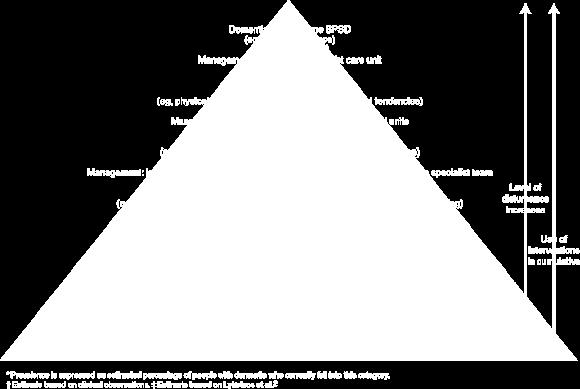
40% of mild cognitive impairment 60% of patients in early stage of dementia
|
|
|
- Grant Marshall
- 5 years ago
- Views:
Transcription
1 BPSD Vague and under-researched although described clearly by Alois Alzheimer Term ratified by 1996 IPA consensus conference Not fully recognised in current diagnostic systems Bypassed by dementia strategy 2008 Not addressed adequately by some guidelines
2 BPSD Seen in: 40% of mild cognitive impairment 60% of patients in early stage of dementia Affects % of patients with dementia at some point in the course of their illness Gets more frequent and troublesome with advancing dementia
3 BPSD- behavioural symptoms most common common less common Apathy Aggression Wandering (aka walking) Restlessness Eating problems Agitation Disinhibition Pacing Screaming Sundowning Crying Mannerisms

4 BPSD in Alzheimer s Disease (n= 2354) NPI items Mean and SD % patients with symptom (score > 3) Delusions 1.5 ± Hallucinations 0.7 ± Agitation 2.3 ± Depression 2.8 ± Anxiety 2.7 ± Euphoria 0.4 ± Apathy 4.2 ± Disinhibition 0.8 ± Irritability 2.4 ± Aberrant motor behaviour 2.0 ± Night-time behaviour disturbances Appetite and eating abnormalities 1.5 ± ± Aalten et al 2007; Dem.Ger.Cog.Dis; 24(6):457-63
5 BPSD- psychological symptoms most common common less common Depression Anxiety Insomnia Delusions Hallucinations Misidentification
6 Frequency of BPSD
7 BPSD Alzheimer s Vascular Lewy body Frontotemporal Apathy Apathy Hallucinations Apathy Agitation Depression Delusions Disinhibition Depression Delusions Depression Elation Anxiety Irritability Sleep disturbance Obsessions
8 mild severe 10 0 apathy depression irritability anxiety agitation delusions disinhibition wandering

9 BPSD stages
10 Why Are BPSD Important? They result in: excess disability increased hospitalization premature institutionalization suffering for patient and caregiver substantial increase in financial costs Finkel 1996
11 Diagnosis and Assessment of BPSD Phenomenology is the basis of diagnosis Direct interview Direct observation Proxy report Measurements and scales Need for accurate descriptions Think of physical illness Think of sensory impairment
12 Variation With Dementia Type Visual hallucinations are more common in Diffuse Lewy Body Dementia Disinhibition symptoms occur early in the some of the Frontotemporal Dementias Earlier onset of behavioral symptoms has been described in Huntington s chorea, Creutzfeldt-Jacob disease and Pick s disease
13 Symptom Complexes of BPSD Psychosis Depression Agitation Anxiety Altered circadian rhythms
14 Psychosis in BPSD
15 Diagnostic Criteria for Psychosis of AD Characteristic symptoms Presence of one or more of the following symptoms: visual or auditory hallucinations delusions Primary diagnosis All the criteria for dementia of the Alzheimer type are met * *For other dementias, such as vascular dementia, Criterion B will need to be modified appropriately. Jeste, Finkel 2000
16 Diagnostic Criteria for Psychosis of AD Chronology of the onset of symptoms of psychosis Vs onset of symptoms of dementia There is evidence from the history that the psychotic symptoms have not been present continuously since prior to the onset of dementia.
17 Diagnostic Criteria for Psychosis of AD Duration and severity The psychotic symptom(s) have been present, at least intermittently, for 1 month or longer. Symptoms are severe enough to cause some disruption in patients and/or others functioning.
18 Diagnostic Criteria for Psychosis of AD Exclusion of schizophrenia and related psychotic disorders Criteria for schizophrenia, schizoaffective disorder, delusional disorder or mood disorder with psychotic features, have never been met. Relationship to delirium The disturbance does not occur exclusively during the course of a delirium. Exclusion of other causes of psychotic symptoms. The disturbance is not better accounted for by another general medical condition or direct physiological effects of a substance (e.g. drug abuse, a medication). Jeste, Finkel 2000
19 Differential Diagnosis of Psychosis of AD Vs Psychosis of Schizophrenia in the Elderly Psychosis of AD Schizophrenia Bizarre or complex delusions Rare Frequent Misidentifications of caregivers Frequent Rare Common form of hallucinations Visual Auditory Schneiderian first-rank symptoms Rare Frequent Active suicidal ideation Rare Frequent Past history of psychosis Rare Frequent Jeste, Finkel 2000
20 Differential Diagnosis of Psychosis of AD Vs Psychosis of Schizophrenia in the Elderly-2

21 Depression in BPSD
22 Prevalence of Depression in Dementia Depression has long been recognized as a major co-morbidity of dementia syndromes. Prevalence of depression in AD 0%-20%, but lacking diagnostic criteria specific for depression in dementia, most studies report prevalence of depressive symptoms Prevalence rates in Vascular Dementia 19% - 43%
23 Depression as the First Sign of Dementia Patients initially diagnosed with depressive pseudodementia or "reversible dementia" may not achieve complete cognitive recovery following remission of depression. An average of 11-23% of patients with initially reversible dementia become irreversibly demented every year Irreversible dementia begins to be diagnosed about two years after the initial recovery from depression
24 Clinical Characteristics of Depression in BPSD Depressive symptoms in dementia patients often fluctuate Depressed patients with AD exhibited more selfpity, rejection sensitivity, anhedonia and psychomotor disturbance than depressed older patients without dementia. Major depression in DAT is associated with an increased mortality rate, but no acceleration of cognitive decline.
25 Etiology of Depression in Dementia Major depression in AD has been associated with: increased degeneration of brainstem aminergic nuclei, particularly the locus coeruleus Relative preservation of the cholinergic nucleus basalis of Meynert No increase in the numbers of senile plaques or neurofibrillary tangles in the neocortex or allocortex Modest decreases in the levels of serotonin and 5-HIAA Environmental and psychosocial factors

26 Circadian Rhythm Disturbances
27 Circadian Rhythm Disturbances-1 Disturbances of sleep and day-night reversals are common Sleep disturbances may be more common in certain dementias, such as vascular dementia, Lewy Body dementia and supranuclear palsy, compared to those found in Alzheimer s disease Aldrich, Foster, et al Aharon-Peretz, Masiah, et al Boeve et al., 2001

28 Normal circadian rhythm
29 Circadian Rhythm Disturbances Functional and anatomic changes occur in the suprachiasmatic nucleus in dementias Alterations of the daily rhythm of serum melatonin have been correlated to some cases of sleep disturbances in Alzheimer s disease Stopa, Volicer, et al Uchida, Okamoto, et al. 1996
30 Circadian Rhythm Disturbances Nonpharmacologic therapies include: keeping patients awake during the day with various external stimuli sometimes structuring short nap after lunch to avoid sundowning early evening activities stimulus control at night white noise bright light exposure Jean-Louis, Zizi, et al. 1998
31 Circadian Rhythm Disturbances Pharmacologic interventions include melatonin, nonbenzodiazepine hypnotics e.g. zolpidem, benzodiazepines, trazodone Caregiver interventions include: educational programs, respite, and assistance with their own sleep needs Jean-louis, Zizi, et al Lyketos, Veiel et al Ohashi, Okamoto, et al Shelton and Hocking 1997 Van Someren, Kessler, et al. 1997

32 Circadian Rhythm Disturbances

33 Agitation in BPSD
34 Agitation Some patients have symptoms that do not neatly fit into the better defined symptom complexes of BPSD (e.g. psychosis, depression or anxiety). Koss, Weiner, et al Agitation can be defined as inappropriate verbal, vocal or motor activity that is not judged by an outside observer to result directly from the needs or confusion of the person Cohen-Mansfield and Billig, 1986
35 Agitation Symptoms - I Physically Non-Aggressive General Restlessness Repetitive Mannerisms Pacing Hiding Objects Inappropriate Handling Shadowing Escaping protected environment Inappropriate Dressing/Undressing Cohen-Mansfield, 1989
36 Agitation Symptoms - II Physically Aggressive Hitting Pushing Scratching Grabbing Kicking Biting Spitting Cohen-Mansfield, 1989
37 Agitation Symptoms - III Verbally Non-Aggressive Negativism Chanting Repetitive Sentences Constant Interruptions Constant Requests for Attention Cohen-Mansfield, 1989
38 Agitation Symptoms - IV Verbally Aggressive Screaming Cursing Temper Outbursts Socially Inappropriate Commentary Cohen-Mansfield, 1989
39 Agitation treatment-1
40 Agitation treatment-2
41 Disinhibition Syndrome Impulsive and inappropriate behaviors Emotionally unstable Poor insight and judgement
42 Disinhibition Syndrome (continued) Symptoms include crying, euphoria, verbal aggression, physical aggression, self-destructive behavior, sexual disinhibition, intrusiveness, wandering, shoplifting, impulse buying and other unrestrained behaviors
43 Aggression 12% of patients showed aggressive episodes (5% with verbal aggression, 7% with physical aggression) during the preceding 4 weeks Physical aggression is significantly associated with more frequent delusions and more severe irritability Chemerinski E et.al., 1998
44 Aggression Symptom complexes include: Aggression associated with delirium Aggression associated with depression Aggression associated with psychosis Spontaneous disinhibited aggression Reactive aggression associated with personal care, discomfort
45 Catastrophic Reactions Sudden, excessive emotional response or physical behavior Occur in approximately 40% of mildmoderately impaired dementia patients During neuropsychological evaluation, 16% of dementia patients demonstrated catastrophic reactions Can be precipitated by other BPSD such as misperception, hallucinations or delusions
46 Anxiety Symptoms in BPSD
47 Clinical Characteristics of Anxiety Symptoms No specific definition of anxiety in BPSD is available The most common clinical forms are: Generalized Anxiety Disorder type symptoms Godot syndrome repeatedly asking questions on a forthcoming event Fear of being left alone Pacing Wringing of hands, fidgeting Chanting
48 Possible Biological Correlates of Anxiety Symptoms in Dementia Decrease concentration of 5-HT and 5-HIAA in cortex, basal ganglia and brainstem Neuronal loss in raphe nucleus Decrease in GABA activity Nazarali et al,1992 Reinikainen et al, 1988
49 Ham-A Items that Differentiate Between AD-GAD and AD-Controls Anxious Mood Tension Fears Insomnia Muscular Symptoms Somatic Symptoms Cardiovascular Symptoms Respiratory Symptoms Gastrointestinal Symptoms Autonomic Symptoms Chemerinsky E, Petraca G, Manes F et al, 1998
50 Treatment of BPSD
51 Treatment of BPSD Patients with BPSD should be evaluated for delirium. Consider changes in environment, medication, fecal impaction, pneumonia, urinary infection, etc. Evaluate for needs that the dementia patient is unable to communicate normally e.g. pain Behavioral management or situational manipulation are the initial strategies of choice for mild to moderate BPSD. Pharmacological interventions are useful if symptoms are severe or do not respond to nonpharmacologic strategies alone
52 BPSD: Nonpharmacologic Therapy Environmental modifications such as music, white noise, plants, animals Speak slowly, keep commands simple and positive, use gestures, gentle touch Behavioral management techniques Structured activities and use of schedules Massage, exercise Rowe, Alfred 1999 Gerdner, Swanson 1993
53 If Pharmacological Therapy Is Needed: Look for symptom complexes such as depression, psychosis or anxiety to guide initial choice of agent If enlightened empiric therapy is needed, chose agents that minimize side-effect potential and maximize chance of efficacy In most situations, medications should be given in lower doses than are typically recommended for an adult population. However, it is noteworthy that the elderly are heterogeneous and the range of medication dosage is substantial Ideally, use agents with demonstrable efficacy as first line agents
54 Treatment options Identify cause Wait and see Education and counselling Prophylaxis Environmental modification Direct behavioural approaches Medication
55 Course and Presentation of Depression in Dementia Some research suggests that depression in older adults with dementia tends to increase as cognitive decline progresses. Other research indicates a higher prevalence of depression in the early stages of dementia, with diminished prevalence as cognitive function becomes severely impaired and insight is lost. Apathy is related to a higher frequency of both minor and major depression.
56 Consequences of Depression in Older Adults with Dementia Persons with pre-existing depression have about double the risk of developing subsequent dementia that those without a history of depression have. Depression may be a risk factor for progression from MCI to dementia. Depression in persons with MCI or dementia has been linked with increased severity of cognitive deficits.
57 Consequences of Depression in Older Adults with Dementia Co-morbid cognitive impairment and depression associated with other negative consequences, e.g., increased risk of death, reduced quality of life; reports from dementia patients and their caregivers. Although suicide attempts observed in < 1% of dementia patients, suicidal ideation, intent, passive death wishes, and feelings that life is not worth living reported in up to 42% of dementia patients, particularly those with depression.
58 Treatment of Depression in Dementia: Pharmacotherapy Pharmacotherapy Depression more likely to respond to medication than other BPSD. Pharmacological treatment of depression in dementia challenging due to the high level of comorbidity, use of multiple medications and risk of drug interactions, physical and cognitive frailty, and impaired ability to communicate among older adults with dementia.
59 Treatment of Depression in Dementia: Pharmacotherapy Pharmacotherapy Antidepressants: Older adults with depression in dementia respond to tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs). Significant declines in cognitive scores are seen in individuals taking TCAs. At this time SSRIs are the preferred treatment for depression in older adults with dementia.
60 Treatment of Depression in Dementia: Pharmacotherapy Antipsychotics: Different antipsychotic drugs have been used with varying degrees of success in treating BPSD, including depression. Older adults with dementia are at high risk for developing extrapyramidal symptoms (EPS), such as Parkinsonism and tardive dyskinesia. Atypical antipsychotic drugs, such as rispiridone and olanzepine,, have significant, though modest, effects and reduced risk of EPS at lower doses. However, there have been reports of increased risk of strokes and mortality with these drugs, though there is controversy about the degree of this risk or even whether there is any.
61 Treatment of Depression in Dementia: Pharmacotherapy Memory enhancers: Cholinesterase inhibitors are used to treat both the cognitive deficits of dementia and BPSD. Positive effects have been found for rivastigmine in patients with a wide range of dementia. Apathy and anxiety are among the behavioral domains demonstrating the most consistent positive response. Memantine has been found to improve cognitive functioning as well as psychological symptoms of dementia (such as depression).
62 Treatment of Depression in Dementia: Pharmacotherapy Other medications: Anticonvulsant drugs, such as valproate and lamotrigene,, have yielded some positive findings, though there is insufficient research to support conclusions about the effectiveness of this type of medications. Some support for the effectiveness of a gingko biloba extract for improving cognitive functioning and enhancing mood among older adults with dementia and BPSD, though there is controversy about the effectiveness of this intervention.
63 Treatment of Depression in Dementia: Non-pharmacological treatments Clinical guidelines Use of nonpharmacological treatments for BPSD before pharmacological treatments are tried.
64 Treatment of Depression in Dementia: Non-pharmacological treatments Emotion-oriented therapies Reality Orientation groups were originally intended to reduce confusion by giving repeated orientation clues, e.g., the time of day, date, and season, but this was only partially successful. Research has suggested that the main benefits were the stimulation of the social group and the positive impact on staff, who acquired a better knowledge of the residents and their earlier lives and interests.
65 Treatment of Depression in Dementia: Non-pharmacological treatments Emotion-oriented therapies Reminiscence Therapy encourages persons with dementia to talk about their pasts, and may utilize audiovisual aids such as old family photos and objects to retrieve positive events and emotions. Reminiscence provides a chance to interact positively with others, can enhance individuals' sense of identity, sense of worth, or general well-being, and may also stimulate memory processes.
66 Treatment of Depression in Dementia: Non-pharmacological treatments Cognitive and behavioral therapies Behavior therapy requires a period of detailed assessment in which the personal triggers, behaviors, and reinforcers are identified, and their relationships made clear to the patient. While a number of studies have demonstrated the effectiveness of behavior therapy for behavioral symptoms of dementia, there is limited support for it effectiveness in reducing the symptoms of depression.
67 Treatment of Depression in Dementia: Non-pharmacological treatments Cognitive and behavioral therapies Cognitive behavioral interventions. Several small-studies and case reports have demonstrated the effectiveness of group and individual cognitive behavioral techniques, such as distraction, relaxation, and cognitive restructuring,, in reducing symptoms of depression in individuals with early stages of dementia. However, there have been no large- scale trials of CBT in this population.
68 Treatment of Depression in Dementia: Non-pharmacological treatments Cognitive and behavioral therapies Scientific evidence for cognitive and behavioral therapies is somewhat stronger than that for emotion-oriented therapies. Results of a few randomized trials were consistent and showed benefits as compared to control groups, and outcome effects on depression reductions were maintained over time.
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL
 TOOL") DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
Management of the Acutely Agitated Long Term Care Patient
 Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care
 Summary document for Primary Care") Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego
 Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Pharmacological Treatment of Aggression in the Elderly
 Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Introduction to Dementia: Complications
 Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Behavioral Management in Dementia. a.k.a. Public Enemy Number One a.k.a. Proteins Gone Bad
 Behavioral Management in Dementia a.k.a. Public Enemy Number One a.k.a. Proteins Gone Bad Game Plan 1. Definition 2. Epidemiology 3. Assessment: IT S OVER 4. Nonpharmacologic Strategies: 4 S 5. Nonpharmacologic:
Behavioral Management in Dementia a.k.a. Public Enemy Number One a.k.a. Proteins Gone Bad Game Plan 1. Definition 2. Epidemiology 3. Assessment: IT S OVER 4. Nonpharmacologic Strategies: 4 S 5. Nonpharmacologic:
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Dementia is a common neuropsychiatric disorder characterized by progressive impairment of
 Focused Issue of This Month Diagnosis and Treatment for Behavioral and Psychological Symptoms of Dementia Byoung Hoon Oh, MD Department of Psychiatry, Yonsei University College of Medicine E - mail : drobh@yuhs.ac
Focused Issue of This Month Diagnosis and Treatment for Behavioral and Psychological Symptoms of Dementia Byoung Hoon Oh, MD Department of Psychiatry, Yonsei University College of Medicine E - mail : drobh@yuhs.ac
Depressive and Bipolar Disorders
 Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Management of Behavioral Symptoms in Dementia. Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal
 Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches
 Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
A Comparison between Anxious-Depressive Disorders of Stroke and Multiple Sclerosis Patients, Evaluated with Specific Twin Scales
 A Comparison between Anxious-Depressive Disorders of Stroke and Multiple Sclerosis Patients, Evaluated with Specific Twin Scales The Post Stroke Depression Rating Scale The examiner must choose for each
A Comparison between Anxious-Depressive Disorders of Stroke and Multiple Sclerosis Patients, Evaluated with Specific Twin Scales The Post Stroke Depression Rating Scale The examiner must choose for each
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Welcome to the Medication Safety Community of Practice Webinar Series
 Welcome to the Medication Safety Community of Practice Webinar Series Hosted by ISMP Canada March 21, 2012 Opportunities for Quality Improvement: Contemporary Issues in the Use of Psychotropic Medications
Welcome to the Medication Safety Community of Practice Webinar Series Hosted by ISMP Canada March 21, 2012 Opportunities for Quality Improvement: Contemporary Issues in the Use of Psychotropic Medications
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Managing agitation in dementia using non-pharmacological therapies
 Managing agitation in dementia using non-pharmacological therapies Gill Livingston Lynsey Kelly, Elanor Lewis-Holmes, Gianluca Baio, Rumana Omar, Stephen Morris, Nishma Patel, Cornelius Katona, Claudia
Managing agitation in dementia using non-pharmacological therapies Gill Livingston Lynsey Kelly, Elanor Lewis-Holmes, Gianluca Baio, Rumana Omar, Stephen Morris, Nishma Patel, Cornelius Katona, Claudia
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Chapter 15: Late Life and Psychological Disorders
 \ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
\ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care
 in Primary Care") Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care Dr. John Puxty Ontario s Ontario s Strategy Strategy for Alzheimer for Disease and Related Dementia: Initiative #2, #2, Physician
Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care Dr. John Puxty Ontario s Ontario s Strategy Strategy for Alzheimer for Disease and Related Dementia: Initiative #2, #2, Physician
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Behavior Problems: in Long Term Care and Assisted Living
 Behavior Problems: Dementia and Mental Illness in Long Term Care and Assisted Living Module I Dr. David A. Smith, M.D., FAAFP, CMD mmlearn.org is a program of Morningside Ministries Cell Phones and Pagers
Behavior Problems: Dementia and Mental Illness in Long Term Care and Assisted Living Module I Dr. David A. Smith, M.D., FAAFP, CMD mmlearn.org is a program of Morningside Ministries Cell Phones and Pagers
GENI Jeopardy: Geriatric Mental Health. Part of the brain responsible for executive functioning
 GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Psychotic disorders Dr. Sarah DeLeon, MD PGYIV, Psychiatry ConceptsInPsychiatry.com
 Psychotic disorders Dr. Sarah DeLeon, MD PGYIV, Psychiatry ConceptsInPsychiatry.com Introduction Psychotic spectrum disorders include schizotypal personality disorder, delusional disorder, brief psychotic
Psychotic disorders Dr. Sarah DeLeon, MD PGYIV, Psychiatry ConceptsInPsychiatry.com Introduction Psychotic spectrum disorders include schizotypal personality disorder, delusional disorder, brief psychotic
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Responsive Behaviours in the Dining Room
 How BSO and Dietary Can Work Together Responsive Behaviours in the Dining Room April 5, 2016 TWC Culinary and Nutrition Summit Teresa Tibbo RPN, Twinkle Patel RD Seasons Care Dietitian Network Carol Donovan,
How BSO and Dietary Can Work Together Responsive Behaviours in the Dining Room April 5, 2016 TWC Culinary and Nutrition Summit Teresa Tibbo RPN, Twinkle Patel RD Seasons Care Dietitian Network Carol Donovan,
Depression in the Eldery Handout Package
 Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia: Managing Difficult Behaviors. No conflicts of interest. Off-label medication use will be discussed during this talk.
 Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Lewy Body Disease. Dementia Education for the First Responder July 27, 2017
 Lewy Body Disease Dementia Education for the First Responder July 27, 2017 Dylan Wint, M.D. NV Energy Chair for Brain Health Education Cleveland Clinic Lou Ruvo Center for Brain Health OUTLINE Lewy body
Lewy Body Disease Dementia Education for the First Responder July 27, 2017 Dylan Wint, M.D. NV Energy Chair for Brain Health Education Cleveland Clinic Lou Ruvo Center for Brain Health OUTLINE Lewy body
Subject Index A abuse 18, 38 active ageing 16, 17, 19, 44 activity of daily living 17 ADI (Alzheimer s Disease International) 45 advance care-planning
 45 advance care-planning") Subject Index A abuse 18, 38 active ageing 16, 17, 19, 44 activity of daily living 17 ADI (Alzheimer s Disease International) 45 advance care-planning 118, 120 African medicine 92 ageing active ageing
Subject Index A abuse 18, 38 active ageing 16, 17, 19, 44 activity of daily living 17 ADI (Alzheimer s Disease International) 45 advance care-planning 118, 120 African medicine 92 ageing active ageing
Every 67seconds, someone will develop Alzheimer's.
 We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D.
 HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
HDSA welcomes you to Caregiver s Corner. Funded by an educational grant from
 HDSA welcomes you to Caregiver s Corner Funded by an educational grant from Caregiver s Corner Webinar, DATE Managing Psychiatric Symptoms Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics
HDSA welcomes you to Caregiver s Corner Funded by an educational grant from Caregiver s Corner Webinar, DATE Managing Psychiatric Symptoms Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Stroke and Behaviour Change
 Stroke and Behaviour Change Kathy Baker BA (Psych), BScN, MAL (Health) Mary-Lou Nolte, Ph.D., C. Psych. Objectives Describe relationships among cognition, mood and behaviour change after stroke Describe
Stroke and Behaviour Change Kathy Baker BA (Psych), BScN, MAL (Health) Mary-Lou Nolte, Ph.D., C. Psych. Objectives Describe relationships among cognition, mood and behaviour change after stroke Describe
Let s s talk about behaviour
 Let s s talk about behaviour Common Terms: Coma Restless Agitated Disoriented Confused Disinhibition Disrupted sleep cycle Amnestic Combative Inappropriate Vocalizing Some less accurate terminology Rude
Let s s talk about behaviour Common Terms: Coma Restless Agitated Disoriented Confused Disinhibition Disrupted sleep cycle Amnestic Combative Inappropriate Vocalizing Some less accurate terminology Rude
DEMENTIA AND MANAGING BEHAVIORS
 DEMENTIA AND MANAGING BEHAVIORS Dementia is a general term that describes a group of similar symptoms caused by temporary or permanent damage to the brain or neurons. Memory loss Judgment Language Complex
DEMENTIA AND MANAGING BEHAVIORS Dementia is a general term that describes a group of similar symptoms caused by temporary or permanent damage to the brain or neurons. Memory loss Judgment Language Complex
Drugs used to relieve behavioural and psychological symptoms in dementia
 alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
Psychosis and Agitation in Dementia
 Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Anxiety Disorders. Theories: Anxiety Disorders (cont'd) 10/2/2014
 10/2/2014") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
Dementia Training Session for Carers. By Dr Rahul Tomar Consultant Psychiatrist
 Dementia Training Session for Carers By Dr Rahul Tomar Consultant Psychiatrist Dementia in the UK: Facts & Figures National Dementia strategy launched in 2009 800,000 people living with dementia (2012)
Dementia Training Session for Carers By Dr Rahul Tomar Consultant Psychiatrist Dementia in the UK: Facts & Figures National Dementia strategy launched in 2009 800,000 people living with dementia (2012)
12/17/2012. Unnecessary Drugs
 Nursing Home Social Work Webinar Series December 19, 2012 Dr. Robin P. Bonifas, PhD, MSW Arizona State University School of Social Work Importance of familiarity with psychotropic medication regulations.
Nursing Home Social Work Webinar Series December 19, 2012 Dr. Robin P. Bonifas, PhD, MSW Arizona State University School of Social Work Importance of familiarity with psychotropic medication regulations.
6/22/2012. Co-morbidity - when two or more conditions occur together. The two conditions may or may not be causally related.
 Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Pharmacological Management of Dementia-Related Behaviors
 Welcomes You To Pharmacological Management of Dementia-Related Behaviors Presented by Brett Lu, MD, PhD Associate Professor of Psychiatry John A. Burns School of Medicine September 5, 2017 10:00 11:00
Welcomes You To Pharmacological Management of Dementia-Related Behaviors Presented by Brett Lu, MD, PhD Associate Professor of Psychiatry John A. Burns School of Medicine September 5, 2017 10:00 11:00
2/9/2018. Certificate of Completion: Pharmacological Management of Dementia Related Behaviors. Welcomes You To
 Welcomes You To Pharmacological Management of Dementia Related Behaviors Presented by Brett Lu, MD, PhD Associate Professor of Psychiatry John A. Burns School of Medicine September 5, 2017 10:00 11:00
Welcomes You To Pharmacological Management of Dementia Related Behaviors Presented by Brett Lu, MD, PhD Associate Professor of Psychiatry John A. Burns School of Medicine September 5, 2017 10:00 11:00
Bipolar and Affective Disorders. Harleen Johal
 + Bipolar and Affective Disorders Harleen Johal hkj1g11@soton.ac.uk + Affective (mood) disorders n Depression n Bipolar disorder n Anxiety n Treatment + Depression: Definition n Pervasiveand persistent
+ Bipolar and Affective Disorders Harleen Johal hkj1g11@soton.ac.uk + Affective (mood) disorders n Depression n Bipolar disorder n Anxiety n Treatment + Depression: Definition n Pervasiveand persistent
These conditions can have similar and overlapping symptoms, and many of them can only be diagnosed with certainty by autopsy of the brain.
 Progression MIDDLE STAGE This document is one in a five-part series on the stages of Alzheimer s disease and is written for the person with the disease, their family 1 and caregivers. The middle stage
Progression MIDDLE STAGE This document is one in a five-part series on the stages of Alzheimer s disease and is written for the person with the disease, their family 1 and caregivers. The middle stage
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Assessment and management of behavioral and psychological symptoms of dementia
 Assessment and management of behavioral and psychological symptoms of dementia Helen C Kales, 1 2 3 Laura N Gitlin, 4 5 6 Constantine G Lyketsos 7 1 Section of Geriatric Psychiatry, Department of Psychiatry,
Assessment and management of behavioral and psychological symptoms of dementia Helen C Kales, 1 2 3 Laura N Gitlin, 4 5 6 Constantine G Lyketsos 7 1 Section of Geriatric Psychiatry, Department of Psychiatry,
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Mental illness A Broad Overview. Dr H Pathmanandam March 2017
 Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Announcements. The final Aplia gauntlet: Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+
 The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Managing Challenging Behaviors
 Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine & Lorin M. Scher, MD Attending Psychiatrist, HDSA Center of Excellence UC
Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine & Lorin M. Scher, MD Attending Psychiatrist, HDSA Center of Excellence UC
Evidence for the effectiveness of a sensory garden in improving the quality of life of people with dementia and prominent negative experience
 Evidence for the effectiveness of a sensory garden in improving the quality of life of people with dementia and prominent negative experience Bernie McCarthy MAPS McCarthy Psychology Services Acknowledgements
Evidence for the effectiveness of a sensory garden in improving the quality of life of people with dementia and prominent negative experience Bernie McCarthy MAPS McCarthy Psychology Services Acknowledgements
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Managing Challenging Behaviors
 Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine In partnership with Drs. Lorin Scher, MD and Vicki Wheelock, MD 1 Our Goal
Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine In partnership with Drs. Lorin Scher, MD and Vicki Wheelock, MD 1 Our Goal
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations
 Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Brief Notes on the Mental Health of Children and Adolescents
 Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES
 FACULTY DEVELOPMENT MASTERWORKS SERIES") UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
To gather information related to psychological and social factors including: Behavior and emotions and symptoms of diseases Addictions
 Psychosocial About this Domain (Psychosocial) To gather information related to psychological and social factors including: Behavior and emotions and symptoms of diseases Addictions To identify potential
Psychosocial About this Domain (Psychosocial) To gather information related to psychological and social factors including: Behavior and emotions and symptoms of diseases Addictions To identify potential
N.C. Nurse Aide I Curriculum MODULE T. Dementia and Alzheimer s Disease. DHSR/HCPR/CARE NAT I Curriculum - July
 N.C. Nurse Aide I Curriculum MODULE T Dementia and Alzheimer s Disease DHSR/HCPR/CARE NAT I Curriculum - July 2013 1 Objectives Define the terms dementia, Alzheimer s s disease, and delirium. Describe
N.C. Nurse Aide I Curriculum MODULE T Dementia and Alzheimer s Disease DHSR/HCPR/CARE NAT I Curriculum - July 2013 1 Objectives Define the terms dementia, Alzheimer s s disease, and delirium. Describe
Current Treatments for Dementia and Future Prospects. James Warner St Charles Hospital, London
 Current Treatments for Dementia and Future Prospects James Warner St Charles Hospital, London Dementia Cognitive Non-cognitive (BPSD) Memory orientation language other cognitive abilities praxis planning
Current Treatments for Dementia and Future Prospects James Warner St Charles Hospital, London Dementia Cognitive Non-cognitive (BPSD) Memory orientation language other cognitive abilities praxis planning
ADRC Dementia Care Training. Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium
 ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
Dementia Information Kit for HACC Workers
 Dementia Information Kit for HACC Workers This presentation has been compiled as part of the Loddon Mallee region Dementia Management Strategy project in 2002 and revised in 2008 to assist HACC workers
Dementia Information Kit for HACC Workers This presentation has been compiled as part of the Loddon Mallee region Dementia Management Strategy project in 2002 and revised in 2008 to assist HACC workers
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
MODULE III Challenging Behaviors
 Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident MODULE III Challenging Behaviors S WEHRY 2004 Objectives: Part One Describe principles of communication Describe behavior as
Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident MODULE III Challenging Behaviors S WEHRY 2004 Objectives: Part One Describe principles of communication Describe behavior as
Mental Health Nursing: Organic Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Depressive, Bipolar and Related Disorders
 Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
Deidre Pye MClinPsych Senior Behaviour Consultant Dementia Behaviour Management Advisory Service (Qld)
") Deidre Pye MClinPsych Senior Behaviour Consultant Dementia Behaviour Management Advisory Service (Qld) Not about reinventing the wheel Processes May feel uncomfortable or challenged by different ideas
Deidre Pye MClinPsych Senior Behaviour Consultant Dementia Behaviour Management Advisory Service (Qld) Not about reinventing the wheel Processes May feel uncomfortable or challenged by different ideas