Changes to the diagnosis and management of Barrett s Oesophagus
|
|
|
- Juniper Bennett
- 5 years ago
- Views:
Transcription



1 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer in Gastroenterology Consultant Gastroenterologist

2


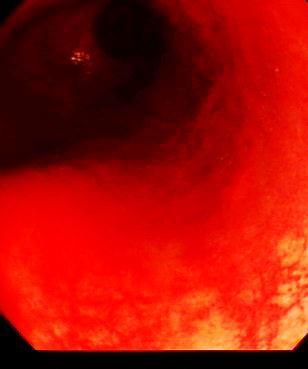
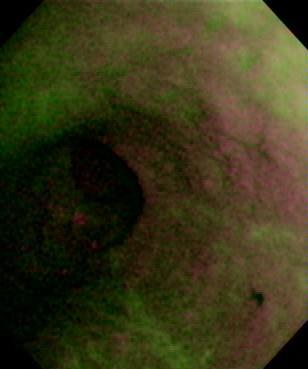
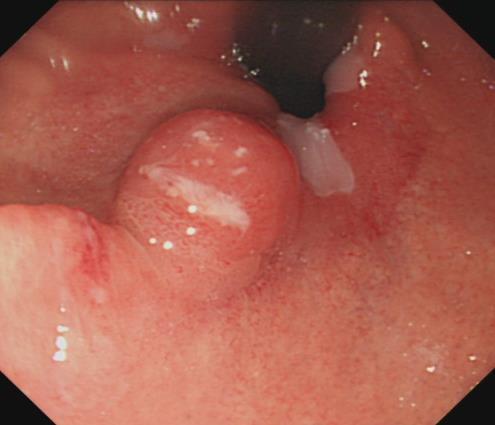
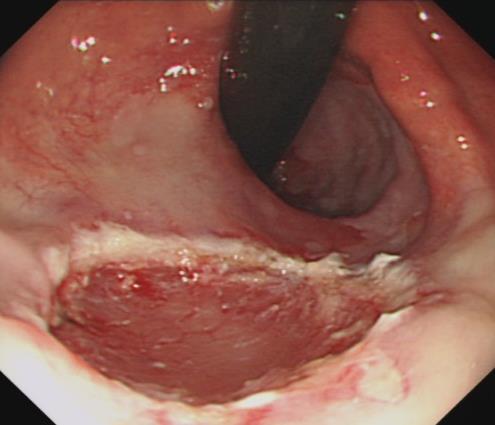
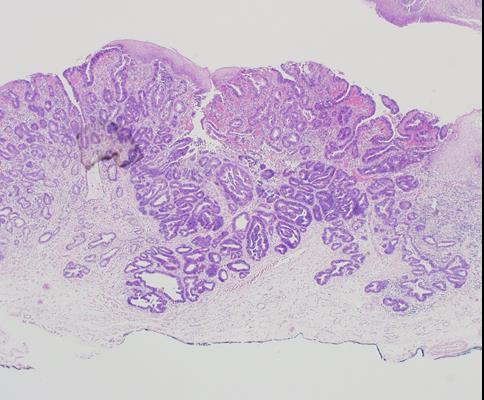
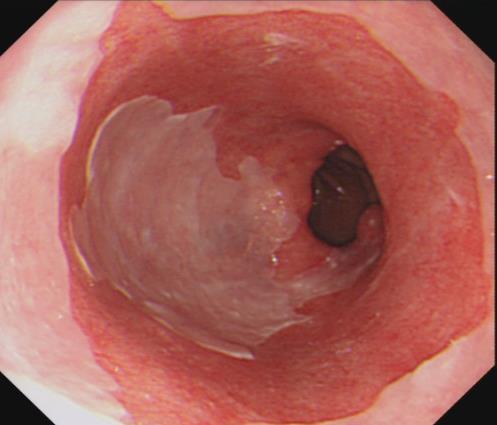
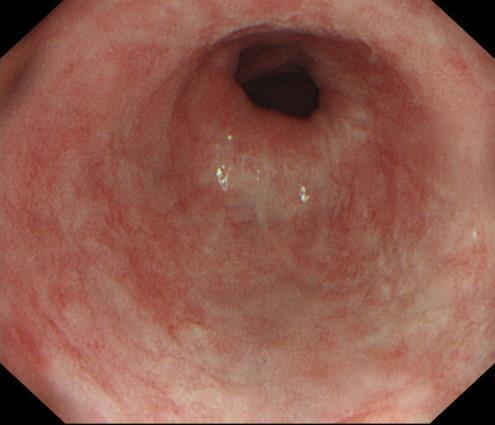
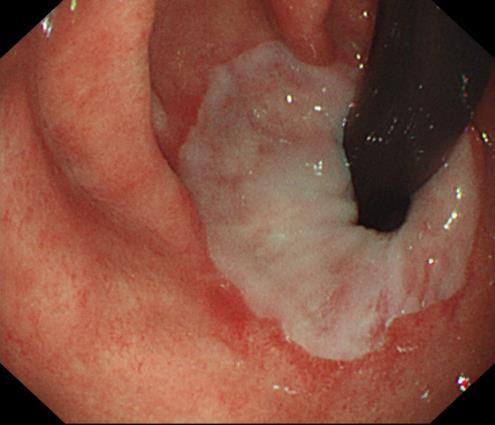
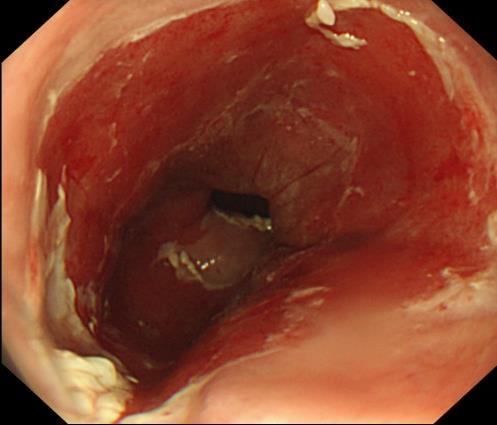
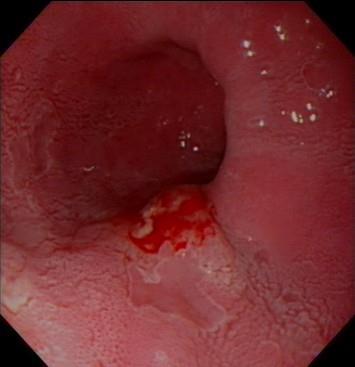
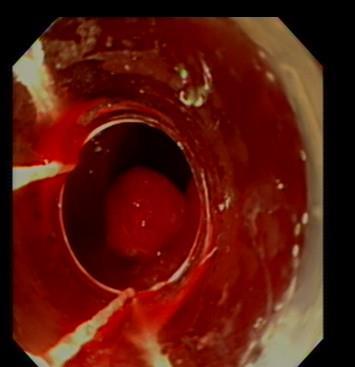
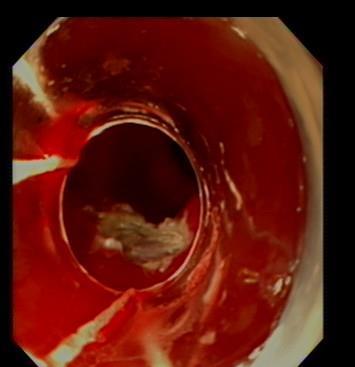
3 A flavour of endoscopic appearances in Barrett s Oesophagus



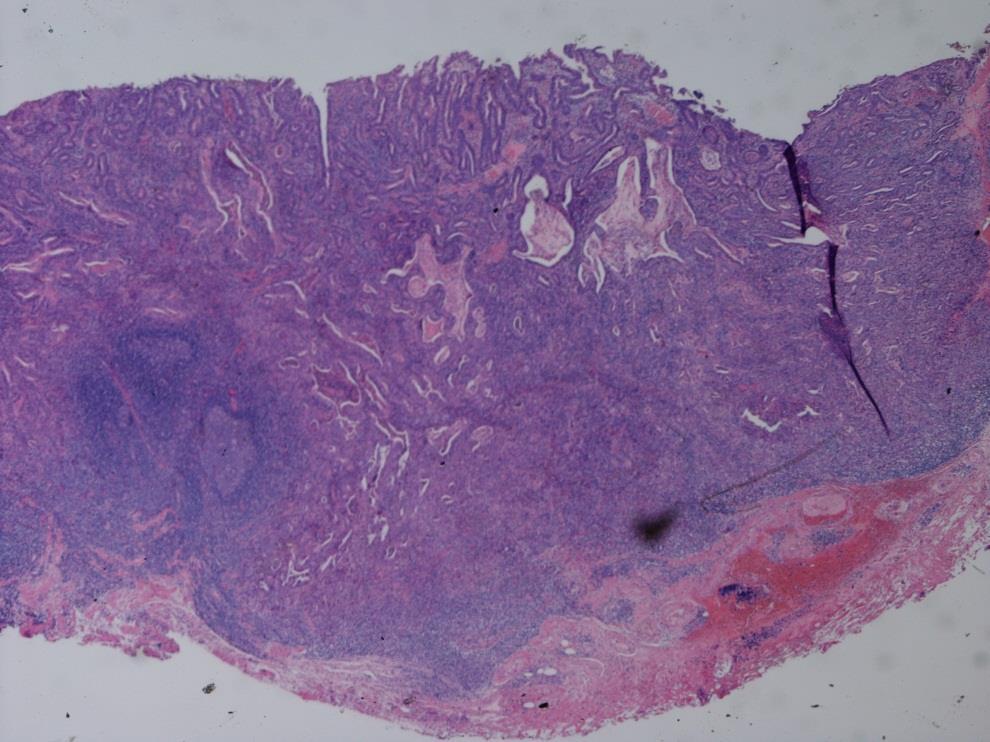
4 JH 2 recent patients with BO and HGD

5 TF
 Standards for training and QA for")
6 The New BSG Barrett s Guidelines ( ) Definition of Barrett s Oesophagus Who should undergo surveillance High risk factors to be taken into consideration for determining surveillance intervals Managing dysplasia in Barrett s (NICE guidance followed BSG) Standards for training and QA for endoscopic treatment


7 BSG guidance Visible dysplasia, HGD and T-1a For HGD and Barrett s-related adenocarcinoma confined to the mucosa endoscopic therapy is preferred over oesophagectomy or endoscopic surveillance. (Recommendation Grade B) 90% agreement (53% A+, 37% A, 10%U) ER should be considered the therapy of choice for dysplasia associated with visible lesions and T1a adenocarcinoma. (Recommendation Grade B) 95% agreement (58% A+, 37% A, 5%U)
 above")
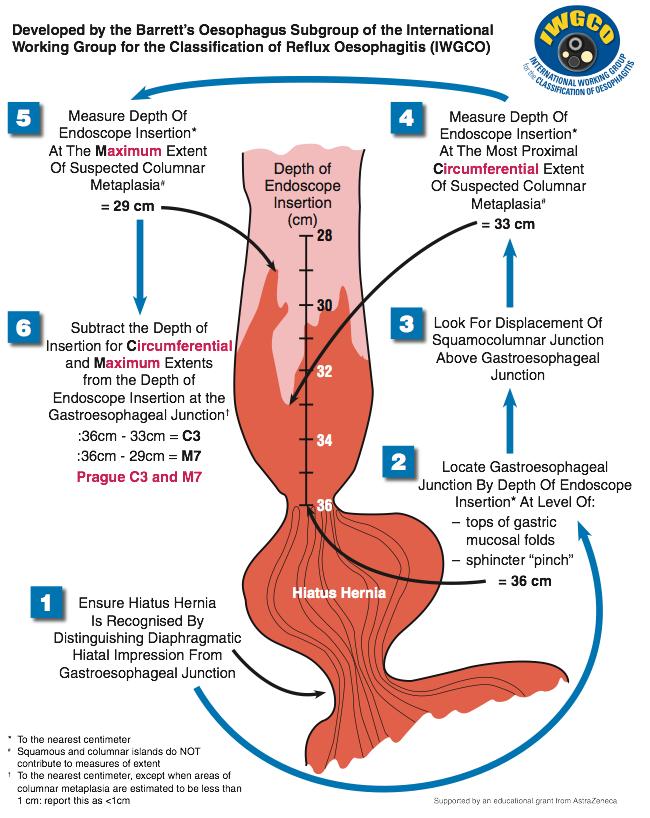
8 Diagnosing and reporting BO Is this Barrett s Oesophagus? BO defined as change to the distal squamous epithelium by metaplastic columnar epithelium, clearly visible endoscopically (>1cm) above GOJ, and confirmed histopathologically. GOJ is the proximal end of gastric folds
9

10 Standardisation of BO endoscopic reporting
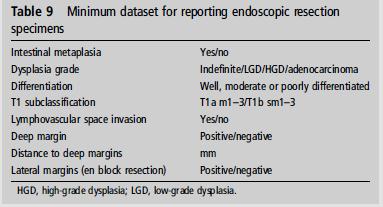
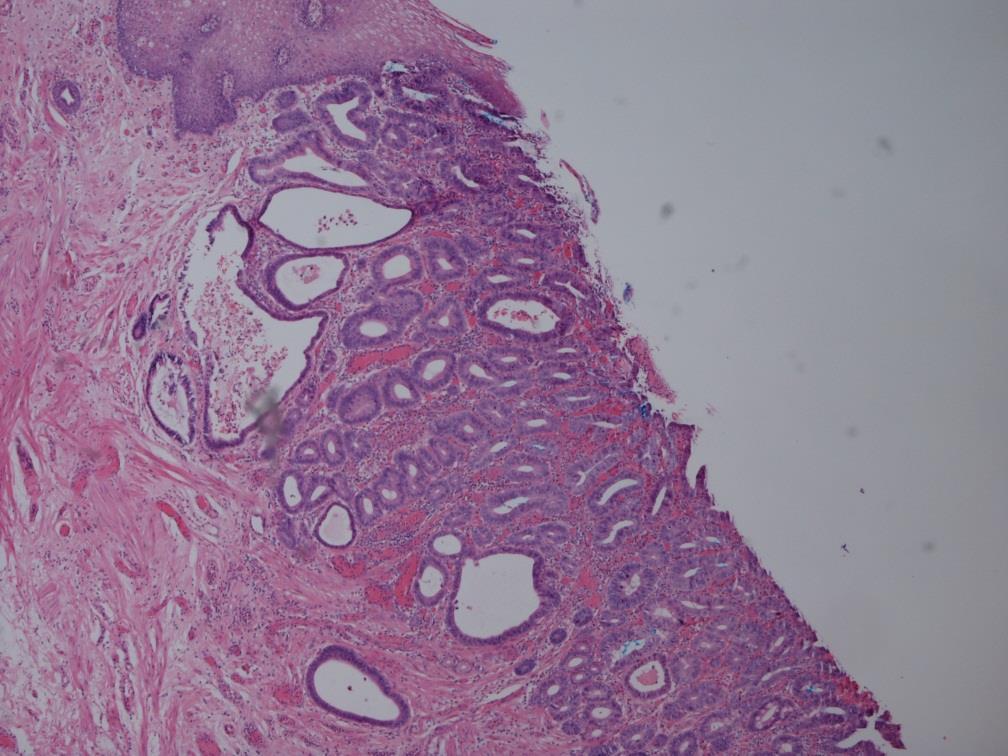
11 Standardisation of Histopathology for BO
12 Guidelines-1: Diagnosing BO CLO, no need for SIM-Histological corroboration Screening not recommended CLO-Report using Prague criteria (CM) Screening not recommended routinely Consider screening in high risk population Age >50, white race, male sex, obesity, family H/O Barrett s cancer
13 Guidelines-2: Surveillance yearly surveillance Target biopsy + Quadrantic biopsies every 2 cm 2014 High resolution endoscopy should be used Short segment (< 3 cm) with no SIM on repeat biopsy-no need for surveillance Short segment BO + SIM- Surveillance 3-5 yearly Long segment-2-3 yearly Target biopsy + Quadrantic biopsies every 2 cm
14 Guidelines ID-Re-biopsy after PPIfurther surveillance in 6 months LGD-re-biopsy after intense acid suppression in 8-12 weeks-6 monthly surveillance ID-Re-biopsy after PPIfurther surveillance in 6 months LGD-acid suppression-6 monthly surveillance (note that NICE Guidance now offers them RFA) Phoa et al, JAMA 2014
 CT/PET/EUS has limited role for staging in HGD/T1 cancers prior to ER Flat HGD-RFA Surgery for")
15 Guidelines HGD or early visible lesionsendoscopic therapy preferred HGD-If changes persist after intense acid suppression-surgery If unfit for surgeryablation/emr ER is the therapy of choice for HGD and T1a (lesions) CT/PET/EUS has limited role for staging in HGD/T1 cancers prior to ER Flat HGD-RFA Surgery for T1b and beyond
16
17 Surveillance Flow Chart for NDBO
18 Surveillance Flow Chart for Dysplastic BO

19 Flow Chart for management of HGD/IMC

20 Treatment concept and considerations RFA ER Surgery LGIN HGIN IMC superficial sm invasion deep sm invasion
21 Service Provision Endoscopic therapy of Barrett's neoplasia should be performed at centres where endoscopic and surgical options can be offered to patients. (Recommendation grade C) 89% agreement (72% A+, 17% A, 11%U) ER should be performed in high volume tertiary referral centres. RFA should be performed in centres equipped with ER facilities and expertise. (Recommendation Grade C) Round 1: 74% agreement (42% A+, 32% A, 16%U, 5% D, 5% D+) 94% agreement (33% A+, 61% A, 6%U) There is not sufficient evidence to guide on minimum procedure volume per centre, however consensus was reached for 15 ERs per year





22 Radiofrequency ablation 2003: new simple, ablation technique for removal of BE Balloon-based electrode for circumferential RFA: HALO 360 Catheter-based electrode to treat residual islands: HALO 90




23 AIM-dysplasia study Treatment protocol LGD/HGD in BE Randomization 0 mo HALO 360 2:1 Sham procedure HALO 90 2,4,9 mo Surveillance 12 mo EGD + biopsies EGD + biopsies Outcome EGD + 4Q/1cm bx: HGD: 3 monthly, LGD: 6 monthly

 Note: all lost-to-fu cases")
24 AIM-dysplasia study Primary outcome CR-IM: 77% vs 2% (p<0.001) CR-D: 86% vs 21% (p<0.001) Note: all lost-to-fu cases were considered failures







25 RFA for HGD: EURO II cohort Treatment protocol HGD/EC in BE ER of visible lesion Primary HALO 360 HALO 360/90 every 2-3 months Max 2 x HALO 360 Max 3 x HALO 90 Residual BE? EGD with NBI/lugol And 4Q/1cm Bx Escape ER
26 EURO II cohort Conclusions Results (November 2009): 118 patients / 55 completed therapy CR-Neoplasia 100%, CR-IM 96% Adverse events (no intervention required) 12 superficial mucosal lacerations 1 melena Conclusions: When performed by trained, expert endoscopists in carefully selected patients after ER, adverse events related to RFA are infrequent and mild
 3 average RFA sessions, consistent with US registry 0% BG in ER specimens (<1% in bx samples, all at the SCJ) \"The favorable")
27 RFA for Dysplasia/Early Cancer Is Durable Out to 5 Years AMC 5 Years Data (Phoa, Gastroenterology, 2013) First European Prospective Study at 5 years in HGD/EC patients >90% of patients remain in CR-IM; CR- NEO at 5 years (3 recurrences all treated endoscopically) 3 average RFA sessions, consistent with US registry 0% BG in ER specimens (<1% in bx samples, all at the SCJ) "The favorable long-term outcomes validate this treatment approach as a safe and effective alternative to esophagectomy "

28 BADCAT Consensus Statement (Jankowski, Gastro, 2012) An int l multidisciplinary, evidence-based review of different management strategies for BE 80% agreement was used to establish consensus for each statement, including Risk of progression from HGD to cancer is approx 10% per yr. Endoscopic treatment should be preferred over surgical treatment for management of most patients with HGD in BE and over surveillance for HGD/T1m RFA is currently the best available ablation technique for the treatment of flat HGD and for eradication of residual BE mucosa after local EMR 28

29 United Kingdom RFA Registry Participants 2014
30 HALO RADIOFREQUENCY ABLATION (RFA) REGISTRY FLOW CHART 0 mo PRIMARY HALO RFA PROCEDURE HGD/ IMC x 2 3 mo VISIBLE BE HALO NO VISIBLE BE BIOPSY Barrett s No Barrett s 6 mo VISIBLE BE HALO NO VISIBLE BE RESCUE EMR AT ANY STAGE FOR VISIBLE LESIONS BIOPSY HALO SURVEILLANCE Barrett s No Barrett s 9 mo VISIBLE BE HALO NO VISIBLE BE BIOPSY HALO SURVEILLANCE VISIBLE BE HALO NO VISIBLE BE BIOPSY 12 mo All patients undergo endoscopy with biopsy at 12 months and then re-enter surveillance programme based on entry grade or physician preference
31 Results (n=508, Completed Protocol ) Male:Female (%) 81:19 Mean age 69 (40-90) Baseline Histology (%) IMC HGD LGD Barrett s length (M) prior to RFA (mean) 5.6 cm (1-20) Mean No. HALO Ablations during protocol (range) - Mean no. HALO Mean no. HALO 90 EMR before RFA (%) RESCUE EMR DURING RFA 2.5 (1-6) % 7% Median follow up after ablation 24 months (IQR )
 Complete eradication all Dysplasia (n= 429) Complete")
32 Proportion with Complete Eradication % 12 month outcomes % 87% 50 70% 25 Shaheen NJ et al. N Engl J Med 2009;360: Complete eradication BE (n=353) Complete eradication all Dysplasia (n= 429) Complete eradication HGD (n=445)
33 No. Patients completed Treatment Protocol P value Mean age (Range) 68 (40-87) 69 (44-90) Male: Female (%) 80:20 84:16 Baseline Histology (%) - LGD - HGD - IMC Previous PDT (%) Baseline BE length at start of RFA (maximum extent, cm) 6 (1-20) 4.7 (1-16) EMR prior to RFA (%) 128/265 48% Rescue EMR during RFA treatment (%) Median time to End of protocol (months) 35/265 13% Reversal of IM at end of protocol (%) 149/265 56% Reversal of Dysplasia at end of treatment protocol (%) 145/245 59% 8/245 3% /265 77% 200/245 82% 222/245 91% Progression to Cancer 10/265 (4%) 7/245 (2.9%) P0.56 Median time to most recent biopsy from first Treatment for those still in follow up, (months) 31 (3-72) n= (2-32) n=211 % free of Dysplasia at most recent 97% 90% follow up % Free of IM at most recent follow up 91% 93% P < P< CHI2 P< CH2
34 A surveillance programme in your Trust Is your Trust surveillance strategy designed to detect dysplasia? An agreed surveillance protocol Structured surveillance lists, at least 2 slots/pt. Trained endoscopists to improve lesion recognition Use of simple techniques e.g. good mucosal wash with Infacol, HRWLE imaging and enhanced imaging (2.5% acetic acid or NBI) Seattle biopsy protocol followed Designated GI Pathologist, x2?
35 Surveillance for Barrett s Oesophagus in local Trusts Is there an agreed Dysplasia management pathway in your Cancer Network? Are dysplasias discussed at SMDT with appropriate Staging CT 2 pathologists reviewing histology at SMDT Trained Endoscopist to do ER Are your surgeons on board with endoscopic management of HGD Pathway for RFA referral (regional centres)
36 So here s what your balance sheet might look like. CANCER NETWORK DURHAM & NTH TEES Population (Taken from cancer network website) 1,200,000 Adult Population 960,000 Estimated Number of patients with Barrett's Oesophagus 15,360 LGD 614 HGD 138 Cancer Risk per Year 77 Actual Mortality Oesophageal Cancer in this Network 385 If 20% of the patients with HGD are treated with RFA TOTAL NUMBER OF PATIENTS TO TREAT CAPITAL COSTS AND WARRANTY OVER 5 YEARS Generator and Trolley 49,500 Extended warrany for addttional 4 years (total 5 years) 9,000 Total set up costs for 5 years 58,500 ANNUAL RUNNING COSTS FOR RFA ABLATION Ist Procedure Halo Sizing Balloon (3441C) 1,300 1 Halo 360 Ablation Catheter (32041-xx) 25 1 Halo Cleaning Cap (CP-001B/002B) 2nd Follow Up at 10 Weeks Halo 90 Ablation Catheter for focal treatment ( ) 920 Potential 3rd follow up at 20 Weeks 920 Halo 90 Ablation Catheter for focal treatment ( ) Consumable cost per course of treatment per patient 3,635 Consumables for all patients per year 101,780 Saving on Oesophagectomy is 2760 per patient (NICE) 2,760 Savings for all patients per year 77,280 Savings over 5 years (including set up costs) 327,900
37 A Step by Step approach NICE guidance CG 106 & IPG 244/344 to justify need for audit (eg UK National Registry) Local new techniques and medical devices panel Trust and directorate/hos support; cancer network support Training operator and support team Dedicated lists & organisation Business case to CCG commissioners Demand and capacity (Nov-Feb usually) OPCS and HRG codes FZ24A/B/C Multiple CCGs but usually one will often take lead for specifics Activity paid by PbR; excluded devices pass through consumables costs Service developments should be cost neutral ; cost efficiency ; quality benefits; bed days saving; align with Trust objectives QIPP pump priming




38 Thank you for your attention
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System
 Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System Used abbreviations BE: Barrett s esophagus EC: Early cancer ER: Endoscopic resection HGD:
Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System Used abbreviations BE: Barrett s esophagus EC: Early cancer ER: Endoscopic resection HGD:
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
CLINICAL GUIDELINE FOR THE MANAGEMENT OF BARRETT S OESOPHAGUS Summary.
 CLINICAL GUIDELINE FOR THE MANAGEMENT OF BARRETT S OESOPHAGUS Summary. Page 1 of 12 Recurrent LGD at any point- discuss at MDT And consider RFA Patients with LGD should have a repeat endoscopy in 6 months.
CLINICAL GUIDELINE FOR THE MANAGEMENT OF BARRETT S OESOPHAGUS Summary. Page 1 of 12 Recurrent LGD at any point- discuss at MDT And consider RFA Patients with LGD should have a repeat endoscopy in 6 months.
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Opinion Statement. Esophagus (E Dellon, Section Editor)
") Curr Treat Options Gastro (2016) 14:1 18 DOI 10.1007/s11938-016-0080-4 Esophagus (E Dellon, Section Editor) Current Controversies in Radiofrequency Ablation Therapy for Barrett s Esophagus Kamar Belghazi,
Curr Treat Options Gastro (2016) 14:1 18 DOI 10.1007/s11938-016-0080-4 Esophagus (E Dellon, Section Editor) Current Controversies in Radiofrequency Ablation Therapy for Barrett s Esophagus Kamar Belghazi,
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign
 THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
The National Oesophago-gastric Cancer Awareness Campaigna locality outcome analysis from County Durham
 The National Oesophago-gastric Cancer Awareness Campaigna locality outcome analysis from County Durham Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Reader in Medicine, Durham University
The National Oesophago-gastric Cancer Awareness Campaigna locality outcome analysis from County Durham Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Reader in Medicine, Durham University
Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I.
 UvA-DARE (Digital Academic Repository) Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I. Link to publication Citation for published version
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
Barrett s Esophagus. Radiofrequency Ablation with the HALO Technology A Reference Book
 Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
National Oesophago-Gastric Cancer Audit Progress Report 2014
 National Oesophago-Gastric Cancer Audit Progress Report 2014 An Audit of the care received by people with Oesophago-Gastric Cancer in England and Wales 1 This report was prepared by Clinical Effectiveness
National Oesophago-Gastric Cancer Audit Progress Report 2014 An Audit of the care received by people with Oesophago-Gastric Cancer in England and Wales 1 This report was prepared by Clinical Effectiveness
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's oesophagus. Ablative therapy for the treatment of Barrett's oesophagus. Issued: August NICE clinical guideline 106
 Barrett's oesophagus Ablative therapy for the treatment of Barrett's oesophagus Issued: August 2010 NICE clinical guideline 106 guidance.nice.org.uk/cg106 NICE has accredited the process used by the Centre
Barrett's oesophagus Ablative therapy for the treatment of Barrett's oesophagus Issued: August 2010 NICE clinical guideline 106 guidance.nice.org.uk/cg106 NICE has accredited the process used by the Centre
evidence note Radiofrequency ablation for Barrett s oesophagus with highgrade What is an evidence note Key points Literature search Introduction
 In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
Treat Barrett s, Remove the Risk. HALO System
 Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Efficacy of Radiofrequency Ablation Combined With Endoscopic Resection for Barrett s Esophagus With Early Neoplasia
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:23 29 ENDOSCOPY CORNER Efficacy of Radiofrequency Ablation Combined With Endoscopic Resection for Barrett s Esophagus With Early Neoplasia ROOS E. POUW,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:23 29 ENDOSCOPY CORNER Efficacy of Radiofrequency Ablation Combined With Endoscopic Resection for Barrett s Esophagus With Early Neoplasia ROOS E. POUW,*
Section: Medicine Effective Date: July 15, 2015 Subsection: Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus. Original Policy Date
 MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus: A Comprehensive Review
 Gastroenterology Research and Practice Volume 2016, Article ID 4249510, 8 pages http://dx.doi.org/10.1155/2016/4249510 Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus:
Gastroenterology Research and Practice Volume 2016, Article ID 4249510, 8 pages http://dx.doi.org/10.1155/2016/4249510 Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus:
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Clinical guideline Published: 11 August 2010 nice.org.uk/guidance/cg106
 Barrett's oesophagus: ablative therapy Clinical guideline Published: 11 August 2010 nice.org.uk/guidance/cg106 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Barrett's oesophagus: ablative therapy Clinical guideline Published: 11 August 2010 nice.org.uk/guidance/cg106 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell
 Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
Chapter 2 Complications of Gastroesophageal Reflux Disease
 Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
What Is Barrett s Esophagus?
 What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
Current status of gastric ESD in Korea. Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea
 Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Missed Lesions at Endoscopy. Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand
 Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Barrett s Esophagus: State of the Art. Food Getting Stuck
 Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
The incidence of esophageal adenocarcinoma is rising in the ENDOSCOPY CORNER
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of photodynamic therapy for Barrett s oesophagus Barrett s oesophagus is a condition
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of photodynamic therapy for Barrett s oesophagus Barrett s oesophagus is a condition
Pathology of the oesophagus and the stomach. Neil A Shepherd Gloucester, UK. Bristol Pathology 1 st Year Training School, The layers of the GI tract
 Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
Radiofrequency ablation for early esophageal squamous cell neoplasia
 Radiofrequency ablation for early esophageal squamous cell neoplasia Authors Y. M. Zhang 1, J. J. G. H. M. Bergman 2, B. Weusten 2, 3, S. M. Dawsey 4, D. E. Fleischer 5,N.Lu 6,S.He 1,G.Q.Wang 1 Institutions
Radiofrequency ablation for early esophageal squamous cell neoplasia Authors Y. M. Zhang 1, J. J. G. H. M. Bergman 2, B. Weusten 2, 3, S. M. Dawsey 4, D. E. Fleischer 5,N.Lu 6,S.He 1,G.Q.Wang 1 Institutions
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement
 Position Statement") Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Bas Weusten 1, 2,RafBisschops 3,EmanuelCoron 4,MárioDinis- Ribeiro 5,Jean-MarcDumonceau
Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Bas Weusten 1, 2,RafBisschops 3,EmanuelCoron 4,MárioDinis- Ribeiro 5,Jean-MarcDumonceau
Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I.
 UvA-DARE (Digital Academic Repository) Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Advances in endoscopic resection and radiofrequency ablation of early esophageal neoplasia van Vilsteren, F.G.I. Link to publication Citation for published version
Evaluating endoscopy capacity across the NHS in England
 Evaluating endoscopy capacity across the NHS in England Hilary Brown, HSMC, University of Birmingham Steven Wyatt, Midlands and Lancashire Commissioning Support Unit Methodology Literature and evidence
Evaluating endoscopy capacity across the NHS in England Hilary Brown, HSMC, University of Birmingham Steven Wyatt, Midlands and Lancashire Commissioning Support Unit Methodology Literature and evidence
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging
 Alimentary Pharmacology & Therapeutics Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging G. K. ANAGNOSTOPOULOS*, K. YAO*, P. KAYE,
Alimentary Pharmacology & Therapeutics Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging G. K. ANAGNOSTOPOULOS*, K. YAO*, P. KAYE,
Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection
 Editor s choice Scan to access more free content ORIGINAL ARTICLE Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection Mario Anders, 1 Christina Bähr, 1 Muhammad
Editor s choice Scan to access more free content ORIGINAL ARTICLE Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection Mario Anders, 1 Christina Bähr, 1 Muhammad
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Technical and Endoscopic Factors in. in CDH1 Mutation Carriers
 Technical and Endoscopic Factors in Gastric Cancer Surveillance in CDH Mutation Carriers Carol A. Burke,3,5, Michael Cruise 2,5, Lisa LaGuardia 3,5, Margaret O Malley 3,5, Matthew Kalady 3,5, James Church
Technical and Endoscopic Factors in Gastric Cancer Surveillance in CDH Mutation Carriers Carol A. Burke,3,5, Michael Cruise 2,5, Lisa LaGuardia 3,5, Margaret O Malley 3,5, Matthew Kalady 3,5, James Church
Targeting care in Barrett s oesophagus
 HEPATO-GASTROENTEROLOGY Clinical Medicine 2014 Vol 14, No 6: s78 s83 Targeting care in Barrett s oesophagus Authors: Sebastian Zeki A and Rebecca C Fitzgerald B ABSTRACT Barretts oesophagus represents
HEPATO-GASTROENTEROLOGY Clinical Medicine 2014 Vol 14, No 6: s78 s83 Targeting care in Barrett s oesophagus Authors: Sebastian Zeki A and Rebecca C Fitzgerald B ABSTRACT Barretts oesophagus represents
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>