Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care
|
|
|
- Clement James
- 5 years ago
- Views:
Transcription
1 Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care Dr. John Puxty Ontario s Ontario s Strategy Strategy for Alzheimer for Disease and Related Dementia: Initiative #2, #2, Physician Physician Education Education
2 Behavioural and Psychological Symptoms of Dementia (BPSD) Behaviour is responsive. It occurs in response to stimuli in the physical, social, or emotional environments. Variety of changes occurring in dementia that can alter a behavioural response to an external event or interaction. These include changes: in an individual s perception and interpretation of external stimuli, capacity for attention and filtering, and degree to which emotional and instinctive responses are moderated The resulting changes in behaviour and mood are often referred to as Behavioural and Psychological Symptoms of Dementia (BPSD).
 aggressive physical (hitting) verbal (cursing) Resistance to care Disinhibition Diurnal rhythm disturbances Sleep disorders Sexually inappropriate")
3 Categories of Major Behavioural and Psychological Disturbances in Dementia Depression Psychosis Agitation non-aggressive physical (wandering) verbal (screaming) aggressive physical (hitting) verbal (cursing) Resistance to care Disinhibition Diurnal rhythm disturbances Sleep disorders Sexually inappropriate behaviour
 had one or more BPSD at initial evaluation (Devanand, et al., 1997). The majority of these people were living at home.")
4 Frequency of Behavioural and Psychological Problems in Dementia Any symptom can occur during any stage in dementia, and virtually all patients demonstrate some type of BPSD (Reisberg et al., 1989). One study of BPSD found that 64% of patients with Alzheimer s Disease (AD) had one or more BPSD at initial evaluation (Devanand, et al., 1997). The majority of these people were living at home. Another study of just community living elderly with dementia reported at least 61% had an example of BPSD and a third of the symptoms were moderate to severe (Lyketso et al 2000).

5 Common Behavioural Changes throughout the Course of Alzheimer s Disease
6 BPSD in Dementia other than Alzheimer s Disease (Vascular Dementia) Some studies have found noted differences between the prevalence and type of BPSD in Alzheimer s Disease (AD) and Vascular Dementia (VaD) (Cohen et al., 1993; Tariot and Blazina, 1994), for example a higher rate of delusions in AD and a higher rate of depression in VaD (Lyketsos et al., 2000).
7 BPSD in Dementia other than Alzheimer s Disease (Frontotemporal Dementia) Frontotemporal dementia is typically associated with a higher incidence of BPSD early in the course of the illness. The reason for initial consultation is more likely to be related to behavioural difficulties than memory loss. These include disinhibition (socially tactless), impulsivity, compulsive behaviours (including over-eating), grabbing, hypersexuality, and verbal outbursts. The anatomic distribution of asymmetric atrophy in frontotemporal dementia has been correlated with specific behavioural manifestations.
8 BPSD in Dementia other than Alzheimer s Disease (Lewy Body Dementia) Lewy Body Dementia is characterized by the early appearance of visual hallucinations, relatively mild abnormalities of cognition and features of extrapyramidal impairment. The visual hallucination are often characterized by being structured and often non-distressing to the individual. Attempts to treat these with anti-psychotics may be associated with marked extrapyramidal side-effects Over half may present with an acute fluctuations of cognition resembling delirium. After resolution of which they often have findings of impaired attention, executive, visuospatial function, & constructional abilities with relatively intact memory.
9 Impact of BPSD on Caregivers Caregiver burden and stress present a major issue in moderate to severe dementia both in community and long-term care setting Certain behavioral problems are more likely to precipitate a request for admission to LTC, including: physical and verbal aggression night-time behavioural issues paranoia/hallucinations depressive symptoms wandering (Hope T et al. Int J Geriatr Psychiatr 1998;13(10): , Gilley DW et al. Psychol Med 2004;34(6): )
 might react, interpret and act differently.")
10 Understanding Brain and Behaviour A Structural / Functional Approach Understanding the normal functions of the brain and their impact on function and behaviour provides an insight as to why the person with dementia (with damage to certain parts of the brain) might react, interpret and act differently. Their reality is not our reality.
11 Case: The Imposter A 74-year old woman has a 5-year history of mild memory problems. She has had occurrences where she does not recognize her friends, or she has become lost. Her family has become distressed by these new behaviours. She has recently started to accuse her husband of being an imposter; saying that this old man is not her husband. She has become increasingly agitated and has wandered from her home, necessitating her return by police. She calls her daughter at night and asks to be taken home. She has started locking her bedroom door.
12 Summary of Brain Function and Behaviour Brain area Function Deficient Behaviour Frontal lobes Executive function Social inhibition Language Temporal lobes Language Memory Parietal lobes Language analysis, Calculations, Spatial perception, Sequencing Occipital lobes Vision Depth perception Cerebellum Brain stem Sub-cortical areas Limbic Hippocampus Balance Voluntary & Involuntary movements Memory retrieval Connects behaviour with memories Regulates sleep, appetite
13 Summary of Brain Function and Behaviour Brain area Function Deficient Behaviour Frontal lobes Temporal lobes Executive function Social inhibition Language Language Memory Problems with planning, initiating, executing in a planned, organized manner Re-emergence primitive reflexes Motor Aphasia Unable to initiate (may appear lazy, uncooperative with requests) Impulsivity, may be disinhibited Can t plan holiday, activities of the day, dinner party, etc Grabbing (Grasp reflex) and Paratonia. Parietal lobes Language analysis, Calculations, Spatial perception, Sequencing Occipital lobes Vision Depth perception Cerebellum Brain stem Sub-cortical areas Limbic Hippocampus Balance Voluntary & Involuntary movements Memory retrieval Connects behaviour with memories Regulates sleep, appetite
14 Summary of Brain Function and Behaviour Brain area Function Deficient Behaviour Frontal lobes Temporal lobes Executive function Social inhibition Language Language Memory Problems with planning, initiating, executing in a planned, organized manner Re-emergence primitive reflexes Motor Aphasia Aphasia Amnesia Unable to initiate (may appear lazy, uncooperative with requests) Impulsivity, may be disinhibited Can t plan holiday, activities of the day, dinner party, etc Grabbing (Grasp reflex) and Paratonia. Frustration with aphasia, annoying repetitions, unsafe use of tools, stove, disorientation. Parietal lobes Language analysis, Calculations, Spatial perception, Sequencing Occipital lobes Vision Depth perception Cerebellum Brain stem Sub-cortical areas Limbic Hippocampus Balance Voluntary & Involuntary movements Memory retrieval Connects behaviour with memories Regulates sleep, appetite
15 Summary of Brain Function and Behaviour Brain area Function Deficient Behaviour Frontal lobes Temporal lobes Executive function Social inhibition Language Language Memory Problems with planning, initiating, executing in a planned, organized manner Re-emergence primitive reflexes Motor Aphasia Aphasia Amnesia Unable to initiate (may appear lazy, uncooperative with requests) Impulsivity, may be disinhibited Can t plan holiday, activities of the day, dinner party, etc Grabbing (Grasp reflex) and Paratonia. Frustration with aphasia, annoying repetitions, unsafe use of tools, stove, disorientation. Parietal lobes Language analysis, Calculations, Spatial perception, Sequencing Difficulty understanding Visual-spatial planning difficulties Difficulty sequencing movements Apraxia Agnosia Anosognosia Vague historian, Unable to manage finances or driving Dressing, gait or eating difficulties may be present Failure recognize people/objects Lacks insight into disease Occipital lobes Vision Depth perception Cerebellum Brain stem Sub-cortical areas Balance Voluntary & Involuntary movements Limbic Hippocampus Memory retrieval Connects behaviour with memories Regulates sleep, appetite
16 Summary of Brain Function and Behaviour Brain area Function Deficient Behaviour Frontal lobes Temporal lobes Executive function Social inhibition Language Language Memory Problems with planning, initiating, executing in a planned, organized manner Re-emergence primitive reflexes Motor Aphasia Aphasia Amnesia Unable to initiate (may appear lazy, uncooperative with requests) Impulsivity, may be disinhibited Can t plan holiday, activities of the day, dinner party, etc Grabbing (Grasp reflex) and Paratonia. Frustration with aphasia, annoying repetitions, unsafe use of tools, stove, disorientation. Parietal lobes Language analysis, Calculations, Spatial perception, Sequencing Difficulty understanding Visual-spatial planning difficulties Difficulty sequencing movements Apraxia Agnosia Anosognosia Vague historian, Unable to manage finances or driving Dressing, gait or eating difficulties may be present Failure recognize people/objects Lacks insight into disease Occipital lobes Vision Depth perception May not scan or interpret environment properly Startled response Afraid of tub water (appears too deep) Messy when pouring liquids, etc. Cerebellum Brain stem Sub-cortical areas Balance Voluntary & Involuntary movements Limbic Hippocampus Memory retrieval Connects behaviour with memories Regulates sleep, appetite
17 Summary of Brain Function and Behaviour Brain area Function Deficient Behaviour Frontal lobes Temporal lobes Executive function Social inhibition Language Language Memory Problems with planning, initiating, executing in a planned, organized manner Re-emergence primitive reflexes Motor Aphasia Aphasia Amnesia Unable to initiate (may appear lazy, uncooperative with requests) Impulsivity, may be disinhibited Can t plan holiday, activities of the day, dinner party, etc Grabbing (Grasp reflex) and Paratonia. Frustration with aphasia, annoying repetitions, unsafe use of tools, stove, disorientation. Parietal lobes Language analysis, Calculations, Spatial perception, Sequencing Difficulty understanding Visual-spatial planning difficulties Difficulty sequencing movements Apraxia Agnosia Anosognosia Vague historian, Unable to manage finances or driving Dressing, gait or eating difficulties may be present Failure recognize people/objects Lacks insight into disease Occipital lobes Vision Depth perception May not scan or interpret environment properly Startled response Afraid of tub water (appears too deep) Messy when pouring liquids, etc. Cerebellum Brain stem Sub-cortical areas Balance Voluntary & Involuntary movements Abnormal gait/balance, Slowness of movement Swallowing problem Falls Slow movements Aspiration pneumonia Limbic Hippocampus Memory retrieval Connects behaviour with memories Regulates sleep, appetite
18 Summary of Brain Function and Behaviour Brain area Function Deficient Behaviour Frontal lobes Temporal lobes Executive function Social inhibition Language Language Memory Problems with planning, initiating, executing in a planned, organized manner Re-emergence primitive reflexes Motor Aphasia Aphasia Amnesia Unable to initiate (may appear lazy, uncooperative with requests) Impulsivity, may be disinhibited Can t plan holiday, activities of the day, dinner party, etc Grabbing (Grasp reflex) and Paratonia. Frustration with aphasia, annoying repetitions, unsafe use of tools, stove, disorientation. Parietal lobes Language analysis, Calculations, Spatial perception, Sequencing Difficulty understanding Visual-spatial planning difficulties Difficulty sequencing movements Apraxia Agnosia Anosognosia Vague historian, Unable to manage finances or driving Dressing, gait or eating difficulties may be present Failure recognize people/objects Lacks insight into disease Occipital lobes Vision Depth perception May not scan or interpret environment properly Startled response Afraid of tub water (appears too deep) Messy when pouring liquids, etc. Cerebellum Brain stem Sub-cortical areas Balance Voluntary & Involuntary movements Abnormal gait/balance Slowness of movement Swallowing problem Falls Slow movements Aspiration pneumonia Limbic Hippocampus Memory retrieval Connects behaviour with memories Regulates sleep, appetite Misinterprets events Emotional lability Blaming others Irritability and depression Day-night reversal Hot/cold perception changes

19 Case: The Imposter Her new behaviours are likely attributable to a combination of agnosia, anosognosia and amnesia. She does not recognize her husband; nor does she appreciate that they have aged or that she has memory problems. Management should be mainly nonpharmacological. If she is not on ACEI such as Donepezil it should be considered. A trial of an SSRI may be indicated.
20
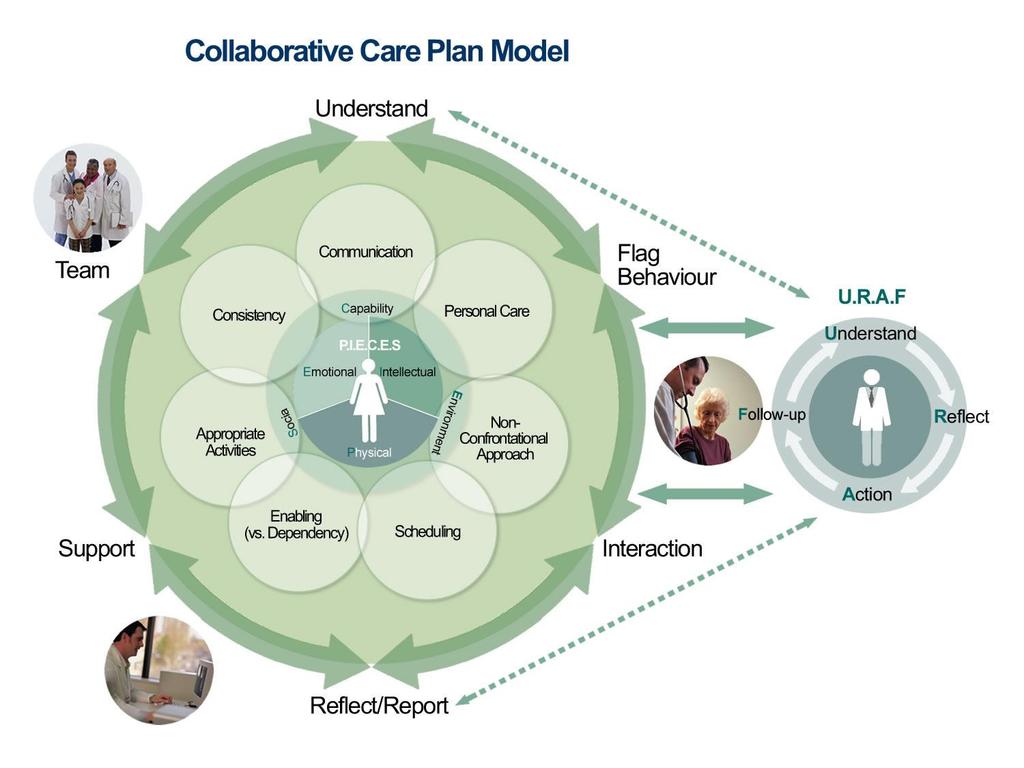
21 Physician s Approach to Collaborative Care Planning in BPSD: 5 Questions 1. What has changed and what are the main concerns of caregivers? 2. What are the consequences or risks of the behaviours or psychological symptoms, if allowed to continue? 3. What are possible contributory factors to the behaviours or psychological symptoms (think P.I.E.C.E.S.)? 4. What needs to be done? 5. How should things be monitored and re-evaluated?

22 Case: Applying the 5 Questions John is a 72-yr old man with a 3-year history of AD who has recently started to sleep on the couch downstairs while watching TV His wife hears him scream one night that there is an intruder in the house, and hears him leave She finds him some time later wandering the neighborhood with a stick and threatening passersby The next day John s distressed wife and daughter bring him to your office. You find him to be similar to previous visits and cooperative.
23 Case: Understand (Q1) Q1. What are the main concerns and what has changed? The main concerns of the family are the risk for wandering outside the house and potential return of sudden and uncharacteristic threatening behaviour. On reviewing his cognitive deficits you note that he has problems with short-term memory, difficulty in verbal fluency (naming 10 animals), spatial orientation (clock and pentagon completion), and abstraction. His family reports that he has been withdrawing from previous hobbies (gardening and cards), and is less attentive of self-grooming. On occasions he has become lost in normally familiar situations. He appears to have a mild to moderate stage of AD with multiple deficits noted. This is the first time a disruptive behaviour of this type has been seen, and therefore represents the most important change.
24 Case: Understand (Q2) Q2. What are the consequences and risks of the behaviours or psychological symptoms if allowed to continue? If one cannot identify the causes of this new behaviour, it may occur again and put John at risk of wandering outside the home, inappropriately dressed for the weather. It may also cause fear in the neighborhood. In the immediate situation there is also a danger that a single incident may result in John being labeled as aggressive and threatening, which may negatively influence care providers.
25 Case: Understand (Q3) Q3. What are likely contributory factors to the behaviours or psychological symptoms (think P.I.E.C.E.S.)? His behaviour likely arises from his perception that an intruder has actually entered his home. The impaired perception may be caused by a combination of agnosia (people on TV are actually inside the house) and grogginess on first awaking. Believing intruders were threatening his family, John attempted to chase them away. Subsequently he became lost and fearful, hence his threatening behaviour.
26 Case: Action (Q4) Q4. What needs to be done? Screen for sensory miscues (hearing or vision) that could potentially contribute to John s perceptual problems Review medication use, especially alcohol and across the counter medication, for potential anticholinergic or somnolence effects Exclude any new medical issues (e.g. Urinary Tract Infection) that may be causing a delirium Management ideally should be non-pharmacological to minimize the risk of recurrence of the behaviour. This might include: reducing any sensory miscues (e.g. lighting, review vision and hearing), improving sleep habit/hygiene - use of a snooze timer education of family in contributory factors and supportive care strategies
27 Case: Follow-Up (Q5) 5. How should things be monitored and re-evaluated? The event is situational and hopefully will respond to measures as previously discussed, however, it would be important to review and discuss the potential for similar responsive behaviours in the future

28 Approach to Assessing and Managing BPSD What has changed? What are the risks and consequences? What are the contributory factors? What should be done? How should things be monitored? Pharmacological Non-pharmacological
29 Behaviours that will not respond to medications Simple wandering Inappropriate urination / defecation Inappropriate dressing / undressing Repetitive activities (perseveration) or vocalizations Hiding / hoarding Eating inedibles Tugging at / removal of restraints Pushing wheelchair bound co-patients
30 BPSD that may get worse with medications BPSD: aggressive / disinhibited visual hallucinations / confusion motor restlessness apathetic / withdrawn May get worse with: benzodiazepines & alcohol drugs with anti-cholinergic properties anti-psychotics (akathisia) benzodiazepines or antipsychotics
31 Non-pharmacological management of BPSD Derived from an understanding of the contributing factors to the behaviours Strategies that reduce and/or contain the behaviours Reinforcement of retained skills/abilities Crucial features: Timing Priming Miming The only safe and efficacious treatment for those problems that will not respond to medication
32 Non-pharmacological management of BPSD Non-Pharmacological Strategies Approach Schedule Communication Minimize failure without dependency Appropriate activity/environment Attention to personal care Preventative care (bowels/bladder/sleep) Hydration / nutrition Medication use

33 Approach to Assessing and Managing BPSD What has changed? What are the risks and consequences? What are the contributory factors? What should be done? How should things be monitored? Pharmacological Non-pharmacological

34 Consider pharmacological treatment of BPSD when: Behaviour is: dangerous to self or others distressing to self or others damaging to social relationships persistent AND has not responded to comprehensive non-pharmacological treatment plan, including the removal of possibly offending drugs OR The individual requires emergency treatment to allow proper investigation of underlying health issues
35 Behaviours that may respond to medications Physical aggression Verbal aggression Anxiety and restlessness Sadness, crying, anorexia, insomnia and other symptoms indicative of depression Withdrawal and apathy Sleep disturbance Wandering with agitation / aggression Elation, pressured speech and hyperactivity (manic-like symptoms) Persistent delusions and hallucinations Sexually inappropriate behaviour with agitation
36 Pharmacological management of BPSD - Guiding principles: Optimize treatment for underlying health issues Remove medications that are possible precipitants Introduce one drug at a time, and monitor the effect Start low (dose) and go slow (titration) Optimize the dose and duration to allow an adequate trial before switching to another medication Ensure that the chosen medication won t worsen dementia or other health issues Check for potential drug-drug interactions before finalizing the choice of medication
37 Medications for treating BPSD Target Symptoms Medication Starting Dose (mg/day) Average Target Dose (mg/day) Delusions Atypical Antipsychotics: Hallucination Risperidone Aggression Olanzapine Quetiapine Sadness Antidepressants: Irritability Citalopram Anxiety Sertraline Insomnia Venlafaxine Mirtazapine Trazodone
38 Medications for treating BPSD Target Symptoms Medication Starting Dose (mg/day) Average Target Dose (mg/day) Mood swings Euphoria Impulsivity Mood stabilizers: Valproic Acid Agitation Apathy Cholinesterase Inhibitors Memantine As directed 5 mg daily As directed 10 mg BID Irritability Anxiety (short term use in predictable situations) Anxiolytics: Lorazepam Oxazepam

39 Treatment of severe agitation likely due to delirium Low dose Haloperidol: consider for emergency, short-term use (days) while addressing cause(s) of delirium Consider atypicals: Quetiapine, Risperidone Consider Loxapine or Perphenazine: Assess 3 C s: Cholinergic Cardiovascular Constriction (EPS)
40 Treatment of behavioural problems due to Lewy Body Dementia (LBD) Cholinesterase inhibitors: now first line of treatment need to try over several weeks Trazodone: if cholinesterase inhibitors ineffective or too early in treatment watch BP Antipsychotics should generally be avoided in residents with LBD: potential for severe adverse effects If an antipsychotic is absolutely necessary in LBD or Parkinson s: Quetiapine may be less likely than other atypicals to exacerbate the motor symptoms (Friedman & Factor, 2000)
41 Sleep disruption may exacerbate BPSD Possible causes: Physical: pain urination Intellectual Brain Changes: REM Behavioural Disorder seizures Sleep Disorders: Sleep Apnea Restless Leg and Periodic Leg Movement No Sleep = Seriously Effects Daytime Behavior (DOS)
42 Summary Take Home Messages Health Care Teams have an important role in helping care providers understand, how the changes in the brain that occur in dementia affect a person s behaviour. They can help to guide caregiver interactions with the individual, and identify supportive care strategies that enable the individual s functional abilities/potential rather than confront their cognitive losses. In this way, challenges related to the behavioural changes that occur in cognitive impairment will be minimized for the individual and others. is a resource for both informational and clinical resources on Dementia and BPSD
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Chapter 5. BPSD: Behavioural Problems Throughout the Course of Dementia. Dr. John Puxty Dr. William Dalziel Dr. Ken Le Clair Dr. Marie-France Rivard
 Chapter 5 BPSD: Behavioural Problems Throughout the Course of Dementia Dr. John Puxty Dr. William Dalziel Dr. Ken Le Clair Dr. Marie-France Rivard Chapter Index Frequency of Behavioural and Psychological
Chapter 5 BPSD: Behavioural Problems Throughout the Course of Dementia Dr. John Puxty Dr. William Dalziel Dr. Ken Le Clair Dr. Marie-France Rivard Chapter Index Frequency of Behavioural and Psychological
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Chapter 2. Brain and Behaviour. Dr. John Puxty Dr. Ken Le Clair Dr. Marie-France Rivard. BPSD Handbook for Family Physicians
 Chapter 2 Brain and Behaviour Dr. John Puxty Dr. Ken Le Clair Dr. Marie-France Rivard Chapter Index Overview...1 Key Concepts...1 Understanding Brain and Behaviour: A Structural/Functional Approach...2
Chapter 2 Brain and Behaviour Dr. John Puxty Dr. Ken Le Clair Dr. Marie-France Rivard Chapter Index Overview...1 Key Concepts...1 Understanding Brain and Behaviour: A Structural/Functional Approach...2
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Dementia Training Session for Carers. By Dr Rahul Tomar Consultant Psychiatrist
 Dementia Training Session for Carers By Dr Rahul Tomar Consultant Psychiatrist Dementia in the UK: Facts & Figures National Dementia strategy launched in 2009 800,000 people living with dementia (2012)
Dementia Training Session for Carers By Dr Rahul Tomar Consultant Psychiatrist Dementia in the UK: Facts & Figures National Dementia strategy launched in 2009 800,000 people living with dementia (2012)
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches
 Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Pharmacological Treatment of Aggression in the Elderly
 Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
GENI Jeopardy: Geriatric Mental Health. Part of the brain responsible for executive functioning
 GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego
 Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Management of the Acutely Agitated Long Term Care Patient
 Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Assessment and management of behavioral and psychological symptoms of dementia
 Assessment and management of behavioral and psychological symptoms of dementia Helen C Kales, 1 2 3 Laura N Gitlin, 4 5 6 Constantine G Lyketsos 7 1 Section of Geriatric Psychiatry, Department of Psychiatry,
Assessment and management of behavioral and psychological symptoms of dementia Helen C Kales, 1 2 3 Laura N Gitlin, 4 5 6 Constantine G Lyketsos 7 1 Section of Geriatric Psychiatry, Department of Psychiatry,
Stroke and Behaviour Change
 Stroke and Behaviour Change Kathy Baker BA (Psych), BScN, MAL (Health) Mary-Lou Nolte, Ph.D., C. Psych. Objectives Describe relationships among cognition, mood and behaviour change after stroke Describe
Stroke and Behaviour Change Kathy Baker BA (Psych), BScN, MAL (Health) Mary-Lou Nolte, Ph.D., C. Psych. Objectives Describe relationships among cognition, mood and behaviour change after stroke Describe
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
NCFE Level 2 Certificate in The Principles of Dementia Care
 The Principles of Dementia Care S A M P LE NCFE Level 2 Certificate in The Principles of Dementia Care Part A 1 These learning resources and assessment questions have been approved and endorsed by ncfe
The Principles of Dementia Care S A M P LE NCFE Level 2 Certificate in The Principles of Dementia Care Part A 1 These learning resources and assessment questions have been approved and endorsed by ncfe
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Alzheimer s disease and related disorders. Patient risks
 Alzheimer s disease and related disorders Patient risks ALZHEIMER BELGIQUE Alzheimer Belgique is a patient association founded in 1985 by families affected by the disease Some of our missions: Inform the
Alzheimer s disease and related disorders Patient risks ALZHEIMER BELGIQUE Alzheimer Belgique is a patient association founded in 1985 by families affected by the disease Some of our missions: Inform the
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Lead From Where You Stand
 Lead From Where You Stand EXTRA Research Project: Reducing Antipsychotic Medications Module 3:The Brain and Behavior The Brain To expect a personality to survive the disintegration of the brain is like
Lead From Where You Stand EXTRA Research Project: Reducing Antipsychotic Medications Module 3:The Brain and Behavior The Brain To expect a personality to survive the disintegration of the brain is like
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
11/11/2016. Disclosures. Natural history of BPSD. Objectives. Assessment of BPSD. Behavioral Management of Persons with Alzheimer s Disease
 Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care
 Summary document for Primary Care") Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Management of Behavioral Symptoms in Dementia. Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal
 Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Managing Challenging Behaviors
 Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine & Lorin M. Scher, MD Attending Psychiatrist, HDSA Center of Excellence UC
Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine & Lorin M. Scher, MD Attending Psychiatrist, HDSA Center of Excellence UC
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
Dementia: Managing Difficult Behaviors. No conflicts of interest. Off-label medication use will be discussed during this talk.
 Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Dementia Information Kit for HACC Workers
 Dementia Information Kit for HACC Workers This presentation has been compiled as part of the Loddon Mallee region Dementia Management Strategy project in 2002 and revised in 2008 to assist HACC workers
Dementia Information Kit for HACC Workers This presentation has been compiled as part of the Loddon Mallee region Dementia Management Strategy project in 2002 and revised in 2008 to assist HACC workers
October 28, Geriatrics Update Course. Lesley Wiesenfeld, MD, MHCM, FRCPC. Managing BPSD. Geriatric Psychiatrist, Mount Sinai Hospital
 October 28, 2016 Geriatrics Update Course Managing BPSD Lesley Wiesenfeld, MD, MHCM, FRCPC Geriatric Psychiatrist, Mount Sinai Hospital Disclosures ~No Pharmaceutical or Industry Support ~ No Health Without
October 28, 2016 Geriatrics Update Course Managing BPSD Lesley Wiesenfeld, MD, MHCM, FRCPC Geriatric Psychiatrist, Mount Sinai Hospital Disclosures ~No Pharmaceutical or Industry Support ~ No Health Without
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D.
 HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL
 TOOL") DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Introduction to Dementia: Complications
 Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Managing Challenging Behaviors
 Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine In partnership with Drs. Lorin Scher, MD and Vicki Wheelock, MD 1 Our Goal
Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine In partnership with Drs. Lorin Scher, MD and Vicki Wheelock, MD 1 Our Goal
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Decline in Mental Capacity
 Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
NeuroPharmac Journal ISSN: Alzheimer s Disease: Pharmacotherapy of noncognitive symptoms Aslam Pathan; Abdulrahman M.
 ISSNISSN ISSN: 2456-3927 NeuroPharmac Journal Alzheimer s Disease: Pharmacotherapy of noncognitive symptoms Aslam Pathan; Abdulrahman M. Alshahrani www. neuropharmac.com Jan-April 2018, Volume 3, Issue
ISSNISSN ISSN: 2456-3927 NeuroPharmac Journal Alzheimer s Disease: Pharmacotherapy of noncognitive symptoms Aslam Pathan; Abdulrahman M. Alshahrani www. neuropharmac.com Jan-April 2018, Volume 3, Issue
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
6/22/2012. Co-morbidity - when two or more conditions occur together. The two conditions may or may not be causally related.
 Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Chapter 2: Alzheimer s Disease and Other Dementias
 By Eun-Shim Nahm, PhD, RN Assistant Professor University of Maryland School of Nursing OUTLINE What is Alzheimer s disease? Causes of Alzheimer s disease? Cognitive Changes Behavioral, Psychiatric issues
By Eun-Shim Nahm, PhD, RN Assistant Professor University of Maryland School of Nursing OUTLINE What is Alzheimer s disease? Causes of Alzheimer s disease? Cognitive Changes Behavioral, Psychiatric issues
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Every 67seconds, someone will develop Alzheimer's.
 We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
Mental Health Disorders Civil Commitment UNC School of Government
 Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Causes of Transient Incontinence. Geriatrics: Urinary Incontinence, Dementia, and Delirium. Classification of Established Incontinence
 Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
9/11/2012. Clare I. Hays, MD, CMD
 Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Mental Health Nursing: Organic Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE?
- WHAT IS THE EVIDENCE?") USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE? Mugdha Thakur, MD Associate Professor of Psychiatry and Behavioral Sciences Duke University
USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE? Mugdha Thakur, MD Associate Professor of Psychiatry and Behavioral Sciences Duke University
Pamela S. Klonoff, PhD Clinical Director Center for Transitional Neuro-Rehabilitation Barrow Neurological Institute, Phoenix, Arizona
 Neuropsychology Pamela S. Klonoff, PhD Clinical Director Center for Transitional Neuro-Rehabilitation Barrow Neurological Institute, Phoenix, Arizona Top Ten Ways to Understand and Cope with a Brain Tumor
Neuropsychology Pamela S. Klonoff, PhD Clinical Director Center for Transitional Neuro-Rehabilitation Barrow Neurological Institute, Phoenix, Arizona Top Ten Ways to Understand and Cope with a Brain Tumor
A Healthy Brain. An Injured Brain
 A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
40% of mild cognitive impairment 60% of patients in early stage of dementia
 BPSD Vague and under-researched although described clearly by Alois Alzheimer Term ratified by 1996 IPA consensus conference Not fully recognised in current diagnostic systems Bypassed by dementia strategy
BPSD Vague and under-researched although described clearly by Alois Alzheimer Term ratified by 1996 IPA consensus conference Not fully recognised in current diagnostic systems Bypassed by dementia strategy
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Antipsychotics for Dementia Under Control or Over-Prescribed?
 Antipsychotics for Dementia Under Control or Over-Prescribed? Nathaniel Hedrick, PharmD ProCare HospiceCare, Manager of Clinical Services Learning Objectives Summarize the disease progression and most
Antipsychotics for Dementia Under Control or Over-Prescribed? Nathaniel Hedrick, PharmD ProCare HospiceCare, Manager of Clinical Services Learning Objectives Summarize the disease progression and most
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
Delirium, Dementia, and Amnestic Disorders. Dr.Al-Azzam 1
 Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
An Approach to Dementia-related Behaviours at the End of Life. Elisabeth Drance MD FRCP(C) Ger. Psych Clinical Associate Professor Psychiatry UBC
 Ger. Psych Clinical Associate Professor Psychiatry UBC") An Approach to Dementia-related Behaviours at the End of Life Elisabeth Drance MD FRCP(C) Ger. Psych Clinical Associate Professor Psychiatry UBC Objectives List the common behaviours occurring in late
An Approach to Dementia-related Behaviours at the End of Life Elisabeth Drance MD FRCP(C) Ger. Psych Clinical Associate Professor Psychiatry UBC Objectives List the common behaviours occurring in late
Chapter 7. BPSD: Psychosis in Dementia. Dr. Ken Le Clair Dr. Marie-France Rivard. BPSD Handbook for Family Physicians
 Chapter 7 BPSD: Psychosis in Dementia Dr. Ken Le Clair Dr. Marie-France Rivard Chapter Index Introduction...1 Part A: Psychosis as Primary Issue...3 Definition of Psychosis...3 The Differential Diagnosis
Chapter 7 BPSD: Psychosis in Dementia Dr. Ken Le Clair Dr. Marie-France Rivard Chapter Index Introduction...1 Part A: Psychosis as Primary Issue...3 Definition of Psychosis...3 The Differential Diagnosis