Non small cell Lung Cancer
|
|
|
- Walter Morton
- 5 years ago
- Views:
Transcription

1 Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
2 Outline Screening Staging and investigation Management by stages (NSCLC) ES-NSCLC LA-NSCLC Radiation techniques
3 Screening for lung cancer Why? High morbidity and mortality identified risk factors allowing targeted screening for high risk therapy is more effective in early stage disease J Thorac Oncol 2007; 2:706
4 Screening for lung cancer Annual chest X-ray Biannual chest X-ray Annual chest X-ray plus sputum cytology No benefit to reduce mortality rate in lung cancer
5 Screening for lung cancer National Lung Screening Trial: low-dose chest CT scanning VS. chest x-ray for 3 years High risk population: age years with history of at least 30 pack-years of smoking included current smokers and discontinued smoking within 15 years of enrollment Low dose CT Chest X-ray Positive test 24.2% 6.9% False positive 96.4% 94.5% Death (per 100,000 person-yr) Relative reduction in mortality 20.0% (95% CI, 6.8 to 26.7; P=0.004) N Engl J Med. 2011;365(5):395.
6 Pretreatment evaluation Complete blood count Serum electrolytes, calcium LFT: alkaline phosphatase, albumin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin Creatinine Pulmonary function test (PFT) Counseling smoking cessation
7 Staging for lung cancer CT chest (including liver and adrenal glands) with contrast Tumor: tumor size, separated nodules, atelectasis, invasion adjacent structure Mediastinal LN: sensitivity 51% specificity 86% Most area: normal mediastinal LN size < 10 mm. but subcarinal LN size mm. Rare area: retrocrural region, para-aortic region, or pericardial fat If LN. > 8 mm. suspected pathologic nodes Chest. 2007;132(3 Suppl):178S.
8 Staging for lung cancer Positron emission tomography/ct (PET/CT) sensitivity 91%, specificity 86 % (Petterman RM, NEJM 2000) Good negative predictive value PET/CT for contouring change radiation portal 35-62% (most mediastinum LN) False negative: Lesion less than 1 cm, DM, During 1st week after chemotherapy
9 Staging for lung cancer Bone scan Imaging brain: MRI or CT Suspected mediastinal LN from imaging Mediatinoscopy Mediastinotomy EBUS with biopsy
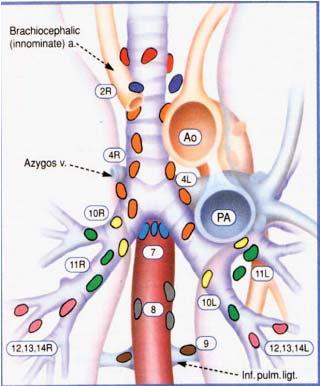
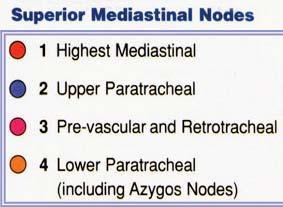
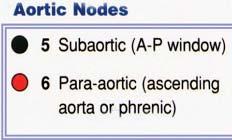
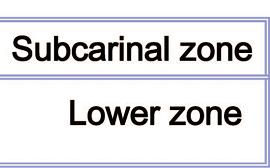
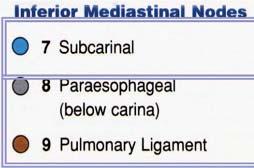
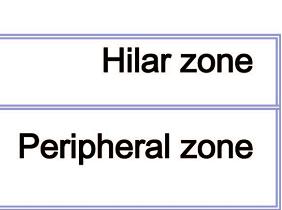
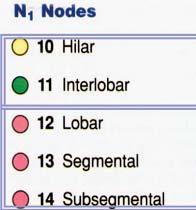
10 Mediastinal LN: Station J Thorac Oncol. 2007;2:
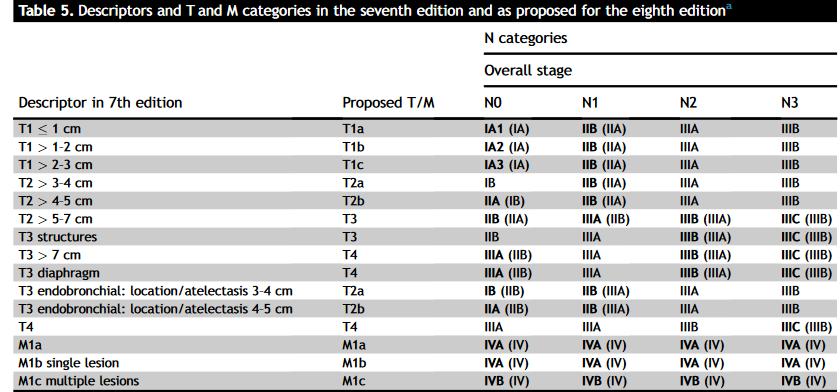
11 Update 8 th edition AJCC 7 th edition T0 : No evidence of primary tumor Tis : Carcinoma in situ T1 : Tumor 3 cm, surrounded by lung or visceral pleura, without bronchoscopic evidence of invasion more proximal than the lobar bronchus T1a : Tumor 2 cm T1b : Tumor 2- (<) 3 cm 8 th edition o T0: No evidence of primary tumor o Tis: Carcinoma in situ o T1 : Tumor 3 cm, surrounded by lung or visceral pleura, without bronchoscopic evidence of invasion more proximal than the lobar bronchus o T1a(mi): Minimally invasive adenocarcinoma** o T1a : Tumor 1 cm o T1b : Tumor 1- (<) 2 cm o T1c : Tumor 2- (<) 3 cm **Solitary adenocarcinoma, < 3cm with a predominately lepidic pattern and < 5mm invasion in any one focus
12 Update 8 th edition AJCC 7 th edition T2 : Tumor 3 (<) 7 cm with involves main bronchus, > 2 cm distal to the carina; invades visceral pleura (PL1 or PL2); associated with atelectasis or obstructive pneumonitis that extends to the hilar region but does not involve the entire lung T2a : Tumor 3 - (<) 5 cm T2b : Tumor 5 - (<) 7 cm 8 th edition o T2 : Tumor 3 (<) 5 cm with involves main bronchus not carina, > 2 cm distal to the carina; invades visceral pleura (PL1 or PL2); Associated with atelectasis or obstructive pneumonitis that extends to the hilar region, involving part or all of the lung o T2a : Tumor 3 - (<) 4 cm o T2b : Tumor 4 - (<) 5 cm
13 Update 8 th edition AJCC T2 7 th edition T3 : Tumor > 7 cm or one that directly invades any of the following: parietal pleural (PL3), chest wall (including superior sulcus tumors), diaphragm, phrenic nerve, mediastinal pleura, parietal pericardium; tumor in the main bronchus < 2 cm distal to the carina but without involvement of the carina associated atelectasis or obstructive pneumonitis of the entire lung separate tumor nodule(s) in the same lobe 8 th edition o T3: Tumor 5 (<) 7 cm or associated with o directly invades any of the following structures: chest wall (including the parietal pleura and superior sulcus tumors), phrenic nerve,parietal pericardium o separate tumor nodule(s) in the same lobe as the primary tumor
14 Update 8 th edition AJCC 7 th edition T4 : Tumor of any size that invades any of the following: mediastinum, heart, great vessels, trachea, recurrent laryngeal nerve, esophagus vertebral body Carina separate tumor nodule(s) in a different ipsilateral lobe 8 th edition o T4: Tumor > 7 cm or associated with o separate tumor nodule(s) in a different ipsilateral lobe than that of the primary tumor o invades any of the following structures: diaphragm, mediastinum, heart, great vessels, trachea, recurrent laryngeal nerve, esophagus, vertebral body, and carina
15 Update 8 th edition AJCC 7 th edition No changes 8 th edition NX : Regional lymph nodes cannot be assessed N0 : No regional lymph node metastases N1 : Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes, including involvement by direct extension N2 : Metastasis in ipsilateral mediastinal and/or subcarinal lymph node(s) N3 : Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s) o o o o o NX : Regional lymph nodes cannot be assessed N0 : No regional lymph node metastases N1 : Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes, including involvement by direct extension N2 : Metastasis in ipsilateral mediastinal and/or subcarinal lymph node(s) N3 : Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s)
16
17 Update 8 th edition AJCC 7 th edition M0 : No distant metastasis M1 : Distant metastasis M1a : Separate tumor nodule(s) in a contralateral lobe, tumor with pleural nodules or malignant pleural (or pericardial) effusion M1b : Distant metastasis (in extrathoracic organs) 8 th edition o M0: No distant metastasis o M1: Distant metastasis present o M1a: Separate tumor nodule(s) in a contralateral lobe; tumor with pleural or pericardial nodule(s)or malignant pleural or pericardial effusion o M1b: Single extrathoracic metastasis o M1c: Multiple extrathoracic metastases in one or more organs
18
19 Treatment of Non-small cell lung cancer - ES-NSCLC - LA-NSCLC
20 Treatment of Non-small cell lung cancer - ES-NSCLC: Surgical candidate case Medically inoperable case
21 Early stages: stage I or II Surgery is standard treatment for patients with clinical stage I and II Primary Lung mass Lobectomy: Standard procedure Open thoracotomy Video-assisted thoracoscopic surgery (VATS) Sublobar resection: Segmentectomy or wedge resection Compromised pulmonary function, advanced age, extensive comorbidity Limited tumor < 3 cm.
22 Early stages: Lobectomy VS. Sublobar resection Loco-regional free survival Increased50% 5 yrs OS Lobectomy 65% VS. Sublobar resection 45% Ongoing study: CALGB (NCT ) Lobectomy VS. Sublobar resection in peripheral tumors 2 cm (stage IA) Ann Thorac Surg 1995;60:615-23
23 Early stages: stage I or II Mediastinal LN surgery Systemic mediastinal lymph node dissection Sampling mediastinal lymph node Right: 2R, 4R, 7, and 10R Cochrane meta-analysis Left: 5, 6, 7, and 10L European Society of Thoracic Surgeons guidelines recommended systematic lymph node dissection in all cases T h e Cochran e Li brar y 2010, Issue 4

24 Complete resection from NCCN Complete resection requires: free resection margins + Systematic node dissection or sampling + highest mediastinal node negative for tumor
25 Treatment of Non-small cell lung cancer - ES-NSCLC: Surgical candidate case Medically inoperable case
26 Stereotactic Body RadioTherapy (SBRT) Stereotactic ABlative Radiotherapy (SABR) = high dose radiation per day (> 10 Gy) = small number of fraction (< 5 fractions)
27
28 Medically inoperable stage I non-small cell lung cancer
29 Outcome: SBRT/SABR Authors Patient Dose(Gy) Stage 3 yr Local Control (%) Prospective SBRT trials 3 yr Overall Survival (%) 5 yr OS 5 yr LC Baumann Gy x 3F IA/B %, 79% Fakiris Gy x 3F IA/B Koto Gy x 3F 7.5 Gy x 8F IA/B/IIA T1: 78 T2: 40 Systematic review: 5-yr OS 40% (17-83%) 5-yr LC 90% (83-95%) Ricardi 15 Gy x 3F IA/B Timmerman Gy x 3F IA/B/IIA %, 62% Nagata Gy x 4F IA/B Retrospective SBRT studies Nyman Gy x 3F IA/B Onishi Gy x 1- IA/B F Timmerman Gy x 3F IA/B 95 (2 yr) 55 (2yr) Uematsu Gy x 10F IA/B 94 (2 yr) 66 (2 yr) 72


30 Peripheral location Central location Radiotherapy dose 18 Gy x 3 fractions

31 70 patients treated with SBRT: develop five (7%) grade 5 toxicity (3 pneumonia, 1 hemoptysis, 1 respiratory failure)
32 ASCO recommendation Delivery of SBRT in more than 3 (ie, 4 or 5 ) fractions may reduce the risk of severe toxicity. For central tumors for which SBRT is deemed too high-risk (eg, tumors directly abutting or invading the esophagus or proximal bronchial tree), hypofractionated radiotherapy utilizing 6-15 fractions or conventionally fractionated radiotherapy may be considered.
33 Medically operable ESNSCLC - Standard operative risk - High operative risk

34 Criticize Under power to test benefit of SBRT Thoracotomy surgery Chang 2015
35 Overall survival Lobectomy SBRT 59% 29% SBRT: excluded medically inoperative patients Rosen 2016
36 ASCO recommendation Standard operative risk and stage I NSCLC, SBRT is not recommended as an alternative to surgery outside of a clinical trial. For this population, lobectomy with systematic mediastinal/hilar lymph node evaluation remains the recommended treatment, though a sublobar resection may be considered in select clinical scenarios.

37 Median FU: 2.9 yr SBRT Surgery HR: 1.92 ( ), P,.001 OS: video-assisted thoracoscopic resection vs SBRT Paul 2016
38 ASCO recommendation High operative risk: cannot tolerate lobectomy, but are candidates for sublobar resection SBRT as a potential alternative to surgery are encouraged within the multidisciplinary cancer care team. In cases where SBRT is offered, patients should be informed that while SBRT may have decreased risks from treatment in the short term, the longer-term outcomes > 3 years are not wellestablished.
39 Summary1: role of SBRT in ES-NSCLC Medically inoperable ES-NSCLC SBRT as standard of care Medically operable ES-NSCLC: high risk patient SBRT as alternative treatment to surgery Medically operable ES-NSCLC: standard risk patient SBRT is not recommended
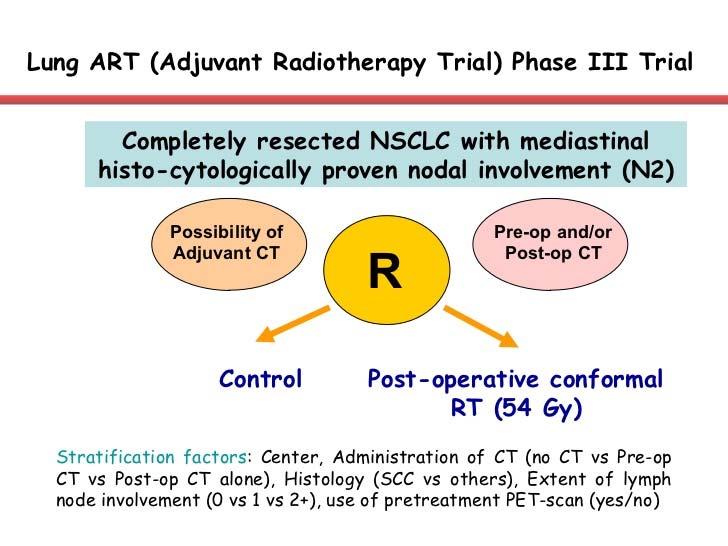
40 Postoperative RT
41 Retrospective ANITA trial N1 N2 Median OS (yr) No CMT CMT No RT RT Median OS (yr) No CMT CMT No RT RT Int. J. Radiation Oncology Biol. Phys., 2008
42 Criticize for PORT meta-analysis 25% patients had T1N0 disease Initial staging inadequate by today s standards Cobalt 60 used in 4 trial (5 yr survival Co-60 8% vs 30% for Mev) Conventional RT High dose (60Gy) and fractionation (up to 3.0 Gy/Fx) PORT meta-analysis 2005
43
44 Complete resected N2 Lymph node sampling or systematic dissection of lymph nodes RUL/RML: levels 2, 4 and 7 RLL: levels 4, 7, 8 and 9 LUL: levels 5, 6 and 7 LLL: levels 7, 8 and 9 3 intrapulmonary and hilar nodes at least 3 nodes from mediastinal nodes
45 Summary 2: PORT Complete node resection N0-1: no role of PORT N2: controversy Incomplete resection R1/2: PORT
46 Treatment of Non-small cell lung cancer - LA-NSCLC
47 LA-NSCLC: operable case - Trimodality - Definite CCRT
48 Induction CCRT+Sx VS CCRT Intergroup INT-0139 (RTOG 93-09, SWOG 93-36) stage IIIA (pn2) NSCLC Cisplatin/Etoposide +RT 45Gy/25F Radical surgery Consolidation CMT Cis+Eto 396 patients Cisplatin/Etoposide +RT 61Gy Consolidation CMT Cis+Eto Pattern Failure PFS Preop CCRT Definite OS CCRT Primary tumor 2% 14% Regional LN 7% 3% Brain metastasis 11% 15% Distant metastasis 37% 42% Albain KS, The Lancet 2009
49 Induction CCRT+Sx VS CCRT Intergroup INT-0139 (RTOG 93-09, SWOG 93-36) Lobectomy Pneumonectomy Pathological N0 surrogate for better 5 yr OS Albain KS, The Lancet 2009

50 German GLCCG Stage IIIA-B NSCLC 524 patients Cisplatin+Etoposide 3 cycle Cisplatin+Etoposide 3 cycle RT 45Gy/30 F bid plus carboplatin Surgery surgery Postoperative RT Overall survival and Progression free survival: not difference Pneumonectomy after induction treatment increase mortality Thomas M, Lancet Oncol. 2008
51 Summary 3: Operable LA-NSCLC Trimodality Preoperative CCRT Lobectomy + node dissection Preoperative CMT Lobectomy + node dissection PORT Definitive CCRT
52 Inoperable LA-NSCLC
53 Concurrent CMT-RT VS Sequential CMT RT





54 RTOG 9410 Medically or surgically inoperable AJCC stage II, IIIA, or IIIB 595 pts Arm I 2 cycles of CDDP + VBL Arm II CMT-RT63 Gy, 2 Gy/F Arm III CMT-RT69.6 Gy, 1.2 Gy/f, bid RT 63 Gy, 2 Gy/F Median OS 17 mo 5 yr OS 16% Median OS 15.6 mo 5 yr OS 13% Median OS 14.6 mo 5 yr OS 10% Curran W et al. J Natl Cancer Inst. 2011
55 NSCLC Collaborative Group Meta-analysis: individual patients data of 6 trials (CALGB 8831, WJLCG, RTOG 9410, GMMA Ankara, GLOT-GFPC NPC 95-01, EORTC 08972) OS absolute benefit at 3-years of 5.7% (18% to 24%), 5-years 4.5% (11% to 15%) Auperin A, J Clin Oncol 2010
56 Concurrent CMT-RT + Induction CMT


57 Vokes EE, J Clin Oncol. 2007
58 CALGB B39801 Conclusion: addition of induction chemo added toxicity without survival benefit
59 RT alone

60 Very accelerated RT: shortening of the total duration > 50% Moderately accelerated RT: shortening of the total duration 15-50% Hyperfractionated RT with identical total dose Hyperfractionated RT with increased total dose.
61 absolute benefit of 2.5% (8.3% to 10.8%) at 5 years
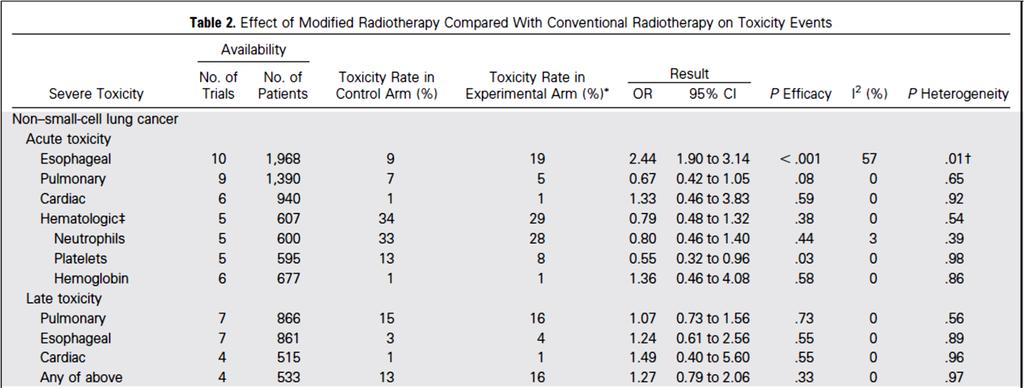
62 Toxicity
63 Summary 4: Inoperable LA-NSCLC Definitive CCRT Sequential CMT RT RT alone: Conventional fraction, altered/hyperfractionation
64 Radiation Technique - Volume - Dose - Technique
65 Volume of RT Recommended Involve-field radiotherapy RCTs from Shangdong et al IFRT ENI RT dose Gy Gy Local control 51% 36% RP 17% 29% ENF 7% 4% MSKCC: evaluated 524 pts. Elective node failure (ENF) 6% Lung Cancer Aug;41(2):
66 Radiation dose Recommended dose: Gy RTOG 7301 (Conventional RT): randomly escalated dose 40, 50, 60 Gy Local control 52%, 62%, 73% Standard dose: 60 Gy Michigan escalated dose: RT alone with 3D-CRT/ IFRT 5-yr OS 4% (63-69 Gy), 22% (74-84 Gy), and 28% ( Gy). 5-yr LRC 12%, 35%, and 49% Int J Radiat Oncol Biol Phys. 1986;12(4):539.


67 Stage IIIA: 60% AdenoCA ~ SCC 58% 44%

68 Local failure and Distant metastasis

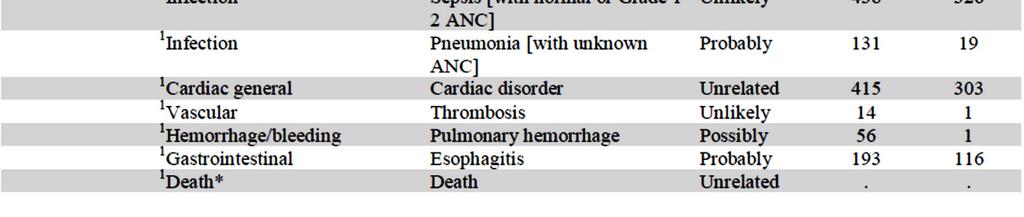
69 Treatment related death

70


71 Lung Heart
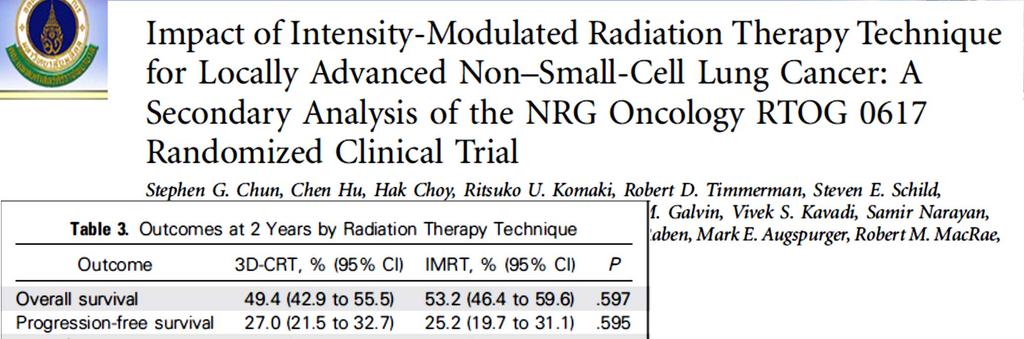
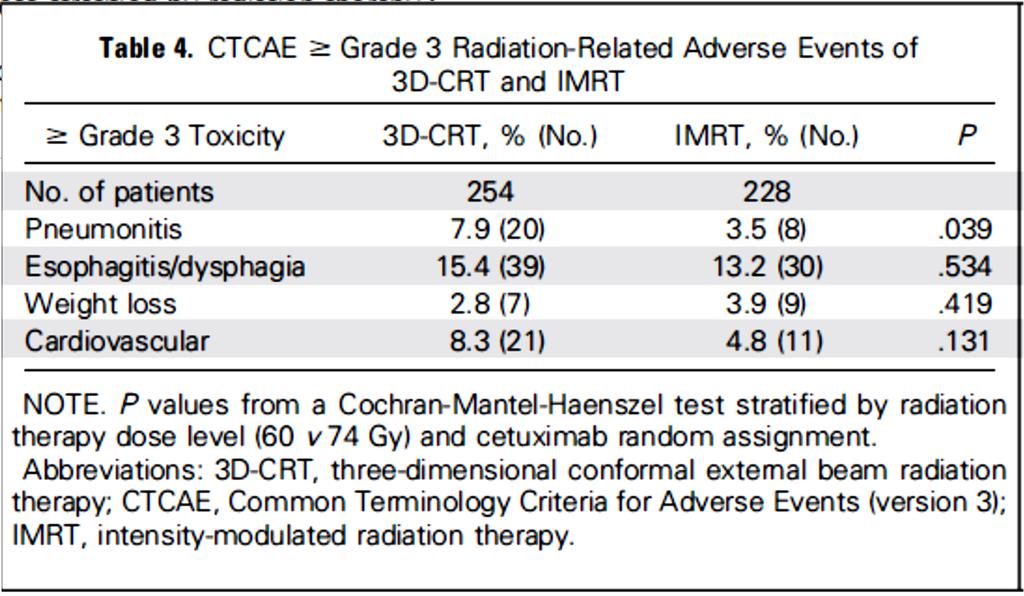
72 G3 Radiation pneumonitis Local failure G3 RP IMRT 6.5% vs PSPT 10.5%

73
74 Q & A
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer. Doug Rahn 6/1/12
 Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Lung 8/7/14. Collecting Cancer Data: Lung NAACCR Webinar Series. August 7, 2014
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY?
 STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY? MICHAEL LANUTI, MD American Association of Thoracic Surgeons Minneapolis, MN 2013 STAGE I INOPERABLE NSCLC RADIOFREQUENCY
STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY? MICHAEL LANUTI, MD American Association of Thoracic Surgeons Minneapolis, MN 2013 STAGE I INOPERABLE NSCLC RADIOFREQUENCY
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Disclosures. Preoperative Treatment: Chemotherapy or ChemoRT? Adjuvant chemotherapy helps. so what about chemo first?
 Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
NAACCR Webinar Series 1
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
LONG-TERM SURGICAL OUTCOMES OF 1018 PATIENTS WITH EARLY STAGE NSCLC IN ACOSOG Z0030 (ALLIANCE) TRIAL
 TRIAL") LONG-TERM SURGICAL OUTCOMES OF 1018 PATIENTS WITH EARLY STAGE NSCLC IN ACOSOG Z0030 (ALLIANCE) TRIAL Stacey Su, MD; Walter J. Scott, MD; Mark S. Allen, MD; Gail E. Darling, MD; Paul A. Decker, MS; Robert
LONG-TERM SURGICAL OUTCOMES OF 1018 PATIENTS WITH EARLY STAGE NSCLC IN ACOSOG Z0030 (ALLIANCE) TRIAL Stacey Su, MD; Walter J. Scott, MD; Mark S. Allen, MD; Gail E. Darling, MD; Paul A. Decker, MS; Robert
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard
 Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Lung /1/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
ACOSOG Thoracic Committee. Kemp H. Kernstine, MD PhD
 ACOSOG Thoracic Committee Kemp H. Kernstine, MD PhD ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy Govindan, M.D. Carolyn Reed, MD
ACOSOG Thoracic Committee Kemp H. Kernstine, MD PhD ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy Govindan, M.D. Carolyn Reed, MD
VATS after induction therapy: Effective and Beneficial Tips on Strategy
 VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Lung Cancer. Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD
 Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Lung Cancer Staging: The Revised TNM Classification
 Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
WHITE PAPER - SRS for Non Small Cell Lung Cancer
 WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System
 Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI
 EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Surgery for early stage NSCLC
 1-3 March 2017, Manchester, UK Surgery for early stage NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France what
1-3 March 2017, Manchester, UK Surgery for early stage NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France what
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
LungStage. Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies
 LungStage Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies Medical Team: Bram Stieltjes, MD PhD; Alex Sauter, MD; Gregor Sommer, MD;
LungStage Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies Medical Team: Bram Stieltjes, MD PhD; Alex Sauter, MD; Gregor Sommer, MD;
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Surgical management of lung cancer
 Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD
 Alliance Thoracic Committee Kemp H. Kernstine, MD PhD") ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD 7-12-12 ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy
ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD 7-12-12 ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Medically inoperable stage I non-small cell lung cancer: best practices and long-term outcomes
 Review Article Medically inoperable stage I non-small cell lung cancer: best practices and long-term outcomes J. Isabelle Choi Department of Radiation Oncology, University of Maryland, Baltimore, MD, USA
Review Article Medically inoperable stage I non-small cell lung cancer: best practices and long-term outcomes J. Isabelle Choi Department of Radiation Oncology, University of Maryland, Baltimore, MD, USA
Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer. Quick Reference Chart and Diagrams
 CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
ESMO Preceptorship Programme NSCLC Singapore 15 November 2017
 ESMO Preceptorship Programme NSCLC Singapore 15 November 2017 State of the art: Standard of care for resectable NSCLC Adjuvant chemotherapy Is there a place for neo-adjuvant chemotherapy? Pr Jaafar BENNOUNA
ESMO Preceptorship Programme NSCLC Singapore 15 November 2017 State of the art: Standard of care for resectable NSCLC Adjuvant chemotherapy Is there a place for neo-adjuvant chemotherapy? Pr Jaafar BENNOUNA
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Is the Neo-adjuvant Approach Better than Adjuvant Approach? Comparative Levels of Evidence: Randomized Trials
 Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
HISTORY SURGERY FOR TUMORS WITH INVASION OF THE APEX 15/11/2018
 30 EACTS Annual Meeting Barcelona, Spain 1-5 October 2016 SURGERY FOR TUMORS WITH INVASION OF THE APEX lung cancer of the apex of the chest involving any structure of the apical chest wall irrespective
30 EACTS Annual Meeting Barcelona, Spain 1-5 October 2016 SURGERY FOR TUMORS WITH INVASION OF THE APEX lung cancer of the apex of the chest involving any structure of the apical chest wall irrespective
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL
 LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
According to the current International Union
 Treatment of Stage II Non-small Cell Lung Cancer* Walter J. Scott, MD, FCCP; John Howington, MD, FCCP; and Benjamin Movsas, MD Based on clinical assessment alone, patients with stage II non-small cell
Treatment of Stage II Non-small Cell Lung Cancer* Walter J. Scott, MD, FCCP; John Howington, MD, FCCP; and Benjamin Movsas, MD Based on clinical assessment alone, patients with stage II non-small cell
Radiation Therapy in SCLC. What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department
 Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
RTOG Lung Cancer Committee 2012 Clinical Trial Update. Wally Curran RTOG Group Chairman
 RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
Lung Cancer Clinical Guidelines: Surgery
 Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
Dr. Andres Wiernik. Lung Cancer
 Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
11/21/ M with LUL Mass Case Presentation / Round Table Discussion. Multiple-choice question What stage is this tumor?
 MS 62M with LUL Mass Case Presentation / Round Table Discussion Dr. Jasleen Kukreja and Johannes Kratz Department of Thoracic Surgery University of California, San Francisco 62M, presented to clinic 6/2009
MS 62M with LUL Mass Case Presentation / Round Table Discussion Dr. Jasleen Kukreja and Johannes Kratz Department of Thoracic Surgery University of California, San Francisco 62M, presented to clinic 6/2009
N.E. Verstegen A.P.W.M. Maat F.J. Lagerwaard M.A. Paul M.I. Versteegh J.J. Joosten. W. Lastdrager E.F. Smit B.J. Slotman J.J.M.E. Nuyttens S.
 N.E. Verstegen A.P.W.M. Maat F.J. Lagerwaard M.A. Paul M.I. Versteegh J.J. Joosten W. Lastdrager E.F. Smit B.J. Slotman J.J.M.E. Nuyttens S.Senan Submitted 10 Salvage surgery for local failures after stereotactic
N.E. Verstegen A.P.W.M. Maat F.J. Lagerwaard M.A. Paul M.I. Versteegh J.J. Joosten W. Lastdrager E.F. Smit B.J. Slotman J.J.M.E. Nuyttens S.Senan Submitted 10 Salvage surgery for local failures after stereotactic
surgical approach for resectable NSCLC
 surgical approach for resectable NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France 1933 Graham EA, Singer JJ.
surgical approach for resectable NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France 1933 Graham EA, Singer JJ.
Early and locally advanced non-small-cell lung cancer (NSCLC)
") Early and locally advanced non-small-cell lung cancer (NSCLC) ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up P. E. Postmus, K. M. Kerr, M. Oudkerk, S. Senan, D. A. Waller, J.
Early and locally advanced non-small-cell lung cancer (NSCLC) ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up P. E. Postmus, K. M. Kerr, M. Oudkerk, S. Senan, D. A. Waller, J.
Case 1: Early Stage NSCLC. Dr. Dhar Dr. Coughlin Dr. Kay Dr. Hirmiz
 Case 1: Early Stage NSCLC Dr. Dhar Dr. Coughlin Dr. Kay Dr. Hirmiz 62M with 2 months of worsening cough, productive of white sputum. No significant dyspnea. ROS otherwise negative. PMHx: Hypertension,
Case 1: Early Stage NSCLC Dr. Dhar Dr. Coughlin Dr. Kay Dr. Hirmiz 62M with 2 months of worsening cough, productive of white sputum. No significant dyspnea. ROS otherwise negative. PMHx: Hypertension,
Pneumonectomy After Induction Rx: Is it Safe?
 Pneumonectomy After Induction Rx: Is it Safe? David J. Sugarbaker, M.D. Director, Chief, Division of Thoracic Surgery The Olga Keith Weiss Chair of Surgery of Medicine at, Pneumonectomy after induction
Pneumonectomy After Induction Rx: Is it Safe? David J. Sugarbaker, M.D. Director, Chief, Division of Thoracic Surgery The Olga Keith Weiss Chair of Surgery of Medicine at, Pneumonectomy after induction
Stereotactic body radiation therapy versus surgery for patients with stage I non-small cell lung cancer
 Review Article Page 1 of 9 Stereotactic body radiation therapy versus surgery for patients with stage I non-small cell lung cancer Tomoki Kimura Department of Radiation Oncology, Hiroshima University Hospital,
Review Article Page 1 of 9 Stereotactic body radiation therapy versus surgery for patients with stage I non-small cell lung cancer Tomoki Kimura Department of Radiation Oncology, Hiroshima University Hospital,
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
Heterogeneity of N2 disease
 Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Lung cancer Surgery. 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY March, 2017 Berlin, Germany
 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
American Society of Clinical Oncology All rights reserved.
 Stereotactic Body Radiotherapy for Early Stage Non- Small Cell Lung Cancer: American Society of Clinical Oncology Endorsement of the American Society for Radiation Oncology Evidence-based Guideline Introduction
Stereotactic Body Radiotherapy for Early Stage Non- Small Cell Lung Cancer: American Society of Clinical Oncology Endorsement of the American Society for Radiation Oncology Evidence-based Guideline Introduction
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Video-Mediastinoscopy Thoracoscopy (VATS)
") Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
Chemo-radiotherapy in non-small cell lung cancer. HARMESH R NAIK, MD. September 25, 2002
 Chemo-radiotherapy in non-small cell lung cancer HARMESH R NAIK, MD. September 25, 2002 Epidemiology Estimated 170000 new cases Estimated 157,000 deaths Second commonest cancer diagnosis in men and women
Chemo-radiotherapy in non-small cell lung cancer HARMESH R NAIK, MD. September 25, 2002 Epidemiology Estimated 170000 new cases Estimated 157,000 deaths Second commonest cancer diagnosis in men and women
Lung Cancer Update. Disclosures. None
 Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Is Resection Superior to SBRT for Stage I Lesions. Traves Crabtree MD Professor of Surgery Southern Illinois University School of Medicine
 Is Resection Superior to SBRT for Stage I Lesions Traves Crabtree MD Professor of Surgery Southern Illinois University School of Medicine I have nothing pertinent to disclose. Patterns of Recurrence for
Is Resection Superior to SBRT for Stage I Lesions Traves Crabtree MD Professor of Surgery Southern Illinois University School of Medicine I have nothing pertinent to disclose. Patterns of Recurrence for
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery
 Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
Adjuvant Radiotherapy for completely resected NSCLC
 Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Lung and Aerodigestive malignancies
 Lung and Aerodigestive malignancies Nabil F Saba MD, FACP Professor, Director of the Head and Neck Oncology Program, Winship Cancer Institute Emory University COI I am a consultant for GSK, Merck, BMS,
Lung and Aerodigestive malignancies Nabil F Saba MD, FACP Professor, Director of the Head and Neck Oncology Program, Winship Cancer Institute Emory University COI I am a consultant for GSK, Merck, BMS,
8th Edition of the TNM Classification for Lung Cancer. Proposed by the IASLC
 8th Edition of the TNM Classification for Lung Cancer Proposed by the IASLC Introduction Stage classification - provides consistency in nomenclature - improves understanding of anatomic extent of tumour
8th Edition of the TNM Classification for Lung Cancer Proposed by the IASLC Introduction Stage classification - provides consistency in nomenclature - improves understanding of anatomic extent of tumour
Sagar Damle, MD University of Colorado Denver May 23, 2011
 Sagar Damle, MD University of Colorado Denver May 23, 2011 We have debated many times. Here are the topics, and a recap of the last few Pre-operative nutrition Babu pro; Damle con Utility of ECMO Babu
Sagar Damle, MD University of Colorado Denver May 23, 2011 We have debated many times. Here are the topics, and a recap of the last few Pre-operative nutrition Babu pro; Damle con Utility of ECMO Babu
Lung Cancer Radiotherapy
 Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer
 Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
The population of patients with stage III non
 GREGORY M.M. VIDETIC, MD, CM, FRCPC Department of Radiation Oncology, Taussig Cancer Center, Cleveland Clinic, Cleveland, OH Locally advanced non small cell lung cancer: What is the optimal concurrent
GREGORY M.M. VIDETIC, MD, CM, FRCPC Department of Radiation Oncology, Taussig Cancer Center, Cleveland Clinic, Cleveland, OH Locally advanced non small cell lung cancer: What is the optimal concurrent
Lung cancer LUNG CANCER. Box 1 Clinical signs
 22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
CALGB Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer
 CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000