DISCLOSURES. This program meets the requirements for GI specific Category 1 contact hours. M
|
|
|
- Leslie Harmon
- 5 years ago
- Views:
Transcription
1 DISCLOSURES Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest: Planners disclose no conflict of interest; the speaker discloses a relationship with the supporting company. The speaker has signed a statement agreeing to present information fairly and without bias. Commercial company support: Fees are underwritten by education funding provided by Covidien-GI Solutions. Non-commercial company support: None. Alternative or Complementary Therapy: None. This program meets the requirements for GI specific Category 1 contact hours. 1

2 DIAGNOSIS AND TREATMENT 2
3 EXPECTED OUTCOMES The Nurses will have increased knowledge on the disease state and treatment options for Barrett s esophagus, thus being better prepared for patient education and teaching Nurses will be better informed regarding the latest techniques for endoscopic eradication therapies 3
4 OBJECTIVES Describe the disease process for Barrett's esophagus Contrast various approaches to managing Barrett s esophagus 4
 Metaplasia = change in cell-type")
: 175 82 Allison PR, Johnstone AS (June 1953). The oesophagus lined with gastric mucous membrane. Thorax 8 (2): 87 101.")
5 BARRETT S ESOPHAGUS INTESTINAL METAPLASIA Image source of Professor N. Barrett internet search public domain. First described by Professor Norman Barrett in 1950 as a tubular portion of stomach being trapped in the chest Related to the esophagus in 1953 (Allison/Johnstone) Metaplasia = change in cell-type Prof. Norman Barrett Intestinal Metaplasia is when the esophageal squamous cells change to specialized intestinal cells Barrett NR (October 1950). "Chronic peptic ulcer of the oesophagus and 'esophagitis'". Br J Surg 38 (150): Allison PR, Johnstone AS (June 1953). The oesophagus lined with gastric mucous membrane. Thorax 8 (2): Barrett NR (June 1957). "The lower esophagus lined by columnar epithelium". Surgery 41 (6): Spechler SJ, Goyal RK (February 1996). "The columnar-lined esophagus, intestinal metaplasia, and Norman Barrett". Gastroenterology 110 (2):


6 WHAT IS BARRETT S ESOPHAGUS? Image: ablation1.jpg Image: 6
7 WHAT IS GASTROESOPHAGEAL REFLUX DISEASE GERD? Chronic heartburn (GERD symptom) is a physical condition Inability of the lower esophageal sphincter (LES) to prevent reflux of acid from the stomach into the esophagus Causative factor of Barrett s Esophagus Image: 7
8 CAUSE OF INTESTINAL METAPLASIA BARRETT S ESOPHAGUS A response to chronic exposure of gastric acid Cells of the esophageal lining undergo changes in organization Results in formation of Intestinal Metaplasia (Barrett s esophagus) 8
9 ESOPHAGEAL HISTOLOGY Esophageal Epithelium ~500µm Lamina Propria Muscularis Mucosae ~1000µm Submucosa Muscularis Propria Image: 9
 Fleischer DE, Odze R, et al. The Case for Endoscopic Treatment of Non-dysplastic and Low-Grade Dysplastic Barrett s Esophagus, Dig Dis Sci DOI 10.")
10 STAGES OF BARRETT S ESOPHAGUS Non Dysplastic Intestinal Metaplasia (NDIM) Indefinite Low-Grade Dysplasia High-Grade Dysplasia Barrett s Esophagus left untreated could lead to Intramucosal Carcinoma (Adenocarcinoma) Fleischer DE, Odze R, et al. The Case for Endoscopic Treatment of Non-dysplastic and Low-Grade Dysplastic Barrett s Esophagus, Dig Dis Sci DOI /s

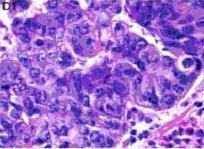
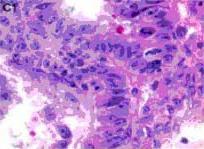
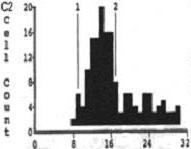
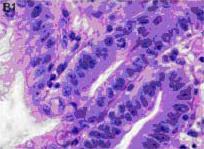
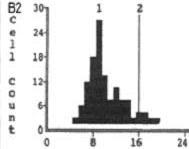
11 CAN YOU TELL WHAT STAGE THESE HISTOLOGY SLIDES SHOW? Inter-observer agreement is moderate at best, and in some studies it is poor It s called discordance For the diagnosis for Barrett s with dysplasia, it is recommended that two pathologist should agree or bring in a third to concur Non-dysplastic Low-grade dysplasia High-grade dysplasia Adenocarcinoma Fleischer DE, Odze R, et al. The Case for Endoscopic Treatment of Non-dysplastic nd Low-Grade Dysplastic Barrett s Esophagus, Dig Dis Sci DOI /s Image from: Huang Q, et al. BMC Clin Pathol Aug 12;5:7




12 BARRETT S ESOPHAGUS AND ASSOCIATED RISK LEVEL Esophageal Adenocarcinoma 1.4 % per patient per year (IM to HGD and EAC) High-Grade Dysplasia 6.6% per patient per year (HGD to EAC) Low-Grade Dysplasia 1.7% per patient per year (LGD to EAC) 4.0% per patient per year (IM to LGD) Non- Dysplastic 0.5% per patient per year (IM to EAC) 0.9% per patient per year (IM to HGD )

")



13 EVOLUTION OF BARRETT S AND CANCER Squamous esophagus Injury Acid & bile reflux nitrous oxide Chronic inflammation Barrett's metaplasia Genetics Gender, race, & other factors (cox-2) Low-grade dysplasia High-grade dysplasia Invasive Adenocarcinoma Accumulate Genetic Changes Morales CP et al. Lancet 2002; 360: Sharma P, Falk GW, Weston AP, et al. Dysplasia and cancer in a large multicenter cohort of patients with Barrett s esophagus. Clin Gastroenterol Hepatol 2006; 4:


14 DID YOU KNOW THAT BARRETT S AND A COLON POLYP HAVE SOMETHING IN COMMON? Barrett s 0.5%/patient/year cancer 0.9%/patient/year HGD Colon Polyp 0.5%/patient/year cancer 7.5M colonoscopies/year Sharma P, Falk GW, Weston AP, Reker D, Johnston M, Sampliner RE. Dysplasia and Cancer in a Large Multicenter Cohort of Patients with Barrett s Esophagus. Clinical Gastroenterology and Hepatology 2006;4:
15 RELATIVE CHANGE IN ESOPHAGEAL ADENOCARCINOMA INCIDENCE Esophagus Melanoma Prostate Lung/Breast Colorectal From: Pohl H, Welch HG. Natl Cancer Inst

16 DEMOGRAPHICS OF BARRETT S ESOPHAGUS About 13% of Caucasian men over age 50 who have chronic reflux GERD will develop Barrett's esophagus A study by the Veteran Affairs Healthcare System and Stanford University found that 25% of patients over 50 without GERD symptoms had Barrett's esophagus Westhoff B, Brotze S, Weston A, et al. The frequency of Barrett s esophagus in high-risk patients with chronic gerd. Gastrointestinal Endosc. 2005; 61: Gerson LB, Shetler K, and Triadafilopoulos G. Prevalence of Barrett s esophagus in asymptomatic individuals. Gastroenterology 2002;123:
 Ronkainen J, et al. Prevalence of BE Gastroenterology 2005;129:1825-31.")
...ddw 2009. Hayeck TJ, et al.")
 Rex DK, et al. Screening for Barrett s.")
17 BARRETT S PREVALENCE ESTIMATES 1.6% of general adult population (3.3 M) Ronkainen J, et al. Prevalence of BE Gastroenterology 2005;129: % 5.6% of general adult population ( M) Tristan J, et al. The Prevalence of BE in the US (model)...ddw Hayeck TJ, et al. The Prevalence of BE in the US (model) Dis Esophagus 2010;23: % of persons over age 40 (8.7 M) Rex DK, et al. Screening for Barrett s... Gastroenterology 2003; 125:
18 THREE MANAGEMENT STRATEGIES FOR BARRETT S ESOPHAGUS 1. Surveillance and Medical Management 2. Surgery and or Endoscopic Mucosal Resection 3. Ablation: Destroy the abnormal cells to allow normal squamous cells to re-populate. A. Chemical Photodynamic Therapy APC B. Freezing C. Thermal Cryotherapy Circumferential and Focal RFA Sharma P. Strategies and recommendations for diagnosing and managing Barrett's esophagus Dec 31, 2009 New England Journal of Medicine. 18


19 SURVEILLANCE Technique: AGA recommends the Seattle protocol Four quadrants every 1cm-2 cm through the Intestinal Metaplasia visible areas Intervals: Based on pathology of : dysplasia months or non-dysplasia 3-5 years Goal: The early detection of dysplasia and early cancer Limitations: Does not remove Barrett s, and increases patient anxiety Samples only 4-6% of esophagus Sampling errors and pathology discordance Surveillance intervals are arbitrary and have never been subject to a clinical trial. Endoscopic Surveillance, 2005 ClevelandClinic.org, The Cleveland Clinic, 9 August 2005 < 19

20 HUMAN ESOPHAGUS Esophageal mucosa Biopsy depth Submucosa with esophageal G glands G Muscularis mucosa Muscularis propria. Image: Prateek Sharma, M.D.. N Engl J Med 361;26 NEJM.org December 24,



21 Reserved for patients with high-grade dysplasia and cancer Definitive therapy Operative mortality rate of 3-12% Rate of serious operative complications of 30-50%. Luna RA, Gilbert E, Hunter JG. High-grade dysplasia and intramucosal adenocarcinoma in Barrett's esophagus: the role of esophagectomy in the era of endoscopic eradication therapy. Curr Opin Gastroenterol 2012;28: Markar SR, Karthikesalingam A, Low DE. Outcomes assessment of the surgical management of esophageal cancer in younger and older patients. Ann Thorac Surg 2012;94:
22 ENDOSCOPIC MUCOSAL RESECTION (EMR) Indications Focal, raised lesion(s) Larger areas suspicious for malignancy Complement to other therapies Goal: Remove lesion(s) so the tissue can be examined under a microscope to determine if all of the cancer (or dysplasia) has been removed. 22





23 ENDOSCOPIC MUCOSAL RESECTION (EMR) One Technique: Several Techniques The focal EMR is done using a small cap that has a small wire loop that fits on the end of the endoscope. The nodule is suctioned into the cap and the wire loop is closed while cautery is applied. Step 1: Injection of Target Lesion Step 2: Positioning the Snare Step 3: Suction and Snare of Lesion Images: Second Technique: The focal EMR is done using a small ligation band, followed by a cautery loop The cautery loop is around the nodule and energy applied. Once the nodule is released from the mucosal wall, it is retrieved in the usual fashion. Images; 23

24 ENDOSCOPIC MUCOSAL RESECTION (EMR) Advantages:I Enables evaluation of changes in diseased tissue Can be used to obtain large biopsies for diagnosis and local tumor staging Frequently reveals more advanced tumor stages Often recommended in combination with additional ablation techniques Limitations and possible complications Creates a scarring effect If done circumferentially EMR has up to an 88% chance of causing a stricture mages: van Vilsteren FG, et al. Stepwise radical endoscopic resection versus radiofrequency ablation for Barrett s oesophagus with high-grade dysplasia or early cancer: a multicentre randomized trial.gut, epub January
25 HUMAN ESOPHAGUS Esophageal Mucosa Image: Submucosa with esophageal G glands G Muscularis mucosa EMR Depth Radical EMR CR-D : 100% CR-IM : 92% Strictures: 88% # Therapeutic Sessions: 6 Muscularis propria Esophagectomy Operative mortality rate of 3-12% Rate of serious operative complications of 30-50%. Surgical Depth van Vilsteren FG, et al. Stepwise radical endoscopic resection versus radiofrequency ablation for Barrett s oesophagus with high-grade dysplasia or early cancer: a multicentre randomized trial. Gut, epub January
26 Indications ARGON PLASMA COAGULATION Focal area of Barrett s (NDIM) Goal: Remove the Barrett s lesion Technique: Utilizes an argon gas device that employs chemical energy Through a hand-held device, it creates an electrical arc on the tissue to a specific focal area Advantages: Hand held Small focal areas Image: oal+resection++photos&qpvt=endoscopic Limitations and possible complications Technically demanding Non-uniform ablation effect User variability Buried glands Anatomy of distal esophagus not considered, its not round 26
27 HUMAN ESOPHAGUS Esophageal mucosa Image: APC Submucosa with esophageal G glands G Muscularis mucosa) Varied results CR-IM: 42%-98% Strictures: 2.9%-10% Persistent Buried Barrett's (SSIM): 8%- 30% Muscularis propria Multiple cases of adenocarcinoma arising under the squamous reepithelialization have been observed after APC. Deviere J. Argon plasma coagulation therapy for ablation of Barrett s oesophagus Gut December; 51(6): Menon et al. Endoscopic treatments for Barrett s esophagus: a systematic review of safety and effectiveness compared to esophagectomy BMC Gastroenterology 2010, 10:


28 Indications Goal: PHOTODYNAMIC THERAPY High-Grade Dysplasia (HGD) Barrett's esophagus Eliminate HGD using an endoscopic therapy rather than surgical esophagectomy PDT Technique: A. Photosensitizer drug given intravenously B. Affected esophagus exposed to non-ablative laser light for ~12 minutes B. Oxygen free radicals induced in high light dose areas C. Free radicals induce cell death Images: Overholt BF, Lightdale CJ, Wang KK et al. Photodynamic therapy with porfimer sodium for ablation of high-grade dysplasia in Barrett's esophagus: international, partially blinded, randomized phase III trial. Gastrointestinal Endoscopy, 2005,62(4);
29 HUMAN ESOPHAGUS Esophageal mucosa Image: PDT Submucosa with esophageal G glands G Muscularis mucosa Meta Analysis of 101 studies CR-IM: 51.6% CR-D: 77.5% Strictures: 18.5% Buried Barrett s (SSIM): 14.2% Muscularis propria Photosensitivity: 26.4% Menon et al. Endoscopic treatments for Barrett s esophagus: a systematic review of safety and effectiveness compared to esophagectomy BMC Gastroenterology 2010, 10:111 Gray NA, Odze RD, Spechler SJ., Buried metaplasia after Endoscopic Ablation n of Barrett's Esophagus: a Systematic Review. AM J Gastroenterology, 2011 Aug 9, doi /aja 2011: 255[epub ahead of print] 29
 Strictures that are stenotic and fibrotic Photosensitivity Chest pain")

30 Advantages: PDT Photodynamic therapy was the first treatment to have been shown to significantly decrease high-grade dysplasia and cancer in patients with Barrett s esophagus Limitations and possible complications Its use has been limited, primarily because of its costs and side effects Subsquamous Barrett's (buried glands) Strictures that are stenotic and fibrotic Photosensitivity Chest pain Nausea Vomiting Photosensitivity Stricture Subsquamous Barrett s Wang KK, Nijhawan PK. Complications of photodynamic therapy in gastrointestinal disease. Gastrointest Endosc Clin N Am 2000; 10: Overholt BF, Lightdale CJ, Wang KK et al. Photodynamic therapy with porfimer sodium for ablation of high-grade dysplasia in Barrett's esophagus: international, partially blinded, randomized phase III trial. Gastrointestinal Endoscopy, 2005,62(4);
 it will remove the abnormal cells and allow")

31 Indications Goal: Barrett's esophagus with high-grade dysplasia and persistent low-grade dysplasia Early stage esophageal cancer not amenable to standard therapies including surgery, chemotherapy, and radiation therapy By freezing the tissues using extreme cold, (-196 Celsius) it will remove the abnormal cells and allow re-growth of new, healthy cells in their place. Technique: CRYOTHERAPY There are currently two different types of cryotherapy available Rapid flow of CO 2 or liquid nitrogen Sprayed to the affected esophageal lining Repeat treatments necessary 3 up to 8 times reported Images: websites for CSA and GI Supply CSA Website accessed
32 HUMAN ESOPHAGUS Ablation Target Nicholas J. Shaheen, MD, MPH, et al. Safety and efficacy of endoscopic spray cryotherapy for Barrett s esophagus with high-grade dysplasia. Gastrointest Endosc April ; 71(4): doi: /j.gie CRYOTHERAPY One retrospective study of 98 patients reported 60 patients completed the therapy 58 patients had complete response to removing HGD=97%, BUT Submucosa with esophageal G glands G Muscularis mucosa) of those, 52 of them had showed only downgrading of histology: 87% HGD to Non-Dysplastic, not a complete removal of disease. Muscularis propria 34 patients had a completed response to Intestinal metaplasia= 57%. Did not achieve CR-IM in all patients or remove all of the Barrett s Image: 32

33 Advantages: CRYOTHERAPY Able to treat large, or stricture areas Coating of ice creates a whitened appearance Thru the scope device Limitations and possible complications: User variability Gastric distention Limited support in the 2011 AGA position statement Limited data, no RCT Image: AGA Institute Medical Position Panel, Gastro,



34 RADIOFREQUENCY CIRCUMFERENTIAL AND FOCAL ABLATION Fleischer DE et al. Endoscopic Ablation of BE a multicenter study with 2.5 year follow-up GIE 2007 Fleischer DE, et al. Endoscopic Radiofrequency Ablation for Barrett s Esophagus: Five-Year Durability Outcomes from a Prospective Multi-Center Trial. GIE Indications Goal: Barrett s esophagus Non-nodular, NDIM, LGD and HGD Delivery of ablative energy in less than 1 second allows long or short segments of Barrett s to be treated quickly Consistent application of bipolar energy uniformly removes the esophageal epithelium, reducing potential for buried glands and improving patient tolerability Controlled treatment depth of less than 1,000 μm reduces risk of stricture formation Shaheen NJ, et al. Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med May 28;360(22):



35 RADIOFREQUENCY CIRCUMFERENTIAL AND FOCAL ABLATION Technique: Endoscopic evaluation of Barrett s extent Size Ablate with visual placement Clean Repeat 35
36 HUMAN ESOPHAGUS RFA resulted in complete eradication of disease in 98% of NDBE patients, with 2.5-years follow-up. At 5 years, 92% of patients maintained durable cure, and no patients demonstrated neoplastic progression. Rigorous RCT Dysplasia (per protocol) CR-IM: 83% CR-LGD: 95% CR-HGD: 90% Strictures: 1.7% procedures Published in the NEJM Durability 91 to 98% dysplasia & IM eradication rate at 2 & 3 yrs. 90+ publications Ablation Target Submucosa with esophageal G glands Muscularis propria Image: G Circumferential and Focal RFA Controlling ablation depth minimizes complications Muscularis mucosa (Ablation Target Depth) Fleischer DE et al. Endoscopic Ablation of BE a multicenter study with 2.5 year follow-up GIE 2007 Fleischer DE, et al. Endoscopic Radiofrequency Ablation for BE: Five-Year Durability Outcomes from a Prospective Multi-Center Trial. GIE 2010 Shaheen NJ, et al. Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med May 28;360(22): Shaheen, et al. Durability of Radiofrequency Ablation in Barrett s Esophagus with Dysplasia. Gastroenterology


37 RADIOFREQUENCY ABLATION Limitations and possible complications Therapeutic procedural time (28-36 minutes for Circumferential and minutes for Focal) versus diagnostic time of EGD (~20 minutes) Multiple intubations Possible mucosal laceration, esophageal stricture and minor acute bleeding Advantages: Automated energy delivery No user variability Controlled depth of ablation extent to ~ μm 90+ clinical publications Safety and efficacy to 5 years Clinical reports of > 90% CR-IM and CR-D Post-RFA: 2-5 years Fleischer DE,et al. Endoscopic Ablation of BE a multicenter study with 2.5 year follow-up GIE Fleischer DE, et al. Endoscopic Radiofrequency Ablation for BE: Five-Year Durability Outcomes from a Prospective Multi-Center Trial. GIE 2010 Shaheen NJ, Sharma P, Overholt BF, et al. Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med May 28;360(22): Baseline Circumferential ablation 37
38 HUMAN ESOPHAGUS Ablation Target Circumferential and Focal RFA APC, PDT, CRYO Submucosa with esophageal G glands G Controlling ablation depth minimizes complications EMR Depth Muscularis propria Muscularis mucosa (Ablation Target Depth) Surgical Depth Image: 38
 Surgery remains option for HGD and IMC NDBE, IND, LGD may be effectively eradicated with RFA (Level I")
39 SOCIETY OF AMERICAN GASTROINTESTINAL AND ENDOSCOPIC SURGEONS (SAGES) GUIDELINES Guideline for surgical treatment of GERD Includes section on BE management with evidence grading HGD and IMC can be managed with RFA ± EMR for eradication of lesion and reduction in cancer (Level I evidence) Surgery remains option for HGD and IMC NDBE, IND, LGD may be effectively eradicated with RFA (Level I evidence) Anti-reflux surgery for GERD may be performed in patients with NDBE, IND, LGD in conjunction with endoscopic eradication therapy (i.e., before, during, after RFA) Source: 39

40 THE 2011 AGA MEDICAL POSITION STATEMENT SUGGESTS RFA AS AN OPTION FOR BARRETT S ESOPHAGUS PATIENTS AGA Medical Position Statement (Gastroenterology 2011;140: ) HGD: Endotherapy with RFA, PDT, or EMR is recommended rather than surveillance LGD: RFA should be a therapeutic option for treatment of patients with confirmed LGD NDBE: RFA with or without EMR should be a therapeutic option for select individuals with NDBE who are judged to be at increased risk for progression to HGD or cancer AGA Institute Medical Position Panel, Gastro,

41 Non-Dysplastic BE Management: Endoscopic ablation therapy may be a preferred management option in select patients with NDBE, such as those with a family history of EAC. Progression Risk Factors: Risk factors for BE and EAC include male sex, white race, age older than 50 years, family history of BE, increased duration of reflux symptoms, smoking, and obesity. 41 ASGE Standards of Practice Committee. Guideline - Role of endoscopy in BE and other premalignant conditions of the esophagus. GIE 2012

42 Low-Grade Dysplasia Management: Ablation as an alternative to surveillance should be considered and discussed with these patients. High-Grade Dysplasia Management: We recommend that eradication with endoscopic resection or RFA be considered for flat HGD ASGE Standards of Practice Committee. Guideline - Role of endoscopy in BE and other premalignant conditions of the esophagus. GIE


43 If Barrett s ablation therapy is safe and efficacious, we predict it will and possibly should become a routine response to the discovery of Barrett s esophagus, just as polypectomy is to the discovery of a colorectal polyp. (El-Serag, Graham. Gastroenterology, 2010) Barrett's esophagus Colon Polyp 43
44 CONCLUSION OF MODULE This concludes the CNE educational activity Understanding Barrett's Esophagus. Please turn in your completed evaluations. 44
45 ACCREDITATION Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation. One contact hour will be awarded to participants successfully completing the entire activity, including any question and answer session. Provider approved by: California Board of Registered Nursing, Provider Number District of Columbia Board of Nursing, Provider Number Florida Board of Registered Nursing, Provider Number Iowa Board of Nursing, Provider Number 317 West Virginia Board of Examiners for Registered Professional Nurses, Provider Number WV R 45
46 SOURCE LIST Allison PR, Johnstone AS (June 1953). The oesophagus lined with gastric mucous membrane. Thorax 8 (2): Barrett NR (October 1950). "Chronic peptic ulcer of the oesophagus and 'esophagitis'". Br J Surg 38 (150): Barrett NR (June 1957). "The lower esophagus lined by columnar epithelium". Surgery 41 (6): Cadiere GB, Rajan A. Rqibate M, et al. Endoluminal fundoplication (ELF) evolution of Esophyx, a new surgical device for transoral surgery. Minim Invasive Therapy Allied Technology. 2006; 15: Deviere J. Argon plasma coagulation therapy for ablation of Barrett s oesophagus Gut December; 51(6): Eisen GM. Ablation therapy for Barrett's esophagus. Gastrointestinal Endosc. 2003; 58: Fastest Rising Form of Cancer in the U.S. Webmd.com WebMD. Accessed October Fleischer DE et al. Endoscopic Ablation of BE a multicenter study with 2.5 year follow-up GIE Fleischer DE, et al. Endoscopic Radiofrequency Ablation for BE: Five-Year Durability Outcomes from a Prospective Multi- Center Trial. Gastrointest Endosc 2010;71:AB Fleischer DE, Odze R, et al. The Case for Endoscopic Treatment of Non-dysplastic and Low-Grade Dysplastic Barrett s Esophagus, Dig Dis Sci DOI /s Gerson LB, Shetler K, and Triadafilopoulos G. Prevalence of Barrett s esophagus in asymptomatic individuals. Gastroenterology 2002;123: Gray NA, Odze RD, Spechler SJ., Buried metaplasia after Endoscopic Ablation of Barrett's Esophagus: a Systematic Review. AM J Gastroenterology, 2011 Aug 9, doi /aja 2011: 255[epub ahead of print] 46
47 SOURCE LIST Heiko Pohl and H.G. Welch. The role of over diagnosis and reclassification in the Marked Increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005: 97: Luna RA, Gilbert E, Hunter JG. High-grade dysplasia and intramucosal adenocarcinoma in Barrett's esophagus: the role of esophagectomy in the era of endoscopic eradication therapy. Curr Opin Gastroenterol 2012;28: Markar SR, Karthikesalingam A, Low DE. Outcomes assessment of the surgical management of esophageal cancer in younger and older patients. Ann Thorac Surg 2012;94: Menon et al. Endoscopic treatments for Barrett s esophagus: a systematic review of safety and effectiveness compared to esophagectomy BMC Gastroenterology 2010, 10:111 Morales CP et al Hallmarks of CA progression in BO, Lancet 2002 Overholt BF, Lightdale CJ, Wang KK et al. Photodynamic therapy with porfimer sodium for ablation of high-grade dysplasia in Barrett's esophagus: international, partially blinded, randomized phase III trial. Gastrointestinal Endoscopy, 2005,62(4); Pohl H, Welch HG. Natl Cancer Inst 2005 Pouw RE, Gondrie JJ, Rygiel AM, et al. Properties of the neosquamous epithelium after radiofrequency ablation of Barrett s esophagus containing neoplasia. Am J Gastroenterol 2009;104:
48 SOURCE LIST Reid B.J and Weinstein W. M. Barrett's esophagus and adenocarcinoma. Gastroenterology Clinics of North America 1987; 38: Ronkainen J, Aro P, Storskrubb T, et al. Prevalence of Barrett s esophagus in the general population: an endoscopic study. Gastroenterology 2005; 129: Shaheen N, Ransohoff DF. Gastroesophageal reflux, Barrett s esophagus and esophageal cancer. Journal of the American Medical Association. 2002; 287: Shaheen NJ, Sharma P, Overholt BF, et al. Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med May 28;360(22): Shaheen, et al. Durability of Radiofrequency Ablation in Barrett s Esophagus with Dysplasia. Gastroenterology 2011 Shaheen NJ, MD, MPH, and Greenwald, G et al. Safety and efficacy of endoscopic spray cryotherapy for Barrett s esophagus with high-grade dysplasia. Gastrointest Endosc April ; 71(4): doi: /j.gie Sharma P, Falk GW, Weston AP, Reker D, Johnston M, Sampliner RE. Dysplasia and Cancer in a Large Multicenter Cohort of Patients with Barrett s Esophagus. Clinical Gastroenterology and Hepatology 2006;4: Sharma P. Strategies and recommendations for diagnosing and managing Barrett's esophagus Dec 31, 2009 New England Journal of Medicine. 48
49 SOURCE LIST Spechler SJ, Goyal RK (February 1996). "The columnar-lined esophagus, intestinal metaplasia, and Norman Barrett". Gastroenterology 110 (2): Study provides first estimate of U.S. population affected by Barrett s esophagus. Gastro.org American Gastroenterological Association. Accessed August van Vilsteren FG, et al. Stepwise radical endoscopic resection versus radiofrequency ablation for Barrett s oesophagus with high-grade dysplasia or early cancer: a multicentre randomized trial. Gut, epub January Wang KK, Nijhawan PK. Complications of photodynamic therapy in gastrointestinal disease. Gastrointest Endosc Clin N Am 2000; 10: Wani S, Puli SR, Shaheen NJ, Westhoff B, Slehria S, Bansal A, Rastogi A, Sayana H, Sharma P. Esophageal adenocarcinoma in Barrett's esophagus after endoscopic ablative therapy: a meta-analysis and systematic review. Am J Gastroenterol Feb;104(2): Westhoff B, Brotze S, Weston A, et al. The frequency of Barrett s esophagus in high-risk patients with chronic gerd. Gastrointestinal Endosc. 2005; 61: What Are the Key Statistics about Cancer of the Esophagus?" Cancer.org.. American Cancer Society. Accessed October MEDICAL SOCIETIES POSITION STATEMENTS AGA Institute Medical Position Panel, Gastroenterology 2011;140: ASGE Standards of Practice Committee. Guideline - Role of endoscopy in BE and other premalignant conditions of the esophagus. GIE 2012 SAGES Guideline Stefanidis, Surg Endosc,
Slide 1. Slide 2. Slide 3 DISCLOSURES EXPECTED OUTCOMES DIAGNOSIS AND TREATMENT
 Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus. Radiofrequency Ablation with the HALO Technology A Reference Book
 Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Treat Barrett s, Remove the Risk. HALO System
 Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus. Original Policy Date
 MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Section: Medicine Effective Date: July 15, 2015 Subsection: Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Populations Interventions Comparators Outcomes Individuals: With Barrett esophagus with high-grade dysplasia
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett (20180) Medical Benefit Effective Date: 01/01/16 Next Review Date: 09/19 Preauthorization No Review Dates: 05/09, 03/10, 03/11, 03/12, 07/12,
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett (20180) Medical Benefit Effective Date: 01/01/16 Next Review Date: 09/19 Preauthorization No Review Dates: 05/09, 03/10, 03/11, 03/12, 07/12,
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
RADIOFREQUENCY ABLATION OR CRYOABLATION FOR ESOPHAGEAL DISORDERS
 DISORDERS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
DISORDERS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus
 Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell
 Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
CLINICAL TRIAL OUTCOMES: RADIOFREQUENCY ABLATION (RFA) FOR BARRETT S ESOPHAGUS
 FOR BARRETT S ESOPHAGUS") CLINICAL TRIAL OUTCOMES: RADIOFREQUENCY ABLATION (RFA) FOR BARRETT S ESOPHAGUS CLIN-0115 (Rev. D) Clinical Trial Outcomes of RFA for BE (Ref. ECO#12339) Page 1 of 82 T ABLE OF C O N T E N T S 1. INTRODUCTION...
CLINICAL TRIAL OUTCOMES: RADIOFREQUENCY ABLATION (RFA) FOR BARRETT S ESOPHAGUS CLIN-0115 (Rev. D) Clinical Trial Outcomes of RFA for BE (Ref. ECO#12339) Page 1 of 82 T ABLE OF C O N T E N T S 1. INTRODUCTION...
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Opinion Statement. Esophagus (E Dellon, Section Editor)
") Curr Treat Options Gastro (2016) 14:1 18 DOI 10.1007/s11938-016-0080-4 Esophagus (E Dellon, Section Editor) Current Controversies in Radiofrequency Ablation Therapy for Barrett s Esophagus Kamar Belghazi,
Curr Treat Options Gastro (2016) 14:1 18 DOI 10.1007/s11938-016-0080-4 Esophagus (E Dellon, Section Editor) Current Controversies in Radiofrequency Ablation Therapy for Barrett s Esophagus Kamar Belghazi,
Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus: A Comprehensive Review
 Gastroenterology Research and Practice Volume 2016, Article ID 4249510, 8 pages http://dx.doi.org/10.1155/2016/4249510 Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus:
Gastroenterology Research and Practice Volume 2016, Article ID 4249510, 8 pages http://dx.doi.org/10.1155/2016/4249510 Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus:
Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign
 THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
evidence note Radiofrequency ablation for Barrett s oesophagus with highgrade What is an evidence note Key points Literature search Introduction
 In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
NIH Public Access Author Manuscript Gastrointest Endosc. Author manuscript; available in PMC 2012 July 13.
 NIH Public Access Author Manuscript Published in final edited form as: Gastrointest Endosc. 2012 July ; 76(1): 32 40. doi:10.1016/j.gie.2012.02.003. Characterization of buried glands before and after radiofrequency
NIH Public Access Author Manuscript Published in final edited form as: Gastrointest Endosc. 2012 July ; 76(1): 32 40. doi:10.1016/j.gie.2012.02.003. Characterization of buried glands before and after radiofrequency
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Are You Living with Barrett s Esophagus?
 Are You Living with Barrett s Esophagus? Wouldn t you rather live without it? If you re living with Barrett s esophagus you are not alone. Barrett s esophagus is caused by the long-term exposure of your
Are You Living with Barrett s Esophagus? Wouldn t you rather live without it? If you re living with Barrett s esophagus you are not alone. Barrett s esophagus is caused by the long-term exposure of your
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Barrett s esophagus (BE) is a precancerous state
 is a precancerous state") CLINICAL ALIMENTARY TRACT Gastroenterology 2017;153:681 688 Late Recurrence of Barrett s Esophagus After Complete Eradication of Intestinal Metaplasia is Rare: Final Report From Ablation in Intestinal
CLINICAL ALIMENTARY TRACT Gastroenterology 2017;153:681 688 Late Recurrence of Barrett s Esophagus After Complete Eradication of Intestinal Metaplasia is Rare: Final Report From Ablation in Intestinal
CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE
 CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE STUDYDESIGN 16 major academic GI centers participated in a double-blind, randomized, crossover study in which 160 high-risk patients undergoing BE surveillance
CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE STUDYDESIGN 16 major academic GI centers participated in a double-blind, randomized, crossover study in which 160 high-risk patients undergoing BE surveillance
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
235 60th Street, West New York, NJ T: (201) F: (201) Main Street, Hackensack, NJ T: (201)
 F: (201) Main Street, Hackensack, NJ T: (201)") 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Barrett's Esophagus WHAT IS BARRETTT'S ESOPHAGUS? Barrett's esophagus
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Barrett's Esophagus WHAT IS BARRETTT'S ESOPHAGUS? Barrett's esophagus
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Barrett s esophagus (BE), a known complication of chronic
, a known complication of chronic") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:220 227 Patients With Nondysplastic Barrett s Esophagus Have Low Risks for Developing Dysplasia or Esophageal Adenocarcinoma SACHIN WANI,* GARY FALK, MATTHEW
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:220 227 Patients With Nondysplastic Barrett s Esophagus Have Low Risks for Developing Dysplasia or Esophageal Adenocarcinoma SACHIN WANI,* GARY FALK, MATTHEW
What Is Barrett s Esophagus?
 What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
Endoscopic Therapy of Barrett s Esophagus and Esophageal Adenocarcinoma
 Clinical imaging / therapy Endoscopic Therapy of Barrett s Esophagus and Esophageal Adenocarcinoma Marcel Tantau, Ofelia Mosteanu, Teodora Pop, Alina Tantau, Gabriela Mester University of Medicine and
Clinical imaging / therapy Endoscopic Therapy of Barrett s Esophagus and Esophageal Adenocarcinoma Marcel Tantau, Ofelia Mosteanu, Teodora Pop, Alina Tantau, Gabriela Mester University of Medicine and
Accepted Manuscript. CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D
 Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Achieving Clinically Proven Treatment Results With Photodynamic Therapy (PDT) and PHOTOFRIN (porfimer sodium) for Injection
 and PHOTOFRIN (porfimer sodium) for Injection") Achieving Clinically Proven Treatment Results With Photodynamic Therapy () and PHOTOFRIN (porfimer sodium) for Injection PHOTOFRIN (porfimer sodium) IS INDICATED FOR Palliation of patients with completely
Achieving Clinically Proven Treatment Results With Photodynamic Therapy () and PHOTOFRIN (porfimer sodium) for Injection PHOTOFRIN (porfimer sodium) IS INDICATED FOR Palliation of patients with completely
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection
 Editor s choice Scan to access more free content For numbered affiliations see end of article. Correspondence to Professor Thomas Rösch, Department of Interdisciplinary Endoscopy, University Hospital Hamburg-Eppendorf,
Editor s choice Scan to access more free content For numbered affiliations see end of article. Correspondence to Professor Thomas Rösch, Department of Interdisciplinary Endoscopy, University Hospital Hamburg-Eppendorf,
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
Current challenges in Barrett s esophagus
 MEDICAL GRAND ROUNDS TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY Current challenges in Barrett s esophagus GARY W. FALK, MD * Director, Center for Swallowing and Esophageal
MEDICAL GRAND ROUNDS TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY Current challenges in Barrett s esophagus GARY W. FALK, MD * Director, Center for Swallowing and Esophageal
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
surgery ACA Acta Chirurgica Austriaca
 Eur Surg (2009) 41/1: 19 25 DOI 10.1007/s10353-009-0447-z Springer-Verlag 2009 european surgery ACA Acta Chirurgica Austriaca Printed in Austria Radiofrequency ablation of Barrett's esophagus G. Arora
Eur Surg (2009) 41/1: 19 25 DOI 10.1007/s10353-009-0447-z Springer-Verlag 2009 european surgery ACA Acta Chirurgica Austriaca Printed in Austria Radiofrequency ablation of Barrett's esophagus G. Arora
Barrett s Esophagus: State of the Art. Food Getting Stuck
 Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands
 DDW HIGHLIGHTS F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands Many new and exciting endoscopy-related studies on Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis were presented
DDW HIGHLIGHTS F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands Many new and exciting endoscopy-related studies on Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis were presented
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
National Digestive Diseases Information Clearinghouse
 Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
Follow this and additional works at:
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 217 Recurrence of intestinal metaplasia and early neoplasia after endoscopic eradication therapy for Barrett s esophagus:
Washington University School of Medicine Digital Commons@Becker Open Access Publications 217 Recurrence of intestinal metaplasia and early neoplasia after endoscopic eradication therapy for Barrett s esophagus:
Abstract. n engl j med 360;22 nejm.org may 28,
 The new england journal of medicine established in 1812 may 28, 2009 vol. 360 no. 22 Radiofrequency Ablation in Barrett s Esophagus with Dysplasia Nicholas J. Shaheen, M.D., M.P.H., Prateek Sharma, M.D.,
The new england journal of medicine established in 1812 may 28, 2009 vol. 360 no. 22 Radiofrequency Ablation in Barrett s Esophagus with Dysplasia Nicholas J. Shaheen, M.D., M.P.H., Prateek Sharma, M.D.,
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Treatment of High-Grade Dysplasia and Early Stage Esophageal Adenocarcinoma with an Endoscope: The Ultimate in Minimally Invasive, Curative Therapy
 Curr Surg Rep (2014) 2:66 DOI 10.1007/s40137-014-0066-x ESOPHAGEAL/REFLUX SURGERY (SR DEMEESTER, SECTION EDITOR) Treatment of High-Grade Dysplasia and Early Stage Esophageal Adenocarcinoma with an Endoscope:
Curr Surg Rep (2014) 2:66 DOI 10.1007/s40137-014-0066-x ESOPHAGEAL/REFLUX SURGERY (SR DEMEESTER, SECTION EDITOR) Treatment of High-Grade Dysplasia and Early Stage Esophageal Adenocarcinoma with an Endoscope:
Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection
 Editor s choice Scan to access more free content ORIGINAL ARTICLE Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection Mario Anders, 1 Christina Bähr, 1 Muhammad
Editor s choice Scan to access more free content ORIGINAL ARTICLE Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection Mario Anders, 1 Christina Bähr, 1 Muhammad
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Sex and race and/or ethnicity differences in patients undergoing radiofrequency ablation for Barrett's esophagus: results from the U.S. RFA Registry.
 Thomas Jefferson University Jefferson Digital Commons Department of Medicine Faculty Papers Department of Medicine 8-1-2015 Sex and race and/or ethnicity differences in patients undergoing radiofrequency
Thomas Jefferson University Jefferson Digital Commons Department of Medicine Faculty Papers Department of Medicine 8-1-2015 Sex and race and/or ethnicity differences in patients undergoing radiofrequency
Barrett s esophagus (BE), the premalignant condition
, the premalignant condition") GASTROENTEROLOGY 2009;136:2101 2114 A Cost-Utility Analysis of Ablative Therapy for Barrett s Esophagus JOHN M. INADOMI,*, MA SOMSOUK,*, RYAN D. MADANICK, JENNIFER P. THOMAS, and NICHOLAS J. SHAHEEN *Division
GASTROENTEROLOGY 2009;136:2101 2114 A Cost-Utility Analysis of Ablative Therapy for Barrett s Esophagus JOHN M. INADOMI,*, MA SOMSOUK,*, RYAN D. MADANICK, JENNIFER P. THOMAS, and NICHOLAS J. SHAHEEN *Division
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Efficacy of Radiofrequency Ablation Combined With Endoscopic Resection for Barrett s Esophagus With Early Neoplasia
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:23 29 ENDOSCOPY CORNER Efficacy of Radiofrequency Ablation Combined With Endoscopic Resection for Barrett s Esophagus With Early Neoplasia ROOS E. POUW,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:23 29 ENDOSCOPY CORNER Efficacy of Radiofrequency Ablation Combined With Endoscopic Resection for Barrett s Esophagus With Early Neoplasia ROOS E. POUW,*
Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I.
 UvA-DARE (Digital Academic Repository) Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I. Link to publication Citation for published version
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of photodynamic therapy for Barrett s oesophagus Barrett s oesophagus is a condition
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of photodynamic therapy for Barrett s oesophagus Barrett s oesophagus is a condition
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of