EPIDEMIOLOGY. Long established risk factors for CCA: hepatobiliaryflukes, PSC, biliary tract cysts, epatolithiasis.
|
|
|
- Marion Brown
- 5 years ago
- Views:
Transcription


1
2 EPIDEMIOLOGY Intrahepatic cholangiocarcinoma(icc) is the second most common (15%) primary liver cancer after hepatocellular carcinoma (HCC), with a rate of about 2.1/100,000 people per year in western countries. Long established risk factors for CCA: hepatobiliaryflukes, PSC, biliary tract cysts, epatolithiasis. More recently recognized risk factors for iccaare similar to those known for HCC: cirrhosis, chronic hepatitis B and C and alcohol. The prevalence of these risk factors is much lower for iccathan for HCC. Bridgewater J et al J. Hepatol. 2014;60, Yang JD et al. Am. J. Gastroenterol. 2012;107, Khan SA et al. Lancet. 2005;366: Palmer WCet al. J Hepatol. 2012;57:69 76
3 CLASSIFICATION The classificationof the diseaseisbasedon the anatomiclocation: intra and extrahepatic cholangiocarcinoma. Intrahepaticcholangiocarcinoma(ICC) constitutesno more than5 15% of allcases. The prognosisof the diseaseisdismal and surgicalresectionisthe onlycurative treatment option with five-year survival rates varying from 14% to 40% (unspecific clinical symptoms and central localization). Anderson CD et al. Oncologist. 004;9:43-57 Poultsides GA et al. Surg Clin North Am 2010;90: Tan JCet al. Ann Surg Oncol 2008;15:600-8
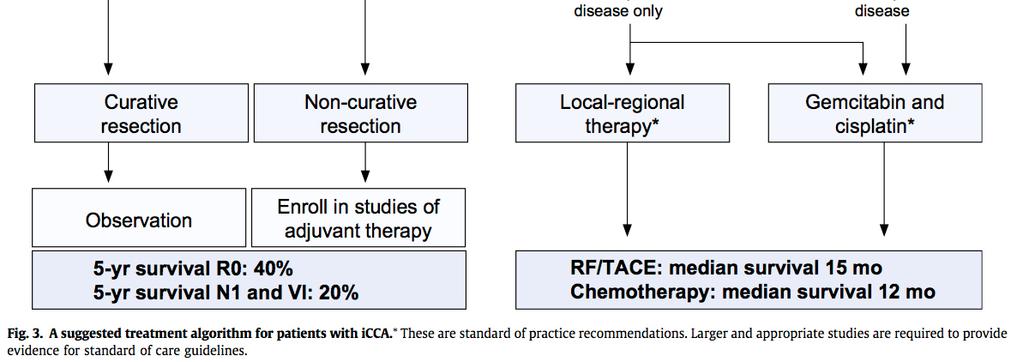
4 TREATMENT Surgical resection is the mainstay for treatment of icca. Unfortunately, only about 20 40% of ICCs are diagnosed at a stage which meets the criteria for curative resection. Moreover, curative-intent surgery is mainly limited by the high recurrence rate of this cancer. If untreated, unresectableiccs have a median survival of less than 8 months which can be increased to approximately 12 months with systemic chemotherapy (gemcitabine and cisplatin). Tan JC et al. Ann Surg Oncol. 2008;15: Bridgewater J et al J. Hepatol. 2014;60,
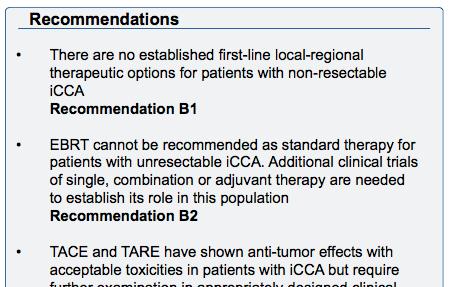
5 LR-THERAPIES Over the last decade, the use of image-guided loco-regional therapies (LRT) as a palliative option in unresectable ICC has become increasingly accepted among multidisciplinary teams that manage this subset of liver cancer patients. Intra-arterial therapies (IAT) are the most commonly used approaches for the treatment of ICC. Embolic materials and/or chemotherapeutic agents or internal radiation can be delivered directly to the tumor with high doses within the tumor tissue while significantly reducing its systemic distribution. Most commonly used IAT: HAI/TACI, C-TACE, DEB-TACE and TARE. Burger I et al. J Vasc Interv Radiol 2005;16: Dodson RM et al. J Am Coll Surg. 2013;217:
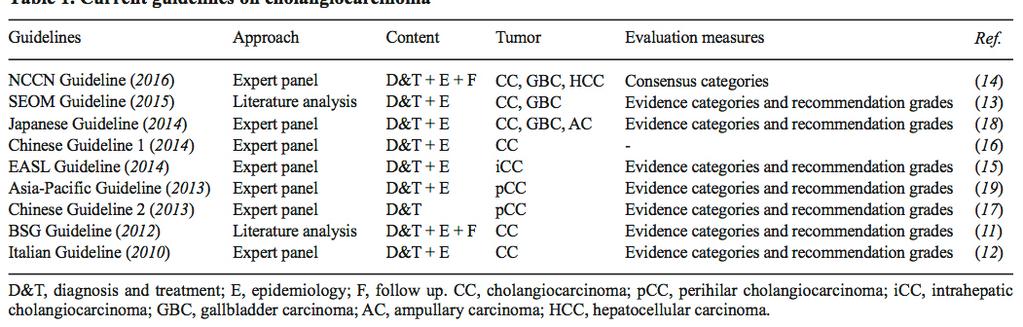
6 GUIDELINES
7 GUIDELINES
8 GUIDELINES
9 GUIDELINES
10 HAI/TACI Hepatic arterial infusion chemotherapy, through an implanted port system (HAI), represents a loco-regional approach that administers a continuous infusion of drug directly into the liver. The greatest experience with HAI has been in patients with colorectal liver metastases. Several studies have demonstrated the efficacy of HAI with significantly higher response rates, less toxicity and a potential survival benefit compared to systemic chemotherapy alone. By contrast, experience with HAI in primary liver cancers is much more limited. Sullivan RD et al. N Engl J Med :321 7 House MG et al. Annals of surgery. 2011; 254(6): Yamashita T et al. Oncology. 2011; 81(5 6):281 90

11 HAI/TACI HAI 25 patients via a percutaneous were enrolled implanted from may port 2004 system to november (femoral or subclavian access). 11 Istlogically patientsconfirmed with unresectable ICC Not responder ICC were treated to other with cht.infusion of fluorouracil combined with a variety of other ECOG agents 2 or less. (doxorubicin, mitomycin C, cisplastin). Mean Median survival survival of340d. 26 months. Tanaka The disease et al control reportedrate theand most MST favorable were acceptable, survival outcomes but, considering in the literature that thefor implanted patients with unresectable ICC, catheter-port despite a system patient was cohort required that included for HAI as 63% a painful (7/11) with procedure, extrahepatic it cannot disease. be claimed that this protocol has an advantage over systemic treatment.
 and 93 (HAI + SYS). Patients with ICC had a higher response rate (53.8%) compared with those with HCC (25%).")
.")
12 HAI/TACI (HAI) with1/2000 floxuridine (FUDR) and Between and 8/2012, 525 dexamethasone patients with ICC(dex). were evaluated. Thirty-four unresectable patients (26 ICCtoand HCC) from 2003 to with unresecable disease confined the 8liver were enrolled: (SYS) and 93 (HAI + SYS). Patients with ICC had a higher response rate (53.8%) compared with those with HCC (25%). HAI: FUDR (+ mitomycin or gemcitabine). One patient withinicc to undergo resection. Overall survival theresponded combined sufficiently group was longer compared to patients who received SYS alone (30.8 The median survival was 29.5 months. months vs 18.4 months). Eight patients who initially presented with unresectable tumors responded enough to undergo complete resection and had a median overall survival of 37 months (range= months).
13 C-TACE Conventional TACE is the most commonly used intra-arterial modality in unresectable ICC. During ctace, an emulsion of chemotherapeutics and an oil-based contrast agent (Ethiodol or Lipiodol) is injected into the tumor-supplying branches, followed by the administration of an embolizing agent. The most commonly used drug combination in the US and Europe consists of doxorubicin, cisplatin and mitomycin-c, but gemcitabine has also been used. TACE is tolerated well by the majority of patients without major adverse events. Most studies that investigate clinical outcomes in ICC treated with ctace are retrospective and do not use a standardized procedure protocol. However, the available literature suggests potential survival benefits in patients with unresectable lesions. Yamada Ret al. Osaka City Med J. 1980;26:81-96 Kiefer MV et al. Cancer. 2011;117: Cohen MJ et al World J Gastroenterol. 2013;19: Hyder O et al. Ann Surg Oncol. 2013;20:
 patients or were Embosphere diagnosedparticles(biosphere with")
![inoperable ICC Medical, with Rockland, a mean tumor MA). diameter of 10.8±4.6 cm and multifocal Liverfunctionwasgenerallypreserved(15of17Child-PughclassA),aswellas(PS)(14of17[ECOG]PS<2).](/docs-images/84/90817518/images/14-3.jpg "disease in seven patients Previous Patients underwent treatmentsa were median reported of two TACE for seven sessions. patients including liver resection (n=1, 6.7%), RFA (n=2, 13.")
14 C-TACE A17patientstreatedbetween1995and2004. retrospective analysis included 15 TreatmentwithcTACEusingmitomycin-c(10mg)for59treatmentsessionsoveraperiodofsixyears. Conventional TACE regimen consisting of cisplatin, doxorubicin, andmitomycin-c, followed by embolization with polyvinyl The alcohol(pva) patients or were Embosphere diagnosedparticles(biosphere with inoperable ICC Medical, with Rockland, a mean tumor MA). diameter of 10.8±4.6 cm and multifocal Liverfunctionwasgenerallypreserved(15of17Child-PughclassA),aswellas(PS)(14of17[ECOG]PS<2). disease in seven patients Previous Patients underwent treatmentsa were median reported of two TACE for seven sessions. patients including liver resection (n=1, 6.7%), RFA (n=2, 13.3%) Medianand overall systemic survival chemotherapy was 23 months. (n=4, 26.7%). One patient (6.7%) had liver cirrhosis, however, Child PughscorewasAin14(93.3%)andBinonepatient(6.7%) Two patients were deemed to have resectable disease following TACE. MedianOSof16.3months.
 had regimens received consisting prior chemotherapy, of gemcitabine and combined 7 patients with (11%) orhad followed prior liver by resection")
15 C-TACE Retrospectiveanalysis included 62 patients Treatedwith conventional TACE (cisplatin, doxorubicin, and mitomycin-c A retrospective infusion trialfollowed includedby a total PVA embolization) of 42 patients Eighteen ctace patients with different (29%) had regimens received consisting prior chemotherapy, of gemcitabine and combined 7 patients with (11%) orhad followed prior liver by resection cisplatin and Extrahepatic oxaliplatin disease was present in 19 patients (31%) One ThemedianOSfortheentirecohortwas9.1months patient had ECOG PS of 2; remainder of cohort had ECOG PS 0 to 1 Patients Patients underwent with SD a showed mean of a2.7 median TACE OS sessions of 13.1 months compared to 6.9 months for patients with PD Median (P=0.017) survival was 20 months from time of diagnosis, and 15 months from initial chemoembolization. Patients having received prior systemic chemotherapy survived longer than those who did not (28 months versus 16 months

 of the Hypervascular supportive care tumors group. were present in 62 patients (54%). Median survival OS in the was TACE 13 months group(12.")
16 C-TACE Prospective Comparedtrials ctace included (n=72) 115 withpatients symptomatic with unresectableicc supportive therapy treated (n=83) with intace the palliative from 1999 treatment to of 155 TACE patients regimens withvaried, unresectable mitomycin-c, ICC. gemcitabine, both mitomycin-c and gemcitabine and cisplatin. Patients Extrahepatic with Child-Pugh disease was class found C liver indisease 39 patients or extrahepatic (54%) of the disease TACE cohort were excluded. and in 50 patients (60%) of the Hypervascular supportive care tumors group. were present in 62 patients (54%). Median survival OS in the was TACE 13 months group(12.2 from initial months) chemoembolization. compared to the supportive treatment group(3.3 months). No significant survival difference was observed between TACE regimens. Tumor vascularity was identified as a positive prognostic indicator, among other factors.
17 DEB-TACE Drug-eluting bead (DEB) therapy consists of highly absorbent microspheres mixed with high doses of chemotherapy, prior to hepatic arterial delivery similar to conventional TACE procedures. Multiple DEB platforms are available that have been used to deliver both doxorubicin and oxaliplatin and irinotecan chemotherapy regimens. Only a few series to date have investigated DEB-TACE therapy in the treatment of ICC. Lewis AL et al. J Vasc Interv Radiol 006;17(8): Hong K et al. Clin Cancer Res 2006;12: Varela M et al. J Hepatol 2007;46(3):
 All microspheres patients had (HepaSpheres, received prior Biosphere systemic chemotherapy Medical, France) and/or combined hepatic with resection.")

18 DEB-TACE 11 Small patients retrospective who underwent comparative TACE study with DC including Beads 9 (Biocompatibles patients treatedwith UK, Surrey, oxaliplatin-preloaded UK) loaded with doxorubicin. (50 mg) All microspheres patients had (HepaSpheres, received prior Biosphere systemic chemotherapy Medical, France) and/or combined hepatic with resection. systemic chemotherapy (oxaliplatin A and median gemcitabine). of three treatment sessions was performed. Median These patients survival were was compared 13 months to following a retrospectively the first DEB-TACE acquired session. group of eleven patients, who were treated with chemotherapy (FOLFOX) only. With one exception, Child Pugh class B and C as well as extrahepaticdisease were exclusion factors in both groups. The median OS after DEB-TACE and chemotherapy was 30 months compared to 12.7 months for chemotherapy alone.
.")
 consisted of doxorubicin (150 Compared to ctace chemotherapy, DEBIRI revealedwith prolonged OS (5.7 vs.")
19 DEB-TACE DEBIRI (irinotecan 200 mg; DC/LC Beads, Biocompatibles/BTG, UK; n=26). A prospectively designed multi-institutional review included 24 patients with unresectable ICC total of 42 ctace (mitomycin-c DEB-TACE sessions. 15 mg; gelfoam; n=10). Systemic chemotherapy (gemcitabine and oxaliplatin; n=31). The DEB-TACE regimen using DC/LC Beads (Biocompatibles, Farnham, UK) consisted of doxorubicin (150 Compared to ctace chemotherapy, DEBIRI revealedwith prolonged OS (5.7 vs. vs. mg) and irinotecan (75and mg;systemic range, mg) and was combined systemicmedian chemotherapy in 11 eight 11.7 months. patients (33.3%). The median OS was 17.5 months Three patients (12.5%) were converted to surgical resection postprocedurally.
20 Y-90 Y90-RE is a form of selective internal radiation therapy (SIRT). The concept consists of the intra-arterial delivery of small embolic particles (20 40 μm) containing the radionucleotide Y90, that emits β-radiation. Y90-RE allows maximization of treatment efficacy while sparing the healthy liver parenchyma from radiation-induced injury Currently, two major devices are available: glass-based microspheres (TheraSphere, MDS, Nordion, Ottawa, Ontario, Canada) and resin-based microspheres(sir-sphere, Sirtex, New South Wales, Australia). Given the small size and the severe radiation potency of Y90-particles, complications may derive from unintended extrahepatic deployment of the payload. All patients must be subjected to shunt evaluation using technetium-99 macroagglutinated albumin(tc-maa), SPECT and angiographic imaging. Veeze-Kuijpers B et al. Int J Radiat Oncol Biol Phys 1990;18:63-7 Hoffmann RT et al. Cardiovasc Intervent Radiol 2012;35: Mouli S et al. J Vasc Interv Radiol 2013;24:
, according to the WHO Criteria, a partialresponse(pr) in 6 Patients patients(27%), were assessed stable at disease 1 month (SD) and in 15 then patients")
 and a PR in 17 lesions (77%). The Survival median was OS significantly was 14.")
21 Y patients with underwent histologically resin-based proven 90 ICC. Y radioembolizationfor unresectableicc between January 2004 and They May showed (follow-up available for 22 patients), according to the WHO Criteria, a partialresponse(pr) in 6 Patients patients(27%), were assessed stable at disease 1 month (SD) and in 15 then patients 3-month (68%) intervals and disease after progression treatment. in one patient (5%), and according A median OS to the of 9.3 EASL months. Criteria, a complete response in two lesions (9%) and a PR in 17 lesions (77%). The Survival median was OS significantly was 14.9 months correlated from to the two time factors, of the peripheral first treatment. tumor type (vsinfiltrative; p = 0.004) and an Median ECOG performance survival was status significantly of 0 (vs1 prolonged and 2; p in < 0.001). patients with ECOG performance status 0 than in those with status 1 and 2 (31.8 vs6.1 and 1 month, respectively, p < ). The median survival for patients with and without portal vein thrombosis was 5.7 and 31.8 months, respectively The median survival of patients with peripheral versus infiltrative tumors was 31.8 and 5.7 months, respectively.

, 0 versus infiltrative ECOG 1 or (6.1 2 (median vs15.")
22 Y-90 In The a series current of study 33 patients. expands upon the prior report if ibrahim. A Including median forty-six OS of 22 patients months with from unresectableicc the time of the first who treatment. were treated with Y90 radioembolizationat a single The institution median from time July to progression 2003 May(TTP) was 9.8 months. Survival and varied TTP according were significantly to the presence prolonged of multifocal in patients (5.7 with vs14.6 ECOG months), 0 versus infiltrative ECOG 1 or (6.1 2 (median vs15.6 OS: months) 29.4, or 10 bilobar and 5.1 disease months, (10.9 respectively; vs 11.7 months). TTP: 17.5, 6.9 and 2.4 months, respectively), in those with a tumor burden Five 25% patients (OS: 26.7 (11%) vs6 were months; downstaged TTP: 17.5 to vs2.3 resection months) after or treatment. in those with tumor response (PR or SD vs progressive disease; OS: 35.5, 17.7 vs 5.7 months, respectively; TTP: 31.9, 9.8 vs 2.5 months, respectively).

23 Y-90 Comprehensive Showed that SIRT combined chemotherapy promising of strategy as first-line for90yreview of thewith current studies andseems clinicala outcomes unresectable ICCstreatment treated with unresectable ICC TARE 24 patientswith treated with data SIRT control group treated with CIS-GEM 12 studies relevant Median progression-free survival was 15.5survival months after TARE of 10.3 months Longer progression-free survival when of chemotherapy was given all concomitantly than when However, the authors pointed outwas theobserved heterogeneity the study populations: the studies reported chemotherapy was given before SIRT, with median 20.0 versus 8.8 monthssystemic (p = 0.001) survival since the initiation of 90Y-TARE butrespective in some cases the of patients had undergone chemotherapy prior to or during the treatment

24 Y patients between The overall median survival was 17.9 months. Longer survival in naive patients as compared with patients in whom TARE was preceded by other treatments.
25 ?


26 The overall median survival across the four strategies was 14.5 months confirming a beneficial effect. The results, however, must be interpreted cautiously due to the potential selection bias across the treatment groups No standardized chemotherapeutic drug or schedule HAI involves the implantation of a chemoinfusion pump or port which may predispose patients to a greater set of risks when compared with other intra-arterial strategies

27 GUIDELINES
28 Conclusion ICC still represents a complex and heterogeneous scenario in which no evidencebased algorithms of care exist. A similar to HCC diagnostic and therapeutic algorithm is recommended for ICC. Despite the lack of randomized controlled trials, current literature indicates evidence in support of the use of LRT for patients with unresectableicc. In particular, IAT have proven feasible, safe and effective in inducing local tumor response. Moreover current clinical evidence suggests survival benefits for IAT over systemic chemotherapy and the ability of downstagingtumors until eligible to resection. A multidisciplinary team of experts is necessary to ensure the best patient selection and to obtain optimal results; this is possible only in tertiary level centers having certified expertise, after thorough training of the staff.
29
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Transarterial Therapies for the Treatment of Intrahepatic Cholangiocarcinoma
 21 Transarterial Therapies for the Treatment of Intrahepatic Cholangiocarcinoma Joseph J. Zechlinski, MD 1 William S. Rilling, MD, FSIR 1 1 Division of Interventional Radiology, Medical College of Wisconsin,
21 Transarterial Therapies for the Treatment of Intrahepatic Cholangiocarcinoma Joseph J. Zechlinski, MD 1 William S. Rilling, MD, FSIR 1 1 Division of Interventional Radiology, Medical College of Wisconsin,
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days
 94% of radiation delivered within 11 days") 100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer
 Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
treatment options for primary liver malignancies and metastatic disease
 State of the art treatment options for primary liver malignancies and metastatic disease Peter Huppert Prof. of Radiology and Neuroradiology Klinikum Darmstadt Certified Vascular and Oncologic Center Disclosure
State of the art treatment options for primary liver malignancies and metastatic disease Peter Huppert Prof. of Radiology and Neuroradiology Klinikum Darmstadt Certified Vascular and Oncologic Center Disclosure
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES. Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí
 INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Guidelines for SIRT in HCC An Evolution
 Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE METASTASES
 LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
Helping you access curative therapies for liver cancer patients
 Metastatic colorectal cancer (mcrc) Helping you access curative therapies for liver cancer patients Biocompatibles Excellence in Interventional Oncology Biocompatibles UK Ltd is a BTG International group
Metastatic colorectal cancer (mcrc) Helping you access curative therapies for liver cancer patients Biocompatibles Excellence in Interventional Oncology Biocompatibles UK Ltd is a BTG International group
Radioembolization for Primary and Metastatic Tumors of the Liver
 Page: 1 of 28 Last Review Status/Date: September 2015 Description Radioembolization (RE), also referred to as selective internal radiotherapy (SIRT), is the intra-arterial delivery of small beads (microspheres)
Page: 1 of 28 Last Review Status/Date: September 2015 Description Radioembolization (RE), also referred to as selective internal radiotherapy (SIRT), is the intra-arterial delivery of small beads (microspheres)
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Transcatheter Arterial Chemoembolization to Treat Primary or Metastatic Liver Malignancies
 Transcatheter Arterial Chemoembolization to Treat Primary or Metastatic Liver Malignancies Policy Number: 8.01.11 Last Review: 6/2018 Origination: 8/2005 Next Review: 6/2019 Policy Blue Cross and Blue
Transcatheter Arterial Chemoembolization to Treat Primary or Metastatic Liver Malignancies Policy Number: 8.01.11 Last Review: 6/2018 Origination: 8/2005 Next Review: 6/2019 Policy Blue Cross and Blue
DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data
![DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data](/thumbs/78/77499894.jpg "DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data") DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data Professor Thomas J Vogl Goethe University Hospital Frankfurt-am-Main,
DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data Professor Thomas J Vogl Goethe University Hospital Frankfurt-am-Main,
MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC
 Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
in Hepatocellular Carcinoma
 in Hepatocellular Carcinoma The following summarises the key data supporting the use of SIR-Spheres Y-90 resin microspheres in the treatment of primary liver cancer due to hepatocellular carcinoma (HCC):
in Hepatocellular Carcinoma The following summarises the key data supporting the use of SIR-Spheres Y-90 resin microspheres in the treatment of primary liver cancer due to hepatocellular carcinoma (HCC):
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
Transcatheter Arterial Chemoembolization (TACE) to Treat Primary or Metastatic Liver Malignancies
 to Treat Primary or Metastatic Liver Malignancies") Transcatheter Arterial Chemoembolization (TACE) to Treat Primary or Metastatic Liver Malignancies Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its
Transcatheter Arterial Chemoembolization (TACE) to Treat Primary or Metastatic Liver Malignancies Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its
Description. Section: Therapy Effective Date: July 15, 2014 Subsection: Therapy Original Policy Date: June 7, 2012 Subject: Page: 1 of 23
 Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
Transcatheter hepatic arterial chemoembolization may be considered medically necessary to
 Original Issue Date (Created): July 1, 2002 Most Recent Review Date (Revised): September 24, 2013 Effective Date: November 1, 2013 I. POLICY Hepatocellular carcinoma Transcatheter hepatic arterial chemoembolization
Original Issue Date (Created): July 1, 2002 Most Recent Review Date (Revised): September 24, 2013 Effective Date: November 1, 2013 I. POLICY Hepatocellular carcinoma Transcatheter hepatic arterial chemoembolization
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
SIRT for Intermediate and Advanced HCC
 Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
PRIOR AUTHORIZATION Prior authorization is required for BlueCHiP for Medicare members and recommended for Commercial products.
 Medical Coverage Policy Radioembolization for Primary and Metastatic Tumors of the Liver EFFECTIVE DATE: 10 06 2009 POLICY LAST UPDATED: 08 02 2016 OVERVIEW Radioembolization (RE), referred to as selective
Medical Coverage Policy Radioembolization for Primary and Metastatic Tumors of the Liver EFFECTIVE DATE: 10 06 2009 POLICY LAST UPDATED: 08 02 2016 OVERVIEW Radioembolization (RE), referred to as selective
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros)
") HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros) Yi-Hsiang Huang, MD, Ph.D. Professor, Division of Gastroenterology & Hepatology,
HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros) Yi-Hsiang Huang, MD, Ph.D. Professor, Division of Gastroenterology & Hepatology,
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE. clic per modificare lo stile del sottotitolo dello schem
 XII Congresso Nazionale AIMN 2015 16-19 Aprile 2015 Rimini RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE clic per modificare lo stile del sottotitolo dello schem Marco Maccauro Nuclear Medicine
XII Congresso Nazionale AIMN 2015 16-19 Aprile 2015 Rimini RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE clic per modificare lo stile del sottotitolo dello schem Marco Maccauro Nuclear Medicine
Hamad Alsuhaibani,MD KING FAISAL SPECIALIST HOSPITAL &RESEARCH CENTRE.
 Hamad Alsuhaibani,MD KING FAISAL SPECIALIST HOSPITAL &RESEARCH CENTRE. YTTRIUM-90( 90 Y) TRANSARTERIAL HEPATIC RADIOEMBOLIZATION FOR HEPATOCELLULAR CARCINOMA EFFICACY AND SAFETY OF YTTRIUM-90 RADIO- EMBOLIZATION
Hamad Alsuhaibani,MD KING FAISAL SPECIALIST HOSPITAL &RESEARCH CENTRE. YTTRIUM-90( 90 Y) TRANSARTERIAL HEPATIC RADIOEMBOLIZATION FOR HEPATOCELLULAR CARCINOMA EFFICACY AND SAFETY OF YTTRIUM-90 RADIO- EMBOLIZATION
Hepatocellular carcinoma: Intra-arterial treatments
 Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization
 Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Transcatheter Arterial Chemoembolization (TACE) to Treat Primary or Metastatic Liver Malignancies. Original Policy Date
 to Treat Primary or Metastatic Liver Malignancies. Original Policy Date") MP 8.01.09 Transcatheter Arterial Chemoembolization (TACE) to Treat Primary or Metastatic Liver Malignancies Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date
MP 8.01.09 Transcatheter Arterial Chemoembolization (TACE) to Treat Primary or Metastatic Liver Malignancies Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for primary liver cancer Selective internal
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for primary liver cancer Selective internal
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER
 SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
NCCN Guidelines for Hepatobiliary Cancers V Web teleconference on 10/24/17
 Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Long-term follow-up after conventional transarterial chemoembolization (c-tace) with mitomycin for hepatocellular carcinoma (HCC)
 with mitomycin for hepatocellular carcinoma (HCC)") Original Article Long-term follow-up after conventional transarterial chemoembolization (c-tace) with mitomycin for hepatocellular carcinoma (HCC) Ricardo Yamada, Beatriz Bassaco, Stephen Bracewell, Kirkpatrick
Original Article Long-term follow-up after conventional transarterial chemoembolization (c-tace) with mitomycin for hepatocellular carcinoma (HCC) Ricardo Yamada, Beatriz Bassaco, Stephen Bracewell, Kirkpatrick
COMPARING Y90 DEVICES
 COMPARING Y90 DEVICES William S Rilling MD, FSIR Professor of Radiology and Surgery Director, Vascular and Interventional Radiology Medical College of Wisconsin DISCLOSURES Research support : Siemens,
COMPARING Y90 DEVICES William S Rilling MD, FSIR Professor of Radiology and Surgery Director, Vascular and Interventional Radiology Medical College of Wisconsin DISCLOSURES Research support : Siemens,
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?
 of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?") Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
HCC RADIOLOGIC DIAGNOSIS
 UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Portal Vein Invasion and the Role of Liver Directed Therapy. Matthew S Johnson MD FSIR Indiana University May 6, 2016
 Portal Vein Invasion and the Role of Liver Directed Therapy Matthew S Johnson MD FSIR Indiana University May 6, 2016 Matthew Johnson, M.D., FSIR Stock: Endoshape Consultant/Advisory Board: Bayer, BTG,
Portal Vein Invasion and the Role of Liver Directed Therapy Matthew S Johnson MD FSIR Indiana University May 6, 2016 Matthew Johnson, M.D., FSIR Stock: Endoshape Consultant/Advisory Board: Bayer, BTG,
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases
 Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
Reference No: Author(s) Approval date: 12/05/16. Committee. June Operational Date: Review:
 Approval date: 12/05/16. Committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Biliary Tract Cancer (BTC) Dr Colin Purcell, Consultant Medical Oncologist on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Biliary Tract Cancer (BTC) Dr Colin Purcell, Consultant Medical Oncologist on behalf of the GI Oncologists Group, Cancer
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
DEB-TACE vs Conventional TACE in Intermediate HCC: Best Candidates for DEB-TACE?
 DEB-TACE vs Conventional TACE in Intermediate HCC: Best Candidates for DEB-TACE? Ho Jong Chun, MD., PhD Seoul St. Mary s Hospital, The Catholic University of Korea Why Drug-eluting Beads? Clear Rationale
DEB-TACE vs Conventional TACE in Intermediate HCC: Best Candidates for DEB-TACE? Ho Jong Chun, MD., PhD Seoul St. Mary s Hospital, The Catholic University of Korea Why Drug-eluting Beads? Clear Rationale
CHEMOEMBOLISATION USING IODIZED OIL(LIPIODOL ) BASED TECHNIQUES
 BASED TECHNIQUES") CHEMOEMBOLISATION USING IODIZED OIL(LIPIODOL ) BASED TECHNIQUES Peter Huppert Department of Radiology, Neuroradiology and Nuclear Medicine Klinikum Darmstadt ATH Universities of Frankfurt and Heidelberg/Mannhein
CHEMOEMBOLISATION USING IODIZED OIL(LIPIODOL ) BASED TECHNIQUES Peter Huppert Department of Radiology, Neuroradiology and Nuclear Medicine Klinikum Darmstadt ATH Universities of Frankfurt and Heidelberg/Mannhein
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
SIR-Spheres: Des essais cliniques à la pratique courante
 SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
SIRTEX Lunch Symposium, Cebu, 23 Nov Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong
 SIRTEX Lunch Symposium, Cebu, 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong I will not talk on Mechanism of SIRT Data on efficacy of SIRT Epidemiology
SIRTEX Lunch Symposium, Cebu, 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong I will not talk on Mechanism of SIRT Data on efficacy of SIRT Epidemiology
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. Valle J et al. N Engl J Med 2010;362(14):
:") Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Intra-arterial Therapy in Management of HCC: ctace, DEB-TACE, and Y90 Radioembolization
 Intra-arterial Therapy in Management of HCC: ctace, DEB-TACE, and Y90 Radioembolization Department of Radiology, National Cancer Center In Joon Lee Contents Conventional TACE Role of TACE in management
Intra-arterial Therapy in Management of HCC: ctace, DEB-TACE, and Y90 Radioembolization Department of Radiology, National Cancer Center In Joon Lee Contents Conventional TACE Role of TACE in management
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA. Shawn Pelletier, MD
 TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for unresectable primary intrahepatic Intrahepatic
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for unresectable primary intrahepatic Intrahepatic
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
SIRT Dosimetry: Sometimes Less Is More
 SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
Transcatheter embolization therapy in liver cancer: an update of clinical evidences
 Review Article Transcatheter embolization therapy in liver cancer: an update of clinical evidences Yì-Xiáng J. Wáng 1, Thierry De Baere 2, Jean-Marc Idée 3, Sébastien Ballet 3 1 Department of Imaging and
Review Article Transcatheter embolization therapy in liver cancer: an update of clinical evidences Yì-Xiáng J. Wáng 1, Thierry De Baere 2, Jean-Marc Idée 3, Sébastien Ballet 3 1 Department of Imaging and
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
8/1/2017. Disclosures. Outline. SAM Imaging Education Course 90Y-Microsphere Therapy: Emerging Trends and Future Directions
 SAM Imaging Education Course Y-Microsphere Therapy: Emerging Trends and Future Directions Matt Vanderhoek, PhD Henry Ford Health System, Detroit, MI Vanessa Gates, MS Northwestern University, Chicago,
SAM Imaging Education Course Y-Microsphere Therapy: Emerging Trends and Future Directions Matt Vanderhoek, PhD Henry Ford Health System, Detroit, MI Vanessa Gates, MS Northwestern University, Chicago,
Interventional Radiologic Treatment of Hepatocellular Carcinoma
 Interventional Radiologic Treatment of Hepatocellular Carcinoma Fatih Boyvat Abstract The current treatment modalities for patients with hepatocellular carcinoma are discussed in this review. Hepatocellular
Interventional Radiologic Treatment of Hepatocellular Carcinoma Fatih Boyvat Abstract The current treatment modalities for patients with hepatocellular carcinoma are discussed in this review. Hepatocellular
NHS England. Cedar on behalf of NHS England Specialised Commissioning
 NHS England Evidence review: selective internal radiation therapy (SIRT) with ytrrium-90 microspheres for unresectable, liver-only or liver-dominant metastatic colorectal carcinoma who are chemotherapyrefractory
NHS England Evidence review: selective internal radiation therapy (SIRT) with ytrrium-90 microspheres for unresectable, liver-only or liver-dominant metastatic colorectal carcinoma who are chemotherapyrefractory
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Regional Therapy for Metastatic Neuroendocrine Tumors. Janette Durham, MD Professor of Radiology University of Colorado School of Medicine
 Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Clinical Study Real-Life Report on Chemoembolization Using DEBIRI for Liver Metastases from Colorectal Cancer
 Gastroenterology Research and Practice Volume 5, Article ID 75, 6 pages http://dx.doi.org/.55/5/75 Clinical Study Real-Life Report on Chemoembolization Using DEBIRI for Liver Metastases from Colorectal
Gastroenterology Research and Practice Volume 5, Article ID 75, 6 pages http://dx.doi.org/.55/5/75 Clinical Study Real-Life Report on Chemoembolization Using DEBIRI for Liver Metastases from Colorectal
CLINICAL STUDY ABSTRACT
 CLINICAL STUDY Metaanalysis of Survival, Complications, and Imaging Response following Chemotherapy-based Transarterial Therapy in Patients with Unresectable Intrahepatic Cholangiocarcinoma Charles E.
CLINICAL STUDY Metaanalysis of Survival, Complications, and Imaging Response following Chemotherapy-based Transarterial Therapy in Patients with Unresectable Intrahepatic Cholangiocarcinoma Charles E.
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
RADIATION SEGMENTECTOMY. Robert J Lewandowski, MD
 RADIATION SEGMENTECTOMY Robert J Lewandowski, MD Robert Lewandowski, M.D. Consultant/Advisory Board: Cook Medical, LLC, Arsenal, BTG International, Boston Scientific Corp., ABK Reference Unlabeled/Unapproved
RADIATION SEGMENTECTOMY Robert J Lewandowski, MD Robert Lewandowski, M.D. Consultant/Advisory Board: Cook Medical, LLC, Arsenal, BTG International, Boston Scientific Corp., ABK Reference Unlabeled/Unapproved
Tips and tricks. Camillo Aliberti, Massimo Tilli
 Tips and tricks Camillo Aliberti, Massimo Tilli Unit of Oncological Diagnostic and Interventional Radiology, Delta Hospital AUSL Ferrara, Ferrara Italy camy.ali@libero.it mtilli72@libero.it Intra-arterial
Tips and tricks Camillo Aliberti, Massimo Tilli Unit of Oncological Diagnostic and Interventional Radiology, Delta Hospital AUSL Ferrara, Ferrara Italy camy.ali@libero.it mtilli72@libero.it Intra-arterial
hqtace The Next Generation in Liver Cancer Treatment
 HepaSphere Microspheres Quality Targeted to the tumor Absorbs drug Conforms to the vessel Elutes and embolizes hqtace The Next Generation in Liver Cancer Treatment Quality TACE hqtace The No-Compromise
HepaSphere Microspheres Quality Targeted to the tumor Absorbs drug Conforms to the vessel Elutes and embolizes hqtace The Next Generation in Liver Cancer Treatment Quality TACE hqtace The No-Compromise
Hepatic arterial infusion pump chemotherapy for colorectal liver metastases: an old technology in a new era
 Curr Oncol, Vol. 21, pp. e116-121; doi: http://dx.doi.org/10.3747/co.21.1592 HAI PUMP CHEMOTHERAPY FOR CRC METASTASIS REVIEW ARTICLE Hepatic arterial infusion pump chemotherapy for colorectal liver metastases:
Curr Oncol, Vol. 21, pp. e116-121; doi: http://dx.doi.org/10.3747/co.21.1592 HAI PUMP CHEMOTHERAPY FOR CRC METASTASIS REVIEW ARTICLE Hepatic arterial infusion pump chemotherapy for colorectal liver metastases:
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Minimizing Unnecessary Radiation Exposure to Healthcare Professionals and Patients Imagine where we can go.
 ALARA & RADIATION SAFETY Minimizing Unnecessary Radiation Exposure to Healthcare Professionals and Patients Imagine where we can go. What is ALARA? As Low As Reasonably Achievable The use of radiation
ALARA & RADIATION SAFETY Minimizing Unnecessary Radiation Exposure to Healthcare Professionals and Patients Imagine where we can go. What is ALARA? As Low As Reasonably Achievable The use of radiation
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.9 T2 Effective Date: January 1, 2017 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.9 T2 Effective Date: January 1, 2017 Table of Contents Page INSTRUCTIONS
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Cholangiocarcinoma. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2017T0445N Effective Date: January 1, 2017 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2017T0445N Effective Date: January 1, 2017 Table of Contents Page INSTRUCTIONS
Feasibility Study of Transcatheter Arterial Chemoembolization with Epirubicin Drug-eluting Beads for Hepatocellular Carcinoma in Japanese Patients
 Original Research Feasibility Study of Transcatheter Arterial Chemoembolization with Epirubicin Drug-eluting Beads for Hepatocellular Carcinoma in Japanese Patients 1) Department of Diagnostic Radiology,
Original Research Feasibility Study of Transcatheter Arterial Chemoembolization with Epirubicin Drug-eluting Beads for Hepatocellular Carcinoma in Japanese Patients 1) Department of Diagnostic Radiology,
Disclosures. I am on the Onyx speaker bureau I am a paid consultant to. Boston Scientific CeloNova Cook MDS Nordion Sirtex
 Disclosures I am on the Onyx speaker bureau I am a paid consultant to Boston Scientific CeloNova Cook MDS Nordion Sirtex Comparing Y90 Devices Matthew S. Johnson MD, FSIR Indiana University School of Medicine
Disclosures I am on the Onyx speaker bureau I am a paid consultant to Boston Scientific CeloNova Cook MDS Nordion Sirtex Comparing Y90 Devices Matthew S. Johnson MD, FSIR Indiana University School of Medicine
MP Transcatheter Arterial Chemoembolization to Treat Primary or Metastatic Liver Malignancies
 Medical Policy MP 8.01.11 BCBSA Ref. Policy: 8.01.11 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 7.01.75 Cryosurgical Ablation of Primary or Metastatic Liver Tumors
Medical Policy MP 8.01.11 BCBSA Ref. Policy: 8.01.11 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 7.01.75 Cryosurgical Ablation of Primary or Metastatic Liver Tumors
The Management of Advanced Stage Hepatocellular Carcinoma
 The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
Disclosure. Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report:
 Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
ALARA and Radiation Safety
 ALARA and Radiation Safety Experience the power of TheraSphere and deliver hope where it s needed most. Imagine where we can go. btg-im.com What is TheraSphere? TheraSphere is indicated for radiation treatment
ALARA and Radiation Safety Experience the power of TheraSphere and deliver hope where it s needed most. Imagine where we can go. btg-im.com What is TheraSphere? TheraSphere is indicated for radiation treatment