17th ESO ESMO Masterclass in Clinical Oncology
|
|
|
- Brice Austin
- 5 years ago
- Views:
Transcription



1 NSCLC Radiotherapy Prof Corinne Faivre-Finn Manchester Radiotherapy Related Research Group Manchester Lung Cancer Group The Christie, Manchester, UK 17 th ESO-ESMO Masterclass 25 th March 2018
2 Early stage disease SABR Objectives Locally advanced disease Standard radiotherapy Standard chemotherapy Metastatic disease Role of WBRT Case discussions
3 Early stage NSCLC

4 78 yr old male Chest infection CXR LUL lesion PMH COPD, emphysema, MI, ex smoker 52 pack year history WHO PS=2, MRC RS 3 FEV1 32% predicted KCO 36% predicted PETCT- LUL lesion SUV 15 CT guided biopsy SCC Clinical case Treatment options Lobectomy + mediastinal exploration Wedge resection+ mediastinal exploration CHART Standard conformal RT SABR
5 SABR Surgical resection is the optimal curative treatment, but <50% of patients are medically fit for this With standard RT local control (<50%) and survival are inferior to surgery 5 years) What is SABR? High dose RT Hypofractionation (3-8) Allowing precise RT delivery to the tumour Allows to spare nearby healthy organs Requires 4DCT and IGRT SABR offers local tumour control (>90%) comparable with surgery SABR delivered routinely in most academic European centres Roach. JTO 2015
6 Study No. of patient s RT Dose fractionatio n Baumann Gy in 2-4 fractions Lagerwaard x 20 Gy 5 x 12 Gy BED (Gy) Median fu (months) Local control years 180 Gy 132 Gy 12 2 years Nagata 45 4 x 12 Gy 106 Gy 30 2 years Survival Toxicity 55%@5yrs Atelectasis: 2%* Pneumonitis: 1%* Rib fractures: 4%º 64%@2yrs Pneumonitis: 3%* Rib fractures: 2%º 83%@3yrs stage Ia 72%@3yrs stage Ib Nyman 45 3 x 15 Gy 113 Gy 43 80% 55%@3yrs 30%@5yrs Onishi Gy in 1-22 fractions Timmerman 70 3 x 20 Gy 3 x 22 Gy Umetsu Gy in 5-10 fractions Various 38 84% if BED years 180 Gy 122 Gy Guidelines ASTRO ESMO EORTC BTS SABR is a treatment option for medically inoperable, peripheral, early stage NSCLC 18 2 years Pneumonitis: 0%* Pneumonitis: 0%* Rib fractures: 4%º 47%@ 5 yrs Pneumonitis: 5%* 54%@2 yrs Various 36 94% 66%@3 yrs (some operable pts) Pericardial Effusion: 1% (grade 5) Bleeding: 1% (grade 5) Pneumonitis: 6% (grade 5) Pneumonitis: 0%* Rib fractures:4%º

. 4/6 had central tumours Tumour location (hilar/pericentral v peripheral) was a strong predictor of toxicity (p=0.004) x11 Timmerman et al.")
7 SABR in central tumours Phase II- n=70-t1 or T2 ( 7 cm), N0, M0, biopsy-confirmed NSCLC 60 to 66 Gy/3 fractions. Lung or bone tissue density corrections were not used Dose prescribed to the margin of the PTV, which corresponded to the 80% of isocentre dose volume 8 patients experienced Grade 3+ toxicity (pulmonary function tests, pneumonias, pleural effusions, apnea, and skin reaction) SABR may have contributed to the events leading to the death of 6 patients (4 bacterial pneumonia, 1 pericardial effusion and 1 massive hemoptysis). 4/6 had central tumours Tumour location (hilar/pericentral v peripheral) was a strong predictor of toxicity (p=0.004) x11 Timmerman et al. JCO 2006 Fakiris Int J Radiat Oncol Biol Phys 2009 No fly zone= 2cm radius from main airways and proximal bronchial tree

8 SABR in central tumours Chang. JTO 2015 Need to define OAR constraints Haasbeek. JTO 2011; Chang, Int J Radiat Oncol Biol Phys 2008; Xia. Int J Radiat Oncol Biol Phys 2006; Mangona Int J Radiat Oncol Biol Phys 2014 Acceptable regime Gy/4# Gy/5# 60 Gy/8# 70 Gy/10 # EORTC LungTech study ongoing
 Nyman. Radiother Oncol.")
 and oesophagitis (8 vs. 30%) in the SABR arm. No grade 5 events.")
9 SPACE trial-randomised phase II 102 patients - SABR 66 Gy in 3 fractions (one week) - 3DCRT 70 Gy (7 weeks) Nyman. Radiother Oncol Gy/33 fr Primary endpoint-pfs Fewer cases with pneumonitis (19 vs. 34%) and oesophagitis (8 vs. 30%) in the SABR arm. No grade 5 events. QOL worse dyspnea (p = 0.01), chest pain (p = 0.02) and cough (>10 points difference).





10 SABR vs 3DCRT for Peripheral Early Stage NSCLC CHISEL Trial Ball. WCLC 2017 Freedom from LF HR 0.29, 95% CI 0.13, 0.66 P = Randomised phase III 101 medically inoperable patients or refuse surgery Histologic/cytologic confirmation T1-T2a N0 (PET staged) ECOG PS 0-1 Peripheral tumours Overall survival HR % CI 0.29, 0.91 P = 0.020

11 RCTs SABR vs Surgery (completed) SABR: 10% G3 events Surgery: 44% G3-4 events SABR could be an option for treating operable stage I NSCLC Pooled analysis STARS and ROSEL Chang. Lancet Oncol 2015
12 SABR Take home messages Standard of care in medically inoperable, peripheral stage I NSCLC Local control>90% Convenient for patients and RT departments Results from RCTs comparing SABR vs. surgery awaited Patients with central tumours should be treated in prospective clinical trials

13 Locally advanced NSCLC


14 Metastatic relapse The problem ~30% stage III Role surgery is limited Survival is poor 10-30% at 5 yrs Need for CTRT combinations Local relapse Median survival months


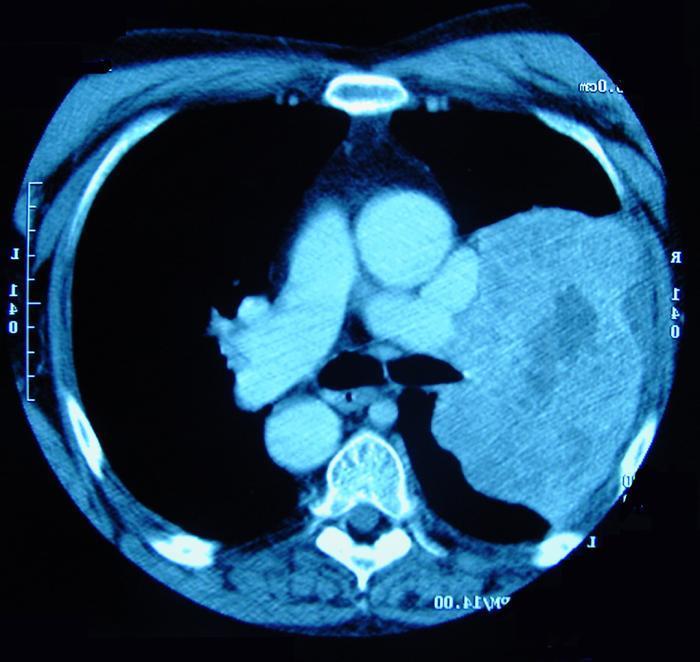
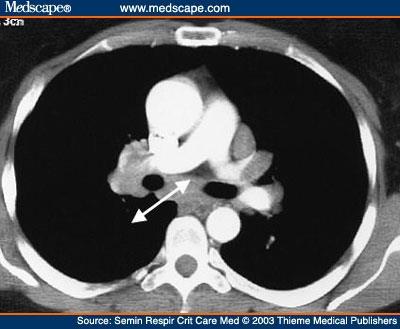
15 53yr old female Locally advanced NSCLC Clinical case Presented with right facial pain, no respiratory symptoms V % PMH hiatus hernia, ex smoker 35 pack year MLD 19.4Gy history Max SC 47.9 Gy WHO PS=0, MRC RS 0 PFTs - FEV1 80% predicted KCO 105% predicted Bronchoscopy - no endobronchial abnormality CT scan - RUL mass and enlarged 4R, 7 lymph nodes T3 N2 M0 EBUS station 4R moderately differentiated adenocarcinoma PET-CT - FDG avid right supraclavicular lymph nodes T3 N3 M0 MR brain - clear 7field IMRT Treatment options Sequential CTRT or Concurrent CTRT CT+Palliative RT 3DCRT or IMRT Induction or consolidation CT?
16 Aupérin. JCO by American Society of Clinical Oncology Meta-analysis concurrent vs. sequential CTRT (A) Survival curves (B) progression-free survival curves 6 RCTs 1,205 patients HR 0.83 (p=0.04); absolute benefit survival 4.5% at 5 years Improved local control Increased acute oesophageal toxicity HR= 4.9 (p < )

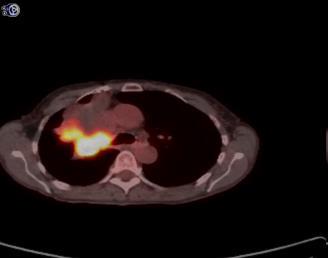
17 P 4DCT PETCT
 Saunders.")

18 60-66 Gy in fractions OD=standard of care CHART study TD>OD RT (54 Gy/36 # over 12 consecutive days vs 60 Gy/30 #/6 weeks) Saunders. Lancet 1997 Altered fractionation>conventional fractionation Mauguen. JCO 2012 No defined role for dose escalation Dose limited by normal tissues Lung - V20, MLD Spinal cord Brachial plexus Oesophagus Heart What RT? Christodoulou. EJC 2014 De Ruysscher. JCO 2010
19 S T R A T I F Y RT Technique 1.3D-CRT 2.IMRT Zubrod PET Staging 1.No 2.Yes Histology 1.Squamous 2.Non- Squamous RTOG 0617 Study Design R A N D O M I Z E Concurrent Treatment Arm A Concurrent chemotherapy* RT to 60 Gy, 5 x per wk for 6 wks Arm B Concurrent chemotherapy* RT to 74 Gy, 5 x per wk for 7.5 wks Arm C Concurrent chemotherapy* and Cetuximab RT to 60 Gy, 5 x per wk for 6 wks Arm D Concurrent chemotherapy* and Cetuximab RT to 74 Gy, 5 x per wk for 7.5 wks *Carboplatin and paclitaxel 90% patients PET staged 185 centres n=464 (high dose vs standard dose; n=544 cetuximab vs no cetuximab) Consolidation Treatment Arm A Consolidation chemotherapy* Arm B Consolidation chemotherapy* Arm C Consolidation chemotherapy* and Cetuximab Arm D Consolidation chemotherapy* and Cetuximab Bradley. Lancet Oncol 2015

 associated with poor")
20 MS (95% CI) Oesophagitis G3+ Treatment related death RTOG Gy 28.7 months ( ) 7% 3 74 Gy 38% greater risk for death in 74 Gy arms Heart dose (V5 and V30) associated with poor survival 20.3 months ( ) 15% 8 Bradley. Lancet Oncol 2015

21 Why Cisplatin as a backbone in the cctrt setting? PE can be combined at full dose with RT Challenged by RTOG 0617 Auperin et al. J Clin Oncol 2010
.")
22 Comparison of concurrent use of carboplatin-paclitaxel versus cisplatin-etoposide with RT for stage III NSCLC Limited data comparing CE vs. CP for definitive chemort for stage III NSCLC. Liang et al, Ann Oncol phase III 200 patients. Median survival 23.3 months EP arm and 20.7 months PC arm (p 0.095, HR 0.76, 95%CI ). Grade 2 radiation pneumonitis higher in the PC arm (33.3% versus 18.9%, p 0.036), Grade3 esophagitis higher in the EP arm (20.0% versus 6.3%, p 0.009). Wang et al, Lung Cancer 2012 small randomized phase II improved PFS and OS for CE vs. CP Santana-Davila et al, JCO 2015 VA retrospective study no difference in PFS or OS, with improved toxicity for CP Literature based meta-analysis , 79 studies (3090 patients from 31 CE studies and 3728 patients from 48 CP studies) Stauer JAMA Oncol 2017
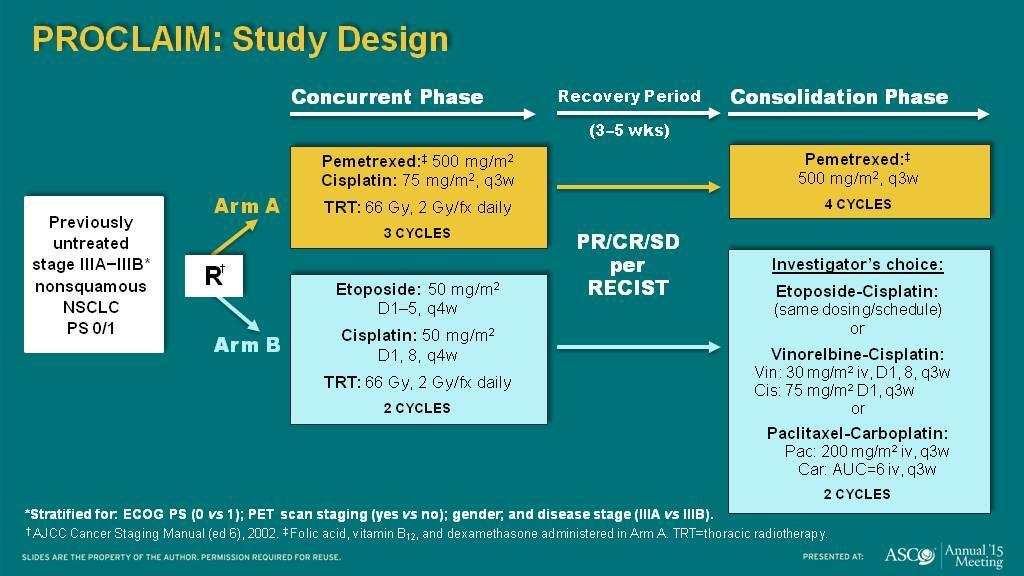

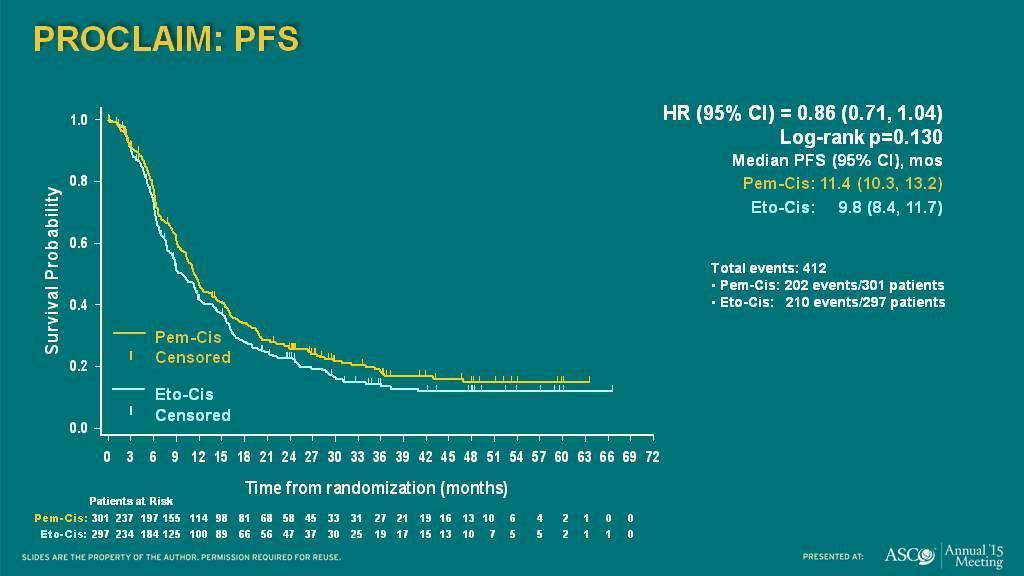
23 Proclaim- Pemetrexed-cisplatin or etoposide-cisplatin plus thoracic radiation therapy in stage III NSCLC Senan. JCO 2016
24 Why induction or consolidation CT? Are 2 or 3 cycles of concurrent CT sufficient concurrently with RT? Concurrent CTRT optimizes local control but distant spread is still a major problem Further systemic chemotherapy to optimize treatment of distant disease?
 32% 36% ns")
25 Vokes. JCO 2007 Induction chemotherapy CALGB CTRT CT CTRT p N Oesophagitis (grade 3-4) 32% 36% ns Pneumonitis (grade 3-4) 4% 10% ns Median survival 12 months 14 months year survival 29% 31%
 EP x2 +/- docetaxel x3 Gefitinib cctrt (61Gy) EP x2 docetaxel x3 +/- gefitinib to PD or 5yrs Hanna")
26 Consolidation chemotherapy Docetaxel cctrt (59.4Gy) EP x2 +/- docetaxel x3 Gefitinib cctrt (61Gy) EP x2 docetaxel x3 +/- gefitinib to PD or 5yrs Hanna et al., J Clin Oncol 2008 Kelly et al. J Clin Oncol 2008
27 Consolidation chemotherapy - KCSG-LU05-04 Multicentre randomised Ph III trial CTRT Cis/Docetaxel weekly x6; RT 66 Gy/33 F CTRT alone v CTRT + Cis/Docetaxel consolidation n=437 Ahn, JCO 2015
 41 trials (7 phase III, 34 phase II) 45 trial arms With consolidation CT (CCT+ ) or without Consolidation CT (CCT- ) Tsujino.")
28 Systematic review Consolidation chemotherapy Pooled analysis of the literature Data from phase II/III concurrent CTRT trials ( ) 41 trials (7 phase III, 34 phase II) 45 trial arms With consolidation CT (CCT+ ) or without Consolidation CT (CCT- ) Tsujino. JTO 2013
) 2:1 Day 1 Max 42 days after the end of CRT Arm 2 Placebo Q2W iv for up to 12 months (Max 26 doses) OS PFS using PI assessments according to RECIST 1.")
29 Role of immunotherapy in stage III NSCLC PACIFIC trial Patients with unresectable Stage III NSCLC No progression following platinum-based ccrt N = 702 Arm 1 Durvalumab 10 mg/kg Q2W for up to 12 months (Max 26 doses)) 2:1 Day 1 Max 42 days after the end of CRT Arm 2 Placebo Q2W iv for up to 12 months (Max 26 doses) OS PFS using PI assessments according to RECIST 1.1* * Disease progression requires confirmation, treatment with MEDI4736 will continue between the initial assessment of progression and confirmation for progression. Co-Primary endpoints: OS and PFS Follow-up Period
30 PFS probability No. at risk Durvalumab Placebo PACIFIC PFS by BICR (Primary Endpoint; ITT) 1.0 (N=476) Median PFS (95% CI), 0.9 months month PFS rate (95% CI) month PFS rate (95% 0.6 CI) Durvalumab Placebo Time from randomization (months) Durvalumab Placebo (N=237) 16.8 ( ) 5.6 ( ) 55.9% ( ) 35.3% ( ) 44.2% ( ) 27.0% ( ) Stratified hazard ratio, 0.52 (95% CI, ) Two-sided P< Antonia. NEJM 2017
31 PACIFIC-Safety Summary Durvalumab (N=475) Placebo (N=234) Any-grade all-causality AEs, n (%) 460 (96.8) 222 (94.9) Grade 3/4 142 (29.9) 61 (26.1) Grade 5 21 (4.4) 13 (5.6) Leading to discontinuation 73 (15.4) 23 (9.8) Any-grade treatment-related AEs, n (%) 322 (67.8) 125 (53.4) SAEs, n (%) 136 (28.6) 53 (22.6) Any-grade immune-mediated AEs, n (%) 115 (24.2) 19 (8.1) Grade 3/4 16 (3.4) 6 (2.6) Pneumonitis (grouped terms) or radiation pneumonitis, n (%)* Durvalumab (N=475) Placebo (N=234) Any grade 161 (33.9) 58 (24.8) Grade ¾ 16 (3.4) 6 (2.6) Grade 5 5 (1.1) 4 (1.7) Leading to discontinuation The 30 Christie (6.3) NHS Foundation 10 (4.3) Trust
32 Combined CTRT Summary Concurrent CTRT is the standard of care in selected good PS patients Standard regime 60Gy in 30 fractions+platinum based chemo Immunotherapy improves PFS in stage III NSCLC. OS data awaited No consensus on the optimal CT regimen No evidence to support the addition of induction and consolidation CT to concurrent CTRT No evidence to support targeted No personalisation of the systemic or RT treatments Lim. Thorax 2010 (BTS guidelines) Bayman. Lung Cancer 2014 Vansteenkiste. Ann Oncol 2013 (ESMO guidelines)

33 Improvement in survival in last 4 decades with CTRT 10.8m 14 m 17 m 28.7m TRT RT Chemo TRT Chemo + TRT Chemo + TRT RTOG m SOCCAR 27.4 m CONCEPT 31 m IDEAL 29 m When the Okies left Oklahoma and moved to California, they raised the average intelligence level in both states
34 Stage IV
35 MDACC: Ph II Trial of local therapy & SOC vs SOC in synchronous oligo-metastatic NSCLC 49 patients Median F/U 12 mths PFS 12 vs 4 mths in favour of local consolidation (LCT) Imbalance in histology? Squamous 4% LCT vs 17% control Mut + Adeno 20% LCT vs 12% control Gomez et al Lancet Oncol 2016
36 Trials in oligometastatic disease Synchronous Untreated Distant Metastasis Untreated Primary Lesion A clinical scenario in which oligometastatic disease is detected at the time of diagnosis of the primary tumour Metachronous Oligo-Recurrent Untreated Distant Metastasis Treated Primary Lesion A clinical scenario in which the development of oligometastatic disease after treatment of the primary tumour Oligo-Progressive Uncontrolled Lesion Controlled Lesions A clinical scenario in which progression of a limited number of metastatic deposits occurs while all other metastases are controlled on systemic therapy SARON CORE HALT
, status of primary disease (absent,")
37 QUARTZ Trial Randomised Controlled Non-Inferiority Design Aim-to exclude >1 week reduction in QALYs with omission of WBRT 80% power March August 2014 Histologically proven NSCLC with brain metastases non-resectable and unsuitable for stereotactic Radiosurgery Stratification Centre, sex, PS, status of BM (progressive disease vs newly diagnosed), status of primary disease (absent, controlled, uncontrolled) R Control Arm: Optimal Supportive Care Dexamethasone + Whole Brain Radiotherapy 20Gy in 5 daily # Investigational Arm: Optimal Supportive Care Dexamethasone Primary outcome quality adjusted life years (QALYS) Weekly phone call Secondary outcomes overall survival symptom scores Subsequent / simultaneous (extra cranial) palliative RT permitted Subsequent systemic treatment permitted at clinician s discretion
 0 8 16 24 32 40 48 56 Time from randomisation (weeks) 269 144 66 32 17 11 9 5 269 141")
38 0 Average QoL At risk OSC + WBRT OSC alone QUARTZ Components of the Primary Outcome Measure Overall survival (all patients) Time from randomisation (weeks) Overall Survival Better Worse OSC+WBRT Health Utility index EuroQoL EQ-5D Time from randomisation (weeks) OSC Alone OSC+WBRT OSC Alone OSC+WBRT OSC Alone Mulvenna. Lancet 2016 OSC+WBRT OSC alone Median survival (weeks) 9.3 weeks (7.4, 10.7) 8.1 weeks (7.6, 9.0) HR 1.05 (0.89, 1.26) P-value 0.52 Quality of Life Weekly-12 weeks Then 4 weekly
39 QUARTZ Primary Outcome Measure: Quality Adjusted Life Years OSC+WBRT OSC+WBRT OSC Alone OSC Alone No clinically relevant difference Time from randomisation (weeks) QALY OSC+WBRT OSC alone Difference Mean QALY (days) 43.3 days 41.4 days -1.9 days 90% CI (Bootstrap) (-9.1, 6.6) Non-inferiority boundary -7 days OSC+WBRT OSC alone better better Aim-to exclude >1 week reduction in QALYs with omission of WBRT 80% power DAYS
40 Conclusions QUARTZ Trial Only large randomized trial of WBRT vs no WBRT for brain metastases from NSCLC WBRT does not appear to be a steroid-sparing modality Similar overall median survival (9.3 weeks vs 8.1 weeks) Similar QALYs (43.3 days vs 41.4 days) The estimate of the difference in QALYs suggests WBRT provides no additional clinically significant benefit for this group of patients However.WBRT should not disappear as a treatment option, consider WBRT in patients with favourable prognosis (TBD) Consider the changing landscape in terms of systemic treatments Khalifa. JTO 2016
41 Stage I-II Role of RT in NSCLC SABR=standard of care Stage III for peripheral disease for medically inoperable patients Concurrent CTRT =standard of care Stage IV For palliation of symptoms Oligometastatic disease (RCTs ongoing) Guidelines BTS Guidelines. Thorax 2010 EORTC guidelines. JCO 2010 ESMO guidelines. Ann Oncol 2012 ESMO consensus conference. Ann Oncol 2014 American College of Chest Physicians. Chest 2013
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Combined modality treatment for NSCLC with N2 disease
 Combined modality treatment for NSCLC with N2 disease Gerry Hanna Senior Lecturer and Consultant in Clinical Oncology Centre for Cancer Research and Cell Biology @gerryhanna E: g.hanna@qub.ac.uk Talk Outline
Combined modality treatment for NSCLC with N2 disease Gerry Hanna Senior Lecturer and Consultant in Clinical Oncology Centre for Cancer Research and Cell Biology @gerryhanna E: g.hanna@qub.ac.uk Talk Outline
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
Heterogeneity of N2 disease
 Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
ENFERMEDAD LOCALMENTE AVANZADA: Estado del Arte y Eventual Papel de las Nuevas Terapias. Dolores Isla H. Clínico Universitario Lozano Blesa ZARAGOZA
 ENFERMEDAD LOCALMENTE AVANZADA: Estado del Arte y Eventual Papel de las Nuevas Terapias Dolores Isla H. Clínico Universitario Lozano Blesa ZARAGOZA Formigal, 28 de Junio de 2018 CÓMO DEFINÍAMOS EL ESTADIO
ENFERMEDAD LOCALMENTE AVANZADA: Estado del Arte y Eventual Papel de las Nuevas Terapias Dolores Isla H. Clínico Universitario Lozano Blesa ZARAGOZA Formigal, 28 de Junio de 2018 CÓMO DEFINÍAMOS EL ESTADIO
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Treatment of LS (Stage I-III) SCLC
 SCLC") Treatment of LS (Stage I-III) SCLC Prof C Faivre-Finn Manchester Lung Cancer Group Manchester Radiation Related Research Group ESMO-The Christie Preceptorship programme on Lung Cancer 9 th March 2018 @finn_corinne
Treatment of LS (Stage I-III) SCLC Prof C Faivre-Finn Manchester Lung Cancer Group Manchester Radiation Related Research Group ESMO-The Christie Preceptorship programme on Lung Cancer 9 th March 2018 @finn_corinne
Combining chemotherapy and radiotherapy of the chest
 How to combine chemotherapy, targeted agents and radiotherapy in locally advanced NSCLC? Dirk De Ruysscher, MD, PhD Radiation Oncologist Professor of Radiation Oncology Leuven Cancer Institute Department
How to combine chemotherapy, targeted agents and radiotherapy in locally advanced NSCLC? Dirk De Ruysscher, MD, PhD Radiation Oncologist Professor of Radiation Oncology Leuven Cancer Institute Department
Radiation Therapy in SCLC. What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department
 Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
NRG Oncology Lung Cancer Portfolio 2016
 NRG Oncology Lung Cancer Portfolio 2016 Roy Decker, MD PhD Yale Cancer Center Walter J Curran, Jr, MD Winship Cancer Institute of Emory University NRG Oncology Lung Cancer Selected Discussion Stage III
NRG Oncology Lung Cancer Portfolio 2016 Roy Decker, MD PhD Yale Cancer Center Walter J Curran, Jr, MD Winship Cancer Institute of Emory University NRG Oncology Lung Cancer Selected Discussion Stage III
Adjuvant radiotherapy for completely resected early stage NSCLC
 Adjuvant radiotherapy for completely resected early stage NSCLC ESMO Preceptorship on lung Cancer Manchester March 2018 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique
Adjuvant radiotherapy for completely resected early stage NSCLC ESMO Preceptorship on lung Cancer Manchester March 2018 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
RTOG Lung Cancer Committee 2012 Clinical Trial Update. Wally Curran RTOG Group Chairman
 RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
CALGB Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer
 CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
Treatment of Stage I-III SCLC
 Treatment of Stage I-III SCLC Prof C Faivre-Finn Manchester Lung Cancer Group Manchester Radiation Related Research Group ESMO-The Christie Preceptorship programme on Lung Cancer 3 rd March 2017 @finn_corinne
Treatment of Stage I-III SCLC Prof C Faivre-Finn Manchester Lung Cancer Group Manchester Radiation Related Research Group ESMO-The Christie Preceptorship programme on Lung Cancer 3 rd March 2017 @finn_corinne
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer
 Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
What is Next for Patients with Stage III Non-Small Cell Lung Cancer?
 What is Next for Patients with Stage III Non-Small Cell Lung Cancer? Walter J Curran, Jr, MD Executive Director Winship Cancer Institute of Emory University Atlanta, GA NRG Oncology Group Chairman 1 Stage
What is Next for Patients with Stage III Non-Small Cell Lung Cancer? Walter J Curran, Jr, MD Executive Director Winship Cancer Institute of Emory University Atlanta, GA NRG Oncology Group Chairman 1 Stage
SABR. Outline. Stereotactic Radiosurgery. Stereotactic Radiosurgery. Stereotactic Ablative Radiotherapy
 CAGPO Conference October 25, 2014 Outline Stereotactic Radiation for Lung Cancer and Oligometastatic Disease What Every GPO should know Dr. David Palma, MD, MSc, PhD Radiation Oncologist, London Health
CAGPO Conference October 25, 2014 Outline Stereotactic Radiation for Lung Cancer and Oligometastatic Disease What Every GPO should know Dr. David Palma, MD, MSc, PhD Radiation Oncologist, London Health
Hot topics in Radiation Oncology for the Primary Care Providers
 Hot topics in Radiation Oncology for the Primary Care Providers Steven Feigenberg, MD Professor Chief, Thoracic Oncology Vice Chair of Clinical Research April 19, 2018 Disclosures NONE 2 Early Stage Disease
Hot topics in Radiation Oncology for the Primary Care Providers Steven Feigenberg, MD Professor Chief, Thoracic Oncology Vice Chair of Clinical Research April 19, 2018 Disclosures NONE 2 Early Stage Disease
Lung Cancer Radiotherapy
 Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
CURRENT ADVANCES IN RADIATION THERAPY
 CURRENT ADVANCES IN RADIATION THERAPY ESMO Summit Africa 2018 Suresh Senan Radiation oncologist, VU University medical center Amsterdam, The Netherlands CONFLICT OF INTEREST DISCLOSURE Research grants:
CURRENT ADVANCES IN RADIATION THERAPY ESMO Summit Africa 2018 Suresh Senan Radiation oncologist, VU University medical center Amsterdam, The Netherlands CONFLICT OF INTEREST DISCLOSURE Research grants:
Adjuvant Therapy in NSCLC. Dr.ssa Chiara Bennati Oncologia Medica S. Maria della Misericordia Perugia
 Adjuvant Therapy in NSCLC Dr.ssa Chiara Bennati Oncologia Medica S. Maria della Misericordia Perugia Agenda What do we expect today from new adjuvant chemotherapy Which data do we have with targeted agents
Adjuvant Therapy in NSCLC Dr.ssa Chiara Bennati Oncologia Medica S. Maria della Misericordia Perugia Agenda What do we expect today from new adjuvant chemotherapy Which data do we have with targeted agents
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Adjuvant Radiotherapy for completely resected NSCLC
 Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Lung cancer update 2007
 Lung cancer update 2007 HARMESH R NAIK, MD. January 24, 2007 Epidemiology (world) Estimated 1.35 million new cases in world in 2002 Estimated 1.179 million deaths in world in 2002 Common cancer diagnosis
Lung cancer update 2007 HARMESH R NAIK, MD. January 24, 2007 Epidemiology (world) Estimated 1.35 million new cases in world in 2002 Estimated 1.179 million deaths in world in 2002 Common cancer diagnosis
Combined Chemotherapy and Radiation Therapy for Locally Advanced NSCLC
 Combined Chemotherapy and Radiation Therapy for Locally Advanced NSCLC George R. Blumenschein, Jr., MD Associate Professor of Medicine Department of Thoracic/Head & Neck Medical Oncology The University
Combined Chemotherapy and Radiation Therapy for Locally Advanced NSCLC George R. Blumenschein, Jr., MD Associate Professor of Medicine Department of Thoracic/Head & Neck Medical Oncology The University
Casi clinici di integrazione multiprofessionale: NSCLC stadio III. Biagio Ricciuti. Scuola di Specializzazione in Oncologia Medica
 Casi clinici di integrazione multiprofessionale: NSCLC stadio III Scuola di Specializzazione in Oncologia Medica Università degli Studi di Perugia Outline Standard treatment Open questions Clinical cases
Casi clinici di integrazione multiprofessionale: NSCLC stadio III Scuola di Specializzazione in Oncologia Medica Università degli Studi di Perugia Outline Standard treatment Open questions Clinical cases
Surgery versus stereotactic body radiation therapy in medically operable NSCLC
 Surgery versus stereotactic body radiation therapy in medically operable NSCLC David H Harpole Jr, MD Professor of Surgery Associate Professor in Pathology Vice Chief, Division of Surgical Services Duke
Surgery versus stereotactic body radiation therapy in medically operable NSCLC David H Harpole Jr, MD Professor of Surgery Associate Professor in Pathology Vice Chief, Division of Surgical Services Duke
STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY?
 STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY? MICHAEL LANUTI, MD American Association of Thoracic Surgeons Minneapolis, MN 2013 STAGE I INOPERABLE NSCLC RADIOFREQUENCY
STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY? MICHAEL LANUTI, MD American Association of Thoracic Surgeons Minneapolis, MN 2013 STAGE I INOPERABLE NSCLC RADIOFREQUENCY
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We
 Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
Allan Price NHS Lothian, Edinburgh, UK
 Allan Price NHS Lothian, Edinburgh, UK Radiotherapy Dose Volume Timing Technique PCI Surgery Systemic agents 1 Study Dose Time Induction CT Ann Arbor 65.1-75.6 Gy Duke 73.6-80 Gy RTOG 77.4 Gy 74 Gy 6.5-7.5
Allan Price NHS Lothian, Edinburgh, UK Radiotherapy Dose Volume Timing Technique PCI Surgery Systemic agents 1 Study Dose Time Induction CT Ann Arbor 65.1-75.6 Gy Duke 73.6-80 Gy RTOG 77.4 Gy 74 Gy 6.5-7.5
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery
 Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer
 Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
Reirradiazione. La radioterapia stereotassica ablativa: torace. Pierluigi Bonomo Firenze
 Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Chemo-radiotherapy in non-small cell lung cancer. HARMESH R NAIK, MD. September 25, 2002
 Chemo-radiotherapy in non-small cell lung cancer HARMESH R NAIK, MD. September 25, 2002 Epidemiology Estimated 170000 new cases Estimated 157,000 deaths Second commonest cancer diagnosis in men and women
Chemo-radiotherapy in non-small cell lung cancer HARMESH R NAIK, MD. September 25, 2002 Epidemiology Estimated 170000 new cases Estimated 157,000 deaths Second commonest cancer diagnosis in men and women
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Non small cell Lung Cancer
 Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
Ruolo emergente dell immunoterapia nello stadio III. Giulia Pasello Medical Oncology 2 Veneto Cancer Institute, Padua (Italy)
") Ruolo emergente dell immunoterapia nello stadio III Giulia Pasello Medical Oncology 2 Veneto Cancer Institute, Padua (Italy) Disclosures Advisory Boards / Honoraria / Speakers fee / Consultant for: MSD,
Ruolo emergente dell immunoterapia nello stadio III Giulia Pasello Medical Oncology 2 Veneto Cancer Institute, Padua (Italy) Disclosures Advisory Boards / Honoraria / Speakers fee / Consultant for: MSD,
Radiotherapy in NSCLC: What are the ESMO Guidelines?
 - The role of radiation in early stage - RT/CT for unresectable NSCLC - Brain metastasis - Oligometastatic disease Radiotherapy in NSCLC: What are the ESMO Guidelines? Jean-Yves DOUILLARD MD PhD Chief
- The role of radiation in early stage - RT/CT for unresectable NSCLC - Brain metastasis - Oligometastatic disease Radiotherapy in NSCLC: What are the ESMO Guidelines? Jean-Yves DOUILLARD MD PhD Chief
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali
 Dr Raj K Shrimali") Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Place de la radiothérapie dans les CBPC métastatiques
 Place de la radiothérapie dans les CBPC métastatiques Cecile Le Péchoux, 12 ème Biennale Monégasque de Cancérologie, 2016 IOT Institut d Oncologie Thoracique CBPC metastatique Rapid doubling time, early
Place de la radiothérapie dans les CBPC métastatiques Cecile Le Péchoux, 12 ème Biennale Monégasque de Cancérologie, 2016 IOT Institut d Oncologie Thoracique CBPC metastatique Rapid doubling time, early
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Estado actual del tratamiento neoadyuvante y adyuvante a la cirugía en estadios iniciales de cáncer de pulmón no microcítico
 Estado actual del tratamiento neoadyuvante y adyuvante a la cirugía en estadios iniciales de cáncer de pulmón no microcítico Enriqueta Felip Vall d Hebron University Hospital Barcelona, Spain Stage I-II
Estado actual del tratamiento neoadyuvante y adyuvante a la cirugía en estadios iniciales de cáncer de pulmón no microcítico Enriqueta Felip Vall d Hebron University Hospital Barcelona, Spain Stage I-II
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Single Technology Appraisal (STA)
") Single Technology Appraisal (STA) Durvalumab for maintenance treatment of locally advanced unresectable non-small cell lung cancer that has not progressed after platinum-based chemoradiation therapy Response
Single Technology Appraisal (STA) Durvalumab for maintenance treatment of locally advanced unresectable non-small cell lung cancer that has not progressed after platinum-based chemoradiation therapy Response
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf
 MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
Adjuvant Chemotherapy
 State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016
 Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Critical Clinical Updates
 Critical Clinical Updates ASTRO Spring Refresher Course JW Marriott Hotel Ramesh Rengan MD PhD Department of Radiation Oncology Friday March 22, 2013 Learning Objectives At the conclusion of this activity,
Critical Clinical Updates ASTRO Spring Refresher Course JW Marriott Hotel Ramesh Rengan MD PhD Department of Radiation Oncology Friday March 22, 2013 Learning Objectives At the conclusion of this activity,
Thoracic and head/neck oncology new developments
 Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Utility of 18 F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer
 Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Locally Advanced NSCLC and its management in the Elderly. Dr Laura Pemberton Consultant Clinical Oncologist, Christie Hospital, UK
 Locally Advanced NSCLC and its management in the Elderly Dr Laura Pemberton Consultant Clinical Oncologist, Christie Hospital, UK Topics covered Concurrent Chemoradiotherapy (concrt) in elderly Radiotherapy
Locally Advanced NSCLC and its management in the Elderly Dr Laura Pemberton Consultant Clinical Oncologist, Christie Hospital, UK Topics covered Concurrent Chemoradiotherapy (concrt) in elderly Radiotherapy
TREATMENT DELIVERY AND CLINICAL EVIDENCE FOR THE TREATMENT OF OLIGOMETASTASIS
 TREATMENT DELIVERY AND CLINICAL EVIDENCE FOR THE TREATMENT OF OLIGOMETASTASIS Dr Gerry Hanna Clinical Senior Lecturer in Radiation Oncology Centre for Cancer Research and Cell Biology Queens University
TREATMENT DELIVERY AND CLINICAL EVIDENCE FOR THE TREATMENT OF OLIGOMETASTASIS Dr Gerry Hanna Clinical Senior Lecturer in Radiation Oncology Centre for Cancer Research and Cell Biology Queens University
Debate on stage III NSCLC: The role of systemic therapy
 1 Debate on stage III NSCLC: The role of systemic therapy Rolf Stahel University Hospital of Zürich Bucharest, 16.6..2015 2 Stage III disease: The problem of heterogeneity, the risk of distant metastases
1 Debate on stage III NSCLC: The role of systemic therapy Rolf Stahel University Hospital of Zürich Bucharest, 16.6..2015 2 Stage III disease: The problem of heterogeneity, the risk of distant metastases
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer. Doug Rahn 6/1/12
 Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Debate 1 Are treatments for small cell lung cancer getting better? No:
 Debate 1 Are treatments for small cell lung cancer getting better? No: Taofeek Owonikoko, MD, PhD Associate Professor Department of Hematology & Medical Oncology Winship Cancer Institute of Emory University
Debate 1 Are treatments for small cell lung cancer getting better? No: Taofeek Owonikoko, MD, PhD Associate Professor Department of Hematology & Medical Oncology Winship Cancer Institute of Emory University
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer
: Targeting Lung Cancer") Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
REVIEW ARTICLE. Hyperfractionated and accelerated radiotherapy in non-small cell lung cancer
 REVIEW ARTICLE Hyperfractionated and accelerated radiotherapy in non-small cell lung cancer Kate Haslett 1, Christoph Pöttgen 2, Martin Stuschke 2, Corinne Faivre-Finn 1,3 1 Radiotherapy Related Research,
REVIEW ARTICLE Hyperfractionated and accelerated radiotherapy in non-small cell lung cancer Kate Haslett 1, Christoph Pöttgen 2, Martin Stuschke 2, Corinne Faivre-Finn 1,3 1 Radiotherapy Related Research,
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Professor and Head Division of Radiation Oncology Stellenbosch University and Tygerberg Hospital Cape Town South Africa
 STAGE III NONSMALL CELL LUNG CANCER TREATMENT APPROACHES WE LIKE TO PRACTICE... ALMOST UNETHICALLY Branislav Jeremic, MD, PhD Professor and Head Division of Radiation Oncology Stellenbosch University and
STAGE III NONSMALL CELL LUNG CANCER TREATMENT APPROACHES WE LIKE TO PRACTICE... ALMOST UNETHICALLY Branislav Jeremic, MD, PhD Professor and Head Division of Radiation Oncology Stellenbosch University and
Radiotherapy in NSCLC: State-of-the-art
 Radiotherapy in NSCLC: State-of-the-art Prof. Dirk De Ruysscher, MD, PhD Radiation Oncologist Maastro clinic, Maastricht University Medical Center, GROW Maastricht The Netherlands Disclosure Advisory board
Radiotherapy in NSCLC: State-of-the-art Prof. Dirk De Ruysscher, MD, PhD Radiation Oncologist Maastro clinic, Maastricht University Medical Center, GROW Maastricht The Netherlands Disclosure Advisory board
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Erlotinib for the third or fourth-line treatment of NSCLC January 2012
 Disease background LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Erlotinib for the third or fourth-line treatment of NSCLC January 2012 Lung cancer is the second most common cancer in the UK (after breast),
Disease background LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Erlotinib for the third or fourth-line treatment of NSCLC January 2012 Lung cancer is the second most common cancer in the UK (after breast),
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Palliative treatments for lung cancer: What can the oncologist do?
 Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Radical treatment of synchronous oligometastatic non-small cell lung carcinoma (NSCLC): patient outcomes and prognostic factors
: patient outcomes and prognostic factors") Chapter 6 Radical treatment of synchronous oligometastatic non-small cell lung carcinoma (NSCLC): patient outcomes and prognostic factors Gwendolyn H.M.J. Griffioen 1, Daniel Toguri 2, Max Dahele 1, Andrew
Chapter 6 Radical treatment of synchronous oligometastatic non-small cell lung carcinoma (NSCLC): patient outcomes and prognostic factors Gwendolyn H.M.J. Griffioen 1, Daniel Toguri 2, Max Dahele 1, Andrew
Disclosures. Preoperative Treatment: Chemotherapy or ChemoRT? Adjuvant chemotherapy helps. so what about chemo first?
 Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Systemic Management of Malignant Pleural Mesothelioma
 ESO-ESMO EASTERN EUROPE AND BALKAN REGION MASTERCLASS IN MEDICAL ONCOLOGY 15.June-19.June 2018 Belgrade, Serbia Systemic Management of Malignant Pleural Mesothelioma Dragana Jovanovic University Hospital
ESO-ESMO EASTERN EUROPE AND BALKAN REGION MASTERCLASS IN MEDICAL ONCOLOGY 15.June-19.June 2018 Belgrade, Serbia Systemic Management of Malignant Pleural Mesothelioma Dragana Jovanovic University Hospital