Evolving Concepts in Breast Surgery in Multidisciplinary Care
|
|
|
- Ethel Armstrong
- 5 years ago
- Views:
Transcription

1 Evolving Concepts in Breast Surgery in Multidisciplinary Care Tina J. Hieken MD, FACS Associate Professor of Surgery, Mayo Clinic 3rd Annual West Cancer Center Oncology Conference Memphis, Tennessee Friday October 27, 2017
2 Evolution of Surgery for Breast Cancer Technical advances Growing data on oncologic safety of new approaches Integrated multidisciplinary care
3 Outline Breast Conservation Decreasing reoperation rates Frozen section Advances in XRT Hypofractionated, APBI Surgery + APBI in 9 days Improving Mastectomy Aesthetics - Nipple Sparing Mastectomy Technical advances Node positive disease; recurrent cancer Limiting Axillary Surgery Shift from ALND to SLN surgery Avoiding SLN Individualized Cancer Care/Personalized Medicine



4 "I wish you pathologists would find a way to tell us surgeons whether a growth is cancer or not while the patient is still on the table." Dr William Mayo Spencer Automatic Freezing Microtime #880 Louis B. Wilson Dr Wilson's publication in the December 2, 1905, issue of The Journal of the American Medical Association (1905;45:1737).
5 Frozen Section Pathology All margins evaluated intraoperatively Close and positive margins re-excised intraoperatively Final pathology report in hours Contributes to quicker recovery time, time to adjuvant recommendations Reoperation rate for margin control after lumpectomy for breast cancer is 3%




6
7 FS Impact on Patient Care 30-day reoperation rates following lumpectomy for cancer were lower at Mayo Clinic Rochester than in the national data 3.6% vs 13.2% (P<.001) 14% 12% Multivariable analysis 10% Patients in the national NSQIP data set were over four 8% times as likely to undergo reoperation as those at the FS institution. 6% Mayo NSQIP 4% 2% Adjusted Odds ratio = % Lumpectomy for Breast Cancer (p=<0.001) Mastectomy for Cancer (p=0.69) Boughey JC, Hieken TJ, Jakub JW, et al. Surgery. 2014;156(1):
8 FS Widespread Expansion Cost Analysis Baseline assumption 35% reoperation rate FS used in 20% cases Annual cost saving $18.2 million to payer $0.4 million providers FS used in 100% cases Annual cost saving $90.9 million to payer $1.8 million providers Boughey JC. J Oncol Pract. 2016;12(4):e413-e422.

9 Advances in XRT ASTRO 2011 guidelines endorse short course WBI for patients >50 years, T1-T2 ER+ tumors
10 Why Women Don t Choose BCS When given the option of BCS + WBI vs mastectomy, mastectomy chosen for (1) Convenience (2) Fear of radiation (3) Distance to RT facility A woman living 75 miles from RT facility would travel ~5000 miles to complete 33 fractions 85% of women who lived within 25 miles of a facility received RT following BCS vs 40% of women who lived over 100 miles away (4) Age (5) Cost (6) Side effects 15% to 45% of patients do not receive RT after BCS Smith GL. Cancer. 2010;116: McBride J. Women s Health. 2013;22: Pan IW. J Natl Cancer Inst. 2014;106:djt340.
11 Rationale for APBI Growing body of data supports favorable local control and cosmesis for selected patients Decrease time and inconvenience of BCT 5-6 weeks 4-5 days Improve utilization of BCT Potentially reduce acute and chronic toxicity WBI: Entire breast, overlying skin, lower axilla, heart, and lung, lower axilla APBI: Smaller volume & dose to normal tissue Improve patient quality of life
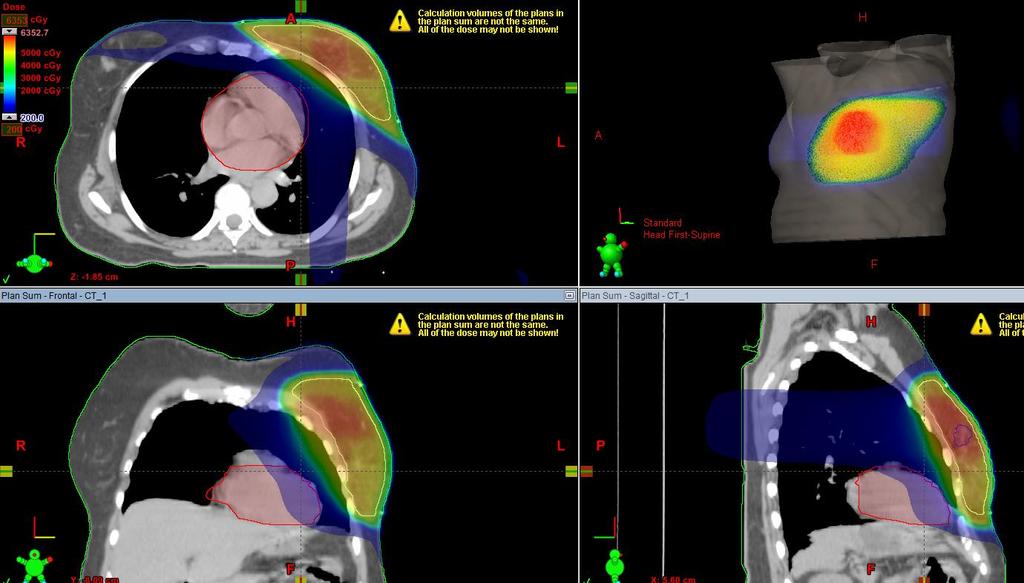
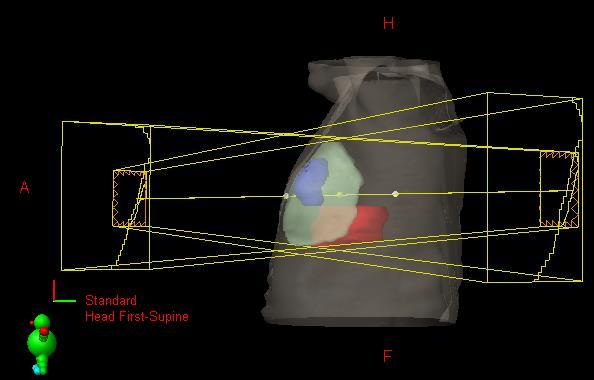
12 Whole-Breast RT Partial-Breast RT
13 APBI Early 1990s 2002 FDA 2010 RTOG 0319 Interstitial Catheter Brachytherapy Longest Experience Balloon/Strut Based Brachytherapy Single lumen multi-lumen strut-based 3D conformal external beam Most commonly employed modality in NSABP B-39

14 Comparison of Techniques SAVI MammoSite 3D EBRT Scanderberg D, et al. J Appl Clin Med Phys. 2010;11(1):


15 SAVI Multi-lumen strut-based device Better dosimetry Favorable toxicity profile Improved long-term cosmesis
16 Patient Selection Guidelines Criteria ABS ASBS ASTRO NSABP B39 Age (y) Histology IDC, DCIS IDC DCIS IDC IDC, DCIS T size (cm) N status (if +, 6 sampled) Margin Neg Neg 2 mm No tumor on ink Shah C, et al. Brachytherapy. 2013;12(4): Correa et al PRO
17 Mayo Clinic Selection Guidelines for APBI Inclusion 50 years 2 cm Margins: 0.2 cm ER (+) Infiltrating ductal, mucinous, tubular, colloidal Pure DCIS Negative axillary US Exclusion LVI Neoadjuvant therapy Prior ipsilateral RT Prior ipsilateral cancer Connective tissue disease Multicentric EIC, LCIS, ILC BRCA1/2
 WLE+SLN SAVI")


18 Work Flow OR (POD 0) WLE+SLN SAVI placement POD 1 Final Path confirmed Rad Onc CT simulation POD Gy BID


19 Work Flow POD 6 Explant SAVI Follow up 3 wk 3 mo 6 mo 12 mo 24 mo
20 Mayo Clinic Rochester Experience APBI with intraoperative SAVI catheter placement Surgery (Postop Day 0) Lumpectomy and SLN mapping Intraoperative pathology (~3% to 5% FN) Intraoperative brachytherapy applicator placement Radiation Oncology Postop Day 1: CT simulation Postop Day 2: Begin treatment Treatment completed within 9 days





21 Postop Day 0 BCS + SAVI Placement



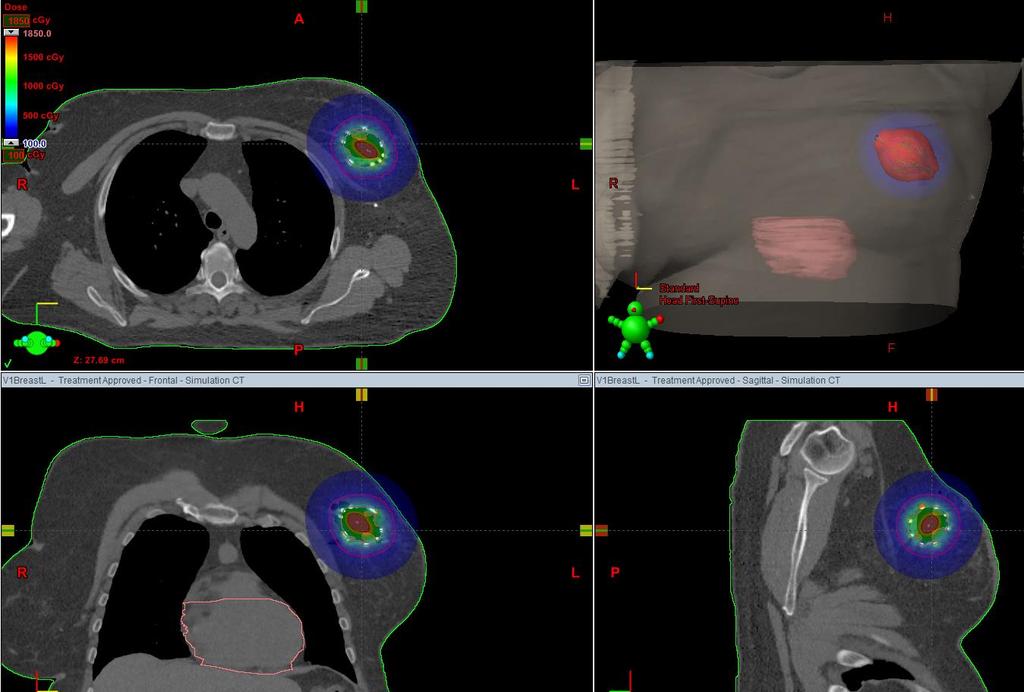
22 Radiation Oncology Workflow (Postop Day 2-5: Imaging Verification and Treatment)
 intraoperative catheter placement 13 excluded based on FS pathology 6 SLN+ 7 disease too extensive 1/110 delayed +SLN had")
23 Intraoperative Pathology: Frozen Section Delayed positive SLN Convert to WBI (ie, ACOSOG Z11) Utilize brachytherapy as boost Delayed positive margin Re-excise and replace catheter Convert to WBI and utilize catheter as boost 123 patients prospectively registered 110 (90%) intraoperative catheter placement 13 excluded based on FS pathology 6 SLN+ 7 disease too extensive 1/110 delayed +SLN had APBI as boost
24 Mayo Clinic APBI Outcomes 30-day complication rate 6% (7 patients) SSI (2 patients) Hematoma (2 patients) Partial wound separation (1 patient) Moist desquamation (1 patient) Atrial fibrillation (1 patient) Cumulative complication rate 17% (14 patients) of 81 patients with 1 year of follow-up Correlated with device size but no patient or tumor variables SSI (5 patients) Symptomatic seroma (5 patients) Fat necrosis on mammogram (2 patients) Fistula, resolved with conservative treatment (1 patient) Hieken TJ, et al. Ann Surg Oncol. 2016;23(10):
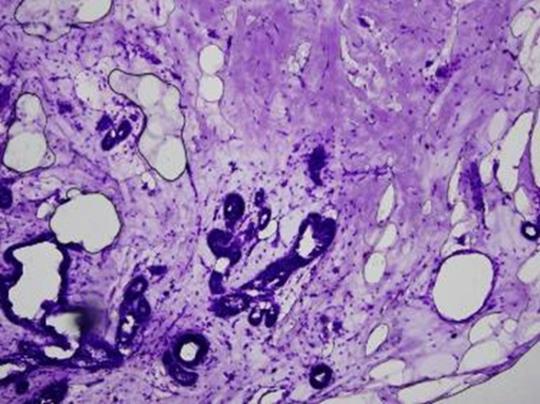
25 Recurrence Mayo Clinic APBI Outcomes Two patients (2%) developed an IBTR in the same quadrant of the breast as the index tumor; one invasive in scar at 8 months, one DCIS at margin of treated field at 26 monthhs Both had negative margins of 0.5 cm at initial operation and received APBI of 34 Gy in 10 fractions over 5 days Both patients recurrence treated with mastectomy Hieken TJ, et al. Ann Surg Oncol. 2016;23(10):
26 Mayo Clinic APBI - Cosmesis Hieken TJ, et al. Ann Surg Oncol. 2016;23(10):




27 Pre-surgery 9/26/ /1/2012 3/6/2013 9/9/2013 9/11/2016 One Year Post-Rx Four Years Post-Rx



28
29 Schedule BED: Early effects (α β = 10Gy) BED: Tumor control and late effects (α β = 3.5 Gy) 2.67 Gy x 15 (START B) Gy x 10 BID (RTOG 3DCRT) Gy x 10 BID (RTOG Brachy) Gy x 3 (Mayo Brachy)* Gy x 3 (Mayo 3DCRT)* Gy(RBE) x 3 (Mayo Proton)* Gy or 5.4Gy x 5 (Fast Forward) *Administered Daily
30 A Phase II Study O\of Accelerated 3 Fraction Photon and Proton Partial Breast External Beam Radiotherapy and Partial Breast Brachytherapy for Early Invasive and Noninvasive Breast Cancer 168 women Age 50, ER+, 2 cm, lumpectomy with negative margins Patient and physician elect APBI technique 1 0 objective: Evaluate cosmesis at 3 years SAVI brachytherapy 7 Gy x 3 daily Proton Therapy (IMPT) 7.3 Gy (RBE) x 3 External Beam 3DCRT 7.3 Gy x 3 Robert Mutter, MD, PI
31 Nipple Sparing Mastectomy




32 Why? Improved aesthetics of NSM have fueled patient demand PREOP POSTOP Bilateral NSM via IFM incisions
33 Potential Benefits of NSM Improved cosmesis with retention of the native nipple Eliminates the need for a second operation to reconstruct a nipple Facilitates one-stage reconstruction (direct to implant or flap)
34 Nipple Sparing Mastectomy Among patients undergoing mastectomy with immediate breast reconstruction, improved aesthetics have fueled increased patient demand for nipplesparing mastectomy (NSM) NCCN guidelines: The nipple should be removed for the majority of breast cancer patients However, NSM may be considered for patients with early stage, low grade, biologically favorable, node-negative and peripheral tumors at least 2 cm from the nipple


35 Current Practice 40% of mastectomies with IBR are NSMs
36 Complications Nipple Necrosis Requiring Nipple Excision Hieken (2015) Coopey (2013) Peled (2012) Spear (2011) Nipples Excised for Necrosis/NSMs (%) 5/566 (0.9%) 11/645 (1.7%) 10/657 (1.5%) 3/162 (1.9%)
37 Cancer Outcomes of NSM Year N* Median F/U (months) LR (%) NACR (%) Krajewski Eisenberg (mean) Sakurai Coopey Peled Spear (mean) 0 0 Kim Gerber (mean) Sakamoto Crowe Sacchini Studies with f/u 5 years LR rates 2% to 12%; NACR rates 1% to 4% *Number of breasts operated on for cancer
38 Shift in Philosophy Mastectomy with immediate breast reconstruction Can we spare the nipple-areolar complex? When do we need to remove it?

39 NSM for Cancer Contraindicated Inflammatory breast cancer Paget s disease Tumor in the nipple Physical examination Imaging Ca++s extending into the nipple Cancer presenting with nipple discharge
40 Variable NSM for LN+ Disease Jan 2009 to June scheduled NSMs cancers in 226 patients 58 LN+ cases compared to 182 LN- cases LN Positive N = 58 LN Negative N = 182 Total N = 240 P Value Age, median (IQR) 46 (41-52) 49 (45-56) 48.5 (43-54) 0.02 ER Positive ER Negative 50 (86%) 8 (14%) 155 (88%) 22 (12%) 205 (87%) 30 (13%) 0.79 HER-2 Positive HER-2 Negative 8 (14%) 48 (86%) 10 (9%) 99 (91%) 19 (11%) 147 (89%) 0.42 LVI present 21 (36%) 5 (4%) 26 (11%) Murphy B, Hieken TJ, et al. Am J Surg. 2017;213(4):
41 Results Nipple Excision for Atypia or Neoplasm Variable LN Positive N = 58 n (%) LN Negative N = 182 n (%) Total N = 240 n (%) P Value Intraoperative 5 (9%) 9 (5%) 14 (6%) 0.32 Postoperative 1 (2%) 4 (2%) 5 (2%) 0.82 Murphy B, Hieken TJ, et al. Am J Surg. 2017;213(4):
42 Results Success of NSM by Nodal Status 100% 90% % 70% Nipple removed for any reason 60% 50% 40% 30% 20% 10% 0% P = 0.73 LN + LN - Converted to SSM NSM Successful Murphy B, Hieken TJ, et al. Am J Surg. 2017;213(4):


43 Results Oncologic Outcomes 7 locoregional recurrences after 25 months median follow-up 5 in LN+ patients 3 skin/subcutaneous in flaps away from the nipple At 13, 30 and 46 months 2 ipsilateral supraclavicular and mediastinal LNs At 24 and 32 months 2 in LN- patients Nipple-areolar complex at 62 months Axillary nodes after negative SLN at 20 months Murphy B, Hieken TJ, et al. Am J Surg. 2017;213(4):
44 Results Oncologic Outcomes 3-year local regional disease-free survival for all invasive cancer patients LN-positive 87% (95% CI 75% to 100%) LN-negative 99% (95% CI 97% to 100%) P = year breast cancer-specific survival for all invasive cancer patients LN-positive 97% (95% CI 92% to 100%) LN-negative 99% (95% CI 98% to 100%) P = 0.40 Murphy B, Hieken TJ, et al. Am J Surg. 2017;213(4):
45 Summary Conversion from planned NSM to SSM did not differ significantly between node-positive and node-negative patients with cancer Nipple-areolar complex recurrences None in LN+ patients One in a LN- patient Short-term oncologic outcomes satisfactory NSM may be appropriate for carefully selected patients with LN+ breast cancer
46 Nipple-Sparing Mastectomy for the Management of Recurrent Breast Cancer ~246,000 patients will be diagnosed with breast cancer in the USA in % are treated with BCS 6% to 15% will have a local recurrence 21 patients at Mayo who underwent NSM for recurrent disease (1/2009-6/2016) Mean patient age Initial cancer diagnosis: 47.8 years Recurrence: 57.6 years Median time to recurrence: 102 months (range months) Siegel RL, et al. CA Cancer J Clin. 2016;66(1):7-30. Mahmood U, et al. Ann Surg Oncol. 2013;20(5): Kummerow KL, et al. JAMA Surg. 2015;150(1):9-16.
47 Percent Operations Performed for Recurrent Breast Cancer n = 89 n = 33 n = 21 NSM SSM Total Mastectomy Operation Murphy BL, Boughey JC, Hieken TJ. Clin Breast Cancer, 2017;17(4):e209-e213.
48 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Clinical Tumor Stage NSM SSM Total Mastectomy P = ct2 ct1 ct0/ctis Murphy BL, Boughey JC, Hieken TJ. Clin Breast Cancer, 2017;17(4):e209-e213.
49 100% Clinical Nodal Stage 95% P = % 85% cn3 cn2 cn1 cn0 80% 75% NSM SSM Total Mastectomy Murphy BL, Boughey JC, Hieken TJ. Clin Breast Cancer, 2017;17(4):e209-e213.
50 Outcomes Conversion to SSM: 2 (9.5%) 19 had prior whole breast radiation 1 recent smoker 4 patients underwent HBOT 1 pre-operative 2 pre and post-operative 1 post-operative >50% of cases used intraoperative SPY perfusion imaging Murphy BL, Boughey JC, Hieken TJ. Clin Breast Cancer, 2017;17(4):e209-e213.
51 Outcomes Complications Cellulitis: 2 (9.5%) Seroma: 2 (9.5%) Superficial skin necrosis: 1 (4.8%) Full thickness necrosis: 1 (4.8%) All 19 patients have retained their native nipple No recurrences Median follow-up 17.5 months Murphy BL, Boughey JC, Hieken TJ. Clin Breast Cancer, 2017;17(4):e209-e213.
52 NSM in Recurrent Breast Cancer NSM may be performed in highly selected patients with recurrent breast cancer Similar complication rates Satisfactory short-term oncologic outcomes



53 SPY Angiography Improves understanding flap perfusion Critical for high-risk patients
:274-281.")
54 SPY Angiography Mayo Protocol Harless CA, Jacobson SR. Breast J. 2016;22(3):


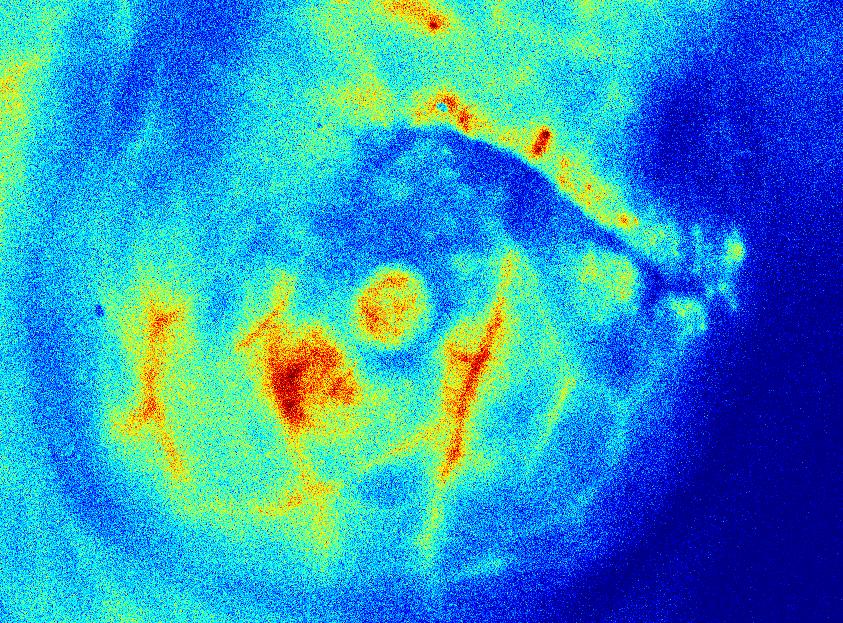

55 SPY Angiography Post mastectomy, no reconstruction Post mastectomy, 300 ml fill Post mastectomy, 200 ml fill


56 Number of Cases SPY Angiography * * * Before LA-ICGA After LA-ICGA Comparison of Complications Before and After LA-ICGA *Denotes statistical significance Harless CA, Jacobson SR. Breast J. 2016;22(3):
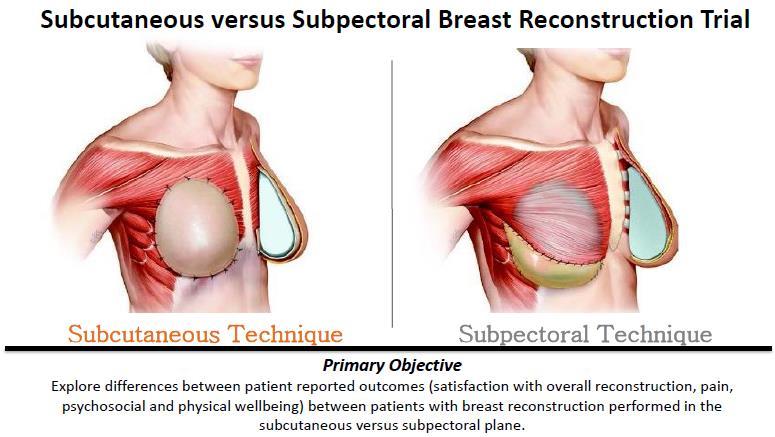
57 Subcutaneous (Pre-Pectoral) Breast Reconstruction breast in 79 patients Expanders/implants wrapped in Alloderm Placed in subq space Improved aesthetic outcomes Decreased OR time Decreased postoperative pain Woo A, et al. Breast J. 2017;23(5):
58
59
60 Methods National Cancer Database ( ) Mayo Rochester Database ( ) Inclusion Invasive breast cancer Women age 70+ HR positive cn0 disease Exclusion Neoadjuvant therapy Recurrent disease M1 disease Welsh JL, et al. Ann Surg Oncol Aug 1. [Epub ahead of print].
61 N = 125,554 N = 667 No axillary surgery 13.6% 8.8% Welsh JL, et al. Ann Surg Oncol Aug 1. [Epub ahead of print].
62 Rates of pn+ in Women 70+ Years With HR+ cn0 Invasive Disease Overall pn+ 18,586/125, % 95/ % Stratified by Clinical T stage T1mic 29/ % 0/9 0% T1a 358/7, % 0/39 0% T1b 1,657/24, % 21/ % T1c 5,045/35, % 42/ % T2 6,502/24, % 27/ % T3 749/1, % 3/8 37.5% T4 329/ % 2/ % Welsh JL, et al. Ann Surg Oncol Aug 1. [Epub ahead of print].
63 Rates of pn+ in Women 70+ Years With HR+ cn0 Invasive Disease Overall pn+ 18,586/125, % 95/ % Stratified by Clinical T stage T1mic 29/ % 0/9 0% T1a 358/7, % 0/39 0% T1b 1,657/24, % 21/ % T1c 5,045/35, % 42/ % T2 6,502/24, % 27/ % T3 749/1, % 3/8 37.5% T4 329/ % 2/ % Stratified by Grade I 3,766/39, % 31/ % II 9,807/60, % 57/ % III 4,148/18, % 7/ % Welsh JL, et al. Ann Surg Oncol Aug 1. [Epub ahead of print].

64 Influence of Combined T Stage and Grade on Nodal Positivity 30% HIGH 20% 10% 0% Grade 1 Grade 2 Grade 1 Grade 2 LOW




65 Nodal Positivity Rates in Low-Risk Group 7.3% 7.7% Low-risk criteria Grade 1 T1a-c Grade 2 T1a-b




66 Nodal Positivity Rates in High-Risk Group 21.8% 22.8% High-risk criteria Grade 3 tumors T2+ tumors Grade 2 T1c tumors


67 Clinical Implications 70+ HR+ Grade 1, T1a-c Grade 2, T1a-b Consider Omit SLN surgery All Grade 3 T2+ tumors Grade 2, T1c tumors Candidates for SLN surgery Consider comorbidities and impact of nodal staging on adjuvant treatment recommendations Welsh JL, et al. Ann Surg Oncol Aug 1. [Epub ahead of print].
68 Discussion Nodal status important for decision-making Radiation therapy Avoid radiation/ partial breast radiation Addition of nodal fields for N+ Endocrine therapy Relative benefit Extended therapy 5-10 years for N+ Patient adherence Model provides a tool for shared decision making when counseling on whether to omit SLN surgery Welsh JL, et al. Ann Surg Oncol Aug 1. [Epub ahead of print].


69 Evolution of Axillary Surgery Routine ALND SLN - cn0 SLN - BCT with 1-2 LN+ SLN - pnac cn+
70 Response to Neoadjuvant Chemotherapy Increasing pcr rates Anthracyclines 10% to 15% Anthracyclines + taxanes 25% to 30% Her2 positive disease: Trastuzumab + chemo 40% to 50% 2 anti-her2 agents + chemo 50% to 60% Nodal response rates (cn1 to ypn0) Anthracyclines 30% Anthracyclines + taxanes 40% HER2-positive disease up to 70% to 75%
 10/50 (20.0%) 27/251 (10.")
71 ACOSOG Z1071 FNR in cn1 Patients With at Least 2 SLNs Examined FNR = 12.6% Mapping Agent Blue dye only Radiolabeled colloid only Both blue dye and radiolabeled colloid Number of SLN Examined patients P Value 2/9 (22.2%) 10/50 (20.0%) 27/251 (10.8%) 19/90 (21.1%) 7/78 (9.0%) 4/60 (6.7%) 9/82 (11.0%) P = P = Boughey JC, et al. JAMA ;;310(14):
72 Impact of Inclusion of Metastases <0.2mm on SLN FNR and pcr rate SLNs from 17 patients revealed disease 0.2mm in size 1 (0.5%) had disease 0.2 mm identified on H&E 16 additional cases had disease 0.2 mm identified on IHC Node positive definition SLN metastases >0.2 mm by H&E SLN metastasis including 0.2 mm on IHC or H&E N Residual disease identified in SLNs or ALND FNR 95% CI (64.0%) 11.3% (66.2%) 8.7% The pathologic complete response rate in the nodes changed from 36.0% to 33.8% with the inclusion of metastasis 0.2 mm Boughey JC, et al. Cancer Res. 2015;75(9 Suppl): Abstract P
 patients with cn1 disease and 2+ SLNs removed had clip placed in LN at diagnosis N Nodal")

73 Clip 170 of 525 (32.4%) patients with cn1 disease and 2+ SLNs removed had clip placed in LN at diagnosis N Nodal residual disease FNR 95% CI Clip placed and found in SLN % 1.9% to 16.5% Clip placed and found in ALND % 5.4% to 41.9% Clip placed, location not known % 3.0% to 36.3% Clip not placed % 9.1% to 18.8% Boughey JC, et al. Ann Surg. 2016;263(4):
74
75 Resection of Clipped Node & SLN Targeted Axillary Dissection Remove SLNs and ensure removal of clipped node (node with biopsy proven disease at presentation) Localize clipped node prior to surgery MDACC experience: 85 patients underwent TAD and ALND 50 patients had residual nodal disease Evaluation of the clipped node in addition to the SLN(s) improved the FNR to 2.0% Caudle AS, et al. J Clin Oncol. 2016;34(10):



")
 FNA-")
 FNA+")
 All")
76 Pre-Treatment Nodal Staging 272 NAC Patients patients Axillary US Negative (61) Suspicious (211) FNA- (42) cn0 (103) FNA+ (169) cn+ (169) All available pre/post-nac imaging evaluated




77 % Patients LN+ at Operation Post-NAC by Post-NAC Imaging Results 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 80% 69% 43% P< % 100% 83% 69% 58% 39% P<0.001 P = 0.03 CR PR NR pnac US pnac MRI pnac PET- CT Hieken TJ, et al. Ann Surg Oncol. 2013;20(10):
:3199-3204.")
78 Patients Node-Positive at Presentation ypn-stage by CR on All Post-NAC Imaging 60% 50% 40% 30% 20% 10% 0% 58% 3% Hieken TJ, et al. Ann Surg Oncol. 2013;20(10): Imaging CR on all modalities performed 30% 14% 20% 14% 9% 3% 7% 2% 27% 14% Residual abnormality on any imaging ypn0 ypn0i+ ypn1mi ypn1 ypn2 ypn3 P = 0.006
 increased from 30% in 2009 to 74% in 2016 (P<0.")
 Nguyen TT, Hoskin T, Day C, Hieken TJ, Boughey JC. Ann Surg Oncol.")
79 Evolution of Axillary Surgery for cn1ln+ Patients After NAC, Mayo Clinic Use of SLN surgery (+/- ALND) increased from 30% in 2009 to 74% in 2016 (P<0.001) Omission of ALND increased from 3% in 2009 to 26% in 2016 (P<0.001) Nguyen TT, Hoskin T, Day C, Hieken TJ, Boughey JC. Ann Surg Oncol. 2017;24(S1):S64.
80 Evolution of Axillary Surgery for cn1+ Patients After NAC, Mayo Clinic Nguyen TT, Hoskin T, Day C, Hieken TJ, Boughey JC. Ann Surg Oncol. 2017;24(S1):S64.



81 Breast Cancer Treatment Is a Multidisciplinary Effort Patient Selection Pathology Systemic Therapies Radiation Surgery

82
83 Evolving Concepts in Breast Surgery in Multidisciplinary Care Tina J. Hieken MD, FACS Associate Professor of Surgery, Mayo Clinic 3rd Annual West Cancer Center Oncology Conference Memphis, Tennessee Friday October 27, 2017
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER
 ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
Consensus Guideline on Accelerated Partial Breast Irradiation
 Consensus Guideline on Accelerated Partial Breast Irradiation Purpose: To outline the use of accelerated partial breast irradiation (APBI) for the treatment of breast cancer. Associated ASBS Guidelines
Consensus Guideline on Accelerated Partial Breast Irradiation Purpose: To outline the use of accelerated partial breast irradiation (APBI) for the treatment of breast cancer. Associated ASBS Guidelines
RADIOTHERAPY IN BREAST CANCER :
 RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Current Status of Accelerated Partial Breast Irradiation. Julia White MD Professor, Radiation Oncology
 Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
Financial Disclosure. Learning Objectives. None. To understand the clinical applicability of the NCDB Breast Cancer PUF
 Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
Hypofractionated Radiotherapy for breast cancer: Updated evidence
 2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Targeting Surgery for Known Axillary Disease. Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center
 Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease?
 Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study
 [ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
[ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
Clinical Trials of Proton Therapy for Breast Cancer. Andrew L. Chang, MD 張維安 Study Chair
 Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Intraoperative. Radiotherapy
 Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
How can surgeons help the Radiation Oncologists?
 How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Advances in Breast Cancer
 Advances in Breast Cancer Developed in collaboration Learning Objectives Upon completion, participants should be able to: Apply genomic medicine to treatment decisions for patients with HR+/HER2- early
Advances in Breast Cancer Developed in collaboration Learning Objectives Upon completion, participants should be able to: Apply genomic medicine to treatment decisions for patients with HR+/HER2- early
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Surgical Issues in Neoadjuvant Chemotherapy
 14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
NIPPLE SPARING MASTECTOMY
 NIPPLE SPARING MASTECTOMY 29th Annual Montefiore-Einstein Controversies in Surgery Symposium Virgilio Sacchini, MD Memorial Sloan-Kettering Cancer Center Professor of Clinical Surgery Weill Cornell Medical
NIPPLE SPARING MASTECTOMY 29th Annual Montefiore-Einstein Controversies in Surgery Symposium Virgilio Sacchini, MD Memorial Sloan-Kettering Cancer Center Professor of Clinical Surgery Weill Cornell Medical
Accelerated Partial Breast Irradiation
 Accelerated Partial Breast Irradiation OSCO/OU Stephenson Cancer Center Saturday, March 5, 2016 Robert Kuske, MD, FAACE Founder, Medical Director Arizona Breast Cancer Specialists Scottsdale, Arizona 1
Accelerated Partial Breast Irradiation OSCO/OU Stephenson Cancer Center Saturday, March 5, 2016 Robert Kuske, MD, FAACE Founder, Medical Director Arizona Breast Cancer Specialists Scottsdale, Arizona 1
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Breast Conservation Therapy
 May 18, 2018 Breast Conservation Therapy One Treatment No Longer Fits All Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. Define stages of breast cancer that are candidates
May 18, 2018 Breast Conservation Therapy One Treatment No Longer Fits All Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. Define stages of breast cancer that are candidates
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice. Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin
 1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
ARROCase - April 2017
 ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective
 Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer
 Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer Cristina Lopez-Peñalver, MD, FACS October 11, 2014 Disclosures I have no relevant commercial relationships to disclose. Discuss
Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer Cristina Lopez-Peñalver, MD, FACS October 11, 2014 Disclosures I have no relevant commercial relationships to disclose. Discuss
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
Clinical outcomes of patients treated with accelerated partial breast irradiation with high-dose rate brachytherapy: Scripps Clinic experience
 Original Article Clinical outcomes of patients treated with accelerated partial breast irradiation with high-dose rate brachytherapy: Scripps Clinic experience Rachel Murray 1, Fantine Giap 2, Ray Lin
Original Article Clinical outcomes of patients treated with accelerated partial breast irradiation with high-dose rate brachytherapy: Scripps Clinic experience Rachel Murray 1, Fantine Giap 2, Ray Lin
Breast Surgery: Yesterday, Today and Tomorrow
 Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
New Technologies in Radiation Oncology. Catherine Park, MD, MPH Advocate Good Shepherd Hospital
 New Technologies in Radiation Oncology Catherine Park, MD, MPH Advocate Good Shepherd Hospital Breast Radiation Early Stage Breast Cancer Whole Breast Radiation Delivered to the whole breast Boost to the
New Technologies in Radiation Oncology Catherine Park, MD, MPH Advocate Good Shepherd Hospital Breast Radiation Early Stage Breast Cancer Whole Breast Radiation Delivered to the whole breast Boost to the
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer
 Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
IORT What We ve Learned So Far
 IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
Partial Breast Irradiation for Breast Conserving Therapy
 To Radiate or Not? Is APBI the Right Compromise Solution? Partial Breast Irradiation for Breast Conserving Therapy Julia White MD Professor, Radiation Oncology Agenda Role of radiotherapy in breast conservation
To Radiate or Not? Is APBI the Right Compromise Solution? Partial Breast Irradiation for Breast Conserving Therapy Julia White MD Professor, Radiation Oncology Agenda Role of radiotherapy in breast conservation
What is an Adequate Lumpectomy Margin in 2018?
 What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
Accelerated Partial Breast Irradiation (APBI)
") Accelerated Partial Breast Irradiation (APBI) Michael Zhang (MSIV), Matthew Spraker, MD, PhD (PGY3) Faculty Mentor: Janice Kim, MD University of Washington/Seattle Cancer Care Alliance Seattle, WA Case
Accelerated Partial Breast Irradiation (APBI) Michael Zhang (MSIV), Matthew Spraker, MD, PhD (PGY3) Faculty Mentor: Janice Kim, MD University of Washington/Seattle Cancer Care Alliance Seattle, WA Case
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY
 EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
Welcome to. American College of Surgeons. Clinical Research Program (ACS-CRP) Breast Surgical Trial Webinar
 Breast Surgical Trial Webinar") American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director Welcome to American College of Surgeons Clinical Research Program (ACS-CRP) Breast Surgical Trial Webinar Moderator:
American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director Welcome to American College of Surgeons Clinical Research Program (ACS-CRP) Breast Surgical Trial Webinar Moderator:
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Conservative Surgery and Radiation Stage I and II Breast Cancer
 Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
Slide 1. Slide 2. Slide 3 History of Nurse Navigator
 Slide 1 The Nurse Navigators role in Early Stage Breast Cancer, and Development of Tailored Treatment Plan Laura Ochoa, RN, ANP-BC, Ph.D. Slide 2 Barnes Jewish Hospital at Washington University Slide 3
Slide 1 The Nurse Navigators role in Early Stage Breast Cancer, and Development of Tailored Treatment Plan Laura Ochoa, RN, ANP-BC, Ph.D. Slide 2 Barnes Jewish Hospital at Washington University Slide 3
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer
 Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!?
 CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Recent Advances in Breast Cancer Treatment
 Recent Advances in Breast Cancer Treatment Pornchai O-charoenrat MD, PhD, FRCST, FICS Professor Chief, Division of Head-Neck & Breast Surgery Department of Surgery, Siriraj Hospital, THAILAND Recent Advances
Recent Advances in Breast Cancer Treatment Pornchai O-charoenrat MD, PhD, FRCST, FICS Professor Chief, Division of Head-Neck & Breast Surgery Department of Surgery, Siriraj Hospital, THAILAND Recent Advances
Case Conference: Post-Mastectomy Radiotherapy
 Case Conference: Post-Mastectomy Radiotherapy Outline - Case Intro Guidelines Studies - Case Conclusion Summary Outline Case Intro to PMRT Guidelines Studies Case conclusion Summary Outline - Case Intro
Case Conference: Post-Mastectomy Radiotherapy Outline - Case Intro Guidelines Studies - Case Conclusion Summary Outline Case Intro to PMRT Guidelines Studies Case conclusion Summary Outline - Case Intro
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS DISCLAIMER CODING INFORMATION REFERENCES POLICY HISTORY
 - Original Issue Date (Created): November 22, 2011 Most Recent Review Date (Revised): May 20, 2014 Effective Date: October 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS
- Original Issue Date (Created): November 22, 2011 Most Recent Review Date (Revised): May 20, 2014 Effective Date: October 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Breast Health. Program Objectives. Facts About Breast Cancer in the United States
 Breast Health Meridian Cancer Care Yolanda Tammaro, M.D. Meridian Medical Group- Specialty Care Breast Surgery, Ocean Medical Center Program Objectives Participants will: Learn some basic breast cancer
Breast Health Meridian Cancer Care Yolanda Tammaro, M.D. Meridian Medical Group- Specialty Care Breast Surgery, Ocean Medical Center Program Objectives Participants will: Learn some basic breast cancer
Brachytherapy: The precise answer for tackling breast cancer. Because life is for living
 Brachytherapy: The precise answer for tackling breast cancer Because life is for living Table of contents Executive summary 3 Introduction 4 Management of early stage breast cancer 5 Radiotherapy options
Brachytherapy: The precise answer for tackling breast cancer Because life is for living Table of contents Executive summary 3 Introduction 4 Management of early stage breast cancer 5 Radiotherapy options
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change
 Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Relevance. Axillary Node Recurrence. Purpose. Case Presentation: Is axillary staging required? Two trends have emerged:
 Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
Outcomes of patients with inflammatory breast cancer treated by breast-conserving surgery
 Breast Cancer Res Treat (2016) 160:387 391 DOI 10.1007/s10549-016-4017-3 EDITORIAL Outcomes of patients with inflammatory breast cancer treated by breast-conserving surgery Monika Brzezinska 1 Linda J.
Breast Cancer Res Treat (2016) 160:387 391 DOI 10.1007/s10549-016-4017-3 EDITORIAL Outcomes of patients with inflammatory breast cancer treated by breast-conserving surgery Monika Brzezinska 1 Linda J.
How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
 in Locally Advanced Breast Cancer") Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Accelerated Partial Breast Irradiation: Potential Roles Following Breast-Conserving Surgery
 APBI is a promising technique in selected patients with early-stage breast cancer, but further study is needed on outcome and toxicity associated with this approach. Nick Patten. Passing Light (detail).
APBI is a promising technique in selected patients with early-stage breast cancer, but further study is needed on outcome and toxicity associated with this approach. Nick Patten. Passing Light (detail).
Nipple Sparing Mastectomy: Tips & Tricks. Rebecca Nelson, MD MSc FRCSC Plastic & Reconstructive Surgeon, Burnaby Hospital
 Nipple Sparing Mastectomy: Tips & Tricks Rebecca Nelson, MD MSc FRCSC Plastic & Reconstructive Surgeon, Burnaby Hospital Nipple Sparing Mastectomy (NSM) Introduction & Technique Safety Evidence Indications/Contraindications
Nipple Sparing Mastectomy: Tips & Tricks Rebecca Nelson, MD MSc FRCSC Plastic & Reconstructive Surgeon, Burnaby Hospital Nipple Sparing Mastectomy (NSM) Introduction & Technique Safety Evidence Indications/Contraindications
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
PMRT for N1 breast cancer :CONS. Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center
 PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
doi: /j.ijrobp
 doi:10.1016/j.ijrobp.2009.12.047 Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 977 984, 2011 Copyright Ó 2011 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ see front matter
doi:10.1016/j.ijrobp.2009.12.047 Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 977 984, 2011 Copyright Ó 2011 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ see front matter
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
SABCS ANCO REVIEW. SABCS 2014 Surgery Review. ! Diagnostic workup! Lumpectomy " Local staging, technique, margins
 Frederick M. Dirbas Associate Professor of Surgery, Stanford Univ School of Medicine Physician Leader, Breast Cancer Clinical Care Prgm, Stanford Cancer Institute SABCS 2014 - ANCO REVIEW SABCS 2014 Surgery
Frederick M. Dirbas Associate Professor of Surgery, Stanford Univ School of Medicine Physician Leader, Breast Cancer Clinical Care Prgm, Stanford Cancer Institute SABCS 2014 - ANCO REVIEW SABCS 2014 Surgery
Radiotherapy Physics and Equipment
 Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Accelerated Breast Irradiation and Brachytherapy Boost Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Accelerated Breast Irradiation and Brachytherapy
Accelerated Breast Irradiation and Brachytherapy Boost Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Accelerated Breast Irradiation and Brachytherapy
Accelerated Partial Breast Irradiation: A Review and Description of an Early North American Surgical Experience With the Intrabeam Delivery System
 A variety of techniques for accelerated partial breast irradiation are available. Photo courtesy of Lisa Scholder. Hidden Power, 24ʺ 28ʺ. Accelerated Partial Breast Irradiation: A Review and Description
A variety of techniques for accelerated partial breast irradiation are available. Photo courtesy of Lisa Scholder. Hidden Power, 24ʺ 28ʺ. Accelerated Partial Breast Irradiation: A Review and Description
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC)
") Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Corporate Medical Policy
 Corporate Medical Policy Breast Brachytherapy for Accelerated Partial Breast Radiotherapy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: breast_brachytherapy_for_accelerated_partial_breast_radiotherapy
Corporate Medical Policy Breast Brachytherapy for Accelerated Partial Breast Radiotherapy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: breast_brachytherapy_for_accelerated_partial_breast_radiotherapy
Accelerated Partial Breast Irradiation. Dr Patricia Lillis MD, MHA,MSS Marshfield Clinic Radiation Oncology
 Accelerated Partial Breast Irradiation Dr Patricia Lillis MD, MHA,MSS Marshfield Clinic Radiation Oncology Outline 1. Rationale 2. Review of selected literature 3. Technical aspects 4. Selection criteria
Accelerated Partial Breast Irradiation Dr Patricia Lillis MD, MHA,MSS Marshfield Clinic Radiation Oncology Outline 1. Rationale 2. Review of selected literature 3. Technical aspects 4. Selection criteria
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Cancer: Management of the Axilla in Greg McKinnon MD FRCSC SON Vancouver Oct 2016
 Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Protocol of Radiotherapy for Breast Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
Surgical Management of the Axilla
 Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
Prophylactic Mastectomy & Reconstructive Implications
 Prophylactic Mastectomy & Reconstructive Implications Minas T Chrysopoulo, MD PRMA Center For Advanced Breast Reconstruction Prophylactic Mastectomy Surgical removal of one or both breasts to reduce the
Prophylactic Mastectomy & Reconstructive Implications Minas T Chrysopoulo, MD PRMA Center For Advanced Breast Reconstruction Prophylactic Mastectomy Surgical removal of one or both breasts to reduce the
How can we Personalize RT as part of Breast-Conserving Therapy?
 How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
What the surgeon wants from the radiologist before breast cancer surgery. Erica Patocskai Isabelle Trop
 What the surgeon wants from the radiologist before breast cancer surgery Erica Patocskai Isabelle Trop Centre Hospitalier de l université de Montréal CAR, April 2013 Plan What is the role of MRI for breast
What the surgeon wants from the radiologist before breast cancer surgery Erica Patocskai Isabelle Trop Centre Hospitalier de l université de Montréal CAR, April 2013 Plan What is the role of MRI for breast
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Cancer. Savita Dandapani
 New Modalities for Breast Cancer Savita Dandapani Disclosures Accuray Talk at ASTRO 10/2015. Xoft provided slides for the partial breast radiation equipment. Early Stage: Deep Inspiratory Breath Hold (DIBH)
New Modalities for Breast Cancer Savita Dandapani Disclosures Accuray Talk at ASTRO 10/2015. Xoft provided slides for the partial breast radiation equipment. Early Stage: Deep Inspiratory Breath Hold (DIBH)
Accelerated Radiation Treatment for Early Stage Breast Cancer. update and perspective
 Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2013 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2013 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
Incorporating Nipple-Sparing Mastectomy Into Your Practice. Michael Howard, MD, FACS Karol A Gutowski, MD, FACS
 Incorporating Nipple-Sparing Mastectomy Into Your Practice Michael Howard, MD, FACS Karol A Gutowski, MD, FACS 1 Disclosures Michael Howard, MD Scientific Advisor, EO2 Concepts Karol Gutowski, MD Speaker's
Incorporating Nipple-Sparing Mastectomy Into Your Practice Michael Howard, MD, FACS Karol A Gutowski, MD, FACS 1 Disclosures Michael Howard, MD Scientific Advisor, EO2 Concepts Karol Gutowski, MD Speaker's
Treatment Planning for Breast Cancer: Contouring Targets. Julia White MD Professor
 Treatment Planning for Breast Cancer: Contouring Targets Julia White MD Professor Outline 1. RTOG Breast Cancer Atlas 2. Target development on Clinical Trials Whole Breast Irradiation 2-D Radiotherapy
Treatment Planning for Breast Cancer: Contouring Targets Julia White MD Professor Outline 1. RTOG Breast Cancer Atlas 2. Target development on Clinical Trials Whole Breast Irradiation 2-D Radiotherapy
Breast Cancer: Current Approaches to Diagnosis and Treatment
 Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018