Multimodal cachexia management
|
|
|
- Russell Holland
- 5 years ago
- Views:
Transcription

 Medical")

1 Multimodal cachexia management Dr Martin Chasen MBChB FCP(SA) MPhil(Pall Care) Medical Oncologist/Director of Palliative care William Osler Health Services Toronto CANADA


2 Do you have anything that you can give me Doc to stop me losing weight? I dread going to the table food for My wife nags me because I am not eating and am losing weight Why am I losing weight?
3
4
5 NSCLC weight loss associated with delivery of fewer cycles of chemotherapy (p<0.003) more treatment delays (p=0.04), more anaemia (p=0.003), more symptoms at presentation(p<0.0001) less symptomatic benefit from chemotherapy (p=0.004).
6 A well designed study to evaluate the benefitof nutritional support in patients with weight loss receiving chemotherapy is needed PJ Ross et al 2004

7 Why has research in cachexia been slow? Unimodal therapy trials Prerequisite of oncology trials Late phase You are not eligible if you are taking part in another trial fastidious vs pragmatic trials gatekeeping Limited pharmaceutical funding Lack of a consensus definition

8 When you can measure what you are speaking about, and express it in numbers, you know something about it; but when you cannot express it in numbers, your knowledge is of a meagre and unsatisfactory kind; it may be the beginning of knowledge, but you have scarcely, in your thoughts, advanced to the stage of science, whatever the matter may be Lord Kelvin

9 Volume 12, Issue 5, May 2011, P A multifactorial syndrome characterised by an ongoing muscle loss (with or without fat loss) that cannot be fully reversed by nutritional support and leads to progressive functional impairment. The pathophysiology is characterized by a negative protein and energy balance driven by a variable combination of reduced nutritional intake and abnormal metabolism
10 Cachexia is Not Starving Starving Metabolism slows down Cachexia Metabolism speeds up (catabolic) LEAP version 1.1 Canadian Pallium Project
11 Diagnosis Mostly a clinical Dx Complete history (trying to determine if secondary causes at play) ESAS appetite score Physical exam Weight, wasting, edema, gait, rising from chair, gross muscle strenght, mucositis, trush, neck masses, abdominal exam etc Laboratory CBC, Cr, lytes, LFTs, TSH, albumin, CRP






12 Body mass index (kg/m²) b 1 a SMI 29.8 cm²/m², BMI 40.2 kg/m² b 2 SMI 29.8 cm²/m², BMI 28.1 kg/m² Skeletal muscle index (cm²/m²) b 3 c 1 c 2 c 3 SMI 29.7 cm²/m², BMI 15.3 kg/m² SMI 33.7 cm²/m², BMI 29.5 kg/m² SMI 46.3 cm²/m², BMI 29.4 kg/m² SMI 58.3 cm²/m², BMI 29.4 kg/m² V Baracos

13 Assessment of Cachexia according to : Anorexia or reduced food intake Catabolic drivers Functional and psychosocial effects Muscle mass and strength Stages of Cancer Cachexia Fearon K, Strasser F, Anker SD, et al. Lancet Oncol 2011; 12:

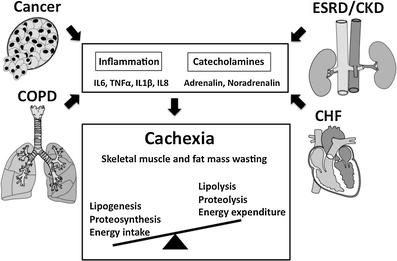
14 Inflammation & Cancer Inflammation Inflammation experimental development Inflammation Targeting inflammation and cancer spread. predisposes to certain tumour types implicated in oncogenic mutations animal models of tumour 1 can be a result of cancer. can reduce cancer risk & 7 th hallmark of cancer 1.Mantovani Nature 2008;454
15 Systemic Inflammatory Response ANABOLIC BLOCKADE Cachexia Anorexia Physical Inactivity


16 Multimodal Therapy: High protein nutrition Anti-inflammatory agents to down regulate the APIR Routine mobilisation programmes to prevent deconditioning and encourage physical activity-induced stimulation of post prandial anabolism. Mantovani G, Maccio A, Madeddu C, et al. Randomized phase III clinical trial of five different arms of treatment in 332 patients with cancer cachexia. Oncologist 2010;15:200-11
17 Exercise prescription FITT structure frequency intensity time type Campbell et al. Br J Sports Med 2011
18 Resistance vs. Aerobic training Dependant on the central aim of training muscle strength & mass: resistance > aerobic fatigue & CV fitness: resistance < aerobic
19 Research has shown that, for people with cancer (including advanced-stage cancer), exercise can decrease anxiety, stress, and depression while improving levels of pain, fatigue, shortness of breath, constipation, and insomnia. Clin J Oncol Nurs Jun 1; 16(3):
20 During cancer cachexia
21 Grande et al. Cochrane Database of Systematic Reviews 2014 insufficient evidence to determine the safety and effectiveness of exercise for patients with cancer cachexia
22 Nutritional interventions in patients with advanced cancer Oral nutritional interventions are effective at increasing nutritional intake and improving some aspects of QOL in patients with cancer who are malnourished or are at nutritional risk but do not appear to improve mortality. (Baldwin et al., J Natl Cancer Inst, 2012) Weight and energy intake may stabilize or increase for a period QoL may improve No evidence for the effect of Function Fatigue Survivial Several nutritional guidelines with conflicting recommendations (Champ et al., Nutr Cancer, 2013)
23 Nutritional interventions in patients with advanced cancer No studies combining nutrition and exercise therapies in patients with advanced lung cancer in a recent review (Payne et al. Curr. Oncol, 2013) In frail elderly studies have shown that nutrition will not usually improve function unless muscles are exercised using resistance exercise (Breen L, Br J Clin Pharmacol, 2013; Tieland M J Am Med Dis Assoc, 2012)
24 Nutritional interventions in patients with Five publications retrieved 3 RCT cachexia Two out of five studies showed less weight loss with dietary counseling Two presented positive effect on energy intake Dietary counseling can effect energy intake and body weight However, not enough proof of evidence that dietary counseling given to patients with cancer is beneficial for improving weight or energy balance in the different cachexia stages (Balstad et al., Crit Rev Oncol Hematol, 2014)
25 Single agents/interventions in isolation have limited benefit ~ 100 clinical trials There is now a persuasive argument that combination therapy should be administered to maximise benefit
26 REVIEW OF MULTIMODAL STUDIES Chasen, MacDonald. Bhargava- CAMJ To date there are only a few reports on programs combining exercise, nutritional counseling and management of symptoms by palliative care professionals. Methodology and selection of reports goes here For this review Rapid Evidence Assessment methodology was employed in which 75 articles which touch on rehabilitation for advanced cancer patients were located from Searches on the following databases were conducted:
27 - All adult patients with stage III and IV cancer; I-Intervention- Rehabilitation delivered by the following professions: Medical Oncologist / Palliative care Physicians, Dietitian, Physiotherapists, Occupational Therapists, Nurse, Psychologist and Social worker ; C-Context- Hospital, hospice, cancer centre and palliative care unit. Only studies published in English were included.. All the databases were searched with combinations of terms related to advanced cancer, cancer rehabilitation common symptoms and /or interventions of interest.
28 4 studies In an Australian non randomised study 25 of 41enrolled participants who remained in the combined program for 2 months demonstrated improved nutritional status and functional status, endurance, and strength, with a decrease in reported symptoms and felt better supported. The MD Anderson program reported on 151 patients assessed at a cachexia clinic. 59 did not return for follow up. All patients received dietary counseling by a dietician and standard exercise recommendations. A combination of simple pharmacological and nonpharmacological interventions improved appetite significantly, and increased weight in one third of patients who were able to return for follow-up. No functional outcomes were reported
29 2003 McGill University CANCER NUTRITION AND REHABILITATION PROGRAM 2009-Elisabeth Bruyere Hospital (University of Ottawa) Significant improvements in: physical performance (P <0.000), nutrition (P =0.001), symptom severity (P=0.005 to P= 0.001), symptom interference in functioning (P =0.003 to P<0.001), fatigue (P=0.001), and physical endurance, mobility, and balance/function (P=0.001 to P<0.001)
30 Strong improvements in the physical and activity dimensions of fatigue (effect sizes = ). moderate reductions in the severity of weakness, depression, nervousness, shortness of breath and distress (effect sizes: ), moderate improvements in six-minute walk distance, maximal gait speed, coping ability and quality of life (effect sizes = ) 77 % of patients either maintained or increased their body weight.


31 Nutritional Rehabilitation (prehabilitation) in Oncology (cancer associated muscle loss) The Refractory Patient Pre-cachexia Cachexia Refractory- exia Death Weight loss <5% Anorexia & metabolic change Weight loss>5% or BMI<20 and weight loss >2% or sarcopenia and weight loss >2% Variable degreeof cachexia. Cancer diseaseboth procatabolic and notresponsive to anti-cancer treatment. LowPS, survival <3 months Tora S Solheim

32

33 Eropean Palliative Care Research Centre (PRC)
34 Anti-inflammatory CANCER Anti-inflammatory Pro-inflammatory
35 What now... rather than systemic inflammation being cause for individual symptoms, inflammation may be implicated in the genesis of multiple cancer symptoms Animal models of cytokine induced sickness behavior have concentrated on cachexia and have confirmed the role of pro-inflammatory cytokines in cachexia development - hypothesis is now a decade old little in the way of work examining the modulation of symptoms by attenuating the inflammatory response.
36 Can we modulate the inflammatory response to treat cachexia through a multimodal approach?
37 Anti-inflammatories Systemic Inflammatory Response Nutritional Intake Cachexia Exercise Anorexia Physical Inactivity Interventions should be multimodal tackling all of these issues simultaneously
38 Multimodal Intervention Critical pre-cachexic phase In combination with anti-cancer therapy
39 First Clinical Intervention Trial of a Nutritional
40 The Perfect Multimodal Cachexia Trial Randomised - Contamination of control group Blinded - possible? Placebo controlled Standardisation of Best Supportive Care Pre-cachexia phase Standardised multimodal intervention Excellent participant compliance Standard oncology care Meaningful endpoints Transferable to real-life clinical setting FEASIBLE
41 HYPOTHESIS: Early intervention to treat or minimise weight loss may improve symptoms and allow anticancer therapy to be given more efficiently with the ultimate aim of improving survival.
42 Challenges.. Trial design (duration, Recruitment Exercise Technical aspects ONS palatability Complications of Frail population Conflicting trials endpoints ) chemotherapy
43 Pre-MENAC study: A feasibility study of Multimodal Exercise/Nutrition/Antiinflammatory treatment for Cachexia A multicentre, open, randomized phase II study comparing a multimodal intervention for cachexia versus standard cancer care The multimodal intervention consisted of: Nutritional supplements enriched with EPA (n-3 fatty acids) and nutritional advice Home-based self-assisted exercise program Anti-inflammatory medication (celecoxib) Results: As of Feb 2014, 399 patients have been screened with 43 patients recruited from three centres across two countries. An interim analysis has been conducted on 34 patients: Intervention 19, Control 15 Primary endpoints: Compliance to the intervention, (>80% of that prescribed): antiinflammatory 80%, ONS 47%, resistance training 26%, aerobic exercise 42% ClinicalTrials.gov Identifier: NCT
44 Forty-six patients were recruited from three regional cancer center s (Glascow (UK), Trondheim and Oslo (Norway). Overall compliance was > 54% in all components of the intervention. Patients in the treatment arm weight increased (0.91% (SD 2.46)), whilst those in the control arm lost weight (-2.12% (SD 2.50)), p < (N = 41). Patients in the control arm lost 2.2% more muscle than the treatment arm, p = 0,69. There were no statistical significant differences in physical activity in the patients that had repeated measurements of physical activity with ActivPal (n = 22). Conclusions: A multimodal cachexia intervention is feasible and improves weight in patients with incurable lung or pancreatic cancer. Based on these exciting findings, a definitive phase III study is now underway
45 MENAC: The Multimodal Exercise/Nutrition/Anti-inflammatory treatment for Cachexia trial MENAC is a large-scale open randomised phase III, multimodal intervention trial. Primary objective To establish whether a multimodal intervention is effective in treating cachexia. This will be assessed after 2 cycles of chemotherapy (study endpoint -between 6-9 weeks) by measuring weight. Secondary objectives To examine the effect of a multimodal intervention for cancer cachexia on muscle mass, physical performance, performance status, health status, nutritional status, quality of life, toxicity, and hospitalisations. Patients Diagnosis of lung cancer, pancreatic cancer or Due to commence anti-cancer therapy Plans/estimation A total of 260 patients will be recruited from out-patient oncology clinics at multiple sites in Europe, Canada and Australia. The inclusion started in 2014
46

47 MENAC: The Multimodal Exercise/Nutrition/Anti-inflammatory treatment for Cachexia trial Nutritional intervention : Dietary counselling - to promote energy and protein balance, in combination with nutritional supplements. Study participants - advised to increase meal frequency and their intake of high calorie food and beverages. Patients will be prescribed 2 cans of Eicosapentaenoic acid (EPA) enriched nutritional supplements consisting of a total of 542 Kcal ProSure (Abbott ). If patients are unable to take these supplements, they will be prescribed oral capsules containing 2g Eicosapentaenoic acid. Exercise intervention: Home-based exercise programme Prescription will consist of three times weekly functional resistance exercises and aerobic training two times weekly. Pharmacological intervention : Ibuprofen a dose of 1200 mg/day (400 mg x3/d). Canadian Institutes of Health Research, Open Operating Grant, 2014
48 Eligibility Criteria Diagnosis of non operable non-small cell lung cancer (NSCLC) (stage III-IV) or pancreatic cancer Due to commence chemotherapy or chemoradiotherapy NOT receiving parenteral nutrition or enteral nutrition via feeding tube NO Weight loss >20% over the previous 6 months NO BMI >30 kg/m 2 NO Severe anorexia (less than 50% pre-illness food intake and unable to take oral supplements)
49 Identification Consent Treatment Arm (Multimodal intervention + Standard cancer care) Control Arm (Standard cancer care) Week 0 Week 6 Participants are offered same treatment as treatment arm (Multimodal intervention) Week 12
50 Endpoints Primary Feasibility, recruitment, retention Secondary LBM, weight, activity, cancer therapy nutritional, toxicity, anti-
51 Anti-inflammatories Systemic Inflammatory Response Nutritional Intake Cachexia Exercise Anorexia Physical Inactivity Immunomodulation!

52 Rudolf Carl Virchow Father of modern pathology Postulated that inflammation was not a single process combination of various inflammatory processes And introduced functio laesa but a Was the first to hypothesize a link between inflammation and cancer. 200 years later still we are still discovering how targeting inflammation can prevent, treat and palliate cancer.
53
54 Acknowledgements BARRY LAIRD Ken Fearon, Stein Kaasa, Tora S.Sol heim, Guro Stene, Trude Balstad, Neil Johns, Marie Fallon, Donald McMillan, Peter Fayers
CANCER CACHEXIA. Barry J A Laird Clinician Scientist in Palliative Medicine, University of Edinburgh & European Palliative Care Research Centre
 CANCER CACHEXIA Barry J A Laird Clinician Scientist in Palliative Medicine, University of Edinburgh & European Palliative Care Research Centre Consultant in Palliative Medicine BWoSCC and Edinburgh Cancer
CANCER CACHEXIA Barry J A Laird Clinician Scientist in Palliative Medicine, University of Edinburgh & European Palliative Care Research Centre Consultant in Palliative Medicine BWoSCC and Edinburgh Cancer
The use of omega-3 fatty acids in the management of cancer cachexia. Rhys White Principal Oncology Dietitian Guys and St Thomas NHS Foundation Trust
 The use of omega-3 fatty acids in the management of cancer cachexia Rhys White Principal Oncology Dietitian Guys and St Thomas NHS Foundation Trust Overview Cancer cachexia Clinical features Pathogenesis
The use of omega-3 fatty acids in the management of cancer cachexia Rhys White Principal Oncology Dietitian Guys and St Thomas NHS Foundation Trust Overview Cancer cachexia Clinical features Pathogenesis
Cancer cachexia: assessment and classification. KCH Fearon University of Edinburgh Scotland
 Cancer cachexia: assessment and classification KCH Fearon University of Edinburgh Scotland 1 What is the cancer cachexia phenotype?...the shoulders, clavicles, chest and thighs melt away. This illness
Cancer cachexia: assessment and classification KCH Fearon University of Edinburgh Scotland 1 What is the cancer cachexia phenotype?...the shoulders, clavicles, chest and thighs melt away. This illness
Nutritional requirements in advanced cancer patients
 Nutritional requirements in advanced cancer patients Paula Ravasco p.ravasco@fmedicina.ulisboa.pt Laboratory of Nutrition Faculty of Medicine of the University of Lisbon Medical School of Lisbon Portugal
Nutritional requirements in advanced cancer patients Paula Ravasco p.ravasco@fmedicina.ulisboa.pt Laboratory of Nutrition Faculty of Medicine of the University of Lisbon Medical School of Lisbon Portugal
ESPEN Congress Geneva 2014 LLL LIVE COURSE: NUTRITIONAL SUPPORT IN CANCER. Multimodal therapy of cancer cachexia K. Fearon (UK)
") ESPEN Congress Geneva 2014 LLL LIVE COURSE: NUTRITIONAL SUPPORT IN CANCER Multimodal therapy of cancer cachexia K. Fearon (UK) Multimodal therapy for cancer cachexia KCH Fearon Learning objectives Understand
ESPEN Congress Geneva 2014 LLL LIVE COURSE: NUTRITIONAL SUPPORT IN CANCER Multimodal therapy of cancer cachexia K. Fearon (UK) Multimodal therapy for cancer cachexia KCH Fearon Learning objectives Understand
A new era of therapeutics for cancer cachexia. Cachexia is a continuum with 3 stages of clinical relevance
 A new era of therapeutics for cancer cachexia I. Depletion of Reserves II. Limitation of food intake III. Catabolic Drivers IV. Impact and outcomes Vickie Baracos PhD Professor and Alberta Cancer Foundation
A new era of therapeutics for cancer cachexia I. Depletion of Reserves II. Limitation of food intake III. Catabolic Drivers IV. Impact and outcomes Vickie Baracos PhD Professor and Alberta Cancer Foundation
ESPEN guidelines: Nutritional interventions in advanced cancer care. -An overview and pending research questions
 1 ESPEN guidelines: Nutritional interventions in advanced cancer care -An overview and pending research questions Tora Skeidsvoll Solheim, MD, PhD Oslo, October 2017 2 3 Definition of cachexia Cancer cachexia
1 ESPEN guidelines: Nutritional interventions in advanced cancer care -An overview and pending research questions Tora Skeidsvoll Solheim, MD, PhD Oslo, October 2017 2 3 Definition of cachexia Cancer cachexia
Dr Barry Laird Clinician Scientist in Palliative Medicine University of Edinburgh and the European Palliative Care Research Centre (PRC)
") 1 Dr Barry Laird Clinician Scientist in Palliative Medicine University of Edinburgh and the European Palliative Care Research Centre (PRC) 2 Acknowledgements Prof Marie Fallon (group lead EPAS) University
1 Dr Barry Laird Clinician Scientist in Palliative Medicine University of Edinburgh and the European Palliative Care Research Centre (PRC) 2 Acknowledgements Prof Marie Fallon (group lead EPAS) University
THE UNIVERSITY of EDINBURGH
 THE UNIVERSITY of EDINBURGH Professor Kenneth Fearon MB ChB(Hons), MD, FRCPS (Glasgow), FRCS (Edinburgh), FRCS (England) Memorial Cancer Cachexia Symposium Royal Society of Edinburgh, George Street, Edinburgh
THE UNIVERSITY of EDINBURGH Professor Kenneth Fearon MB ChB(Hons), MD, FRCPS (Glasgow), FRCS (Edinburgh), FRCS (England) Memorial Cancer Cachexia Symposium Royal Society of Edinburgh, George Street, Edinburgh
Classification of (cancer) cachexia: Any improvements to expect?
 cachexia: Any improvements to expect?") 6 th Research Congress of EAPC Glasgow, June 11th 2010 Session Cachexia of EPCRC and EAPC RN Classification of (cancer) cachexia: Any improvements to expect? The joint work of many persons involved, thank
6 th Research Congress of EAPC Glasgow, June 11th 2010 Session Cachexia of EPCRC and EAPC RN Classification of (cancer) cachexia: Any improvements to expect? The joint work of many persons involved, thank
Ingvar Bosaeus, MD, Sahlgrenska University Hospital, Goteborg, Sweden
 Cachexia in Cancer Ingvar Bosaeus, MD, Sahlgrenska University Hospital, Goteborg, Sweden Severe, progressive malnutrition and wasting often is seen in advanced cancer, with weight loss long associated
Cachexia in Cancer Ingvar Bosaeus, MD, Sahlgrenska University Hospital, Goteborg, Sweden Severe, progressive malnutrition and wasting often is seen in advanced cancer, with weight loss long associated
Malnutrition in advanced CKD
 Malnutrition in advanced CKD Malnutrition Lack of proper nutrition, caused by not having enough to eat, not eating enough of the right things or being unable to use the food that one does eat Jessica Stevenson
Malnutrition in advanced CKD Malnutrition Lack of proper nutrition, caused by not having enough to eat, not eating enough of the right things or being unable to use the food that one does eat Jessica Stevenson
Metabolic issues in nutrition: Implications for daily care
 Metabolic issues in nutrition: Implications for daily care Ingvar Bosaeus Dept of Clinical Nutrition Sahlgrenska University Hospital Göteborg, Sweden Nutritional problems in cancer In western countries,
Metabolic issues in nutrition: Implications for daily care Ingvar Bosaeus Dept of Clinical Nutrition Sahlgrenska University Hospital Göteborg, Sweden Nutritional problems in cancer In western countries,
Nutritional Support in Cancer Topic 26
 Nutritional Support in Cancer Topic 26 Module 26.3 Multimodal Therapy for Cancer Cachexia Kenneth Fearon, MD, FRCS(Glas), FRCS(Ed), FRCS(Eng), Professor of Surgical Oncology, Clinical Surgery, University
Nutritional Support in Cancer Topic 26 Module 26.3 Multimodal Therapy for Cancer Cachexia Kenneth Fearon, MD, FRCS(Glas), FRCS(Ed), FRCS(Eng), Professor of Surgical Oncology, Clinical Surgery, University
Nutrition support for sarcopenia in cancer patients
 Nutrition support for sarcopenia in cancer patients Kalliopi Anna Poulia, RD, MMedSci, PhD Clinical Nutritionist-Dietitian, Laiko General Hospital of Athens Vice President of the Hellenic Dietetic Association
Nutrition support for sarcopenia in cancer patients Kalliopi Anna Poulia, RD, MMedSci, PhD Clinical Nutritionist-Dietitian, Laiko General Hospital of Athens Vice President of the Hellenic Dietetic Association
Diet what helps? Lindsey Allan Macmillan Oncology Dietitian Royal Surrey County Hospital, Guildford
 Diet what helps? Lindsey Allan Macmillan Oncology Dietitian Royal Surrey County Hospital, Guildford Diet and cancer Diet and cancer Nutrition research Lack of funding RCTs Low quality Small sample sizes
Diet what helps? Lindsey Allan Macmillan Oncology Dietitian Royal Surrey County Hospital, Guildford Diet and cancer Diet and cancer Nutrition research Lack of funding RCTs Low quality Small sample sizes
Horizon Scanning Centre November Enobosarm (Ostarine) for cachexia in patients with advanced non-small cell lung cancer first line
 for cachexia in patients with advanced non-small cell lung cancer first line") Horizon Scanning Centre November 2012 Enobosarm (Ostarine) for cachexia in patients with advanced non-small cell lung cancer first line SUMMARY NIHR HSC ID: 5206 This briefing is based on information available
Horizon Scanning Centre November 2012 Enobosarm (Ostarine) for cachexia in patients with advanced non-small cell lung cancer first line SUMMARY NIHR HSC ID: 5206 This briefing is based on information available
Cancer Cachexia. Current and Future Management Options
 Cancer Cachexia Current and Future Management Options Cancer Cachexia Overview Symptoms Pathophysiology Current Treatment Options New Drugs Cancer Cachexia Overview " the shoulders, clavicles, chest and
Cancer Cachexia Current and Future Management Options Cancer Cachexia Overview Symptoms Pathophysiology Current Treatment Options New Drugs Cancer Cachexia Overview " the shoulders, clavicles, chest and
Nutritional Support in Cancer
 Nutritional Support in Cancer Topic 26 Module 26.4 Pharmacological and Multimodal Therapy for Cancer Cachexia Learning Objectives Ingvar Bosaeus Kenneth Fearon Grant Stewart Comprehend the importance of
Nutritional Support in Cancer Topic 26 Module 26.4 Pharmacological and Multimodal Therapy for Cancer Cachexia Learning Objectives Ingvar Bosaeus Kenneth Fearon Grant Stewart Comprehend the importance of
nutrition and cancer Weight loss and Quality of Life (QoL) Nutrition and QoL wound healing Surgery & RT hospital stay rehospitalisations Malabsorption
 Nutrition and QoL wound healing Surgery & RT hospital stay rehospitalisations Malabsorption") The impact of nutrition intervention in cancer patients Paula Ravasco Unidade de Nutrição e Metabolismo Instituto de Medicina Molecular Faculdade de Medicina da Universidade de Lisboa deterioration is
The impact of nutrition intervention in cancer patients Paula Ravasco Unidade de Nutrição e Metabolismo Instituto de Medicina Molecular Faculdade de Medicina da Universidade de Lisboa deterioration is
ABC of palliative care: Anorexia, cachexia, and nutrition
 BMJ 1997;315:1219-1222 (8 November) Clinical review ABC of palliative care: Anorexia, cachexia, and nutrition Eduardo Bruera Top Does the patient have... Why is the patient... Cachexia is a complex syndrome
BMJ 1997;315:1219-1222 (8 November) Clinical review ABC of palliative care: Anorexia, cachexia, and nutrition Eduardo Bruera Top Does the patient have... Why is the patient... Cachexia is a complex syndrome
Single Technology Appraisal (STA) Anamorelin for treating cachexia and anorexia in people with non-small-cell lung cancer
 Anamorelin for treating cachexia and anorexia in people with non-small-cell lung cancer") Single Technology Appraisal (STA) Anamorelin for treating cachexia and anorexia in people with non-small-cell Response to consultee and commentator comments on the draft remit and draft scope (pre-referral)
Single Technology Appraisal (STA) Anamorelin for treating cachexia and anorexia in people with non-small-cell Response to consultee and commentator comments on the draft remit and draft scope (pre-referral)
Medical Oncologist/Palliative care Physician Director Cancer Rehabilitation Program Division of Oncology Royal Victoria Hospital MONTREAL
 Eating Drinking, Living after Curative Therapy for Esophageal cancer Dr. Martin Chasen Medical Oncologist/Palliative care Physician Director Cancer Rehabilitation Program Division of Oncology Royal Victoria
Eating Drinking, Living after Curative Therapy for Esophageal cancer Dr. Martin Chasen Medical Oncologist/Palliative care Physician Director Cancer Rehabilitation Program Division of Oncology Royal Victoria
Renal cachexia. Professor Joanne Reid
 Renal cachexia Professor Joanne Reid Cachexia Cachexia is a complex metabolic syndrome associated with underlying illness and characterised by muscle loss, with or without loss of fat Definition of cachexia
Renal cachexia Professor Joanne Reid Cachexia Cachexia is a complex metabolic syndrome associated with underlying illness and characterised by muscle loss, with or without loss of fat Definition of cachexia
TITLE: Nutritional Supplementation for Patients with Cancer: A Review of the Clinical Effectiveness and Guidelines
 TITLE: Nutritional Supplementation for Patients with Cancer: A Review of the Clinical Effectiveness and Guidelines DATE: 12 February 2014 CONTEXT AND POLICY ISSUES People with cancer who are well nourished
TITLE: Nutritional Supplementation for Patients with Cancer: A Review of the Clinical Effectiveness and Guidelines DATE: 12 February 2014 CONTEXT AND POLICY ISSUES People with cancer who are well nourished
MILK. Nutritious by nature. The science behind the health and nutritional impact of milk and dairy foods
 MILK Nutritious by nature The science behind the health and nutritional impact of milk and dairy foods Muscle mass maintenance in older people There is evidence to suggest a potential role for milk and
MILK Nutritious by nature The science behind the health and nutritional impact of milk and dairy foods Muscle mass maintenance in older people There is evidence to suggest a potential role for milk and
O ρόλος της διατροφής κατά τη θεραπεία του καρκίνου
 O ρόλος της διατροφής κατά τη θεραπεία του καρκίνου I. Gioulbasanis MD, PhD Dept. of Chemotherapy Larissa General Clinic E. Patsidis INTRODUCTION Καρκινογένεση Ενεργός Νόσος Επιβιώσαντες με καρκίνο (cancer
O ρόλος της διατροφής κατά τη θεραπεία του καρκίνου I. Gioulbasanis MD, PhD Dept. of Chemotherapy Larissa General Clinic E. Patsidis INTRODUCTION Καρκινογένεση Ενεργός Νόσος Επιβιώσαντες με καρκίνο (cancer
ANAMORELIN FOR CACHEXIA. Series 20 CASE REPORT FORM
 1 ANAMORELIN FOR CACHEXIA Series 20 CASE REPORT FORM Palliative Care Clinical Studies Collaborative (PaCCSC) RAPID Pharmacovigilance in Palliative Care The case report form (CRF) is to be completed in
1 ANAMORELIN FOR CACHEXIA Series 20 CASE REPORT FORM Palliative Care Clinical Studies Collaborative (PaCCSC) RAPID Pharmacovigilance in Palliative Care The case report form (CRF) is to be completed in
Clinical Nutrition in the 21st Century Malnutrition, sarcopenia and cachexia
 Clinical Nutrition in the 21st Century Malnutrition, sarcopenia and cachexia Stéphane M. Schneider, MD, PhD, FEBGH Professor of Nutrition and ESPEN ECPC Chair In proto-indo-european, Latin and Greek Under
Clinical Nutrition in the 21st Century Malnutrition, sarcopenia and cachexia Stéphane M. Schneider, MD, PhD, FEBGH Professor of Nutrition and ESPEN ECPC Chair In proto-indo-european, Latin and Greek Under
ProSure. Strength to Fight and Get Back to Life. Strength to Fight and Get Back to Life D1
 ProSure Strength to Fight and Get Back to Life ProSure. Strength to Fight and Get Back to Life 5004 1112 166 D1 Cancer care is evolving at an incredibly fast pace, and the prognosis for a person with cancer
ProSure Strength to Fight and Get Back to Life ProSure. Strength to Fight and Get Back to Life 5004 1112 166 D1 Cancer care is evolving at an incredibly fast pace, and the prognosis for a person with cancer
Integration of palliative care into oncology
 1 Integration of palliative care into oncology Stein Kaasa European Palliative Care Research Centre, Faculty of Medicine, NTNU and Department of Oncology, St. Olavs Hospital, Trondheim University Hospital
1 Integration of palliative care into oncology Stein Kaasa European Palliative Care Research Centre, Faculty of Medicine, NTNU and Department of Oncology, St. Olavs Hospital, Trondheim University Hospital
Infographic (right): ESMO 2014 record breaking Congress
: ESMO 2014 record breaking Congress") ESMO 2014 Congress Scientific Meeting Report Supportive and Palliative Care Extract 26-30 September 2014 Madrid, Spain Summary The European Society for Medical Oncology (ESMO) Congress, held September
ESMO 2014 Congress Scientific Meeting Report Supportive and Palliative Care Extract 26-30 September 2014 Madrid, Spain Summary The European Society for Medical Oncology (ESMO) Congress, held September
How do we adapt diet approaches for patients with obesity with or without diabetes? Therese Coleman Dietitian
 How do we adapt diet approaches for patients with obesity with or without diabetes? Therese Coleman Dietitian Developing a specialist weight management programme How did we adapt dietary approaches for
How do we adapt diet approaches for patients with obesity with or without diabetes? Therese Coleman Dietitian Developing a specialist weight management programme How did we adapt dietary approaches for
FATIGUE: PHARMACOLOGICAL AND NON-PHARMACOLOGICAL TREATMENT. Fausto Roila Medical Oncology Division, Terni, Italy
 FATIGUE: PHARMACOLOGICAL AND NON-PHARMACOLOGICAL TREATMENT Fausto Roila Medical Oncology Division, Terni, Italy CONFLICT OF INTERESTS NO CONFLICT FATIGUE: DEFINITION (ASCO, NCCN) Cancer-related fatigue
FATIGUE: PHARMACOLOGICAL AND NON-PHARMACOLOGICAL TREATMENT Fausto Roila Medical Oncology Division, Terni, Italy CONFLICT OF INTERESTS NO CONFLICT FATIGUE: DEFINITION (ASCO, NCCN) Cancer-related fatigue
Learning objectives. What is nutritional care? NUTRITIONAL ISSUES IN CANCER
 NUTRITIONAL ISSUES IN CANCER Jane Hopkinson PhD, RGN Macmillan Post Doctoral Fellow Faculty of Health Sciences, University of Southampton, UK 1 Learning objectives q To understand contributory factors
NUTRITIONAL ISSUES IN CANCER Jane Hopkinson PhD, RGN Macmillan Post Doctoral Fellow Faculty of Health Sciences, University of Southampton, UK 1 Learning objectives q To understand contributory factors
Physical activity in cancer patients
 Physical activity in cancer patients Fernando C. Dimeo, MD Department of Sports Medicine The secret of a long life? Traditional approach Cancer patients should rest, reduce activity and avoid intense efforts
Physical activity in cancer patients Fernando C. Dimeo, MD Department of Sports Medicine The secret of a long life? Traditional approach Cancer patients should rest, reduce activity and avoid intense efforts
Nutritional Counselling, cancer Outcome and Quality of Life!
 Nutritional Counselling, cancer Outcome and Quality of Life! Paula Ravasco p.ravasco@fm.ul.pt Unit of Nutrition and Metabolism, Institute of Molecular Medicine Faculty of Medicine of the University of
Nutritional Counselling, cancer Outcome and Quality of Life! Paula Ravasco p.ravasco@fm.ul.pt Unit of Nutrition and Metabolism, Institute of Molecular Medicine Faculty of Medicine of the University of
Pharmacological treatments. Jann Arends Tumor Biology Center Freiburg, Germany
 Pharmacological treatments Jann Arends Tumor Biology Center Freiburg, Germany Pharmacologic treatment: Basic concept Interfere with undesired physiology Drug a specific target Major problems in cachexia
Pharmacological treatments Jann Arends Tumor Biology Center Freiburg, Germany Pharmacologic treatment: Basic concept Interfere with undesired physiology Drug a specific target Major problems in cachexia
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Altering lifestyle to improve nutritional status in older adults Nutritional interventions to prevent and treat frailty F. Landi (IT) Nutritional interventions to prevent
ESPEN Congress The Hague 2017 Altering lifestyle to improve nutritional status in older adults Nutritional interventions to prevent and treat frailty F. Landi (IT) Nutritional interventions to prevent
A randomized phase II feasibility trial of a multimodal intervention for the management of cachexia in lung and pancreatic cancer
 Journal of Cachexia, Sarcopenia and Muscle (2017) Published online in Wiley Online Library (wileyonlinelibrary.com) ORIGINAL ARTICLE A randomized phase II feasibility trial of a multimodal intervention
Journal of Cachexia, Sarcopenia and Muscle (2017) Published online in Wiley Online Library (wileyonlinelibrary.com) ORIGINAL ARTICLE A randomized phase II feasibility trial of a multimodal intervention
The Challenge of Cancer Cachexia
 The Challenge of Cancer Cachexia Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Director, Solid Tumor Therapeutics Program Duke Cancer Institute Disclosures Advisory Board/Consultant:
The Challenge of Cancer Cachexia Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Director, Solid Tumor Therapeutics Program Duke Cancer Institute Disclosures Advisory Board/Consultant:
To see a description of the Academy Recommendation Rating Scheme (Strong, Fair, Weak, Consensus, Insufficient Evidence) visit the EAL.
 visit the EAL.") WWW.ANDEAL.ORG HEART FAILURE HF: EXECUTIVE SUMMARY OF RECOMMENDATIONS (2017) Executive Summary of Recommendations Below are the major recommendations and ratings for the Academy of Nutrition and Dietetics
WWW.ANDEAL.ORG HEART FAILURE HF: EXECUTIVE SUMMARY OF RECOMMENDATIONS (2017) Executive Summary of Recommendations Below are the major recommendations and ratings for the Academy of Nutrition and Dietetics
Malnutrition in Adults: Guidelines for Identification and Treatment
 Malnutrition in Adults: Guidelines for Identification and Treatment Signatures (e.g. chair of the ratifying committee and lay member) and date Signature...date Designation: Signature...date Designation
Malnutrition in Adults: Guidelines for Identification and Treatment Signatures (e.g. chair of the ratifying committee and lay member) and date Signature...date Designation: Signature...date Designation
Transitioning to palliative care: How early is early palliative care?
 Transitioning to palliative care: How early is early palliative care? Cancer: a growing problem Cancer is an increasing health care problem It is estimated that by 2020, there will be 20 million new cases
Transitioning to palliative care: How early is early palliative care? Cancer: a growing problem Cancer is an increasing health care problem It is estimated that by 2020, there will be 20 million new cases
Nutrition. By Dr. Ali Saleh 2/27/2014 1
 Nutrition By Dr. Ali Saleh 2/27/2014 1 Nutrition Functions of nutrients: Providing energy for body processes and movement. Providing structural material for body tissues. Regulating body processes. 2/27/2014
Nutrition By Dr. Ali Saleh 2/27/2014 1 Nutrition Functions of nutrients: Providing energy for body processes and movement. Providing structural material for body tissues. Regulating body processes. 2/27/2014
Palliative Care The Benefits of Early Intervention
 The Royal Marsden Palliative Care The Benefits of Early Intervention Dr Anna-Marie Stevens, Nurse Consultant Symptom Control and Palliative Care Team, The Royal Marsden NHS Foundation Trust, London, UK
The Royal Marsden Palliative Care The Benefits of Early Intervention Dr Anna-Marie Stevens, Nurse Consultant Symptom Control and Palliative Care Team, The Royal Marsden NHS Foundation Trust, London, UK
BAOJ Palliative medicine
 Vol:, Issue: Abstract Randomised Controlled Trial of Fish Oil Supplement to Treat Cancer Cachexia Dewey A, Higgins B, Baughan C, Stores R, 4 Dean T, Sally Kilburn School of Health Sciences and Social Work,
Vol:, Issue: Abstract Randomised Controlled Trial of Fish Oil Supplement to Treat Cancer Cachexia Dewey A, Higgins B, Baughan C, Stores R, 4 Dean T, Sally Kilburn School of Health Sciences and Social Work,
ROLE OF A DIETITIAN & KEEPING HYDRATED. Emily Capener Haematology Dietitian UHW
 ROLE OF A DIETITIAN & KEEPING HYDRATED Emily Capener Haematology Dietitian UHW We will cover: PART 1 What is a dietitian Where do dietitans work About an acute dietitians role - Screening - Food charts
ROLE OF A DIETITIAN & KEEPING HYDRATED Emily Capener Haematology Dietitian UHW We will cover: PART 1 What is a dietitian Where do dietitans work About an acute dietitians role - Screening - Food charts
Cancer Survivorship NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN. Resources and Tools for the Multidisciplinary Team
 NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN Cancer Survivorship Resources and Tools for the Multidisciplinary Team Your survivorship care plan is a summary of your tumor treatments and recommendations for
NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN Cancer Survivorship Resources and Tools for the Multidisciplinary Team Your survivorship care plan is a summary of your tumor treatments and recommendations for
Dietary practices in patients with chronic kidney disease not yet on maintenance dialysis: What are the relevant components?
 Dietary practices in patients with chronic kidney disease not yet on maintenance dialysis: What are the relevant components? 3 rd International Conference of European Renal Nutrition Working Group of ERA-EDTA
Dietary practices in patients with chronic kidney disease not yet on maintenance dialysis: What are the relevant components? 3 rd International Conference of European Renal Nutrition Working Group of ERA-EDTA
A critical appraisal of: Canadian guideline fysisk aktivitet using the AGREE II Instrument
 A critical appraisal of: Canadian guideline fysisk aktivitet using the AGREE II Instrument Created with the AGREE II Online Guideline Appraisal Tool. No endorsement of the content of this document by the
A critical appraisal of: Canadian guideline fysisk aktivitet using the AGREE II Instrument Created with the AGREE II Online Guideline Appraisal Tool. No endorsement of the content of this document by the
Molecular Mechanisms associated with the Cancer-Cachexia Syndrome
 Molecular Mechanisms associated with the Cancer-Cachexia Syndrome Prof. Dr. Josep M. Argilés Department of Biochemistry & Molecular Biology University of Barcelona, Spain Disclosures: DANONE (Scientific
Molecular Mechanisms associated with the Cancer-Cachexia Syndrome Prof. Dr. Josep M. Argilés Department of Biochemistry & Molecular Biology University of Barcelona, Spain Disclosures: DANONE (Scientific
CANCER CACHEXIA. Negativity cancer nutrition. Do we think it s s important? Lack of past success alimentation trials counselling therapeutic failures
 CANCER CACHEXIA A wasting syndrome characterized by loss of muscle and fat caused by an aberrant host response to a wide variety of chronic illnesses. Anorexia usually accompanies cachexia,, and is caused
CANCER CACHEXIA A wasting syndrome characterized by loss of muscle and fat caused by an aberrant host response to a wide variety of chronic illnesses. Anorexia usually accompanies cachexia,, and is caused
Nutrition Update: Anorexia and Cachexia
 Nutrition Update: Anorexia and Cachexia Kristen Kreamer, AOCNP, APRN-BC, CRNP, MSN Barbara Rogers, CRNP, AOCN, APN-BC, MN Fox Chase Cancer Center Nutrition Update: Anorexia and Cachexia LEARNING OBJECTIVES:
Nutrition Update: Anorexia and Cachexia Kristen Kreamer, AOCNP, APRN-BC, CRNP, MSN Barbara Rogers, CRNP, AOCN, APN-BC, MN Fox Chase Cancer Center Nutrition Update: Anorexia and Cachexia LEARNING OBJECTIVES:
Nutrition Update: Anorexia and Cachexia
 Nutrition Update: Anorexia and Cachexia Kristen Kreamer, AOCNP, APRN-BC, CRNP, MS Fox Chase Cancer Center Faculty Biography Kristen Kreamer, AOCNP, APRN-BC, CRNP, MSN is Nurse Practitioner, Ambulatory
Nutrition Update: Anorexia and Cachexia Kristen Kreamer, AOCNP, APRN-BC, CRNP, MS Fox Chase Cancer Center Faculty Biography Kristen Kreamer, AOCNP, APRN-BC, CRNP, MSN is Nurse Practitioner, Ambulatory
GP, Community Nurse and Specialist Nurse Oral Nutritional Supplement (ONS) Formulary for Adults
 Formulary for Adults") GP, Community Nurse and Specialist Nurse Oral Nutritional Supplement (ONS) Formulary for Adults ALWAYS use the Food First approach before considering prescribing ONS (This includes over the counter ONS
GP, Community Nurse and Specialist Nurse Oral Nutritional Supplement (ONS) Formulary for Adults ALWAYS use the Food First approach before considering prescribing ONS (This includes over the counter ONS
Nutritional care during and after chemo- and radiotherapy. M. Larsson (SE)
") ESPEN Congress Leipzig 2013 Nursing Session Nutritional care during and after chemo- and radiotherapy M. Larsson (SE) Nutritional care during and after chemo- and radiotherapy Maria Larsson, RN, PhD Nurse
ESPEN Congress Leipzig 2013 Nursing Session Nutritional care during and after chemo- and radiotherapy M. Larsson (SE) Nutritional care during and after chemo- and radiotherapy Maria Larsson, RN, PhD Nurse
Prescribing Guidelines for Oral Nutritional Supplements (ONS) for adults
 for adults") Worcestershire Area Prescribing Committee Prescribing Guidelines for Oral Nutritional Supplements (ONS) for adults September 2017 Review Date September 2020 Version 3.0 1 Version Control: Version Type
Worcestershire Area Prescribing Committee Prescribing Guidelines for Oral Nutritional Supplements (ONS) for adults September 2017 Review Date September 2020 Version 3.0 1 Version Control: Version Type
Beyond BMI: Nutritional Strategies to Manage Loss of Muscle Mass and Function in Hospital and Community Francesco Landi, MD, PhD
 Beyond BMI: Nutritional Strategies to Manage Loss of Muscle Mass and Function in Hospital and Community Francesco Landi, MD, PhD Catholic University, Geriatric Center, Gemelli Hospital - Rome, Italy Disclosures
Beyond BMI: Nutritional Strategies to Manage Loss of Muscle Mass and Function in Hospital and Community Francesco Landi, MD, PhD Catholic University, Geriatric Center, Gemelli Hospital - Rome, Italy Disclosures
Combination therapy in cachexia
 Review Article Combination therapy in cachexia Egidio Del Fabbro Virginia Commonwealth University, Richmond, VA, USA Correspondence to: Egidio Del Fabbro, MD. Virginia Commonwealth University, 1101 E Marshall
Review Article Combination therapy in cachexia Egidio Del Fabbro Virginia Commonwealth University, Richmond, VA, USA Correspondence to: Egidio Del Fabbro, MD. Virginia Commonwealth University, 1101 E Marshall
25/11/2015 OVERVIEW DEFINITION OF PALLIATIVE CARE FURTHERMORE.. PALLIATIVE PERFORMANCE SCALE (PPS) CACHEXIA OF ADVANCED DISEASE
 CACHEXIA OF ADVANCED DISEASE") ARTIFICIAL ENTERAL FEEDING IN PATIENTS WITH INCURABLE HEAD & NECK TUMOURS PROGNOSIS INFORMING DECISION MAKING JENNY HANSEN, RN, BN, MNurs CNS Palliative Care Waikato Hospital OVERVIEW What is palliative
ARTIFICIAL ENTERAL FEEDING IN PATIENTS WITH INCURABLE HEAD & NECK TUMOURS PROGNOSIS INFORMING DECISION MAKING JENNY HANSEN, RN, BN, MNurs CNS Palliative Care Waikato Hospital OVERVIEW What is palliative
ESPEN Congress Leipzig 2013
 ESPEN Congress Leipzig 2013 Nutrition and cancer: impact on outcome Survival, quality of life, reduced toxicity: what can be achieved in cancer patients? M.A.E. van Bokhorst - de van der Schueren (NL)
ESPEN Congress Leipzig 2013 Nutrition and cancer: impact on outcome Survival, quality of life, reduced toxicity: what can be achieved in cancer patients? M.A.E. van Bokhorst - de van der Schueren (NL)
Nursing in Scotland. Glasgow & Clyde Weight Management Service
 Nursing in Scotland Glasgow & Clyde Weight Management Service Contact: Dr Marie L Prince Chartered Clinical Psychologist marie.prince@ggc.scot.nhs.uk GCWMS Ward 23 Surgical Block Glasgow Royal Infirmary
Nursing in Scotland Glasgow & Clyde Weight Management Service Contact: Dr Marie L Prince Chartered Clinical Psychologist marie.prince@ggc.scot.nhs.uk GCWMS Ward 23 Surgical Block Glasgow Royal Infirmary
Oxygen Use in Palliative Care Guideline and Flowchart
 Oxygen Use in Palliative Care Guideline and Flowchart Reviewed: October 2013 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy. Title Keywords Ratified Oxygen Use in Palliative
Oxygen Use in Palliative Care Guideline and Flowchart Reviewed: October 2013 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy. Title Keywords Ratified Oxygen Use in Palliative
ESPEN Congress Copenhagen 2016
 ESPEN Congress Copenhagen 2016 PARENTERAL NUTRITION IN ONCOLOGY PATIENTS INDICATIONS AND CONTRAINDICATIONS F. Bozzetti (IT) Parenteral nutrition in oncology patients indications and contraindications Federico
ESPEN Congress Copenhagen 2016 PARENTERAL NUTRITION IN ONCOLOGY PATIENTS INDICATIONS AND CONTRAINDICATIONS F. Bozzetti (IT) Parenteral nutrition in oncology patients indications and contraindications Federico
DIET, NUTRITION AND HEAD AND NECK CANCER TREATMENT
 DIET, NUTRITION AND HEAD AND NECK CANCER TREATMENT DIET, NUTRITION AND HEAD AND NECK CANCER TREATMENT HOW HEAD AND NECK CANCER MAY AFFECT NUTRITION Head and neck cancer may make it hard to eat and drink.
DIET, NUTRITION AND HEAD AND NECK CANCER TREATMENT DIET, NUTRITION AND HEAD AND NECK CANCER TREATMENT HOW HEAD AND NECK CANCER MAY AFFECT NUTRITION Head and neck cancer may make it hard to eat and drink.
Physical exercise interventions in cancer survivors
 Physical exercise in cancer survivors Effects and methodological issues Anne May, PhD September 2 nd, 2016 Hot Topic Conference: Life Course Influences and Mechanisms: Obesity, Physical Activity & Cancer
Physical exercise in cancer survivors Effects and methodological issues Anne May, PhD September 2 nd, 2016 Hot Topic Conference: Life Course Influences and Mechanisms: Obesity, Physical Activity & Cancer
ROLE OF THE DIETITIAN. Aims of Dietetic Treatment NUTRITIONAL ISSUES WHY? MALNUTRITION NUTRITONAL MANAGEMENT OF MOTOR NEURONE DISEASE.
 NUTRITONAL MANAGEMENT OF MOTOR NEURONE DISEASE. ROLE OF THE DIETITIAN SALLY DARBY NEUROLOGY DIETITIAN Not just tube feeding Referral soon after diagnosis Advise on healthy eating for MND Monitor nutritional
NUTRITONAL MANAGEMENT OF MOTOR NEURONE DISEASE. ROLE OF THE DIETITIAN SALLY DARBY NEUROLOGY DIETITIAN Not just tube feeding Referral soon after diagnosis Advise on healthy eating for MND Monitor nutritional
Weakness & Fatigue. Introduction. Assessment
 Weakness & Fatigue Introduction Fatigue is a persistent, subjective feeling of tiredness, weakness or lack of energy related to advanced chronic illness. It has many contributory causes though the exact
Weakness & Fatigue Introduction Fatigue is a persistent, subjective feeling of tiredness, weakness or lack of energy related to advanced chronic illness. It has many contributory causes though the exact
Ruolo della nutrizione clinica nella gestione del paziente anziano fragile con riduzione di forza fisica
 Ruolo della nutrizione clinica nella gestione del paziente anziano fragile con riduzione di forza fisica Roberto Pisati, MD Medical, Regulatory and Public Affairs Balance and gait impairment: major features
Ruolo della nutrizione clinica nella gestione del paziente anziano fragile con riduzione di forza fisica Roberto Pisati, MD Medical, Regulatory and Public Affairs Balance and gait impairment: major features
What are steroids and how do they work?
 For over 20 years boys with Duchenne muscular dystrophy (MD) have been treated with steroids, which is currently the only medication proven to slow the progression of the condition. In Australia, more
For over 20 years boys with Duchenne muscular dystrophy (MD) have been treated with steroids, which is currently the only medication proven to slow the progression of the condition. In Australia, more
Symptom Control in Cancer Rehabilitation. Ying Guo, MD Department of Palliative, Rehabilitation and Integrative Medicine UT MD Anderson Cancer Center
 Symptom Control in Cancer Rehabilitation Ying Guo, MD Department of Palliative, Rehabilitation and Integrative Medicine UT MD Anderson Cancer Center Cancer Patients Symptoms Pain- 90% of patients with
Symptom Control in Cancer Rehabilitation Ying Guo, MD Department of Palliative, Rehabilitation and Integrative Medicine UT MD Anderson Cancer Center Cancer Patients Symptoms Pain- 90% of patients with
Adelaide Circle of Care, Flinders Private Hospital/Flinders University of South Australia, South Australia, Australia Lilian Kow
 Preoperative Treatment with Very Low Calorie Diet Adelaide Circle of Care, Flinders Private Hospital/Flinders University of South Australia, South Australia, Australia Lilian Kow Obesity is the most significant
Preoperative Treatment with Very Low Calorie Diet Adelaide Circle of Care, Flinders Private Hospital/Flinders University of South Australia, South Australia, Australia Lilian Kow Obesity is the most significant
of interventions to promote healthy lifestyle behaviours
 A systematic overview of reviews of the effectiveness and cost effectiveness of interventions to promote healthy lifestyle behaviours in people living with or beyond cancer. Brunel University London RAND
A systematic overview of reviews of the effectiveness and cost effectiveness of interventions to promote healthy lifestyle behaviours in people living with or beyond cancer. Brunel University London RAND
Innovations in Nutritional Therapy for Cats with CKD Rebecca Mullis, DVM, DACVN
 Innovations in Nutritional Therapy for Cats with CKD Rebecca Mullis, DVM, DACVN Content presented at the 2017 Hill s Global Symposium in Washington D.C., May 5-6, 2017. Chronic kidney disease (CKD) is
Innovations in Nutritional Therapy for Cats with CKD Rebecca Mullis, DVM, DACVN Content presented at the 2017 Hill s Global Symposium in Washington D.C., May 5-6, 2017. Chronic kidney disease (CKD) is
Physiotherapy in Breast Cancer: developing clinical practice
 Physiotherapy in Breast Cancer: developing clinical practice Dr Karen Robb Macmillan Cancer Rehabilitation Strategy Development Manager Consultant Physiotherapist Member of Macmillan Consequences of Cancer
Physiotherapy in Breast Cancer: developing clinical practice Dr Karen Robb Macmillan Cancer Rehabilitation Strategy Development Manager Consultant Physiotherapist Member of Macmillan Consequences of Cancer
Frailty in Older Adults. Frailty
 Frailty in Older Adults Nancy Stiles, MD Associate Professor Geriatrics i Sanders-Brown Center on Aging University of Kentucky Frailty Global impairment of physiological reserves involving i multiple l
Frailty in Older Adults Nancy Stiles, MD Associate Professor Geriatrics i Sanders-Brown Center on Aging University of Kentucky Frailty Global impairment of physiological reserves involving i multiple l
What else is new (symptoms)? DR ANDREW DAVIES
? DR ANDREW DAVIES") What else is new (symptoms)? DR ANDREW DAVIES Introduction Outline Rapid onset opioids for episodic breathlessness Alcohol for anorexia (white wine) Rapid onset opioids for episodic breathlessness Episodic
What else is new (symptoms)? DR ANDREW DAVIES Introduction Outline Rapid onset opioids for episodic breathlessness Alcohol for anorexia (white wine) Rapid onset opioids for episodic breathlessness Episodic
Endpoints And Indications For The Older Population
 Endpoints And Indications For The Older Population William J. Evans, Head Muscle Metabolism Discovery Unit, Metabolic Pathways & Cardiovascular Therapy Area Outline Functional Endpoints and Geriatrics
Endpoints And Indications For The Older Population William J. Evans, Head Muscle Metabolism Discovery Unit, Metabolic Pathways & Cardiovascular Therapy Area Outline Functional Endpoints and Geriatrics
Nutritional Interventions for Children with Cystic Fibrosis
 Nutritional Interventions for Children with Cystic Fibrosis Prepared by: Scottish CF Paediatric Dietitians Group Lead Author: Elsie Thomson, Royal Aberdeen Childrens Hospital SPCF MCN Dietetic Protocols
Nutritional Interventions for Children with Cystic Fibrosis Prepared by: Scottish CF Paediatric Dietitians Group Lead Author: Elsie Thomson, Royal Aberdeen Childrens Hospital SPCF MCN Dietetic Protocols
Enhanced Recovery Programme Liver surgery
 Enhanced Recovery Programme Liver surgery General Surgery Patient information leaflet Introduction When you are admitted to hospital for your surgery you will be taking part in an enhanced recovery programme.
Enhanced Recovery Programme Liver surgery General Surgery Patient information leaflet Introduction When you are admitted to hospital for your surgery you will be taking part in an enhanced recovery programme.
ESPEN Congress Geneva 2014 LLL LIVE COURSE: NUTRITIONAL SUPPORT IN CANCER. Mechanisms and clinical features of cachexia P.
 ESPEN Congress Geneva 2014 LLL LIVE COURSE: NUTRITIONAL SUPPORT IN CANCER Mechanisms and clinical features of cachexia P. Ravasco (PT) Mechanisms and clinical features of nutritional patterns in cancer
ESPEN Congress Geneva 2014 LLL LIVE COURSE: NUTRITIONAL SUPPORT IN CANCER Mechanisms and clinical features of cachexia P. Ravasco (PT) Mechanisms and clinical features of nutritional patterns in cancer
Palliative Care Asking the questions that matter to me
 Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Integrating Palliative and Oncology Care in Patients with Advanced Cancer
 Integrating Palliative and Oncology Care in Patients with Advanced Cancer Jennifer Temel, MD Massachusetts General Hospital Cancer Center Director, Cancer Outcomes Research Overview 1. Why should we be
Integrating Palliative and Oncology Care in Patients with Advanced Cancer Jennifer Temel, MD Massachusetts General Hospital Cancer Center Director, Cancer Outcomes Research Overview 1. Why should we be
The physiofirst pilot study: A pilot randomised clinical trial for the efficacy of a targeted physiotherapy intervention for
 The physiofirst pilot study: A pilot randomised clinical trial for the efficacy of a targeted physiotherapy intervention for Click to edit Master title style femoroacetabular impingement syndrome (FAIS)
The physiofirst pilot study: A pilot randomised clinical trial for the efficacy of a targeted physiotherapy intervention for Click to edit Master title style femoroacetabular impingement syndrome (FAIS)
Early Integration of Palliative Care
 Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Integrative Pain Treatment Center Programs Scope of Services
 Integrative Pain Treatment Center Programs Scope of Services The Integrative Pain Treatment Center at Marianjoy Rehabilitation Hospital, part of Northwestern Medicine, offers two specialized 21-day outpatient
Integrative Pain Treatment Center Programs Scope of Services The Integrative Pain Treatment Center at Marianjoy Rehabilitation Hospital, part of Northwestern Medicine, offers two specialized 21-day outpatient
Protein Requirements for Optimal Health in Older Adults: Current Recommendations and New Evidence
 DASPEN 2013 Aarhus, Denmark, May 3 2013 Protein Requirements for Optimal Health in Older Adults: Current Recommendations and New Evidence Elena Volpi, MD, PhD Claude D. Pepper Older Americans Independence
DASPEN 2013 Aarhus, Denmark, May 3 2013 Protein Requirements for Optimal Health in Older Adults: Current Recommendations and New Evidence Elena Volpi, MD, PhD Claude D. Pepper Older Americans Independence
ABDOMEN TREATMENT INFORMATION BOOKLET
 ABDOMEN TREATMENT INFORMATION BOOKLET Department of Radiation Oncology Cancer Services, University Hospital Geelong. CONTENTS 1 What is radiotherapy? 2 What is the process? 5 Will I feel anything? 5 How
ABDOMEN TREATMENT INFORMATION BOOKLET Department of Radiation Oncology Cancer Services, University Hospital Geelong. CONTENTS 1 What is radiotherapy? 2 What is the process? 5 Will I feel anything? 5 How
Breast SSG Education Event Anglia Cancer Network Sally Donaghey Macmillan AHP Lead
 Breast SSG Education Event Anglia Cancer Network 10.2.2012 Sally Donaghey Macmillan AHP Lead sally.donaghey@suffolk.pct.nhs.uk IPx People affected by cancer need information that is timely, relevant, and
Breast SSG Education Event Anglia Cancer Network 10.2.2012 Sally Donaghey Macmillan AHP Lead sally.donaghey@suffolk.pct.nhs.uk IPx People affected by cancer need information that is timely, relevant, and
Non-pharmacological interventions as a means to promote healthy ageing
 Non-pharmacological interventions as a means to promote healthy ageing Dr Theocharis Ispoglou Senior Lecturer in Sport and Exercise Physiology and Nutrition, PhD, MSc, PGCHE, ASCC, Senior HEA Fellow, Carnegie
Non-pharmacological interventions as a means to promote healthy ageing Dr Theocharis Ispoglou Senior Lecturer in Sport and Exercise Physiology and Nutrition, PhD, MSc, PGCHE, ASCC, Senior HEA Fellow, Carnegie
Nutritional Support in the Perioperative Period
 Nutritional Support in the Perioperative Period Topic 17 Module 17.3 Nutritional Support in the Perioperative Period Ken Fearon Learning Objectives Understand the principles behind nutritional care for
Nutritional Support in the Perioperative Period Topic 17 Module 17.3 Nutritional Support in the Perioperative Period Ken Fearon Learning Objectives Understand the principles behind nutritional care for
1st Abbott International Conference for Cancer Nutrition Therapy. Proceedings Booklet
 1st Abbott International Conference for Cancer Nutrition Therapy Proceedings Booklet The 1st Abbott International Conference for Cancer Nutrition Therapy April 12-14, 2010 The 1st Abbott International
1st Abbott International Conference for Cancer Nutrition Therapy Proceedings Booklet The 1st Abbott International Conference for Cancer Nutrition Therapy April 12-14, 2010 The 1st Abbott International
MUST and Malnutrition
 MUST and Malnutrition Presenter Housekeeping Northern Devon Healthcare NHS Trust Confidentiality To respect confidentiality within the group unless it is necessary to address a current concern about the
MUST and Malnutrition Presenter Housekeeping Northern Devon Healthcare NHS Trust Confidentiality To respect confidentiality within the group unless it is necessary to address a current concern about the
Exercise Caroline Belchamber MSc, BSc (Hons), PGCE, FHEA, RFRSM Chartered Physiotherapist and Lecturer: November 2012
, PGCE, FHEA, RFRSM Chartered Physiotherapist and Lecturer: November 2012") Exercise Caroline Belchamber MSc, BSc (Hons), PGCE, FHEA, RFRSM Chartered Physiotherapist and Lecturer: November 2012 What is the recommended number of times a week that you should exercise? 1. 3 to 5
Exercise Caroline Belchamber MSc, BSc (Hons), PGCE, FHEA, RFRSM Chartered Physiotherapist and Lecturer: November 2012 What is the recommended number of times a week that you should exercise? 1. 3 to 5
nutritionday November 2015 in UNITED STATES OF AMERICA
 Country Oncology Report nutritionday November 2015 in UNITED STATES OF AMERICA May 2016 Dear participant, thank you for your participation in nutritionday worldwide in November 2015 and for your effort.
Country Oncology Report nutritionday November 2015 in UNITED STATES OF AMERICA May 2016 Dear participant, thank you for your participation in nutritionday worldwide in November 2015 and for your effort.
Your oncology report reference results are based on data of cancer patients of all specialties of nutritionday 2015.
 Country Oncology Report May 2016 nutritionday November 2015 in JAPAN Dear participant, thank you for your participation in nutritionday worldwide in November 2015 and for your effort. We are now able to
Country Oncology Report May 2016 nutritionday November 2015 in JAPAN Dear participant, thank you for your participation in nutritionday worldwide in November 2015 and for your effort. We are now able to
A snapshot of inpatient oncology rehabilitation: Patient profiles and rehab outcomes Rehabilitation Rounds, University of Toronto April 5, 2012
 A snapshot of inpatient oncology rehabilitation: Patient profiles and rehab outcomes Rehabilitation Rounds, University of Toronto April 5, 2012 Sara McEwen, PT, PhD Research Scientist, St. John s Rehab
A snapshot of inpatient oncology rehabilitation: Patient profiles and rehab outcomes Rehabilitation Rounds, University of Toronto April 5, 2012 Sara McEwen, PT, PhD Research Scientist, St. John s Rehab
Physical activity, Obesity, Diet and Colorectal Cancer Prognosis. Jeffrey Meyerhardt, MD, MPH Dana-Farber Cancer Institute Boston, MA
 Physical activity, Obesity, Diet and Colorectal Cancer Prognosis Jeffrey Meyerhardt, MD, MPH Dana-Farber Cancer Institute Boston, MA Colorectal Cancer Incidence ~148,000 cases in US annually and ~50,000
Physical activity, Obesity, Diet and Colorectal Cancer Prognosis Jeffrey Meyerhardt, MD, MPH Dana-Farber Cancer Institute Boston, MA Colorectal Cancer Incidence ~148,000 cases in US annually and ~50,000