Suicide Risk Assessment, Management and Documentation
|
|
|
- Laura Shana O’Connor’
- 5 years ago
- Views:
Transcription


1 Suicide Risk Assessment, Management and Documentation JIMMIE D. MCADAMS, DO DFAPA Laureate Psychiatric Clinic and Hospital Director Senior Behavioral Health Jeff Mitchell, M.D. Matthew Meyer, M.D. Phillip Leon, M.D. Scott Grantham, M.D. 1
2 1. Identify essential elements in a risk assessment 2. Identify the most important times in an episode of care when risk should be assessed and documented 3. Identify the key elements in risk assessment documentation 10 th ranking cause of death in U.S. overall 2 nd ranking cause of death ages /100,000 in 2013 Rate is gradually increasing (12.9/100,000 in 2012) 1:64 Americans is a survivor of suicide Rate in men remains roughly 3.5 times that in women (although women attempt more often) Highest rate in the years of age group 2

3 g_causes_of_death_by_age_group_2014 a.pdf 3
4 4
5 5

6 6
 Drug overdose deaths have")


7 17.3/100,000 Rate decreased (17.6/100,000 in 2012) Drug overdose deaths have risen 470 deaths in deaths in deaths in 2013 Most involved prescription drugs Drug overdose deaths outnumber motor vehicle fatalities in Oklahoma 2014* 731 suicides in Oklahoma per ME 7
 Conduct a risk assessment that identifies specific patient characteristics and environmental features that may increase or decrease the risk for suicide.")
8 Johnston County 26.57/100,000 Tulsa County 16.68/100,000 Oklahoma County 15.26/100,000 Woods County 7.41/100,000 1) Conduct a risk assessment that identifies specific patient characteristics and environmental features that may increase or decrease the risk for suicide. 2) Address the patient s immediate safety needs and most appropriate setting for treatment. 3) When a patient at risk for suicide leaves the care of the hospital, provide suicide prevention information (such as a crisis hotline) to the patient and his or her family. 8
9 The rate is too low, even in psychiatric populations For example, the highest risk group, previous suicide attempters, has a risk of committing suicide some time within the next year of 0.5% No method of suicide risk assessment can reliably identify who will commit suicide (sensitivity) and who will not (specificity). But risk can be assessed and stratified Suicide is the result of multiple factors, including diagnosis (psychiatric and medical), psychodynamic, genetic, familial, occupational, environmental, social, cultural, existential, and chance factors. The overall purpose is to identify modifiable and treatable risk and protective factors that inform the patient s overall treatment and management requirements. Help determine the need for immediate measures Help determine level of care needed (IPT/IOP/OPT) Develop a treatment plan that enhances protective factors and mitigates risk factors 9
 Onset of physical illness (especially life threatening, disfiguring, associated with severe pain,")

10 Crisis evaluation Intake evaluation (inpatient or outpatient) After a suicide attempt Patient s mental status / conditions / presentation makes an abrupt change (better or worse) Family, others report change in behavior, suicidal thoughts or behaviors Change in observation status (1:1, SP) Onset of physical illness (especially life threatening, disfiguring, associated with severe pain, or loss of executive functioning) Anticipation or experience of a significant interpersonal loss or psychosocial stressor Prior to discharge Current presentation of suicidality Presence of psychiatric disorder Pertinent history especially suicidal behaviors Psychosocial situation Support Employment Religious/cultural issues Coping skills Impulsiveness Insight Past responses to stress 10
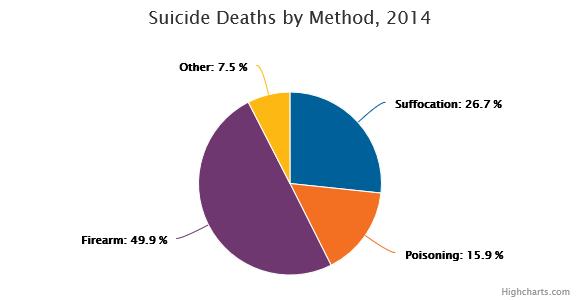
11 Suicidal Thoughts Frequency Intensity Psychotic features e.g., voices Suicidal Plans Frequency Intensity Lethality (expectation of lethality) Access/feasibility (e.g., guns in home, med stockpile) Suicidal Behaviors Rehearsing Attempts Suicidal Intent Substance use in current presentation Presence of hopelessness, anhedonia, panic attacks The likelihood that a particular method will succeed May be different than the perception of lethality Guns, hanging Overdose depends on the substance Acetaminophen, aspirin Insulin, beta blockers Tricyclic antidepressants, lithium Drug/ETOH combinations Assess access to means and document plans to restrict access 11

 Taking steps to avoid detection (waiting for spouse to leave) Giving away possessions Writing will Saying goodbye Suicide note Disorder SMR (SMR of")
12 Planning the act Plan is detailed (e.g., time, place, etc) Plan/method is feasible, realistic Means are available Means are lethal (gun, hanging, toxic drugs/chemicals, etc) Practicing/rehearsing the act (putting gun to head) Taking steps to enact (buying a gun, hoarding pills) Taking steps to avoid detection (waiting for spouse to leave) Giving away possessions Writing will Saying goodbye Suicide note Disorder SMR (SMR of general population is 1) Prior Suicide Attempts Bipolar II 24.1 Bipolar I 17.1 Major Depression Eating Disorders Opioid Abuse Obsessive Compulsive Disorder Panic Disorder Schizophrenia 8.45 Personality Disorders 7.08 AIDS 6.58 Epilepsy 5.11 Spinal Cord Injury 3.82 Intellectual Disability 0.88 SMR: standard mortality ratio 12
 Physical or sexual abuse Family history of suicide, particularly in first degree relatives")
13 Hopelessness Psychic Pain Severe or unremitting anxiety Impulsiveness Sleep disturbance Substance abuse Shame or humiliation Loss of executive function Polarized, black and white thinking Agitation Panic Attacks Cluster B Personality (use suicide as a coping skill) Physical or sexual abuse Family history of suicide, particularly in first degree relatives 13
 presence (+)/absence of external supports quality of family relationships (+/ ) Cultural/religious beliefs about death or suicide (+) Pregnancy (+) Sense of responsibility")
14 Acute psychosocial crises losses financial difficulties family discord/domestic violence sexual or physical abuse Employment status Living situation lack of social support (including living alone) children in the home (+) presence (+)/absence of external supports quality of family relationships (+/ ) Cultural/religious beliefs about death or suicide (+) Pregnancy (+) Sense of responsibility (+) Positive therapeutic relationship (+) Positive problem solving skills and coping skills (+) Reality testing ability (+) Protective factors are those features that counteract the risk factors May be instrumental in the decision to hospitalize/not hospitalize A patient may have many risk factors, but strong protective factors can result in a referral for outpatient services 14
15 Sources of collateral information Potential protective factors Potential risk factors (abuse, toxic relationships) Potential participants in safety planning Patient safety is most important Attempt to get consent Document reasoning and risk The burden of proof for involuntary detention is reason to believe 15
16 Hospitalization? No formula/written standard Risk factors outweigh protective factors Less restrictive options Partial hospitalization: patient has acute symptoms, but good support system Intensive outpatient therapy: patient must be motivated and have adequate resources Outpatient appointment within 7 days Safety plan Agreement to call if in crisis Follow up/no show calls Major Weaknesses of the Suicide Prevention Contract Contracts NOT legally binding Do not protect against legal liability Lack of evidence based support APA: overvalued as a clinical or risk management technique May result in false confidence about patient safety 16
17 Seriously mentally ill patient in acute stages of illness not likely competent to enter into contract Recently admitted inpatient unlikely to have trusting therapeutic relationship with contracting clinician Ignores fundamental understanding of the suicidal mind eg., fraught with ambivalence, difficulty making decisions, distorted judgment Asks the fragile/vulnerable patient to bear the burden of a life threatening responsibility Patient determined to commit suicide views staff as adversary, not ally Joint effort with MH professional, patient, support system when available Elements Reasons for living Removal of means for self harm Description of support system Resources, coping skills patient will use to manage suicidal thoughts urges Follow up, urgent care Plan for what patient will do if these don t work Professional s judgment about the sincerity and thought that goes into the plan can be an assessment factor 17

18 If in doubt, assess the patient Your office Clinical Assessment Department (CAD) Home based assessment (COPES) Unmodifiable risk factors e.g., demographic variables, history of suicide in family, abuse history, financial troubles, unemployment status, others Modifiable risk factors e.g., hopelessness, suicidal thoughts, agitation, anxiety, insomnia, purposelessness, lack of support 18

19 Assess the need for higher level of care The more risk factors, the more you need to address modifiable factors and fortify protective factors Document that you considered these in your assessment of risk legal ramifications: it demonstrates that you provided a thorough screening Caveat: it is impossible to assess all risk factors listed in APA Guidelines, but document all the ones you did assess Anxiety Agitation Hopelessness (correlates more with risk than depression) Insomnia (correlates with suicide risk in mood disorders) Mood lability Hallucinations Delusions Withdrawal symptoms Access to lethal means (guns, pills) 19
20 Short term risk factors are predominantly severe, anxiety driven, and treatable panic attacks psychic anxiety loss of pleasure and interest alcohol abuse diminished concentration insomnia Assess (and document) suicidality on a daily basis Mood status, changes Psychomotor activity Commitment to safety planning Reasons for living Hopefulness Plans or future Status of protective factors Status of modifiable risk factors 20
21 Good care, followed by good documentation, is your best malpractice defense If your patient is in crisis or on an inpatient acute unit, document changes (or lack thereof) in risk at every encounter Assess/document risk at critical junctures in care Patient leaves inpatient unit Lower precaution level Discharge follow up appointment in clinic Suicidal ideation reported, but patient not admitted We are usually good at documenting what we saw and what we did We are generally not as good at documenting why we did the things we did: Why did we let the patient leave the office, leave the unit, move to a lower precaution level? What we write is more important than how much we write 21
22 The only suicidal person is a person who is in the act of attempting suicide. Short of that, he is a person at risk for suicide because of his thoughts or behaviors. To the lay public, Mr. Jones was referred to this clinic because he was suicidal, implies a sense of permanence the author might not have intended. Especially if Mr. Jones eventually commits suicide. Suicide risk fluctuates by the day, hour or minute. Ok to use suicidal to describe thoughts, behaviors, plans but not a person Be thoughtful when using risk level descriptors ( low, moderate, high ) Quantifies suicidal ideation and behavior Validated in adolescent and adult populations Evidence supports that CSSRS can help predict suicide attempts in adolescent and adult populations Used by CDC e version (ec SSRS) utilized by Oklahoma Department of Mental Health and Substance Abuse 22
23 ard_mental_health_professionals.pdf You will rarely feel totally comfortable discharging a patient in crisis or letting him/her leave your office And, no matter how competent you are, you are likely to have a patient who commits suicide Also, you will make mistakes Moreover, you may even make mistakes with patients who eventually commit suicide If an untoward event occurs: Courts will not hold a clinician liable for being wrong about the level of risk a patient presents, as long as the clinician s mistake was based on a reasonable level of care, including documented evidence of the decision making processes that led to treatment planning. Dana Baerger, PhD; Risk Management With the Suicidal Patient: Lessons in Case Law in Professional Psychology: Research and Practice,


24 24
UPMC SAFE-T Training Adapted for Pediatric Primary Care. Sheri L. Goldstrohm, Ph.D.
 UPMC SAFE-T Training Adapted for Pediatric Primary Care Sheri L. Goldstrohm, Ph.D. Prevalence of Suicide in the U.S. 10th most frequent cause of death for all ages 2nd leading cause of death for individuals
UPMC SAFE-T Training Adapted for Pediatric Primary Care Sheri L. Goldstrohm, Ph.D. Prevalence of Suicide in the U.S. 10th most frequent cause of death for all ages 2nd leading cause of death for individuals
Suggested Protocol for Resident Verbalizing Suicidal Ideation or Plan
 Suggested Protocol for Resident Verbalizing Suicidal Ideation or Plan Rationale: In the event a [resident] verbalizes suicidal thoughts or even a plan, the carer will know what steps to take for safety
Suggested Protocol for Resident Verbalizing Suicidal Ideation or Plan Rationale: In the event a [resident] verbalizes suicidal thoughts or even a plan, the carer will know what steps to take for safety
More than 1 million people die worldwide every year from suicide!!!
 Chapter 115 Suicide Episode Overview: 1) Name 10 risk factors for suicide 2) Name an additional 5 risk factors for adolescent suicide 3) Describe the SAD PERSONS scale 4) Describe 4 potential targeted
Chapter 115 Suicide Episode Overview: 1) Name 10 risk factors for suicide 2) Name an additional 5 risk factors for adolescent suicide 3) Describe the SAD PERSONS scale 4) Describe 4 potential targeted
Legal 2000 and the Mental Health Crisis in Clark County. Lesley R. Dickson, M.D. Executive Director, Nevada Psychiatric Association
 Legal 2000 and the Mental Health Crisis in Clark County Lesley R. Dickson, M.D. Executive Director, Nevada Psychiatric Association Civil action: Civil Commitment Definition a legal action to recover money
Legal 2000 and the Mental Health Crisis in Clark County Lesley R. Dickson, M.D. Executive Director, Nevada Psychiatric Association Civil action: Civil Commitment Definition a legal action to recover money
Dr Carmelo Aquilina Senior Staff Specialist & Service Director Sydney West Area Health Service Clinical Senior Lecturer, University of Sydney
 Dr Carmelo Aquilina Senior Staff Specialist & Service Director Sydney West Area Health Service Clinical Senior Lecturer, University of Sydney A suicide Outline Part 1: understanding suicide Part 2: What
Dr Carmelo Aquilina Senior Staff Specialist & Service Director Sydney West Area Health Service Clinical Senior Lecturer, University of Sydney A suicide Outline Part 1: understanding suicide Part 2: What
FIREARMS AND SUICIDE PREVENTION
 FIREARMS AND SUICIDE PREVENTION WHAT LEADS TO SUICIDE? There s no single cause. Suicide most often occurs when several stressors and health issues converge to create an experience of hopelessness and despair.
FIREARMS AND SUICIDE PREVENTION WHAT LEADS TO SUICIDE? There s no single cause. Suicide most often occurs when several stressors and health issues converge to create an experience of hopelessness and despair.
Mental Health Series for Perinatal Prescribers. Severe postpartum syndromes
 Mental Health Series for Perinatal Prescribers Severe postpartum syndromes 2 Maternal Filicides Acutely psychotic - 24% Depression Altruistic - 56% to relieve suffering associated with suicide 80% due
Mental Health Series for Perinatal Prescribers Severe postpartum syndromes 2 Maternal Filicides Acutely psychotic - 24% Depression Altruistic - 56% to relieve suffering associated with suicide 80% due
Chapter 10 Suicide Assessment
 Chapter 10 Suicide Assessment Dr. Rick Grieve PSY 442 Western Kentucky University Not this: Suicide is man s way of telling God, You can t fire me, I quit. Bill Maher 1 Suicide Assessment Personal Reactions
Chapter 10 Suicide Assessment Dr. Rick Grieve PSY 442 Western Kentucky University Not this: Suicide is man s way of telling God, You can t fire me, I quit. Bill Maher 1 Suicide Assessment Personal Reactions
LINEHAN RISK ASSESSMENT AND MANAGEMENT PROTOCOL (LRAMP)
") Client: Person Completing: LINEHAN RISK ASSESSMENT AND MANAGEMENT PROTOCOL (LRAMP) Date Contacted: Date Created: SECTION 1: REASON FOR COMPLETION LRAMP 1. Reason for completing: History of suicide ideation,
Client: Person Completing: LINEHAN RISK ASSESSMENT AND MANAGEMENT PROTOCOL (LRAMP) Date Contacted: Date Created: SECTION 1: REASON FOR COMPLETION LRAMP 1. Reason for completing: History of suicide ideation,
Suicide.. Bad Boy Turned Good
 Suicide.. Bad Boy Turned Good Ross B Over the last number of years we have had a few of the youth who joined our programme talk about suicide. So why with all the services we have in place is suicide still
Suicide.. Bad Boy Turned Good Ross B Over the last number of years we have had a few of the youth who joined our programme talk about suicide. So why with all the services we have in place is suicide still
Directions: Use your mouse or the arrows on your keyboard to click through this tutorial.
 Directions: Use your mouse or the arrows on your keyboard to click through this tutorial. Diamond Healthcare Corporation Suicide Risk Assessment For Outpatient Programs 2009 Objectives 1. Identify the
Directions: Use your mouse or the arrows on your keyboard to click through this tutorial. Diamond Healthcare Corporation Suicide Risk Assessment For Outpatient Programs 2009 Objectives 1. Identify the
Reading: Andreasen & Black, Introductory Textbook of Psychiatry, 3rd edition, Chapter 21, pp
 Psychiatry Sequence (PSY614) Topic: Faculty: Suicide Michael Jibson, M.D., Ph.D. Reading: Andreasen & Black, Introductory Textbook of Psychiatry, 3rd edition, Chapter 21, pp. 553-568 Lecture: Thursday,
Psychiatry Sequence (PSY614) Topic: Faculty: Suicide Michael Jibson, M.D., Ph.D. Reading: Andreasen & Black, Introductory Textbook of Psychiatry, 3rd edition, Chapter 21, pp. 553-568 Lecture: Thursday,
Addressing the Elephant in the Room: Talking About Mental Illness and Suicide. Dana E. Boccio, Ph.D. Wellness Lecture December 8, 2015
 Addressing the Elephant in the Room: Talking About Mental Illness and Suicide Dana E. Boccio, Ph.D. Wellness Lecture December 8, 2015 What is Mental Illness? A mental illness is a condition that impacts
Addressing the Elephant in the Room: Talking About Mental Illness and Suicide Dana E. Boccio, Ph.D. Wellness Lecture December 8, 2015 What is Mental Illness? A mental illness is a condition that impacts
SUICIDE ASSESSMENT AND DOCUMENTATION
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences SUICIDE ASSESSMENT AND DOCUMENTATION AMANDA FOCHT, MD ACTING ASSISTANT PROFESSOR DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences SUICIDE ASSESSMENT AND DOCUMENTATION AMANDA FOCHT, MD ACTING ASSISTANT PROFESSOR DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL
Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating
 Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating the past and current level of functioning of the client
Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating the past and current level of functioning of the client
MATCP When the Severity of Symptoms Interferes with Progress
 MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
DURING A SUICIDAL CRISIS
 DURING A SUICIDAL CRISIS 1 UTAH RANKS 5 TH IN THE NATION 1 6 7 5 3 9 10 4 8 2 Data Source: WONDER 2016 Suicide Fatality Rates ages 10+ 2 Crude Rate of Suicides per 100,000 UTAH AND U.S. SUICIDE TREND Rate
DURING A SUICIDAL CRISIS 1 UTAH RANKS 5 TH IN THE NATION 1 6 7 5 3 9 10 4 8 2 Data Source: WONDER 2016 Suicide Fatality Rates ages 10+ 2 Crude Rate of Suicides per 100,000 UTAH AND U.S. SUICIDE TREND Rate
Suicide Prevention. Kuna High School
 Suicide Prevention Kuna High School Why Suicide Prevention is Important? From the 2015 Youth Risk Behavior Survey (CDC). Suicide 32% (up 4% from 29% - 2013) felt so sad or hopeless almost every day for
Suicide Prevention Kuna High School Why Suicide Prevention is Important? From the 2015 Youth Risk Behavior Survey (CDC). Suicide 32% (up 4% from 29% - 2013) felt so sad or hopeless almost every day for
How do I do a proper suicide assessment and document it in my note? September 27, 2018
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences How do I do a proper suicide assessment and document it in my note? September 27, 2018 Christopher R. DeCou, PhD
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences How do I do a proper suicide assessment and document it in my note? September 27, 2018 Christopher R. DeCou, PhD
Patient Management Tools
 Patient Management Tools Many concrete and easy-to-use tools are available to assist you and your staff in preventing suicide. This section includes pocket-sized tools to facilitate assessment and intervention
Patient Management Tools Many concrete and easy-to-use tools are available to assist you and your staff in preventing suicide. This section includes pocket-sized tools to facilitate assessment and intervention
Chapter 7 - Mood Disorders
 Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
MENTAL HEALTH DISEASE CLASSIFICATIONS
 MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
A Primer on Suicide Risk Assessment
 www.joeobegi.com A Primer on Suicide Risk Assessment Joseph H. Obegi, PsyD October 14 OBJECTIVES Introduction Why do an SRA? When to do an SRA SRA process Accounting Risk factors Warning signs Protective
www.joeobegi.com A Primer on Suicide Risk Assessment Joseph H. Obegi, PsyD October 14 OBJECTIVES Introduction Why do an SRA? When to do an SRA SRA process Accounting Risk factors Warning signs Protective
Chapter 29. Caring for Persons With Mental Health Disorders
 Chapter 29 Caring for Persons With Mental Health Disorders The Whole Person The whole person has physical, social, psychological, and spiritual parts. Mental relates to the mind. Mental health and mental
Chapter 29 Caring for Persons With Mental Health Disorders The Whole Person The whole person has physical, social, psychological, and spiritual parts. Mental relates to the mind. Mental health and mental
3/9/2017. A module within the 8 hour Responding to Crisis Course. Our purpose
 A module within the 8 hour Responding to Crisis Course Our purpose 1 What is mental Illness Definition of Mental Illness A syndrome characterized by clinically significant disturbance in an individual
A module within the 8 hour Responding to Crisis Course Our purpose 1 What is mental Illness Definition of Mental Illness A syndrome characterized by clinically significant disturbance in an individual
IMMINENT SUICIDE RISK & TREATMENT ACTION PLAN
 IMMINENT SUICIDE RISK & TREATMENT ACTION PLAN Client Name: Therapist Name: Client s DOB: Contact Date: REASON FOR IMMINENT RISK & TREATMENT ACTION PLAN 1. Current or History of suicidal ideation, impulses,
IMMINENT SUICIDE RISK & TREATMENT ACTION PLAN Client Name: Therapist Name: Client s DOB: Contact Date: REASON FOR IMMINENT RISK & TREATMENT ACTION PLAN 1. Current or History of suicidal ideation, impulses,
Suicide A National Problem, What Every Physician Needs to Know!
 Suicide A National Problem, What Every Physician Needs to Know! Asim A. Shah M.D. Professor & Executive Vice Chair Menninger Department of Psychiatry, Professor, Department of Community and Family Medicine,
Suicide A National Problem, What Every Physician Needs to Know! Asim A. Shah M.D. Professor & Executive Vice Chair Menninger Department of Psychiatry, Professor, Department of Community and Family Medicine,
Safety Planning and Lethal Means Reduction to Prevent Suicide Fall Substance Use Conference 2015 Doug Thomas, LCSW Director
 Safety Planning and Lethal Means Reduction to Prevent Suicide Fall Substance Use Conference 2015 Doug Thomas, LCSW Director Division of Substance Abuse and Mental Health Overview Suicide Data Where does
Safety Planning and Lethal Means Reduction to Prevent Suicide Fall Substance Use Conference 2015 Doug Thomas, LCSW Director Division of Substance Abuse and Mental Health Overview Suicide Data Where does
L;ve L;fe; Your story is not over yet.
 L;ve L;fe; Your story is not over yet. Suicide is not as rare as some think. Who is more at risk? In the U.S., suicide rates are highest during the spring. Suicide is the 3rd leading cause of death for
L;ve L;fe; Your story is not over yet. Suicide is not as rare as some think. Who is more at risk? In the U.S., suicide rates are highest during the spring. Suicide is the 3rd leading cause of death for
The Difficult Patient. Psychiatric Dilemmas in the Primary Care Setting. No Disclosures. Objectives 10/12/17. Erick K. Hung, MD
 Psychiatric Dilemmas in the Primary Care Setting No Disclosures Erick K. Hung, MD Associate Professor of Clinical Psychiatry University of California, San Francisco Objectives Describe approaches to the
Psychiatric Dilemmas in the Primary Care Setting No Disclosures Erick K. Hung, MD Associate Professor of Clinical Psychiatry University of California, San Francisco Objectives Describe approaches to the
Suicide Prevention and Intervention
 Suicide Prevention and Intervention Kim Myers, MSW May 2, 2017 Division of Substance Abuse and Mental Health Overview Suicide in Utah Suicide Risk & Protective Factors Suicide Warning Signs C-SSRS Safety
Suicide Prevention and Intervention Kim Myers, MSW May 2, 2017 Division of Substance Abuse and Mental Health Overview Suicide in Utah Suicide Risk & Protective Factors Suicide Warning Signs C-SSRS Safety
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS
 SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
BRTC IMMINENT SUICIDE RISK AND TREATMENT ACTIONS NOTE
 BRTC IMMINENT SUICIDE RISK AND TREATMENT ACTIONS NOTE Client Name: Therapist Name: Contact Date: Today s Date: REASON FOR IMMINENT RISK AND TREATMENT ACTION NOTE 1) CURRENT, SINCE LAST SESSION or HISTORY
BRTC IMMINENT SUICIDE RISK AND TREATMENT ACTIONS NOTE Client Name: Therapist Name: Contact Date: Today s Date: REASON FOR IMMINENT RISK AND TREATMENT ACTION NOTE 1) CURRENT, SINCE LAST SESSION or HISTORY
SUBJECT: Suicide Risk Screening and Assessment of Individuals in State Hospitals and State-Operated Crisis Stabilization Programs
 DBHDD SUBJECT: Suicide Risk Screening and Assessment of Individuals in State Hospitals and State-Operated Crisis Stabilization Programs Policy: 03-504 Page 2 of 3 Hospital and CSP Staff Awareness regarding
DBHDD SUBJECT: Suicide Risk Screening and Assessment of Individuals in State Hospitals and State-Operated Crisis Stabilization Programs Policy: 03-504 Page 2 of 3 Hospital and CSP Staff Awareness regarding
CRPS and Suicide Prevention
 1 CRPS and Suicide Prevention Jill Harkavy Friedman, PhD June 23, 2012 RSDSA Board Meeting 2 What we know about suicidal ideation and behavior Majority of people have thought about suicide at some point
1 CRPS and Suicide Prevention Jill Harkavy Friedman, PhD June 23, 2012 RSDSA Board Meeting 2 What we know about suicidal ideation and behavior Majority of people have thought about suicide at some point
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SAMPLE INITIAL EVALUATION TEMPLATE
 I. Demographic Information Date: SAMPLE INITIAL EVALUATION TEMPLATE Name: Address: Phone (Home/Cell): Phone (Work): Date of Birth: Guardianship (for children and adults when applicable): Marital Status:
I. Demographic Information Date: SAMPLE INITIAL EVALUATION TEMPLATE Name: Address: Phone (Home/Cell): Phone (Work): Date of Birth: Guardianship (for children and adults when applicable): Marital Status:
Suicide Spectrum Assessment and Interventions. Welcome to RoseEd Academy. Disclaimer
 RoseEd Module 7 Suicide Spectrum Assessment and Interventions Suicide Spectrum Assessment and Interventions J. Scott Nelson MA NCC LPC CRADC Staff Education Coordinator Welcome to RoseEd Academy Disclaimer
RoseEd Module 7 Suicide Spectrum Assessment and Interventions Suicide Spectrum Assessment and Interventions J. Scott Nelson MA NCC LPC CRADC Staff Education Coordinator Welcome to RoseEd Academy Disclaimer
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS
 DISORDERS and ANXIETY DISORDERS") MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
Suicide, Para suicide and Risk Assessment
 Suicide, Para suicide and Risk Assessment LPT Gondar Mental Health Group www.le.ac.uk Objectives: Definition of suicide, Para suicide/dsh Changing trends of methods used Epidemiology Clinical Variables
Suicide, Para suicide and Risk Assessment LPT Gondar Mental Health Group www.le.ac.uk Objectives: Definition of suicide, Para suicide/dsh Changing trends of methods used Epidemiology Clinical Variables
Cluster 1 Common Mental Health Problems (mild)
") Cluster 1 Common Mental Health Problems (mild) You have recently sought help for the first time. You have experienced depression and/or anxiety. This may cause distraction or minor disruption to you as
Cluster 1 Common Mental Health Problems (mild) You have recently sought help for the first time. You have experienced depression and/or anxiety. This may cause distraction or minor disruption to you as
Suicide Awareness & Prevention The Silent Epidemic Kristin A. Drake Cell:
 Suicide Awareness & Prevention The Silent Epidemic Kristin A. Drake Cell: 915 525 8937 What is Suicidality? ~According to Dr. Osvaldo Gaytan, Child and Adolescent Psychiatrist for El Paso Behavioral, Suicidality
Suicide Awareness & Prevention The Silent Epidemic Kristin A. Drake Cell: 915 525 8937 What is Suicidality? ~According to Dr. Osvaldo Gaytan, Child and Adolescent Psychiatrist for El Paso Behavioral, Suicidality
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Suicide Risk Assessment
 Suicide Risk Assessment Interviewing Basics Prepared by: Dr. Aviva Rostas Psychiatry Resident, University of Toronto Epidemiology Suicide is common. According to Statistics Canada, in 2009 there were 3,890
Suicide Risk Assessment Interviewing Basics Prepared by: Dr. Aviva Rostas Psychiatry Resident, University of Toronto Epidemiology Suicide is common. According to Statistics Canada, in 2009 there were 3,890
Mary Schepler
 Mary Schepler Mary.Schepler@thresholds.org WHAT WORDS OR PHRASES HAVE YOU HEARD ASSOCIATED WITH MENTAL ILLNESS? People with mental illness frighten and embarrass us and so we marginalize people who most
Mary Schepler Mary.Schepler@thresholds.org WHAT WORDS OR PHRASES HAVE YOU HEARD ASSOCIATED WITH MENTAL ILLNESS? People with mental illness frighten and embarrass us and so we marginalize people who most
Phone Screen. Beginning the Psychoeducational Process: The Intake. The Psychoeducational Process and Elements throughout Care
 Brian McKain, RN, MSN Christina Hanna, MS 1. Identify and explain the components used to assess and diagnose depression 2. How to share the wealth with both patients and their parents 3. Understand that
Brian McKain, RN, MSN Christina Hanna, MS 1. Identify and explain the components used to assess and diagnose depression 2. How to share the wealth with both patients and their parents 3. Understand that
Screening for Depression and Suicide
 Screening for Depression and Suicide Christa Smith, PsyD Western Interstate Commission for Higher Education Boulder, Colorado 10/2/2008 Background My background A word about language Today stopics Why
Screening for Depression and Suicide Christa Smith, PsyD Western Interstate Commission for Higher Education Boulder, Colorado 10/2/2008 Background My background A word about language Today stopics Why
Mental Health and Stress Management
 Mental Health and Stress Management In recent years, psychologists have become more interested in positive psychology Focus on positive emotions, characteristics, strengths, and conditions that create
Mental Health and Stress Management In recent years, psychologists have become more interested in positive psychology Focus on positive emotions, characteristics, strengths, and conditions that create
TOOL 1: QUESTIONS BY ASAM DIMENSIONS
 TOOL 1: QUESTIONS BY ASAM DIMENSIONS The following tool highlights specific questions that should be asked of the patient for each ASAM dimension. Name Date of Birth Date of Interview Address Referred
TOOL 1: QUESTIONS BY ASAM DIMENSIONS The following tool highlights specific questions that should be asked of the patient for each ASAM dimension. Name Date of Birth Date of Interview Address Referred
Suicide Risk Management Clinical Strategies
 Suicide Risk Management Clinical Strategies March 12, 2015 Steven Vannoy, PhD, MPH steven.vannoy@umb.edu Department of Counseling and School Psychology University of Massachusetts Boston Review: What Explains
Suicide Risk Management Clinical Strategies March 12, 2015 Steven Vannoy, PhD, MPH steven.vannoy@umb.edu Department of Counseling and School Psychology University of Massachusetts Boston Review: What Explains
Copyright 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill
 Copyright 2014 All rights reserved. No reproduction or distribution without the prior written consent of CHAPTER PREVIEW Defining/Explaining Abnormal Behavior Anxiety-Related Disorders Mood-Related Disorders
Copyright 2014 All rights reserved. No reproduction or distribution without the prior written consent of CHAPTER PREVIEW Defining/Explaining Abnormal Behavior Anxiety-Related Disorders Mood-Related Disorders
Operation S.A.V.E Campus Edition
 Operation S.A.V.E Campus Edition 1 Suicide Prevention Introduction Objectives: By participating in this training you will learn: The scope and importance of suicide prevention The negative impact of myths
Operation S.A.V.E Campus Edition 1 Suicide Prevention Introduction Objectives: By participating in this training you will learn: The scope and importance of suicide prevention The negative impact of myths
MENTAL ILLNESSES, CONSIDERATIONS FOR YOUTH AND AVAILABILITY OF PROGRAMS
 MENTAL ILLNESSES, CONSIDERATIONS FOR YOUTH AND AVAILABILITY OF PROGRAMS Queen Elizabeth High School Parent Council May 15 2017 DR A G M B U L L O C H, D E P U T Y D I R E C T O R M A T H I S O N C E N
MENTAL ILLNESSES, CONSIDERATIONS FOR YOUTH AND AVAILABILITY OF PROGRAMS Queen Elizabeth High School Parent Council May 15 2017 DR A G M B U L L O C H, D E P U T Y D I R E C T O R M A T H I S O N C E N
MINDFUL WELLNESS CENTER, PLLC
 PATIENT HISTORY NAME DATE PLEASE TAKE YOUR TIME AND COMPLETE THE ENTIRE FORM. You may use the back if needed for more explanation. Identifying Information: Date of Birth: Age: Sex: Place of Birth: Religion:
PATIENT HISTORY NAME DATE PLEASE TAKE YOUR TIME AND COMPLETE THE ENTIRE FORM. You may use the back if needed for more explanation. Identifying Information: Date of Birth: Age: Sex: Place of Birth: Religion:
Explain to patients and families the meaning and ramifications of FDA warnings regarding antidepressants. Appropriately monitor patients on
 Antidepressants in Children and Adolescents: The Good, The Bad & The Ugly Raymond C. Love, Pharm.D., BCPP, FASHP Associate Dean and Professor, Pharmacy Practice & Science University of Maryland, School
Antidepressants in Children and Adolescents: The Good, The Bad & The Ugly Raymond C. Love, Pharm.D., BCPP, FASHP Associate Dean and Professor, Pharmacy Practice & Science University of Maryland, School
Initial Evaluation Template
 Demographic Information (Please complete all questions on this form) Member Name: Date: Name: Address: Phone (Home): Phone (Work): Date of Birth: Social Security #: Guardianship (for children and adults
Demographic Information (Please complete all questions on this form) Member Name: Date: Name: Address: Phone (Home): Phone (Work): Date of Birth: Social Security #: Guardianship (for children and adults
Depression: Assessment and Treatment For Older Adults
 Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Psychosis, Mood, and Personality: A Clinical Perspective
 Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
Suicide Risk Assessment Self-Test
 Suicide Risk Assessment Self-Test The 30 item true or false self-test is designed to enhance clinician suicide risk assessment by incorporating evidence-based risk and protective factors. This self-test
Suicide Risk Assessment Self-Test The 30 item true or false self-test is designed to enhance clinician suicide risk assessment by incorporating evidence-based risk and protective factors. This self-test
medical attention. Source: DE MHA, 10 / 2005
 Mental Health EMERGENCIES Mental Health: Emergencies This presentation deals with teen suicide, which is a most difficult topic to consider. It is presented upon recommendations from national public and
Mental Health EMERGENCIES Mental Health: Emergencies This presentation deals with teen suicide, which is a most difficult topic to consider. It is presented upon recommendations from national public and
Some Common Mental Disorders in Young People Module 3B
 Some Common Mental Disorders in Young People Module 3B MENTAL ILLNESS AND TEENS About 70% of all mental illnesses can be diagnosed before 25 years of age When they start, most mental illnesses are mild
Some Common Mental Disorders in Young People Module 3B MENTAL ILLNESS AND TEENS About 70% of all mental illnesses can be diagnosed before 25 years of age When they start, most mental illnesses are mild
A NEW MOTHER S. emotions. Your guide to understanding maternal mental health
 A NEW MOTHER S emotions Your guide to understanding maternal mental health It is not your fault It is treatable Understanding Maternal Mental Health Life with a new baby is not always easy and the adjustment
A NEW MOTHER S emotions Your guide to understanding maternal mental health It is not your fault It is treatable Understanding Maternal Mental Health Life with a new baby is not always easy and the adjustment
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
8/23/2016. Chapter 34. Care of the Patient with a Psychiatric Disorder. Care of the Patient with a Psychiatric Disorder
 Chapter 34 Care of the Patient with a Psychiatric Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Care of the Patient with a Psychiatric
Chapter 34 Care of the Patient with a Psychiatric Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Care of the Patient with a Psychiatric
Suicide/Homicide Precautions OFFICE OF BEHAVIORAL HEALTH
 Suicide/Homicide Precautions OFFICE OF BEHAVIORAL HEALTH Disclaimer Information in this presentation should not be relied upon for diagnosis or treatment of a mental health condition. Resources referenced
Suicide/Homicide Precautions OFFICE OF BEHAVIORAL HEALTH Disclaimer Information in this presentation should not be relied upon for diagnosis or treatment of a mental health condition. Resources referenced
Child/ Adolescent Questionnaire
 Oconee Center for Behavioral Health 1360 Caduceus Way Building 400, Suite 102 Tel 706-286-8442 Fax 706-310-6907 Child/ Adolescent Questionnaire Patient s Name: Date of Birth: / / Patient s Birthplace:
Oconee Center for Behavioral Health 1360 Caduceus Way Building 400, Suite 102 Tel 706-286-8442 Fax 706-310-6907 Child/ Adolescent Questionnaire Patient s Name: Date of Birth: / / Patient s Birthplace:
Demographic Information Form
 PATIENT INFORMATION Demographic Information Form / / Mailing: Male Female SSN#: - - Home Cell Relationship Status (circle one): Single / Married / Divorced / Widowed / Other: ( ) - ( ) - (Preferred Phone
PATIENT INFORMATION Demographic Information Form / / Mailing: Male Female SSN#: - - Home Cell Relationship Status (circle one): Single / Married / Divorced / Widowed / Other: ( ) - ( ) - (Preferred Phone
DSM5: How to Understand It and How to Help
 DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
Suicide Prevention in the Older Adult
 Suicide Prevention in the Older Adult Nina R. Ferrell, MA Geriatric Outreach Professional Relations Salt Lake Behavioral Health Hospital Presentation Content Credits 1. Addressing Suicidal Thoughts and
Suicide Prevention in the Older Adult Nina R. Ferrell, MA Geriatric Outreach Professional Relations Salt Lake Behavioral Health Hospital Presentation Content Credits 1. Addressing Suicidal Thoughts and
Suicide: Starting the Conversation. Jennifer Savner Levinson Bonnie Swade SASS MO-KAN Suicide Awareness Survivors Support
 Suicide: Starting the Conversation Jennifer Savner Levinson Bonnie Swade SASS MO-KAN Suicide Awareness Survivors Support What We Do Know About Suicide Suicidal thoughts are common. Suicidal acts, threats
Suicide: Starting the Conversation Jennifer Savner Levinson Bonnie Swade SASS MO-KAN Suicide Awareness Survivors Support What We Do Know About Suicide Suicidal thoughts are common. Suicidal acts, threats
Announcements. The final Aplia gauntlet: Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+
 The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
I m in Crisis. Now what?
 Tammy M. White, LPCC I m in Crisis. Now what? Crisis: a time of intense difficulty, trouble, or danger. Welcome Tammy M. White, LPCC School-Community Liaison & Therapist Health Officer Mental Health and
Tammy M. White, LPCC I m in Crisis. Now what? Crisis: a time of intense difficulty, trouble, or danger. Welcome Tammy M. White, LPCC School-Community Liaison & Therapist Health Officer Mental Health and
Mental Health Disorder Prevalence among Active Duty Service Members in the Military Health System, Fiscal Years
 Mental Health Disorder Prevalence among Active Duty Service Members in the Military Health System, Fiscal Years 2005 2016 Prepared by the Deployment Health Clinical Center Released January 2017 by Deployment
Mental Health Disorder Prevalence among Active Duty Service Members in the Military Health System, Fiscal Years 2005 2016 Prepared by the Deployment Health Clinical Center Released January 2017 by Deployment
Dr Chong Yew Siong BSc, MD, MMed (Psych) Lecturer & Psychiatrist Faculty of Medicine & Health Sciences USIM
 Lecturer & Psychiatrist Faculty of Medicine & Health Sciences USIM") Dr Chong Yew Siong BSc, MD, MMed (Psych) Lecturer & Psychiatrist Faculty of Medicine & Health Sciences USIM Introduction Recent Updates & Statistics Suicide Risk Assessment Management Q & A Suicide is
Dr Chong Yew Siong BSc, MD, MMed (Psych) Lecturer & Psychiatrist Faculty of Medicine & Health Sciences USIM Introduction Recent Updates & Statistics Suicide Risk Assessment Management Q & A Suicide is
Suicide Awareness & Assessment
 Suicide Awareness & Assessment Western Psychiatric Institute and Clinic of UPMC Presbyterian Shadyside 1 Dr. Jennifer Beckjord, PsyD; Senior Director, Clinical Services Jeffrey Magill, MS; Emergency Management
Suicide Awareness & Assessment Western Psychiatric Institute and Clinic of UPMC Presbyterian Shadyside 1 Dr. Jennifer Beckjord, PsyD; Senior Director, Clinical Services Jeffrey Magill, MS; Emergency Management
Chapter 2 Lecture. Health: The Basics Tenth Edition. Promoting and Preserving Your Psychological Health
 Chapter 2 Lecture Health: The Basics Tenth Edition Promoting and Preserving Your Psychological Health OBJECTIVES Define each of the four components of psychological health, and identify the basic traits
Chapter 2 Lecture Health: The Basics Tenth Edition Promoting and Preserving Your Psychological Health OBJECTIVES Define each of the four components of psychological health, and identify the basic traits
Psychology Session 11 Psychological Disorders
 Psychology Session 11 Psychological Disorders Date: November 18th, 2016 Course instructor: Cherry Chan Mothercraft College Agenda 1. Normal vs. Abnormal 2. Communication disorders 3. Anxiety disorders
Psychology Session 11 Psychological Disorders Date: November 18th, 2016 Course instructor: Cherry Chan Mothercraft College Agenda 1. Normal vs. Abnormal 2. Communication disorders 3. Anxiety disorders
Suicide Risk Factors
 Suicide Prevention Suicide Risk Factors Mental Health disorders, in particular: o Depression or bipolar (manic-depressive) disorder o Alcohol or substance abuse or dependence o Schizophrenia o Post Traumatic
Suicide Prevention Suicide Risk Factors Mental Health disorders, in particular: o Depression or bipolar (manic-depressive) disorder o Alcohol or substance abuse or dependence o Schizophrenia o Post Traumatic
What to do if You or Your Friend is Thinking about Suicide, or Hurting Themselves:
 What to do if You or Your Friend is Thinking about Suicide, or Hurting Themselves: Suicide is a serious concern in the US. Parents are often unaware of the risk of suicide among youth. Youth are usually
What to do if You or Your Friend is Thinking about Suicide, or Hurting Themselves: Suicide is a serious concern in the US. Parents are often unaware of the risk of suicide among youth. Youth are usually
Mental Health Rotation Educational Goals & Objectives
 Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
Orientation for New Child and Adolescent Psychiatry Residents: Module Two - Assessment
 Orientation for New Child and Adolescent Psychiatry Residents: Module Two - Assessment Objectives: To describe important aspects of emergency evaluations of children and adolescents. Steps to Completion
Orientation for New Child and Adolescent Psychiatry Residents: Module Two - Assessment Objectives: To describe important aspects of emergency evaluations of children and adolescents. Steps to Completion
10. Psychological Disorders & Health
 10. Psychological Disorders & Health We will now study different psychological disorders and theories for treating psychopathology. We will also cover health, stress and how to cope with them. The sections
10. Psychological Disorders & Health We will now study different psychological disorders and theories for treating psychopathology. We will also cover health, stress and how to cope with them. The sections
Department of Public Welfare PSYCHOLOGICAL IMPAIRMENT REPORT
 Department of Public Welfare PSYCHOLOGICAL IMPAIRMENT REPORT The purpose of this report is to outline the information needed to make a disability determination. This is not a required format; however,
Department of Public Welfare PSYCHOLOGICAL IMPAIRMENT REPORT The purpose of this report is to outline the information needed to make a disability determination. This is not a required format; however,
Crisis Management. Crisis Management Goals. Emotionally Disturbed Persons 10/29/2009
 Crisis Management Crisis Management Goals try to ensure safety for yourself, other officers, subjects, and other citizens establish and maintain control resolve the situation positively when appropriate,
Crisis Management Crisis Management Goals try to ensure safety for yourself, other officers, subjects, and other citizens establish and maintain control resolve the situation positively when appropriate,
BAPTIST HEALTH SCHOOL OF NURSING NSG 3037: PSYCHIATRIC MENTAL HEALTH. Safety: Suicidal Crisis
 F 1 BAPTIST HEALTH SCHOOL OF NURSING NSG 3037: PSYCHIATRIC MENTAL HEALTH Safety: Suicidal Crisis Lecture Objectives: 1. Discuss epidemiological statistics and risk factors related to suicide. 2. Describe
F 1 BAPTIST HEALTH SCHOOL OF NURSING NSG 3037: PSYCHIATRIC MENTAL HEALTH Safety: Suicidal Crisis Lecture Objectives: 1. Discuss epidemiological statistics and risk factors related to suicide. 2. Describe
Youth Suicide Assessment and Intervention in Primary Care. Tina Walde, DNP, PMHNP OHSU School of Nursing
 Youth Suicide Assessment and Intervention in Primary Care Tina Walde, DNP, PMHNP OHSU School of Nursing Objectives Role of the NP History Terms Epidemiology Groups with increased risk Warning signs The
Youth Suicide Assessment and Intervention in Primary Care Tina Walde, DNP, PMHNP OHSU School of Nursing Objectives Role of the NP History Terms Epidemiology Groups with increased risk Warning signs The
Self Injury Information
 Self Injury Information 1. What is self-abuse? When people act in such a way as to cause injury to themselves, those actions are called self - abuse. These actions can also be labeled self-injury, self-inflicted
Self Injury Information 1. What is self-abuse? When people act in such a way as to cause injury to themselves, those actions are called self - abuse. These actions can also be labeled self-injury, self-inflicted
Date of Onset is defined as the first day the claimant meets the definition of disability as defined in the Act and regulations.
 THESE ARE THE FORMS I USE THIS IS NOT LEGAL ADVICE AND INTENDED TO SUPPLEMENT YOUR PARTICULAR FACTUAL SITUATION ONLY It is crucial you educate yourself on the Social Security Regulations that define and
THESE ARE THE FORMS I USE THIS IS NOT LEGAL ADVICE AND INTENDED TO SUPPLEMENT YOUR PARTICULAR FACTUAL SITUATION ONLY It is crucial you educate yourself on the Social Security Regulations that define and
Rates of Co-Occurring Disorders Among Youth. Working with Adolescents with Substance Use Disorders
 1 Working with Adolescents with Substance Use Disorders Michael S. Levy, Ph.D. CAB Health & Recovery Services, Inc. Health and Education Services 8% of 12-17 year old youth have substance abuse or dependence
1 Working with Adolescents with Substance Use Disorders Michael S. Levy, Ph.D. CAB Health & Recovery Services, Inc. Health and Education Services 8% of 12-17 year old youth have substance abuse or dependence
Threat to Self: Suicide & Self-Injurious Behavior. David Towle, Ph.D. UNI Counseling Center Director
 Threat to Self: Suicide & Self-Injurious Behavior David Towle, Ph.D. UNI Counseling Center Director What do you do? You check your e-mail and find a message from a student, apparently sent about 3 a.m.,
Threat to Self: Suicide & Self-Injurious Behavior David Towle, Ph.D. UNI Counseling Center Director What do you do? You check your e-mail and find a message from a student, apparently sent about 3 a.m.,
ACOEM Commercial Driver Medical Examiner Training Program
 ACOEM Commercial Driver Medical Examiner Training Program Module 7: Psychological Psychological 49 CFR 391.41(b)(9) "A person is physically qualified to drive a commercial motor vehicle if that person
ACOEM Commercial Driver Medical Examiner Training Program Module 7: Psychological Psychological 49 CFR 391.41(b)(9) "A person is physically qualified to drive a commercial motor vehicle if that person
BUILDING BARRIERS TO SUICIDE:
 BUILDING BARRIERS TO SUICIDE: Mr. F 78 yo male CAD, HTN, CABGx5 Depression? PCP of course you re depressed, your old Sig for anti depressant
BUILDING BARRIERS TO SUICIDE: Mr. F 78 yo male CAD, HTN, CABGx5 Depression? PCP of course you re depressed, your old Sig for anti depressant
AN INTRODUCTION TO...
 AN INTRODUCTION TO... The National Alliance on Mental Illness had its beginning in 1979. In the beginning NAMI began because of a need the families of people affected by mental health conditions were unable
AN INTRODUCTION TO... The National Alliance on Mental Illness had its beginning in 1979. In the beginning NAMI began because of a need the families of people affected by mental health conditions were unable
Major Depression Major Depression
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
22q11.2 Deletion Syndrome Fact Sheet - Treatable Psychiatric Illnesses in Adults
 22q11.2 Deletion Syndrome Fact Sheet - Treatable Psychiatric Illnesses in Adults Anne S. Bassett (MD, FRCPC) Professor of Psychiatry, University of Toronto Director, Clinical Genetics Research Program,
22q11.2 Deletion Syndrome Fact Sheet - Treatable Psychiatric Illnesses in Adults Anne S. Bassett (MD, FRCPC) Professor of Psychiatry, University of Toronto Director, Clinical Genetics Research Program,
Psychological Disorders. Schizophrenia Spectrum & Other Psychotic Disorders. Schizophrenia. Neurodevelopmental Disorders 4/12/2018
 Psychological s Schizophrenia Spectrum & Other Psychotic s Schizophrenia Spectrum & Other Psychotic s 0Presence of delusions, hallucinations, disorganized thinking/speech, disorganized or abnormal motor
Psychological s Schizophrenia Spectrum & Other Psychotic s Schizophrenia Spectrum & Other Psychotic s 0Presence of delusions, hallucinations, disorganized thinking/speech, disorganized or abnormal motor
WORD WALL. Write 3-5 sentences using as many words as you can from the list below.
 WORD WALL Write 3-5 sentences using as many words as you can from the list below. Suicide Phobia Bipolar Obsessive compulsive disorder(ocd) Anxiety Depression Mood Post traumatic stress disorder (PTSD)
WORD WALL Write 3-5 sentences using as many words as you can from the list below. Suicide Phobia Bipolar Obsessive compulsive disorder(ocd) Anxiety Depression Mood Post traumatic stress disorder (PTSD)
Workshop Description Assessment, Management, and Treatment of Suicide: Abbreviated Course. Learning Objectives Act 74 of 2016
 Workshop Description Assessment, Management, and Treatment of Suicide: Abbreviated Course Samuel Knapp, Ed.D., ABPP Fall 2017 Suicide is the 10 th leading cause of death in the United States and the most
Workshop Description Assessment, Management, and Treatment of Suicide: Abbreviated Course Samuel Knapp, Ed.D., ABPP Fall 2017 Suicide is the 10 th leading cause of death in the United States and the most
Understanding Mental Illness A Review of the Disorders
 Understanding Mental Illness A Review of the Disorders Objectives Define and describe mental illness To be able to recognize signs, symptoms, and behaviors of the major categories of mental illness Recognition
Understanding Mental Illness A Review of the Disorders Objectives Define and describe mental illness To be able to recognize signs, symptoms, and behaviors of the major categories of mental illness Recognition
Contemporary Psychiatric-Mental Health Nursing Third Edition. Introduction. Introduction 9/10/ % of US suffers from Mood Disorders
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional