A Critical Review of. Current Guidelines for Bipolar Disorder. R. Hamish McAllister-Williams, MD, PhD, MRCPsych
|
|
|
- Andrew Smith
- 5 years ago
- Views:
Transcription


1 A Critical Review of Psychobiology Research Group Current Guidelines for Bipolar Disorder R. Hamish McAllister-Williams, MD, PhD, MRCPsych Reader in Clinical Psychopharmacology University of Newcastle Hon. Consultant Psychiatrist Regional Affective Disorders Service, RVI
2 Remit: Guidelines Focus on: British Association of Psychopharmacology (BAP) Goodwin et al. 2003, J.Psychopharm. Compare with: American Psychiatric Association (APA) Texas Implementation of Medication Algorithms (TIMA) Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines NICE 2 nd draft bipolar guidelines
3 Remit: Patients and Treatments Bipolar I and II (and bipolar spectrum) Adults of working age Will not cover comorbidity and treatment in special situations (e.g. pregnancy) Focus on pharmacotherapy but will mention other treatment modalities
4 The course of Bipolar Disorder Mania Hypomania Euthymia Minor Depression Major Depression Preliminary Phase Preventative Phase
5 Guidelines BAP APA TIMA CANMAT NICE Acute mania Acute Depression Maintenance Agenda
6 Psychobiology Research Group Guidelines

7 BAP Guidelines for the Management of Bipolar Disorder G.M. Goodwin Evidenced based guidelines for treating bipolar disorder: recommendations from the BAP. J Psychopharmacology 17(2)
8 Methodology Meeting on 24 th May Brief presentations on key areas emphasis on systematic reviews and randomised controlled trials (RCTs). discussion to identify consensus and uncertainty Review and recommendations circulated to participants (2 iterations, Nov, 2002, Feb 2003). Feedback as far as possible incorporated into the final version of the guidelines (Feb 2003)
9 Guidelines The principle recommendations usually apply to the average patient. Recommendations may be expected to apply about 70% of the time so we have used expressions like Clinicians should consider.. However, there will be occasions when adhering to such a recommendation unthinkingly could do more harm than good.
10 STRENGTH OF EVIDENCE AND RECOMMENDATIONS TREATMENT Ia: meta-analysis of RCTs Ib: at least one RCT IIa-b: at least one controlled or exptl. study (no R) III: descriptive studies IV: expert committee reports, opinions and/or clinical experience OBSERVATIONAL I: large representative population samples II: small, limited samples III: non-representative surveys, case reports IV: expert committee reports, opinions and/or clinical experience
11 Outline Guidelines Fundamentals of patient management Diagnosis Access to services and the safety of the patient and others Enhanced care Treatment of different phases of bipolar illness Acute Manic or Mixed Episodes Acute Depressive episode Long-term treatment Treatment in special situations Review Appendix

12 Practice Guidelines for the Treatment of Patients with Bipolar Disorder Hirschfeld et al., Am. J. Psychiatry 2002
13 Methodology Developed by psychiatrists who are active in clinical practice Some contributors primarily involved in research or other academic activities Issues re conflicts of interest Extensively reviewed by members of APA Objective evaluation of evidence C.of I. notified to APA Dept. of Quality Improvement and Psychiatric Services and discussed with work group chair and chair of Steering Committee on Practice Guidelines Multiple drafts and widespread review Approval by the APA Assembly and Board of Trustees
14 Guidelines These parameters of practice should be considered guidelines only. Adherence to them will not ensure a successful outcome in every case. The ultimate judgement regarding a particular clinical procedure or treatment plan must be made by the psychiatrist
15 STRENGTH OF EVIDENCE AND RECOMMENDATIONS I: Recommendation with substantial clinical confidence II: Recommendation with moderate clinical confidence III: May be recommended on the basis of individual circumstances
 guidelines for the management of patients")

16 Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: consensus and controversies Yatham et al Bipolar Disorders 7(suppl. 3) 5-69
17 Methodology Update of guidelines published in 1997 Little information regarding methodology Guideline Committee, Section Leaders and Co- Chairs (Yatham & Kennedy) identified Invited experts from outside Canada to comment Supported by an unrestricted educational grant from Lilly, AstraZeneca and Janssen-Ortho Modified criteria for rating strength of evidence Produced treatment algorithms
18 Evidence criteria and strength of recommendations Evidence Criteria 1. Meta-analysis or replicated double-blind RCT (DBRCT) that includes placebo 2. At least one DBRCT with placebo or active comparator 3. Prospective uncontrolled trial with 10+ subjects 4. Anecdotal reports or expert opinion Treatment recommendations First line level 1 or 2 evidence plus clinical support for efficacy and safety Second line Level 3 or higher evidence plus clinical support for efficacy and safety Third line - Level 4 or higher evidence plus clinical support for efficacy and safety Not recommended Level 1 or 2 evidence for lack of efficacy

19 The Texas Implementation of Medication Algorithms (TIMA): Update to the algorithms for treatment of bipolar I disorder Suppes et al J. Clin. Psychiatry 66:
20 Methodology Texas expert consensus panel Updating previous algorithms published in day meeting with bipolar experts, pharmacists, community and inpatient physicians, advocates and consumers Reviewed data presented at meetings as well as that published in peer review journals No industry support, individuals declarations of interest made in the publication
21 Strength of Evidence A randomised, blind, placebo-controlled trials B open, controlled trials, large case series, large retrospective analyses C preliminary but unconfirmed findings, case reports and series, expert consensus Algorithms based on quantity and quality of data of efficacy and effectiveness, expert opinion, consumer input and safety and tolerability issues
22 NICE Clinical Guideline Second Draft, Feb 2006 Bipolar Disorder: The management of bipolar disorder in adults, children and adolescents, in primary and secondary care
23 Methodology Funded by NICE 23 member Guideline Development Group Convened by the National Collaborating Centre for Mental Health (RCPsych CRTU and BPS equivalent) Chair Nicol Ferrier Psychiatrists (adult and CAMS), Psychologists, Pharmacists, OT, Nurses, Users and Carers, Reviewers and Economists Special Advisors consulted 2 drafts sent to stakeholders for comments (Nov 2005, Feb 2006) Final version due July 2006 N.B. multiple versions (2 nd draft: 77 and 341 pages)
24 NICE Guidelines Full guideline 341 pages 10 pages of contents comprehensive guidelines! 25 pages of methodology thorough / obsessional guidelines!

25 NICE Review Process
26 Nature of NICE guidelines Guidelines are systematically developed statements that assist clinicians and patients in making decisions about appropriate treatment for specific conditions (DOH 1996) From best available evidence reviewed using predetermined and systematic methods This guideline does not.the individual responsibility of health care professionals to make appropriate decisions in the circumstances of the individual patient, in consultation with the patient and/or carer. In addition to clinical evidence, cost effectiveness also taken into account
27 NICE Strength of Recommendations
28 Psychobiology Research Group Acute Mania
29 Acute Manic or Mixed Episodes For patients not already on long term treatment for bipolar disorder* Initiate oral administration of an (atypical) antipsychotic or valproate (A) The lowest doses necessary should be employed (A). Do not escalate the dose of antipsychotic simply to obtain a sedative effect (S). For less ill manic patients lithium or carbamazepine may be considered as a short term treatment (A). To promote sleep consider adjunctive benzodiazepine (B) Antidepressants should be tapered and stopped (B) Treatment choice guided by patient preference (S)
30 Acute Manic or Mixed Episodes For patients who suffer an episode while on long term treatment: Ensure highest well-tolerated dose / lithium in therapeutic range (A) Start antipsychotic or valproate as above Use same principles as above Consider if current episode is due to poor adherence Consider more tolerable regimen If episode due to lithium discontinuation, use of lithium may not be indicated (B)
31 Acute Manic or Mixed Episodes If symptoms uncontrolled and/or mania is very severe Add another first-line medicine. Consider the combination of lithium or valproate with an antipsychotic (A). Consider clozapine in more refractory illness (B). ECT may be considered for manic patients who are severely ill and/or whose mania is treatment resistant and patients with severe mania during pregnancy (C).
32 Acute Mania First line Li + antipsychotic or Valproate + antipsychotic [I] Less severe, Li, valproate or antipsychotic [I] Otherwise almost exactly the same as BAP guidelines
33 Acute treatment of mania
34
35 Acute Mania: Those not on anti-manic treatment Atypical antipsychotic (olanzapine, risperidone, quetiapine) for those with severe mania If ineffective consider adding Li or valproate Valproate or Li if previous good response and compliance Avoid valproate in women of child baring potential Li only if less severe Don t use carbamazepine routinely and avoid gabapentin, lamotrigine and topiramte
36 Acute Mania: Those on anti-manic treatment Optimise treatment Li level Valproate to max. licensed dose (depending on SEs) Don t generally increase carbamazepine Add olanzapine, risperidone or quetiapine
37 Acute Mania: Summary Fair degree of consensus: Li, valproate and atypicals all considered first line treatments BAP argue Li only for less severe mania NICE suggest atypicals main choice (N.B. beware valproate in women) TIMA express concern re olanzapine APA tends to be aggressive and go for combination treatment early
38 Psychobiology Research Group Acute Depression
39 Depression is THE Problem Bipolar I (Judd et al. Archives of General Psychiatry 59: , 2002) Asymptomatic 53% Symptomatic 47% Depressed 67% Manic/ hypomanic 20% Mixed 13% Bipolar II (Judd LL et al. Archives of General Psychiatry 60: , 2003) Asymptomatic 46% Symptomatic 54% Depressed 94% Hypomanic 2% Mixed 4%
40 Bipolar Depressive and Mixed Episodes are Difficult to Treat 0.0 Cumulative Proportion of Patients Remitted Mixed/cycling (n = 35) Depressed (n = 79) * ** Weeks of Preliminary Phase Treatment *p < vs Manic; **p<.0001 vs Manic and p < 0.05 vs Dep Kupfer DJ et al. Acta Neuropsychiatrica 12: , 2000 Manic (n = 37)
41 Acute Depression For patients not already on long-term treatment for bipolar disorder Treat with an antidepressant (e.g. SSRI) and an antimanic drug (e.g. lithium, valproate or an antipsychotic) together (B). Antidepressant monotherapy is not recommended for patients with a history of mania (B). Consider adding antipsychotic especially if psychotic symptoms present (A) Consider ECT for patients with high suicidal risk, psychosis, severe depression during pregnancy or lifethreatening inanition (A).
42 Acute Depression For patients who suffer a depressive episode while on long term treatment Optimize doses of medicines and serum levels of lithium (B). Address current stressors, if any (B). Ensure current long-term treatment will prevent manic relapse (e.g. lithium, valproate, antipsychotic) (A). If the patient fails to respond to optimization of long-term treatment, and especially if depressive symptoms are significant, initiate an antidepressant (or consider augmentation or change of antidepressant) (A).
43 Acute Depression Choice of antidepressant Antidepressants work in bipolar disorder (Ia) There is a risk of switch to mania or mood instability during treatment for depression (I). Antidepressants less likely to induce mania when added to lithium, valproate or antipsychotic (IIa). Tricyclic antidepressants more likely (Ia) and not recommended except for treatment resistant patients (C). Consider lamotrigine, esp. if an antidepressant has previously appeared to provoke mood instability (A).
44 Acute depression Start either lithium [I] or lamotrigine [II] If on long term treatment optimise this [II] Don t use antidepressant monotherapy Consider Li + antidepressant [III] Consider ECT [I] If fails first line therapy consider adding lamotrigine [I], buproprion [II] or paroxetine [II] Alternatives: another SSRI [II], venlafaxine [II] or an MAOI [II]
45 Acute treatment of depression
46
47 Acute Depression First line: SSRI plus antimanic agent If on antimanic: SSRI or quetiapine (if not on antipsychotic) If recent unstable mood: avoid antidepressants increase antimanic and consider lamotrigine NB avoid lamotrigine as a single first line agent in bipolar I but consider this in bipolar II If doesn t respond to SSRI switch to mirtazepine or venlafaxine or add quetiapine or olanzapine if not on an antipsychotic Taper antidepressants after symptoms reduced for 8 weeks
48 Acute Depression: Summary Much less consensus: Don t use antidepressant monotherapy esp. in bipolar I BAP use SSRIs and not TCAs APA, CANMAT and TIMA: increased use of lamotrigine and buproprion CANMAT, TIMA and NICE: increased use of quetiapine
49 Psychobiology Research Group Maintenance
50 What is a Mood Stabiliser Treats depression plus mania without making either pole worse and/or has prophylactic effects for both mania and depression BAP: An ideal mood stabilizer would prevent relapse to either pole of the illness actually more effective against one pole than the other APA and CANMAT: Absence of a consensus definition NICE A term best avoided
51 Manic Syndrome Manic Syndrome Acute Continuation/Maintenance Manic Symptoms Relapse Recurrence Remission Euthymia Depressive Symptoms Relapse Recurrence Depressive Syndrome Response
52 Relationship between cycle length and number of episodes Cycle Length (Months) Kraepelin, 1921 Zis et al, 1980 Angst, 1981 Roy-Byrne et al, Episode
53 Mood Disorders: Risk of relapse Bipolar Disorder, constant risk of relapse over 40yrs; 0.4episodes/year Angst et al. Eur Arch Psychiatry Clin Neurosci. 2003
54 Long-term treatment: Why? High risk of recurrence (Ia) Preventing early relapse may lead to a more benign illness course (D) High frequency of chronic sub-threshold symptoms (most commonly depressive) (II) Cognitive distortions similar to unipolar illness (II) Neuropsychological deficits can be disabling and often neglected (II)

55 Beyond Symptomatic Control? Moorel et al Lancet 2000
56 Long-term treatment: When? Prevention of new episodes Consider long term treatment after a single manic episode or as early as acceptable to patient and their family (D). Need active acceptance of need for long-term treatment: Consider a wider package of treatment offering enhanced psychological and social support (A). Where a patient has done very well, they should be strongly advised to continue indefinitely, because the risks of relapse remain high (A). Consider extrapolating above for Bipolar I to II despite absence of good clinical trials (D)
57 Long-term treatment: How? Options for long-term treatment Continuous rather than intermittent therapy Short term add-ons (e.g. benzos, atypicals) when stressors present or early signs of relapse (esp. sleep disturbance) Consider supplying treatment prospectively to patients (D) Increases dose may sometimes be an alternative to addons May help patients comply with their treatment regime
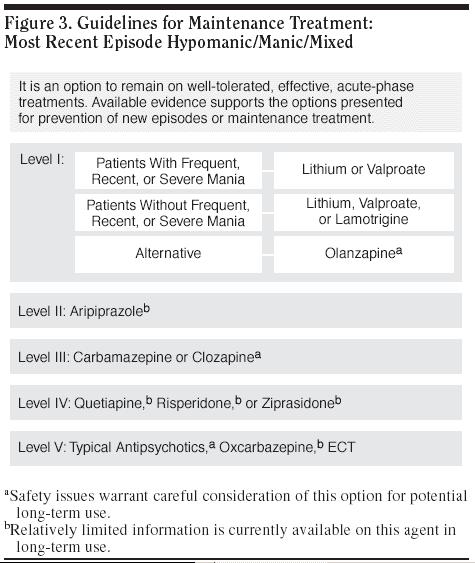
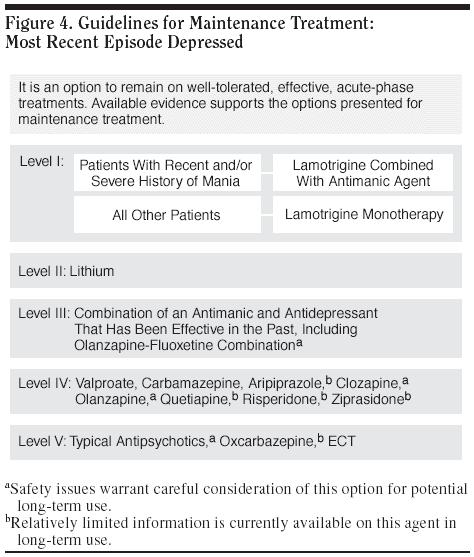
58 Long-term treatment: What? Choice of long-term treatments Consider lithium monotherapy (A) Lithium protects against both mania and depression, but is more effective at preventing mania (Ia) Long term treatment with lithium decreases the risk of suicide (I) If lithium ineffective or poorly tolerated Valproate protects against mania (and depression) (Ia) Olanzapine protects against mania (and depression) (Ia) Carbamazepine is less effective than lithium (Ib) but may be used especially in non-classical illness (B). Oxcarbazepine has fewer pharmacokinetic interactions Lamotrigine protects against depression (? and mania) (Ia) Gabapentin ineffective (Ib) Acute response to an agent favours its use long term (B)
59 Long-term treatment: Non-response If the patient fails monotherapy Consider long term combination treatment (C). Where the burden is mania, combine predominantly antimanic agents (e.g. lithium, valproate, an antipsychotic) (D). Where the burden is depressive, lamotrigine or an antidepressant may be more appropriate in combination with an anti-manic long-term agent (D). Maintenance ECT if respond acutely and do badly on oral treatments (D) Consider clozapine in treatment resistant patients (C).
60 Long-term treatment: Rapid cycling Rapid cycling Identify and treat hypothyroidism or substance misuse that may contribute (C) Taper and discontinue antidepressants (C) For initial treatment consider lithium, valproate or lamotrigine (A) Combinations often required. Evaluate over 6 months or more. Discontinue ineffective treatments (D)
61 Long-term treatment: Stopping Discontinuation of long term treatment Following discontinuation of medicines, the risk of relapse remains, even after years of sustained remission (I). Discontinuation of any medicine should normally be tapered over at least 2 weeks and preferably longer (A and S). Early relapse to mania is an early risk of abrupt lithium discontinuation (Ia). Discontinuation of medicines should not be equated with withdrawal of services to patients (S).
62 Long-term treatment Maintenance recommended after a single manic episode [I] Consideration of similar maintenance therapy in bipolar II strongly warranted [II]
63 Long-term treatment: Key differences from BAP guidelines If antipsychotic used for the acute episode its ongoing use should be reviewed at the maintenance phase [I] Discontinue antipsychotics unless: Required for control of, or persistent, psychosis [I] Prophylaxis against recurrence [III] Consider atypicals for maintenance [III] but no definitive evidence as effective as lithium or valproate
64 Maintenance therapy: when? At least one moderately severe manic episode If refuse Psychoeducation Continue acute treatments for at least 3-6 months (Antidepressants after 1-3 months)
65 Maintenance choice of treatment Lithium Best evidence base Antisuicidal effects Treatment of choice for typical bipolar disorder Olanzapine and divalproex More suitable for patients with manic relapses Lamotrigine Mainly for preventing depressive relapses Avoid monotherapy if history of severe or frequent mania
66 Maintenance pharmacotherapy of bipolar disorder First line Lithium (1), lamotrigine (if only mild mania ; 1/2), divalproex (2), olanzapine (2) Second Line Carbamazepine (2), Li+DVP (2), Li+CBZ (2), Li or DVP+olanz (2), aripirazole (2*), risperidone (3), quetiapine (3), ziprasidone (?), Li+risp or quet (?), Li+lam or SSRI or buproprion (?) Third Line Adjunctive phenytoin (3), clozapine (3), ECT (3), topiramate (3), gabapentin (3), omega-3-fatty acids (2), oxcarbazepine (3) Not Recommended Benzodiazepines, adjunctive flupenthixol, monotherapy with gabapentin, topiramate, antidepressants
67 Maintenance Different algorithms depending on polarity of most recent episode Much more info re treatment following elevated mood episode Maintenance for those stabilised on acute treatment continuation of acute phase treatment followed by simplification of treatment regimes Medication changes often made on the basis of subsyndromal symptoms In clinical practice most patients on combinations but evidence base focused on single treatments
68
69
70 Other issues Rapid cycling No specific recommendations Often need combinations Bipolar II Clinical considerations coincide with those for bipolar I Evidence for lithium, lamotrigine, valproate and antidepressant monotherapy
71 Long-term Treatment: When? Single manic episode with significant risk/consequences 2+ episodes in bipolar I In bipolar II if: Significant risk Frequent episodes Significant functional impairment
72 Long-term Treatment: What? First line: an atypical antipsychotic Same one used in acute phase or olanzapine Second Line: Valproate esp. if prone to depressive Sx, but N.B. women of child baring potential Lithium If fails monotherapy over 6 months Li + valp, Li + olanz, Valp + olanz If combination fails Consider lamotrigine (esp. BPII), carbamazepine, referral to tertiary centre NOT antidepressants routinely (unless no mania X 5 yrs) Normally treat for at least 5 years
73 Rapid Cycling First line: Li + valproate Second line: Li Avoid antidepressants Consider Li or valproate + lamotrigine (esp in BPII) Check TFTs (+ antibodies) every 6 months
74 Maintenance: Summary Shifts in recommendations evident from APA to NICE Increased recommendations for use of atypicals Increased caution recommended re use of antidepressants NICE emphasise the need for physical health monitoring
75 Finally. Shift of olanzapine to stage 1B in TIMA represents acknowledgement that efficacy not the only consideration Singling out olanzapine may be premature Acute phase recommendations increasingly being driven by maintenance considerations Guidelines limited by evidence base (esp. maintenance) Outstanding issues: Is combination of atypical plus mood stabiliser better than atypical alone? What is the optimal combination for maintenance? How to balance efficacy with tolerability and safety (esp. for maintenance)?
76 The course of Bipolar Disorder Mania Hypomania Euthymia Minor Depression Major Depression Preliminary Phase Frank E, et al. Biol Psychiatry. 2000;48(6): Preventative Phase
77 The study of MEDICINE is prosecuted under two relations, namely as a Science and as an Art The Science and Practice of Medicine W. Aitken 1872
The Pharmacological Management of Bipolar Disorder: An Update
 Psychobiology Research Group The Pharmacological Management of Bipolar Disorder: An Update R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon.
Psychobiology Research Group The Pharmacological Management of Bipolar Disorder: An Update R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon.
What s new in the treatment of bipolar disorder?
 What s new in the treatment of bipolar disorder? Dr. David Cousins MRC Clinician Scientist Institute of Neuroscience Newcastle University NCMD 2017 What s new in the treatment of bipolar disorder? Dr.
What s new in the treatment of bipolar disorder? Dr. David Cousins MRC Clinician Scientist Institute of Neuroscience Newcastle University NCMD 2017 What s new in the treatment of bipolar disorder? Dr.
Clinical Guideline for the Management of Bipolar Disorder in Adults
 Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Psychopharmacology. Psychopharmacology. Hamish McAllister-Williams Reader in Clinical. Department of Psychiatry, RVI
 Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Your footnote
 MANIA Your footnote Your footnote Cipriani A, Barbui C, Salanti G et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis. The Lancet 2011;
MANIA Your footnote Your footnote Cipriani A, Barbui C, Salanti G et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis. The Lancet 2011;
Practical Guide to Long-Term Pharmacotherapy in Bipolar Disorder: An Updated Synthesis of Current Clinical Guidelines
 SECOND-GENERATION ANTIPSYCHOTICS IN BIPOLAR DISORDER Practical Guide to Long-Term Pharmacotherapy in Bipolar Disorder: An Updated Synthesis of Current s Flavio Guzman, MD Editor Psychopharmacology Institute
SECOND-GENERATION ANTIPSYCHOTICS IN BIPOLAR DISORDER Practical Guide to Long-Term Pharmacotherapy in Bipolar Disorder: An Updated Synthesis of Current s Flavio Guzman, MD Editor Psychopharmacology Institute
How to treat depression with medication: Some rules of thumb
 How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
PDF created with pdffactory Pro trial version
 با ی د ر ا ر وه روا ز ش ی دا ه ع وم ش ی ا ان Treatment Challenges in BD Major depressive episode Mixed states= 20% Rapid cycling= 18% (annually), 31.5% (lifetime) Psychiatric Comorbidity (substance abuse,
با ی د ر ا ر وه روا ز ش ی دا ه ع وم ش ی ا ان Treatment Challenges in BD Major depressive episode Mixed states= 20% Rapid cycling= 18% (annually), 31.5% (lifetime) Psychiatric Comorbidity (substance abuse,
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care
 Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Multistate Outcome Analysis of Treatment MOAT
 Multistate Outcome Analysis of Treatment MOAT Charles L. Bowden, M.D. Presented with Fond Memories of an Outstanding Statistician and Investigative Scientist Andy Leon Design contributors to low generalizability
Multistate Outcome Analysis of Treatment MOAT Charles L. Bowden, M.D. Presented with Fond Memories of an Outstanding Statistician and Investigative Scientist Andy Leon Design contributors to low generalizability
Resubmission. Scottish Medicines Consortium
 Scottish Medicines Consortium Resubmission aripiprazole 5mg, 10mg, 15mg, 0mg tablets; 10mg, 15mg orodispersible tablets; 1mg/mL oral solution (Abilify ) No. (498/08) Bristol-Myers Squibb Pharmaceuticals
Scottish Medicines Consortium Resubmission aripiprazole 5mg, 10mg, 15mg, 0mg tablets; 10mg, 15mg orodispersible tablets; 1mg/mL oral solution (Abilify ) No. (498/08) Bristol-Myers Squibb Pharmaceuticals
Formulary and Prescribing Guidelines
 Formulary and Prescribing Guidelines SECTION 3: TREATMENT OF BIPOLAR AFFECTIVE DISORDER This section provides information regarding the pharmacological management of Bipolar affective disorder in secondary
Formulary and Prescribing Guidelines SECTION 3: TREATMENT OF BIPOLAR AFFECTIVE DISORDER This section provides information regarding the pharmacological management of Bipolar affective disorder in secondary
Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents
 BadgerCare Plus Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice
BadgerCare Plus Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice
Prescribing medications for people with a personality disorder A service evaluation of a community mental health team
 Prescribing medications for people with a personality disorder A service evaluation of a community mental health team Dr Umama Khan, Consultant Psychiatrist Dr Venkatesh Ballagere, Specialist Registrar
Prescribing medications for people with a personality disorder A service evaluation of a community mental health team Dr Umama Khan, Consultant Psychiatrist Dr Venkatesh Ballagere, Specialist Registrar
CHAIR SUMMIT 7TH ANNUAL #CHAIR2014. Master Class for Neuroscience Professional Development. September 11 13, Westin Tampa Harbour Island
 #CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Bipolar Depression: Putting the End Goal
#CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Bipolar Depression: Putting the End Goal
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Kelly Godecke, MD Department of Psychiatry University of Utah
 Kelly Godecke, MD Department of Psychiatry University of Utah Epidemiology and Impact -module 2 session 1 overview of mood disorders Diagnostic Criteria of Bipolar Disorders Medications Used in Bipolar
Kelly Godecke, MD Department of Psychiatry University of Utah Epidemiology and Impact -module 2 session 1 overview of mood disorders Diagnostic Criteria of Bipolar Disorders Medications Used in Bipolar
Is there consensus across international evidence-based guidelines for the management of bipolar disorder?
 Acta Psychiatr Scand 2017: 135: 515 526 All rights reserved DOI: 10.1111/acps.12717 2017 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd ACTA PSYCHIATRICA SCANDINAVICA Review Is there consensus
Acta Psychiatr Scand 2017: 135: 515 526 All rights reserved DOI: 10.1111/acps.12717 2017 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd ACTA PSYCHIATRICA SCANDINAVICA Review Is there consensus
Challenges in identifying and treating bipolar depression: a guide
 Challenges in identifying and treating bipolar depression: a guide Dr. Paul Stokes Clinical Senior Lecturer, Centre for Affective Disorders, Department of Psychological Medicine Overview Challenges in
Challenges in identifying and treating bipolar depression: a guide Dr. Paul Stokes Clinical Senior Lecturer, Centre for Affective Disorders, Department of Psychological Medicine Overview Challenges in
Treatment of Bipolar disorder
 8/6/215 Treatment of Bipolar disorder Pichai Ittasakul, M.D. Department of Psychiatry, Ramathibodi Hospital, Mahidol University Bipolar disorder Manic-depressive Illness. is characterized by the occurrence
8/6/215 Treatment of Bipolar disorder Pichai Ittasakul, M.D. Department of Psychiatry, Ramathibodi Hospital, Mahidol University Bipolar disorder Manic-depressive Illness. is characterized by the occurrence
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 05 May 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 05 May 2010 LAMICTAL 2 mg, dispersible / chewable tablet B/30 (CIP: 354 581-7) LAMICTAL 5 mg, dispersible / chewable
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 05 May 2010 LAMICTAL 2 mg, dispersible / chewable tablet B/30 (CIP: 354 581-7) LAMICTAL 5 mg, dispersible / chewable
Management of Bipolar Depression
 Management of Bipolar Depression Haresh M. Tharwani, M.D. Associate Clinical Professor Medical Director-DRH & Duke Psychiatry Specialty Clinic of Cary, N.C. Bipolar Disorders (Manic-Depressive illness)
Management of Bipolar Depression Haresh M. Tharwani, M.D. Associate Clinical Professor Medical Director-DRH & Duke Psychiatry Specialty Clinic of Cary, N.C. Bipolar Disorders (Manic-Depressive illness)
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]
![SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]](/thumbs/80/80440271.jpg "SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]") SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
Mixing and Matching: Layering Medications as Family Physicians
 Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Are they still doing that?
 Are they still doing that? Why we still give ECT and when to refer Nicol Ferrier BSc (Hons), MD, FRCP(Ed), FRCPsych Emeritus Professor of Psychiatry Newcastle University Rates of prescribing ECT in the
Are they still doing that? Why we still give ECT and when to refer Nicol Ferrier BSc (Hons), MD, FRCP(Ed), FRCPsych Emeritus Professor of Psychiatry Newcastle University Rates of prescribing ECT in the
Pregnancy. General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition)
") Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Bipolar Disorders. Disclosure Statement. I have no financial disclosures or conflicts of interest
 Bipolar Disorders Ahsan Naseem, MD Diplomate American Board of Psychiatry and Neurology Adult and Geriatric Psychiatry Medical Director Bryan Heartland Psychiatry Bryan Physician Network Partner Cheney
Bipolar Disorders Ahsan Naseem, MD Diplomate American Board of Psychiatry and Neurology Adult and Geriatric Psychiatry Medical Director Bryan Heartland Psychiatry Bryan Physician Network Partner Cheney
PRESCRIBING GUIDELINES
 The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES. MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) KEY ISSUES
 KEY ISSUES") MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
Bipolar Disorder in Youth
 Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital Pediatric-Onset
Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital Pediatric-Onset
Mental Health Pathway
 Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
Affective Disorders.
 Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
It's Cycling, Not Polarity Understanding and Diagnosing the Bipolar Spectrum
 It's Cycling, Not Polarity Understanding and Diagnosing the Bipolar Spectrum Session 4022: American Psychiatric Nurses Association National Conference, Louisville, KY Andrew Penn, RN, MS, NP, CNS Psychiatric
It's Cycling, Not Polarity Understanding and Diagnosing the Bipolar Spectrum Session 4022: American Psychiatric Nurses Association National Conference, Louisville, KY Andrew Penn, RN, MS, NP, CNS Psychiatric
PORT, 2009 Spain, 2009 Malaysia, 2009 Singapore, 2009 BAP, 2011 WFSBP, 2012 SIGN, 2013 Harvard NICE RANZCP, 2016
 Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Antipsychotics in Bipolar
 Use of Second-Generation Antipsychotics in Bipolar Disorder: A Practical Guide Flavio Guzman, MD Editor Psychopharmacology Institute This practical guide is an update on the use of second-generation antipsychotics
Use of Second-Generation Antipsychotics in Bipolar Disorder: A Practical Guide Flavio Guzman, MD Editor Psychopharmacology Institute This practical guide is an update on the use of second-generation antipsychotics
Document Title Pharmacological Management of Generalised Anxiety Disorder
 Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Mood Disorders and Addictions: A shared biology?
 Mood Disorders and Addictions: A shared biology? Dr. Paul Stokes Clinical Senior Lecturer, Centre for Affective Disorders, Department of Psychological Medicine Disclosures No relevant disclosures: No paid
Mood Disorders and Addictions: A shared biology? Dr. Paul Stokes Clinical Senior Lecturer, Centre for Affective Disorders, Department of Psychological Medicine Disclosures No relevant disclosures: No paid
Lithium in bipolar disorders.
 Lithium in bipolar disorders. S. Mehdi Samimi Ardestani M.D. Department of Psychiatry, Shahid Beheshti University of Medical Science, Behavioral science research center Iranian psychiatric association,
Lithium in bipolar disorders. S. Mehdi Samimi Ardestani M.D. Department of Psychiatry, Shahid Beheshti University of Medical Science, Behavioral science research center Iranian psychiatric association,
Improving the Recognition and Treatment of Bipolar Depression
 Handout for the Neuroscience Education Institute (NEI) online activity: Improving the Recognition and Treatment of Bipolar Depression Learning Objectives Apply evidence-based tools that aid in differentiating
Handout for the Neuroscience Education Institute (NEI) online activity: Improving the Recognition and Treatment of Bipolar Depression Learning Objectives Apply evidence-based tools that aid in differentiating
DISEASES AND DISORDERS
 DISEASES AND DISORDERS 13. The mood (affective) disorders 99 14. The psychotic disorders: schizophrenia 105 15. The anxiety and somatoform disorders 111 16. Dementia and delirium 117 17. Alcohol and substance-related
DISEASES AND DISORDERS 13. The mood (affective) disorders 99 14. The psychotic disorders: schizophrenia 105 15. The anxiety and somatoform disorders 111 16. Dementia and delirium 117 17. Alcohol and substance-related
asenapine 5mg, 10mg sublingual tablet (Sycrest ) SMC No. (762/12) Lundbeck Ltd
 SMC No. (762/12) Lundbeck Ltd") asenapine 5mg, 10mg sublingual tablet (Sycrest ) SMC No. (762/12) Lundbeck Ltd 10 February 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
asenapine 5mg, 10mg sublingual tablet (Sycrest ) SMC No. (762/12) Lundbeck Ltd 10 February 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
Comparison of the Usefulness of Lithium and Valproate
 Review Article CNPT4(2013) 1-5 Comparison of the Usefulness of Lithium and Valproate, M.D., Ph.D. Department of Neuropsychiatry, Oita University Faculty of Medicine ABSTRACT This review shows that lithium
Review Article CNPT4(2013) 1-5 Comparison of the Usefulness of Lithium and Valproate, M.D., Ph.D. Department of Neuropsychiatry, Oita University Faculty of Medicine ABSTRACT This review shows that lithium
Approach to Bipolar Disorder Family Medicine Forum November 14 17, 2018 Toronto, Ontario
 Approach to Bipolar Disorder Family Medicine Forum November 14 17, 2018 Toronto, Ontario Jon Davine, MD, CCFP, FRCP(C) Associate Professor, McMaster University Faculty/Presenter Disclosure Faculty: Dr.
Approach to Bipolar Disorder Family Medicine Forum November 14 17, 2018 Toronto, Ontario Jon Davine, MD, CCFP, FRCP(C) Associate Professor, McMaster University Faculty/Presenter Disclosure Faculty: Dr.
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A
 Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
The treatment of bipolar disorder in adults, children and adolescents
 DRAFT FOR CONSULTATION The treatment of bipolar disorder in adults, children and adolescents The paragraphs in the draft are numbered for the purposes of consultation. The final version will not contain
DRAFT FOR CONSULTATION The treatment of bipolar disorder in adults, children and adolescents The paragraphs in the draft are numbered for the purposes of consultation. The final version will not contain
BIPOLAR DISORDERS DIAGNOSTIC AND TREATMENT ISSUES RICHARD RIES MD
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences BIPOLAR DISORDERS DIAGNOSTIC AND TREATMENT ISSUES RICHARD RIES MD PROFESSOR DEPARTMENT OF PSYCHIATRY UNIVERSITY
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences BIPOLAR DISORDERS DIAGNOSTIC AND TREATMENT ISSUES RICHARD RIES MD PROFESSOR DEPARTMENT OF PSYCHIATRY UNIVERSITY
Volume 4; Number 5 May 2010
 Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Florida Best Practice Medication Guidelines Principles of Practice for Adults
 http://flmedicaidbh.fmhi.usf.edu Florida Best Practice Medication Guidelines Principles of Practice for Adults 1. Goal of the Guidelines Persistent gaps exist in the quality of mental health care delivered
http://flmedicaidbh.fmhi.usf.edu Florida Best Practice Medication Guidelines Principles of Practice for Adults 1. Goal of the Guidelines Persistent gaps exist in the quality of mental health care delivered
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Single Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Single Technology Appraisal Aripiprazole for the treatment and prevention of acute manic and mixed episodes in bipolar disorder in children and adolescents
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Single Technology Appraisal Aripiprazole for the treatment and prevention of acute manic and mixed episodes in bipolar disorder in children and adolescents
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder,
 Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A
 Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Pharmacy Prior Authorization GMH/SA and Non-Title 19/21 SMI Non-Formulary and Prior Authorization Guidelines
 Non-Formulary Behavioral Health Medications ADHD medications for children under The patient must have a diagnosis for which the requested medication is: o Approved based on FDA indication and limits; OR
Non-Formulary Behavioral Health Medications ADHD medications for children under The patient must have a diagnosis for which the requested medication is: o Approved based on FDA indication and limits; OR
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Professor Tony Holland, Department of Psychiatry, University of Cambridge
 INFORMATION SHEET The Use of Medication for Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction Challenging behaviours displayed by people with
INFORMATION SHEET The Use of Medication for Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction Challenging behaviours displayed by people with
Medication for Anxiety and Depression. PJ Cowen Department of Psychiatry, University of Oxford
 Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
As we have seen, bipolar disorder is a
 LONG-TERM MOOD STABILIZATION: PHARMACOLOGIC TREATMENT STRATEGIES * Susan Simmons-Alling, MSN, APRN, BC ABSTRACT This article focuses primarily on the pharmacologic strategies recommended for bipolar disorder.
LONG-TERM MOOD STABILIZATION: PHARMACOLOGIC TREATMENT STRATEGIES * Susan Simmons-Alling, MSN, APRN, BC ABSTRACT This article focuses primarily on the pharmacologic strategies recommended for bipolar disorder.
Bipolar Disorder 4/6/2014. Bipolar Disorder. Symptoms of Depression. Mania. Depression
 Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
A systematic review of the evidence on the treatment of rapid cycling bipolar disorder
 Bipolar Disorders 2013: 15: 115 137 Review Article Ó 2013 John Wiley and Sons A/S Published by Blackwell Publishing Ltd. BIPOLAR DISORDERS A systematic review of the evidence on the treatment of rapid
Bipolar Disorders 2013: 15: 115 137 Review Article Ó 2013 John Wiley and Sons A/S Published by Blackwell Publishing Ltd. BIPOLAR DISORDERS A systematic review of the evidence on the treatment of rapid
CME Article Ministry of Health Clinical Practice Guidelines: Bipolar Disorder
 Clinical Practice Guidelines Singapore Med J 2011; 52(12) : 914 CME rticle Ministry of Health Clinical Practice Guidelines: Bipolar Disorder Mok Y M, Chan H N, Chee K S, Chua T E, Lim B L, Marziyana R,
Clinical Practice Guidelines Singapore Med J 2011; 52(12) : 914 CME rticle Ministry of Health Clinical Practice Guidelines: Bipolar Disorder Mok Y M, Chan H N, Chee K S, Chua T E, Lim B L, Marziyana R,
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
35-year-old woman with Hx of BPII Dx; currently separated from husband; has 1 child
 Stephen M. Strakowski, MD Chart Review: Bipolar Disorder PATIENT INFO 35 Age: Female Sex: 35-year-old woman with Hx of BPII Dx; currently separated from husband; has 1 child Background: SI and hospitalization
Stephen M. Strakowski, MD Chart Review: Bipolar Disorder PATIENT INFO 35 Age: Female Sex: 35-year-old woman with Hx of BPII Dx; currently separated from husband; has 1 child Background: SI and hospitalization
35-year-old woman with Hx of BPII Dx; currently separated from husband; has 1 child
 Stephen M. Strakowski, MD Chart Review: Bipolar Disorder PATIENT INFO 35 Age: Female Sex: 35-year-old woman with Hx of BPII Dx; currently separated from husband; has 1 child Background: SI and hospitalization
Stephen M. Strakowski, MD Chart Review: Bipolar Disorder PATIENT INFO 35 Age: Female Sex: 35-year-old woman with Hx of BPII Dx; currently separated from husband; has 1 child Background: SI and hospitalization
Mental Health Pathway
 Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
DSM-5 Criteria: Bipolar Disorders
 DSM-5 Criteria: Bipolar Disorders Box 1. Bipolar I Disorder: For a diagnosis of bipolar I disorder, it is necessary to meet the following criteria for a manic episode. The manic episode may have been preceded
DSM-5 Criteria: Bipolar Disorders Box 1. Bipolar I Disorder: For a diagnosis of bipolar I disorder, it is necessary to meet the following criteria for a manic episode. The manic episode may have been preceded
Class Update: Oral Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
Surveillance report Published: 26 October 2017 nice.org.uk
 Surveillance report 2017 Bipolar disorder: assessment and management (2014) NICE guideline Surveillance report Published: 26 October 2017 nice.org.uk NICE 2017. All rights reserved. Subject to Notice of
Surveillance report 2017 Bipolar disorder: assessment and management (2014) NICE guideline Surveillance report Published: 26 October 2017 nice.org.uk NICE 2017. All rights reserved. Subject to Notice of
Management of. Depression: Some observations
 Management of Psychobiology Research Group Depression: Some observations Hamish McAllister-Williams Reader in Clinical Psychopharmacology, Newcastle University Hon. Consultant Psychiatrist, Regional Affective
Management of Psychobiology Research Group Depression: Some observations Hamish McAllister-Williams Reader in Clinical Psychopharmacology, Newcastle University Hon. Consultant Psychiatrist, Regional Affective
Manual of Clinical Psychopharmacology
 Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Summary of guideline for the. treatment of depression RANZCP CLINICAL PRACTICE GUIDELINES ASSESSMENT
 RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
Professor Tony Holland, Department of Psychiatry, University of Cambridge
 INFORMATION SHEET The Use of Medication in the Treatment of Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction The use of medication is but one
INFORMATION SHEET The Use of Medication in the Treatment of Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction The use of medication is but one
resources/guidelines-policies/locg.html
 BIPOLAR AND RELATED DISORDERS Optum Coverage Determination Guideline Policy Number: BH803BPD0518 Effective Date: May 9, 2018 Table of Contents Page BENEFIT CONSIDERATIONS...1 COVERAGE RATIONALE...1 EVIDENCE-BASED
BIPOLAR AND RELATED DISORDERS Optum Coverage Determination Guideline Policy Number: BH803BPD0518 Effective Date: May 9, 2018 Table of Contents Page BENEFIT CONSIDERATIONS...1 COVERAGE RATIONALE...1 EVIDENCE-BASED
Pharmacists as a vital part of the mental health of the nation
 Pharmacists as a vital part of the mental health of the nation P H I L I P P I N E S P H A R M A C Y A S S O C I A T I O N C O N V E N T I O N A P R I L 2 5, 2 0 1 5 B A C O L O D T R U D I H I L T O N
Pharmacists as a vital part of the mental health of the nation P H I L I P P I N E S P H A R M A C Y A S S O C I A T I O N C O N V E N T I O N A P R I L 2 5, 2 0 1 5 B A C O L O D T R U D I H I L T O N
Aggression (Severe) in Children under Age 6
 in Children under Age 6") Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
April 2016 Prepared By: Kimberly D. Griego, PharmD, CGP
 April 2016 Prepared By: Kimberly D. Griego, PharmD, CGP Bipolar disorder (BD), also referred to as manic-depression, presents with dramatic swings in a person s mood and energy level, which affects their
April 2016 Prepared By: Kimberly D. Griego, PharmD, CGP Bipolar disorder (BD), also referred to as manic-depression, presents with dramatic swings in a person s mood and energy level, which affects their
Clinical Perspective on Conducting TRD Studies. Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark
 Clinical Perspective on Conducting TRD Studies Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark Overview of Presentation Treatment-Resistant Depression (TRD)
Clinical Perspective on Conducting TRD Studies Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark Overview of Presentation Treatment-Resistant Depression (TRD)
Guidelines for the Utilization of Psychotropic Medications for Children in Foster Care. Illinois Department of Children and Family Services
 Guidelines for the Utilization of Psychotropic Medications for Children in Foster Care Illinois Department of Children and Family Services Introduction With few exceptions, children and adolescents in
Guidelines for the Utilization of Psychotropic Medications for Children in Foster Care Illinois Department of Children and Family Services Introduction With few exceptions, children and adolescents in
Appendix C - Summary form
 National Institute for Health and Clinical Excellence Appendix C - Summary form Single Techn Appraisal (STA) Agomelatine for the treatment of major depressive episodes Response to consultee and commentator
National Institute for Health and Clinical Excellence Appendix C - Summary form Single Techn Appraisal (STA) Agomelatine for the treatment of major depressive episodes Response to consultee and commentator
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
APPENDIX 33: HEALTH ECONOMICS ECONOMIC EVIDENCE PROFILES
 APPENDIX 33: HEALTH ECONOMICS ECONOMIC EVIDENCE PROFILES 1.1 Case identification assessment of adults with bipolar disorder... 2 1.1.1 Clinical/economic question: Mood Disorder Questionnaire (MDQ) versus
APPENDIX 33: HEALTH ECONOMICS ECONOMIC EVIDENCE PROFILES 1.1 Case identification assessment of adults with bipolar disorder... 2 1.1.1 Clinical/economic question: Mood Disorder Questionnaire (MDQ) versus
Treating treatment resistant depression
 Treating treatment resistant depression These slides are the intellectual property of Ian Anderson and must not be reproduced Ian Anderson Neuroscience and Psychiatry Unit University of Manchester and
Treating treatment resistant depression These slides are the intellectual property of Ian Anderson and must not be reproduced Ian Anderson Neuroscience and Psychiatry Unit University of Manchester and
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression
 Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 2012 PSYCHOPHARMACOLOGY SERIES. Guna Kanniah Waikato Hospital
 POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 212 PSYCHOPHARMACOLOGY SERIES Guna Kanniah Waikato Hospital POLYPHARMACY FIVE REASONS FOR POLYPHARMACY 1. To treat a concomitant disorder 2. To treat an
POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 212 PSYCHOPHARMACOLOGY SERIES Guna Kanniah Waikato Hospital POLYPHARMACY FIVE REASONS FOR POLYPHARMACY 1. To treat a concomitant disorder 2. To treat an
Technology appraisal guidance Published: 24 July 2013 nice.org.uk/guidance/ta292
 Aripiprazole for treating moderate to severe ere manic episodes in adolescents with bipolar I disorder Technology appraisal guidance Published: 24 July 2013 nice.org.uk/guidance/ta292 NICE 2018. All rights
Aripiprazole for treating moderate to severe ere manic episodes in adolescents with bipolar I disorder Technology appraisal guidance Published: 24 July 2013 nice.org.uk/guidance/ta292 NICE 2018. All rights
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Roles of primary care physicians in managing bipolar disorders in adults
 CPG UPDATE Roles of primary care physicians in managing bipolar disorders in adults Awaluddin A, Jali N, Bahari R, Jamil Z, Haron N on behalf of Development Group Clinical Practice Guidelines Management
CPG UPDATE Roles of primary care physicians in managing bipolar disorders in adults Awaluddin A, Jali N, Bahari R, Jamil Z, Haron N on behalf of Development Group Clinical Practice Guidelines Management
3. Depressione unipolare
 3. Depressione unipolare Depressione unipolare con mancata risposta al trattamento con SSRI Question: Should switching from SSRIs to another antidepressant class vs switching within class (SSRIs) be used
3. Depressione unipolare Depressione unipolare con mancata risposta al trattamento con SSRI Question: Should switching from SSRIs to another antidepressant class vs switching within class (SSRIs) be used
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 18 February 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 February 2009 ABILIFY 5 mg tablets, pack of 28 (CIP: 364 069-7) ABILIFY 10 mg tablets, pack of 28 (CIP: 364 073-4)
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 February 2009 ABILIFY 5 mg tablets, pack of 28 (CIP: 364 069-7) ABILIFY 10 mg tablets, pack of 28 (CIP: 364 073-4)
Psychotropic Drug Therapy in Adults with Learning Disability. Steve Wilkinson
 Psychotropic Drug Therapy in Adults with Learning Disability Steve Wilkinson Outline and Aims of the Session Drug use in learning disability Two distinct areas of drug therapy I. Treatment of common psychiatric
Psychotropic Drug Therapy in Adults with Learning Disability Steve Wilkinson Outline and Aims of the Session Drug use in learning disability Two distinct areas of drug therapy I. Treatment of common psychiatric
5 COMMON QUESTIONS WHEN TREATING DEPRESSION
 5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
Practical Psychopharmacology for More Complex Mental Health Presentations
 MINISTRY OF CHILDREN AND YOUTH SERVICES Practical Psychopharmacology for More Complex Mental Health Presentations Part 2: Antipsychotics & Mood Stabilizers Dr. Ajit Ninan & Joel Lamoure 1 : Who are we?
MINISTRY OF CHILDREN AND YOUTH SERVICES Practical Psychopharmacology for More Complex Mental Health Presentations Part 2: Antipsychotics & Mood Stabilizers Dr. Ajit Ninan & Joel Lamoure 1 : Who are we?
Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs
 Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs (Version 3 January 2015) Principal Author: Dr Jenny Cooke Consultant Psychiatrist, Brighton & Hove Perinatal Mental Health Service
Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs (Version 3 January 2015) Principal Author: Dr Jenny Cooke Consultant Psychiatrist, Brighton & Hove Perinatal Mental Health Service
Objectives. Objectives. A practice review. 02-Nov-16 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS
 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
GUIDELINES FOR THE USE OF PSYCHOACTIVE MEDICATIONS IN INDIVIDUALS WITH CO-OCCURRING SUBSTANCE USE DISORDERS
 City and County of San Francisco Mayor Gavin Newsom Department of Public Health Community Behavioral Health Services 1380 Howard Street 5 th Floor San Francisco, CA 94103 GUIDELINES FOR THE USE OF PSYCHOACTIVE
City and County of San Francisco Mayor Gavin Newsom Department of Public Health Community Behavioral Health Services 1380 Howard Street 5 th Floor San Francisco, CA 94103 GUIDELINES FOR THE USE OF PSYCHOACTIVE
ECT in children and adolescents
 ECT in children and adolescents Adi Sharma MD MRCPsych PhD Clinical Senior Lecturer & Hon Consultant in Child & Adolescent Psychiatry National Adolescent Bipolar Service 1 Conflicts None relevant to this
ECT in children and adolescents Adi Sharma MD MRCPsych PhD Clinical Senior Lecturer & Hon Consultant in Child & Adolescent Psychiatry National Adolescent Bipolar Service 1 Conflicts None relevant to this
Commentary: Evidence-based pharmacotherapy of bipolar disorder
 International Journal of Neuropsychopharmacology (2003), 6, 303 308. Copyright f 2003 CINP DOI: 10.1017/S1461145703003626 Commentary: Evidence-based pharmacotherapy of bipolar disorder SPECIAL SERIES S.
International Journal of Neuropsychopharmacology (2003), 6, 303 308. Copyright f 2003 CINP DOI: 10.1017/S1461145703003626 Commentary: Evidence-based pharmacotherapy of bipolar disorder SPECIAL SERIES S.
Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula
 Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula Official Name Bipolar Disorder; also referred to as Manic Depression Definitions (DSM-IV-TR, 2000) Bipolar I Disorder
Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula Official Name Bipolar Disorder; also referred to as Manic Depression Definitions (DSM-IV-TR, 2000) Bipolar I Disorder
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Drug Treatments for Mental Illnesses: Advances, Controversies and Scandals
 Regional Affective Disorders Service Drug Treatments for Mental Illnesses: Advances, Controversies and Scandals Hamish McAllister-Williams Reader in Clinical Psychopharmacology and Honorary Consultant
Regional Affective Disorders Service Drug Treatments for Mental Illnesses: Advances, Controversies and Scandals Hamish McAllister-Williams Reader in Clinical Psychopharmacology and Honorary Consultant