RESECTION OF TUBERCULOUS STRICTURES OF THE MAIN BRONCHI IN THREE CASES
|
|
|
- Suzan Bond
- 5 years ago
- Views:
Transcription
 Until recent years the excision of an obstructive lesion of a bronchus has had to include the")
1 Thorax (1955), 10, 229. RESECTION OF TUBERCULOUS STRICTURES OF THE MAIN BRONCHI IN THREE CASES BY J. W. JACKSON, P. H. JONES, AND T. HOLMES SELLORS From the London Chest and Harefield Hospitals (RECEIVED FOR PUBLICATION APRIL 28, 1955) Until recent years the excision of an obstructive lesion of a bronchus has had to include the corresponding lung segment. In many cases this lung tissue is irretrievably damaged by bronchiectasis or infective changes and requires removal, but on occasions the lung is not diseased and merits preservation. The introduction of plastic surgery of the bronchus is one of the latest developments in thoracic surgery and has proved itself of considerable value in conservation of pulmonary tissue-a feature of great importance in the treatment of pulmonary tuberculosis. Many surgeons have had experience of reconstructive operations of the bronchus after pulmonary resection, principally where a growth has extended along a main bronchus into the wall of the trachea or where an adenoma has invaded part of a bronchus which the surgeon had hoped to leave intact, but the records of success in the treatment of tuberculous strictures are infrequent. Direct closure of a defect made in a bronchus is a s-mple procedure and can be carried out effectively wherever sutures can be placed without narrowing other bronchi. The closure of a bronchial stump after lobectomy or pneumonectomy is the most common example. If sutures are likely to lead to narrowing, the defect can be closed by " patching" or covering, and here dermal grafts (Gebauer, 1950) have earned considerable popularity. The use of fascia lata and lung affords no problem so long as the defect is not so large that the graft is not supported and falls or is sucked into the bronchus or trachea and obstructs it. In such cases a framework of stainless steel or tantalum gauze gives support to the graft or the graft can be stiffened by steel threads passed through it. Resection of a wedge of bronchus followed by direct suture has also been carried out on many occasions, but complete sleeve resection has been parformed less frequently. Early attempts at bronchoplastic operations carried the risk of fistula formation with resulting pleural infection and non-expansion of lung-circumstances with which thoracic surgeons were only too familiar 10 or 15 years ago. The early successful sleeve resections were concerned with traumatic rupture of a main bronchus when the rigid wall of the tube was fractured, sometimes without loss of continuity of the mucosal lining. Direct end-to-end suture of a ruptured bronchus led to preservation of the lung in three instances in our experience, and recently attention was directed to pathological strictures beyond which there was complete or partial healthy lung tissue. To put the problem simply: many patients with a stricture or benign tumour of a main stem bronchus were treated in the past by pneumonectomy because the risks of a local resection of the bronchus were too high. Now it seems possible to perform a sleeve resection in selected cases and yet preserve a lobe or the whole of the lung. Tuberculosis is one of the most common causes of bronchial stricture, and the role played by endobronchitis in the course of the disease has been recognized as one of the most important pathological features. The healing of an endobronchial lesion, which is greatly helped by streptomycin, often leads to a fibrous stricture which may or may not be sufficiently severe to produce damage in the lung beyond. There are other methods of producing bronchostenosis, as for example by the external pressure of involved lymph glands or by ulceration of a caseous gland into the bronchial lumen. The site and severity of the stricture determine the fate of the lung, which may be left unaffected or may undergo atelectasis, bronchiectasis, abscess formation and retention, or pneumonitis. In some cases one lobe is unaffected while its neighbour is permanently damaged. The present article is concerned with the treatment of strictures of the main bronchi in which the Thorax: first published as /thx on 1 September Downloaded from on 20 September 2018 by guest. Protected by

2 230 J. W. JACKSON, P. H. JONES, and T. HOLMES SELLORS narrowing has not been so complete as to cause pathological changes in the whole lung, but has been restricted to damage and loss of function in one lobe only. One of the patients showed constriction in the left main bronchus with obliteration of the left upper lobe; the other two were concerned with strictures in the right main bronchus in which the right upper lobe was completely destroyed. In all cases an upper lobectomy was performed and at the same time a ring-shaped length of the main bronchus was excised and continuity restored with an end-to-end junction. In this way a useful functioning lower lobe was preserved. The problem of ensuring early and complete healing of a bronchial anastomosis is dependent on a variety of factors. The most important points are the production of an air-tight and accurate suture line between the divided ends, and early and complete re-expansion of lung so that no dead space persists. Antibiotics contribute to the control of infection, and in tuberculous patients they are of great value, as it is almost certain that some tuberculous tissue will have been incised during the course of the operation. The bronchial artery supply to the distal segment is inevitably interrupted by the division of the main stem bronchus, but this does not appear to jeopardize the vitality of the junction. The technical points in sleeve resection include a clean upper cut above the tuberculous stricture and fashioning the lower cut obliquely so that the bronchus when rejoined is directed more horizontally and laterally than it would be normally. Non-absorbable sutures are used and two or three mattress stitches on the posterior border give good approximation and support to the rest of the anastomosis. The slightly everted edge can then be secured by fine additional stitches. It was not found necessary to use any flap or graft of tissue round the suture line, and in the cases reported there were no complications and to date there has been no recurrence of the stenosis at the site of the junction. In general, resection of tuberculous strictures is more hazardous than the resection of simple strictures or of a simple growth within a bronchus, but a number of recent reports have been encouraging. Mathey and Maillard (1954) record three successful sleeve or ring resections for tuberculous stricture and Paulson and Shaw (1955) another three satisfactory examples. The field for this form of surgery is not extensive, but its ability to conserve healthy lung tissue in a number of patients constitutes a definite advance. CASE REPORTS CASE 1.-D. N., a woman aged 24 years, was diagnosed as having pulmonary tuberculosis at the age of 15, when an abnormal shadow at the left hilum was noted and the sputum was positive for tubercle bacillus. After six months in hospital she was discharged home free of symptoms and remained well until May, 1953, when she developed persistent cough with 2 oz. of purulent sputum a day. The sputum was negative and the radiographic appearances had not changed. She was treated with penicillin and postural drainage, with marked improvement of symptoms. In November, 1953, the sputum was positive. On admission to the London Chest Hospital in January, 1954, she had a cough with 1 oz. purulent sputum and some dyspnoea on exertion. She complained of a persistent wheeze in the chest, and this wheeze was clearly audible at the foot of the bed and made worse by lying on the left side. Sputum was positive, and the radiographs showed a calcified opacity projecting from the left hilum. Bronchograms showed a stenosis of the left main bronchus beginning just below the carina and terminating below the orifice of the left upper lobe. There were bronchiectatic changes in the lingular and anterolateral segments of the upper lobe and the apicoposterior segments were not filled. The lower lobe was normal. Bronchoscopy showed marked stenosis of the left main bronchus, beginning 1 cm. below the level of the carina. The bronchus was uniformly narrowed to a lumen of 4 mm. The mucosa was normal and the wall rigid. A period of four months' chemotherapy (streptomycin, P.A.S., and isoniazid) was given with some general improvement. Thoracotomy (May 10, 1954).-The patient was in the prone position and the pleural cavity was entered through the bed of the fifth rib. The left upper lobe was smaller than normal and nodular disease was palpab'e, mainly in the anterior segment. There were enlarged peri-bronchial lymph nodes, but no disease in the lower lobe. The upper lobe was dissected free and its bronchus divided after three arteries and the superior pulmonary vein had been secured. The lymph glands were removed from the main bronchus where they were very adherent, and the pulmonary artery freed from the posterior aspect of the main bronchus. The whole length of the main bronchus from the carina to the lower lobe branches was cleared and the stenotic area resected. The sleeve removed was 11 in. long and extended from the carina close to the bronchus to the apex of the lower lobe. The two ends were brought together and an end-toend anastomosis carried out with interrupted mattress sutures of non-absorbable material. The junction was tested for air leak and the chest wall closed with drainage after satisfactory expansion of the lower lobe had been observed. Thorax: first published as /thx on 1 September Downloaded from on 20 September 2018 by guest. Protected by

3 RESECTIONS OF STRICTURES IN MAIN BRONCHI The post-operative condition was satisfactory with good aeration of the left lower lobe, but on the second day partial atelectasis occurred; this was treated by bronchoscopic aspiration and resolved without incident. The subsequent course was uneventful, the remaining left lower lobe aerating satisfactorily. There was no evidence of wheeze. Four months later bronchoscopy showed that the left main bronchus was patent. Its orifice was threequarters the normal size, but the junction permitted passage of the bronchoscope and full visualization of the lower lobe orifices. A suture projecting into the lumen on the medial wall was removed, and this was the only evidence of any abnormality. The pathological report confirmed the presence of a strong fibrous stenosis beyond which there was bronchiectasis and widespread caseous tuberculosis. The bronchus at the point of section was oedematous but did not show giant cell systems. The general condition of the patient has remained completely satisfactory. CASE 2.-F. G., a housewife aged 44 years, had been in ill health from 1942 following tonsillectomy. The following year she was married, but continued to work as a saleswoman. Two years later her health deteriorated, and in the autumn of 1946 a radiograph of the chest showed extensive infiltration of the right upper lobe. This improved during three months of bed rest. In August, 1948, there was a spread into the right mid-zone and progressive collapse of the right upper lobe was noted. In December, 1952, following removal of a uterine polyp, her general condition deteriorated and extensive disease in the apical segment of the right lower lobe was recorded. Sputum was positive for tubercle bacilli. A six months' course of chemotherapy produced some improvement. On admission to Harefield Hospital at the beginning of 1954 she complained of dyspnoea on exertion and a wheeze which she stated had been present since This wheeze was easily audible from the end of the bed and there were rhonchi over the right chest. Her general condition was good; there was no cyanosis or clubbing. In June, 1954, bronchography showed complete absence of any filling of the right upper lobe because of a stricture of the right main bronchus at the level of the upper lobe orifice. Bronchoscopy revealed a severe stricture of the right main bronchus close to the carina. The upper lobe orifice could not be seen. A course of chemotherapy was given for the next six weeks. Thoracotomy (July 18, 1954).-With the patient in the face-down position, the pleural cavity was entered through the bed of the fifth rib. The right upper lobe was found shrunken, collapsed, and airless, firmly adherent in the greater fissure, with some calcified lesions felt in the apex of the lower lobe. The bronchus was dissected free with some difficulty, and a section of the bronchus from the carina to the level of the middle lobe orifice excised. The vessels S 231 to the upper lobe were secured and the upper lobe removed with the stenosed section of the main bronchus. Continuity was restored by an end-to-end anastomosis using interrupted mattress sutures. The lung re-expanded easily and the chest was closed with drainage. Her post-operative convalescence was uneventful, there being normal breath sounds the day after the operation and no wheeze. Bronchoscopy two months later showed a short right main bronchus which was not narrowed and with a direct view into the orifices of the middle and lower lobe branches. The line of suture could not be detected. A limited thoracoplasty was carried out, and the general condition of the patient has remained satisfactory. The specimen showed the narrowed main bronchus with an upper lobe branch which was completely occluded. The lobe showed fibrotic changes of recent and healed tuberculous disease. CASE 3.-M. H., a man aged 57 years, by occupation a civil servant, had pulmonary tuberculosis first diagnosed by mass radiography in June, Three years later the sputum was found to be positive, and he spent six months at home in bed. There was considerable improvement, but two years ago he developed bronchitis with cough and purulent sputum. The radiograph showed atelectasis of the right upper lobe; sputum was positive. He was treated in a sanatorium by bed rest and chemotherapy. Bronchoscopy in November, 1953, reported a stenosis of the right upper lobe orifice with scarring resulting from tuberculous endocarditis. In June, 1954, he had no symptoms, but the right upper lobe was atelectatic and small. In October, 1954, he was admitted to the London Chest Hospital. He had little sputum, which was negative, and the radiograph showed a collapsed right upper lobe with some infiltration and probably collapse of the middle lobe. Bronchoscopy showed stenosis of the right main bronchus, the opening being barely a quarter of the normal size and sited at the level of the carina; it was not possible to pass any instrument beyond this. A bronchogram confirmed the bronchoscopic findings and showed the absence of filling of the right upper lobe. A course of chemotherapy was started. Thoracouemy (December 21, 1954).-With the patient in the face-down position, the pleural cavity was entered through the bed of the fifth rib. The right upper lobe was collapsed and shrunken and there was a palpable lesion in the middle lobe. The trachea and the right main bronchus were dissected free and the stricture excised by incision through the carina and on to the lateral wall of the trachea. Anaesthesia was maintained by a cuff tube guided down the left main bronchus. The bronchus below the stricture was then divided just above the middle lobe opening, and this section containing the stricture was removed with the upper lobe after the appropriate vessels had been divided. Continuity was restored by an anastomosis of the bronchus Thorax: first published as /thx on 1 September Downloaded from on 20 September 2018 by guest. Protected by



4 232 J. W. JACKSON, P. H. JONES, and T. HOLMES SELLORS FIG. 1.-Case 1. Pre-operative radiograph showing calcified mass at the left hilum. FIGS. 2 AND 3.-Case 1. Bronchograms showing stricture close to the trachea and no filling of the upper lobe. (UK FIG. 2a FIG. 2-1 *X7l.q_ Thorax: first published as /thx on 1 September Downloaded from FIo. 1 FIG. 3 on 20 September 2018 by guest. Protected by


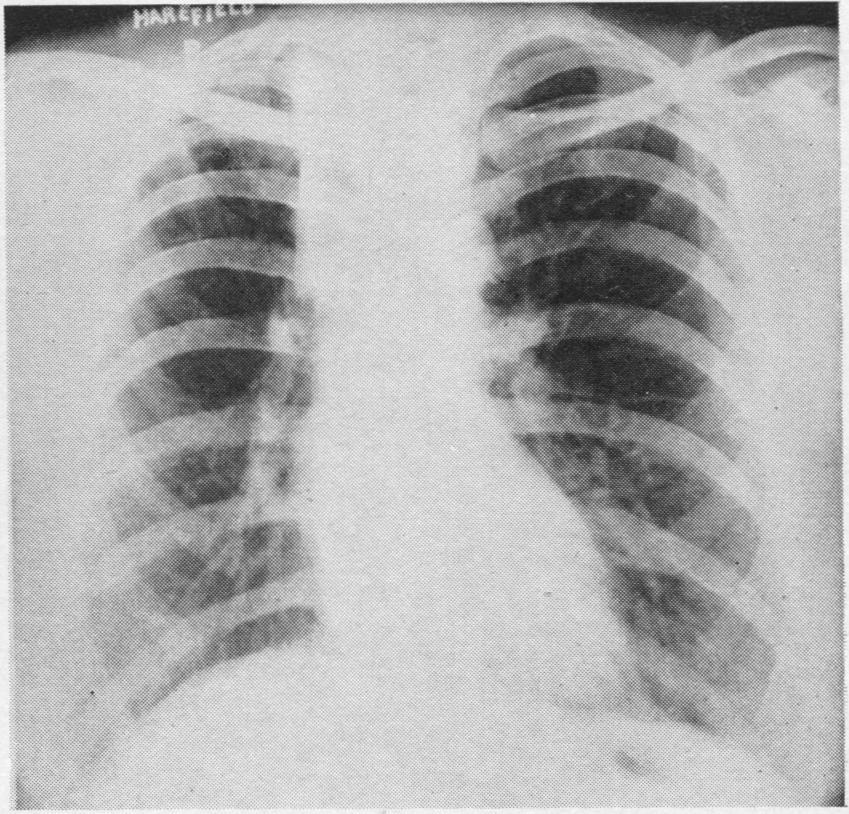
5 RESECTIONS OF STRICTURES IN MAIN BRONCHI 233 FiG. 4 ':.. ji FIGs. 4 AND 5.-Case 1. Post-operative radiographs. The outline of the left bronchus shows no narrowing. FIG. 6.-Case 1. Pre-operative radiograph showing complete collapse of the right upper lobe. FIG. 5a.:.:::-' - ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Thorax: first published as /thx on 1 September Downloaded from FIG. 5 Fio. 6 A on 20 September 2018 by guest. Protected by



6 234 *01 cpueq!,gj disdoc:, < - J. W. JACKSON, P. H. JONES, and T. HOLMES SELLORS :tricture 3verikppcs 9, upturned middli lobe nu co:- -r,c hus gjl. Thorax: first published as /thx on 1 September Downloaded from FIGS. 7 and 8.-Case 2. Bronchograms showing stricture just beyond the tracheal bifurcation, non-filling of the upper lobe, and bronchiectasis of the middle lobe. FIG. 9.-Case 2. Post-operative appearance. A small thoracoplasty has been performed in addition to the resection of the stricture and upper lobe. Flo. 9 on 20 September 2018 by guest. Protected by



7 RESECTIONS Uiplurned m -ddklobe rmtd, ci FIG. 10 Bcs6l brood FIG. 1Oa.^;os5tion of _ anostemosis OF STRICTURES IN MAIN BRONCHI Position of aonstomoes.is lst dorsol bronchus -; 2nd dorsal bronchus-- FIG. 11 FIG. - Upturned right middle lobe bronchi t -BosI bronchi lla 235 Thorax: first published as /thx on 1 September Downloaded from FIG. 12 FIGS. 10 AND 11.-Case 2. Bronchograms showing absence of any stricture in the right main bronchus, which is considerably shortened. FIG. 12.-Case 3. Pre-operative radiograph showing collapse right upper lobe. of the on 20 September 2018 by guest. Protected by



8 236 J W. JACKSON, P. H. JONES, and T. HOLMES SELLORS FIG. 13.-Case 3. Bronchogram showing stenosis where the right stem emerges from the trachea and no sign of an upper lobe bronchus. direct on to the trachea, interrupted non-absorbable stitches being used. The suture line was reinforced by a flap of mediastinal pleura and the middle and lower lobes were easily expanded before the chest was closed with drainage. A modified thoracoplasty was performed to reduce space and to control the disease in the middle lobe. FIG. 15.-Case 3. Bronchogram showing no narrowing at the site of the tracheo-bronchial anastomosis. FIG. 14.-Case 3. Post-operative radiograph. A small thoracoplasty has been performed. Thorax: first published as /thx on 1 September Downloaded from on 20 September 2018 by guest. Protected by The post-operative course was uneventful; there was a minimal air leak, and the tubes were removed three days after operation. Bronchoscopy six weeks after operation showed a normal calibre of the bronchus, and the only evidence of the anastomosis was a small irregular pit on the medial wall at the level of the carina. A bronchogram confirmed these findings. The patient's general condition has remained satisfactory. SUMMARY Tuberculous strictures of the main bronchi may produce secondary changes involving a lobe or the whole of the lung. This depends on the site and severity of the narrowing. In some cases surgical treatment involves the sacrifice of the whole lung; in others excision of the stricture and restoration of continuity may allow a considerable part of the lung to be preserved. Three cases are described in which a tuberculous stricture had destroyed one lobe only. The stricture and diseased lobe were excised and an end-to-end anastomosis performed. A successful result was achieved in each case, the remainder of the lung being preserved. BIBLIOGRAPHY Belcher, J. R. (1950). Brit. J. Surg., 38, 121. Carter, M. G., and Strieder, J. W. (1950). J. thorac. Surg., 20, 613. Gebauer, P. W. (1950). Ibid., 19, 604. Gravel, J. A. (1954). Ibid., 27, 244. Jackson, T. L., Lefkin, P., Tuttle, W., and Hampton, F. (1949). Ibid., 18, 630. Mathey, J., and Maillard, J. N. (1954). Sem. H6p. Paris, 7, 1. Paulson, D. L., and Shaw, R. R. (1955). J. thorac. Surg., 29, 238.
PULMONARY RESECTION FOR TUBERCULOSIS
 Thorax (1951), 6, 375. PULMONARY RESECTION FOR TUBERCULOSIS IN CHILDREN BY COLIN A. ROSS From Shotley Bridge Hospital and Poole Sanatorium (RECEIVED FOR PUBLICATION JULY 9, 1951) The literature concerning
Thorax (1951), 6, 375. PULMONARY RESECTION FOR TUBERCULOSIS IN CHILDREN BY COLIN A. ROSS From Shotley Bridge Hospital and Poole Sanatorium (RECEIVED FOR PUBLICATION JULY 9, 1951) The literature concerning
squamous-cell carcinoma1
 Thorax (1975), 30, 152. Local ablative procedures designed to destroy squamous-cell carcinoma1 J. M. LEE, FREDERICK P. STITIK, DARRYL CARTER, and R. ROBINSON BAKER Departments of Surgery, Pathology, and
Thorax (1975), 30, 152. Local ablative procedures designed to destroy squamous-cell carcinoma1 J. M. LEE, FREDERICK P. STITIK, DARRYL CARTER, and R. ROBINSON BAKER Departments of Surgery, Pathology, and
Lobectomy with sleeve resection in the
 Thorax (970), 25, 60. Lobectomy with sleeve resection in the treatment of bronchial tumours G. M. REES and M. PANETH Brompton Hospital, London, S.W3 Fortysix patients with malignant tumours involving the
Thorax (970), 25, 60. Lobectomy with sleeve resection in the treatment of bronchial tumours G. M. REES and M. PANETH Brompton Hospital, London, S.W3 Fortysix patients with malignant tumours involving the
PULMONARY INFARCTS ASSOCIATED WITH BRONCHOGENIC CARCINOMA
 Thor-ax (1954), 9, 304. PULMONARY INFARCTS ASSOCIATED WITH BRONCHOGENIC CARCINOMA W. J. HANBURY, R. J. R. CURETON, AND G. SIMON From St. Bartholomew's Hospital, London BY (RECEIVED FOR PUBLICATION JUNE
Thor-ax (1954), 9, 304. PULMONARY INFARCTS ASSOCIATED WITH BRONCHOGENIC CARCINOMA W. J. HANBURY, R. J. R. CURETON, AND G. SIMON From St. Bartholomew's Hospital, London BY (RECEIVED FOR PUBLICATION JUNE
APICAL SEGMENT OF THE LOWER LOBE IN RESECTIONS FOR BRONCHIECTASIS
 Thorax (1955), 10, 137. THE LATE RESULTS OF THE CONSERVATION OF THE APICAL SEGMENT OF THE LOWER LOBE IN RESECTIONS FOR BRONCHIECTASIS BY E. HOFFMAN From the Regional Thoracic Surgery Centre, Shotley Bridge
Thorax (1955), 10, 137. THE LATE RESULTS OF THE CONSERVATION OF THE APICAL SEGMENT OF THE LOWER LOBE IN RESECTIONS FOR BRONCHIECTASIS BY E. HOFFMAN From the Regional Thoracic Surgery Centre, Shotley Bridge
Parenchyma-sparing lung resections are a potential therapeutic
 Lung Segmentectomy for Patients with Peripheral T1 Lesions Bryan A. Whitson, MD, Rafael S. Andrade, MD, and Michael A. Maddaus, MD Parenchyma-sparing lung resections are a potential therapeutic option
Lung Segmentectomy for Patients with Peripheral T1 Lesions Bryan A. Whitson, MD, Rafael S. Andrade, MD, and Michael A. Maddaus, MD Parenchyma-sparing lung resections are a potential therapeutic option
Total collapse of the lung in aspergillosis
 Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
CAVERNOUS HAEMANGIOMA OF THE LUNG BY
 Thorax (1947), 2, 58 CAVERNOUS HAEMANGIOMA OF THE LUNG BY Leeds Cavernous haemangiomata of the lung are rare, and a survey of the French, American, and English literature on the subject has revealed only
Thorax (1947), 2, 58 CAVERNOUS HAEMANGIOMA OF THE LUNG BY Leeds Cavernous haemangiomata of the lung are rare, and a survey of the French, American, and English literature on the subject has revealed only
PERFORATION OF THE TRACHEA AND BRONCHUS BY THE BRONCHOSCOPE
 Thlorax (1950), 5, 369. PERFORATION OF THE TRACHEA AND BRONCHUS BY THE BRONCHOSCOPE BY Fronm the Regional Thoracic Surgery Centre, Shotley Bridge Hospital, Newcastle-upon-Tyne (RECEIVED FOR PUBLICATION
Thlorax (1950), 5, 369. PERFORATION OF THE TRACHEA AND BRONCHUS BY THE BRONCHOSCOPE BY Fronm the Regional Thoracic Surgery Centre, Shotley Bridge Hospital, Newcastle-upon-Tyne (RECEIVED FOR PUBLICATION
CASE REPORTS. Inflammatory Polyp of the Bronchus. V. K. Saini, M.S., and P. L. Wahi, M.D.
 CASE REPORTS V. K. Saini, M.S., and P. L. Wahi, M.D. I n 1932 Jackson and Jackson [l] first reported a number of clinical cases under the title Benign Tumors of the Trachea and Bronchi with Especial Reference
CASE REPORTS V. K. Saini, M.S., and P. L. Wahi, M.D. I n 1932 Jackson and Jackson [l] first reported a number of clinical cases under the title Benign Tumors of the Trachea and Bronchi with Especial Reference
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
Primary chondrosarcoma of lung
 Thorax,(1970), 25, 366. Primary chondrosarcoma of lung G. M. REES Department of Surgery, Brompton Hospital, Lontdonl, S.W.3 A case of primary chondrosarcoma of the lung is described in a 64-year-old man.
Thorax,(1970), 25, 366. Primary chondrosarcoma of lung G. M. REES Department of Surgery, Brompton Hospital, Lontdonl, S.W.3 A case of primary chondrosarcoma of the lung is described in a 64-year-old man.
EXCISION OF THE LUNG FOR PULMONARY TUBERCULOSIS
 Thorax (1949), 4, 82. EXCISION OF THE LUNG FOR PULMONARY TUBERCULOSIS BY T. HOLMES SELLORS AND M. D. HICKEY Fronm the London Chest Hospital Until recently the fear of the effects of injury to tuberculous
Thorax (1949), 4, 82. EXCISION OF THE LUNG FOR PULMONARY TUBERCULOSIS BY T. HOLMES SELLORS AND M. D. HICKEY Fronm the London Chest Hospital Until recently the fear of the effects of injury to tuberculous
IN THE SPREAD OF PULMONARY TUBERCULOSIS
 Thorax (1951), 6, 417. THE IMPORTANCE OF SLEEPING POSTURE IN THE SPREAD OF PULMONARY TUBERCULOSIS BY W. H. HELM From the London Chest Hospital (RECEIVED FOR PUBLICATION AUGUST 22, 195 1) When an infective
Thorax (1951), 6, 417. THE IMPORTANCE OF SLEEPING POSTURE IN THE SPREAD OF PULMONARY TUBERCULOSIS BY W. H. HELM From the London Chest Hospital (RECEIVED FOR PUBLICATION AUGUST 22, 195 1) When an infective
Surgical treatment of bronchial obstruction in primary tuberculosis in children: report of seven cases
 Thorax, 1979, 34, 464-469 Surgical treatment of bronchial obstruction in primary tuberculosis in children: report of seven cases A J NAKVI AND H C NOHL-OSER From the Cardiothoracic Unit, Harefield Hospital,
Thorax, 1979, 34, 464-469 Surgical treatment of bronchial obstruction in primary tuberculosis in children: report of seven cases A J NAKVI AND H C NOHL-OSER From the Cardiothoracic Unit, Harefield Hospital,
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
OSAMA A. ABDULMAJID, ABDELMOMEN M. EBEID, MOHAMED M. MOTAWEH, and IBRAHIM S. KLEIBO
 Aspirated foreign bodies in the tracheobronchial tree: report of 250 cases Thorax (1976), 31, 635. OSAMA A. ABDULMAJID, ABDELMOMEN M. EBEID, MOHAMED M. MOTAWEH, and IBRAHIM S. KLEIBO Thoracic Surgical
Aspirated foreign bodies in the tracheobronchial tree: report of 250 cases Thorax (1976), 31, 635. OSAMA A. ABDULMAJID, ABDELMOMEN M. EBEID, MOHAMED M. MOTAWEH, and IBRAHIM S. KLEIBO Thoracic Surgical
PULMONARY TUBERCULOSIS
 RESECTION FOR PULMONARY TUBERCULOSIS By W. P. CLELAND, M.R.C.P., F.R.C.S. Surgeon, Brompton Chest Hospital, Thoracic Surgeon, King's College Hospital Removal of tuberculous organs or tissues has long been
RESECTION FOR PULMONARY TUBERCULOSIS By W. P. CLELAND, M.R.C.P., F.R.C.S. Surgeon, Brompton Chest Hospital, Thoracic Surgeon, King's College Hospital Removal of tuberculous organs or tissues has long been
BRONCHOLITHIASIS. Report of Two Cases. H. S. VanORDSTRAND, M.D., PAUL M. MOORE, Jr., M.D. and H. E. HARRIS, M.D.
 Report of Two Cases H. S. VanORDSTRAND, M.D., PAUL M. MOORE, Jr., M.D. and H. E. HARRIS, M.D. In patients presenting the symptoms and physical findings of partial to complete bronchial obstruction, a broncholith
Report of Two Cases H. S. VanORDSTRAND, M.D., PAUL M. MOORE, Jr., M.D. and H. E. HARRIS, M.D. In patients presenting the symptoms and physical findings of partial to complete bronchial obstruction, a broncholith
RECOGNITION OF NON-OPAQUE FOREIGN
 THE IMPORTANCE OF BRONCHOSCOPY IN THE RECOGNITION OF NON-OPAQUE FOREIGN BODY IN INFANTS AND CHILDREN BY N. ASHERSON, M.A., M.B., B.S., F.R.C.S. Surgeon to the Central London Throat, Nose and Ear Hospital
THE IMPORTANCE OF BRONCHOSCOPY IN THE RECOGNITION OF NON-OPAQUE FOREIGN BODY IN INFANTS AND CHILDREN BY N. ASHERSON, M.A., M.B., B.S., F.R.C.S. Surgeon to the Central London Throat, Nose and Ear Hospital
Uniportal video-assisted thoracoscopic sleeve lobectomy and other complex resections
 Surgical Technique Uniportal video-assisted thoracoscopic sleeve lobectomy and other complex resections Diego Gonzalez-Rivas,2, Eva Fieira, Maria Delgado, Mercedes de la Torre,2, Lucia Mendez, Ricardo
Surgical Technique Uniportal video-assisted thoracoscopic sleeve lobectomy and other complex resections Diego Gonzalez-Rivas,2, Eva Fieira, Maria Delgado, Mercedes de la Torre,2, Lucia Mendez, Ricardo
Empyema due to Klebsiella pneumoniae
 Thorax (1967), 22, 170. Empyema due to Klebsiella pneumoniae J. M. REID, R. S. BARCLAY, J. G. STEVENSON, T. M. WELSH, AND N. McSWAN From thle Cardio-thoracic Unit, Mearnskirk Hospital, Renifrewshire Three
Thorax (1967), 22, 170. Empyema due to Klebsiella pneumoniae J. M. REID, R. S. BARCLAY, J. G. STEVENSON, T. M. WELSH, AND N. McSWAN From thle Cardio-thoracic Unit, Mearnskirk Hospital, Renifrewshire Three
The pure distal left main bronchial sleeve resection with total lung parenchymal preservation: report of two cases and literature review
 Case Report The pure distal left main bronchial sleeve resection with total lung parenchymal preservation: report of two cases and literature review Jian Tang 1, Min Cao 1, Liqiang Qian 2, Yujie Fu 1,
Case Report The pure distal left main bronchial sleeve resection with total lung parenchymal preservation: report of two cases and literature review Jian Tang 1, Min Cao 1, Liqiang Qian 2, Yujie Fu 1,
SURGICAL TECHNIQUE. Radical treatment for left upper-lobe cancer via complete VATS. Jun Liu, Fei Cui, Shu-Ben Li. Introduction
 SURGICAL TECHNIQUE Radical treatment for left upper-lobe cancer via complete VATS Jun Liu, Fei Cui, Shu-Ben Li The First Affiliated Hospital of Guangzhou Medical College, Guangzhou, China ABSTRACT KEYWORDS
SURGICAL TECHNIQUE Radical treatment for left upper-lobe cancer via complete VATS Jun Liu, Fei Cui, Shu-Ben Li The First Affiliated Hospital of Guangzhou Medical College, Guangzhou, China ABSTRACT KEYWORDS
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Sir Clement Price Thomas performed the first sleeve lobectomy
 Parenchymal-Sparing Procedures in Lung Cancer: Sleeve Resection of the Lung for Proximal Lesions Simon Ashiku, MD, and Malcolm M. DeCamp, Jr., MD Sir Clement Price Thomas performed the first sleeve lobectomy
Parenchymal-Sparing Procedures in Lung Cancer: Sleeve Resection of the Lung for Proximal Lesions Simon Ashiku, MD, and Malcolm M. DeCamp, Jr., MD Sir Clement Price Thomas performed the first sleeve lobectomy
Robotic-assisted right upper lobectomy
 Robotic Thoracic Surgery Column Robotic-assisted right upper lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital, Shenyang 110015,
Robotic Thoracic Surgery Column Robotic-assisted right upper lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital, Shenyang 110015,
March The patients, two men and nine. an average of 54 years. In 10 of these patients. the cervical trachea was affected.
 Thorax, 1978, 33, 378-386 Resection of thyroid carcinoma infiltrating the trachea T. ISHIHARA, K. KIKUCHI, T. IKEDA, H. INOUE, S. FUKAI, K. ITO', AND T. MIMURA' From the Department of Surgery, School of
Thorax, 1978, 33, 378-386 Resection of thyroid carcinoma infiltrating the trachea T. ISHIHARA, K. KIKUCHI, T. IKEDA, H. INOUE, S. FUKAI, K. ITO', AND T. MIMURA' From the Department of Surgery, School of
Video-assisted thoracic surgery pneumonectomy: the first case report in Poland
 Case report Videosurgery Video-assisted thoracic surgery pneumonectomy: the first case report in Poland Cezary Piwkowski, Piotr Gabryel, Mariusz Kasprzyk, Wojciech Dyszkiewicz Thoracic Surgery Department,
Case report Videosurgery Video-assisted thoracic surgery pneumonectomy: the first case report in Poland Cezary Piwkowski, Piotr Gabryel, Mariusz Kasprzyk, Wojciech Dyszkiewicz Thoracic Surgery Department,
COLLAPSE OF THE LUNG ASSOCIATED WITH PRIMARY
 Thorax (1960), 15, 346. COLLAPSE OF THE LUNG ASSOCIATED WITH PRIMARY TUBERCULOSIS: A REVIEW OF 51 CASES BY A. MARGARET C. MACPHERSON, P. A. ZORAB, AND LYNNE REID From the Children's Contact Clinics of
Thorax (1960), 15, 346. COLLAPSE OF THE LUNG ASSOCIATED WITH PRIMARY TUBERCULOSIS: A REVIEW OF 51 CASES BY A. MARGARET C. MACPHERSON, P. A. ZORAB, AND LYNNE REID From the Children's Contact Clinics of
Localised airway narrowing in sarcoidosis
 Thorax 1982;37:443-447 JW HADFIELD, RL PAGE, CDR FLOWER, JE STARK From Papworth Hospital, Papworth Everard, Cambridge, and Addenbrooke's Hospital, Cambridge ABSTRACr Four patients developed multiple narrowings
Thorax 1982;37:443-447 JW HADFIELD, RL PAGE, CDR FLOWER, JE STARK From Papworth Hospital, Papworth Everard, Cambridge, and Addenbrooke's Hospital, Cambridge ABSTRACr Four patients developed multiple narrowings
BRONCHOGRAPHY RESIDUAL IODIZED OIL FOLLOWING. bronchiectasis are to be undertaken, a previous inadequate bronchogram which
 Thorax (1946), 1, 93. RESIDUAL IODIZED OIL FOLLOWING BRONCHOGRAPHY BY H. E. COUNIHAN Thoracic Unit, Kewstoke Emergency Hospital Residual oil in the bronchial tree following bronchography is always undesirable;
Thorax (1946), 1, 93. RESIDUAL IODIZED OIL FOLLOWING BRONCHOGRAPHY BY H. E. COUNIHAN Thoracic Unit, Kewstoke Emergency Hospital Residual oil in the bronchial tree following bronchography is always undesirable;
Inhaled Foreign Bodies in Children
 Arch. Dis. Childh., 1966, 41, 402. Inhaled Foreign Bodies in Children An analysis of 40 cases CONSTANCE M. DAVIS From the Royal Liverpool Children's Hospital and Alder Hey Children's Hospital, Liverpool
Arch. Dis. Childh., 1966, 41, 402. Inhaled Foreign Bodies in Children An analysis of 40 cases CONSTANCE M. DAVIS From the Royal Liverpool Children's Hospital and Alder Hey Children's Hospital, Liverpool
CHAPTER 7 Procedures on Respiratory System
 CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Uniportal video-assisted thoracic surgery for complicated pulmonary resections
 Review Article on Thoracic Surgery Uniportal video-assisted thoracic surgery for complicated pulmonary resections Ding-Pei Han, Jie Xiang, Run-Sen Jin, Yan-Xia Hu, He-Cheng Li Jiaotong University School
Review Article on Thoracic Surgery Uniportal video-assisted thoracic surgery for complicated pulmonary resections Ding-Pei Han, Jie Xiang, Run-Sen Jin, Yan-Xia Hu, He-Cheng Li Jiaotong University School
Ruijin robotic thoracic surgery: S segmentectomy of the left upper lobe
 Case Report Page 1 of 5 Ruijin robotic thoracic surgery: S 1+2+3 segmentectomy of the left upper lobe Han Wu, Su Yang, Wei Guo, Runsen Jin, Yajie Zhang, Xingshi Chen, Hailei Du, Dingpei Han, Kai Chen,
Case Report Page 1 of 5 Ruijin robotic thoracic surgery: S 1+2+3 segmentectomy of the left upper lobe Han Wu, Su Yang, Wei Guo, Runsen Jin, Yajie Zhang, Xingshi Chen, Hailei Du, Dingpei Han, Kai Chen,
Robotic-assisted right inferior lobectomy
 Robotic Thoracic Surgery Column Page 1 of 6 Robotic-assisted right inferior lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital,
Robotic Thoracic Surgery Column Page 1 of 6 Robotic-assisted right inferior lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital,
SIX CASES OF TRAUMATIC RUPTURE OF THE BRONCHUS
 Thorax (1956), 11, 312. SIX CASES OF TRAUMATIC RUPTURE OF THE BRONCHUS BY MICHAEL BATES AND HARVEY J. BEARD From the North Middlesex Hospital and Kelling Hospital, Norfolk (RECEIVED FOR PUBLICATION APRIL
Thorax (1956), 11, 312. SIX CASES OF TRAUMATIC RUPTURE OF THE BRONCHUS BY MICHAEL BATES AND HARVEY J. BEARD From the North Middlesex Hospital and Kelling Hospital, Norfolk (RECEIVED FOR PUBLICATION APRIL
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Transbronchial fine needle aspiration
 Thorax 1982;37 :270-274 Transbronchial fine needle aspiration J LEMER, E MALBERGER, R KONIG-NATIV From the Departments of Cardio-thoracic Surgery and Cytology, Rambam Medical Center, Haifa, Israel ABSTRACT
Thorax 1982;37 :270-274 Transbronchial fine needle aspiration J LEMER, E MALBERGER, R KONIG-NATIV From the Departments of Cardio-thoracic Surgery and Cytology, Rambam Medical Center, Haifa, Israel ABSTRACT
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
A new approach to left sleeve pneumonectomy: complete VATS left pneumonectomy followed by right thoracotomy for carinal resection and reconstruction
 Fujino et al. Surgical Case Reports (2018) 4:91 https://doi.org/10.1186/s40792-018-0496-2 CASE REPORT A new approach to left sleeve pneumonectomy: complete VATS left pneumonectomy followed by right thoracotomy
Fujino et al. Surgical Case Reports (2018) 4:91 https://doi.org/10.1186/s40792-018-0496-2 CASE REPORT A new approach to left sleeve pneumonectomy: complete VATS left pneumonectomy followed by right thoracotomy
Lung & Pleura. The Topics :
 Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Routine reinforcement of bronchial stump after lobectomy or pneumonectomy with pedicled pericardial flap (PPF)
") Routine reinforcement of bronchial stump after lobectomy or pneumonectomy with pedicled pericardial flap (PPF) Abstract The results of 25 cases underwent a pedicled pericardial flap coverage for the bronchial
Routine reinforcement of bronchial stump after lobectomy or pneumonectomy with pedicled pericardial flap (PPF) Abstract The results of 25 cases underwent a pedicled pericardial flap coverage for the bronchial
Lung scanning in carcinoma of the bronchus
 Thorax (1971), 26, 23. Lung scanning in carcinoma of the bronchus R. H. SECKER WALKER, J. L. PROVAN1, J. A. JACKSON, and J. GOODWIN The Medical Unit, University College Hospital Medical School, University
Thorax (1971), 26, 23. Lung scanning in carcinoma of the bronchus R. H. SECKER WALKER, J. L. PROVAN1, J. A. JACKSON, and J. GOODWIN The Medical Unit, University College Hospital Medical School, University
PDF hosted at the Radboud Repository of the Radboud University Nijmegen
 PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/23566
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/23566
The Surgical Treatment of Tracheobronchial Tuberculosis. The Thoracic Department of Beijing Chest Hospital, Capital Medical University
 The Surgical Treatment of Tracheobronchial Tuberculosis ) The Thoracic Department of Beijing Chest Hospital, Capital Medical University Named also: endobronchial tuberculosis,ebtb defined as tuberculous
The Surgical Treatment of Tracheobronchial Tuberculosis ) The Thoracic Department of Beijing Chest Hospital, Capital Medical University Named also: endobronchial tuberculosis,ebtb defined as tuberculous
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
Lung cancer or primary malignant tumors of the mediastinum
 Technique of Superior Vena Cava Resection for Lung Carcinomas David R. Jones, MD Division of Thoracic and Cardiovascular Surgery, Department of Surgery, University of Virginia School of Medicine, Charlottesville,
Technique of Superior Vena Cava Resection for Lung Carcinomas David R. Jones, MD Division of Thoracic and Cardiovascular Surgery, Department of Surgery, University of Virginia School of Medicine, Charlottesville,
TREATMENT OF PULMONARY TUBERCULOSIS BY THORA- COPLASTY IN PATIENTS OVER 50 YEARS OF AGE
 Thorax (1954), 9, 2 1. TREATMENT OF PULMONARY TUBERCULOSIS BY THORA- COPLASTY IN PATIENTS OVER 50 YEARS OF AGE BY PETER BEACONSFIELD, H. S. COULTHARD, AND F. G. KERGIN From the Toronto Hospital for the
Thorax (1954), 9, 2 1. TREATMENT OF PULMONARY TUBERCULOSIS BY THORA- COPLASTY IN PATIENTS OVER 50 YEARS OF AGE BY PETER BEACONSFIELD, H. S. COULTHARD, AND F. G. KERGIN From the Toronto Hospital for the
CULOSIS IN CHILDHOOD AND ADOLESCENCE
 Thorax (1956), 11, 186. THE SURGICAL TREATMENT OF PULMONARY TUBER- CULOSIS IN CHILDHOOD AND ADOLESCENCE BY D. W. HUISH From the Regional Thoracic Surgical Centre, Dundee (RECEIVED FOR PUBLICATION OCTOBER
Thorax (1956), 11, 186. THE SURGICAL TREATMENT OF PULMONARY TUBER- CULOSIS IN CHILDHOOD AND ADOLESCENCE BY D. W. HUISH From the Regional Thoracic Surgical Centre, Dundee (RECEIVED FOR PUBLICATION OCTOBER
THORACOPLASTY WITH PLOMBAGE: A REVIEW OF
 Thorax (1950), 5, 248. THORACOPLASTY WITH PLOMBAGE: A REVIEW OF THE EARLY RESULTS IN 125 CASES BY B. G. B. LUCAS AND W. P. CLELAND London Cavity closure and sputum conversion by the modern thoracoplasty
Thorax (1950), 5, 248. THORACOPLASTY WITH PLOMBAGE: A REVIEW OF THE EARLY RESULTS IN 125 CASES BY B. G. B. LUCAS AND W. P. CLELAND London Cavity closure and sputum conversion by the modern thoracoplasty
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
Destructive pulmonary disease due to mixed anaerobic infection
 Thorax (1970), 25, 41. Destructive pulmonary disease due to mixed anaerobic infection 0. SERIKI, A. ADEYOKUNNU, T. 0. DE LA CRUZ Departments of Paediatrics and Surgery, University College Hospital, Ibadan,
Thorax (1970), 25, 41. Destructive pulmonary disease due to mixed anaerobic infection 0. SERIKI, A. ADEYOKUNNU, T. 0. DE LA CRUZ Departments of Paediatrics and Surgery, University College Hospital, Ibadan,
Lab #3. Mohammad Hisham Al-Mohtaseb. Jumana Jihad. Ammar Ramadan. 0 P a g e
 Lab #3 Mohammad Hisham Al-Mohtaseb Jumana Jihad Ammar Ramadan 0 P a g e Last anatomy lab: Lungs and structure on the mediastinal surfs: 1-the right lung: How do we know it s the right lung??? -the 3 lobes
Lab #3 Mohammad Hisham Al-Mohtaseb Jumana Jihad Ammar Ramadan 0 P a g e Last anatomy lab: Lungs and structure on the mediastinal surfs: 1-the right lung: How do we know it s the right lung??? -the 3 lobes
THE TREATMENT OF PULMONARY HYDATID DISEASE BY M. P. SUSMAN From the Sydney Hospital and the Royal North Shore Hospital, Sydney, Australia
 Thorax (1948), 3, 71. THE TREATMENT OF PULMONARY HYDATID DISEASE BY M. P. SUSMAN From the Sydney Hospital and the Royal North Shore Hospital, Sydney, Australia There is at present no medical treatment
Thorax (1948), 3, 71. THE TREATMENT OF PULMONARY HYDATID DISEASE BY M. P. SUSMAN From the Sydney Hospital and the Royal North Shore Hospital, Sydney, Australia There is at present no medical treatment
and errors VINCENT POWELL Midhurst, Sussex other years; not all cases are reported in the
 Thorax (1965), 20, 48. Inhaled foreign bodies: and errors VINCENT POWELL Midhurst, Sussex The inhalation of a foreign body is a commonplace accident. Most things that 'go the wrong way' are coughed up,
Thorax (1965), 20, 48. Inhaled foreign bodies: and errors VINCENT POWELL Midhurst, Sussex The inhalation of a foreign body is a commonplace accident. Most things that 'go the wrong way' are coughed up,
Video-assisted thoracic surgery right upper lobe bronchial sleeve resection
 Original Article on Thoracic Surgery Video-assisted thoracic surgery right upper lobe bronchial sleeve resection Qianli Ma, Deruo Liu Department of Thoracic Surgery, China-Japan Friendship Hospital, Beijing
Original Article on Thoracic Surgery Video-assisted thoracic surgery right upper lobe bronchial sleeve resection Qianli Ma, Deruo Liu Department of Thoracic Surgery, China-Japan Friendship Hospital, Beijing
Innovations in Lung Cancer Diagnosis and Surgical Treatment
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Dana Alrafaiah. - Moayyad Al-Shafei. -Mohammad H. Al-Mohtaseb. 1 P a g e
 - 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
- 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
THE GOOFY ANATOMIST QUIZZES
 THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
Tracheal stenosis in infants and children is typically characterized
 Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
Empyema and ruptured lung abscess in adults'
 Thorax (1964), 19, 492. Empyema and ruptured lung abscess in adults' ROWAN NICKS From the Thoracic Surgical Unit, Page Chest Pavilion, Royal Prince Alfred Hospital, Melbourne This brief annotation concerns
Thorax (1964), 19, 492. Empyema and ruptured lung abscess in adults' ROWAN NICKS From the Thoracic Surgical Unit, Page Chest Pavilion, Royal Prince Alfred Hospital, Melbourne This brief annotation concerns
Radiological Anatomy of Thorax. Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem
 Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Discussing feline tracheal disease
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai
 Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
CHIECTASIS, AND IN MASSIVE COLLAPSE
 Thorax (1952), 7, 98. THE CARTILAGE OF THE INTRAPULMONARY BRONCHI IN NORMAL LUNGS, IN BRON- CHIECTASIS, AND IN MASSIVE COLLAPSE BY JOHN HAYWARD AND LYNNE McA. REID* From the Royal Melbourne Hospital, Melbourne,
Thorax (1952), 7, 98. THE CARTILAGE OF THE INTRAPULMONARY BRONCHI IN NORMAL LUNGS, IN BRON- CHIECTASIS, AND IN MASSIVE COLLAPSE BY JOHN HAYWARD AND LYNNE McA. REID* From the Royal Melbourne Hospital, Melbourne,
Quality of Life (QOL) versus Curability for Lung Cancer Surgery
 versus Curability for Lung Cancer Surgery") Quality of Life (QOL) versus Curability for Lung Cancer Surgery Hirokuni Yoshimura, MD Standard operations for lung cancer patients are generally accepted as performing lobectomy or pneumonectomy on the
Quality of Life (QOL) versus Curability for Lung Cancer Surgery Hirokuni Yoshimura, MD Standard operations for lung cancer patients are generally accepted as performing lobectomy or pneumonectomy on the
Understanding surgery
 What does surgery for lung cancer involve? Surgery for lung cancer involves an operation, which aims to remove all the cancer from the lung. Who will carry out my operation? In the UK, we have cardio-thoracic
What does surgery for lung cancer involve? Surgery for lung cancer involves an operation, which aims to remove all the cancer from the lung. Who will carry out my operation? In the UK, we have cardio-thoracic
TWO CASES OF INTRALOBAR SEQUESTRATION OF THE LUNG
 Thorax (1955), 10, 73. TWO CASES OF INTRALOBAR SEQUESTRATION OF THE LUNG BY C. McDOWELL, DOUGLAS ROBB, AND J. S. INDYK From the Thoracic Unit, Green Lane Hospital, Auckland. N.Z. (RECEIVED FOR PUBLICATION
Thorax (1955), 10, 73. TWO CASES OF INTRALOBAR SEQUESTRATION OF THE LUNG BY C. McDOWELL, DOUGLAS ROBB, AND J. S. INDYK From the Thoracic Unit, Green Lane Hospital, Auckland. N.Z. (RECEIVED FOR PUBLICATION
mih.ocial solve more rapidly under their influence.
 Thorax (1957), 12, 329. A CRITICAL EXAMINATION OF THE ROLE OF StJRGERY IN THE TREATMENT OF PRIMARY PULMONARY TUBERCULOSIS IN CHILDREN BY J. K. CAMERON, J. D. HAY, AND L. J. TEMPLE From1 Leasowe Children's
Thorax (1957), 12, 329. A CRITICAL EXAMINATION OF THE ROLE OF StJRGERY IN THE TREATMENT OF PRIMARY PULMONARY TUBERCULOSIS IN CHILDREN BY J. K. CAMERON, J. D. HAY, AND L. J. TEMPLE From1 Leasowe Children's
A POSSIBLE CASE OF OEDEMATOUS FIBROMA WITH INFLAMMATORY CHANGES
 Thorax (1951), 6, 154. A POSSIBLE CASE OF OEDEMATOUS FIBROMA WITH INFLAMMATORY CHANGES BY VIGGO ESKELUND From the Institute of Pathological Anatomy, University of Copenhagen With the advances made in lung
Thorax (1951), 6, 154. A POSSIBLE CASE OF OEDEMATOUS FIBROMA WITH INFLAMMATORY CHANGES BY VIGGO ESKELUND From the Institute of Pathological Anatomy, University of Copenhagen With the advances made in lung
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
A Comparative Study of Video-Assisted Thoracic Surgery with Thoracotomy for Middle Lobe Syndrome
 World J Surg (2017) 41:780 784 DOI 10.1007/s00268-016-3777-6 ORIGINAL SCIENTIFIC REPORT A Comparative Study of Video-Assisted Thoracic Surgery with Thoracotomy for Middle Lobe Syndrome Jian Li 1,2 Chengwu
World J Surg (2017) 41:780 784 DOI 10.1007/s00268-016-3777-6 ORIGINAL SCIENTIFIC REPORT A Comparative Study of Video-Assisted Thoracic Surgery with Thoracotomy for Middle Lobe Syndrome Jian Li 1,2 Chengwu
FIBROMA OF THE VISCERAL PLEURA*
 Thorax (1953), 8, 180. FIBROMA OF THE VISCERAL PLEURA* BY SIR CLEMENT PRICE THOMAS AND C. E. DREW From the Brompton and Westminster Hospitals, London Intrathoracic fibromas are rare tumours, but as might
Thorax (1953), 8, 180. FIBROMA OF THE VISCERAL PLEURA* BY SIR CLEMENT PRICE THOMAS AND C. E. DREW From the Brompton and Westminster Hospitals, London Intrathoracic fibromas are rare tumours, but as might
Uniportal video-assisted thoracoscopic right upper posterior segmentectomy with systematic mediastinal lymphadenectomy
 Surgical Technique Uniportal video-assisted thoracoscopic right upper posterior segmentectomy with systematic mediastinal lymphadenectomy Guofei Zhang 1, Zhijun Wu 2, Yimin Wu 1, Gang Shen 1, Ying Chai
Surgical Technique Uniportal video-assisted thoracoscopic right upper posterior segmentectomy with systematic mediastinal lymphadenectomy Guofei Zhang 1, Zhijun Wu 2, Yimin Wu 1, Gang Shen 1, Ying Chai
Monitor Images for Respiratory System Dissection
 Monitor Images for Respiratory System Dissection **This document includes extra images of the radiology of the bronchopulmonary segments. These imaged are an excellent way to review the three-dimensional
Monitor Images for Respiratory System Dissection **This document includes extra images of the radiology of the bronchopulmonary segments. These imaged are an excellent way to review the three-dimensional
Thoracoplasty for the Management of Postpneumonectomy Empyema
 ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 9 Number 2 Thoracoplasty for the Management of Postpneumonectomy Empyema S Mullangi, G Diaz-Fuentes, S Khaneja Citation S Mullangi,
ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 9 Number 2 Thoracoplasty for the Management of Postpneumonectomy Empyema S Mullangi, G Diaz-Fuentes, S Khaneja Citation S Mullangi,
Anatomy of the Lungs. Dr. Gondo Gozali Department of anatomy
 Anatomy of the Lungs Dr. Gondo Gozali Department of anatomy 1 Pulmonary Function Ventilation and Respiration Ventilation is the movement of air in and out of the lungs Respiration is the process of gas
Anatomy of the Lungs Dr. Gondo Gozali Department of anatomy 1 Pulmonary Function Ventilation and Respiration Ventilation is the movement of air in and out of the lungs Respiration is the process of gas
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Pyopneumothorax in rheumatoid lung disease
 Thorax (1966), 21, 230. Pyopneumothorax in rheumatoid lung disease DEWI DAVIES From Ransom Hospital, Mansfield, Notts Rheumatoid nodules in the lung, in the absence of exposure to mineral dust, are uncommon.
Thorax (1966), 21, 230. Pyopneumothorax in rheumatoid lung disease DEWI DAVIES From Ransom Hospital, Mansfield, Notts Rheumatoid nodules in the lung, in the absence of exposure to mineral dust, are uncommon.
Thorax Lecture 2 Thoracic cavity.
 Thorax Lecture 2 Thoracic cavity. Spring 2016 Dr. Maher Hadidi, University of Jordan 1 Enclosed by the thoracic wall. Extends between (thoracic inlet) & (thoracic outlet). Thoracic inlet At root of the
Thorax Lecture 2 Thoracic cavity. Spring 2016 Dr. Maher Hadidi, University of Jordan 1 Enclosed by the thoracic wall. Extends between (thoracic inlet) & (thoracic outlet). Thoracic inlet At root of the
The posterolateral thoracotomy is still probably the
 Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
Thoracoscopic left upper lobectomy with systematic lymph nodes dissection under left pulmonary artery clamping
 GCTAB Column Thoracoscopic left upper lobectomy with systematic lymph nodes dissection under left pulmonary artery clamping Yi-Nan Dong, Nan Sun, Yi Ren, Liang Zhang, Ji-Jia Li, Yong-Yu Liu Department
GCTAB Column Thoracoscopic left upper lobectomy with systematic lymph nodes dissection under left pulmonary artery clamping Yi-Nan Dong, Nan Sun, Yi Ren, Liang Zhang, Ji-Jia Li, Yong-Yu Liu Department
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Mastering Thoracoscopic Upper Lobectomy
 Mastering Thoracoscopic Upper Lobectomy Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery, Duke University Medical
Mastering Thoracoscopic Upper Lobectomy Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery, Duke University Medical
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Wheezing, Bronchial Ulcers and Atelectasis
 Wheezing, Bronchial Ulcers and Atelectasis I. L. CUTLER, M.D.** Rutland, Massachusetts A very troublesome syndrome, namely, wheezing, bronchial ulcers, and atelectasis, when present in sanatorium patients,
Wheezing, Bronchial Ulcers and Atelectasis I. L. CUTLER, M.D.** Rutland, Massachusetts A very troublesome syndrome, namely, wheezing, bronchial ulcers, and atelectasis, when present in sanatorium patients,
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
bronchopleural fistula
 Role of automatic staplers in the aetiology of bronchopleural fistula MOHSIN HAKIM, BB MILSTEIN From the Department of Cardiothoracic Surgery, Papworth Hospital, Cambridge Thorax 1985;40:27-31 ABSTRACT
Role of automatic staplers in the aetiology of bronchopleural fistula MOHSIN HAKIM, BB MILSTEIN From the Department of Cardiothoracic Surgery, Papworth Hospital, Cambridge Thorax 1985;40:27-31 ABSTRACT
Thoracoscopy for Lung Cancer
 Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
CASE REPORTS. Idiopathic Unilateral Hyperlucent Lung
 CASE REPORTS Idiopathic Unilateral Hyperlucent Lung The Swyer-James Syndrome J. Judson McNamara, M.D., Harold C. Urschel, M.D., J. H. Arndt, M.D., Herman Ulevitch, M.D., and W. B. Kingsley, M.D. I diopathic
CASE REPORTS Idiopathic Unilateral Hyperlucent Lung The Swyer-James Syndrome J. Judson McNamara, M.D., Harold C. Urschel, M.D., J. H. Arndt, M.D., Herman Ulevitch, M.D., and W. B. Kingsley, M.D. I diopathic
FISTULAS AFTER LUNG RESECTION FOR PULMONARY TUBERCULOSIS
 Thorax (1951), 6, 397. THE SURGICAL TREATMENT OF BRONCHIAL FISTULAS AFTER LUNG RESECTION FOR PULMONARY TUBERCULOSIS BY OLIVIER MONOD, GEORGE BABOU, AND JEAN LO From the Hospital-Sanatorium, Chalons sur
Thorax (1951), 6, 397. THE SURGICAL TREATMENT OF BRONCHIAL FISTULAS AFTER LUNG RESECTION FOR PULMONARY TUBERCULOSIS BY OLIVIER MONOD, GEORGE BABOU, AND JEAN LO From the Hospital-Sanatorium, Chalons sur