Clinical impact of (18)F-choline PET/CT in patients with recurrent prostate cancer
|
|
|
- Willa Fleming
- 5 years ago
- Views:
Transcription
1 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich Year: 2012 Clinical impact of (18)F-choline PET/CT in patients with recurrent prostate cancer Soyka, Jan D; Muster, Marco A; Schmid, Daniel T; Seifert, Burkhardt; Schick, Ulrike; Miralbell, Raymond; Jorcano, Sandra; Zaugg, Kathrin; Seifert, Hans-Helge; Veit-Haibach, Patrick; Strobel, Klaus; Schaefer, Niklaus G; Husarik, Daniela B; Hany, Thomas F Abstract: PURPOSE: To investigate the clinical value of (18)F-fluorocholine PET/CT (CH-PET/CT) in treatment decisions in patients with recurrent prostate cancer (rpca). METHODS: The study was a retrospective evaluation of 156 patients with rpca and CH-PET/CT for restaging. Questionnaires for each examination were sent to the referring physicians months after examination. Questions included information regarding initial extent of disease, curative first-line treatment, and the treatment plan before and after CH-PET/CT. Additionally, PSA values at diagnosis, after initial treatment, before CH-PET/CT and at the end of follow-up were also obtained from the questionnaires. RESULTS: Mean follow-up was 42 months. The mean Gleason score was 6.9 at initial diagnosis. Initial treatment was: radical prostatectomy in 110 patients, radiotherapy in 39, and combined prostatectomy and radiotherapy in 7. Median PSA values before CH-PET/CT and at the end of follow-up were 3.40 ng/ml and 0.91 ng/ml. PSA levels remained stable, decreased or were below measurable levels in 108 patients. PSA levels increased in 48 patients. In 75 of the 156 patients (48%) the treatment plan was changed due to the CH-PET/CT findings. In 33 patients the therapeutic plan was changed from palliative treatment to treatment with curative intent. In 15 patients treatment was changed from curative to palliative. In 8 patients treatment was changed from curative to another strategy and in 2 patients from one palliative strategy to another. In 17 patients the treatment plan was adapted. CONCLUSION: CH-PET/CT has an important impact on the therapeutic strategy in patients with rpca and can help to determine an appropriate treatment. DOI: Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: Journal Article Accepted Version Originally published at: Soyka, Jan D; Muster, Marco A; Schmid, Daniel T; Seifert, Burkhardt; Schick, Ulrike; Miralbell, Raymond; Jorcano, Sandra; Zaugg, Kathrin; Seifert, Hans-Helge; Veit-Haibach, Patrick; Strobel, Klaus; Schaefer, Niklaus G; Husarik, Daniela B; Hany, Thomas F (2012). Clinical impact of (18)F-choline PET/CT in patients with recurrent prostate cancer. European Journal of Nuclear Medicine and Molecular Imaging, 39(6): DOI:
2 Clinical impact of 18F-Choline PET/CT in patients with recurrent prostate cancer Authors: Jan D. Soyka MD 1, Marco A. Muster 1, Daniel T. Schmid MD 1, Burkhardt Seifert PhD 2, Ulrike Schick MD 3, Raymond Miralbell MD 3, Sandra Jorcano MD 4, Kathrin Zaugg MD 5, Hans-Helge Seifert MD 6, Patrick Veit-Haibach MD 1, Klaus Strobel MD 1, Niklaus G. Schaefer MD 1, Daniela B. Husarik MD 7, Thomas F. Hany MD 1 Affiliations: 1. Dept. of Nuclear Medicine, University Hospital Zurich, Switzerland 2. Division of Biostatistics, Institute of Social and Preventive Medicine, University of Zurich Switzerland 3. Dept. of Radiation-Oncology, University Hospital Geneva, Switzerland 4. Dept. of Radiation-Oncology, Instituto Oncológico Teknon Barcelona, Spain 5. Dept. of Radiation-Oncology, University Hospital Zurich, Switzerland 6. Dept. of Urology, University Hospital Zurich, Switzerland 7. Dept. of Radiology, University Hospital Zurich, Switzerland Corresponding Author: Jan D. Soyka M.D. Dept. Nuclear Medicine, University Hospital Zurich Raemistrasse Zurich Switzerland
3 Phone: Fax: Word count: 2820
4 ABSTRACT Purpose: To investigate the clinical value of 18F-Fluorocholine PET/CT (CH- PET/CT) regarding treatment decisions in patients with recurrent prostate cancer (rpca). Methods: Retrospective evaluation of 156 patients with rpca and CH-PET/CT for restaging. Questionnaires for each examination were sent to the referring physicians months after examination. Questions included information regarding initial extent of disease, curative first-line treatment, as well as the treatment plan before and after CH-PET/CT. Additionally, PSA values were collected from the questionnaire at diagnosis, after initial treatment, before CH-PET/CT and at the end of follow-up. Results: Mean follow-up was 42 months; mean Gleason Score was 6.9 at initial diagnosis. Initial treatment was: Radical prostatectomy (n=110), radiotherapy (n=39), combined prostatectomy and radiotherapy (n=7). Median PSA values before CH- PET/CT and at end of follow-up were 3.40 ng/ml and 0.91 ng/ml. PSA levels remained stable, dropped or were below measurable levels in 108 patients. PSA levels rose in 48 patients. In 75/156 patients (48%) treatment plan changed due to findings in CH-PET/CT. In 33 patients the therapeutic modality changed from a palliative to a curative intended treatment. In 15 patients the therapeutic modality was altered from a curative towards a palliative setting. 8 patients had a change from one curative modality to another and 2 patients from one palliative modality to another. 17 patients had adaptations within their therapeutic modality. Conclusion: CH-PET/CT has an important impact on therapeutic strategy in patients with recurrent prostate cancer and can help to determine an appropriate treatment.
5 INTRODUCTION Adenocarcinoma of the prostate (PCA) is the most common malignant tumor in men in the United States of America with second-most cancer-deaths per year following bronchial carcinoma [1]. Nevertheless current staging and re-staging procedures especially regarding nodal involvement and distant metastases still have many limitations leading to insufficiencies in curatively intended therapies. Consequently as many as % of treated patients with initially curative intention suffer from recurrent disease [2-5]. Rising levels of prostate specific antigen (PSA) in the blood serum of patients indicate tumor progression often long before imaging modalities can detect any abnormalities. In this biochemical relapse situation there are no guidelines giving any conclusive suggestions regarding imaging procedures. Bonescintigraphy and CT are both insensitive and show reliable results only at PSA levels of above 20 ng/ml [6]. Thus according to the current guidelines these examinations can safely be omitted. Depending solely on the kinetics of the rising PSA levels the decision is made whether a local recurrence or a distant recurrence is present. If a local recurrence is suspected patients may qualify for a salvage procedure of the prostate fossa. If distant disease is suspected only palliative antihormonal treatment is suggested. MRI with endorectal coil shows reliable results in the evaluation of the prostate fossa but is not routinely recommended by the guidelines [6-8]. 18F-Choline PET/CT (CH-PET/CT) is a promising examination tool for the detection of recurrent prostate cancer (rpca) [9]. Even though the exact role of the examination is still being discussed it seems that CH-PET/CT starts playing a role in the management of patients with a biochemical relapse [10] [11]. Several studies have demonstrated that CH-PET/CT either labeled with C-11 [12] [13] or with F-18 [14] [15] can detect tumor recurrence at PSA levels of above 2ng/ml giving the clinicians the opportunity of a curative intended salvage procedure at an early time-point of the recurrence [12-15].
6 In certain constellations tumor recurrence can even be detected if PSA levels are below the level of 2ng/ml, however the detection rates drop in these patient populations down to approx % [13] [16]. Even though localized treatment of distant metastases currently is not an established therapy several reports have already been published, showing promising results regarding CH-PET/CT guided radiation therapy and salvage surgery [17-19]. We therefore retrospectively analyzed the impact of the results of CH-PET/CT examinations performed at our institution on treatment decisions.
7 MATERIALS AND METHODS This study was conducted according to the local-ethics committee guidelines for retrospective analyses. Between March 2003 and October 2007 we performed 353 CH-PET/CT examinations in patients with PCA. Of these patients 229 had had rising PSA levels after an initial treatment with surgery, radiation therapy or both, indicating recurrent disease. Since no recommendations were given by the guidelines previous conventional imaging (e.g. bone-scan, MRI, CT) was not required for inclusion into our follow-up study [6-8]. Questionnaires were created and sent to the referring physicians in December 2008, 14 months after the scan of the last included patient. After a waiting period of approximately 4 weeks those physicians who had not returned the questionnaires were once reminded by telephone. CH-PET/CT All the data were acquired on a combined PET/CT in-line system (Discovery LS or Discovery ST, GE Health Systems, Milwaukee, WI). These dedicated systems integrate a PET scanner (GE Advance Nxi, GE Health Systems, Milwaukee, WI) with a multislice helical CT (LightSpeed plus or LightSpeed 16; GE Health Systems, Milwaukee, WI) and permit the acquisition of co-registered CT and PET images in one session. No oral or intravenous CT contrast agent was used. Patients were examined in the supine position. The unenhanced CT scans were acquired with the following parameters: 80 ma, 140 kv, 0.5-second tube rotation, 4.25 mm section thickness, 867 mm scan length, and 22.5 second data acquisition time. The CT scans were acquired during breath hold with the normal expiration position, and scanning included the area from the head to the pelvic floor. The PET emission scan started 3-4 minutes after the injection of a standard dose of MBq 18F- Fluorocholine. After the acquisition of a partial-body scan (pelvic floor to vertex)
8 approx min post-injection a second partial-body scan with same scan-length was acquired, without taking the patient off the examination-table and without voiding of the bladder. The PET images were acquired starting at the level of the pelvis, with an acquisition time of 3 minutes for the emission scan per cradle position and a oneslice overlap. The CT data were used for attenuation correction, and images were reconstructed using a standard 2D-iterative algorithm (ordered subset expectation maximization). For image fusion, 4.25 mm thick CT image-slices were reconstructed. Images were then transferred to a commercially available workstation (GE Advantage Workstation). These workstations allow simultaneous data evaluation of early and late phase PET studies with the corespondig CT images as a single procedure and in an image fusion mode. Both partial-body PET scans were fused with the CT-scan and read side by side. The early scan was primarily used for the evaluation of the prostate fossa because at this time the tracer hasn t arrived in the bladder. The late scan was used for better differentiation between reactive / Inflammatory and malignant lymph nodes [20]. A visually detectable washout of the tracer from lymph nodes over time was considered as benign whereas a persisting or increasing tracer-activity in lymph nodes was considered as a sign for malignancy. Diagnostic Findings All CH-PET/CT examinations were reported by a dual-board-certified radiologist / nuclear medicine physician with 5 years of experience in CH-PET/CT reading. The findings from each CH-PET/CT examination were collected from these written reports. Although performed in some patients a validation of the findings from CH- PET/CT with other imaging methods or with a histological workup could not be
9 obtained consistently due to the retrospective character of the study and was therefore not required for inclusion into the study-population. Questionnaire: The questionnaire consisted of questions regarding the following topics: 1) Initial TNM stage and initial grading according to Gleason 2) Initial therapies and antihormonal treatments 3) Treatment after CH-PET/CT and hypothetical treatment if no CH-PET/CT had been available. 4) PSA values at diagnosis, after initial therapy, before CH-PET/CT and at the end of follow-up. The referring physicians had to indicate the therapeutic strategy of the patient as it had been defined after the results from CH-PET/CT. Then they had to define a hypothetical therapeutic strategy, assuming the results from the CH-PET/CT had not been available. Additionally they had to indicate whether the effectively chosen treatment plan had been influenced by the CH-PET/CT (Table 2). A change in therapy consisted of the choice of a different therapeutic modality (e.g. antihormonal therapy à radiation therapy) or of an alteration within a therapeutic modality (e.g. adaptation of the radiation field) Statistical data analysis: General descriptive statistics were performed to calculate mean age, mean follow-up and median PSA-values. Due to the substantial skew of the PSA value distribution a logarithmic transformation was performed for all PSA values to obtain a symmetric distribution. A constant value of 0.01 was added to all PSA values before transformation to make PSA values of zero valid for transformation. PSA
10 development-ratios from PSA values before and after CH-PET/CT were calculated by subtracting the log transformed post-ch-pet/ct values from the log transformed pre-ch-pet/ct values. Non-parametric testing (Mann-Whitney U Test) was used for comparison of PSA development-ratios among different patient subgroups. The Wilcoxon signed rank test was used for comparison of PSA values before and after CH-PET/CT. P-values < 0.05 were considered significant. All statistical analyses were performed using SPSS for Windows, Release (SPSS Inc., Chicago, IL)
11 RESULTS Disease characteristics A total of 163 questionnaires could be obtained by the referring physicians. 7 patients with returned questionnaires had to be excluded because of missing PSA values before CH-PET/CT and/or at the end of follow-up. Finally 156/229 (68%) completed questionnaires could be used for evaluation (Table 1). Mean follow-up was 42 months (range months). Mean age of the patients at the time of CH-PET/CT was 66 years (range years). At diagnosis the mostly represented tumor stage was T3 N0 M0 with a mean Gleason Score of 6.91 (Table 2). Initial treatment consisted of radical prostatectomy in 110 patients. 39 patients had undergone radiotherapy and 7 patients a combination of both. Diagnostic performance Positive findings in CH-PET/CT were reported in 124/156 (79%) patients. 63/156 (40%) patients had a local recurrence only, 27/156 (17%) patients had lymphatic metastases only and 9/156 (6%) patients had metastases to the bones only. A local recurrence plus nodal metastases were found in 14/156 (8%) patients and 8/156 (5%) of patients had local recurrence plus bony metastases. 4/156 (3%) of patients had tumor manifestations in the prostate fossa, in lymph nodes and in the bones. Effective vs. hypothetical treatment In 75/156 patients (48%) the referring physicians indicated a change of the therapeutic strategy. In 33 patients (21%) the therapeutic modality changed from a palliative to a curative intended treatment (surgery, radiation therapy, HIFU and combined therapies). In 15 patients (10%) the therapeutic modality was altered from
12 a curative towards a palliative setting (watchful waiting, antihormonal treatment or chemotherapy). 8 patients (5%) had a change from one curative modality to another and 2 patients (1%) from one palliative modality to another. 17 patients (11%) had adaptations within their therapeutic modality (Tables 2 and 3). In 8 patients (6%) a change in therapy was indicated even though CH-PET/CT showed no abnormities. Three of these patients (initially operated) scheduled for RT before CH-PET/CT had an adaptation of their radiation field. One patient (initially operated) was changed from RT to surgery. One patient (initially operated) scheduled for surgery had an adaptation of his surgical procedure. One patient (initially operated) scheduled for RT and additional antihormonal treatment was changed to antihormonal treatment only. One patient (initially with RT) was changed from antihormonal treatment to watchful waiting. One patient (initially operated) scheduled for antihormonal treatment had an adaptation of this treatment. PSA values Table 4 summarizes the PSA values of our patient population at the different timepoints. Since 2 patients had extraordinarily high PSA values at the end of follow-up (One patient had a PSA of 150 ng/ml and the other ng/ml) not only mean PSA levels but also median values were calculated to correct for the overwhelming influence of these two patients on the results. PSA levels before CH-PET/CT were significantly higher compared to those at the end of follow-up (P < 0.001; Wilcoxon signed rank test). At the end of follow-up, PSA values declined in 107 patients (69%) due to subsequent therapies. Of these 107 patients 16 (10%) had values below the measurable threshold. 1 patient (1%) had a stable PSA and in 48 patients (31%) the PSA levels increased.
13 PSA values before CH-PET/CT were significantly higher (P < 0.001, Mann-Whitney U Test) in patients with positive CH-PET/CT scans (median PSA 4.50 ng/ml, range ng/ml) compared to those with negative scans (median PSA 1.20 ng/ml, range ng/ml). However there was no significant difference regarding the PSA development-ratios (obtained from the PSA-values before and after CH- PET/CT) in the comparison of patients with positive CH-PET/CT to those with negative scans (P = 0.70, Mann-Whitney U Test). These two groups did not differ regarding initial PSA levels at the time point of diagnosis (P = 0.48, Mann-Whitney U Test). PSA values of the patients where the intended treatment plan was changed after CH- PET/CT (n=75, 48%) were compared with those of patients where no change of treatment had been performed (n=81, 52%). There was no significant difference between these two groups regarding the PSA development-ratios (pre-/post CH- PET/CT) (P = 0.68, Mann-Whitney U Test). Again the PSA values at the time of primary diagnosis were not significantly different in these two groups (P = 0.67, Mann-Whitney U Test)
14 DISCUSSION To our knowledge this retrospective analysis is the first, to analyze the clinical impact of CH-PET/CT on treatment decisions in patients with recurrent prostate cancer. We obtained our data using questionnaires, which were sent to those physicians who had referred their patients for a CH-PET/CT to our institution. The referring physicians had to provide information about the therapy, which had been performed after CH-PET/CT and had to determine a hypothetical therapeutic management without the information obtained from the CH-PET/CT. With this method we could demonstrate a strong clinical impact of CH-PET/CT. The results of our examination lead to changes of the therapy in 48% of patients, which consisted of adaptation of the current treatment-regime or even complete change of the therapeutic approach. Even though a comparison with a non-ch-pet/ct control group was not possible due to the retrospective study design, the performed therapies after CH-PET/CT were effective since a significant decline of the mean PSA values after the examination compared to before could be observed. Interestingly PSA development-ratios of patients with positive findings in CH-PET/CT compared to those with negative findings demonstrated no statistical significance. The same accounted for the comparison of patients with therapeutic changes due to CH-PET/CT compared to those without. We believe that there are several factors, which lead to these results: If patients had no findings in CH-PET/CT the treatment in general followed the standard procedures for recurrent disease [6-8]. According to the guidelines in such a situation if no other findings are present the decision whether a local or distant recurrence is present is made by the PSA kinetics. The standard procedures then are radiation therapy (if initially undergone surgery), antihormonal treatment, salvage resection, or combined approaches. After such a procedure the likelihood of a
15 successful treatment is high, especially since CH-PET/CT (even though per definition false negative due to rising PSA) has excluded gross metastatic spread. Thus it is not surprising that not only those of our patients with positive findings in CH-PET/CT had favourable PSA development-ratios but also those without detectable pathologies in the CH-PET/CT examination. The situation with the subgroup of patients with therapeutic changes compared to those without is quite similar. If CH-PET/CT confirmed the suspected localization of recurrent disease no change of therapy management occurred. The intended treatment-approach remained correctly unchanged for these patients and the PSA development-ratios were of course as favourable as they were for those patients where CH-PET/CT demonstrated findings which led to a change of the therapeutic management. Therefore, it becomes clear that with our study setup it is not possible to make statements about the influence of CH-PET/CT on the outcome of recurrent prostate cancer. Interestingly in 8 patients the referring physicians indicated changes in therapy even though CH-PET/CT demonstrated no positive findings. These results can be explained by the fact that despite the failure to detect the recurrent disease CH- PET/CT was able to exclude gross metastatic spread. This obviously led to changes of the planned treatment such as adaptation of the radiation field. The major limitation of our study is its retrospective character. Our referring physicians had to retrospectively determine which therapy would have been performed if no CH-PET/CT had been available. There is potential bias, since the referring physicians were most likely to support CH-PET/CT. Thus more favourable results regarding therapeutic changes could be assumed compared to a real prospective study design. Nevertheless we believe that no serious bias has been
16 introduced into our study. First of all, according to the guidelines for prostate cancer recurrence the therapeutic options are not very wide. They consist of radiation therapy, antihormonal treatment, salvage surgery, chemotherapy or a combination of these. There were two categories of patients referred for CH-PET/CT. The first category consisted of patients who had had a complete treatment with initial curative therapy, recurrence, salvage procedure and again rising PSA levels. Following the guidelines in such a situation without further diagnostics only a palliative procedure with antihormonal treatment or watchful-waiting was advised. Any therapy aside these two options was therefore very likely to be due to CH-PET/CT and a bias was basically only possible if a change of therapy occurred within the two palliative options, which was indicated in only 2/75 patients. The second category were patients whose PSA didn t decline sufficiently or started rising again after initial curative therapy. For these potentially curable patients the standard procedure according to the guidelines is a salvage locoregional therapy mostly consisting of surgery or radiation therapy. Thus indicated therapeutic changes from a curative to a palliative setting (15/75 patients) or within the same curative modality, like extended lymphadenectomy or extended radiation field (16/75 patients), were most likely correct and not due to a bias. The only potential for biasing was given in those patients where therapeutic changes were indicated from one curative setting to another (8/75 patients).
17 Conclusion According to the results in our patient population CH-PET/CT in patients with recurrent prostate cancer has an important impact on the therapeutic strategy and can help to determine an appropriate treatment for these patients.
18 Conflict of Interest statement All authors declare that they have no conflict of interest.
19 REFERENCES 1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61: doi:caac [pii] /caac Lu-Yao GL, Potosky AL, Albertsen PC, Wasson JH, Barry MJ, Wennberg JE. Follow-up prostate cancer treatments after radical prostatectomy: a population-based study. J Natl Cancer Inst. 1996;88: Bott SR. Management of recurrent disease after radical prostatectomy. Prostate Cancer Prostatic Dis. 2004;7: doi: /sj.pcan [pii]. 4. Fowler FJ, Jr., Barry MJ, Lu-Yao G, Roman A, Wasson J, Wennberg JE. Patient-reported complications and follow-up treatment after radical prostatectomy. The National Medicare Experience: (updated June 1993). Urology. 1993;42: Freedland SJ, Humphreys EB, Mangold LA, Eisenberger M, Dorey FJ, Walsh PC, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005;294: doi:294/4/433 [pii] /jama Mottet N, Bellmunt J, Bolla M, Joniau S, Mason M, Matveev V, et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castrationresistant prostate cancer. Eur Urol. 2011;59: doi:s (11) [pii] /j.eururo Heidenreich A, Bellmunt J, Bolla M, Joniau S, Mason M, Matveev V, et al. EAU guidelines on prostate cancer. Part 1: screening, diagnosis, and treatment of clinically localised disease. Eur Urol. 2011;59: doi:s (10) [pii] /j.eururo NCCN. NCCN Clinical Practice Guidelines in Oncology, Prostate Cancer Schmid DT, John H, Zweifel R, Cservenyak T, Westera G, Goerres GW, et al. Fluorocholine PET/CT in patients with prostate cancer: initial experience. Radiology. 2005;235: doi:235/2/623 [pii] /radiol Picchio M, Briganti A, Fanti S, Heidenreich A, Krause BJ, Messa C, et al. The role of choline positron emission tomography/computed tomography in the management of patients with prostate-specific antigen progression after radical treatment of prostate cancer. Eur Urol. 2011;59: doi:s (10) [pii] /j.eururo Fanti S, Krause B, Weber W, Castellucci P, Grosu AL, de Jong IJ, et al. Re: Nicolas Mottet, Joaquim Bellmunt, Michel Bolla, et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol 2011;59: Eur Urol. 2011;60:e37-8; author reply e9-41. doi:s (11) [pii] /j.eururo Castellucci P, Fuccio C, Nanni C, Santi I, Rizzello A, Lodi F, et al. Influence of trigger PSA and PSA kinetics on 11C-Choline PET/CT detection rate in patients with biochemical relapse after radical prostatectomy. J Nucl Med. 2009;50: doi:jnumed [pii]
20 /jnumed Krause BJ, Souvatzoglou M, Tuncel M, Herrmann K, Buck AK, Praus C, et al. The detection rate of [11C]choline-PET/CT depends on the serum PSA-value in patients with biochemical recurrence of prostate cancer. Eur J Nucl Med Mol Imaging. 2008;35: doi: /s Husarik DB, Miralbell R, Dubs M, John H, Giger OT, Gelet A, et al. Evaluation of [(18)F]-choline PET/CT for staging and restaging of prostate cancer. Eur J Nucl Med Mol Imaging. 2008;35: doi: /s Heinisch M, Dirisamer A, Loidl W, Stoiber F, Gruy B, Haim S, et al. Positron emission tomography/computed tomography with F-18-fluorocholine for restaging of prostate cancer patients: meaningful at PSA < 5 ng/ml? Mol Imaging Biol. 2006;8:43-8. doi: /s Castellucci P, Fuccio C, Rubello D, Schiavina R, Santi I, Nanni C, et al. Is there a role for (1)(1)C-choline PET/CT in the early detection of metastatic disease in surgically treated prostate cancer patients with a mild PSA increase <1.5 ng/ml? Eur J Nucl Med Mol Imaging. 2011;38: doi: /s Souvatzoglou M, Krause BJ, Purschel A, Thamm R, Schuster T, Buck AK, et al. Influence of (11)C-choline PET/CT on the treatment planning for salvage radiation therapy in patients with biochemical recurrence of prostate cancer. Radiother Oncol. 2011;99: doi:s (11) [pii] /j.radonc Wurschmidt F, Petersen C, Wahl A, Dahle J, Kretschmer M. [18F]fluoroethylcholine-PET/CT imaging for radiation treatment planning of recurrent and primary prostate cancer with dose escalation to PET/CT-positive lymph nodes. Radiat Oncol. 2011;6:44. doi: x-6-44 [pii] / X Rigatti P, Suardi N, Briganti A, Da Pozzo LF, Tutolo M, Villa L, et al. Pelvic/retroperitoneal salvage lymph node dissection for patients treated with radical prostatectomy with biochemical recurrence and nodal recurrence detected by [11C]choline positron emission tomography/computed tomography. Eur Urol. 2011;60: doi:s (11) [pii] /j.eururo Kwee SA, Wei H, Sesterhenn I, Yun D, Coel MN. Localization of primary prostate cancer with dual-phase 18F-fluorocholine PET. J Nucl Med. 2006;47: doi:47/2/262 [pii].
21 TABLES Table PCA- patients CH- PET/CT between March October 229 patients rpca with rising PSA after surgery and/or Questionnaires to referring physicians months after Questionnaires returned by referring physicians: 163 patients Questionnaires without missing relevant data: 156 patients Table 1 describes our patient inclusion-pathway.
22 Table 2 Table 2A n=12; (7%) n=1; (1%) n=1; (1%) n=2; (1%) n=5; (3%) n=8; (5%) n=17; (10%) n=27; (17%) n=52; (32%) n=38; (23%) Gleason 2 Gleason 3 Gleason 4 Gleason 5 Gleason 6 Gleason 7 Gleason 8 Gleason 9 Gleason 10 Gleason x
23 Table 2B TNM-Stage N0 N1 Nx M1 T T T T TX Table 2 shows the disease characteristics of our patient population. In table 2A the distribution of Gleason Scores is visualized. Table 2B shows the TNM stages of our patients. For an easier understanding patients with MX were treated as M0 in this table. 5 patients had distant metastases (3 patients T3 N1 M1; 1 patient T4 N0 M1 and 1 patient T4 NX M1)..
24 Table 3 Watchful waiting (no therapy) Antihormonal treatment Radiation therapy Surgery HIFU Chemotherapy Anthormonal and radiation therapy Surgery and radiation therapy Therapy with CH- PET/CT Hypothetical therapy without CH- PET/CT Table 3 shows the effectively performed treatments with CH-PET/CT in the upper column and the hypothetical treatments without CH-PET/CT as indicated by the referring physicians in the lower column.
25 Table 4 PSA At diagnosis Nadir after treatment Before CH- PET/CT At end of followup Available in n= 149/ / / /156 Mean value ng/ml Median value ng/ml Table 4 describes the PSA values of our patients (including the availiability of the measurements) at selected time-points.
.")
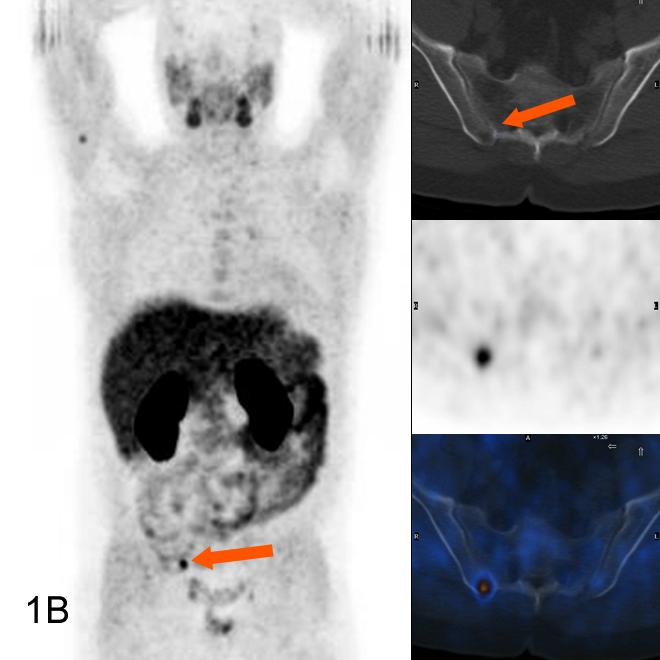
26 FIGURES Figure 1 53 year old patient, 6 years after surgery. Rising PSA 3.0 ng/ml. Bone scintigraphy including SPECT/CT was read as negative, also in the right iliac bone (arrow) (1A). Thus a local recurrence was suspected leading to a hypothetical treatment with radiation therapy of the small pelvis. CH-PET/CT performed 4 weeks later revealed a metastasis in the iliac bone (1B). The therapy-management was changed to a radiation therapy of the iliac bone and additional antihormonal treatment. PSA declined to 2.45ng/ml
27

28 Figure 2 74 year-old patient, 3 years after surgery. Rising PSA 2.2 ng/ml. CH-PET/CT confirmed a clinically suspected local recurrence. No change in therapymanagement. Patient received radiation therapy and PSA declined to 0.43 ng/ml
Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer
 ORIGINAL ARTICLE Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer Giorgio Lamanna, MD,* Claire Tabouret-Viaud,
ORIGINAL ARTICLE Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer Giorgio Lamanna, MD,* Claire Tabouret-Viaud,
Interpretation of 11C choline PET/CT for the diagnosis of local relapse in radically treated prostate cancer
 Matti et al. European Journal of Hybrid Imaging (2017) 1:5 DOI 10.1186/s41824-017-0007-x European Journal of Hybrid Imaging SHORT COMMUNICATION Open Access Interpretation of 11C choline PET/CT for the
Matti et al. European Journal of Hybrid Imaging (2017) 1:5 DOI 10.1186/s41824-017-0007-x European Journal of Hybrid Imaging SHORT COMMUNICATION Open Access Interpretation of 11C choline PET/CT for the
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Evidence of choline PET CT scan for detecting early recurrence or metastatic prostatic cancer
 Original article Evidence of choline PET CT scan for detecting early recurrence or metastatic prostatic cancer Sachin Yallappa, Isthiakul Rizvi Glasgow Royal infirmary, Birmingham Queen Elizabeth Hospital,
Original article Evidence of choline PET CT scan for detecting early recurrence or metastatic prostatic cancer Sachin Yallappa, Isthiakul Rizvi Glasgow Royal infirmary, Birmingham Queen Elizabeth Hospital,
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
european urology 52 (2007)
") european urology 52 (2007) 423 429 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prostate Cancer Detection of Lymph-Node Metastases with Integrated [ 11 C]Choline PET/CT
european urology 52 (2007) 423 429 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prostate Cancer Detection of Lymph-Node Metastases with Integrated [ 11 C]Choline PET/CT
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
PET imaging of cancer metabolism is commonly performed with F18
 PCRI Insights, August 2012, Vol. 15: No. 3 Carbon-11-Acetate PET/CT Imaging in Prostate Cancer Fabio Almeida, M.D. Medical Director, Arizona Molecular Imaging Center - Phoenix PET imaging of cancer metabolism
PCRI Insights, August 2012, Vol. 15: No. 3 Carbon-11-Acetate PET/CT Imaging in Prostate Cancer Fabio Almeida, M.D. Medical Director, Arizona Molecular Imaging Center - Phoenix PET imaging of cancer metabolism
University of Groningen. Morphological aspects of recurrent prostate cancer Rybalov, Maxim
 University of Groningen Morphological aspects of recurrent prostate cancer Rybalov, Maxim IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen Morphological aspects of recurrent prostate cancer Rybalov, Maxim IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
In Western Europe and North America, prostate cancer is
 Journal of Nuclear Medicine, published on April 4, 2013 as doi:10.2967/jnumed.112.110148 Impact of F-Choline PET/CT in Prostate Cancer Patients with Biochemical Recurrence: Influence of Androgen Deprivation
Journal of Nuclear Medicine, published on April 4, 2013 as doi:10.2967/jnumed.112.110148 Impact of F-Choline PET/CT in Prostate Cancer Patients with Biochemical Recurrence: Influence of Androgen Deprivation
Early detection of prostate cancer (PCa) may feasibly lead
 may feasibly lead") ORIGINAL ARTICLE C-11 Choline PET/CT Imaging for Differentiating Malignant From Benign Prostate Lesions Xin Li, MD,* Qi Liu, MD, PhD,* Muwen Wang, MD, PhD,* Xunbo Jin, MD,* Qingwei Liu, MD, PhD,* Shuzhan
ORIGINAL ARTICLE C-11 Choline PET/CT Imaging for Differentiating Malignant From Benign Prostate Lesions Xin Li, MD,* Qi Liu, MD, PhD,* Muwen Wang, MD, PhD,* Xunbo Jin, MD,* Qingwei Liu, MD, PhD,* Shuzhan
University of Groningen. Morphological aspects of recurrent prostate cancer Rybalov, Maxim
 University of Groningen Morphological aspects of recurrent prostate cancer Rybalov, Maxim IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen Morphological aspects of recurrent prostate cancer Rybalov, Maxim IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience.
 Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience. Elisabetta Ponti MD, Gianluca Ingrosso MD, Alessandra Carosi PhD, Luana
Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience. Elisabetta Ponti MD, Gianluca Ingrosso MD, Alessandra Carosi PhD, Luana
Short summary of published results of PET with fluoromethylcholine (18F) in prostate cancer
 in prostate cancer") Short summary of published results of PET with fluoromethylcholine (18F) in prostate cancer JN TALBOT and all the team of Service de Médecine Nucléaire Hôpital Tenon et Université Pierre et Marie Curie,
Short summary of published results of PET with fluoromethylcholine (18F) in prostate cancer JN TALBOT and all the team of Service de Médecine Nucléaire Hôpital Tenon et Université Pierre et Marie Curie,
The Use of PET Scanning in Urologic Oncology
 The Use of PET Scanning in Urologic Oncology Dr Nicholas C. Buchan Uro-oncology Fellow 1 2 Aims To understand the basic concepts underlying PET scanning. Understand the emerging role of PET Scanning for
The Use of PET Scanning in Urologic Oncology Dr Nicholas C. Buchan Uro-oncology Fellow 1 2 Aims To understand the basic concepts underlying PET scanning. Understand the emerging role of PET Scanning for
Alexander Winter 1*, Rolf-Peter Henke 2 and Friedhelm Wawroschek 1
 Winter et al. BMC Urology (2015) 15:10 DOI 10.1186/s12894-015-0004-y RESEARCH ARTICLE Open Access Targeted salvage lymphadenectomy in patients treated with radical prostatectomy with biochemical recurrence:
Winter et al. BMC Urology (2015) 15:10 DOI 10.1186/s12894-015-0004-y RESEARCH ARTICLE Open Access Targeted salvage lymphadenectomy in patients treated with radical prostatectomy with biochemical recurrence:
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Using PET/CT in Prostate Cancer
 Using PET/CT in Prostate Cancer Legal Disclaimer These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
Using PET/CT in Prostate Cancer Legal Disclaimer These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Whole Body MRI. Dr. Nina Tunariu. Prostate Cancer recurrence, progression and restaging
 Whole Body MRI Prostate Cancer recurrence, progression and restaging Dr. Nina Tunariu Consultant Radiology Drug Development Unit and Prostate Targeted Therapies Group 12-13 Janeiro 2018 Evolving Treatment
Whole Body MRI Prostate Cancer recurrence, progression and restaging Dr. Nina Tunariu Consultant Radiology Drug Development Unit and Prostate Targeted Therapies Group 12-13 Janeiro 2018 Evolving Treatment
L approccio alle stazioni linfonodali in presentazione di malattia ed all eventuale recidiva nodale: il punto di vista dell urologo
 L approccio alle stazioni linfonodali in presentazione di malattia ed all eventuale recidiva nodale: il punto di vista dell urologo Paolo Gontero Division of Urology Città della Salute e della Scienza
L approccio alle stazioni linfonodali in presentazione di malattia ed all eventuale recidiva nodale: il punto di vista dell urologo Paolo Gontero Division of Urology Città della Salute e della Scienza
Staging of Prostatic Carcinoma - The evolving use of SPECT-CT and Positron Emission Tomography (PET)
") Staging of Prostatic Carcinoma - The evolving use of SPECT-CT and Positron Emission Tomography (PET) Poster No.: C-2477 Congress: ECR 2015 Type: Educational Exhibit Authors: B. Rawal, N. Vasdev, R. P.
Staging of Prostatic Carcinoma - The evolving use of SPECT-CT and Positron Emission Tomography (PET) Poster No.: C-2477 Congress: ECR 2015 Type: Educational Exhibit Authors: B. Rawal, N. Vasdev, R. P.
Evaluation of [ 18 F]-choline PET/CT for staging and restaging of prostate cancer
![Evaluation of [ 18 F]-choline PET/CT for staging and restaging of prostate cancer](/thumbs/88/114834683.jpg "Evaluation of [ 18 F]-choline PET/CT for staging and restaging of prostate cancer") Eur J Nucl Med Mol Imaging (2008) 35:253 263 DOI 10.1007/s00259-007-0552-9 ORIGINAL ARTICLE Evaluation of [ 18 F]-choline PET/CT for staging and restaging of prostate cancer Daniela B. Husarik & Raymond
Eur J Nucl Med Mol Imaging (2008) 35:253 263 DOI 10.1007/s00259-007-0552-9 ORIGINAL ARTICLE Evaluation of [ 18 F]-choline PET/CT for staging and restaging of prostate cancer Daniela B. Husarik & Raymond
Colorectal cancer is one of the most common cancer
 Journal of Nuclear Medicine, published on February 20, 2008 as doi:10.2967/jnumed.107.048249 Staging Pathways in Recurrent Colorectal Carcinoma: Is Contrast-Enhanced 18 F-FDG PET/CT the Diagnostic Tool
Journal of Nuclear Medicine, published on February 20, 2008 as doi:10.2967/jnumed.107.048249 Staging Pathways in Recurrent Colorectal Carcinoma: Is Contrast-Enhanced 18 F-FDG PET/CT the Diagnostic Tool
Urological Oncology. Objective. Results. Patients and Methods
 Urological Oncology Clinical utility of 18 F-fluorocholine positron-emission tomography/computed tomography (PET/CT) in biochemical relapse of prostate cancer after radical treatment: results of a multicentre
Urological Oncology Clinical utility of 18 F-fluorocholine positron-emission tomography/computed tomography (PET/CT) in biochemical relapse of prostate cancer after radical treatment: results of a multicentre
Salvage Stereotactic Body Radiotherapy for Patients With Limited Prostate Cancer Metastases: Deferring Androgen Deprivation Therapy
 Salvage Stereotactic Body Radiotherapy for Patients With Limited Prostate Cancer Metastases: Deferring Androgen Deprivation Therapy Patrick Berkovic, 1 Gert De Meerleer, 1 Louke Delrue, 2 Bieke Lambert,
Salvage Stereotactic Body Radiotherapy for Patients With Limited Prostate Cancer Metastases: Deferring Androgen Deprivation Therapy Patrick Berkovic, 1 Gert De Meerleer, 1 Louke Delrue, 2 Bieke Lambert,
Role of 18 F-choline PET/CT in evaluation of patients with prostate carcinoma
 research article 17 Role of F-choline PET/CT in evaluation of patients with prostate carcinoma Marina Hodolic Department for Nuclear Medicine, University Medical Centre Ljubljana, Slovenia Received 4 October
research article 17 Role of F-choline PET/CT in evaluation of patients with prostate carcinoma Marina Hodolic Department for Nuclear Medicine, University Medical Centre Ljubljana, Slovenia Received 4 October
Accepted Manuscript. S (18) /j.adro Reference: ADRO 244. To appear in: Advances in Radiation Oncology
 /j.adro Reference: ADRO 244. To appear in: Advances in Radiation Oncology") Accepted Manuscript Percutaneous image guided nodal biopsy after C-11 Choline PET/CT for Biochemically Recurrent Prostate Cancer: Imaging Predictors of Disease and Clinical Implications B.T. Welch, A.T.
Accepted Manuscript Percutaneous image guided nodal biopsy after C-11 Choline PET/CT for Biochemically Recurrent Prostate Cancer: Imaging Predictors of Disease and Clinical Implications B.T. Welch, A.T.
Colorectal Cancer and FDG PET/CT
 Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου
 Η θέση του PET/CT στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου 2014 : the Guidelines year. PRINCIPLES OF IMAGING Imaging is performed for the detection
Η θέση του PET/CT στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου 2014 : the Guidelines year. PRINCIPLES OF IMAGING Imaging is performed for the detection
F choline PET/CT in Prostate Cancer
 18 F choline PET/CT in Prostate Cancer WV Vogel, Antoni van Leeuwenhoek, Amsterdam OS Hoekstra, VUmc, Amsterdam E Vegt, Antoni van Leeuwenhoek, Amsterdam MJ Roef, Catharina Ziekenhuis, Eindhoven B de Keizer,
18 F choline PET/CT in Prostate Cancer WV Vogel, Antoni van Leeuwenhoek, Amsterdam OS Hoekstra, VUmc, Amsterdam E Vegt, Antoni van Leeuwenhoek, Amsterdam MJ Roef, Catharina Ziekenhuis, Eindhoven B de Keizer,
Impact of fasting on 18 F-fluorocholine gastrointestinal uptake and detection of lymph node metastases in patients with prostate cancer
 Wondergem et al. EJNMMI Research (2016) 6:2 DOI 10.16/s13550-015-0159-2 SHORT COMMUNICATION Open Access Impact of fasting on F-fluorocholine gastrointestinal uptake and detection of lymph node metastases
Wondergem et al. EJNMMI Research (2016) 6:2 DOI 10.16/s13550-015-0159-2 SHORT COMMUNICATION Open Access Impact of fasting on F-fluorocholine gastrointestinal uptake and detection of lymph node metastases
MRI and metastases of PCa
 MRI and metastases of PCa François CORNUD Céline COUVIDAT David EISS Arnaud LEFEVRE IRM Paris 16, France, Paris, France Université Paris Descartes, Paris, France When imaging should be considered for detection
MRI and metastases of PCa François CORNUD Céline COUVIDAT David EISS Arnaud LEFEVRE IRM Paris 16, France, Paris, France Université Paris Descartes, Paris, France When imaging should be considered for detection
PET/CT imaging and RIT of prostate cancer. Kirsten Bouchelouche, MD, DMSc PET & Cyclotron Unit Rigshospitalet, Copenhagen Denmark
 PET/CT imaging and RIT of prostate cancer Kirsten Bouchelouche, MD, DMSc PET & Cyclotron Unit Rigshospitalet, Copenhagen Denmark Prostate cancer Prostate cancer is the most common malignancy in men Imaging
PET/CT imaging and RIT of prostate cancer Kirsten Bouchelouche, MD, DMSc PET & Cyclotron Unit Rigshospitalet, Copenhagen Denmark Prostate cancer Prostate cancer is the most common malignancy in men Imaging
Staging recurrent ovarian cancer with 18 FDG PET/CT
 ONCOLOGY LETTERS 5: 593-597, 2013 Staging recurrent ovarian cancer with FDG PET/CT SANJA DRAGOSAVAC 1, SOPHIE DERCHAIN 2, NELSON M.G. CASERTA 3 and GUSTAVO DE SOUZA 2 1 DIMEN Medicina Nuclear and PET/CT
ONCOLOGY LETTERS 5: 593-597, 2013 Staging recurrent ovarian cancer with FDG PET/CT SANJA DRAGOSAVAC 1, SOPHIE DERCHAIN 2, NELSON M.G. CASERTA 3 and GUSTAVO DE SOUZA 2 1 DIMEN Medicina Nuclear and PET/CT
Diffusion-Weighted Magnetic Resonance Imaging Detects Local Recurrence After Radical Prostatectomy: Initial Experience
 EUROPEAN UROLOGY 61 (2012) 616 620 available at www.sciencedirect.com journal homepage: www.europeanurology.com Case Study of the Month Diffusion-Weighted Magnetic Resonance Imaging Detects Local Recurrence
EUROPEAN UROLOGY 61 (2012) 616 620 available at www.sciencedirect.com journal homepage: www.europeanurology.com Case Study of the Month Diffusion-Weighted Magnetic Resonance Imaging Detects Local Recurrence
Assessment of Skeletal Metastases in Prostate Cancer: 68Ga-PSMA PET vs 99mTc-MDP WBBS - A Case Series
 Assessment of Skeletal Metastases in Prostate Cancer: 68Ga-PSMA PET vs 99mTc-MDP WBBS - A Case Series Poster No.: R-0094 Congress: 2016 ASM Type: Scientific Exhibit Authors: O. Bennett, Y.-T. T. Huang;
Assessment of Skeletal Metastases in Prostate Cancer: 68Ga-PSMA PET vs 99mTc-MDP WBBS - A Case Series Poster No.: R-0094 Congress: 2016 ASM Type: Scientific Exhibit Authors: O. Bennett, Y.-T. T. Huang;
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE
 PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE DISCLOSURES/CONFLICTS NONE OBJECTIVES Understand current diagnostic role
PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE DISCLOSURES/CONFLICTS NONE OBJECTIVES Understand current diagnostic role
Since the beginning of the prostate-specific antigen (PSA) era in the. Characteristics of Insignificant Clinical T1c Prostate Tumors
 era in the. Characteristics of Insignificant Clinical T1c Prostate Tumors") 2001 Characteristics of Insignificant Clinical T1c Prostate Tumors A Contemporary Analysis Patrick J. Bastian, M.D. 1 Leslie A. Mangold, B.A., M.S. 1 Jonathan I. Epstein, M.D. 2 Alan W. Partin, M.D., Ph.D.
2001 Characteristics of Insignificant Clinical T1c Prostate Tumors A Contemporary Analysis Patrick J. Bastian, M.D. 1 Leslie A. Mangold, B.A., M.S. 1 Jonathan I. Epstein, M.D. 2 Alan W. Partin, M.D., Ph.D.
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE. ELENA CASTRO Spanish National Cancer Research Centre
 VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Choline PET/CT for imaging prostate cancer: an update
 DOI 10.1007/s12149-013-0731-7 REVIEW ARTICLE Choline PET/CT for imaging prostate cancer: an update Kazuhiro Kitajima Robert C. Murphy Mark A. Nathan Received: 12 February 2013 / Accepted: 16 April 2013
DOI 10.1007/s12149-013-0731-7 REVIEW ARTICLE Choline PET/CT for imaging prostate cancer: an update Kazuhiro Kitajima Robert C. Murphy Mark A. Nathan Received: 12 February 2013 / Accepted: 16 April 2013
INDICATIONS AND USAGE
 1. INDICATIONS AND USAGE a) Axumin is indicated for positron emission tomography (PET) in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following
1. INDICATIONS AND USAGE a) Axumin is indicated for positron emission tomography (PET) in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following
Rare Small Cell Carcinoma in Genitourinary Tract: Experience from E-Da Hospital
 E-Da Medical Journal 20;():-5 Original Article Rare Small Cell Carcinoma in Genitourinary Tract: Experience from E-Da Hospital Wei-Ting Kuo, I-Wei Chang2, Kevin Lu, Hua-Pin Wang, Tsan-Jung u, Victor C.
E-Da Medical Journal 20;():-5 Original Article Rare Small Cell Carcinoma in Genitourinary Tract: Experience from E-Da Hospital Wei-Ting Kuo, I-Wei Chang2, Kevin Lu, Hua-Pin Wang, Tsan-Jung u, Victor C.
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Detection of recurrent prostate cancer with 18F-fluorocholine PET/CT in relation to PSA level at the time of imaging
 Ann Nucl Med (2012) 26:501 507 DOI 10.1007/s12149-012-0601-8 ORIGINAL ARTICLE Detection of recurrent prostate cancer with 18F-fluorocholine PET/CT in relation to PSA level at the time of imaging Sandi
Ann Nucl Med (2012) 26:501 507 DOI 10.1007/s12149-012-0601-8 ORIGINAL ARTICLE Detection of recurrent prostate cancer with 18F-fluorocholine PET/CT in relation to PSA level at the time of imaging Sandi
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
11C-Choline Pet/Ct in the Detection of Prostate Cancer Relapse in Patients After Radical Treatment With Psa Level < 10 Ng/Ml
 The 2nd International Symposium on Physics, Engineering and Technologies for Biomedicine Volume 2018 Corresponding Author: Diana Pursanova dmpursanova@bakulev.ru Received: 17 January 2018 Accepted: 25
The 2nd International Symposium on Physics, Engineering and Technologies for Biomedicine Volume 2018 Corresponding Author: Diana Pursanova dmpursanova@bakulev.ru Received: 17 January 2018 Accepted: 25
Phillip J. Koo, MD Division Chief of Diagnostic Imaging Banner MD Anderson Cancer Center, USA
 ADVANCED PET IMAGING IN PROSTATE CANCER Phillip J. Koo, MD Division Chief of Diagnostic Imaging Banner MD Anderson Cancer Center, USA PET, positron-emission tomography DISCLAIMER Please note: The views
ADVANCED PET IMAGING IN PROSTATE CANCER Phillip J. Koo, MD Division Chief of Diagnostic Imaging Banner MD Anderson Cancer Center, USA PET, positron-emission tomography DISCLAIMER Please note: The views
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
BJUI. Study Type Diagnostic (case series) Level of Evidence 4 OBJECTIVES
 Level of Evidence 4 OBJECTIVES") 2009 THE AUTHORS. JOURNAL COMPILATION 2009 BJU INTERNATIONAL Original Articles PET/CT FOR LYMPH NODE STAGING OF PATIENTS WITH PROSTATE CANCER POULSEN ET AL. BJUI BJU INTERNATIONAL [ 18 F]-fluorocholine
2009 THE AUTHORS. JOURNAL COMPILATION 2009 BJU INTERNATIONAL Original Articles PET/CT FOR LYMPH NODE STAGING OF PATIENTS WITH PROSTATE CANCER POULSEN ET AL. BJUI BJU INTERNATIONAL [ 18 F]-fluorocholine
Ga 68 -HBED- PSMA. A/ProfLouise Emmett St Vincent s Hospital Sydney
 Ga 68 -HBED- PSMA A/ProfLouise Emmett St Vincent s Hospital Sydney Glu-NH-CO-NH-Lys-(Ahx)- [68Ga(HBED-CC)] Prostate specific membrane antigen 35 pub-med publications 15 clinical 3 retrospective larger
Ga 68 -HBED- PSMA A/ProfLouise Emmett St Vincent s Hospital Sydney Glu-NH-CO-NH-Lys-(Ahx)- [68Ga(HBED-CC)] Prostate specific membrane antigen 35 pub-med publications 15 clinical 3 retrospective larger
Genitourinary Oncology Service, Department of Medicine, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, Box 444 New York, NY 10021, USA 2
 Editorial commentary 11 C-acetate PET imaging in prostate cancer Michael J. Morris 1, Howard I. Scher 2 1 Genitourinary Oncology Service, Department of Medicine, Memorial Sloan-Kettering Cancer Center,
Editorial commentary 11 C-acetate PET imaging in prostate cancer Michael J. Morris 1, Howard I. Scher 2 1 Genitourinary Oncology Service, Department of Medicine, Memorial Sloan-Kettering Cancer Center,
Does Imaging of Advanced PC change a suggested treatment?
 Does Imaging of Advanced PC change a suggested treatment? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict
Does Imaging of Advanced PC change a suggested treatment? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict
WHAT DOES PET IMAGING ADD TO CONVENTIONAL STAGING OF HEAD AND NECK CANCER PATIENTS?
 doi:10.1016/j.ijrobp.2006.12.044 Int. J. Radiation Oncology Biol. Phys., Vol. 68, No. 2, pp. 383 387, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
doi:10.1016/j.ijrobp.2006.12.044 Int. J. Radiation Oncology Biol. Phys., Vol. 68, No. 2, pp. 383 387, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
NIH Public Access Author Manuscript Diagn Imaging Eur. Author manuscript; available in PMC 2014 November 10.
 NIH Public Access Author Manuscript Published in final edited form as: Diagn Imaging Eur. 2013 January ; 29(1): 12 15. PET-directed, 3D Ultrasound-guided prostate biopsy Baowei Fei, Department of Radiology
NIH Public Access Author Manuscript Published in final edited form as: Diagn Imaging Eur. 2013 January ; 29(1): 12 15. PET-directed, 3D Ultrasound-guided prostate biopsy Baowei Fei, Department of Radiology
Radioligand imaging & treatment of prostate cancer
 Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
18 F, respectively, they become imaging markers of tissue sites. 18 F-choline PET/CTAC is well supported for recurrent disease, there
 ORIGINAL ARTICLE Prostate-Specific Antigen and Prostate-Specific Antigen Velocity as Threshold Indicators in C-Acetate PET/CTAC Scanning for Prostate Cancer Recurrence Reginald W. Dusing, MD,* Warner Peng,
ORIGINAL ARTICLE Prostate-Specific Antigen and Prostate-Specific Antigen Velocity as Threshold Indicators in C-Acetate PET/CTAC Scanning for Prostate Cancer Recurrence Reginald W. Dusing, MD,* Warner Peng,
PET-MRI in malignant bone tumours. Lars Stegger Department of Nuclear Medicine University Hospital Münster, Germany
 PET-MRI in malignant bone tumours Lars Stegger Department of Nuclear Medicine University Hospital Münster, Germany Content From PET to PET/MRI General considerations Bone metastases Primary bone tumours
PET-MRI in malignant bone tumours Lars Stegger Department of Nuclear Medicine University Hospital Münster, Germany Content From PET to PET/MRI General considerations Bone metastases Primary bone tumours
Diagnostic role of fluorodeoxyglucose positron emission tomography computed tomography in prostate cancer
 ONCOLOGY LETTERS 7: 2013-2018, 2014 Diagnostic role of fluorodeoxyglucose positron emission tomography computed tomography in prostate cancer YIYAN LIU Nuclear Medicine Service, Department of Radiology,
ONCOLOGY LETTERS 7: 2013-2018, 2014 Diagnostic role of fluorodeoxyglucose positron emission tomography computed tomography in prostate cancer YIYAN LIU Nuclear Medicine Service, Department of Radiology,
The European Board of Urology
 Page 1 of 15 The European Board of Urology Sub-specialty certification application: Prostate cancer, A - General information A1 - APPLICATION IDENTIFICATION 1a. Application code blank 1b. EBU internal
Page 1 of 15 The European Board of Urology Sub-specialty certification application: Prostate cancer, A - General information A1 - APPLICATION IDENTIFICATION 1a. Application code blank 1b. EBU internal
Bone PET/MRI : Diagnostic yield in bone metastases and malignant primitive bone tumors
 Bone PET/MRI : Diagnostic yield in bone metastases and malignant primitive bone tumors Lars Stegger, Benjamin Noto Department of Nuclear Medicine University Hospital Münster, Germany Content From PET to
Bone PET/MRI : Diagnostic yield in bone metastases and malignant primitive bone tumors Lars Stegger, Benjamin Noto Department of Nuclear Medicine University Hospital Münster, Germany Content From PET to
Prostate Cancer Basics: Background Information for Outreach Activities with Oncologists, Urologists and Surgeons
 Prostate Cancer Basics: Background Information for Outreach Activities with Oncologists, Urologists and Surgeons Legal Disclaimer These materials were prepared in good faith by MITA as a service to the
Prostate Cancer Basics: Background Information for Outreach Activities with Oncologists, Urologists and Surgeons Legal Disclaimer These materials were prepared in good faith by MITA as a service to the
Whole body F-18 sodium fluoride PET/CT in the detection of bone metastases in patients with known malignancies: A pictorial review
 Whole body F-18 sodium fluoride PET/CT in the detection of bone metastases in patients with known malignancies: A pictorial review Poster No.: C-1196 Congress: ECR 2014 Type: Educational Exhibit Authors:
Whole body F-18 sodium fluoride PET/CT in the detection of bone metastases in patients with known malignancies: A pictorial review Poster No.: C-1196 Congress: ECR 2014 Type: Educational Exhibit Authors:
Consequence of the introduction of routine FCH PET/CT imaging for patients with prostate cancer: a dual centre survey
 20 research article Consequence of the introduction of routine FCH PET/CT imaging for patients with prostate cancer: a dual centre survey Marina Hodolic 1, Laure Michaud 2,3, Virginie Huchet 2, Sona Balogova
20 research article Consequence of the introduction of routine FCH PET/CT imaging for patients with prostate cancer: a dual centre survey Marina Hodolic 1, Laure Michaud 2,3, Virginie Huchet 2, Sona Balogova
Radioimmunoscintigraphy (Monoclonal Antibody Imaging) With Indium 111 Capromab Pendetide for Prostate Cancer
 With Indium 111 Capromab Pendetide for Prostate Cancer") Last Review Status/Date: December 2016 Page: 1 of 9 Antibody Imaging) With Indium 111 Capromab Description Radioimmunoscintigraphy (RIS) involves the administration of radiolabeled monoclonal antibodies
Last Review Status/Date: December 2016 Page: 1 of 9 Antibody Imaging) With Indium 111 Capromab Description Radioimmunoscintigraphy (RIS) involves the administration of radiolabeled monoclonal antibodies
How to deal with patients who fail intracavitary treatment
 How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
Elevated PSA. Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017
 Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Low risk. Objectives. Case-based question 1. Evidence-based utilization of imaging in prostate cancer
 Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice
 european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
Sensitivity and specificity of PET/CT regarding the detection of lymph node metastases in prostate cancer recurrence
 Osmonov et al. SpringerPlus 2014, 3:340 a SpringerOpen Journal RESEARCH Open Access Sensitivity and specificity of PET/CT regarding the detection of lymph node metastases in prostate cancer recurrence
Osmonov et al. SpringerPlus 2014, 3:340 a SpringerOpen Journal RESEARCH Open Access Sensitivity and specificity of PET/CT regarding the detection of lymph node metastases in prostate cancer recurrence
Austin Radiological Association Nuclear Medicine Procedure PROSTATE CANCER STUDY (In-111-Capromab Pendetide [ProstaScint ])
![Austin Radiological Association Nuclear Medicine Procedure PROSTATE CANCER STUDY (In-111-Capromab Pendetide [ProstaScint ])](/thumbs/81/82771892.jpg "Austin Radiological Association Nuclear Medicine Procedure PROSTATE CANCER STUDY (In-111-Capromab Pendetide [ProstaScint ])") Austin Radiological Association Nuclear Medicine Procedure PROSTATE CANCER STUDY (In-111-Capromab Pendetide [ProstaScint ]) Overview Indications The Prostate Cancer Study with an indium-111 labeled murine
Austin Radiological Association Nuclear Medicine Procedure PROSTATE CANCER STUDY (In-111-Capromab Pendetide [ProstaScint ]) Overview Indications The Prostate Cancer Study with an indium-111 labeled murine
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps?
 Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
PET in Prostate Cancer
 PET in Prostate Cancer Tom R. Miller, M.D., Ph.D. Mallinckrodt Institute of Radiology Washington University School of Medicine St. Louis, Missouri, USA Prostate Imaging Bone Scintigraphy primarily for
PET in Prostate Cancer Tom R. Miller, M.D., Ph.D. Mallinckrodt Institute of Radiology Washington University School of Medicine St. Louis, Missouri, USA Prostate Imaging Bone Scintigraphy primarily for
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
POSITRON EMISSION TOMOGRAPHY (PET)
") Status Active Medical and Behavioral Health Policy Section: Radiology Policy Number: V-27 Effective Date: 08/27/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Radiology Policy Number: V-27 Effective Date: 08/27/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Bone Scanning Who Needs it Among Patients with Newly Diagnosed Prostate Cancer?
 Bone Scanning Who Needs it Among Patients with Newly Diagnosed Prostate Cancer? Megumi Hirobe 1, Atsushi Takahashi 1, Shin-ichi Hisasue 1, Hiroshi Kitamura 1, Yasuharu Kunishima 1, Naoya Masumori 1, Akihiko
Bone Scanning Who Needs it Among Patients with Newly Diagnosed Prostate Cancer? Megumi Hirobe 1, Atsushi Takahashi 1, Shin-ichi Hisasue 1, Hiroshi Kitamura 1, Yasuharu Kunishima 1, Naoya Masumori 1, Akihiko
Case Report An Incidental Finding of Mucinous Colon Cancer by. Clinical Management of a Patient with Recurrent Prostate Adenocarcinoma
 Case Reports in Oncological Medicine, Article ID 297031, 4 pages http://dx.doi.org/10.1155/2014/297031 Case Report An Incidental Finding of Mucinous Colon Cancer by 18 F-Choline PET/CT Determining a Change
Case Reports in Oncological Medicine, Article ID 297031, 4 pages http://dx.doi.org/10.1155/2014/297031 Case Report An Incidental Finding of Mucinous Colon Cancer by 18 F-Choline PET/CT Determining a Change
In recent years PET has undergone explosive growth and
 Positron Emission Tomography and Positron Emission Tomography/Computerized Tomography of Urological Malignancies: An Update Review Kirsten Bouchelouche* and Peter Oehr From the Positron Emission Tomography
Positron Emission Tomography and Positron Emission Tomography/Computerized Tomography of Urological Malignancies: An Update Review Kirsten Bouchelouche* and Peter Oehr From the Positron Emission Tomography
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Molecular Imaging in Prostate Cancer. Carlos Artigas Nuclear Medicine Institut Jules Bordet
 Molecular Imaging in Prostate Cancer Carlos Artigas Nuclear Medicine Institut Jules Bordet Introduction 3 different stages of the disease Local treatment with curative intent Introduction 3 different stages
Molecular Imaging in Prostate Cancer Carlos Artigas Nuclear Medicine Institut Jules Bordet Introduction 3 different stages of the disease Local treatment with curative intent Introduction 3 different stages
Financial and Other Disclosures
 Financial and Other Disclosures Off-label use of drugs, devices, or other agents: None Data from IRB-approved human research is not presented I have the following financial interests or relationships to
Financial and Other Disclosures Off-label use of drugs, devices, or other agents: None Data from IRB-approved human research is not presented I have the following financial interests or relationships to
Triage of Limited Versus Extensive Disease on 18 F-FDG PET/CT Scan in Small Cell lung Cancer
 Triage of Limited Versus Extensive Disease on F-FDG PET/CT Scan in Small Cell lung Cancer Riaz Saima 1*, Bashir Humayun 1, Niazi Imran Khalid 2 1 Department of Nuclear Medicine, Shaukat Khanum Memorial
Triage of Limited Versus Extensive Disease on F-FDG PET/CT Scan in Small Cell lung Cancer Riaz Saima 1*, Bashir Humayun 1, Niazi Imran Khalid 2 1 Department of Nuclear Medicine, Shaukat Khanum Memorial
PSMA PET in patients with prostate cancer
 PSMA PET in patients with prostate cancer Thomas Hope, MD Assistant Professor of Radiology, UCSF Abdominal Imaging and Nuclear Medicine Co-director, PET/MRI Chief of MRI, San Francisco VA Medical Center
PSMA PET in patients with prostate cancer Thomas Hope, MD Assistant Professor of Radiology, UCSF Abdominal Imaging and Nuclear Medicine Co-director, PET/MRI Chief of MRI, San Francisco VA Medical Center
Alberto Briganti, M.D., PhD
 Alberto Briganti, M.D., PhD Professore Orinario di Urologia IRCCS San Raffaele Divisione di Oncologia / Unità di Urologia Urological Research Institute (URI) Università Vita-Salute San Raffaele, Milano
Alberto Briganti, M.D., PhD Professore Orinario di Urologia IRCCS San Raffaele Divisione di Oncologia / Unità di Urologia Urological Research Institute (URI) Università Vita-Salute San Raffaele, Milano
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
10/30/2018. Martha K. Terris, MD Witherington Distinguished Professor and Chair Medical College of Georgia Urology November 5, 2018
 Martha K. Terris, MD Witherington Distinguished Professor and Chair Medical College of Georgia Urology November 5, 2018 Elevated PSA and/or nodule on digital rectal examination Prostate biopsies If initial
Martha K. Terris, MD Witherington Distinguished Professor and Chair Medical College of Georgia Urology November 5, 2018 Elevated PSA and/or nodule on digital rectal examination Prostate biopsies If initial
Imaging of prostate cancer local recurrences : why and how?
 Imaging of prostate cancer local recurrences : why and how? Olivier Rouvière Department of Urinary and Vascular Imaging Hospices Civils de Lyon Lyon - France 1. Preliminary Remarks Preliminary Remarks
Imaging of prostate cancer local recurrences : why and how? Olivier Rouvière Department of Urinary and Vascular Imaging Hospices Civils de Lyon Lyon - France 1. Preliminary Remarks Preliminary Remarks
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to