SSTIs. Dr Carlos Dobles R. San José, 29 de abril de 2017
|
|
|
- Cornelius Reed
- 5 years ago
- Views:
Transcription
1 SSTIs Dr Carlos Dobles R. San José, 29 de abril de 2017
2
3 NORMAL SKIN FLORA Propionibacterium acnes Corynebacterium sp. Staphylococci Staphylococcus epidermidis Staphylococcus aureus Streptococci sp. Candida albicans (yeast) Many others
4 TYPES The various types of SSTIs, listed according to clinical presentation and anatomic location, include the following: Impetigo Folliculitis Furuncles Carbuncles Erysipelas Cellulitis Necrotizing fasciitis Pyomyositis
5
6 Erysipela Is an acute infection of the upper dermis and superficial lymphatics, usually caused by streptococcus bacteria. Erysipelas is more superficial than cellulitis, and is typically more raised and demarcated.


7

8 Impetigo-Presentation Impetigo is characterised by blisters that rupture and coalesce to become covered with a honey-coloured crust.

9 Tinea cruris




10 Furuncles and carbuncles
11 Cellulitis Is an inflammation of the dermal and subcutaneous tissues due to non suppurative bacterial invasion. Misnomer as lesion is one of the connective tissues and interstitial tissue and not of the cells. The common causative organisms are GAS and staphylococcus.



12


13 Folliculitis

14 Impetigo

15 Herpes Zoster

16 Paronychia
17 What is Localized skin infection? Localized SSSIs include lesions such as furuncles, carbuncles, and abscesses, which would generally be treated by incision and debridement with drainage.


18 Clinical presentations of SSTIs Necrotising SSTI Surgical site infection Cellulitis Skin and soft tissue infections Diabetic foot infection Abscess Infected ulcer Infected wound ~0.1% of adult population requires hospital treatment for SSTIs each year 1 SSTIs may become complicated if require hospitalisation, surgery, involve deeper tissues, co-morbidities or systemic symptoms 1. Eron LJ, et al. J Antimicrob Chemother 2003; 52 Suppl1:i3 17.
19 When to consider it complicated? Surrounding cellulitis, immunocompromised, or the presence of potentially infectable prostheses, such as cardiac valves, orthopedic devises or vascular grafts, mandates antibiotic use and might well mean that the infection would be classed as complicated
20

21
22 Comorbidities In particular, there are a number of underlying comorbidities that should be sought and excluded as being particularly relevant to the patient with an SSSI. Diabetes Vascular insufficiency in the area of the infection Chronic renal or hepatic disease Potentially infectable prostheses Immunosuppression Debilitation or advanced age Recent antimicrobial therapy Recent surgery; and Recent hospitalization

23 Skin Abscess

24 Animal Bites

25 Animal Bites

26
27 What can you expect? superficial Gram Positives Anaerobes GN Deep
 and toxic shock syndrome toxin (TSST-1) SECOND : Group A streptococci ( GAS) (S. pyogenes), much like S.")
 and")
28 What are the three main organisms? FIRST :S. aureus Is the commonest Two potent and clinically relevant exotoxins from S. aureus are the enterotoxins (responsible for food poisoning) and toxic shock syndrome toxin (TSST-1) SECOND : Group A streptococci ( GAS) (S. pyogenes), much like S. aureus can produce a variety of virulence factors. Group A streptococci secrete an array of soluble exotoxins some of which are extremely potent causing systemic toxicity known as streptococcal toxic shock syndrome 9STSS) and necrotizing fascitis. THIRD : Clostridium perfringens is the most frequently isolated, although isolates of C. septicum, C. histolyticum, C. bifermentans, and C. novyii can be equally pathogenics.
 Genetic analysis suggests that meca has")
29 Physiology and Resistance Mechanisms of S aureus S aureus is a virulent human pathogen with the ability to elaborate a range of virulence factors and toxins; gram positive cocci in clusters Resistance to methicillin first appeared in 1961, attributed to inheritance of a meca gene found on the mobile staphylococcal cassette chromosome mec (SCCmec) Genetic analysis suggests that meca has been transferred to S aureus over 20 times, resulting in 5 major lineages MecA gene cassette leads to genetic alteration of penicillin binding protein, conferring resistance to all penicillin and cephalosporin family of antibiotics WTA=wall teichoic acid; PVL=Panton-Valentine leukocidin; CHIP=chemotaxis inhibitory protein. Zetola N et al. Lancet Infect Dis. 2005;5: Deresinski S. Clin Infect Dis. 2005;40: Foster TJ. J Clin Invest. 2004;114:

30
31 Why increasing?? Initially we thought it is pure Ping Pong effects, i e, the same hospital acquired MRSA is now living in the community. But it is clear now that this is not the complete story There is emergence of new CA-MRSA
32 Risk Factors for Community-Associated (CA) MRSA Athletes (close physical contact) Military personnel Children Native Americans HIV MSM Prisoners Young sexually active Family members (don t forget to ask!) Majority of patients have no identifiable risk factors
33 Community-Associated (CA) MRSA Increasing cause of community skin infections Genotypically and phenotypically unique from nosocomial MRSA Less resistant to non-beta-lactam agents Often susceptible to TMP-SMX, clinda, tetracyclines, +/- fluoroquinolones Panton-Valentine leukocidin (PVL) virulence factor Risk Factors Athletes, inmates, military recruits, men who have sex with men, injection drug user, prior antibiotic use Increases need to culture.
34 The emergence of VRE, VRSA and VISA 1997: VISA first reported, in United States 1 and Japan. 2 Developed spontaneously, without genetic exchange 1958: Vancomycin first licensed Mid-1980s: Use of vancomycin increases in response to surge in MRSA 2006: Nine confirmed isolates of VISA and one of VRSA in Europe 3 TODAY: VRE encountered in hospitals in most countries Reports of VISA increasing; VRSA still rare : VRE first reported, in Europe : VRSA first reported, in United States. 5 Result of transfer of VanA gene from VRE to MRSA 6 Increasing reports of S. aureus with heterointermediate resistance to vancomycin (hvisa) 1. CDC. MMWR 1997; 46: Hiramatsu K, et al. J Antimicrob Chemother 1997; 40: EARSS. EARSS annual report, Uttley AH, et al. Lancet 1988; 1: CDC. MMWR 2002; 51: CDC.
35 Percentage of isolates (van MIC = 1 µg/ml) Number of isolates MIC shift: S. aureus susceptibility to vancomycin is decreasing MRSA MSSA Year MRSA MSSA Year S. aureus isolates submitted to UCLA Clinical Microbiology Laboratory (n = 6,003) Wang G, et al. J Clin Microbiol 2006; 44:

36 What the history says? Boucher & SAkoulas CID 2007
37 IDSA GUIDELINE 2005 CID,2005, 41:
38 CLSI vancomycin breakpoints against S. aureus were lowered in 2006 to take account of MIC shift Old breakpoint (µg/ml) New breakpoint (µg/ml) VSSA 4 2 VISA VRSA Tenover FC & Moellering RC Jr. CID 2007; 44:
39 Linezolid first Oxazolidinon O Linezolid N F N O O N H O C CH 3 337,35 Dalton 1449,27 Dalton H 3 C HO + H 3 N CH 3 O HO O O HO O CH 2OH O O Cl Vancomycin Size relationship 1 : 4 O HO O NH N H O Cl H N O O N H O H N O OH O N H CH 3 NH 2 + CH 3 O HO OH OH NH 2 CH 3
40 Emergence of a New Kind of MRSA The majority of CA-MRSA infections are SSSI and adequate drainage/debridement and/or antibiotics is sufficient therapy for cure these infections. Other reports of invasive CA-MRSA infections include necrotizing pneumonia and necrotizing fascitis CA-MRSA prevalence rate was 30.2% (range %), whereas for the prospective studies 636 patients) the prevalence rate was 37.3% (range %).
41 PVL toxin: a toxin produced by MRSA The Panton-Valentine leukocidin (PVL) toxin,a potent dermatoxin, act synergistically to form pores in the cell membrane of mononuclear and polynmorphonuclear (PMN) cells. of the PVL toxin is predominately found in SCCmecA IV types, in particular the USA300 pulse field pattern.
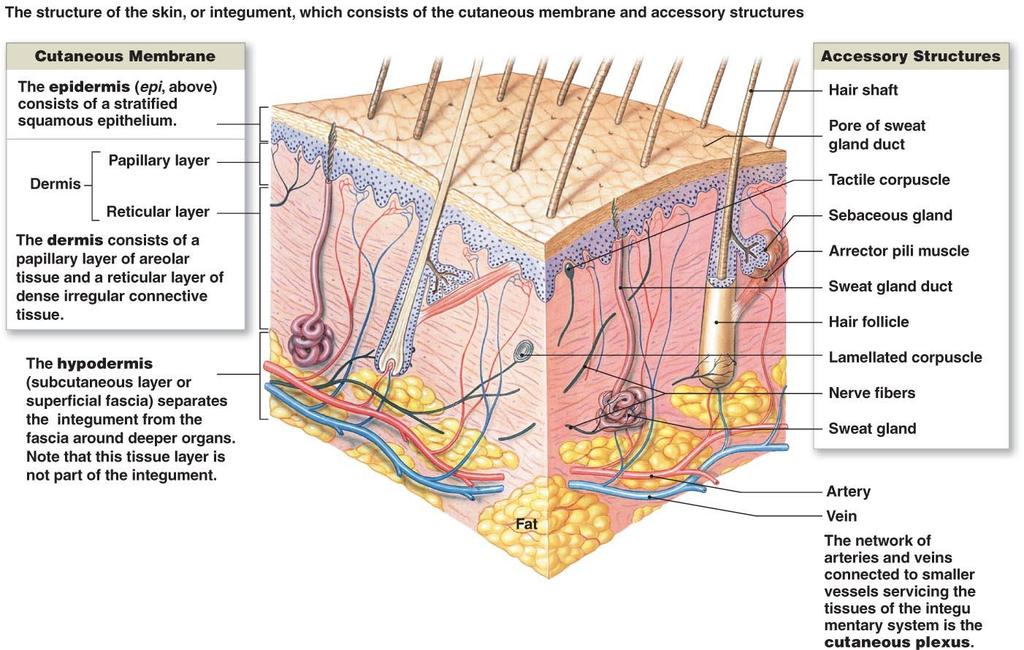
42 Skin and soft tissue infections (SSTIs) Include infections of skin, subcutaneous tissue, fascia, and muscle, encompass a wide spectrum of clinical presentations, ranging from simple cellulitis to rapidly progressive necrotizing fasciitis. Diagnosing the exact extent of the disease is critical for successful management of a patient of soft tissue infection.

43

44
45 Necrotizing Fasciitis Flesh Eating Strep Streptococcus pyogenes (Group A Strep) Tissue digesting enzymes Hyaluronidase Streptokinase Streptolysins Rapidly spreading cellulitis may lead to loss of limb
46 Skin and Soft Tissue Infections Moreover, these infections are commonly associated with the early onset of shock and organ failure. Predisposing factors include varicella, penetrating injuries, minor cuts, burns, splinters, surgical procedures, childbirth, blunt trauma, and muscle strain.
47 Complicated skin and soft tissue infection
48 Diagnosis-LRINEC The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score. It uses six serologic measures: C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose. A score greater than or eqaul to 6 indicates that necrotizing fasciitis should be seriously considered.
49 LRINEC-Criteria The scoring criteria are as follows: CRP (mg/l) 150: 4 points WBC count ( 103/mm3) <15: 0 points 15 25: 1 point >25: 2 points
50 LRINEC-Criteria cont. Hemoglobin (g/dl) >13.5: 0 points : 1 point <11: 2 points Sodium (mmol/l) <135: 2 points Creatinine (umol/l) >141: 2 points Glucose (mmol/l) >10: 1 poin
51

52

53 Infections in, Skin Subcutaneous tissue Fasciae Muscles

54
55 Staphylococcal Scalded Skin Syndrome Pathogen and virulence factors Some Staphylococcus aureus strains One or two different exfoliative toxins cause SSSS Pathogenesis No scarring because dermis is unaffected Death is rare but may be due to secondary infections Epidemiology Disease occurs primarily in infants Transmitted by person-to-person spread of bacteria

56 Desquamation
57 Toxic Shock Syndrome Group A Strep: Any invasive GAS infection (bacteremia, nec fasc, gangrenous myositis flesh eating ) complicated by case definition of TSS Exotoxin superantigens (complicated about 1/3 of invasive GAS infections) Associated bacteremia common Staph aureus toxins: Food poisoning staph enterotoxin Staph Scalded Skin exfoliative toxin CA-MRSA Panton-valentine leukocidin toxin TSS TSST-1 superantigen (interact directly with invariant region of MHC II molecule with activation of up to 20% of all T cells with massive cytokine storm) Previous association with tampons Usually MSSA but MRSA has been reported
58 Necrotizing fascitis A severe and extensive necrosis of the superficial fascia and subcutaneous fat with destruction of those tissues. Gram + and bacteria involved

59

60

61

62
63 Diagnosis of Nec. Fas. History and Physical examination of the patient!!!!! This is a simple diagnostic test that works every time. Microbiology: group A Streptococcus pyogenes, Coliforms, Staphylococcus Aureus, Bacteroides species, and rarely Clostridium septicum

64 Nec.Fasc. Leg shows extensive redness and necrosis.

65 Imaging of Nec. Fas. Radiology Plain x-ray shows gas in tissues only 30% of cases Ultrasound: not useful
66 Radiology Standard x-rays of little use. CT more sensitive. MRI and CT can delineate and determine extent of surgical resection.
67 Nec.Fasc-Symptoms pain or soreness of a muscle. The skin may be warm with red or purplish areas of swelling that spread rapidly. There may be ulcers, blisters or black spots on the skin. Fever, chills, fatigue (tiredness) or vomiting may follow the initial wound or soreness
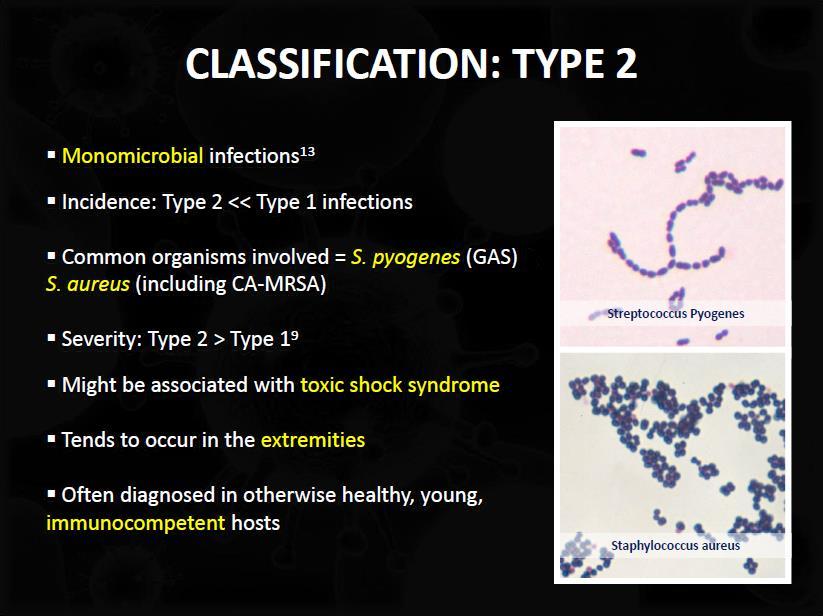
68 NECROTIZING INFECTIONS Necrotizing fasciitis, type 1 Mixed infection; anaerobes plus strep or GNR Incubation = h; progression = hrs days Marked pain, tenderness, swelling, crepitus, foul-smelling Necrotizing fasciitis, type 2 Grp A strep ( flesh-eating bacteria) Incubation = 6-48 h; progression = a few days Often with toxic shock, bullae, no crepitus Pain out of proportion to exam

69

70

71
72
73
74 Six Clinical Criteria of Nec. Fas. 1) Necrosis of the superficial fascia with undermining of the surrounding tissues 2) Systemic toxic reaction with altered mental status 3) Absence of muscle involvement 4) No Clostridia species isolated 5) No arterial inflow occlusion 6) Pathological exam of debrided tissue shows intense leukocytic infiltration, focal fascial and surrounding tissue necrosis and thrombosis of microvasculature ref: Fisher s criteria

75
76 Necrotizing Fasciitis Disease starts as localized infection Pain in area, flu-like symptoms Invasive and spreading May lead to toxic shock (drop in blood pressure) Incidence 1-20/100, % mortality Surgical removal, antibiotics

77 Necrotizing Fasciitis

78 Fasciitis
79 What are the Clinical Features of Necrotizing Fasciitis? The most common site of infection is the distal lower limb, although fascial extension up the leg is common. The progression is often alarmingly rapid from a silent or apparently minor process to a fulminant condition with clinical features of systemic toxicity, extensive destruction with threat to the affected limb, and even imminent death. The first clue may be unexplained and rapidly worsening pain By the time the bullae have appeared, there is usually already extensive necrosis.

80
81 Clinical findings in necrotising fasciitis Early findings 1. Pain 2. Cellulitis 3. Pyrexia 4. Tachycardia 5. Swelling 6. Skin anesthesia Late findings 1. Severe pain 2. Skin discoloration (purple or black) 3. Blistering 4. Hemorrhagic bullae 5. Crepitus 6. Discharge of dishwater fluid 7. Severe sepsis or systemic inflammatory response syndrome 8. Multi-organ failure
82
83 Pyomyositis Pyomyositis, also known as tropical pyomyositis or myositis tropicans, is a bacterial infection of the skeletal muscles which results in a pus-filled abscess Deep infection of muscle usually caused by S. aureus and occasionally by group A streptococci or enteric bacilli. Patients present with fever and tender swelling of the muscle;following exercise or muscle injury, the skin is usually minimally involved.

84

85 Pyomyositis S. aureus & Streptococcus infection of the skeletal muscles pus-filled abscess most common in tropical areas- myositis tropicans can affect any skeletal muscle most often infects the large muscle groups e.g.-quadriceps or gluteal muscles
86 Pyomyostis-Diagnosis Most often infects the large muscle groups. The diagnosis can be readily made, if suspected, by needle aspiration and x-rays. Within 1-2 days of injury, the involved extremity becomes painful and swollen. Gas present in tissue may be obvious by physical exam, x-ray or CT.

87 Fever, Sepsis, Localized inflammation Muscle pain Predisposing factors- Immunodeficiency, IVDAs, Trauma and malnutrition Complications- Abscess, sepsis Rx- Drain surgically and antibiotics
88 Clostridial Myonecrosis Principally C. perfringens but C. novyi and C. septicum also seen. Predisposing event Deep trauma with gross contamination Surgical wound Hematogenous spread from colonic lesion Incubation Period 2-3 days; then explosive spread.
89
90 Gas Gangrene Pathogenesis and epidemiology Traumatic event must introduce endospores into dead tissue Mortality rate exceeds 40% Diagnosis, treatment, and prevention Appearance is usually diagnostic Rapid treatment is crucial Surgical removal of dead tissue Administration of antitoxin and penicillin Prevent with proper cleaning of wounds

91 Gas Gangrene (Clostridial myonecrosis) Clostridium perfringens Extensive tissue destruction gas production by fermentative action of bacteria. Swollen reddish-black foul smelling tissue with crepitus.
")
92 Clinical Features Severe pain at the site of initial infection Tissue necrosis. spreading erythema pain soft tissue crepitus (infection tracks rapidly along the tissue planes) Fever,Tachycardia

93

94 Gas Gangrene Signs and symptoms Blackening of infected muscle and skin Presence of gas bubbles Pathogens and virulence factors Caused by several Clostridium species Bacterial endospores survive harsh conditions Vegetative cells secrete 11 toxins

95 Gas Gangrene Diagnose on signs and symptoms. Imaging- air in the tissues.

96


97 What can you expect? superficial Gram Positives Anaerobes GN Deep
98 Infectious Gangren and gangrenous cellulitis

99
100 SSTIs.. COMPLICADA LOCALIZACION De riesgo NO NO CMPLICADA SINDROME COMPARTIMENTAL presente ausente INMUNOSUPRESION presente ausente HALLAZGOS DE IMAGENES Gas y/o colecciones NO SINDROME DE SHOCK TOXICO presente ausente PROGRESION FULMINANTE SI NO SIGNOS LOCALES clásicos (tardíos) ausentes INTENSIDAD DEL DOLOR ++++/4 + o ++/4 COMPROMISO HEMODINAMICO y/o ORGANICO By Dr Dobles R-UCI HCG presente ausente
101 TREATMENT Supportive, often hemodialysis, pressors, ICU care (intractable hypotension/capillary leak) Strep: Emergent surgical debridement if soft tissue primary source ( pain out of proportion to exam ) Empiric: Clinda (900 iv q8) + imi/dori/meropenem or pip/tazo Taylored: PCN G + Clinda IVIG?immunomodulators ex TNFa inhibitors? MSSA: clinda + oxacillin/naf/cefazolin, IVIG MRSA: clinda + vancomycin, IVIG

102
103 Treatment usually surgical debridement amputation (if necessary) Antibiotics alone are not effective


104 urgent surgical exploration Extensive debridement or amputation (if necessary) Necrotizing fasciitis after debridement

105


106

107

108

109

110
111 Predisposing factors Diabetes Alcoholism Malignancy Drug abuse venous stasis lymphoedema

112

113
114

115
116 Pyomyositis-Treatment Surgical debridement and appropriate antibiotics are curative (nafcillin-oxacillin or vanco 1 gm q12h IV)
117 Treatment Debridement and excision, with amputation necessary in many cases. Antibiotics alone are not effective because they do not penetrate ischaemic muscles sufficiently to be effective.
118 Staphylococcal Scalded Skin Syndrome Diagnosis, treatment, and prevention Diagnosed by characteristic sloughing of skin Treated by administration of antimicrobial drugs Widespread presence of S. aureus makes prevention difficult 2012 Pearson Education Inc.
119 Necrotizing Skin Infections Characteristics Often perineal or lower extremity (especially for mixed infections) Abnormal inflammatory response (less purulent ) Often rapidly spreading Putrid discharge (what organisms?)/crepitance often present Associated with DM Vascular disease Trauma (bites included) Surgery
120 Skin and Soft Tissue Infections The diagnosis of necrotizing fasciitis should be suspected in a patient with a toxic appearance, bullae, crepitus or anaesthesia of the involved skin, overlying skin necrosis, and laboratory evidence of rhabdomyolysis or DIC. While these findings may be present with severe cellulitis and bacteremia, it is essential to rule out necrotizing fasciitis because rapid surgical debridement is essential.

121 INFECTIONS ASSOCIATED WITH UNDERLYING CONDTIONS Infections Post Op wound infections Lower extremity cellulitis Diabetic foot ulcers Decubitus ulcers Bite wound infections Post Trauma infections Perforated bowel Photo courtesy of T. File MD
122 Skin and Soft Tissue Infections Pyomyositis is a deep infection of muscle usually caused by S. aureus and occasionally by group A streptococci or enteric bacilli. Most cases occur in warm or tropical regions, and most among children. Patients present with fever and tender swelling of the muscle;following exercise or muscle injury, the skin is usually minimally involved.
123 Skin and Soft Tissue Infections The diagnosis of necrotizing fasciitis should be suspected in a patient with a toxic appearance, bullae, crepitus or anaesthesia of the involved skin, overlying skin necrosis, and laboratory evidence of rhabdomyolysis or DIC. While these findings may be present with severe cellulitis and bacteremia, it is essential to rule out necrotizing fasciitis because rapid surgical debridement is essential.
124 Ncrotizing Facitis is LIMB + LIFE threatening Immediate extensive surgical debridement must be done ASAP CLINDAMYCIN must be give, it also has antitoxin action

125 Who gets CA-MRSA?
126 Necrotizing Fascitis Necrotizing fascitis is a fulminating inflammation of the fascia that results in thrombosis of the subcutaneous blood vessels and necrosis of the underlying tissue Necrotizing fascitis itself is generally divided into two broad Type I, caused by mixed aerobic/anaerobic bacteria, including enterococci and non-group A streptococci (usually C or G); and Type 2, caused by group A streptococci, either alone or in combination with other organisms
127 When to consider it complicated? Surrounding cellulitis, immunocompromised, or the presence of potentially infectable prostheses, such as cardiac valves, orthopedic devises or vascular grafts, mandates antibiotic use and might well mean that the infection would be classed as complicated

128 Anatomy of the skin



129 csssi Definition Abscess Cellulitis Ulcer Skin/skin structure infections that: Involve deep, soft tissue Require surgical intervention Are associated with significant underlying disease that complicate the response to treatment 36
130 In particular, there are a number of underlying comorbidities that should be sought and excluded as being particularly relevant to the patient with an SSSI. Diabetes Vascular insufficiency in the area of the infection Chronic renal or hepatic disease Potentially infectable prostheses Immunosuppression Debilitation or advanced age Recent antimicrobial therapy Recent surgery; and Recent hospitalization

131 Clostridial Myonecrosis Presentation Severe pain out of proportion to clinical findings Erythema and cutaneous blisters Gangrene Crepitus Brown foul smelling discharge Loss of motor function
132
General surgery department of SGMU Lecturer ass. Khilgiyaev R.H. Anaerobic infection. Gas gangrene
 Anaerobic infection Gas gangrene Anaerobic bacteria Anaerobic bacteria are the most numerous inhabitants of the normal gastrointestinal tract, including the mouth Bacteroides fragilis and Clostridium The
Anaerobic infection Gas gangrene Anaerobic bacteria Anaerobic bacteria are the most numerous inhabitants of the normal gastrointestinal tract, including the mouth Bacteroides fragilis and Clostridium The
Objectives. Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection
 that drive empiric antimicrobial selection") Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
Cellulitis and Soft Tissue Infections. Sally Williams MD
 Cellulitis and Soft Tissue Infections Sally Williams MD Cellulitis: A very common infection 25 cases per 1000 patient years More common in men, obese patients 60% occurs in the lower extremities 74% handled
Cellulitis and Soft Tissue Infections Sally Williams MD Cellulitis: A very common infection 25 cases per 1000 patient years More common in men, obese patients 60% occurs in the lower extremities 74% handled
Morbidity & Mortality Conference Downstate Medical Center. Daniel Kaufman, MD
 Morbidity & Mortality Conference Downstate Medical Center University Case Presentation Hospital of Brooklyn Daniel Kaufman, MD Necrotizing Fasciitis and Soft- Tissue Infections Necrotizing Fasciitis Deep
Morbidity & Mortality Conference Downstate Medical Center University Case Presentation Hospital of Brooklyn Daniel Kaufman, MD Necrotizing Fasciitis and Soft- Tissue Infections Necrotizing Fasciitis Deep
-> Education -> Excellence
 Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Staphylococci. What s to be Covered. Clinical Scenario #1
 Staphylococci Micrococcus, which, when limited in its extent and activity, causes acute suppurative inflammation (phlegmon), produces, when more extensive and intense in its action on the human system,
Staphylococci Micrococcus, which, when limited in its extent and activity, causes acute suppurative inflammation (phlegmon), produces, when more extensive and intense in its action on the human system,
Podcast (Video Recorded Lecture Series): Soft Tissue Infections for the USMLE Step One Exam
: Soft Tissue Infections for the USMLE Step One Exam") Podcast (Video Recorded Lecture Series): Soft Tissue Infections for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com MSK Infections Bone and Joint Infections
Podcast (Video Recorded Lecture Series): Soft Tissue Infections for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com MSK Infections Bone and Joint Infections
Necrotizing Fasciitis. By Lisa Banks
 Necrotizing Fasciitis By Lisa Banks Foot infections are the most common softtissue infections in pts with diabetes Necrotizing fasciitis is the most important soft tissue infection in DM pts involving
Necrotizing Fasciitis By Lisa Banks Foot infections are the most common softtissue infections in pts with diabetes Necrotizing fasciitis is the most important soft tissue infection in DM pts involving
What s to be Covered. Microbiology of staphylococci Epidemiology of S. aureus infections Pathogenesis of S. aureus infections
 Staphylococci Micrococcus, which, when limited in its extent and activity, causes acute suppurative inflammation (phlegmon), produces, when more extensive and intense in its action on the human system,
Staphylococci Micrococcus, which, when limited in its extent and activity, causes acute suppurative inflammation (phlegmon), produces, when more extensive and intense in its action on the human system,
Clinical Case. ! 2am: Call from Surgeon, Ballarat Hospital. ! Suspicion of Necrotizing Fasciitis: ! Need of HBOT?
 Clinical Case! 2am: Call from Surgeon, Ballarat Hospital! Suspicion of Necrotizing Fasciitis:! 59y, Police Officer, diabetic, overweight! 4pm: pain in right arm! 8pm: pain worsening " ED! HD instability
Clinical Case! 2am: Call from Surgeon, Ballarat Hospital! Suspicion of Necrotizing Fasciitis:! 59y, Police Officer, diabetic, overweight! 4pm: pain in right arm! 8pm: pain worsening " ED! HD instability
Skin and Soft Tissue Infections. Masoud Mardani MD, MPH,FIDSA Prof of Infectious Dis Shahid Beheshti Medical University
 Skin and Soft Tissue Infections Masoud Mardani MD, MPH,FIDSA Prof of Infectious Dis Shahid Beheshti Medical University Usual Skin Flora Skin flora consists of those microbes able to adapt to the high salt
Skin and Soft Tissue Infections Masoud Mardani MD, MPH,FIDSA Prof of Infectious Dis Shahid Beheshti Medical University Usual Skin Flora Skin flora consists of those microbes able to adapt to the high salt
A WEATHER FORECAST. It is gonna be cold It is gonna be gray It is gonna last for the rest of your life Groundhog day Bill Murray
 A WEATHER FORECAST It is gonna be cold It is gonna be gray It is gonna last for the rest of your life Groundhog day Bill Murray GOETHE Art is long, Life short, Judgment difficult, Opportunity transient
A WEATHER FORECAST It is gonna be cold It is gonna be gray It is gonna last for the rest of your life Groundhog day Bill Murray GOETHE Art is long, Life short, Judgment difficult, Opportunity transient
Abscess. A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body.
 Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
Cellulitis: a practical guide
 Cellulitis: a practical guide Dr John Day Consultant in Infectious Diseases & General Medicine Southend University Hospital NHS Foundation Trust 77 yr old retired civil servant A&E presentation c/o rigors
Cellulitis: a practical guide Dr John Day Consultant in Infectious Diseases & General Medicine Southend University Hospital NHS Foundation Trust 77 yr old retired civil servant A&E presentation c/o rigors
Pimples and Boils!! Dr Nathan Harvey Anatomical Pathology, PathWest
 Pimples and Boils!! Dr Nathan Harvey Anatomical Pathology, PathWest Overview & Learning Objectives Review the cardinal signs/symptoms of acute inflammation Review the histological features of acute inflammation
Pimples and Boils!! Dr Nathan Harvey Anatomical Pathology, PathWest Overview & Learning Objectives Review the cardinal signs/symptoms of acute inflammation Review the histological features of acute inflammation
Complicated Skin and Soft Tissue Infection diagnosis and severity stratification
 Complicated Skin and Soft Tissue Infection diagnosis and severity stratification Muhammad Hussein Gasem Div Infectious Disease, TropMed, and Immunology Dr. Kariadi Hospital, Diponegoro University Semarang,
Complicated Skin and Soft Tissue Infection diagnosis and severity stratification Muhammad Hussein Gasem Div Infectious Disease, TropMed, and Immunology Dr. Kariadi Hospital, Diponegoro University Semarang,
Gram Positive Coccus Staphylococci Dr. Hala Al Daghistani
 Medical bacteriology Gram Positive Coccus Staphylococci Dr. Hala Al Daghistani The Staphylococci are gram-positive spherical cells, nonmotile, usually arranged in grapelike irregular clusters. Some are
Medical bacteriology Gram Positive Coccus Staphylococci Dr. Hala Al Daghistani The Staphylococci are gram-positive spherical cells, nonmotile, usually arranged in grapelike irregular clusters. Some are
Skin and soft tissue (SSTI) sepsis (surgery, antimicrobial therapy and more)
 sepsis (surgery, antimicrobial therapy and more)") Skin and soft tissue (SSTI) sepsis (surgery, antimicrobial therapy and more) Christian Eckmann Antibiotic Stewardship Expert ECDC Chief of Staff Department of General, Visceral and Thoracic Surgery Klinikum
Skin and soft tissue (SSTI) sepsis (surgery, antimicrobial therapy and more) Christian Eckmann Antibiotic Stewardship Expert ECDC Chief of Staff Department of General, Visceral and Thoracic Surgery Klinikum
Disclosure. Patient Case. Objectives. Patient Case. Patient Case 7/25/2015. An update on the treatment of skin and soft tissue infections
 Disclosure 49th Annual Meeting An update on the treatment of skin and soft tissue infections I do not have a vested interest in or affiliation with any corporate organization offering financial support
Disclosure 49th Annual Meeting An update on the treatment of skin and soft tissue infections I do not have a vested interest in or affiliation with any corporate organization offering financial support
5/1/2010. Jan K Horn, MD, FACS San Francisco General Hospital University of California, San Francisco
 Necrotizing Soft Tissue Infections Jan K Horn, MD, FACS San Francisco General Hospital University of California, San Francisco Soft Tissue Infections Anatomical Layer Infection Epidermis Abscess Dermis
Necrotizing Soft Tissue Infections Jan K Horn, MD, FACS San Francisco General Hospital University of California, San Francisco Soft Tissue Infections Anatomical Layer Infection Epidermis Abscess Dermis
Case 2. Case 3 - course. PE: uncomfortable, but NAD T 38.0 R 22 HR 120 BP130/60
 Case 2 42 y/o man c/o painful right arm and shoulder x 3 days. Hx of IDU ( skin popping heroin ). No other trauma or bite. PE: uncomfortable, but NAD T 38.0 R 22 HR 120 BP130/60 PMH: HCV, HBV, HIV negative,
Case 2 42 y/o man c/o painful right arm and shoulder x 3 days. Hx of IDU ( skin popping heroin ). No other trauma or bite. PE: uncomfortable, but NAD T 38.0 R 22 HR 120 BP130/60 PMH: HCV, HBV, HIV negative,
number Done by Corrected by Doctor Hamed Al-Zoubi
 number 9 Done by Mohammed Al askar & Muhammed Alajmi Corrected by مها أبو عجمية Doctor Hamed Al-Zoubi 1 Gram positive cocci There are 3 types of gram positive cocci :- 1- Staphylococcus ( what we are going
number 9 Done by Mohammed Al askar & Muhammed Alajmi Corrected by مها أبو عجمية Doctor Hamed Al-Zoubi 1 Gram positive cocci There are 3 types of gram positive cocci :- 1- Staphylococcus ( what we are going
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH)
") Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Chapter 19. Pathogenic Gram-Positive Bacteria. Staphylococcus & Streptococcus
 Chapter 19 Pathogenic Gram-Positive Bacteria Staphylococcus & Streptococcus Staphylococcus Normal members of every human's microbiota Can be opportunistic pathogens Facultative anaerobes Cells occur in
Chapter 19 Pathogenic Gram-Positive Bacteria Staphylococcus & Streptococcus Staphylococcus Normal members of every human's microbiota Can be opportunistic pathogens Facultative anaerobes Cells occur in
PYOGENIC INFECTIONS. Dr. Kenéz Éva - Anna Division of Infectious Diseases
 PYOGENIC INFECTIONS Dr. Kenéz Éva - Anna Division of Infectious Diseases 2015.11.10 KEY POINTS The virulence factors of streptococcus and staphylococcus Disease caused by streptococcus and staphylococcus
PYOGENIC INFECTIONS Dr. Kenéz Éva - Anna Division of Infectious Diseases 2015.11.10 KEY POINTS The virulence factors of streptococcus and staphylococcus Disease caused by streptococcus and staphylococcus
In the absence of underlying edema or other skin abnormalities, erysipelas
 ERYSIPELAS Erysipelas is a distinct type of superficial cutaneous cellulitis with marked dermal lymphatic vessel involvement caused by group A β-hemolytic streptococcus (very uncommonly group C or G streptococcus)
ERYSIPELAS Erysipelas is a distinct type of superficial cutaneous cellulitis with marked dermal lymphatic vessel involvement caused by group A β-hemolytic streptococcus (very uncommonly group C or G streptococcus)
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
Skin and Soft Tissue Infections (SSTI): More than a skin deep review. Vicky Parente, MD Sea Pines Conference July 12th, 2018
: More than a skin deep review. Vicky Parente, MD Sea Pines Conference July 12th, 2018") Skin and Soft Tissue Infections (SSTI): More than a skin deep review Vicky Parente, MD Sea Pines Conference July 12th, 2018 Objectives To review the anatomy and classification of SSTIs To understand the
Skin and Soft Tissue Infections (SSTI): More than a skin deep review Vicky Parente, MD Sea Pines Conference July 12th, 2018 Objectives To review the anatomy and classification of SSTIs To understand the
The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA
 The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA Franklin D. Lowy, MD Columbia University College of Physicians & Surgeons New York, NY Topics to Be Covered Background Some
The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA Franklin D. Lowy, MD Columbia University College of Physicians & Surgeons New York, NY Topics to Be Covered Background Some
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
SKIN AND SOFT TISSUE INFECTIONS
 SKIN AND SOFT TISSUE INFECTIONS ZAIN CHAGLA SEA COURSES - PATAGONIA COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in
SKIN AND SOFT TISSUE INFECTIONS ZAIN CHAGLA SEA COURSES - PATAGONIA COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in
Skin and so* +ssue infec+on. N.Nuntachit MD.
 Skin and so* +ssue infec+on N.Nuntachit MD. Non purulent SSTI Impe+go, ecthyma Celluli+s, Erysipelas Erysipeloid Necro+zing infec+on Etc eg Glanders, bubonic plaque Purulent SSTI Furuncle Carbuncle Abscess
Skin and so* +ssue infec+on N.Nuntachit MD. Non purulent SSTI Impe+go, ecthyma Celluli+s, Erysipelas Erysipeloid Necro+zing infec+on Etc eg Glanders, bubonic plaque Purulent SSTI Furuncle Carbuncle Abscess
Skin and soft tissue infections Introduction/overview
 Skin and soft tissue infections Introduction/overview M Al Madadha Sources : Harrisons infectious diseases 2 nd edition, Oxford Handbook of Infectious Diseases and Microbiology 2 nd edition Anatomic relationships:
Skin and soft tissue infections Introduction/overview M Al Madadha Sources : Harrisons infectious diseases 2 nd edition, Oxford Handbook of Infectious Diseases and Microbiology 2 nd edition Anatomic relationships:
MRSA: A TEAM APPROACH
 Eric Bosley, MD Laura Stadler, MD John MD J h Draus, D MRSA: A TEAM APPROACH PART I: OUTPATIENT ISSUES AND MANAGEMENT NOT REQUIRING I&D OR HOSPITALIZATION Eric L. Bosley, MD, FAAP Pediatric Associates,
Eric Bosley, MD Laura Stadler, MD John MD J h Draus, D MRSA: A TEAM APPROACH PART I: OUTPATIENT ISSUES AND MANAGEMENT NOT REQUIRING I&D OR HOSPITALIZATION Eric L. Bosley, MD, FAAP Pediatric Associates,
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Streptococcus pyogenes
 Streptococcus pyogenes From Wikipedia, the free encyclopedia Streptococcus pyogenes S. pyogenes bacteria at 900x magnification. Scientific classification Kingdom: Eubacteria Phylum: Firmicutes Class: Cocci
Streptococcus pyogenes From Wikipedia, the free encyclopedia Streptococcus pyogenes S. pyogenes bacteria at 900x magnification. Scientific classification Kingdom: Eubacteria Phylum: Firmicutes Class: Cocci
Abscess cellulitis pus
 Abscess cellulitis pus An abscess is a collection of pus that has built up within the tissue of the body.. If the condition is thought to be cellulitis rather than abscess,. 13-2-2018 Patients with skin
Abscess cellulitis pus An abscess is a collection of pus that has built up within the tissue of the body.. If the condition is thought to be cellulitis rather than abscess,. 13-2-2018 Patients with skin
13/10. Microbiology Bacterial Skin Infections Dr Hani Masaadeh Areej al-arqan
 13/10 Microbiology Bacterial Skin Infections Dr Hani Masaadeh Areej al-arqan Salam soul, this is the first Microbiology lecture of this system given by Dr.hani masaadeh. I ll do my best to make it easy
13/10 Microbiology Bacterial Skin Infections Dr Hani Masaadeh Areej al-arqan Salam soul, this is the first Microbiology lecture of this system given by Dr.hani masaadeh. I ll do my best to make it easy
Skin & Soft Tissue Infections: Classic Case Presentations
 Skin & Soft Tissue Infections: Classic Case Presentations Mark Beilke, M.D. Professor of Medicine Chief of Infectious Diseases Clement J. Zablocki VA Medical Center Objectives Diagnose and treat water
Skin & Soft Tissue Infections: Classic Case Presentations Mark Beilke, M.D. Professor of Medicine Chief of Infectious Diseases Clement J. Zablocki VA Medical Center Objectives Diagnose and treat water
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
Streptococcus(gram positive coccus) Dr. Hala Al Daghistani
 Dr. Hala Al Daghistani") Streptococcus(gram positive coccus) Dr. Hala Al Daghistani Streptococci Facultative anaerobe Gram-positive usually chains (sometimes pairs) Catalase negative Non motile Hemolysins Lancefield Groups (C-carbohydrate
Streptococcus(gram positive coccus) Dr. Hala Al Daghistani Streptococci Facultative anaerobe Gram-positive usually chains (sometimes pairs) Catalase negative Non motile Hemolysins Lancefield Groups (C-carbohydrate
(NATO STANAG 2122, CENTO STANAG 2122, SEATO STANAG 2122)
") (NATO STANAG 2122, CENTO STANAG 2122, SEATO STANAG 2122) Bacteria Bacteria are microscopic, single-celled forms of plant life, containing no chlorophyll. They live on the skin, on the surface of the stratum
(NATO STANAG 2122, CENTO STANAG 2122, SEATO STANAG 2122) Bacteria Bacteria are microscopic, single-celled forms of plant life, containing no chlorophyll. They live on the skin, on the surface of the stratum
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates
 Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates Xuzhuang Shen Beijing Children's Hospital, Capital Medical University,
Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates Xuzhuang Shen Beijing Children's Hospital, Capital Medical University,
Medical Microbiology
 Lecture 5!!!!!!ƒš!!Œ!!! š!!œ!! Œ!!!! Dr. Ismail I. Daood Medical Microbiology!! Systematic Bacteriology Gram-Positive Cocci : GENUS : Staphylococcus : The general properties of Staphylococcus are Gram-
Lecture 5!!!!!!ƒš!!Œ!!! š!!œ!! Œ!!!! Dr. Ismail I. Daood Medical Microbiology!! Systematic Bacteriology Gram-Positive Cocci : GENUS : Staphylococcus : The general properties of Staphylococcus are Gram-
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
4. The most common cause of traveller s diarrheoa is a. Rotavirus b. E coli c. Shigella d. Giardia e. Salmonella
 INFECTIOUS DISEASE 1. Mumps virus is a a. Adenovirus b. Herpes virus c. Paramyxovirus d. Pox virus e. Picornavirus 2. All of the following cause a clinical effect via the production of exotoxin except
INFECTIOUS DISEASE 1. Mumps virus is a a. Adenovirus b. Herpes virus c. Paramyxovirus d. Pox virus e. Picornavirus 2. All of the following cause a clinical effect via the production of exotoxin except
CLINICAL USE OF GLYCOPEPTIDES. Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel
 CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
World Society of Emergency Surgery (WSES) guidelines for management of skin and soft tissue infections
 guidelines for management of skin and soft tissue infections") Sartelli et al. World Journal of Emergency Surgery 2014, 9:57 WORLD JOURNAL OF EMERGENCY SURGERY REVIEW World Society of Emergency Surgery (WSES) guidelines for management of skin and soft tissue infections
Sartelli et al. World Journal of Emergency Surgery 2014, 9:57 WORLD JOURNAL OF EMERGENCY SURGERY REVIEW World Society of Emergency Surgery (WSES) guidelines for management of skin and soft tissue infections
Staphylococcal Food Poisoning
 Staphylococcal Food Poisoning Pyogenic Cocci Staphylococcus gram-positive Streptococcus gram-positive Neisseria gram-negative Stapylococcus and related organisms S. aureus: major pathogen for humans, may
Staphylococcal Food Poisoning Pyogenic Cocci Staphylococcus gram-positive Streptococcus gram-positive Neisseria gram-negative Stapylococcus and related organisms S. aureus: major pathogen for humans, may
Pressure Injury Complications: Diagnostic Dilemmas
 Pressure Injury Complications: Diagnostic Dilemmas Aimée D. Garcia, MD, CWS, FACCWS Associate Professor, Department of Medicine, Geriatrics Section Baylor College of Medicine Medical Director, Wound Clinic
Pressure Injury Complications: Diagnostic Dilemmas Aimée D. Garcia, MD, CWS, FACCWS Associate Professor, Department of Medicine, Geriatrics Section Baylor College of Medicine Medical Director, Wound Clinic
ESCMID Online Lecture Library. by author
 Hospital Universitario Virgen Macarena, Seville New drugs against MRSA and VRE L. Eduardo López Cortés Seville, 8th July Tedizolid Oxazolidinone Ceftaroline // Ceftobiprole 5 th gen cephalosporin Overview
Hospital Universitario Virgen Macarena, Seville New drugs against MRSA and VRE L. Eduardo López Cortés Seville, 8th July Tedizolid Oxazolidinone Ceftaroline // Ceftobiprole 5 th gen cephalosporin Overview
Necrotizing Fasciitis. Madhuri Rao, MD June 27 th, 2013 Case from Kings County Hospital Center
 Necrotizing Fasciitis Madhuri Rao, MD June 27 th, 2013 Case from Kings County Hospital Center 31 yo F www.downstatesurgery.org Case Presentation PMH: DM (type 1), CRI, verrucous elephantiasis of LE PSH:
Necrotizing Fasciitis Madhuri Rao, MD June 27 th, 2013 Case from Kings County Hospital Center 31 yo F www.downstatesurgery.org Case Presentation PMH: DM (type 1), CRI, verrucous elephantiasis of LE PSH:
Review on Skin and Soft Tissue Infection
 Preface Review on Skin and Soft Tissue Infection Professor Tzong-Luen Wang MD, PhD, JM, FESC, FACC, FCAPSC Chief, ED, Shin-Kong Wu Ho-Su Memorial Hospital Professor, Medical School, Fu-Jen Catholic University
Preface Review on Skin and Soft Tissue Infection Professor Tzong-Luen Wang MD, PhD, JM, FESC, FACC, FCAPSC Chief, ED, Shin-Kong Wu Ho-Su Memorial Hospital Professor, Medical School, Fu-Jen Catholic University
DEFINITION Cellulitis is an acute, spreading inflammation of the dermis and subcutaneous tissue, often complicating a wound or other skin condition.
 DEFINITION Cellulitis is an acute, spreading inflammation of the dermis and subcutaneous tissue, often complicating a wound or other skin condition. Cellulitis may be further classified by the unique area
DEFINITION Cellulitis is an acute, spreading inflammation of the dermis and subcutaneous tissue, often complicating a wound or other skin condition. Cellulitis may be further classified by the unique area
Omar Sami. M.Madadha. 1 P a g e
 4 Omar Sami M.Madadha 1 P a g e Studying microbiology might not seem so appealing to many of us; yet no one denies how important it is. However, microbiology is one of the, if not the most medical sharpening
4 Omar Sami M.Madadha 1 P a g e Studying microbiology might not seem so appealing to many of us; yet no one denies how important it is. However, microbiology is one of the, if not the most medical sharpening
Objectives, Upon completion of this lecture, the student will:
 Lec.2 Dr.Sarmad Zeiny 2013-2014 BCM Genus Streptococci Objectives, Upon completion of this lecture, the student will: Outline the medically important streptococci species. Classification of genus streptococci.
Lec.2 Dr.Sarmad Zeiny 2013-2014 BCM Genus Streptococci Objectives, Upon completion of this lecture, the student will: Outline the medically important streptococci species. Classification of genus streptococci.
Medical Bacteriology- Lecture: 6
 Medical Bacteriology- Lecture: 6 Gram Positive Cocci Streptococcal Disease Streptococcus pyogenes Classification of Streptococci based on (1- Hemolysis reactions on blood agar) (Brown in 1903) The type
Medical Bacteriology- Lecture: 6 Gram Positive Cocci Streptococcal Disease Streptococcus pyogenes Classification of Streptococci based on (1- Hemolysis reactions on blood agar) (Brown in 1903) The type
GROUP A STREPTOCOCCUS (GAS) INVASIVE
 INVASIVE") GROUP A STREPTOCOCCUS (GAS) INVASIVE Case definition CONFIRMED CASE Laboratory confirmation of infection with or without clinical evidence of invasive disease: isolation of group A streptococcus (Streptococcus
GROUP A STREPTOCOCCUS (GAS) INVASIVE Case definition CONFIRMED CASE Laboratory confirmation of infection with or without clinical evidence of invasive disease: isolation of group A streptococcus (Streptococcus
Bacteriemia and sepsis
 Bacteriemia and sepsis Case 1 An 80-year-old man is brought to the emergency room by his son, who noted that his father had become lethargic and has decreased urination over the past 4 days. The patient
Bacteriemia and sepsis Case 1 An 80-year-old man is brought to the emergency room by his son, who noted that his father had become lethargic and has decreased urination over the past 4 days. The patient
Infections Amenable to OPAT. (Nabin Shrestha + Ajay Mathur)
") 3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
Staphylococcus aureus Staphylococcus epidermidis Staphylococcus hominis Staphylococcus haemolyticus Staphylococcus saprophyticus others
 THE GENUS STAPHYLOCOCCUS The genus Staphylococcus contains about 50 species and subspecies today Only some of them are important as human pathogens: Staphylococcus aureus Staphylococcus epidermidis Staphylococcus
THE GENUS STAPHYLOCOCCUS The genus Staphylococcus contains about 50 species and subspecies today Only some of them are important as human pathogens: Staphylococcus aureus Staphylococcus epidermidis Staphylococcus
Common bacterial skin infections
 Common bacterial skin infections Cellulitis A localized area of soft tissue inflammation with skin infiltration with white cells, capillary dilatation and proliferation of bacteria. Staph aureus and Strep
Common bacterial skin infections Cellulitis A localized area of soft tissue inflammation with skin infiltration with white cells, capillary dilatation and proliferation of bacteria. Staph aureus and Strep
ESPID New Bone and Joint Infection Guidelines
 ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
NIH Public Access Author Manuscript J Diabetes Metab. Author manuscript; available in PMC 2014 July 07.
 NIH Public Access Author Manuscript Published in final edited form as: J Diabetes Metab. 2013 November 1; 4(9): 310. doi:10.4172/2155-6156.1000310. Foreign Body with Gas Gangrene in an Elderly Patient
NIH Public Access Author Manuscript Published in final edited form as: J Diabetes Metab. 2013 November 1; 4(9): 310. doi:10.4172/2155-6156.1000310. Foreign Body with Gas Gangrene in an Elderly Patient
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida
 Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Infective endocarditis
 Infective endocarditis Today's lecture is about infective endocarditis, the Dr started the lecture by asking what are the most common causative agents of infective endocarditis? 1-Group A streptococci
Infective endocarditis Today's lecture is about infective endocarditis, the Dr started the lecture by asking what are the most common causative agents of infective endocarditis? 1-Group A streptococci
COMMON SKIN INFECTIONS. Sports Medicine
 COMMON SKIN INFECTIONS Sports Medicine IMPETIGO IS A SUPERFICIAL BACTERIAL INFECTION CAUSED BY: STREPTOCOCCI OR STAPHYLOCOCCUS AUREUS BOULOUS IMPETIGO IMPETIGO COMES IN TWO FORMS: BOULOUS OR NON- BOULOUS
COMMON SKIN INFECTIONS Sports Medicine IMPETIGO IS A SUPERFICIAL BACTERIAL INFECTION CAUSED BY: STREPTOCOCCI OR STAPHYLOCOCCUS AUREUS BOULOUS IMPETIGO IMPETIGO COMES IN TWO FORMS: BOULOUS OR NON- BOULOUS
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
2.3 Invasive Group A Streptococcal Disease
 2.3 Invasive Group A Streptococcal Disease Summary Total number of cases, 2015 = 107 Crude incidence rate, 2015 = 2.3 per 100,000 population Notifications In 2015, 107 cases of invasive group A streptococcal
2.3 Invasive Group A Streptococcal Disease Summary Total number of cases, 2015 = 107 Crude incidence rate, 2015 = 2.3 per 100,000 population Notifications In 2015, 107 cases of invasive group A streptococcal
Pediatric Infections: Treatment of Resistant Pathogens. Focus : MRSA and DRSP Infections, Including Pneumonia. Blaise L. Congeni M.D.
 Pediatric Infections: Treatment of Resistant Pathogens Focus : MRSA and DRSP Infections, Including Pneumonia Blaise L. Congeni M.D. Patient 1-LP 8 yo with 8 days of fever and 6 days of cough. She had consistently
Pediatric Infections: Treatment of Resistant Pathogens Focus : MRSA and DRSP Infections, Including Pneumonia Blaise L. Congeni M.D. Patient 1-LP 8 yo with 8 days of fever and 6 days of cough. She had consistently
Staph Infections. including MRSA
 Staph Infections including MRSA What is a Staph infection? STAPH Staphylococcus aureus, often referred to simply as staph, are bacteria commonly carried on the skin or in the nose of healthy people. SYMPTOMS
Staph Infections including MRSA What is a Staph infection? STAPH Staphylococcus aureus, often referred to simply as staph, are bacteria commonly carried on the skin or in the nose of healthy people. SYMPTOMS
Shapes and Genera of cocci-shaped organisms:
 BIO230 Microbiology 19: Pathogenic Gram-Positive Cocci and Bacilli 1. Gram-positive pathogens Color reaction Shapes and Genera of cocci-shaped organisms: Genera of bacilli-shaped organisms: 2. Staphylococcus
BIO230 Microbiology 19: Pathogenic Gram-Positive Cocci and Bacilli 1. Gram-positive pathogens Color reaction Shapes and Genera of cocci-shaped organisms: Genera of bacilli-shaped organisms: 2. Staphylococcus
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Here is the first Microbiology lecture in this system given by our lovely Dr Hani Masaadeh.
 Here is the first Microbiology lecture in this system given by our lovely Dr Hani Masaadeh. This sheet is complete slides + Dr Comments, so you don t need to go back to the slides. Here is some dermatological
Here is the first Microbiology lecture in this system given by our lovely Dr Hani Masaadeh. This sheet is complete slides + Dr Comments, so you don t need to go back to the slides. Here is some dermatological
Medical Bacteriology- Lecture: 5. Bacterial Pathogens and Diseases of Humans
 Medical Bacteriology Lecture: 5 Bacterial Pathogens and Diseases of Humans Gram Positive Cocci Staphylococci Micrococcaceae Staphylococcus: Pathogenic or commensal Micrococcus: Freeliving saprophytes Staphylococci
Medical Bacteriology Lecture: 5 Bacterial Pathogens and Diseases of Humans Gram Positive Cocci Staphylococci Micrococcaceae Staphylococcus: Pathogenic or commensal Micrococcus: Freeliving saprophytes Staphylococci
Rapid and progressive necrosis of the tissue underlying epidermis (cellulitis)
") Table 1. Infections of the Skin, Eyes and Ears Folliculitis Furuncles (boils) & Carbuncles Staphylococcus aureus (G+) Scald Skin Syndrome Peeling skin on infants Staphylococcus aureus (G+) Impetigo Lesions
Table 1. Infections of the Skin, Eyes and Ears Folliculitis Furuncles (boils) & Carbuncles Staphylococcus aureus (G+) Scald Skin Syndrome Peeling skin on infants Staphylococcus aureus (G+) Impetigo Lesions
Streptococci and Other Streptococci-like Organisms. By:Dr. Aghaei
 Streptococci and Other Streptococci-like Organisms By:Dr. Aghaei Case Study 9-year-old boy complains of fever and sore throat On examination, his pharynx is red and his tonsils are swollen His cervical
Streptococci and Other Streptococci-like Organisms By:Dr. Aghaei Case Study 9-year-old boy complains of fever and sore throat On examination, his pharynx is red and his tonsils are swollen His cervical
Midwifery Management Process for Common Health Problems
 StudentL 1 Lower Limb Cellulitis University of Washington School of Nursing Nurse- Midwifery Education Program NCLIN 512 Fall 2012 Midwifery Management Process for Common Health Problems 1. Common Health
StudentL 1 Lower Limb Cellulitis University of Washington School of Nursing Nurse- Midwifery Education Program NCLIN 512 Fall 2012 Midwifery Management Process for Common Health Problems 1. Common Health
Osteomyelitis and Septic Joints; Practical Considerations. Coleen K. Cunningham
 Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Staphylococci and streptococci
 Staphylococci and streptococci Prof. Marianna Murdjeva, MD, PhD Dept. Microbiology and Immunology Medical University Plovdiv Lecture course in microbiology for English-speaking medical students Staphylococci
Staphylococci and streptococci Prof. Marianna Murdjeva, MD, PhD Dept. Microbiology and Immunology Medical University Plovdiv Lecture course in microbiology for English-speaking medical students Staphylococci
Treatment of infection
 Clinica Ortopedica e Traumatologica Università degli Studi di Pavia Fondazione IRCCS Policlinico San Matteo Chairman: Prof. F. Benazzo Goals: - Healing of infection - Healing of fracture - Try to keep
Clinica Ortopedica e Traumatologica Università degli Studi di Pavia Fondazione IRCCS Policlinico San Matteo Chairman: Prof. F. Benazzo Goals: - Healing of infection - Healing of fracture - Try to keep
a Total Hip Prosthesis by Clostridum perfringens. A Case Report
 Haematogenous Infection of a Total Hip Prosthesis by Clostridum perfringens. A Case Report CHAPTER 5 CHAPTER 5 5.1. Introduction In orthopaedic surgery, an infection of a prosthesis is a very serious,
Haematogenous Infection of a Total Hip Prosthesis by Clostridum perfringens. A Case Report CHAPTER 5 CHAPTER 5 5.1. Introduction In orthopaedic surgery, an infection of a prosthesis is a very serious,
Staph Infection Fact Sheet
 What is Staphylococcus aureus (staph)? Staphylococcus aureus, often referred to simply as staph, are bacteria commonly carried on the skin or in the nose of healthy people. Approximately 25% to 30% of
What is Staphylococcus aureus (staph)? Staphylococcus aureus, often referred to simply as staph, are bacteria commonly carried on the skin or in the nose of healthy people. Approximately 25% to 30% of
Yonekura, Akihiko; Tomita, Masato;
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation Fournier's gangrene a case report Miyamoto, Takashi; Fukushima, Tatsu Yonekura, Akihiko; Tomita, Masato; Acta medica Nagasakiensia, 61(1), p Issue
NAOSITE: Nagasaki University's Ac Title Author(s) Citation Fournier's gangrene a case report Miyamoto, Takashi; Fukushima, Tatsu Yonekura, Akihiko; Tomita, Masato; Acta medica Nagasakiensia, 61(1), p Issue
The Journal of the Korean Society of Fractures Vol.15, No.4, October, 2002
 The Journal of the Korean Society of Fractures Vol15, No4, October, 2002 : 134 TEL : 02-361-5640 FAX : 02-363-1139 E-mail : sbhahn@yumcyonseiackr 608 21 ), c l o s t r i d i u m ( g a s gangrene, clostridial
The Journal of the Korean Society of Fractures Vol15, No4, October, 2002 : 134 TEL : 02-361-5640 FAX : 02-363-1139 E-mail : sbhahn@yumcyonseiackr 608 21 ), c l o s t r i d i u m ( g a s gangrene, clostridial
Most pathogenic Staph cause infection after a breach in the skin. PrepTalk Clicker Questions. First Case - Lulu. Diagnostic information
 Most pathogenic Staph cause infection after a breach in the skin. PrepTalk Clicker Questions A. True B. False Did you Prep? Which factor is most strongly correlated with the virulence of pathogenic staphylococci?
Most pathogenic Staph cause infection after a breach in the skin. PrepTalk Clicker Questions A. True B. False Did you Prep? Which factor is most strongly correlated with the virulence of pathogenic staphylococci?
CRACKCast Episode 137: Skin Infections (Ch th )
") CRACKCast Episode 137: Skin Infections (Ch. 129 9 th ) Episode Overview Key Concepts: Skin infections are common and are rarely life-threatening. Deadly necrotizing skin and soft tissue infections are
CRACKCast Episode 137: Skin Infections (Ch. 129 9 th ) Episode Overview Key Concepts: Skin infections are common and are rarely life-threatening. Deadly necrotizing skin and soft tissue infections are
Life-threatening infections. Frank Bowden October 5, 2018
 Life-threatening infections Frank Bowden October 5, 2018 David Sackett Evidence Based Medicine is the integration of best research evidence with clinical expertise and patient values. The Golden Rules
Life-threatening infections Frank Bowden October 5, 2018 David Sackett Evidence Based Medicine is the integration of best research evidence with clinical expertise and patient values. The Golden Rules
Il ruolo del chirurgo nella gestione delle infezioni di cute e tessuti molli
 Il ruolo del chirurgo nella gestione delle infezioni di cute e tessuti molli Massimo Sartelli U.O. Chirurgia Generale Ospedale di Macerata Surgical Site infections Incisional - Superficial - Deep Non-necrotizing
Il ruolo del chirurgo nella gestione delle infezioni di cute e tessuti molli Massimo Sartelli U.O. Chirurgia Generale Ospedale di Macerata Surgical Site infections Incisional - Superficial - Deep Non-necrotizing
Streptococcus (gram positive coccus)
") #13 made by : aseel al-waked corrected by Shatha Khtoum date : 6/11/2016 Streptococcus (gram positive coccus) Slide 2 (56:00): Streptococci Facultative anaerobe Gram-positive usually chains (sometimes
#13 made by : aseel al-waked corrected by Shatha Khtoum date : 6/11/2016 Streptococcus (gram positive coccus) Slide 2 (56:00): Streptococci Facultative anaerobe Gram-positive usually chains (sometimes
Chapter 4 Inflammation and Infection
 Chapter 4 Inflammation and Infection Defense Mechanisms Three lines of defense protect the body against foreign invasion: Physical or surface barriers Inflammation Immune response Inflammation Non-specific
Chapter 4 Inflammation and Infection Defense Mechanisms Three lines of defense protect the body against foreign invasion: Physical or surface barriers Inflammation Immune response Inflammation Non-specific
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Mechanisms of Pathogenicity
 Mechanisms of Pathogenicity The Microbes Fight Back Medically important bacteria Salmonella Bacillus anthracis Shigella dysenteriae Campylobacter Shigella sonnei Clostridium botulinum Staphylococcus aureus
Mechanisms of Pathogenicity The Microbes Fight Back Medically important bacteria Salmonella Bacillus anthracis Shigella dysenteriae Campylobacter Shigella sonnei Clostridium botulinum Staphylococcus aureus
Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,.
 Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,. 12-10-2017 Group B streptococci are uniformly sensitive to penicillin
Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,. 12-10-2017 Group B streptococci are uniformly sensitive to penicillin
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
The Streptococci. Diverse collection of cocci. Gram-positive Chains or pairs significant pathogens
 The Streptococci Diverse collection of cocci. Gram-positive Chains or pairs significant pathogens Strong fermenters Facultative anaerobes Non-motile Catalase Negative 1 Classification 1 2 Classification
The Streptococci Diverse collection of cocci. Gram-positive Chains or pairs significant pathogens Strong fermenters Facultative anaerobes Non-motile Catalase Negative 1 Classification 1 2 Classification
Foundations in Microbiology
 Foundations in Microbiology Fifth Edition Talaro Chapter 18 Cocci of Medical Importance Chapter 18 2 Cocci of Interest Staphylococcus aureus S. epidermidis, S. hominis, S. capitis S. saprophyticus Streptococcus
Foundations in Microbiology Fifth Edition Talaro Chapter 18 Cocci of Medical Importance Chapter 18 2 Cocci of Interest Staphylococcus aureus S. epidermidis, S. hominis, S. capitis S. saprophyticus Streptococcus
Foot infections are now among the most
 Article Progress in a pedestrian problem: A review of the revised Infectious Diseases Society of America diabetic foot infection guidelines Benjamin A Lipsky This article was first published in The Diabetic
Article Progress in a pedestrian problem: A review of the revised Infectious Diseases Society of America diabetic foot infection guidelines Benjamin A Lipsky This article was first published in The Diabetic