I have no financial disclosures
|
|
|
- Morgan Kelley
- 6 years ago
- Views:
Transcription
1 Pulmonary Medicine Rosemary Adamson, MB BS Assistant Professor, Division of Pulmonary & Critical Care Medicine, UW Attending Physician, Pulmonary & Critical Care, Seattle VA
2 I have no financial disclosures
3 5. Nodules & screening 4. Pulmonary hypertension 3. Restrictive lung diseases 2. Obstructive lung diseases 1. Cough
4 Cough Number 1 reason for PCP visit Acute: <3 weeks Chronic: >8 weeks
5 Cough: Acute bronchitis Cough of less than 3 weeks duration Antibiotics may shorten duration of symptoms BUT Increase adverse events AVOID antibiotic prescription when possible
6 Strategies to avoid prescribing antibiotics for acute bronchitis Prescribe DELAYED antibiotics Recommend symptomatic treatments Recommend returning if not improving 80% patients satisfied with delayed or no antibiotics Spurling et al. Cochrane Database Syst Rev. 2013
7 Cough: Gastroesophageal reflux PPIs suppress acid production but not reflux Lifestyle modifications for GERD: Avoid food for 3 hours before bed Elevate the head of the bed Decrease caffeine, spicey food, mint, alcohol
8 Cough: Upper Airway Syndrome Inhaled nasal steroid Antihistamine Nasal irrigation Really important in all lung diseases
9 Avoid antibiotics for acute bronchitis Recommend symptomatic treatment Recommend returning if not better Consider prescribing delayed antibiotics GERD-induced cough can persist on PPI Upper airway syndrome can require aggressive management 1. Cough
10 5. Nodules & screening 4. Pulmonary hypertension 3. Restrictive lung diseases 2. Obstructive lung diseases 1. Cough


11 Asthma
12 Asthma: outpatient management Short-acting β-agonist Inhaled corticosteroid Review triggers Long-acting β-agonist Discuss lifestyle changes Develop asthma action plan Consider leukotriene receptor antagonist Consider tiotropium, Check inhaler technique Oral corticosteroids, Consider allergy testing Referral to allergy or pulmonary
13 Asthma: action plans Download from NIH.gov. Complete!
14 Asthma: management, additional therapies Omalizumab Moderate-severe persistent asthma with Incomplete control with ICS IgE ve skin or specific IgE test to perennial allergen Dosed by weight & IgE level Subcutaneous injection /2-4wks Mepolizumab Severe asthma with Eosinophilia > 150/microL Subcutaneous injection /4wks Immunotherapy +ve skin or specific IgE test to allergens Subcutaneous injection or sublingual tablets
15 Asthma: management of exacerbations Oral steroids as good as IV Consider magnesium sulfate Early recognition is key! Non-invasive ventilation use increasing Permissive hypercapnia if intubated
16 Increasing exacerbations COPD: evaluation of stable outpatients Increasing Check spirometry for reduced FEV1/FVC ratio symptoms C D A B Vogelmeier et al. Global strategy for the diagnosis, management and prevention of COPD 2017 report. AJRCCM 2017;195:
17 Modified Medical Research Council questionnaire Grade Dyspnea occurs 0 Only with strenuous activity 1 Walking up slight hill or hurrying on flat 2 Walk slower than people of same age, or have to stop, on level ground 3 And have to stop after few minutes or ~100m 4 Performing ADLs; cannot leave house
18 COPD Assessment Tool Rate on scale of 0 (good) to 5 (bad) each of the following: Cough Phlegm Chest tightness Confidence leaving home Dyspnea walking uphill or 1 flight of stairs Limitation to activities in the home Sleep quality Energy level
19 COPD management?+ roflumilast SABA LABA or LAMA LABA + LAMA LABA + LAMA + ICS SABA: short-acting β-agonist LABA: long-acting β-agonist LAMA: long-acting muscarinic agonist ICS: inhaled corticosteroid?+ azithromycin Vogelmeier et al. Global strategy for the diagnosis, management and prevention of COPD 2017 report. AJRCCM 2017;195:
20 COPD management Vaccinations Smoking cessation! Check alpha-1- antitrypsin Pulmonary rehabilitation Opioids & palliative care Consider surgery Vogelmeier et al. Global strategy for the diagnosis, management and prevention of COPD 2017 report. AJRCCM 2017;195:
21 COPD management: recent updates Home oxygen only for severe resting hypoxemia Nocturnal BiLevel may benefit those with hypercapnia Vogelmeier et al. Global strategy for the diagnosis, management and prevention of COPD 2017 report. AJRCCM 2017;195:
22 COPD: management of acute exacerbations 5-7 days of steroids is sufficient Antibiotics not necessary if no sputum purulence Noninvasive ventilation improves outcomes Vogelmeier et al. Global strategy for the diagnosis, management and prevention of COPD 2017 report. AJRCCM 2017;195:
23 You evaluated a 54yo man with a chronic productive cough. CXR showed right lower lobe bronchiectasis so you referred him to pulmonary. He returns to review the recommendations from the pulmonologist with you. Assessment: 54M with focal bronchiectasis due to remote severe pneumonia. Plan: - Airway clearance twice daily with nebulized albuterol, then flutter device - Antibiotics for exacerbations according to sputum culture data
24 Bronchiectasis: Abnormal, permanent dilatation of the airways Mucus plugs distend airways Impaired mucociliary clearance BRONCHIECTASIS & mucus hypersecretion Fibrosis pulls on airways Bacterial biofilms
25 Bronchiectasis: pathology

26 Copious sputum production
27 Bronchiectasis: evaluation Causes of bronchiectasis: Chest CT & pulmonary referral Non-tuberculous mycobacterial infection Cystic fibrosis Alpha-1-antitrypsin deficiency Immunoglobulin deficiency Primary ciliary dyskinesia Aspiration Collagen vascular diseases

28 Bronchiectasis: management Airway clearance techniques Mucus-mobilization Anti-inflammatories Aspiration reduction Antimicrobials
29 Asthma: make action plans COPD: avoid ICS when possible Bronchiectasis: airway clearance is key 2. Obstructive lung diseases
30 5. Nodules & screening 4. Pulmonary hypertension 3. Restrictive lung diseases 2. Obstructive lung diseases 1. Cough
, installation or removal of asbestos")
 Latency >30yrs Basal predominant interstitial fibrosis Diagnosis of")
31 Asbestosis Diffuse parenchymal lung disease due to years of exposure to asbestos from: Mining for asbestos or vermiculite (Libby, MT), installation or removal of asbestos insulation (ships, pipes, boilers), popcorn ceilings, demolition work, vehicle maintenance (brake pads & clutch) Latency >30yrs Basal predominant interstitial fibrosis Diagnosis of exclusion
32 Diffuse Parenchymal Lung Disease Known cause or association Unknown cause Systemic disease Exposures Genetic Idiopathic Interstitial Pneumonias Other pathologies Connective tissue disease IBD Sarcoidosis Pneumoconioses Hypersensitivity pneumonitis Iatrogenic Familial IPF Tuberous sclerosis IPF NSIP DIP RB-ILD LIP COP LAM LCH PAP Eosinophilic pneumonias
33 Disease Associated occupations Exposure duration Asbestosis Mining, vehicle repair, ship-building, boiler/ pipe fitting, demolition Latency Histopathology Imaging findings >10yrs >30yrs Fibrosis Lower lobe predominant Possible pleural plaques Special points Silicosis Coal-workers pneumoconiosis Mining, sandblasting, glassmaking, ceramics, brick foundries years 20-30yrs Nodules Upper lobe eggshell calcification of hilar LNs PMF (progressive massive fibrosis) possible Coal mining Nodules Upper lobe PMF possible Berylliosis Electronics, manufacturing, ceramics, old fluorescent lightbulbs >2yrs Chronic interstitial pneumonitis Upper lobe Hilar LAD Beryllium lymphocyte transformation test. Rx: steroids
34 Diffuse Parenchymal Lung Disease Known cause or association Unknown cause Systemic disease Exposures Genetic Idiopathic Interstitial Pneumonias Other pathologies Connective tissue disease IBD Sarcoidosis Pneumoconioses Hypersensitivity pneumonitis Iatrogenic Familial IPF Tuberous sclerosis IPF NSIP DIP RB-ILD LIP COP LAM LCH PAP Eosinophilic pneumonias
35 Sarcoidosis Multisystem, inflammatory disorder Characterized by non-caseating granulomas Lungs involved in 90% of cases Epidemiology: Female predominance Highest incidence in US & Sweden More common in African-Americans than Caucasian- Americans BUT rare in people from Africa

36 Sarcoidosis: clinical features Iannuzzi M et al. N Engl J Med 2007;357:

37

38 Sarcoidosis: Diagnosis Clinical diagnosis for certain syndromes E.g. Lofgren s syndrome Typically need biopsy Non-caseating granulomas Iannuzzi M et al. N Engl J Med 2007;357:
39 Sarcoidosis: Management Assess severity Evaluate critical systems (eyes, heart, calcium level) Monitor for progression Consider steroids Ask about syncope at every appointment
40 Diffuse Parenchymal Lung Disease Known cause or association Unknown cause Systemic disease Exposures Genetic Idiopathic Interstitial Pneumonias Other pathologies Connective tissue disease IBD Sarcoidosis Pneumoconioses Hypersensitivity pneumonitis Iatrogenic Familial IPF Tuberous sclerosis IPF NSIP DIP RB-ILD LIP COP LAM LCH PAP Eosinophilic pneumonias

41 DPLD: Idiopathic Pulmonary Fibrosis DPLD characterized by findings of Usual Interstitial Pneumonia Natural history: Slowly progressive Median survival 2-3yrs from diagnosis Risk factors: Prevalence & incidence increase with age More common in men Association with gastroesophageal reflux

42 IPF: diagnosis Exclude other causes Characteristic chest CT Characteristic histopathology Biopsy not always necessary Radiographic & histopathologic patterns termed Usual Interstitial Pneumonia
43 IPF: management Supportive care: Vaccinations Pulmonary rehabilitation GERD reduction Oxygen Consider lung transplant Palliative care Specific therapies: Pirfenidone (anti-fibrotic) Nintedanib (TK-inhibitor) Slow rate of decline in PFTs Multiple drug interactions Side effects: GI, rash, hepatotoxicity

44 Restrictive Lung disease: pathophysiology Reduced TLC Increased lung recoil Decreased chest wall recoil Diffuse Parenchymal Lung Disease Chest wall abnormality Neuromuscular weakness
45 Neuromuscular Lung Disease: causes Nervous System Phrenic nerve injury Guillain-Barré syndrome Poliomyelitis Amyotrophic lateral sclerosis Spinal cord injury Neuromuscular Junction Myasthenia gravis Muscle Post-polio syndrome Muscular dystrophy

46 Neuromuscular Lung Disease: clinical features & management Weak cough, recurrent pneumonias Respiratory failure Pulmonary function testing used to assess severity: MIP = Maximum Inspiratory Pressure bedside MIP = NIF = Negative Inspiratory Force MEP = Maximum Expiratory Pressure Cough assist may be required Ventilatory support may be required First at night Then daytime as well
47 3. Restrictive lung diseases Pulmonary restriction is Diagnosed by lung volumes Due to parenchymal or chest wall pathology Evaluation involves either High-resolution chest CT or Neuromuscular strength evaluation For patients with DPLD on chest CT Look for cause or association
48 5. Nodules & screening 4. Pulmonary hypertension 3. Restrictive lung diseases 2. Obstructive lung diseases 1. Cough
49 Pulmonary Hypertension: pathophysiology Pulmonary Vascular Resistance Right Ventricle Left heart overload Left Atrium
50 Pulmonary Hypertension: WHO classification Group 1: pulmonary arterial hypertension Group 2: due to left heart disease Group 3: due to lung disease or hypoxemia Group 4: due to chronic thromboembolic disease Group 5: unclear multifactorial mechanisms
51 Pulmonary hypertension: WHO functional classes Class Description 1 No limitation to activity 2 Ordinary activity causes some symptoms 3 Less than ordinary activity causes symptoms 4 Any activity causes symptoms Syncope
52 Pulmonary Hypertension: management Oxygen Coumadin Calcium Channel Blockers PDE5 Inhibitors Endothelin-Receptor antagonists Prostacyclin Analogues Right Ventricle Diuresis Digoxin Exercise Diuresis Left Atrium
53 4. Pulmonary hypertension PFTs with isolated DLCO reduction are concerning for pulmonary hypertension Pulmonary hypertension should be Screened for with TTE Diagnosed by right heart catheterization Left heart failure is most common cause in US Syncope indicates decompensation
54 5. Nodules & screening 4. Pulmonary hypertension 3. Restrictive lung diseases 2. Obstructive lung diseases 1. Cough

55 Pulmonary nodules: talking to patients Give them a leaflet Show them the size Encourage smoking cessation
56 Pulmonary nodule management: Fleischner guidelines Refer to: Incidentally discovered nodules in patients who are Older than 35 Immunocompentent Without cancer 2017 update: NO follow-up for solid nodules <6mm FIVE years follow-up for sub-solid nodules
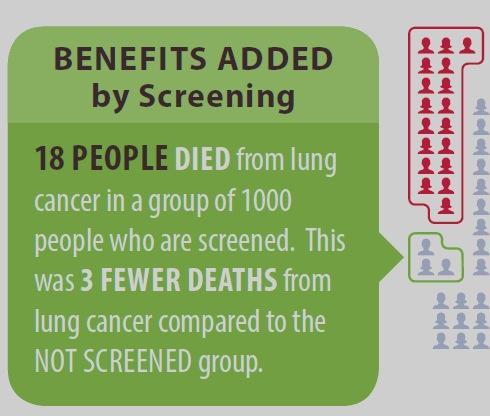
57 Lung cancer screening Give them a leaflet Refer to program if possible Encourage smoking cessation Discuss risks

58
59

60
61 Benefit of quitting smoking is greater than screening

62 Lung cancer screening USPSTF recommends: Annual low-dose chest CT for 55-80year olds with >30 pack-year smoking history who have quit for <15 years
63 Lung nodules Are very common Need to be explained to patients Lung cancer screening Significant pre-screening counselling Encourage smoking cessation 5. Nodules & screening

64 5. Nodules & screening 4. Pulmonary hypertension 3. Restrictive lung diseases 2. Obstructive lung diseases 1. Cough
65 Pulmonary medicine: final take-home points Upper airway syndrome & GERD are common exacerbate all lung diseases may not be obvious Everyone needs to QUIT smoking!
66 Thank you & any questions? Rosemary Adamson, MB BS
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Case Presentations in ILD. Harold R. Collard, MD Department of Medicine University of California San Francisco
 Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
Dr.kassim.m.sultan F.R.C.P
 Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
CALGARY ZONE PULMONARY REFERRAL QUICK REFERENCE
 CALGARY ZONE PULMONARY REFERRAL QUICK REFERENCE EMERGENCY (Patient needs to be seen immediately) Hemoptysis (Active & 2 TBSP per day) Hypoxemia (if resting O2 SAT 85%) Pulmonary embolism (Acute - known
CALGARY ZONE PULMONARY REFERRAL QUICK REFERENCE EMERGENCY (Patient needs to be seen immediately) Hemoptysis (Active & 2 TBSP per day) Hypoxemia (if resting O2 SAT 85%) Pulmonary embolism (Acute - known
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
REFERRAL GUIDELINES RESPIRATORY
 REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Common Pulmonary Problems. Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine
 Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates
 and Updates") Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
COPD Update. Muhammad Talha Khan MD. COPD Exacerbations. COPD Clinical Importance. COPD Pathophysiology. Overview/Objectives
 Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines
 Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Decramer 2014 a &b [21]
![Decramer 2014 a &b [21]](/thumbs/90/101390504.jpg "Decramer 2014 a &b [21]") Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Lines and crackles. Making sense of ILD
 Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
Supported by an educational grant from
 IDIOPATHIC PULMONARY FIBROSIS: PATIENT INFORMATION BROCHURE Supported by an educational grant from 08232-106 CONTENTS What is Pulmonary Fibrosis?.......................................................
IDIOPATHIC PULMONARY FIBROSIS: PATIENT INFORMATION BROCHURE Supported by an educational grant from 08232-106 CONTENTS What is Pulmonary Fibrosis?.......................................................
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
LUNG DISEASES DUE TO ORGANIC&INORGANIC DUSTS. Dr.kassim.m.sultan F.R.C.P
 LUNG DISEASES DUE TO ORGANIC&INORGANIC DUSTS Dr.kassim.m.sultan F.R.C.P efinition of hypersensitivity pneumonitis(extrinsic allergic alveolitis): Inflammatory disorder of the lung, involving alveolar walls
LUNG DISEASES DUE TO ORGANIC&INORGANIC DUSTS Dr.kassim.m.sultan F.R.C.P efinition of hypersensitivity pneumonitis(extrinsic allergic alveolitis): Inflammatory disorder of the lung, involving alveolar walls
Disclosures. Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting. Relevant financial relationships: None. Off-label usage: None
 Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Common Pulmonary Problems. Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine
 Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
DIAGNOSTIC NOTE TEMPLATE
 DIAGNOSTIC NOTE TEMPLATE SOAP NOTE TEMPLATE WHEN CONSIDERING A DIAGNOSIS OF IDIOPATHIC PULMONARY FIBROSIS (IPF) CHIEF COMPLAINT HISTORY OF PRESENT ILLNESS Consider IPF as possible diagnosis if any of the
DIAGNOSTIC NOTE TEMPLATE SOAP NOTE TEMPLATE WHEN CONSIDERING A DIAGNOSIS OF IDIOPATHIC PULMONARY FIBROSIS (IPF) CHIEF COMPLAINT HISTORY OF PRESENT ILLNESS Consider IPF as possible diagnosis if any of the
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Epidemiology and classification of smoking related interstitial lung diseases
 Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 5: restrictive lung diseases, part 1: fibrosing lung diseases
 DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 5: restrictive lung diseases, part 1: fibrosing lung diseases Reference: Robbins, 9 th : 472-478, 10 th : 506-512 INTRODUCTION: RESTRICTIVE
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 5: restrictive lung diseases, part 1: fibrosing lung diseases Reference: Robbins, 9 th : 472-478, 10 th : 506-512 INTRODUCTION: RESTRICTIVE
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Presented by UIC College of Nursing
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Chronic Obstructive Pulmonary Disease 1/18/2018
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Pulmonary Test Brenda Shinar
 Pulmonary Test 2016 Brenda Shinar 1. What is a Renal Tubular Acidosis? What is the difference between the types of RTAs in terms of who gets them and how to diagnose them? Type 1, 2, and 4? Metabolic acidosis
Pulmonary Test 2016 Brenda Shinar 1. What is a Renal Tubular Acidosis? What is the difference between the types of RTAs in terms of who gets them and how to diagnose them? Type 1, 2, and 4? Metabolic acidosis
COPD Diagnosis, Management and Program
 COPD Diagnosis, Management and Program RYAN MARTIN, MD NEBRASKA PULMONARY SPECIALTIES Initial diagnosis Setting matters: Inpatient. Usually sicker, oftentimes avoiding healthcare. Outpatient. Often seeking
COPD Diagnosis, Management and Program RYAN MARTIN, MD NEBRASKA PULMONARY SPECIALTIES Initial diagnosis Setting matters: Inpatient. Usually sicker, oftentimes avoiding healthcare. Outpatient. Often seeking
Update on Pulmonary Diseases. Jeffrey Lessar, MD
 Update on Pulmonary Diseases Jeffrey Lessar, MD 1 No disclosures to make No conflicts 2 Goals Update on key changes in Pulmonary Therapy 3 Spirometry Spirometry FEV1- forced expiratory Volume in 1 Sec
Update on Pulmonary Diseases Jeffrey Lessar, MD 1 No disclosures to make No conflicts 2 Goals Update on key changes in Pulmonary Therapy 3 Spirometry Spirometry FEV1- forced expiratory Volume in 1 Sec
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
A Review of Interstitial Lung Diseases
 Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
#POMAD8 #ChoosePOMA #POMAD8 #ChoosePOMA #POMAD8 #ChoosePOMA
 Where There s Smoke There s Obstruction Stephen G. Basheda, D.O., F.C.C.P. 1 Disclosures Dr. Basheda is an independent contractor for AstraZeneca Pharmaceuticals, LP and GlaxoSmithKline and on the speaker
Where There s Smoke There s Obstruction Stephen G. Basheda, D.O., F.C.C.P. 1 Disclosures Dr. Basheda is an independent contractor for AstraZeneca Pharmaceuticals, LP and GlaxoSmithKline and on the speaker
A Review of Interstitial Lung Diseases. Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco
 A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
Bill Davies PAC RRT. Dyspnea: Uncovering Restrictive lung Disorders in Your Setting
 Bill Davies PAC RRT Dyspnea: Uncovering Restrictive lung Disorders in Your Setting Bill Davies PAC RRT Confluence Health Division of Pulmonary/ Sleep Disorders Conversation Topic Brief Review of Dyspnea
Bill Davies PAC RRT Dyspnea: Uncovering Restrictive lung Disorders in Your Setting Bill Davies PAC RRT Confluence Health Division of Pulmonary/ Sleep Disorders Conversation Topic Brief Review of Dyspnea
Pediatric and Adult. Disclosure. Asthma. Learning Objectives. EPR-3: What s Changed? Asthma: Pediatric and Adult
 Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy
 Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
Diseases of the Lung and Respiratory Tract, Part I. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
9/15/11. Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September Scleroderma. Hard skin
 Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Surveillance report Published: 6 April 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Take My Breath Away: COPD Update. Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care
 Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
There are four general types of congenital lung disorders:
 Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Pulmonary Function Testing
 Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Pulmo-Park Pom-Pom Shooter: Measuring the Effect of Restricted Breathing on Peak Expiratory Flow (PEF) Student Information Page Activity 5D
 Student Information Page Activity 5D") Pom-Pom Shooter: Measuring the Effect of Restricted Breathing on Peak Expiratory Flow (PEF) Student Information Page Activity 5D Students with asthma or other respiratory problems should not perform the
Pom-Pom Shooter: Measuring the Effect of Restricted Breathing on Peak Expiratory Flow (PEF) Student Information Page Activity 5D Students with asthma or other respiratory problems should not perform the
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath