Immuno-Oncology. Glioblastoma and CNS tumors 5 July 2016 Siena, Italy
|
|
|
- Osborn Allison
- 6 years ago
- Views:
Transcription


1 ESMO Preceptorship Programme Immuno-Oncology From the essentials of tumour immunology to clinical application Glioblastoma and CNS tumors 5 July 2016 Siena, Italy Michael Weller Department of Neurology & Brain Tumor Center University Hospital Zurich Frauenklinikstrasse 26 CH-8091 Zurich michael.weller@usz.ch
2
3
4 Immunosuppression in glioblastoma: challenging a popular assumption The brain is an immunoprivileged site: is there need for additional immunosuppression? Glioblastoma cells (may) lack tumor-specific antigens: why additional suppression of a blinded immune system? Is there evidence that immune surveillance accounts for the low incidence of systemic metastasis in glioblastoma? The increased incidence of glioblastoma in the elderly may relate to immune senescence, but why is there no increased risk with immunodeficiency states including AIDS?
5 Current approaches of immunotherapy for glioblastoma Ipilimumab (anti-ctla-4) (Yervoy, BMS) Pembrolizumab (anti-pd-1) (Keytruda, MSD) Nivolumab (anti-pd-1) (Opdivo, BMS) Atezolizumab (anti-pd-l1) (Roche) TGF-β antisense oligonucleotide (Trabedersen, Antisense Pharma/Isarna) TGF-β receptor antagonists (LY , Galunisertib, Lilly) Vaccination against EGFRvIII (Rindopepimut, Rintega, Celldex) DC/peptide-based immunotherapy (ICT-107, Immunocellular) DC/lysate-based immunotherapy (DCVax, NW Biotherapeutics) Personalized multipeptide vaccination (IMA950, Immatics GAPVAC) DC/CMV-targeted immunotherapy (Duke) IDH-targeted immunotherapy (Heidelberg, and others) Chimeric antigen receptor (CAR) therapy (e.g., EGFRvIII)
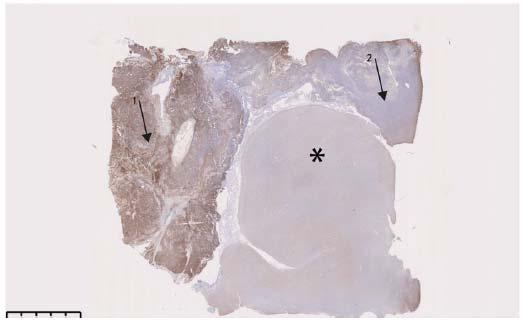
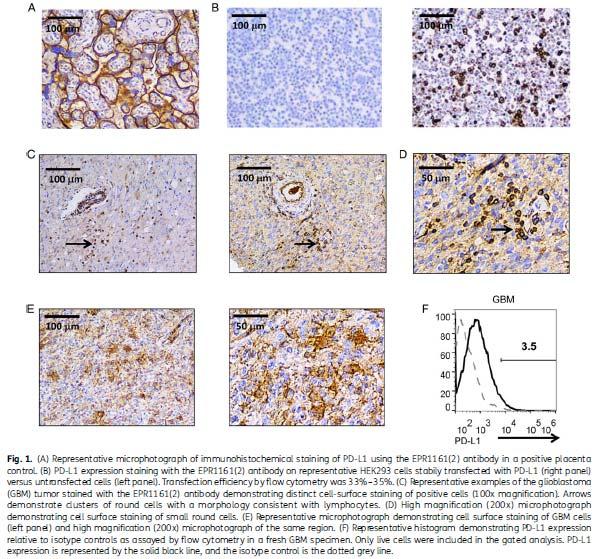
6 Expression and prognostic role of PD-L1 in glioblastoma
7 Current status of the PD-1/PD-L-1 axis in glioblastoma PD-L1 is expressed in human glioblastoma in vivo TCGA and other public data bases do not define a major prognostic role for PD-L1 expression in glioblastoma The significance as a biomarker of tumoral versus nontumoral PD-L1 expression remains to be determined in glioblastoma, like in many other cancers Preclinical studies demonstrate activity of PD-1 inhibition in rodent glioma models

8 Immunosuppression in the glioblastoma microenvironment Nduom et al. Neuro-Oncology 2015:17:vii9-vii14
9 Current approaches of immunotherapy for glioblastoma CheckMate 143

10 CheckMate 143 Transition from phase II to III
11 Trial name / ClinicalTrials.gov Identifier Target population Treatment arms Phase Primary endpoint Status (as per March 2016) CheckMate 143 NCT First recurrence of glioblastoma Experimental: nivolumab Comparator: bevacizumab III OS Accrual completed CheckMate 498 NCT Newly diagnosed glioblastoma Unmethylated MGMT promoter Experimental: RT + nivolumab Comparator: TMZ/RT TMZ III OS Not yet recruiting CheckMate 548 NCT Newly diagnosed glioblastoma Methylated MGMT promoter Experimental: TMZ/RT TMZ + nivolumab Comparator: TMZ/RT TMZ + placebo II OS Not yet recruiting NCT Newly diagnosed or recurrent glioblastoma requiring surgery Nivolumab (neoadjuvant, before surgery) II PD-L1 expression (lymphocytes, tumor) Recruiting NCT Newly diagnosed glioblastoma Arm 1: TMZ + ipilimumab Arm 2: TMZ + nivolumab Arm 3: TMZ + ipilimumab + nivolumab I MTD (ipilimumab, nivolumab, combination) Recruiting NCT Recurrent high grade glioma Hypofractionated stereotactic re- RT + bevacizumab + pembrolizumab I MTD (pembrolizumab) Recruiting NCT Recurrent glioblastoma Cohort A: pembrolizumab + bevacizumab Cohort B: pembrolizumab II Cohort A: PFS-6 Cohort B: MTD (pembrolizumab) Not recruiting NCT Recurrent glioblastoma Pembrolizumab II PFS-6 Recruiting NCT Recurrent glioblastoma, Pembrolizumab n/a Response rate Recruiting hypermutator phenotype NCT Newly diagnosed or recurrent glioblastoma MEDI4736, Bevacizumab + MEDI4736, RT + MEDI4736 II OS-12, PFS-6, OS-6 (depending on treatment) Recruiting
12 Current approaches of immunotherapy for glioblastoma Ipilimumab (anti-ctla-4) (Yervoy, BMS) Pembrolizumab (anti-pd-1) (Keytruda, MSD) Nivolumab (anti-pd-1) (Opdivo, BMS) Atezolizumab (anti-pd-l1) (Roche) TGF-β antisense oligonucleotide (Trabedersen, Antisense Pharma/Isarna) TGF-β receptor antagonists (LY , Galunisertib, Lilly) Vaccination against EGFRvIII (Rindopepimut, Rintega, Celldex) DC/peptide-based immunotherapy (ICT-107, Immunocellular) DC/lysate-based immunotherapy (DCVax, NW Biotherapeutics) Personalized multipeptide vaccination (IMA950, Immatics GAPVAC) DC/CMV-targeted immunotherapy (Duke) IDH-targeted immunotherapy (Heidelberg, and others) Chimeric antigen receptor (CAR) therapy (e.g., EGFRvIII)
13 TGF-β and immunosuppression in glioblastoma: clinical studies
14 Current approaches of immunotherapy for glioblastoma Ipilimumab (anti-ctla-4) (Yervoy, BMS) Pembrolizumab (anti-pd-1) (Keytruda, MSD) Nivolumab (anti-pd-1) (Opdivo, BMS) Atezolizumab (anti-pd-l1) (Roche) TGF-β antisense oligonucleotide (Trabedersen, Antisense Pharma/Isarna) TGF-β receptor antagonists (LY , Galunisertib, Lilly) Vaccination against EGFRvIII (Rindopepimut, Rintega, Celldex) DC/peptide-based immunotherapy (ICT-107, Immunocellular) DC/lysate-based immunotherapy (DCVax, NW Biotherapeutics) Personalized multipeptide vaccination (IMA950, Immatics GAPVAC) DC/CMV-targeted immunotherapy (Duke) IDH-targeted immunotherapy (Heidelberg, and others) Chimeric antigen receptor (CAR) therapy (e.g., EGFRvIII)
15


")
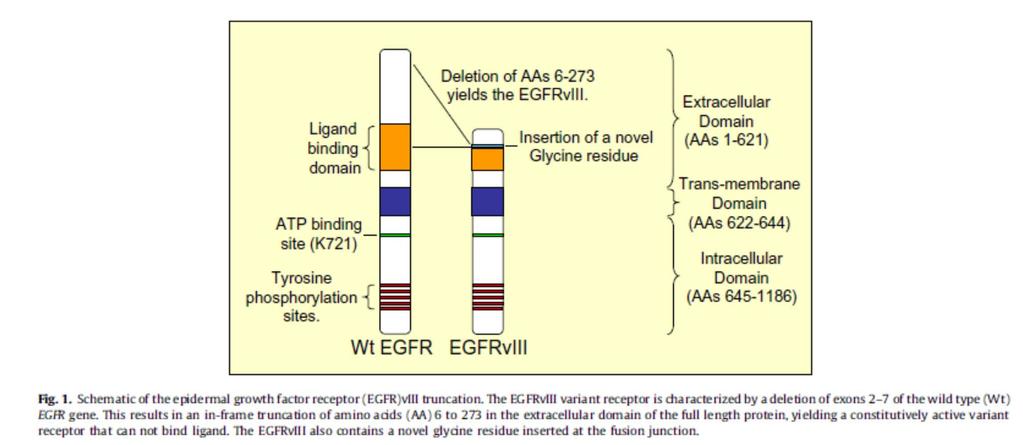
16 Coexpression of wild-type EGFR and EGFRvIII expression in glioblastoma EGFRwt (3C6) GB 1097 EGFRvIII (L8A4) Overlap GB 1097 GB 1122

17

18 Are EGFRvIII-positive cells special? Inda et al. Genes Dev 2010;24:

19 Cooperation of wild-type EGFR and EGFRvIII in experimental glioblastoma Fan et al. Cancer Cell 2013;24:438-49
 chemically conjugated to Keyhole Limpet Hemocyanin Delivered as intradermal injection of 500ug rindopepimut with 150ug GM-CSF as an adjuvant Stable,")
20 Rindopepimut (CDX-110) Vaccine designed to generate a specific immune response against EGFRvIII-expressing tumors Off the shelf vaccine recognized across HLA types Consists of the EGFRvIII antigen (unique 13 amino acid peptide sequence) chemically conjugated to Keyhole Limpet Hemocyanin Delivered as intradermal injection of 500ug rindopepimut with 150ug GM-CSF as an adjuvant Stable, lyophilized formulation LEEKKGNYVVTDHC O S N O O N KLH >30
21 Progression-free survival (from diagnosis) Survival Probability p = 0.44 Median (months) Comparison to Historical Control ACT III (n=65) 12.3 p = ACT II (n=22) 15.3 p = ACTIVATE (n=18) 14.2 p = Matched historical control (n=17) 6.4 PFS from diagnosis (months) ACT III Primary Endpoint Progression-free survival (PFS) at 5.5 months from vaccination ( 8.5 months from diagnosis): PFS = 66% p = vs. null hypothesis (H 0 ) 53% Vaccinations begin approximately 3 months after diagnosis
22 Overall survival (from diagnosis) Median (months) OS at 24 Months OS at 36 Months Comparison to Historical Control Survival Probability p = 0.46 ACT III (n=65) % 31% p = < ACT II (n=22) % 23% p = ACTIVATE (n=18) % 33% p = Matched historical control (n=17) % 6% OS from diagnosis (months) Vaccinations begin approximately 3 months after diagnosis Median duration of follow-up: ACT III: 48.7 months ACT II: 71.8 months ACTIVATE: 99.3 months

 were EGFRvIII(+) at recurrence Robust anti-egfrviii titers in most patients; titers maintained for > 6")
23 Does Rindopepimut mediate EGFRvIII elimination at recurrence? Pre-Vaccine Primary Tumor Post Vaccine Recurrent Tumor EGFRvIII was selectively eliminated in recurrent tumors for 26/32 (81%) patients across all three studies 15/15 control patients treated with RT/TMZ (+/- CPT-11, bevacizumab or erlotinib) were EGFRvIII(+) at recurrence Robust anti-egfrviii titers in most patients; titers maintained for > 6 months following cessation of treatment 1. Mehta, et. al. JCO 2011
24 ACT IV Study Design R A N D O M I Z A T I O N Vaccine Priming D1 D15 C1D1 C1D22 Adjuvant Temozolomide and Vaccine Therapy (TMZ-V, 6-12 cycles) Vaccine Maintenance Therapy (VMT) C2D22 C3D22 etc. C1D1 C2D1 etc Follow Up Dose vaccine days 1 and 15 of Vaccine Priming cycle Start cycle within 4 days after randomization and within 7-14 days after completion of CRT Vaccine or control (KLH) is administered Day 22 of each TMZ cycle Begin TMZ no sooner than 6 days after administration of the second vaccine priming dose Begin TMZ no sooner than 28 days after completion of CRT Begin TMZ when ANC 1000/ L and platelets 100,000/ L TMZ dosed days 1-5 of each 28 day cycle If no disease progression after TMZ, continue dosing vaccine every 28 days (Day 1 ±3 days of each 28 day cycle) until intolerance or disease progression Follow-up for overall survival every 12 weeks after disease progression Temozolomide Dosing Vaccine or Control (KLH) Dosing CRT Chemoradiation Therapy Treatment will be discontinued upon disease progression, unacceptable treatment-related toxicity, or patient refusal to continue study treatment
25
26
 Progression during or within two months of bevacizumab Open-label treatment Study vaccine + bevacizumab 27")
27 ReACT Bevacizumab naïve Study vaccine + Randomization (1:1) (n=70) bevacizumab No prior bevacizumab or VEGF/ Double-blind VEGF receptor-targeted agents treatment Control + bevacizumab Bevacizumab refractory (Initial cohort: n=25 Expansion cohort: n=up to 73) Progression during or within two months of bevacizumab Open-label treatment Study vaccine + bevacizumab 27 27
28 Overall Survival Median, months (95% CI) OS 12 OS 18 OS 24 Rindopepimut + BV 11.3 (9.9, 16.2) 44% 32% 25% Control + BV 9.3 (7.1, 11.4) 32% 13% 0% HR = 0.53 (0.32, 0.88) p = * Per-protocol population analyses: HR = 0.53 (0.31, 0.90) p = * Five patients in the rindopepimut + BV arm, and 1 patient in the control + BV arm, continue survival follow-up without progression per expert review. * Log-rank test (2-sided) 28

29 Where do we go from here? Rindopepimut Bevacizumab


30
31 Current approaches of immunotherapy for glioblastoma Ipilimumab (anti-ctla-4) (Yervoy, BMS) Pembrolizumab (anti-pd-1) (Keytruda, MSD) Nivolumab (anti-pd-1) (Opdivo, BMS) Atezolizumab (anti-pd-l1) (Roche) TGF-β antisense oligonucleotide (Trabedersen, Antisense Pharma/Isarna) TGF-β receptor antagonists (LY , Galunisertib, Lilly) Vaccination against EGFRvIII (Rindopepimut, Rintega, Celldex) DC/peptide-based immunotherapy (ICT-107, Immunocellular) DC/lysate-based immunotherapy (DCVax, NW Biotherapeutics) Personalized multipeptide vaccination (IMA950, Immatics GAPVAC) DC/CMV-targeted immunotherapy (Duke) IDH-targeted immunotherapy (Heidelberg, and others) Chimeric antigen receptor (CAR) therapy (e.g., EGFRvIII)
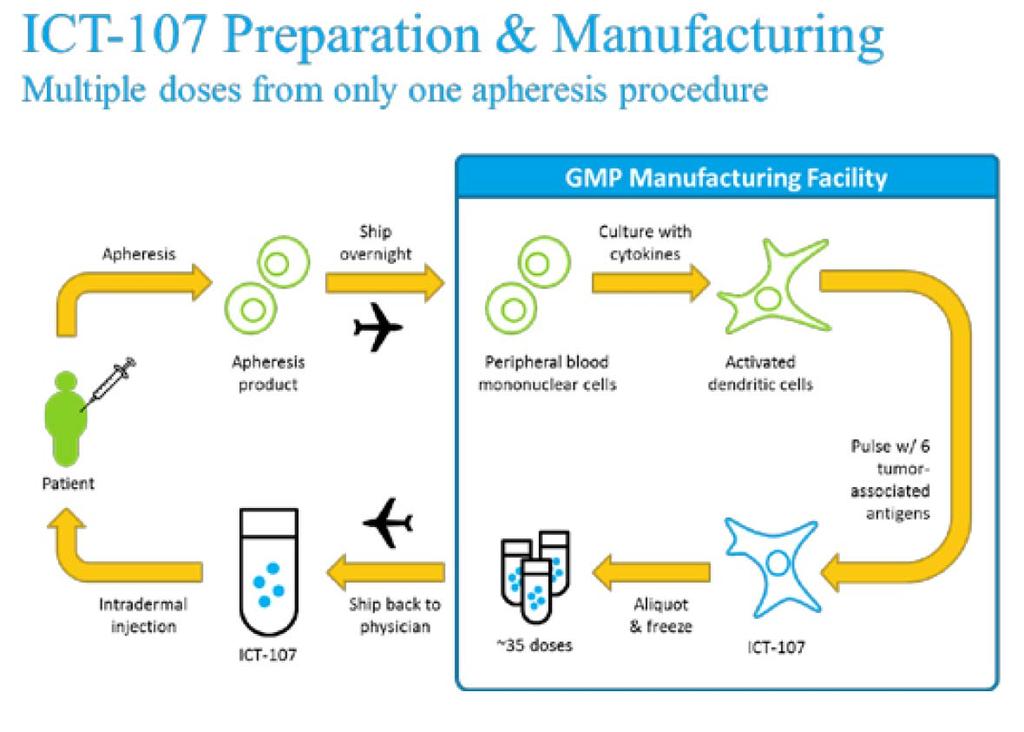
32 ICT-107: an autologous six-antigen DC vaccine Matured, Activated, Peptide-loaded DC MHC Class I Six 9-10 amino acid antigen epitopes MAGE-1 (HLA - A1) AIM-2 (A1) gp100 (HLA - A2) IL-13Rα2 (A2) HER2/neu (A2) TRP-2 (A2) Rationale for antigen choice Targeting multiple antigens minimizes tumor escape High expression levels for all antigens on GBM samples Bias toward TAA associated with cancer stem cells Control used in Ph II Matured, activated DC without peptide loading
33 ICT-107 Phase II Trial Design Surgery Consent Screen and Enroll SOC Chemoradiation Randomize Eligibility Confirmation Vaccine Induction Phase Patient Specific Vaccination ICT 107 or Control 1/wk for 4 wks Maintenance Phase Week 1 SOC Maintenance TMZ Week 2 Rest Week Week 3 Clinical Assessments + maintenance vaccine (ICT 107 or Control) + tumor assessments Week 4 Rest Week Maintenance includes vaccination on a 1, 3, 6, 6 monthly schedule as long as the patient does not recur
34
35 Patient demographics Population Characteristic ICT-107 (N=81) Control (N=43) Total (N=124) P-Value Fishers Exact Gender [n(%)] Male 44 (54.3%) 31 (72.1%) 75 (60.5%) Female 37 (45.7%) 12 (27.9%) 49 (39.5%) Age Category [n(%)] <50 years 20 (24.7%) 12 (27.9%) 32 (25.8%) >50 years 61 (75.3%) 31 (72.1%) 92 (74.2%) MGMT status [n (%)] Methylated 28 (34.6%) 18 (41.9%) 46 (37.1%) Unmethylated 47 (58.0%) 24 (55.8%) 71 (57.3%) KPS Category [n (%)] (29.6%) 8 (18.6%) 32 (25.8%) (44.4%) 18 (41.9%) 54 (43.5%) <90 20 (24.7%) 17 (39.5%) 37 (29.8%) HLA Type [n (%)] A1=Positive, A2=Negative 33 (40.7%) 14 (32.6%) 47 (37.9%) A1=Negative, A2=Positive 42 (51.9%) 22 (51.2%) 64 (51.6%) A1=Positive, A2=Positive 6 (7.4%) 7 (16.3%) 13 (10.5%) Resection Status Complete resection 58 (71.6%) 32 (74.4%) 90 (72.6%) Subtotal resection 23 (28.4%) 11 (25.6%) 34 (27.4%)
36 Progression-free survival ITT population 100% 90% ICT 107 Control 80% ITT Population (N=124) PERCENT SURVIVING 70% 60% 50% 40% 30% 20% Statistically significant treatment benefit ICT 107 N = 81 (63 events) Median = 11.4 months Age stratified HR = ( ) Age stratified P = Control N = 43 (41 events) Median = 10.1 months 10% 0% DAYS
37 Overall survival ITT population 100% 90% ICT 107 PERCENT SURVIVING 80% 70% 60% 50% 40% 30% ITT Population (N=124) ICT 107 N = 81 (56 events) Median = 18.3 months Age stratified HR = ( ) Age stratified P = Insignificant difference Control 20% 10% Control N = 43 (32 events) Median = 16.7 months 0% DAYS
 Consent HLA-A2 typing Apheresis Stratifications MGMT Age No vs residual < 1 cm 3 tumor Randomize Surgery Screen MRI MGMT and enroll TMZ/RT Eligibility Confirmation MRI")
38 A phase III randomized double-blind, controlled study of ICT-107 with maintenance temozolomide (TMZ) in newly diagnosed glioblastoma following resection and concomitant TMZ chemoradiotherapy (STING - EORTC 1507 Alliance - ICT) Consent HLA-A2 typing Apheresis Stratifications MGMT Age No vs residual < 1 cm 3 tumor Randomize Surgery Screen MRI MGMT and enroll TMZ/RT Eligibility Confirmation MRI Vaccine Induction Phase Patient-Specific Vaccination ICT-107 or Control 1/wk for 4 wks Maintenance Phase DC therapy Maintenance Phase: Maintenance with monthly ICT-107 (patient-specific DC therapy) for 11 months, and once every 6 months thereafter Week until 2depletion or confirmation of progressive disease. CT-107 and TMZ will be administered Rest Weektwo weeks apart during cycle 1 to cycle 6 maintenance TMZ. TMZ will be given Days 1-5 ± 2 days on a 28-day cycle. Study DC therapy will be given on Day 21 ± 2 days. 38
39 Current approaches of immunotherapy for glioblastoma Ipilimumab (anti-ctla-4) (Yervoy, BMS) Pembrolizumab (anti-pd-1) (Keytruda, MSD) Nivolumab (anti-pd-1) (Opdivo, BMS) Atezolizumab (anti-pd-l1) (Roche) TGF-β antisense oligonucleotide (Trabedersen, Antisense Pharma/Isarna) TGF-β receptor antagonists (LY , Galunisertib, Lilly) Vaccination against EGFRvIII (Rindopepimut, Rintega, Celldex) DC/peptide-based immunotherapy (ICT-107, Immunocellular) DC/lysate-based immunotherapy (DCVax, NW Biotherapeutics) Personalized multipeptide vaccination (IMA950, Immatics GAPVAC) DC/CMV-targeted immunotherapy (Duke) IDH-targeted immunotherapy (Heidelberg, and others) Chimeric antigen receptor (CAR) therapy (e.g., EGFRvIII)

40 Chimaeric antigen receptor (CAR) therapy: the molecular concept CD28 4-1BB CD3ζ Heczey, Discov Med 16: , 2013
41 Does immunotherapy for glioblastoma have a future? Most promising field of cancer therapy globally Immunotherapy requires sophisticated logistics Immunotherapy is expensive Immunotherapy may only work in young patients with minimal residual tumor (?)
 WFNO 2017 & EANO ZURICH, SWITZERLAND Kongresshaus Zürich May 3-7, 2017 INVITATION www.")
42 Quadrennial Meeting of the World Federation of Neuro-Oncology WFNO 2017 in conjunction with the Meeting of the European Association of Neuro-Oncology (EANO) WFNO 2017 & EANO ZURICH, SWITZERLAND Kongresshaus Zürich May 3-7, 2017 INVITATION
Immuno-Oncology. Glioblastoma 3 November 2016 Zurich, Switzerland
 ESMO Preceptorship Programme Immuno-Oncology From the essentials of tumour immunology to clinical application Glioblastoma 3 November 2016 Zurich, Switzerland Michael Weller Department of Neurology & Brain
ESMO Preceptorship Programme Immuno-Oncology From the essentials of tumour immunology to clinical application Glioblastoma 3 November 2016 Zurich, Switzerland Michael Weller Department of Neurology & Brain
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA
 IN GLIOBLASTOMA") RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
Pioneering vaccines that transform lives.
 Pioneering vaccines that transform lives. Immunomic Therapeutics, Inc. LAMP-Vax for Glioblastoma: CMV-LAMP-Vax Executive Summary Executive Summary pp65-lamp-vax First Line Therapy for Glioblastoma Multiforme
Pioneering vaccines that transform lives. Immunomic Therapeutics, Inc. LAMP-Vax for Glioblastoma: CMV-LAMP-Vax Executive Summary Executive Summary pp65-lamp-vax First Line Therapy for Glioblastoma Multiforme
NCT HEIDELBERG NATIONAL CENTER FOR TUMOR DISEASES. Sao Paulo, Can immunotherapy be the new weapon in the treatment of gliomas?
 NATIONAL CENTER FOR TUMOR DISEASES NCT HEIDELBERG Sao Paulo, 28.04.2017 Can immunotherapy be the new weapon in the treatment of gliomas? Wolfgang Wick Neurology Clinic, University of Heidelberg Neurooncology
NATIONAL CENTER FOR TUMOR DISEASES NCT HEIDELBERG Sao Paulo, 28.04.2017 Can immunotherapy be the new weapon in the treatment of gliomas? Wolfgang Wick Neurology Clinic, University of Heidelberg Neurooncology
Celldex Therapeutics' Rindopepimut Demonstrates Promising Clinical Activity in Patients with EGFRvIII-positive Recurrent Glioblastoma at SNO
 November 24, 2013 Celldex Therapeutics' Rindopepimut Demonstrates Promising Clinical Activity in Patients with EGFRvIII-positive Recurrent Glioblastoma at SNO Strong interim survival trend (12.0 vs 7.9
November 24, 2013 Celldex Therapeutics' Rindopepimut Demonstrates Promising Clinical Activity in Patients with EGFRvIII-positive Recurrent Glioblastoma at SNO Strong interim survival trend (12.0 vs 7.9
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
HHS Public Access Author manuscript Transl Cancer Res. Author manuscript; available in PMC 2018 October 01.
 Lessons learned from rindopepimut treatment in patients with EGFRvIII-expressing glioblastoma David C. Binder 1, Erik Ladomersky 2, Alicia Lenzen 2, Lijie Zhai 2, Kristen L. Lauing 2, Sebastian D. Otto-Meyer
Lessons learned from rindopepimut treatment in patients with EGFRvIII-expressing glioblastoma David C. Binder 1, Erik Ladomersky 2, Alicia Lenzen 2, Lijie Zhai 2, Kristen L. Lauing 2, Sebastian D. Otto-Meyer
Immunotherapy and checkpoint inhibitors for gliomas
 Pearce et al. Neuroimmunol Neuroinflammation 2018;5:47 DOI: 10.20517/2347-8659.2018.46 Neuroimmunology and Neuroinflammation Review Open Access Immunotherapy and checkpoint inhibitors for gliomas Clairice
Pearce et al. Neuroimmunol Neuroinflammation 2018;5:47 DOI: 10.20517/2347-8659.2018.46 Neuroimmunology and Neuroinflammation Review Open Access Immunotherapy and checkpoint inhibitors for gliomas Clairice
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics. Timothy Cloughesy, MD University of California, Los Angeles
 Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics Timothy Cloughesy, MD University of California, Los Angeles Disclosure 2 FDA Endpoints for the Approval of Cancer
Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics Timothy Cloughesy, MD University of California, Los Angeles Disclosure 2 FDA Endpoints for the Approval of Cancer
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
ESMO PRECEPTORSHIP IN IMMUNO-ONCOLOGY
 ESMO PRECEPTORSHIP IN IMMUNO-ONCOLOGY LUGANO, MAY 4-5, 2018 Clinical development in ovarian cancer C. Sessa, CH CONTENT Rationale for immunotherapy in ovarian cancer Clinical data with single agent immune
ESMO PRECEPTORSHIP IN IMMUNO-ONCOLOGY LUGANO, MAY 4-5, 2018 Clinical development in ovarian cancer C. Sessa, CH CONTENT Rationale for immunotherapy in ovarian cancer Clinical data with single agent immune
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Off-Label Treatments. Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease. Outline
 Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Copyright. Tocagen Inc. Lead Product Candidate: Toca 511 & Toca FC Preclinical Overview
 Lead Product Candidate: Toca 511 & Toca FC Preclinical Overview Toca 511, delivers CD prodrug activator gene selectively to cancer cells Regulatory genes Structural RRV genes CD gene Regulatory genes Toca
Lead Product Candidate: Toca 511 & Toca FC Preclinical Overview Toca 511, delivers CD prodrug activator gene selectively to cancer cells Regulatory genes Structural RRV genes CD gene Regulatory genes Toca
Immunotherapy for Malignant Brain Cancer: Overcoming Immune Suppression to Improve the Clinical Experience
 Immunotherapy for Malignant Brain Cancer: Overcoming Immune Suppression to Improve the Clinical Experience Derek Wainwright, PhD Assistant Professor Departments of Neurological Surgery, Microbiology-Immunology
Immunotherapy for Malignant Brain Cancer: Overcoming Immune Suppression to Improve the Clinical Experience Derek Wainwright, PhD Assistant Professor Departments of Neurological Surgery, Microbiology-Immunology
University of Zurich. Temozolomide and MGMT forever? Zurich Open Repository and Archive. Weller, M. Year: 2010
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
General Information, efficacy and safety data
 Horizon Scanning in Oncology Horizon Scanning in Oncology 23 rd Prioritization 2 nd quarter 2015 General Information, efficacy and safety data Eleen Rothschedl Anna Nachtnebel Priorisierung XXIII HSS Onkologie
Horizon Scanning in Oncology Horizon Scanning in Oncology 23 rd Prioritization 2 nd quarter 2015 General Information, efficacy and safety data Eleen Rothschedl Anna Nachtnebel Priorisierung XXIII HSS Onkologie
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
2015 EUROPEAN CANCER CONGRESS
 2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
TGFβR1 Kinase Inhibitor
 TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Prud homme GJ 1 ; Flavell RA, et al 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase 1b/2 Dose-Escalation
TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Prud homme GJ 1 ; Flavell RA, et al 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase 1b/2 Dose-Escalation
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
TGFβR1 Kinase Inhibitor
 TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Derived from Prud homme GJ 1 ; Flavell RA, et al. 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase
TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Derived from Prud homme GJ 1 ; Flavell RA, et al. 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Antiangiogenic drugs in unresectable glioblastoma. Dra. Carmen Balañá. /
 Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immuno-Oncology Clinical Trials Update: Therapeutic Anti-Cancer Vaccines Issue 7 April 2017
 Delivering a Competitive Intelligence Advantage Immuno-Oncology Clinical Trials Update: Therapeutic Anti-Cancer Vaccines Issue 7 April 2017 Immuno-Oncology CLINICAL TRIALS UPDATE The goal of this MONTHLY
Delivering a Competitive Intelligence Advantage Immuno-Oncology Clinical Trials Update: Therapeutic Anti-Cancer Vaccines Issue 7 April 2017 Immuno-Oncology CLINICAL TRIALS UPDATE The goal of this MONTHLY
Neuro-Oncology Program
 Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
Immunotherapy for the Treatment of Brain Metastases
 Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
Transforming science into medicine
 Transforming science into medicine 2 Forward-looking statements This presentation contains forward-looking statements. These statements include words like may, expects, believes, plans, scheduled, and
Transforming science into medicine 2 Forward-looking statements This presentation contains forward-looking statements. These statements include words like may, expects, believes, plans, scheduled, and
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Media Release. Basel, 07 December 2017
 Media Release Basel, 07 December 2017 Phase III IMpower150 study showed Tecentriq (atezolizumab) and Avastin (bevacizumab) plus chemotherapy reduced the risk of disease worsening or death by 38 percent
Media Release Basel, 07 December 2017 Phase III IMpower150 study showed Tecentriq (atezolizumab) and Avastin (bevacizumab) plus chemotherapy reduced the risk of disease worsening or death by 38 percent
Immuno-Oncology. Axel Hoos, MD, PhD Senior Vice President, Oncology R&D. February 24, 2016
 Immuno-Oncology Axel Hoos, MD, PhD Senior Vice President, Oncology R&D February 24, 216 GSK Pipeline Oncology R&D strategy Focusing on 3 areas fundamental to oncology Cancer Epigenetics Long-Term Survival
Immuno-Oncology Axel Hoos, MD, PhD Senior Vice President, Oncology R&D February 24, 216 GSK Pipeline Oncology R&D strategy Focusing on 3 areas fundamental to oncology Cancer Epigenetics Long-Term Survival
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates
 Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Ruolo emergente dell immunoterapia nello stadio III. Giulia Pasello Medical Oncology 2 Veneto Cancer Institute, Padua (Italy)
") Ruolo emergente dell immunoterapia nello stadio III Giulia Pasello Medical Oncology 2 Veneto Cancer Institute, Padua (Italy) Disclosures Advisory Boards / Honoraria / Speakers fee / Consultant for: MSD,
Ruolo emergente dell immunoterapia nello stadio III Giulia Pasello Medical Oncology 2 Veneto Cancer Institute, Padua (Italy) Disclosures Advisory Boards / Honoraria / Speakers fee / Consultant for: MSD,
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
HHS Public Access Author manuscript Immunotherapy. Author manuscript; available in PMC 2015 December 16.
 Overview of current immunotherapeutic strategies for glioma Anda-Alexandra Calinescu 1, Neha Kamran 1, Gregory Baker 1, Yohei Mineharu 2, Lowenstein Pedro Ricardo 1,3, and Castro Maria Graciela *,1,3 1
Overview of current immunotherapeutic strategies for glioma Anda-Alexandra Calinescu 1, Neha Kamran 1, Gregory Baker 1, Yohei Mineharu 2, Lowenstein Pedro Ricardo 1,3, and Castro Maria Graciela *,1,3 1
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
CHMP Type II variation assessment report
 26 January 2017 EMA/CHMP/59238/2017 Invented name: Avastin International non-proprietary name: bevacizumab Procedure No. EMEA/H/C/000582/II/0093 Marketing authorisation holder (MAH): Roche Registration
26 January 2017 EMA/CHMP/59238/2017 Invented name: Avastin International non-proprietary name: bevacizumab Procedure No. EMEA/H/C/000582/II/0093 Marketing authorisation holder (MAH): Roche Registration
Cancer Immunotherapy Survey
 CHAPTER 8: Cancer Immunotherapy Survey All (N=100) Please classify your organization. Academic lab or center Small biopharmaceutical company Top 20 Pharma Mid-size pharma Diagnostics company Other (please
CHAPTER 8: Cancer Immunotherapy Survey All (N=100) Please classify your organization. Academic lab or center Small biopharmaceutical company Top 20 Pharma Mid-size pharma Diagnostics company Other (please
A robust new approach. A rising trend
 A robust new approach Since its inception in the mid-0th century, chemotherapy has been the mainstay of cancer treatment and has become increasingly specific and effective. But with the increasing incidence
A robust new approach Since its inception in the mid-0th century, chemotherapy has been the mainstay of cancer treatment and has become increasingly specific and effective. But with the increasing incidence
Advances in Systemic Therapy Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016
 Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016") Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Douglas Jolly Executive VP R&D Tocagen Inc.
 REPLICATING RETROVIRUSES FOR MANIPULATION OF THE TUMOR IMMUNE ECOSYSTEM: PRECLINICAL AND CLINICAL OUTCOMES. Douglas Jolly Executive VP R&D Tocagen Inc. PEGS 2018 IT Track Boston May 1 2018 Outline Phase
REPLICATING RETROVIRUSES FOR MANIPULATION OF THE TUMOR IMMUNE ECOSYSTEM: PRECLINICAL AND CLINICAL OUTCOMES. Douglas Jolly Executive VP R&D Tocagen Inc. PEGS 2018 IT Track Boston May 1 2018 Outline Phase
DCVax Novel Personalized Immune Therapies For Solid Tumor Cancers. SMi 4 th Annual Cancer Vaccines Conference September 16, 2015
 DCVax Novel Personalized Immune Therapies For Solid Tumor Cancers SMi 4 th Annual Cancer Vaccines Conference September 16, 2015 Disclaimer Certain statements made in this presentation are forward-looking
DCVax Novel Personalized Immune Therapies For Solid Tumor Cancers SMi 4 th Annual Cancer Vaccines Conference September 16, 2015 Disclaimer Certain statements made in this presentation are forward-looking
Marizomib (MRZ): Brain Penetrant Irreversible Pan-Proteasome Inhibitor
: Brain Penetrant Irreversible Pan-Proteasome Inhibitor") MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Emerging Targets in Immunotherapy
 Emerging Targets in Immunotherapy So Jin Shin, M.D. Department of Obstetrics and Gynecology, Keimyung University, School of Medicine, Daegu, Korea no-0ncology Todays is.. ancer Immunotherapy? nd immunotherapy
Emerging Targets in Immunotherapy So Jin Shin, M.D. Department of Obstetrics and Gynecology, Keimyung University, School of Medicine, Daegu, Korea no-0ncology Todays is.. ancer Immunotherapy? nd immunotherapy
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
GSK Oncology. Axel Hoos, MD, PhD Senior Vice President, Oncology R&D. March 8, 2017
 GSK Oncology Axel Hoos, MD, PhD Senior Vice President, Oncology R&D March 8, 217 GSK pipeline Oncology R&D Strategy Maximizing survival through transformational medicines and combinations Cancer Epigenetics
GSK Oncology Axel Hoos, MD, PhD Senior Vice President, Oncology R&D March 8, 217 GSK pipeline Oncology R&D Strategy Maximizing survival through transformational medicines and combinations Cancer Epigenetics
2011 Oncology Highlights News from ASCO 2011:
 2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
University of Colorado Cancer Center Brain Disease Site Schema
 GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
2018 KSMO Immune Oncology Forum. Immune checkpoint inhibitors in hematologic. malignancies: evidences and perspectives 서울아산병원종양내과 홍정용
 2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
Cancer immunology > what should happen (immunosurveillance)
") 11 th Perspectives in Lung Cancer Vaccines: any expectations? J Vansteenkiste Dept Pulmonology q Cancer immunology, immunotherapy, vaccination q Agents in phase III development o MAGE-A3 A3 ASCI o MUC1
11 th Perspectives in Lung Cancer Vaccines: any expectations? J Vansteenkiste Dept Pulmonology q Cancer immunology, immunotherapy, vaccination q Agents in phase III development o MAGE-A3 A3 ASCI o MUC1
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care
 Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
MOLOGEN AG. Pioneering Immune Therapy. Annual Results Analysts Call March 25, 2014
 Pioneering Immune Therapy Annual Results 2013 Analysts Call March 25, 2014 Disclaimer Certain statements in this presentation contain formulations or terms referring to the future or future developments,
Pioneering Immune Therapy Annual Results 2013 Analysts Call March 25, 2014 Disclaimer Certain statements in this presentation contain formulations or terms referring to the future or future developments,
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
GLIOBLASTOMA MULTIFORME. agivingsmarterguideto acceleratingresearchprogress
 GLIOBLASTOMA MULTIFORME agivingsmarterguideto acceleratingresearchprogress CONTENTS Executive Summary... 4 Disease Biology... 5 Molecular Pathways and Targets... 5 Prognostic Indicators... 6 DNA Methylations
GLIOBLASTOMA MULTIFORME agivingsmarterguideto acceleratingresearchprogress CONTENTS Executive Summary... 4 Disease Biology... 5 Molecular Pathways and Targets... 5 Prognostic Indicators... 6 DNA Methylations
Dendritic Cell Based Cancer Vaccine Development
 Dendritic Cell Based Cancer Vaccine Development November 10, 2005 CVCWG Meeting Rob Hershberg, MD, PhD Chief Medical Officer 1 Meeting the challenges of developing cancer vaccines-- APC8015 (Provenge TM
Dendritic Cell Based Cancer Vaccine Development November 10, 2005 CVCWG Meeting Rob Hershberg, MD, PhD Chief Medical Officer 1 Meeting the challenges of developing cancer vaccines-- APC8015 (Provenge TM
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Immunotherapy for Genitourinary Cancers
 Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Primary Endpoint The primary endpoint is overall survival, measured as the time in weeks from randomization to date of death due to any cause.
 CASE STUDY Randomized, Double-Blind, Phase III Trial of NES-822 plus AMO-1002 vs. AMO-1002 alone as first-line therapy in patients with advanced pancreatic cancer This is a multicenter, randomized Phase
CASE STUDY Randomized, Double-Blind, Phase III Trial of NES-822 plus AMO-1002 vs. AMO-1002 alone as first-line therapy in patients with advanced pancreatic cancer This is a multicenter, randomized Phase
Radiation Therapy and Immunotherapy: New Frontiers
 Radiation Therapy and Immunotherapy: New Frontiers Nevada Oncology Society Fall Meeting November 16 th, 2017 Anshu K. Jain, MD Radiation Oncologist, Ashland Bellefonte Cancer Center Assistant Clinical
Radiation Therapy and Immunotherapy: New Frontiers Nevada Oncology Society Fall Meeting November 16 th, 2017 Anshu K. Jain, MD Radiation Oncologist, Ashland Bellefonte Cancer Center Assistant Clinical
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Brain Schema March 2018
 Breast Cancer w/brain Mets 14 2283 / Lilly Abemaciclib PO Breast Ca or Melanoma mets allowed Leptomeningeal mets excluded Want brain met tissue Melanoma w/brain Mets 14 2209 / Bristol Myers Squibb Nivolumab
Breast Cancer w/brain Mets 14 2283 / Lilly Abemaciclib PO Breast Ca or Melanoma mets allowed Leptomeningeal mets excluded Want brain met tissue Melanoma w/brain Mets 14 2209 / Bristol Myers Squibb Nivolumab
Appendices. Appendix A Search terms
 Appendices Appendix A Search terms Database Search terms Medline 1. Ipilimumab; 2. MDX-010; 3. MDX-101; 4. Yervoy; 5. BMS-734016; 6. Nivolumab; 7. ONO-4538; 8. BMS-936558; 9. MDX-1106; 10. Opdivo; 11.
Appendices Appendix A Search terms Database Search terms Medline 1. Ipilimumab; 2. MDX-010; 3. MDX-101; 4. Yervoy; 5. BMS-734016; 6. Nivolumab; 7. ONO-4538; 8. BMS-936558; 9. MDX-1106; 10. Opdivo; 11.
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases
 Immunotherapy for the Treatment of Brain Metastases") Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM
 Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre Madrid GEINO 1402. Phase Ib, open-label,
Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre Madrid GEINO 1402. Phase Ib, open-label,
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and