHAT IS THE TEMPOROMANDIBULAR JOINT? WHAT ARE TMJ DISORDERS? WHAT CAUSES TMJ DISORDERS?
NORTH BAY SYMPOSIUM SATURDAY JANUARY 20 TH 2018
 NORTH BAY SYMPOSIUM SATURDAY JANUARY 20 TH 2018 ROBERT HAIMSON, M.D. ORTHOPEDIC SURGEON SMGR FELLOW IN AAOS DIPLOMATE IN ABOS COMMON MUSCULOSKELETAL CONDITIONS COMMON MUSCULOSKELETAL CONDITIONS: WHAT
NORTH BAY SYMPOSIUM SATURDAY JANUARY 20 TH 2018 ROBERT HAIMSON, M.D. ORTHOPEDIC SURGEON SMGR FELLOW IN AAOS DIPLOMATE IN ABOS COMMON MUSCULOSKELETAL CONDITIONS COMMON MUSCULOSKELETAL CONDITIONS: WHAT
All rights reserved.
 RODNEY GRAHAME UNIVERSITY COLLEGE LONDON SCHOOL OF MEDICINE, U. WASHINGTON HMS 1967 EDS III 1968 (KIRK et al) (BEIGHTON) RHEUMATOLOGY GENETICS ERIC BYWATERS VICTOR McKUSICK HMS 1967 EDS III 1968 (KIRK
RODNEY GRAHAME UNIVERSITY COLLEGE LONDON SCHOOL OF MEDICINE, U. WASHINGTON HMS 1967 EDS III 1968 (KIRK et al) (BEIGHTON) RHEUMATOLOGY GENETICS ERIC BYWATERS VICTOR McKUSICK HMS 1967 EDS III 1968 (KIRK
Forthomme B, Croisier JL, Crielaard JM. Departement of physical medicine and rehabilitation ULg.
 Contribution to an adapted physiotherapy in the hyperlaxity syndromes. Kaux JF, Foidart-Dessalle M, Toussaint G, Forthomme B, Croisier JL, Crielaard JM. Departement of physical medicine and rehabilitation
Contribution to an adapted physiotherapy in the hyperlaxity syndromes. Kaux JF, Foidart-Dessalle M, Toussaint G, Forthomme B, Croisier JL, Crielaard JM. Departement of physical medicine and rehabilitation
West Suffolk Hospital
 For staff use only: Patient Details: First names: Hospital no: (Use hospital identification label) West Suffolk Hospital Patient information leaflet Carpal Tunnel Syndrome 2-3 Patient agreement to investigation
For staff use only: Patient Details: First names: Hospital no: (Use hospital identification label) West Suffolk Hospital Patient information leaflet Carpal Tunnel Syndrome 2-3 Patient agreement to investigation
SAMPLE. Osteopathy and Back pain a safe and effective approach
 Osteopathy and Back pain a safe and effective approach Back pain will affect 8 out of 10 people at some point in their life - mild or severe, acute or chronic. Common causes of back pain include: heavy
Osteopathy and Back pain a safe and effective approach Back pain will affect 8 out of 10 people at some point in their life - mild or severe, acute or chronic. Common causes of back pain include: heavy
Acute Lower Back Pain. Physiotherapy department
 Acute Lower Back Pain Physiotherapy department Back pain is a common condition and in the UK it affects 7 out of 10 people at some point in their lives. Back pain can be very uncomfortable but it is not
Acute Lower Back Pain Physiotherapy department Back pain is a common condition and in the UK it affects 7 out of 10 people at some point in their lives. Back pain can be very uncomfortable but it is not
A Patient s Guide to Elbow Dislocation
 A Patient s Guide to Elbow Dislocation 2 Introduction When the joint surfaces of an elbow are forced apart, the elbow is dislocated. The elbow is the second most commonly dislocated joint in adults (after
A Patient s Guide to Elbow Dislocation 2 Introduction When the joint surfaces of an elbow are forced apart, the elbow is dislocated. The elbow is the second most commonly dislocated joint in adults (after
About Arthritis
 About Arthritis www.arthritis.org.nz Did you know? Arthritis affects more than 530,000 New Zealanders. In fact, it is the greatest cause of disability in this country. Arthritis literally means inflammation
About Arthritis www.arthritis.org.nz Did you know? Arthritis affects more than 530,000 New Zealanders. In fact, it is the greatest cause of disability in this country. Arthritis literally means inflammation
Non-inflammatory joint pain
 Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Ehlers-Danlos Syndrome (EDS) at a Glance
 at a Glance") Ehlers-Danlos Syndrome (EDS) at a Glance Ehlers Danlos Syndrome (EDS) is a group of hereditary disorders that affect mainly the skin and joints. EDS results in weakness and/or excessive flexibility of
Ehlers-Danlos Syndrome (EDS) at a Glance Ehlers Danlos Syndrome (EDS) is a group of hereditary disorders that affect mainly the skin and joints. EDS results in weakness and/or excessive flexibility of
Hypermobility and Ehlers-Danos Syndromes
 Hypermobility and Ehlers-Danos Syndromes An Overview of the Classification Anna Higo MCSP Overview The 2017 International Classification of the Ehlers Danos Syndromes Where does Hypermobility fit? Current
Hypermobility and Ehlers-Danos Syndromes An Overview of the Classification Anna Higo MCSP Overview The 2017 International Classification of the Ehlers Danos Syndromes Where does Hypermobility fit? Current
Carpal Tunnel Decompression Surgery. (Minor procedure in Primary Care)
") Carpal Tunnel Decompression Surgery (Minor procedure in Primary Care) Information for Patients Gateshead Upper Limb Unit Page 1 of 5 What is carpal tunnel syndrome? Carpal tunnel syndrome is a common condition
Carpal Tunnel Decompression Surgery (Minor procedure in Primary Care) Information for Patients Gateshead Upper Limb Unit Page 1 of 5 What is carpal tunnel syndrome? Carpal tunnel syndrome is a common condition
Shoulder acromioclavicular joint injury Information for patients Out Patient Fracture Care Team: Shared care plan
 Shoulder acromioclavicular joint injury Information for patients Out Patient Fracture Care Team: Shared care plan Orthopaedic Department Tunbridge Wells Hospital Tonbridge Road Pembury TN2 4QJ Telephone:
Shoulder acromioclavicular joint injury Information for patients Out Patient Fracture Care Team: Shared care plan Orthopaedic Department Tunbridge Wells Hospital Tonbridge Road Pembury TN2 4QJ Telephone:
NEURO QUIZ 45 EHLERS DANLOS SYNDROME
 NEURO QUIZ 45 EHLERS DANLOS SYNDROME Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D START 1. Regarding
NEURO QUIZ 45 EHLERS DANLOS SYNDROME Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D START 1. Regarding
A new website is underconstruction with the latesest updated information. Please us ethe below as a general guide only.
 Important Note A new website is underconstruction with the latesest updated information. Please us ethe below as a general guide only. The Below has become of historical interest only. Reproduced verbatim
Important Note A new website is underconstruction with the latesest updated information. Please us ethe below as a general guide only. The Below has become of historical interest only. Reproduced verbatim
Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai
 Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai Case History 9 year old boy presented with a 3 week history of: Swelling of major lower limb joints Progression was additive (right ankle followed
Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai Case History 9 year old boy presented with a 3 week history of: Swelling of major lower limb joints Progression was additive (right ankle followed
Ehlers Danlos Syndrome in an Adult Woman: A Hidden Syndrome
 Ehlers Danlos Syndrome in an Adult Woman: A Hidden Syndrome Diana Spinelli a, Francesca Minonzio b, Alessandra Bassotti c, Cinzia Hu b, Maria Domenica Cappellini a,b,c a Specialty of Internal Medicine,
Ehlers Danlos Syndrome in an Adult Woman: A Hidden Syndrome Diana Spinelli a, Francesca Minonzio b, Alessandra Bassotti c, Cinzia Hu b, Maria Domenica Cappellini a,b,c a Specialty of Internal Medicine,
Assisting hand and arm recovery after stroke
 INFORMATION FOR PATIENTS Assisting hand and arm recovery after stroke Positioning your arm When your arm is affected by a stroke it is important to protect it from injury and to try to keep it in a normal
INFORMATION FOR PATIENTS Assisting hand and arm recovery after stroke Positioning your arm When your arm is affected by a stroke it is important to protect it from injury and to try to keep it in a normal
Staff Information Leaflet
 Posture Staff Information Leaflet This leaflet is designed to give you an understanding of posture and some advice on what you can do to help yourself. If your symptoms persist you should seek advice from
Posture Staff Information Leaflet This leaflet is designed to give you an understanding of posture and some advice on what you can do to help yourself. If your symptoms persist you should seek advice from
Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair Elbow Anatomy Spectrum of injuries
 Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair This information aims to help you understand your condition and gain maximum benefit from your
Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair This information aims to help you understand your condition and gain maximum benefit from your
A Patient s Guide to Carpal Tunnel Syndrome
 A Patient s Guide to Carpal Tunnel Syndrome Concord Orthopaedics 264 Pleasant Street Concord, NH 03301 Phone: 6032243368 Fax: 6032287268 marketing.copa@concordortho.com DISCLAIMER: The information in this
A Patient s Guide to Carpal Tunnel Syndrome Concord Orthopaedics 264 Pleasant Street Concord, NH 03301 Phone: 6032243368 Fax: 6032287268 marketing.copa@concordortho.com DISCLAIMER: The information in this
Common Elbow Problems
 Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
A Patient s Guide to Elbow Dislocation
 A Patient s Guide to Elbow Dislocation 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet
A Patient s Guide to Elbow Dislocation 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet
Basics of Soft- Tissue Examination
 Basics of Soft- Tissue Examination Basics of Soft Tissue Exam For practitioners who primarily use their hands to treat the human structure: Examination must include functional tests to determine the type
Basics of Soft- Tissue Examination Basics of Soft Tissue Exam For practitioners who primarily use their hands to treat the human structure: Examination must include functional tests to determine the type
Total elbow replacement. Information for patients Orthopaedics - Upper Limb
 Total elbow replacement Information for patients Orthopaedics - Upper Limb Introduction The Upper Limb Unit team would like you and your family to understand as much as possible about the operation you
Total elbow replacement Information for patients Orthopaedics - Upper Limb Introduction The Upper Limb Unit team would like you and your family to understand as much as possible about the operation you
Total Elbow Replacement Operation
 Total Elbow Replacement Operation Information for patients The Nottingham Shoulder and Elbow Unit This document can be provided in different languages and formats. For more information please contact:
Total Elbow Replacement Operation Information for patients The Nottingham Shoulder and Elbow Unit This document can be provided in different languages and formats. For more information please contact:
DEPARTMENT OF PEDIATRIC CARDIOLOGY AND CARDIAC SURGERY Pediatric Cardiology and Cardiac Arrhythmia/Syncope Unit Responsible: Dr.
 Title of Project Heart and rhythm disorders in children with Ehlers-Danlos syndrome: Principal Investigator Information: Fabrizio Drago, MD Head of IRCCS Children Hospital and Research Institute Piazza
Title of Project Heart and rhythm disorders in children with Ehlers-Danlos syndrome: Principal Investigator Information: Fabrizio Drago, MD Head of IRCCS Children Hospital and Research Institute Piazza
Referral Criteria: Carpal Tunnel Syndrome Feb
 Referral Criteria: Carpal Tunnel Syndrome Feb 2019 1 5.2. Carpal Tunnel Syndrome Background Carpal tunnel syndrome present with non-traumatic tingling of the fingers due to compression of the median nerve
Referral Criteria: Carpal Tunnel Syndrome Feb 2019 1 5.2. Carpal Tunnel Syndrome Background Carpal tunnel syndrome present with non-traumatic tingling of the fingers due to compression of the median nerve
Acromioclavicular Joint Injury (dislocation) Shoulder 3
 Shoulder 3") Acromioclavicular Joint Injury (dislocation) Shoulder 3 Fracture Care Team: Shared Care Plan Eastbourne 01323 414928 Conquest - 01424 757576 Email - esht.vfc@nhs.net This information leaflet follows up
Acromioclavicular Joint Injury (dislocation) Shoulder 3 Fracture Care Team: Shared Care Plan Eastbourne 01323 414928 Conquest - 01424 757576 Email - esht.vfc@nhs.net This information leaflet follows up
UNIT 2.- SPORT INJURIES: SYMPTOMS AND TREATMENT
 UNIT 2.- SPORT INJURIES: SYMPTOMS AND TREATMENT Every year, millions of teenagers participate in high school sports. An injury to a high school athlete can be a significant disappointment for the teen,
UNIT 2.- SPORT INJURIES: SYMPTOMS AND TREATMENT Every year, millions of teenagers participate in high school sports. An injury to a high school athlete can be a significant disappointment for the teen,
RISKS AND COMPLICATIONS
 PATIENT INFORMATION SHEET RISKS AND COMPLICATIONS TOTAL HIP REPLACEMENT Page 1 of 8 INTRODUCTION A hip replacement is an extremely successful operation. At least 95% of patients are satisfied with their
PATIENT INFORMATION SHEET RISKS AND COMPLICATIONS TOTAL HIP REPLACEMENT Page 1 of 8 INTRODUCTION A hip replacement is an extremely successful operation. At least 95% of patients are satisfied with their
Contents. Introduction 3. Neck Pain 7. Shoulder Pain - Gradual Onset 9. Shoulder Pain Acute onset 11. Elbow Pain 13.
 1 Contents Introduction 3 Neck Pain 7 Shoulder Pain - Gradual Onset 9 Shoulder Pain Acute onset 11 Elbow Pain 13 Low Back Pain 15 Knee Pain Gradual Onset 17 Knee Pain Acute Onset 19 Shin Pain 21 Ankle
1 Contents Introduction 3 Neck Pain 7 Shoulder Pain - Gradual Onset 9 Shoulder Pain Acute onset 11 Elbow Pain 13 Low Back Pain 15 Knee Pain Gradual Onset 17 Knee Pain Acute Onset 19 Shin Pain 21 Ankle
Arthroscopic capsular release. Information for patients Orthopaedics - Upper Limb
 Arthroscopic capsular release Information for patients Orthopaedics - Upper Limb Introduction The Upper Limb Unit team would like you and your family to understand as much as possible about the operation
Arthroscopic capsular release Information for patients Orthopaedics - Upper Limb Introduction The Upper Limb Unit team would like you and your family to understand as much as possible about the operation
Dupuytren s Contracture. Produced by The Orthopaedic Hand and Upper Limb Service
 Dupuytren s Contracture Produced by The Orthopaedic Hand and Upper Limb Service What is Dupuytren s disease? The soft tissues in your hand and fingers are arranged in special layers. The layer just under
Dupuytren s Contracture Produced by The Orthopaedic Hand and Upper Limb Service What is Dupuytren s disease? The soft tissues in your hand and fingers are arranged in special layers. The layer just under
Chronic Shoulder Instability
 Chronic Shoulder Instability The shoulder is the most moveable joint in your body. It helps you to lift your arm, to rotate it, and to reach up over your head. It is able to turn in many directions. This
Chronic Shoulder Instability The shoulder is the most moveable joint in your body. It helps you to lift your arm, to rotate it, and to reach up over your head. It is able to turn in many directions. This
How to Protect Your Joints
 Form: D-5855 How to Protect Your Joints For people with arthritis Arthritis can be painful and make every day activities difficult. This booklet will show you how to protect your joints. This can help
Form: D-5855 How to Protect Your Joints For people with arthritis Arthritis can be painful and make every day activities difficult. This booklet will show you how to protect your joints. This can help
Joint hypermobility is a liability for the performing artist
 International Symposium on Performance Science ISBN 978-90-9022484-8 The Author 2007, Published by the AEC All rights reserved Joint hypermobility is a liability for the performing artist Rodney Grahame
International Symposium on Performance Science ISBN 978-90-9022484-8 The Author 2007, Published by the AEC All rights reserved Joint hypermobility is a liability for the performing artist Rodney Grahame
Clavicle (Collar bone) Fracture (undisplaced) Shoulder 4
 Fracture (undisplaced) Shoulder 4") Clavicle (Collar bone) Fracture (undisplaced) Shoulder 4 Fracture Care Team: Shared Care Plan Eastbourne - 01323 414928 Conquest - 01424 757576 Email - esht.vfc@nhs.net This information leaflet follows
Clavicle (Collar bone) Fracture (undisplaced) Shoulder 4 Fracture Care Team: Shared Care Plan Eastbourne - 01323 414928 Conquest - 01424 757576 Email - esht.vfc@nhs.net This information leaflet follows
Ankle Fracture Orthopaedic Department Patient Information Leaflet. Under review. Page 1
 Ankle Fracture Orthopaedic Department Patient Information Leaflet Page 1 Ankle Fracture Welcome to the Dudley Group NHS Foundation Trust. This leaflet will provide you with information regarding the diagnosis
Ankle Fracture Orthopaedic Department Patient Information Leaflet Page 1 Ankle Fracture Welcome to the Dudley Group NHS Foundation Trust. This leaflet will provide you with information regarding the diagnosis
物理治療中心. Physiotherapy Centre. Multi-disciplinary Chronic Pain Rehabilitation Programme. Physiotherapy Centre. Physiotherapy Centre
 物理治療中心 Physiotherapy Centre Multi-disciplinary Chronic Pain Rehabilitation Programme For enquiries and appointments, please contact us at: Physiotherapy Centre 5/F, Li Shu Pui Block Hong Kong Sanatorium
物理治療中心 Physiotherapy Centre Multi-disciplinary Chronic Pain Rehabilitation Programme For enquiries and appointments, please contact us at: Physiotherapy Centre 5/F, Li Shu Pui Block Hong Kong Sanatorium
P.O. Box Sierra Park Road Mammoth Lakes, CA Orthopedic Surgery & Sports Medicine
 P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb
 Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb Introduction Trigger finger and trigger thumb are conditions affecting the movement of the tendons as they bend the
Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb Introduction Trigger finger and trigger thumb are conditions affecting the movement of the tendons as they bend the
Shoulder Stabilisation A guide for patients Gateshead Upper Limb Unit Mr Andreas Hinsche Mr John Harrison Mr Jagannath Chakravarthy
 Shoulder Stabilisation A guide for patients Gateshead Upper Limb Unit Mr Andreas Hinsche Mr John Harrison Mr Jagannath Chakravarthy Page 1 of 7 Shoulder Instability Your shoulder is a ball and socket joint
Shoulder Stabilisation A guide for patients Gateshead Upper Limb Unit Mr Andreas Hinsche Mr John Harrison Mr Jagannath Chakravarthy Page 1 of 7 Shoulder Instability Your shoulder is a ball and socket joint
many patients seen on secondary referral as normal results in the presence of what had been considered
 Archives of Disease in Childhood, 1983, 58, 988-992 Articular hypermobility simulating chronic rheumatic disease R M LEWKONIA AND B M ANSELL Division of Rheumatology, Medical Research Council Clinical
Archives of Disease in Childhood, 1983, 58, 988-992 Articular hypermobility simulating chronic rheumatic disease R M LEWKONIA AND B M ANSELL Division of Rheumatology, Medical Research Council Clinical
Preferred phone: Best time to call you: Morning Afternoon Evening
 Page 1 of 7 Address: City: State: Zip: County: Email address: Phone Number: (Home) (Work) (Cell) Preferred phone: Best time to call you: Morning Afternoon Evening CONTACT INFORMATION Patients over 18 years
Page 1 of 7 Address: City: State: Zip: County: Email address: Phone Number: (Home) (Work) (Cell) Preferred phone: Best time to call you: Morning Afternoon Evening CONTACT INFORMATION Patients over 18 years
RISKS AND COMPLICATIONS
 PATIENT INFORMATION SHEET RISKS AND COMPLICATIONS TOTAL HIP REPLACEMENT Page 1 of 12 RISKS AND COMPLICATIONS - TOTAL HIP REPLACEMENT Index Pages INTRODUCTION 3 (1) ANAESTHETIC AND MEDICAL: 4 (2) BLOOD
PATIENT INFORMATION SHEET RISKS AND COMPLICATIONS TOTAL HIP REPLACEMENT Page 1 of 12 RISKS AND COMPLICATIONS - TOTAL HIP REPLACEMENT Index Pages INTRODUCTION 3 (1) ANAESTHETIC AND MEDICAL: 4 (2) BLOOD
International Symposium on the Ehlers-Danlos Syndromes
 It is with great pleasure that we invite you to participate in the International Symposium on the Ehlers-Danlos Syndromes September 26 29, 2018 The conference will take place in beautiful Ghent, Belgium,
It is with great pleasure that we invite you to participate in the International Symposium on the Ehlers-Danlos Syndromes September 26 29, 2018 The conference will take place in beautiful Ghent, Belgium,
Stabilisation of the shoulder joint
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Stabilisation of the shoulder joint Physiotherapy Department Information leaflet for Name of Patient: Date: Name of Physiotherapist:
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Stabilisation of the shoulder joint Physiotherapy Department Information leaflet for Name of Patient: Date: Name of Physiotherapist:
Cubital Tunnel release
 Cubital Tunnel release Information for patients Nottingham Shoulder and Elbow Unit This document can be provided in different languages and formats. For more information please contact: Physiotherapy Department
Cubital Tunnel release Information for patients Nottingham Shoulder and Elbow Unit This document can be provided in different languages and formats. For more information please contact: Physiotherapy Department
Temporomandibular Joint Treatment
 Temporomandibular Joint Treatment Preamble As stated in the AAMT Position Statement, the Code of Ethics and Standards of Practice governing massage therapy apply to treating the Temporomandibular Joint
Temporomandibular Joint Treatment Preamble As stated in the AAMT Position Statement, the Code of Ethics and Standards of Practice governing massage therapy apply to treating the Temporomandibular Joint
Your Stabilisation procedure Information for Patients
 Your Stabilisation procedure Information for Patients This leaflet will provide you with general information about the anterior stabilisation procedure. It will briefly explain the operation procedure
Your Stabilisation procedure Information for Patients This leaflet will provide you with general information about the anterior stabilisation procedure. It will briefly explain the operation procedure
Medical Care of Patients with a Joint Hypermobility Disorder
 Medical Care of Patients with a Joint Hypermobility Disorder This article is intended for medical generalists caring for patients with the commoner joint hypermobility conditions. I encourage patients
Medical Care of Patients with a Joint Hypermobility Disorder This article is intended for medical generalists caring for patients with the commoner joint hypermobility conditions. I encourage patients
EHLERS-DANLOS SYNDROME TYPE III: HYPERMOBILITY TYPE 1
 EHLERS-DANLOS SYNDROME TYPE III: HYPERMOBILITY TYPE 1 Ehlers-Danlos Syndrome Type III: Hypermobility Type Rachel Conley Bellingham Technical College Anatomy and Physiology 241 EHLERS-DANLOS SYNDROME TYPE
EHLERS-DANLOS SYNDROME TYPE III: HYPERMOBILITY TYPE 1 Ehlers-Danlos Syndrome Type III: Hypermobility Type Rachel Conley Bellingham Technical College Anatomy and Physiology 241 EHLERS-DANLOS SYNDROME TYPE