Should peripheral T-cell lymphoma be treated by autologous or allogeneic SCT?
|
|
|
- Justina Hall
- 5 years ago
- Views:
Transcription

1 Francesco d Amore, MD, PhD Dept. Of Hematology Aarhus University Hospital, Aarhus, Denmark Should peripheral T-cell lymphoma be treated by autologous or allogeneic SCT? Disclosure of Interest: Nothing to Disclose
 Overall (all subtypes): 5 yr OS 38.5% ALCL (overall) 56.")
2 Upfront ASCT in PTCL: Scenario with conventional CHOP/CHOP-like approach Meta-analysis of CHOP/CHOP-like outcome in PTCL 31 clinical trials: tot 2815 pts ( period: ) Overall (all subtypes): 5 yr OS 38.5% ALCL (overall) 56.5% Abouyabi s et al, ISNR Hematology 2011
3 Autotransplantation in PTCL (retrospective) Salvage Treatment Author n CR OS Comment Vose (1990) 17 59% 35% (2y) Fanin (1999) 64 n.d. 70% (5y) ALCL Rodriguez (2001) 29 79% 39% (3y) subgroup Blystad (2001) 40 80% 58% (3y) Song (2003) 36 42% 48% (3y) Rodriguez (2003) 78 68% 56% (5y) subgroup Schetelig (2003) 15 67% 44% (5y) AIL, subgroup Jagasia (2004) 28 50% 69% (3y) incl. CTCL Jantunen (2004) 37 76% 54% (5y) subgroup Kewalramani (2006) 24 n.d. 33% (5y) Nademanee (2006) 57 n.d. 45% (2y) subgroup Kim (2007) 40 n.d. 11.5m subgroup Smith (2007) 32 n.d. 43% (3y) subgroup Chen (2008) 53 79% 40% (5y) subgroup Khouri (2008) 59 80% 43.5m subgroup
4 Autotransplantation in PTCL (retrospective) - 1. Line Treatment Author n Regimen CR OS Comment Rodriguez (2007) 19 Rodriguez (2007) 74 BEAM, BEAC, CVB, Cy+TBI BEAM, BEAC, CVB, Cy+TBI 79% 60% (5y) only AILT, subgroup n.d. 68% (5y) incl. ALCL Feyler (2007) 64 misc n.d. 53% (3y) incl. ALK+ALCL Kyriakou (2008) 146 misc 70% 59% (4y) only AILT, subgroup Khouri (2008) 79 mainly BEAM n.d. 60% (5y) incl. ALCL, subgroup Lee (2008) 47 misc n.d. 86% (5y DFS) only extranodal PTCL Yang (2009) 64 misc n.d. 53% (3y) only PTCLu Nademanee A (2011) 67 misc n.d. 54% (5y) 66 mo med follow-up Prochazcha V (2011) 29 misc 66% 65% (2y) PTCL-NOS, alk-neg ALCL, AILT, EATL Iriyama N (2013) 28 Double CHOP> Cy+Eto+Ranimustine 68% 63% (5y) Alk+ ALCL excluded

5 Proportion HDT in PTCL-NOS Retrospective data from the International T-cell Project Proportion possibly an advantage and, if so, rather upfront 1.0 Overall survival 1.0 Failure-free survival p= p< Time Time HD Therapy yes no CENSOR FAIL TOTAL MEDIAN Transplantation CENSOR FAIL TOTAL MEDIAN 1. line line Armitage, Vose, et al. J Clin Oncol (2008)
6 Largest prospective PTCL trials with HDT in 1st line Study Histology Type Design N of pts (ITTP) Med follow-up Accrual status Efficacy (Ref) Treatment naive PTCL ACT sptcl IIS phase mo Ongoing ASH 2012 NLG-T-01 sptcl IIS phase mo Closed JCO 2012 Reimer et al sptcl IIS phase mo Closed JCO 2009 IIS = Investigator-initiated study
 (n=83) 1 0,8 Progression-free survival 5 yr OS 3 yr PFS 40% 36% 0,6 0,4 0,2 0 0 12 24 36 48 60 Time (months)")
7 Overall survival 1 0,8 0,6 Parameter N pts 83 Schedule - CHOP-21 x Mobilizing DexaBEAM - TBI+CY Median follow-up 33 mo 0,4 0, Time (months) (n=83) 1 0,8 Progression-free survival 5 yr OS 3 yr PFS 40% 36% 0,6 0,4 0, Time (months) (n=83)

 61-67 yrs: (n=42) 60 mo")
P-14d x 3 (stem")
 NC,PD NC,PD JCO")
8 Excluded: Precursor TCL alk+ ALCL CTCL Primary leukemic PTCL CHO(E)P : yrs: CHOEP-14 (n=118) yrs: (n=42) 60 mo median follow-up CHO(E)P-14d x 3 CR, PR CHO(E)P-14d x 3 (stem cell collection) CR, PR HDT (BEAM) NC,PD NC,PD JCO 2012;30(25): Follow-up


9 NLG-T-01: OS and PFS Median follow-up: 5 yrs (range 2-8 yrs) OS, whole cohort 5-yr OS 51% N of evaluable patients: 160 Median age: 57 yrs months Number at risk % CI Survivor function Dose-dense induction followed by HDT/ASCT: is well tolerated PFS, whole cohort 5-yr PFS 44% leads to long-term PFS in 44% of pts best in alk-neg ALCL (5y PFS:61%; OS:70%) useful reference for future studies months Number at risk % CI Survivor function
10 ASCT 1st line in PTCL OS +PFS in the Nordic and German trial Comparison of treatment schedules Induction Conditioning regimen Nordic trial CHOEP-14 x6 BEAM German trial CHOP-21 x4-6 + DexaBEAM/ESHAP (mobilizing) HdCy+TBI OS Nordic trial German trial PFS Nordic trial German trial 3-yrs 57% 48% 5-yrs 51% 40% 3-yrs 49% 36% 5-yrs 44% n.d.
11 NLG-T-01: OS and PFS - largest subtypes Median follow-up: 5 years 1.0 OS, largest subtypes 1.0 PFS, largest subtypes p=0.21 (logrank test) 0.2 p=0.26 (logrank test) months months PTCL-NOS Alk-negative ALCL AILT EATL PTCL-NOS Alk-negative ALCL AILT EATL Histology 5-yr OS 95% CI ALCL 70% 50%-83% AILT 52% 33%-69% EATL 48% 26%-67% PTCL-NOS 47% 34%-59% Meta-analysis CHOP 5y OS (Abouyaby, 2011) 56.5 % 36.5 % 21 % 34% Histology 5-yr PFS 95% CI ALCL 61% 42%-76% AILT 49 % 30%-65% EATL 38 % 18%-57% PTCL-NOS 38 % 25%-50%
 CHOP-like IfosfVepEpi + MTX+ASCT CHOP-like IfosfVepEpi + MTX+ASCT N tot = 54 N tot = 26 1994-1998 1998-2009 5 yr OS")
12 Intensified induction + upfront ASCT in EATL Retrospective analysis of prospectively collected data Parameter Comment Values N pts Data period Outcome (historical comparison) CHOP-like IfosfVepEpi + MTX+ASCT CHOP-like IfosfVepEpi + MTX+ASCT N tot = 54 N tot = yr OS 22 vs 52%
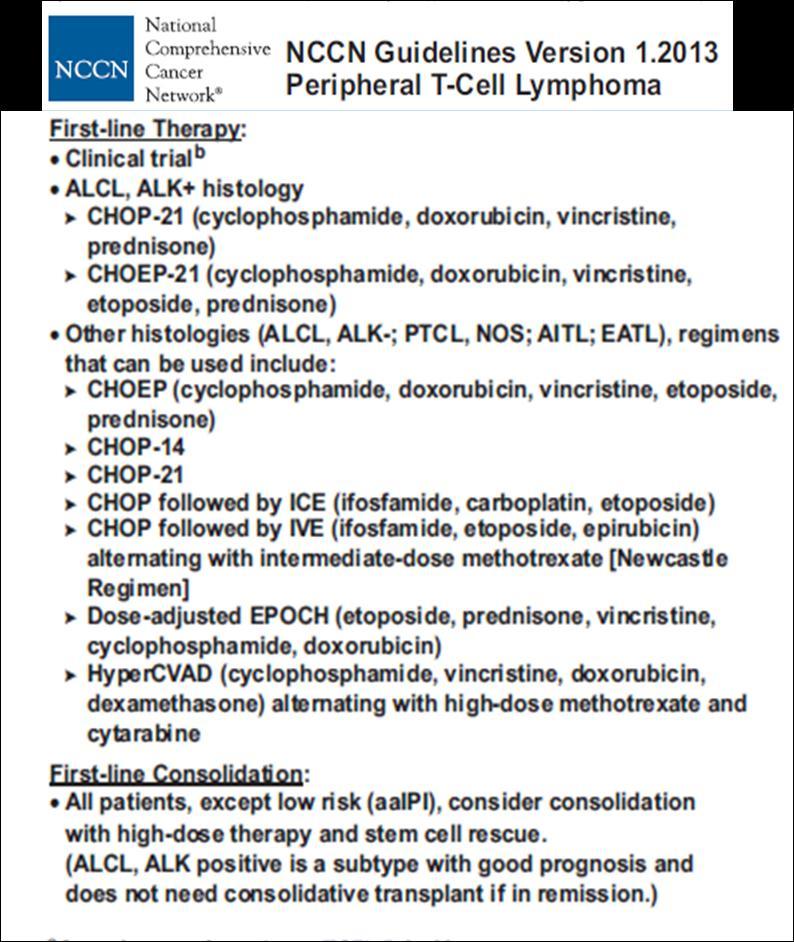
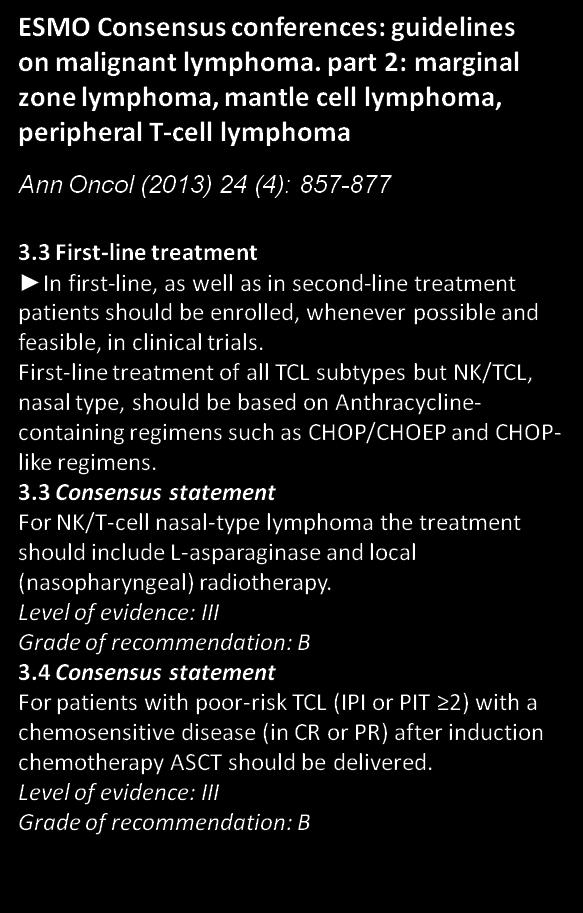
13 Guidelines ESMO + NCCN

14 1st line treatment of PTCL Patterns of treatment failure 26% 18% 7% Diagnosis 2 yr 3 yr est 5 yrs PFS = 44% End of induction, consolidation Improve induction Improve consolidation/ consider maintenance New trials


15 18 yrs The ACT trial 65 yrs 80 yrs R R A 30 - A 30 - A 30 - A 30 - A 30 - A 30 - A 30 - A 30 - HDT HDT N=133 N=250 N=117
16 Proportion Proportion ACT-1 Response rates and time-related end-points 15 mo median follow-up Response rates Response rates N (%) ORR 42 (67) CR/CRu 38 (61) PR 4 (6) SD 3 (5) PD 16 (25) Not evaluable 2 (3) Total 63 (100) Time-related end-points (not arm-specific) Primary EFS Months End-point 1-yr (95% CI) EFS 55% (42-67) PFS 54% (42-67) OS 78% (67-88) Secondary PFS Months d Amore et al, ASH 2012 abs #57
17 The ACT and NLG-T-01 trials Outcome meta-analysis with regard to ASCT R R NLG-T-01 (>60y) A 30 - A 30 - CHO(E)P-14 A 30 - A 30 - CHO(E)P-14 A 30 - A 30 - CHO(E)P-14 A 30 - A 30 - CHO(E)P-14 CHO(E)P-14 CHO(E)P-14 Auto Auto Auto Meta-analysis Cohort Est. N NLG-T-01 Std ACT yrs (CHOP + HDT) yrs (CHOP + HDT) Std ACT yrs (CHOP) 60-70
18 NLG-T-01: long-term follow-up (8 yr median) Induction Consolidation Follow-up 1st yr Follow-up 2nd yr Follow-up 3rd yr Follow-up 4th yr Follow-up 5th yr Follow-up 6th yr Follow-up 7th yr Follow-up Median 98 ( ) months Histology Early (<2yrs) post-therapeutic relapses Late ( 2yrs) post-therapeutic relapses N Time points for relapse (yrs) N Time points for relapse (yrs) PTCL-NOS 8 0.2; 0.2; 0.3; 0.3; 0.5; 0.9; 1.3; ; 3.6; 3.8; 3.9; 5.3 AILT 6 0.2; 0.3; 0.3; 0.5; 1.0; ; 4.2; 6.1 ALCL (alk-) 6 0.2; 0.3; 0.3; 0.3; 0.3; ; 5.0; 6.4 EATL 5 0.3; 0.4; 0.8; 0.8; ; 7.1 SCPL HSTCL d Amore et al. 12th ICML Lugano 2013; abs #

19
20 #155: Intensified chemo-immunotherapy for patients affected by nodal peripheral T-cell lymphomas (PTCLs) at diagnosis: Final results of a phase II multicentre prospective trial P. Corradini et al. Italian phase II study performed (NCT ) A: yrs: 2 x CHOP-21 + Campath (30 mg) 2 x Hyper-C-Hidam (Cy-AraC-Mtx) Responding pts received auto-sct or allo-sct based on genetic stratification B: yrs: 6 x CHOP-21 + Campath (10 mg) Cohort of 86 pts (A: n=61; B: n=25) PTCL-NOS: 49% AILT: 24% ALCL Alk-neg: 22% EATL: 5%
21 P. Corradini et al. FINDINGS: A: yrs B: yrs Median follow-up 40 mo 48 mo Estimated 4yrs OS PFS DFS 48.8% (95% CI, %) 44.0% (95% CI, %) 79.0% (95% CI, %) 31.5% (95% CI, %) 26.7% (95% CI, %) 44.4% (95% CI, %) NRM 13% (majority of pts belonged to the allo-sct cohort) 12% ORR at the end of induction 67% (CR 56%; PR 11%) - Consolidation Multivariate analysis (PFS, OS) Auto-SCT: 14 pts (OS vs non-transpl:hr 0.04; p=0.004) Allo-SCT: 23 pts (OS vs non-transpl:hr 0.22; p=0.008) No consolidation: 23 (PD: 18 pts; toxic deaths: 5 pts) 1 pt maintained remission without consolidation ccr for at least 6 mo: significant for both PFS and OS Undergo transplantation: significant for OS - CONCLUSION: Upfront transplantation was associated with a prolonged DFS in younger patients. No outcome improvement for the chemoimmunotherapy treated elderly cohort

22 Modality N pts Med age Histologies (N) Auto yrs ALCL: 53 PTCL-NOS: 34 AITL: 13 Allo yrs ALCL: 51 PTCL-NOS: 63 AITL: 12 Total 241
 RIC vs Myabl")
23 Auto vs Allo PFS and OS (all pts) Auto vs Allo NRM Auto vs Allo PFS and OS (CR1 excl) RIC vs Myabl NRM
24 Should SCT in 1st remission be the standard of care for patients with PTCL? Treatment setting Ptt. Description No. of ptt. in the cohort (%) young & fit 241/470 (51) 1st-line* ( 65 y & PS 2) elderly & fit 164/470 (35) (> 65 y & PS 2) Frail (PS>2) 65/470 (14) Bjerregaard-Pedersen M 12th ICML, abs #234, Ann Oncol Suppl 2013 age >65-67yrs (45-50%) alk+alcl (no pediatric cases) (3%) stage I low-risk non-bulk disease (2%) severe co-morbidity (4%) (only for allosct): no donor availability For approximately 50-60% of them => no
25 Should high-dose therapy with autologous stem cell support be recommended in 1st remission for the 40-50% transplant eligible patients with PTCL? yes, as it probably provides the possibility to improve the quality of remission and thereby the duration of respons Although no randomized clinical trials are presently available to answer the question in a definitive way And limited to 1 transplant- and risk-eligible 2 chemosensitive (CR, CRu, PR) 3 risk-eligible (i.e. stage I non-bulk, IPI 0-1 excluded)
26

27 Should peripheral T-cell lymphoma be treated by auto or allogeneic SCT? F. d Amore Aarhus University Hospital, Aarhus, Denmark Berlin, October 2013
28 NLG-T-01: Flow chart 166 pts enrolled 6 pts inclusion criteria not fulfilled Flow chart of the NLG-T-01 study cohort showing the number and types of treatment failures and the responding patients throughout the different stages of the treatment algorithm. 160 pts confirmed diagnosis 156 pts Evaluable response Intention-to-treat population 4 pts not evaluable response ORR pre-tx 131 (82%) CR/CRu 82 (51%) PR 49 (31%) % Tx 115 (72%) 131 pts CR/PR after 6xCHOEP 115 pts transplanted 25 pts primary refractory 16 pts PD/tox/mobilisation failure/other before Tx CR/CRu 100d post-tx 90 (56%) 90 pts CR/CRu 3 mo post Tx 25 pts PR/PD/tox
29 NLG-T-01: CHOP vs elderly CHOEP Median follow-up: 5 years Subcohort 5yr OS 5yr PFS yrs CHOEP (n=50) 40% 39% yrs CHOP (n=42) 45% 34% NLG-T01: OS for CHOP vs 'elderly' CHOEP, p= analysis time CHOEP CHOP
30 NLG-T-01: OS and PFS ALCL vs non-alcl histology Median follow-up: 5 years NLG-T01: OS - ALCL vs non-alcl, p=0.026 NLG-T01: PFS - ALCL vs non-alcl, p= analysis time analysis time alcl = Not ALCL alcl = ALCL alcl = Not ALCL alcl = ALCL
31 NLG-T-01: ALCL vs non-alcl No difference in age, CS, IPI and BM involvement Age Clinical stage Histology median (yrs) Rank-sum (obs/exp) p-value* Histology CS I-II N (%) CS III-IV N (%) p-value (Fisher s exact) ALCL 53.8 yrs 10632/10385 non-alcl 50.2 yrs 2248/ ALCL 8 (26%) 23 (74%) non-alcl 23 (18%) 106 (82%) * Two-sample Wilcoxon rank-sum (Mann-Whitney) test IPI BM involvement Histology IPI low N (%) IPI int-high N (%) p-value (Fisher s exact) Histology No N (%) Yes N (%) p-value (Fisher s exact) ALCL 12 (39%) 19 (61%) non-alcl 33 (26%) 96 (74%) ALCL 23 (74%) 8 (26%) non-alcl 96 (74%) 33(26%) 1.000
32 NLG-T-01: Prognostic factors Parameter OS PFS HR CI 95% p-value HR CI 95% p-value Univariate analysis Female gender Age (per year) PS BM involvement ALCL histology Elevated s-ldh CS III-IV Multivariate analysis ALCL histology Age (per year) PS Female gender BM involvement
33 Population-based clinicopathological features Danish Lymphoma Registry LYFO ( ) PTCL-NOS (n=218) AITL (n=91) ALK+ ALCL (n=49) ALK- ALCL (n=89) EATL (n=15) All (n=462) Med age (yrs) M/F ratio Stage III/IV (%) PS (ECOG) (%) 0 I II III IV >1 Exnod site (%) BM involvement, % Approximately 49% of the pts were not eligible (e.g. high age, poor PS) for trials involving upfront SCT. Approximately 80% of pts were considered eligible for any interventional clinical trial (age, PS, comorbidity, unable to give informed consent etc). Of the potential 80% candidates (any trial), only 11% were actually included in a clinical trial emphasizing the need of optimizing recruitment strategies and trial designs, particularly for the frailest subset of pts. Pedersen et al. 12th ICML Lugano 2013; abs # 234



34 HDT in PTCL Summary and perspectives Did NLG-T-01 improve upon a comparable historical cohort? Possibly 1.0 OS, whole cohort % months Number at risk % CI Survivor function A characterization of long-term responders vs refractory and relapsing patients should be attempted Trial-specific TMA and nucleic acid analysis from FFPE samples Work in progress NGS acgh GEP mirna Protein analysis on frozen tissue samples and validation with WB and IH
35 NLG-T-01: Demographics Characteristic No. of patients (%) Age, yrs - Median - Range Sex - Male - Female (67) 53 (33) B-symptoms 94 (59) Pre-therapeutic clinicopathological patient characteristics (N=160) Elevated s-ldh 99 (62) PS 2 46 (29) Bulk 26 (17) CS III-IV 129 (81) BM involvement 41 (26) IPI ( 2) 115 (72) Histological subtype - PTCL-NOS - ALK-neg ALCL - AILT - EATL - Panniculitis-like - T/NK nasal type - Hepatosplenic 62 (39) 31 (19) 30 (19) 21 (13) 6 (4) 5 (3) 5 (3) ALCL PL HSL T/NK EATL AILT NOS
36 NLG-T-01: Toxicity and causes of death Toxicity Gr.3-4 % of total Hematological 65% Non-hematological 45% - Infection 37% - Gastrointestinal 4% - Mucositis 4% Cause of death N pts % of deceased % of total Lymphoma 54 75% 34% Toxicity 7 10% 4% 2nd cancer 2 3% 1% Other causes 6 8% 3% Unknown 3 4% 2% Total % 45%
37 NLG-T-01: OS - rare subtypes Median follow-up: 5 years OS, rare subtypes Histology 3-yr OS 95% CI PL 50% 11%-80% HS 40% 5%-75% T/NK 40% 5%-75% analysis time panniculitis-like (PL) Hepatosplenic (HS) Extranodal T/NK (T/NK)
38 NLG-T-01: PFS - rare subtypes Median follow-up: 5 years PFS, rare subtypess Histology 3-yr OS 95% CI PL 50% 11%-80% HS 40% 5%-75% T/NK analysis time panniculitis-like (PL) Hepatosplenic (HS) extranodal T/NK (T/NK)
 2/ 3 (0.67) 8/ 18 (0.44) 6x + A (n=22) 13/ 5 (2.60) 13/ 17 (0.76) Total (n=43) 15/8 (1.89) 21/ 35(0.60) Blood 2011; 118:1755")
39 ACT-1 SAEs before and after the ALZ dose amendment Treatment group Before amendment (n=8) SAE per patient After amendment (n=35) 6x (n=21) 2/ 3 (0.67) 8/ 18 (0.44) 6x + A (n=22) 13/ 5 (2.60) 13/ 17 (0.76) Total (n=43) 15/8 (1.89) 21/ 35(0.60) Blood 2011; 118:1755
40 Proportion of patients ACT-1 Feasibility (Blood 2011; 118:1755) Schedule adherence 6 x median: 73 6 x + A median: Days Infections Haematological toxicity CTC Leukocytopenia WHO= 4 Thrombocytopenia WHO= 3, 4 Anemia WHO= 3, 4 6 x CHOP SC harvest and recovery % pts 6 x CHOP - A all Type of infection 6x 6x + A Bacterial 54.8% 45.9% Fungal 6.5% 5.4% Viral 29.0% 35.1% Unknown 71.0% 75.7% Parameter N reinfused CD34+ cells (10 6 )/ kg b.w. Days to ANC >0.5x10 9 /l Days to Platelets >50x10 9 /l 6x Median 6x + A Median p- value
41 ACT-1 vs NLG-T-01 ORR and 1-year PFS/OS 15 mo median follow-up ACT-1 (not arm-specific, no ALCL) NLG-T-01 (without ALCL) 50% CHOP -14x6 50% A- x6 + ASCT CHOEP-14 x6 +ASCT ORR % CR-CRu (%) yr PFS (%) 1-yr OS (%) 54.4 (95% CI: 42;67) 77.6 (95% CI: 67;88) 57,5 (95% CI: 50; 65) 68,3 (95% CI: 61; 75) The non arm-specific outcome of the ACT-1 trial is similar to the one of the NLG-T-01 trial for ORR, CR,1-yr PFS and OS d Amore et al, ASH 2012 abs #57
42 Efficacy of Alemtuzumab in combination with doseadjusted EPOCH in untreated nodal PTCL Grant C et al ASCO 2012, Abstr.8051 Nodal PTCL Nodal PTCL ATLL ATLL P=0.06 P=0.08 Prior dose-finding Phase I study (Janik et al, ASH 2007) 30 mg pr course of daepoch Courtesy of dr. Cliona Grant (adapted) 45 mo median follow-up CD52 expression Jiang BJH 2009 Geissinger L& L 2009 PTCL-NOS 93% 90 % AILT 100% 90% ALCL --- 0% HS 100% T/NK 25%
43 HDT in PTCL some statements HDT with ASCR per se does probably not make a major difference in PTCL 25-35% 15-25% 5-10% Diagnosis SCT 1 yr 3 yr 5 yrs PFS Improve induction Consolidate response Maintain response Retrospective and prospective data favour the use of HDT as part of a dose-dense induction/consolidation strategy in chemosensitive patients in the upfront setting On the basis of the experience from the first large PTCL-restricted prospective trials a heterogeneity of responses should be acknowledged with regard to specific subtypes and to individual patients within the single subtypes
44 Autotransplantation in PTCL - 1. Line Treatment Prospective PTCL-restricted trials N pts Age Regimen Tx rate (%) CR/PR (%) TRM (%) OS FU Corradini (Leukemia 2006) 62 (inkl.alk+ ALCL) 43 1.APO>DHAP>HD Mito/Mel 2. MACOP-B> hdarac/ Mito> BEAM % (12 y) 76 mo Rodriguez (EJH2006) MegaCHOP/IFE % (3y) 35 mo Mercadal (Ann Oncol 2008) HighCHOP/ESHAP altern. > BEAM/BEAC n.d. 39% (4y) 3.2 y
45 Aims of NLG-T-01 To provide a PTCL-restricted prospective trial with a cohort of sufficient size to perform subtype analysis N=160 To provide a cohort with a risk-profile as close as possible to the spectrum of transplant-eligible patients seen in daily clinical practice Median age: 57yrs; IPI 2 : 72% To provide a follow-up of sufficient length to allow an appropriate estimate of both early and late failures Median follow-up: 5 years; Report of 9-yrs median follow-up analysis planned for 2014
46 HDT in PTCL some statements HDT with ASCR per se does probably not make a major difference in PTCL If at all, retrospective and prospective data seem to favour the use of HDT as part of a dose-dense induction + consolidation strategy in chemosensitive patients in the upfront setting On the basis of the experience from the first large PTCLrestricted prospective trials a heterogeneity of responses should be acknowledged with regard to specific subtypes and to individual patients within the single subtypes (trial-specific correlative biological studies are warranted to biologically differentiate responders form non-responders)
Peripheral T-Cell Lymphoma. Pro auto. Peter Reimer. Klinik für Hämatologie / intern. Onkologie und Stammzelltransplantation
 Peripheral T-Cell Lymphoma Pro auto Peter Reimer Klinik für Hämatologie / intern. Onkologie und Stammzelltransplantation Kliniken Essen Süd, Evang. Krankenhaus Essen-Werden ggmbh COSTEM, Berlin 09.09.2011
Peripheral T-Cell Lymphoma Pro auto Peter Reimer Klinik für Hämatologie / intern. Onkologie und Stammzelltransplantation Kliniken Essen Süd, Evang. Krankenhaus Essen-Werden ggmbh COSTEM, Berlin 09.09.2011
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center
 Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
Angioimmunoblastic T-cell lymphoma: nobody knows what to do...
 Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
What is the best approach to the initial therapy of PTCL? standards of treatment? Should all
 What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
TCH em Linfomas T. Fábio R. Kerbauy
 TCH em Linfomas T Fábio R. Kerbauy T-Cell Lymphomas ( 6000 cases/y USA) J Clin Oncol 2008;26:4124-4130 Proportion T-cell lymphomas prognosis by subtipe 1.0 0.9 0.8 0.7 0.6 0.5 ALCL ALK+ 0.4 0.3 0.2 0.1
TCH em Linfomas T Fábio R. Kerbauy T-Cell Lymphomas ( 6000 cases/y USA) J Clin Oncol 2008;26:4124-4130 Proportion T-cell lymphomas prognosis by subtipe 1.0 0.9 0.8 0.7 0.6 0.5 ALCL ALK+ 0.4 0.3 0.2 0.1
Is there a Role for Upfront Stem Cell Transplantation in Peripheral T-Cell Lymphoma: YES!
 Is there a Role for Upfront Stem ell Transplantation in Peripheral T-ell Lymphoma: YES! Norbert Schmitz Dep. Hematology, Oncology and Stem ell Transplantation AK St. Georg Hamburg, Germany OS in the common
Is there a Role for Upfront Stem ell Transplantation in Peripheral T-ell Lymphoma: YES! Norbert Schmitz Dep. Hematology, Oncology and Stem ell Transplantation AK St. Georg Hamburg, Germany OS in the common
Controversies and Approaches to T cell Lymphoma Therapy in 2016
 Controversies and Approaches to T cell Lymphoma Therapy in 2016 Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Associate Professor of Medicine Weill
Controversies and Approaches to T cell Lymphoma Therapy in 2016 Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Associate Professor of Medicine Weill
Prognostic Factors for PTCL. Julie M. Vose, M.D., M.B.A. University of Nebraska Medical Center
 Prognostic Factors for PTCL Julie M. Vose, M.D., M.B.A. University of Nebraska Medical Center jmvose@unmc.edu Distribution of 1314 Cases by Consensus Diagnosis International T-Cell Lymphoma Project Vose
Prognostic Factors for PTCL Julie M. Vose, M.D., M.B.A. University of Nebraska Medical Center jmvose@unmc.edu Distribution of 1314 Cases by Consensus Diagnosis International T-Cell Lymphoma Project Vose
Updates in T cell Lymphoma
 Winship Cancer Institute of Emory University Updates in T cell Lymphoma Mary Jo Lechowicz August 2014 Objectives Update current care for patients with Peripheral T cell Non Hodgkin lymphomas (PTCL) upfront
Winship Cancer Institute of Emory University Updates in T cell Lymphoma Mary Jo Lechowicz August 2014 Objectives Update current care for patients with Peripheral T cell Non Hodgkin lymphomas (PTCL) upfront
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients
 Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
The treatment of DLBCL. Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona
 The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Peripheral T-cell lymphoma. Matt Ahearne Clinical Lecturer, Leicester
 Peripheral T-cell lymphoma Matt Ahearne Clinical Lecturer, Leicester PTCL Objectives To understand the natural history of PTCL To appreciate the importance of accurate diagnosis of PTCL including recent
Peripheral T-cell lymphoma Matt Ahearne Clinical Lecturer, Leicester PTCL Objectives To understand the natural history of PTCL To appreciate the importance of accurate diagnosis of PTCL including recent
Changing the landscape of treatment in Peripheral T-cell Lymphoma
 Changing the landscape of treatment in Peripheral T-cell Lymphoma Luis Fayad Associate Professor MD Anderson Cancer Center Department of Lymphoma and Myeloma 1 6 What is peripheral 2008 WHO CLASSIFICATION
Changing the landscape of treatment in Peripheral T-cell Lymphoma Luis Fayad Associate Professor MD Anderson Cancer Center Department of Lymphoma and Myeloma 1 6 What is peripheral 2008 WHO CLASSIFICATION
FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting?
 Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
Peripheral T-cell lymphomas (PTCL) Specified and Unspecified. Eric Van Den Neste Cliniques universitaires Saint-Luc Bruxelles
 Specified and Unspecified. Eric Van Den Neste Cliniques universitaires Saint-Luc Bruxelles") Peripheral T-cell lymphomas (PTCL) Specified and Unspecified Eric Van Den Neste Cliniques universitaires Saint-Luc Bruxelles BHS seminar 12, 07 March 2015 Peripheral T-cell lymphomas (PTCL) Specified and
Peripheral T-cell lymphomas (PTCL) Specified and Unspecified Eric Van Den Neste Cliniques universitaires Saint-Luc Bruxelles BHS seminar 12, 07 March 2015 Peripheral T-cell lymphomas (PTCL) Specified and
Outcomes of patients with peripheral T-cell lymphoma in first complete remission: data from three tertiary Asian cancer centers
 Tang et al. (2017) 7:653 DOI 10.1038/s41408-017-0030-y CORRESPONDENCE Outcomes of patients with peripheral T-cell lymphoma in first complete remission: data from three tertiary Asian cancer centers Open
Tang et al. (2017) 7:653 DOI 10.1038/s41408-017-0030-y CORRESPONDENCE Outcomes of patients with peripheral T-cell lymphoma in first complete remission: data from three tertiary Asian cancer centers Open
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University
 Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
PET-CT in Peripheral T-cell Lymphoma: To Be or Not To Be
 PET-CT in Peripheral T-cell Lymphoma: To Be or Not To Be Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, DC, USA So What is the Question(s)? What is
PET-CT in Peripheral T-cell Lymphoma: To Be or Not To Be Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, DC, USA So What is the Question(s)? What is
T-cell Lymphomas Biology and Management
 T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma
 How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr Claire Burney, Lymphoma Clinical Fellow, Bristol Haematology and Oncology Centre, UK
 EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
Development of Mogamulizumab, a defucosylated anti-ccr4 humanized monoclonal antibody
 New Drugs in Hematology Development of Mogamulizumab, a defucosylated anti-ccr4 humanized monoclonal antibody Michinori Ogura, MD, PhD Department of Hematology Tokai Central Hospital Bologna, Royal Hotel
New Drugs in Hematology Development of Mogamulizumab, a defucosylated anti-ccr4 humanized monoclonal antibody Michinori Ogura, MD, PhD Department of Hematology Tokai Central Hospital Bologna, Royal Hotel
SEQUENCING FOLLICULAR LYMPHOMA
 SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
Mantle Cell Lymphoma: Update in Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency
 Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Role of consolidation therapy in Multiple Myeloma. Pieter Sonneveld. Erasmus MC Cancer Institute Rotterdam The Netherlands
 Role of consolidation therapy in Multiple Myeloma Pieter Sonneveld Erasmus MC Cancer Institute Rotterdam The Netherlands Disclosures Research support : Amgen, Celgene, Janssen, Karyopharm Advisory Boards/Honoraria:
Role of consolidation therapy in Multiple Myeloma Pieter Sonneveld Erasmus MC Cancer Institute Rotterdam The Netherlands Disclosures Research support : Amgen, Celgene, Janssen, Karyopharm Advisory Boards/Honoraria:
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
GVHD & GVL in the lymphoma setting: The case of CLL
 GVHD & GVL in the lymphoma setting: The case of CLL Peter Dreger Dept. Internal Medicine V University of Heidelberg EBMT: SCT for CLL 2000-2010 Update January 2012 allo auto 400 350 300 250 200 150 100
GVHD & GVL in the lymphoma setting: The case of CLL Peter Dreger Dept. Internal Medicine V University of Heidelberg EBMT: SCT for CLL 2000-2010 Update January 2012 allo auto 400 350 300 250 200 150 100
Open questions in the treatment of Follicular Lymphoma. Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland
 Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
AIH, Marseille 30/09/06
 ALLOGENEIC STEM CELL TRANSPLANTATION FOR MYELOID MALIGNANCIES Transplant and Cellular Therapy Unit Institut Paoli Calmettes Inserm U599 Université de la Méditerranée ée Marseille, France AIH, Marseille
ALLOGENEIC STEM CELL TRANSPLANTATION FOR MYELOID MALIGNANCIES Transplant and Cellular Therapy Unit Institut Paoli Calmettes Inserm U599 Université de la Méditerranée ée Marseille, France AIH, Marseille
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Interim PET in Diffuse Large B Cell Lymphoma.The GEL/TAMO experience
 Interim PET in Diffuse Large B Cell Lymphoma.The GEL/TAMO experience MD. Caballero, Hospital Universitario, Salamanca, Spain. Chair of The GEL/TAMO Group Menton,9 april 2010 Disclosures for Dolores Caballero
Interim PET in Diffuse Large B Cell Lymphoma.The GEL/TAMO experience MD. Caballero, Hospital Universitario, Salamanca, Spain. Chair of The GEL/TAMO Group Menton,9 april 2010 Disclosures for Dolores Caballero
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al:
 Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents
 Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
LYMPHOMA in HIV PATIENTS. Silvia Montoto, St Bartholomew s Hospital, London, UK ESMO Preceptorship on Lymphoma
 LYMPHOMA in HIV PATIENTS Silvia Montoto, St Bartholomew s Hospital, London, UK ESMO Preceptorship on Lymphoma Lugano, 3-4 November 2017 Disclosures: Roche: honoraria Gilead: travel grant ESMO Preceptorship
LYMPHOMA in HIV PATIENTS Silvia Montoto, St Bartholomew s Hospital, London, UK ESMO Preceptorship on Lymphoma Lugano, 3-4 November 2017 Disclosures: Roche: honoraria Gilead: travel grant ESMO Preceptorship
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
MUD SCT for Paediatric AML?
 7 th South African Symposium on Haematopoietic Stem Cell Transplantation MUD SCT for Paediatric AML? Alan Davidson Haematology / Oncology Service Red Cross Children s Hospital THE SCENARIO A 10 year old
7 th South African Symposium on Haematopoietic Stem Cell Transplantation MUD SCT for Paediatric AML? Alan Davidson Haematology / Oncology Service Red Cross Children s Hospital THE SCENARIO A 10 year old
Induction Therapy & Stem Cell Transplantation for Myeloma
 Induction Therapy & Stem Cell Transplantation for Myeloma William Bensinger, MD Professor of Medicine, Division of Oncology University of Washington School of Medicine Director, Autologous Stem Cell Transplant
Induction Therapy & Stem Cell Transplantation for Myeloma William Bensinger, MD Professor of Medicine, Division of Oncology University of Washington School of Medicine Director, Autologous Stem Cell Transplant
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL
 Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham
 Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Multiple Myeloma Updates 2007
 Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
allosct and CLL in the BCRi era time for a study
 allosct and CLL in the BCRi era time for a study Patient characteristics in BCRi studies and allosct candidates DIFFER Facts on BCRi no Cure Risk factors for shorter BCRi efficacy in MV analysis? PA-refractory
allosct and CLL in the BCRi era time for a study Patient characteristics in BCRi studies and allosct candidates DIFFER Facts on BCRi no Cure Risk factors for shorter BCRi efficacy in MV analysis? PA-refractory
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
Aktuelle Therapiestrategien beim peripheren T-NHL , Hannover
 Aktuelle Therapiestrategien beim peripheren T-NHL 16.1.2009, Hannover Bertram Glass Asklepios Klinik St.Georg, Hamburg Abteilung Hämatologie und Stammzelltransplantation Mature (peripheral) T-NHL Histologic
Aktuelle Therapiestrategien beim peripheren T-NHL 16.1.2009, Hannover Bertram Glass Asklepios Klinik St.Georg, Hamburg Abteilung Hämatologie und Stammzelltransplantation Mature (peripheral) T-NHL Histologic
Update: Chronic Lymphocytic Leukemia
 ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes
 Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Brentuximab, Nivolumab: L esperienza Real Word della REP. Dr.ssa Clara De Risi Az. Osp. Card. G. Panico - Tricase
 Brentuximab, Nivolumab: L esperienza Real Word della REP Dr.ssa Clara De Risi Az. Osp. Card. G. Panico - Tricase MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY IMPROVE
Brentuximab, Nivolumab: L esperienza Real Word della REP Dr.ssa Clara De Risi Az. Osp. Card. G. Panico - Tricase MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY IMPROVE
Recent Advances in the Treatment of Peripheral T-Cell Lymphoma
 Hematologic Malignancies Recent Advances in the Treatment of Peripheral T-Cell Lymphoma KAMEL LARIBI, a MUSTAPHA ALANI, a CATHERINE TRUONG, b ALIX BAUGIER DE MATERRE c a Department of Hematology, Centre
Hematologic Malignancies Recent Advances in the Treatment of Peripheral T-Cell Lymphoma KAMEL LARIBI, a MUSTAPHA ALANI, a CATHERINE TRUONG, b ALIX BAUGIER DE MATERRE c a Department of Hematology, Centre
Confronto Real world e studi registrativi
 Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Immune checkpoint inhibitors in lymphoma. Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust
 Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
LYSA PET adapted programs. O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France
 LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
BACKGROUND AND RATIONALE
 SYNOPSIS Observational study on the use of B cell receptor kinase inhibitors and BCL2 antagonists prior to allogeneic hematopoietic stem cell transplantation for B cell malignancies: A joint project of
SYNOPSIS Observational study on the use of B cell receptor kinase inhibitors and BCL2 antagonists prior to allogeneic hematopoietic stem cell transplantation for B cell malignancies: A joint project of
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pralatrexate (Folotyn) for Peripheral T-cell Lymphoma
 for Peripheral T-cell Lymphoma") pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pralatrexate (Folotyn) for Peripheral T-cell Lymphoma January 31, 2019 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pralatrexate (Folotyn) for Peripheral T-cell Lymphoma January 31, 2019 DISCLAIMER Not a Substitute for Professional Advice This report
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin
 What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
Multiple myeloma, 25 (45) years of progress. The IFM experience in patients treated with frontline ASCT. Philippe Moreau, Nantes
 years of progress. The IFM experience in patients treated with frontline ASCT. Philippe Moreau, Nantes") Multiple myeloma, 25 (45) years of progress The IFM experience in patients treated with frontline ASCT Philippe Moreau, Nantes Shibata T. Prolonged survival in a case of multiple myeloma treated with high
Multiple myeloma, 25 (45) years of progress The IFM experience in patients treated with frontline ASCT Philippe Moreau, Nantes Shibata T. Prolonged survival in a case of multiple myeloma treated with high
What s new in Blood and Marrow Transplant? Saar Gill, MD PhD Jan 22, 2016
 What s new in Blood and Marrow Transplant? Saar Gill, MD PhD Jan 22, 2016 Division of Hematology-Oncology University of Pennsylvania Perelman School of Medicine 1 Who should be transplanted and how? Updates
What s new in Blood and Marrow Transplant? Saar Gill, MD PhD Jan 22, 2016 Division of Hematology-Oncology University of Pennsylvania Perelman School of Medicine 1 Who should be transplanted and how? Updates
Treatment outcomes of IMEP as a front-line chemotherapy for patients with peripheral T-cell lymphomas
 BLOOD RESEARCH VOLUME 51 ㆍ NUMBER 3 September 2016 ORIGINAL ARTICLE Treatment outcomes of IMEP as a front-line chemotherapy for patients with peripheral T-cell lymphomas Ji Young Lee 1, Sang Min Lee 1,
BLOOD RESEARCH VOLUME 51 ㆍ NUMBER 3 September 2016 ORIGINAL ARTICLE Treatment outcomes of IMEP as a front-line chemotherapy for patients with peripheral T-cell lymphomas Ji Young Lee 1, Sang Min Lee 1,
The case for maintenance rituximab in FL
 New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
Haploidentical Transplants for Lymphoma. Andrea Bacigalupo Universita Cattolica Policlinico Gemelli Roma - Italy
 Haploidentical Transplants for Lymphoma Andrea Bacigalupo Universita Cattolica Policlinico Gemelli Roma - Italy HODGKIN NON HODGKIN Non Myelo Ablative Regimen Luznik L et al BBMT 2008 Comparison of Outcomes
Haploidentical Transplants for Lymphoma Andrea Bacigalupo Universita Cattolica Policlinico Gemelli Roma - Italy HODGKIN NON HODGKIN Non Myelo Ablative Regimen Luznik L et al BBMT 2008 Comparison of Outcomes
Philadelphia-positive Acute Lymphoblastic Leukemia
 Philadelphia-positive Acute Lymphoblastic Leukemia Nicolas Boissel Service d Hématologie Unité Adolescents et Jeunes Adultes Hôpital Saint-Louis, Paris Ph+ acute lymphoblastic leukemia DR+, CD19+, CD22+,
Philadelphia-positive Acute Lymphoblastic Leukemia Nicolas Boissel Service d Hématologie Unité Adolescents et Jeunes Adultes Hôpital Saint-Louis, Paris Ph+ acute lymphoblastic leukemia DR+, CD19+, CD22+,
Adult ALL: NILG experience
 Adult ALL: NILG experience R Bassan USC Ematologia, Ospedali Riuniti, Bergamo SIE Interregionale, Padova 12 5 2011 Now and then Northern Italy Leukemia Group 2000-10 Prospective clinical trials 09/00 10/07
Adult ALL: NILG experience R Bassan USC Ematologia, Ospedali Riuniti, Bergamo SIE Interregionale, Padova 12 5 2011 Now and then Northern Italy Leukemia Group 2000-10 Prospective clinical trials 09/00 10/07
AHSCT in Hodgkin lymphoma - indication and challenges. Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital
 AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
Which is the best treatment for relapsed APL?
 Which is the best treatment for relapsed APL? 7th International Symposium on Acute Promyelocytic Leukemia, Rome, September 24 27, 2017 Eva Lengfelder Department of Hematology and Oncology University Hospital
Which is the best treatment for relapsed APL? 7th International Symposium on Acute Promyelocytic Leukemia, Rome, September 24 27, 2017 Eva Lengfelder Department of Hematology and Oncology University Hospital
REVIEW. KEY WORDS: Diffuse large B cell lymphoma, Hematopoietic stem cell transplantation, Systematic evidencebased review, Therapy, Adult
 REVIEW The Role of Cytotoxic Therapy with Hematopoietic Stem Cell Transplantation in the Treatment of Diffuse Large B Cell Lymphoma: Update of the 2001 Evidence-Based Review Denise M. Oliansky, 1 Myron
REVIEW The Role of Cytotoxic Therapy with Hematopoietic Stem Cell Transplantation in the Treatment of Diffuse Large B Cell Lymphoma: Update of the 2001 Evidence-Based Review Denise M. Oliansky, 1 Myron
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Initial Therapy For Transplant-Eligible Patients With Multiple Myeloma. Michele Cavo, MD University of Bologna Bologna, Italy
 Initial Therapy For Transplant-Eligible Patients With Multiple Myeloma Michele Cavo, MD University of Bologna Bologna, Italy Treatment Paradigm for Autotransplant-Eligible Patients With Multiple Myeloma
Initial Therapy For Transplant-Eligible Patients With Multiple Myeloma Michele Cavo, MD University of Bologna Bologna, Italy Treatment Paradigm for Autotransplant-Eligible Patients With Multiple Myeloma
Bendamustine: A Transversal * Chemotherapy Agent
 Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011
 Joan Bladé Berlin, September 9 th, 2011") Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011 Significant impact of ASCT before the availability of novel agents? Randomized trials: Single
Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011 Significant impact of ASCT before the availability of novel agents? Randomized trials: Single
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
CME Information LEARNING OBJECTIVES
 CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant
 Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES!
 Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Acute Myeloid Leukemia
 Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
East Midlands Cancer Network Guidelines for diagnosis and management of mature T cell and NK cell lymphomas (excluding cutaneous T cell lymphoma)
") East Midlands Cancer Network Guidelines for diagnosis and management of mature T cell and NK cell lymphomas (excluding cutaneous T cell lymphoma) Written by: Dr Chris Fox with input from Dr Fiona Miall
East Midlands Cancer Network Guidelines for diagnosis and management of mature T cell and NK cell lymphomas (excluding cutaneous T cell lymphoma) Written by: Dr Chris Fox with input from Dr Fiona Miall
CONSIDERATIONS IN DESIGNING ACUTE GVHD PREVENTION TRIALS: Patient Selection, Concomitant Treatments, Selecting and Assessing Endpoints
 CONSIDERATIONS IN DESIGNING ACUTE GVHD PREVENTION TRIALS: Patient Selection, Concomitant Treatments, Selecting and Assessing Endpoints CENTER FOR INTERNATIONAL BLOOD AND MARROW TRANSPLANT RESEARCH Potential
CONSIDERATIONS IN DESIGNING ACUTE GVHD PREVENTION TRIALS: Patient Selection, Concomitant Treatments, Selecting and Assessing Endpoints CENTER FOR INTERNATIONAL BLOOD AND MARROW TRANSPLANT RESEARCH Potential
Transformed lymphoma: biology and treatment
 Transformed lymphoma: biology and treatment Silvia Montoto Centre for Haemato-Oncology Barts Cancer Institute 1.00 0.75 0.50 0.25 0.00 N =330 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 Years %Viability
Transformed lymphoma: biology and treatment Silvia Montoto Centre for Haemato-Oncology Barts Cancer Institute 1.00 0.75 0.50 0.25 0.00 N =330 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 Years %Viability
Inotuzumab Ozogamicin in ALL. Hagop Kantarjian M.D. May 2016 Bologna, Italy
 Inotuzumab Ozogamicin in ALL Hagop Kantarjian M.D. May 2016 Bologna, Italy Immuno Oncology in ALL Monoclonals + cytotoxic agents e.g.inotuzumab Bispecific monoclonals (CD3 + CD19) e.g.blinatumomab Modified
Inotuzumab Ozogamicin in ALL Hagop Kantarjian M.D. May 2016 Bologna, Italy Immuno Oncology in ALL Monoclonals + cytotoxic agents e.g.inotuzumab Bispecific monoclonals (CD3 + CD19) e.g.blinatumomab Modified
Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA
 Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA Disclosures Consulting advice: Hospira, Bayer, Juno Therapeutics, Teva, Oncotracker, Gilead
Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA Disclosures Consulting advice: Hospira, Bayer, Juno Therapeutics, Teva, Oncotracker, Gilead
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Aggressive B and T cell lymphomas: Treatment paradigms in 2018
 Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate