LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE METASTASES
|
|
|
- Blaise Austin
- 5 years ago
- Views:
Transcription
1 LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami Miller School of Medicine Sylvester Comprehensive Cancer Center
 4 th highest mortality rate (~ 608,000/yr) CRC US")
 Worldwide Developed Developing CA: A Cancer Journal for")
2 CRC as worldwide health problem CRC Global Statistics: 3 rd highest incidence rate (~ 1,200,000/yr) 4 th highest mortality rate (~ 608,000/yr) CRC US Statistics: 3 rd highest incidence rate (~ 143,000/yr) 2 nd highest mortality rate (~ 51,500/yr) Worldwide Developed Developing CA: A Cancer Journal for Clinicians 2011;61:69-90
3 Scope of the Problem Nearly 25% of patients present with synchronous metastatic disease at first diagnosis An additional 40-50% develop metastases during the course of their disease Liver involvement is a major source of organ failure, morbidity and mortality in the majority of patients Surgical resection is the standard treatment in pts with resectable liver metastases 5-year survival after resection is ~ 25-35% 40-60% of patients who undergo surgery have recurrent disease Despite new, active chemotherapy regimens, the majority of MCRC patients have progressive disease Ablative techniques or locoregional drug delivery may allow localized minimally invasive therapy and low systemic toxicity Rees M, et al. Annals of Surgery. 247(1) 2008
4 Liver directed therapy options for unresectable CRC liver metastases to be discussed Regional Therapies Trans-arterial chemoembolization (TACE) Selective Internal Radiation Therapy (SIRT) Local Ablation techniques Radiofrequency ablation (RFA) Irreversible electroporation (Nanoknife)


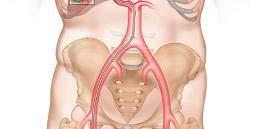
5 Rationale for regional/intraarterial therapies Tumors receive % of their blood supply from hepatic artery Normal liver receives > 75% of its blood supply from portal vein
 Transarterial embolization with chemotherapy (TACE) Embolic particles mixed with")
 currently studied in MCRC 1 Kemeny NE, et al. JCO. 24(9) 2006. 2 Llovet JM, et al. Lancet.")
6 Hepatic Intra-arterial arterial Chemotherapy Regional chemotherapy through the hepatic artery Hepatic intra-arterial chemotherapy FUDR via implantable pump Better than FU/LV 1 Historical Interest (not commonly used) Transarterial embolization with chemotherapy (TACE) Embolic particles mixed with chemotherapeutic drugs, producing a shutdown of blood flow and simultaneous release of high dose of drug Approved for intermediate stage HCC without portal invasion 2 Drug Eluting Beads (irinotecan) currently studied in MCRC 1 Kemeny NE, et al. JCO. 24(9) Llovet JM, et al. Lancet. 369:







7 Drug Eluting Beads Soft deformable microspheres loaded with a chemotherapeutic agent, slowly degradable Reduce blood flow to tumor Slowly release of drug, enhancing local anti-tumor tumor effect and decreased systemic exposure
8 Procedure is performed under conscious sedation, antibiotic prophylaxis, hl and antiemetic i drugs Demonstrate liver arterial anatomy and the feeding vessels of the tumor Injection of loaded beads into the feeding vessels using 3 french micro catheter catheter COMPLICATIONS* Most common: Post embolization syndrome (abdominal pain, nausea, vomiting, fever (40 63%) Liverenzyme enzyme elevation (allpatients; > 3xULN: 58% Bilirubin elevation: 18% Hypertension transient (maybe related to pain) *Fiorentini et al. Anticancer Research, 2012.
")
 vs. 15 months (95% CI 12-18); p 0.031 PFS: 7 (CI 3-11) vs. 4 months (3-5) p 0.")
9 DEBIRI vs. FOLFIRI 74 pts Liver only metastases, occupying less than 50% of parenchyma Prior chemotherapy (2-3 lines) allowed 36 pts (DEBIRI); 38 pts (FOLFIRI) Number of cycles: Debiri: 2; FOLFIRI: 8 Median survival: 22 (95% CI 21-23) vs. 15 months (95% CI 12-18); p PFS: 7 (CI 3-11) vs. 4 months (3-5) p Time to extrahepatic progression: 13 (CI 10-16) vs. 9 (CI 5-13) months (NS) Fiorentini G, et al. Anticancer research. 32(4) 2012
10 Systemic Chemotherapy + DEBIRI Randomized controlled trial of irinotecan drug eluting beads with simultaneous FOLFOX and bevacizumab for patients with unresectable colorectal liver-limited metastasis N: 70 patients 40 pts randomized to FOLFOX-Bev/DEBIRI O (alternate (ate ate weeks) 30 pts randomized to FOLFOX/Bev ORR: 78% vs. 54% (2 months), 76 vs. 60% (6 months) Greater downsizing to resection (35% vs 16%) Improved mpfs (15.3 vs. 7.6 months) Grade 3/4 AEs: 54% vs. 46% Martin RC, et at. ASCO GI Symposium, 2014



 per")



11 Selective Internal Radiation Therapy To selectively target a radiation dose high enough to kill tumors cells within the liver, while maintaining a low radiation dose to normal parenchyma SIR-Spheres Y-90 bound to microspheres Biocompatible resin (32) µmicron diameter 50 Bq/sphere x 10(6) per 3 GBq vial Y-90: Beta emitter Physical half life: 64.1 hours Maximum energy: 2.28 MeV / Mean energy: 938 kev Mean tissue penetration: 2.5 mm Tumor vessels 25μm -75μm diameter End arterioles 8μm diameter SIR-Spheres microspheres mean diameter 32.5μm
12 Who are candidates for Y-90 treatment? Patients with liver metastasis from GI, Breast or other tumor primary Bilirubin < 2 mg/dl Albumin above 3 No history of ascites or hepatic encephalopathy Well controlled primary cancer Performance status, ECOG 0-2 Life expectancy >3 months





13 SIRT: Planning Procedures Angiographic evaluation of hepatic vasculature Evaluation of lung shunting/ TcMAA Treatment Planning
14 SIR-Spheres microspheres + 5FU in mcrc Salvage age Therapy: Design Eligible ibl Patients t Liver-only mcrc, PS 0 2, refractory to chemotherapy Stratify Institution Interval to progression on chemotherapy 5FU protracted IV infusion (300 mg/m 2 D1 14 q3w) Random Assignment Arm A: Arm B: 90 Y resin microspheres on Day 1 (D1) Cycle 1 (C1) + 5FU protracted IV infusion (225 mg/m 2 D1 14 C1 and 300 mg/m 2 D1 14 q3w thereafter) Eligible Patients Liver-dominant mcrc, PS 0 2 Hendlisz A et al. J Clin Oncol 2010; 28: until progression 90 Y resin microspheres until progression
15 Proport tion of pa atients without pr rogressio on SIR-Spheres microspheres + 5FU in mcrc Salvage Therapy: Primary Endpoint Time to Liver Progression Time to Progression at: Any Site Liver 5FU 5FU + radioembolization ( censored) HR: %CI: P = Time from Random Assignment (months) Hendlisz A et al. J Clin Oncol 2010; 28: M-PPP US rev. 0
16 SIR-Spheres microspheres + 5FU in mcrc Salvage Therapy: Time to Progression & Overall Survival 5FU alone 5FU + Hazard Ratio SIR-Spheres (95% CI) n=23 n=21 p value Median Time to 0.38 ( ) Liver Progression: 2.1 months 5.5 months p=0.003 TTLP censored to 0.35 ( ) change of Tx plan: 2.1 months 5.6 months p=0.002 Median Time to 051( ( ) 0 Progression: 2.1 months 4.5 months p=0.03 Median Overall 0.92 ( ) Survival: 7.3 months * 10.0 months p= months * note: 10 patients in the 5FU arm received SIR-Spheres as salvage therapy after disease progression Hendlisz A et al. J Clin Oncol 2010; 28:
17 SIR-Spheres microspheres + 5FU in mcrc Salvage Therapy: Results Best Overall Hepatic Response 5FU alone 5FU + SIR-Spheres n=23 n=21 p value Partial Response, n (%): 0 2 (10%) p=0.22 Stable Disease, n (%): 8 (35%) 16 (76%) Disease Control Rate, n (%):8 (35%) 18 (85%) p=0.001 Progressive Disease, n (%):14 (61%) 2 (10%) Not Evaluable, n (%): 1 (4%) 1 (5%) Surgical Resection, n (%): 0 1 (5%) One patient in Arm B was sufficiently down-sized to enable an R0 resection to be performed successfully Hendlisz A et al. J Clin Oncol 2010; 28:
18 SIR-Spheres microspheres + 5FU in mcrc Salvage Therapy: Toxicity Assessments Parameter 5FU alone 5FU + SIR-Spheres n = 23 n = 21 Grades 1 2 Grades 3 4 Grades 1 2 Grade 3 4 Gastrointestinal Stomatitis Diarrhea Nausea Vomiting Constipation Anorexia Gastrointestinal t ti Pain Abdominal pain Myalgia Pain other Hendlisz A et al. J Clin Oncol 2010; 28:
19 SIR-Spheres microspheres + 5FU in mcrc Salvage Therapy: Toxicity Assessments Parameter 5FU alone 5FU + SIR-Spheres n = 23 n = 21 Grades 1 2 Grades 3 4 Grades 1 2 Grade 3 4 Constitutional Fatigue Fever Dermatological/Skin Skin Hand-foot syndrome Pulmonary Dyspnea Pulmonary Neurological Neurosensorial Cognitive disturbance Cardiac arrhythmia Allergy Other Toxicity Hendlisz A et al. J Clin Oncol 2010; 28: ascites; 1 with thrombocytopenia, 1 with stomach ulcer, ascites



20 Radiofrequency Thermal Ablation (RFA) HIGH FREQUENCY ALTERNATING CURRENT DELIVERED TO TUMOR VIA AN ELECTRODE. THE CURRENT AGITATES THE TISSUE AROUND THE TIP, CAUSING CHARGED MOLECULES, MAINLY H2O TO RAPIDLY OSCILLATE ALONG A 180º AXIS



")
21 Radiofrequency Ablation Approach: Open, laparoscopic, percutaneous Success depends on tumor size, location, physician experience Retrospective series suggest that local recurrence rates are lower in tumors < 3 cm. Complications (uncommon): hemorrhage, hepatic abscess, infarction, pleural effusion, bronchobiliary fistula, bowel perforation, thrombosis, skin burn. RFA is inferior to resection (higher local recurrence rates) No prospective studies comparing RFA vs. other liver directed therapies

 vs. 9.9 mos *oxaliplatin based Ruers T et al.")
22 RFA in combination with systemic chemotherapy EORTC 40004: RFA + systemic therapy vs. systemic therapy alone in pts with non-resectable colorectal liver metastases Systemic therapy*: 59 pts Systemic therapy* +RFA: 60 pts PFS rate at 3 years: 27.6% vs. 10.6% Median PFS: 16.8 ( ) vs. 9.9 mos *oxaliplatin based Ruers T et al. Ann Oncol 2012;23:
23 Role of RFA in the management of unresectable CRC liver metastases No prospective data to demonstrate better OS over chemotherapy alone. Potential option in patients with potentially resectable isolated liver metastases who are not surgical candidates Best results with RFA in patients with < 3 lesions, < 3.5 cm in diameter that are not located near major vascular structures. It is sometimes used intraoperatively following incomplete resection in patients with isolated liver metastases
24 Irreversible Electroporation (IRE) A FOCAL NON THERMAL ABLATION THERAPY THAT USES HIGH VOLTAGE LOW ENERGY DC ELECTRICAL PULSES TO PERMANENTLY OPEN PORES IN THE CELL MEMBRANES CAUSING CELLS TO DIE.



 and delivers 1 energy pulse.")
 the ventricular refractory period.")
25 IRREVERSIBLE ELECTROPORATION? Nanoknife Tissue Nanoknife ablation AccuSync 72 ECG Ablation System monopolar probe trigger monitor DSync device (e.g. AccuSync 72) senses the rising slope of the R-wave, and sends a signal to the NanoKnife. The NanoKnife waits 50 milliseconds (.05 sec) and delivers 1 energy pulse. The energy pulse is delivered d during (or just before) the ventricular refractory period. Delivering an IRE Pulse during the vulnerable period could induce an arrhythmia.

 Preservation of vital structures")
, compared")


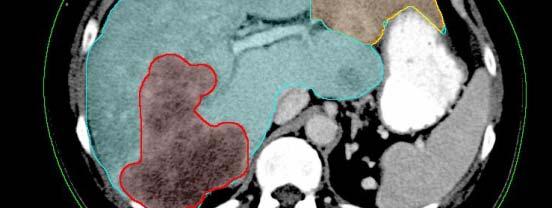
26 IRE: Potential Advantages 3.5 cm hypodense lesion immediately adjacent to IVC, with mass effect on the adjacent hepatic veins. Short ablation time (usually under 5 minutes) Preservation of vital structures t (vessels, bile ducts) within IRE ablated zone IRE induces cell death by apoptosis, without significant inflammatory reaction (and scarring), compared to other ablative techniques. Avoids heat/cold sink effect (which may cause incomplete ablation in perivascular tumor cells) IRE induces complete ablation with well demarcated margin This is a relatively new technique, used in liver and extrahepatic (i.e. pancreas) tumors Early experience indicates that procedure is well tolerated, and postprocedure pain is not different compared to RFA* *Narayanan G, et el. Sem. Intervent. Radiol. 2013
27 Conclusions o s An increasing number of local/regional treatment options exist for patients with unresectable colorectal liver metastases Decisions on indication, strategies, and timing REQUIRES multidisciplinary evaluation (medical oncologist, surgeon, radiation therapist, interventional radiologist There is increasing prospective clinical trial data on the safe and effective use of radioembolization and TACE with irinotecan drug eluting beads The role of local ablative techiques (RFA, IRE) is evolving They should not replace resection as the standard in the appropriate settings IRE may play a role in lesions not amenable by RFA
28
SIR-Spheres: Des essais cliniques à la pratique courante
 SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
Role of SIRT Beyond First Line Therapy in Colorectal Cancer. Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore
 Role of SIRT Beyond First Line Therapy in Colorectal Cancer Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore MILESTONES IN THE TREATMENT OF COLON CANCER SIR-Spheres microspheres
Role of SIRT Beyond First Line Therapy in Colorectal Cancer Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore MILESTONES IN THE TREATMENT OF COLON CANCER SIR-Spheres microspheres
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES. Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí
 INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
+ Radioembolization for ColoRectal Cancer Metastatic to the Liver
 + Radioembolization for ColoRectal Cancer Metastatic to the Liver Oct 4 th 2017 Alain Hendlisz, Institut Jules Bordet 1 st International Course on THERANOSTICS & MOLECULAR RADIOTHERAPY Indication and Rationale
+ Radioembolization for ColoRectal Cancer Metastatic to the Liver Oct 4 th 2017 Alain Hendlisz, Institut Jules Bordet 1 st International Course on THERANOSTICS & MOLECULAR RADIOTHERAPY Indication and Rationale
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER
 SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
Clinical Study Real-Life Report on Chemoembolization Using DEBIRI for Liver Metastases from Colorectal Cancer
 Gastroenterology Research and Practice Volume 5, Article ID 75, 6 pages http://dx.doi.org/.55/5/75 Clinical Study Real-Life Report on Chemoembolization Using DEBIRI for Liver Metastases from Colorectal
Gastroenterology Research and Practice Volume 5, Article ID 75, 6 pages http://dx.doi.org/.55/5/75 Clinical Study Real-Life Report on Chemoembolization Using DEBIRI for Liver Metastases from Colorectal
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer
 Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
P < vs. 5FU/LV LD 0% 60.0% 3.6 months P < P = 0.113
 in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers
 Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Regional Therapy for Metastatic Neuroendocrine Tumors. Janette Durham, MD Professor of Radiology University of Colorado School of Medicine
 Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Guidelines for SIRT in HCC An Evolution
 Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
NHS England. Cedar on behalf of NHS England Specialised Commissioning
 NHS England Evidence review: selective internal radiation therapy (SIRT) with ytrrium-90 microspheres for unresectable, liver-only or liver-dominant metastatic colorectal carcinoma who are chemotherapyrefractory
NHS England Evidence review: selective internal radiation therapy (SIRT) with ytrrium-90 microspheres for unresectable, liver-only or liver-dominant metastatic colorectal carcinoma who are chemotherapyrefractory
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
Disclosure. Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report:
 Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases
 Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
State-of-the-art minimally invasive interventions for liver tumors
 William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days
 94% of radiation delivered within 11 days") 100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data
![DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data](/thumbs/78/77499894.jpg "DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data") DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data Professor Thomas J Vogl Goethe University Hospital Frankfurt-am-Main,
DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data Professor Thomas J Vogl Goethe University Hospital Frankfurt-am-Main,
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Incorporating biologics in the management of older patients with metastatic colorectal cancer
 Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Treatment of 200 Locally Advanced (Stage III) Pancreatic Adenocarcinoma Patients with Irreversible Electroporation: Safety and Efficacy
 Pancreatic Adenocarcinoma Patients with Irreversible Electroporation: Safety and Efficacy") The following three articles refer to the same April 2015 ASA presentation, and the same research. But, more data is offered in the third article. Treatment of 200 Locally Advanced (Stage III) Pancreatic
The following three articles refer to the same April 2015 ASA presentation, and the same research. But, more data is offered in the third article. Treatment of 200 Locally Advanced (Stage III) Pancreatic
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
treatment options for primary liver malignancies and metastatic disease
 State of the art treatment options for primary liver malignancies and metastatic disease Peter Huppert Prof. of Radiology and Neuroradiology Klinikum Darmstadt Certified Vascular and Oncologic Center Disclosure
State of the art treatment options for primary liver malignancies and metastatic disease Peter Huppert Prof. of Radiology and Neuroradiology Klinikum Darmstadt Certified Vascular and Oncologic Center Disclosure
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology
 Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Helping you access curative therapies for liver cancer patients
 Metastatic colorectal cancer (mcrc) Helping you access curative therapies for liver cancer patients Biocompatibles Excellence in Interventional Oncology Biocompatibles UK Ltd is a BTG International group
Metastatic colorectal cancer (mcrc) Helping you access curative therapies for liver cancer patients Biocompatibles Excellence in Interventional Oncology Biocompatibles UK Ltd is a BTG International group
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads
 with Drug-Eluting Beads") Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads A minimally invasive treatment for liver cancer Provided as an educational service by Biocompatibles UK Ltd, a BTG International group company
Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads A minimally invasive treatment for liver cancer Provided as an educational service by Biocompatibles UK Ltd, a BTG International group company
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Tips and tricks. Camillo Aliberti, Massimo Tilli
 Tips and tricks Camillo Aliberti, Massimo Tilli Unit of Oncological Diagnostic and Interventional Radiology, Delta Hospital AUSL Ferrara, Ferrara Italy camy.ali@libero.it mtilli72@libero.it Intra-arterial
Tips and tricks Camillo Aliberti, Massimo Tilli Unit of Oncological Diagnostic and Interventional Radiology, Delta Hospital AUSL Ferrara, Ferrara Italy camy.ali@libero.it mtilli72@libero.it Intra-arterial
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
New Energy Sources for Local Ablation Therapy. Jeong Kyong Lee, MD Ewha Womans University
 New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
SUMMARY OF THE SIRFLOX RESULTS
 SUMMARY OF THE SIRFLOX RESULTS The SIRFLOX study results on the combination of SIR-Spheres Y-90 resin microspheres with first-line chemotherapy were published in Journal of Oncology in early 2016. 1 There
SUMMARY OF THE SIRFLOX RESULTS The SIRFLOX study results on the combination of SIR-Spheres Y-90 resin microspheres with first-line chemotherapy were published in Journal of Oncology in early 2016. 1 There
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma
 Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
Corporate Medical Policy
 Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
SIRT in Neuroendocrine Tumors
 SIRT in Neuroendocrine Tumors Marnix G.E.H. Lam, MD PhD Professor of Nuclear Medicine AVL Amsterdam UMC Utrecht ENETS Center of Excellence, The Netherlands Disclosure of speaker s interests Consultant
SIRT in Neuroendocrine Tumors Marnix G.E.H. Lam, MD PhD Professor of Nuclear Medicine AVL Amsterdam UMC Utrecht ENETS Center of Excellence, The Netherlands Disclosure of speaker s interests Consultant
Description. Section: Therapy Effective Date: July 15, 2014 Subsection: Therapy Original Policy Date: June 7, 2012 Subject: Page: 1 of 23
 Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
C.W. Nutting & J.S. Zager on behalf of the DCTH P3 Investigators
 Chemosaturation Therapy with Percutaneous Hepatic Perfusions of Melphalan Versus Standard of Care in Patients with Hepatic Metastases from Melanoma: A Randomized Multicenter Phase 3 Study C.W. Nutting
Chemosaturation Therapy with Percutaneous Hepatic Perfusions of Melphalan Versus Standard of Care in Patients with Hepatic Metastases from Melanoma: A Randomized Multicenter Phase 3 Study C.W. Nutting
Clinical Commissioning Policy Proposition:
 Clinical Commissioning Policy Proposition: Selective internal radiation therapy (SIRT) in the treatment of chemotherapy refractory and intolerant, unresectable metastatic colorectal cancer (Adults) Reference:
Clinical Commissioning Policy Proposition: Selective internal radiation therapy (SIRT) in the treatment of chemotherapy refractory and intolerant, unresectable metastatic colorectal cancer (Adults) Reference:
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Evaluation of SIRFLOX Study Results. Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany
 Evaluation of SIRLX Study Results Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany ESM Guideline: Response is a Goal of Treatment Performance Status of the
Evaluation of SIRLX Study Results Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany ESM Guideline: Response is a Goal of Treatment Performance Status of the
NHS England Reference: P
 Clinical Commissioning Policy: Selective internal radiation therapy (SIRT) for chemotherapy refractory / intolerant metastatic colorectal cancer (adults) NHS England Reference: 170102P 1 NHS England INFORMATION
Clinical Commissioning Policy: Selective internal radiation therapy (SIRT) for chemotherapy refractory / intolerant metastatic colorectal cancer (adults) NHS England Reference: 170102P 1 NHS England INFORMATION
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE. clic per modificare lo stile del sottotitolo dello schem
 XII Congresso Nazionale AIMN 2015 16-19 Aprile 2015 Rimini RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE clic per modificare lo stile del sottotitolo dello schem Marco Maccauro Nuclear Medicine
XII Congresso Nazionale AIMN 2015 16-19 Aprile 2015 Rimini RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE clic per modificare lo stile del sottotitolo dello schem Marco Maccauro Nuclear Medicine
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Selective Internal Radiation Therapy. Jefferson R. Pagsisihan, MD, DPSNM The Medical City St. Luke s Medical Center
 Selective Internal Radiation Therapy Jefferson R. Pagsisihan, MD, DPSNM The Medical City St. Luke s Medical Center S Selective Internal Radiation Therapy catheter-based liver directed modality for patients
Selective Internal Radiation Therapy Jefferson R. Pagsisihan, MD, DPSNM The Medical City St. Luke s Medical Center S Selective Internal Radiation Therapy catheter-based liver directed modality for patients
EPIDEMIOLOGY. Long established risk factors for CCA: hepatobiliaryflukes, PSC, biliary tract cysts, epatolithiasis.
 EPIDEMIOLOGY Intrahepatic cholangiocarcinoma(icc) is the second most common (15%) primary liver cancer after hepatocellular carcinoma (HCC), with a rate of about 2.1/100,000 people per year in western
EPIDEMIOLOGY Intrahepatic cholangiocarcinoma(icc) is the second most common (15%) primary liver cancer after hepatocellular carcinoma (HCC), with a rate of about 2.1/100,000 people per year in western
General summary GENERAL SUMMARY
 General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Study Objective and Design
 Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Y90 SIRT Therapy Dosimetric Aspects
 Y90 SIRT Therapy Dosimetric Aspects David Chee-Eng Ng MBBS, BSc, MSc, MRCP, FAMS, FRCP (Edin) Head and Senior Consultant, Department of Nuclear Medicine and PET Singapore General Hospital Adjunct Assistant
Y90 SIRT Therapy Dosimetric Aspects David Chee-Eng Ng MBBS, BSc, MSc, MRCP, FAMS, FRCP (Edin) Head and Senior Consultant, Department of Nuclear Medicine and PET Singapore General Hospital Adjunct Assistant
SIRT for Intermediate and Advanced HCC
 Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Advances in percutaneous ablation for hepatocellular carcinoma
 Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT Dosimetry: Sometimes Less Is More
 SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
First-line therapy for unresectable HCC:
 ESMO GI Cancer Preceptorship 15 November 2017 Singapore First-line therapy for unresectable HCC: an oncologist s viewpoint Chiun Hsu, MD, PhD G raduate I n stitute of Oncology, National Taiwan Univers
ESMO GI Cancer Preceptorship 15 November 2017 Singapore First-line therapy for unresectable HCC: an oncologist s viewpoint Chiun Hsu, MD, PhD G raduate I n stitute of Oncology, National Taiwan Univers
Clinical Study Yttrium-90 Radioembolization for Colorectal Cancer Liver Metastases: A Single Institution Experience
 International Journal of Surgical Oncology Volume 20, Article ID 5726, 9 pages doi:0.55/20/5726 Clinical Study Yttrium-90 Radioembolization for Colorectal Cancer Liver Metastases: A Single Institution
International Journal of Surgical Oncology Volume 20, Article ID 5726, 9 pages doi:0.55/20/5726 Clinical Study Yttrium-90 Radioembolization for Colorectal Cancer Liver Metastases: A Single Institution
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
OPTIMA Phase III Clinical Trial: Study Design and Protocols
 OPTIMA Phase III Clinical Trial: Study Design and Protocols Riccardo Lencioni, MD, FSIR, EBIR Professor of Radiology University of Pisa School of Medicine Division of Diagnostic Imaging & Intervention
OPTIMA Phase III Clinical Trial: Study Design and Protocols Riccardo Lencioni, MD, FSIR, EBIR Professor of Radiology University of Pisa School of Medicine Division of Diagnostic Imaging & Intervention
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
HCC RADIOLOGIC DIAGNOSIS
 UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
Tumors in the Randomized German AIO study KRK-0306
 FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
Future Needs for Standards in 90 Y Microsphere Therapy. CIRMS 2012 Reed Selwyn, PhD, DABR 24 October 2012
 Future Needs for Standards in 90 Y Microsphere Therapy CIRMS 2012 Reed Selwyn, PhD, DABR 24 October 2012 Objectives I. General Description Microsphere Distribution Product Comparison II. Dosimetry Models
Future Needs for Standards in 90 Y Microsphere Therapy CIRMS 2012 Reed Selwyn, PhD, DABR 24 October 2012 Objectives I. General Description Microsphere Distribution Product Comparison II. Dosimetry Models
The Management of Advanced Stage Hepatocellular Carcinoma
 The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC
 Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY