Supra-Regional Audit Anticoagulation in Palliative Care. 4 th March Denise Farrance
|
|
|
- Lydia Harrison
- 5 years ago
- Views:
Transcription
1 Supra-Regional Audit Anticoagulation in Palliative Care 4 th March 2010 Dr Helen Emms Dr Carolyn Watt Denise Farrance Dr Richard Latten Dr Leslie Johnny
2 Overview Review of current standard & guidelines Helen Emms Summary of coagulation & anti-coagulants Carolyn Watt Literature review Leslie Johnny Audit Data Richard Latten Proposed updates to standards & guidelines Helen Emms
3 Review of current standards & guidelines Dr Helen Emms Consultant in Palliative Medicine St John s Hospice Wirral
4 Guidelines General management of suspected Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE) Decisions surrounding the use of anticoagulation in patients with advanced cancer should be discussed with a senior physician. Figure 3.1 illustrates some general guidelines regarding the investigation and management of thromboembolic disease. [Level 4]
5
6 Aims and duration of anticoagulation Table 3.1 illustrates: The suggested duration of treatment for patients on warfarin and LMWH, and The target INR for patients on warfarin. [Level 4] Oral anticoagulation may be stopped abruptly when the duration of therapy is completed. [Level 2] Advice on the management of bleeding and /or high INR is given in Table 3.2. [Level 3]

7

8
9 Low Molecular Weight Heparin (LMWH) In some patients LMWH may be a better choice for patients than warfarin. Possible clinical indications for use of LMWH include: Treatment of thromboembolic disease e.g. DVT / PE whilst warfarin therapy is being initiated. Heparin treatment is usually temporary and is stopped when adequate anticoagulation with warfarin is achieved i.e. INR >2. [Level 4] Long term treatment of thromboembolic disease where warfarin therapy is not appropriate e.g. liver disease, unstable INR, difficult venepuncture (see Figure 3.1). [Level 4] Extension of the thrombus despite the use of warfarin. [Level 1+]
10 Low Molecular Weight Heparin (LMWH) - continued Prophylaxis of DVT in appropriate patients e.g. first five months of treatment with thalidomide in patients with additional thrombotic risk factors; 15 in patients taking diethylstilboestrol there is a significant increase in the risk of deep vein thrombosis and decisions should be made on an individual patient basis. Daily injections are more acceptable to patients than anti-embolic stockings. [Level 2++] There are a number of Low Molecular Weight Heparins available. They include Dalteparin, Enoxaparin and Tinzaparin. Choice will vary according to local policies. They are all given using a once-daily administration schedule via the subcutaneous route. There may be clinical situations where a split twice-daily dose schedule gives better symptom control. [Level 4]
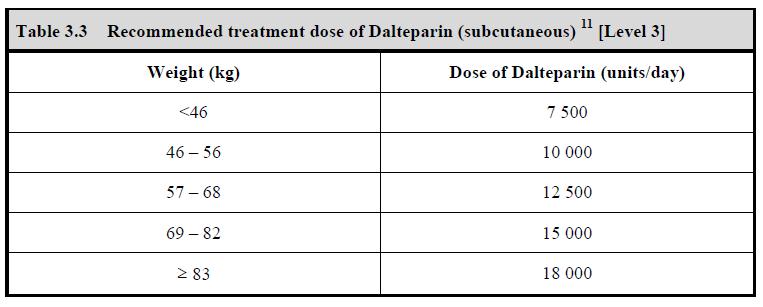
11 Low Molecular Weight Heparin (LMWH) - continued Renal function should be checked prior to, and during treatment with LMWH. Renal impairment may require dose adjustment. [Level 4] All LMWH treatment doses are calculated according to the weight of the patient. Table 3.3 gives the dosing schedule for dalteparin. Other drug doses are available in the BNF. [Level 3] The recommended prophylactic dose of dalteparin is 5000 units daily via the subcutaneous route. [Level 3] Contraindications to treatment with LMWH are listed in Table 3.4. [Level 3]
12 Table 3.3

13 Table 3.4
14 Low Molecular Weight Heparin (LMWH) - continued The risk of heparin-induced thrombocytopenia is low with LMWH but may occur after 5-10 days. Platelet counts should be measured just before commencing treatment with heparin. Regular monitoring of the platelet count is recommended if it is given for longer than 4 days. If there is a 50% reduction of the platelet count, heparin should be stopped. [Level 4] Inhibition of aldosterone secretion by heparin can result in hyperkalaemia. Patients with diabetes mellitus, chronic renal failure, acidosis, raised plasma potassium or those taking potassium-sparing drugs seem to be more susceptible. The risk appears to increase with the duration of therapy. Plasma potassium concentration should be measured in patients at risk of hyperkalaemia before starting LMWH. It should then be monitored at regular intervals, especially if the heparin is to be continued for longer than 7 days. [Level 3]
15 Low Molecular Weight Heparin (LMWH) - continued For patients requiring long-term therapy with LMWH, monitoring anti-factor Xa activity levels may be advisable and it is best to seek advice from the local haematologist. This especially applies especially to patients who are under or over-weight, those with renal impairment and those at risk of bleeding. [Level 4] Treatment should be kept under regular review as continuation of LMWH may not be appropriate in certain circumstances e.g. if the patient is in the dying phase. [Level 4]
16 Standards 1. The following information should be documented in the case notes: [Grade D] All patients on anticoagulation - Indication for anticoagulation Patients commencing warfarin - Target INR Patients commencing on LMWH - Weight (kg) - Intended duration of treatment - Daily warfarin dose and INR when checked (inpatients) - Renal function - Platelet count
17 2. The full blood count, urea and electrolytes should be checked as follows: [Grade C] - Prior to commencing treatment with LMWH. - Seven days after starting treatment with LMWH. - Every 4 weeks during treatment with LMWH (if appropriate) 3. All patients receiving anticoagulation should be issued with the standard anticoagulation booklet. [Grade D] 4. For patients on warfarin, clinician responsibility for both INR monitoring and patient follow-up should be clearly documented in the case notes and the patient-held anticoagulation booklet. [Grade D]
18 Summary of coagulation & anticoagulants Dr C.S.Watt Consultant in Palliative Medicine St John s Hospice, Lancaster
19 Coagulation - how it happens Anti-coagulant Drugs - how they affect the process Anti-Coagulant Drugs of coagulation - how they affect the process of coagulation
20 Injury to blood vessel Coagulation a) vascular constriction b) exposed collagen + von Willebrands factor affect platelets Aggregation adherence to surface LOOSE PLATELET PLUG c) COAGULATION CASCADE
21 Coagulation Cascade Intrinsic Pathway Surface Collagen XII XIIa Prekallekrein HMW Kininogen Extrinsic Pathway Tissue Factor XI Ca HMWK XIa Ca VII VIIa Ca Phospholipids IX IXa Ca VIII VIIIa PL V Va X Prothrombin II Ca PL Xa Thrombin IIa Fibrinogen I Fibrin Ia Forms Mesh CLOT XIIa
22 Coagulation Coagulation Cascade Intrinsic and Extrinsic Pathway Common Pathway to produce Prothombinase Prothombinase converts Prothombin Thrombin Thrombin converts Fibrinogen Fibrin Fibrin forms x-linked mesh to stabilise platelet plug and form CLOT
23 Anticoagulant Action XII XIIa VIIa and Tissue Factor XI Xla Antithrombin Protein C Protein S Thrombomodulin ---- = Inhibitory Effect IX IXa X Xa VIII VIIIa Prothrombin Thrombin V Va Fibrinogen Fibrin
24 Anticoagulants Coumarin Anticoagulant Warfarin Mode of Action:» Antagonising the effect of vitamin K» Vitamin K is required in the synthesis of coagulation factors, II, VII, IX, X and many cofactors including protein C, protein S and thrombomodulin» (vitamin K dependent carboxylation)
25 Anticoagulants Unfractionated Heparin Mode of Action:» Binds to anti-thrombin» inhibitory effect on factors IIa, IXa, Xa, XIa, XIIa» Tissue Factor Pathway Inhibitor» Inhibits thrombin induced activation of platelets and factors V, VIII» Affects platelet aggregation Low Molecular Weight Heparin -Enoxaparin, Tinzaparin, Dalteparin Mode of Action:» Inactivates factor Xa» Tissue Factor Pathway Inhibitor
26 Anticoagulants Fondaparinux Sodium Mode of Action:» Inhibits Factor Xa
27 New oral anticoagulants Rivaroxaban - Factor Xa inhibitor Dabigatran - Direct thrombin inhibitor Marketing authorisation for the prevention of venous thromboembolism (VTE) in adult patients undergoing elective hip or knee replacement surgery Fixed daily oral dosing without monitoring Recent DTB review of dabigatran (Pradaxa ) and rivaroxaban (Xarelto ) concluded: until more robust clinical efficacy and safety data are available for both drugs, it is advisable to use a more established alternative where possible.
28 New oral anticoagulants Apixaban (seeking European regulatory approval 2010) Oral Factor Xa inhibitor to prevent and treat venous thromboembolism in patients who have had orthopaedic surgery
29 References Oxford Handbook of Clinical Medicine 5 th Edition Longmore et al O.U.P. ISBN : Pg 650 Principles of Anatomy and Physiology 2003 Tortora and Grabowski. John Wiley and Sons Inc. USA ISBN : Oxford Textbook of Medicine IV Edition 2003 Warrell et al O.U.P. ISBN : Vol 3 Pg British National Formulary vol58. ISBN; Pg Hirsh J. et al. Heparin and Low-Molecular-Weight Heparin Mechanisms of action, pharmacokinetics, dosing, monitoring, efficacy and safety. Chest 119:64S-94S,2001 (suppl 1)
30 Literature Review Dr Leslie Johnny Speciality Registrar in Palliative Medicine St John s Hospice, Wirral
31 General Principles Thromboembolic events are among the leading causes of death in cancer patients Frequently asymptomatic Up to 15% of patients with cancer are thought to develop symptomatic VTE
32 General Principles VTE common among malignant brain tumours, adenocarcinoma of ovary, pancreas, colon, stomach, lung, prostate and kidney. Direct alterations to the coagulation pathway can cause a hypercoagulable state. Specific risk estimates of VTE by cancer type, stage and treatment are largely unknown (Geerts et al) Further increases in risk can be caused by a whole range of factors many of which are common in palliative care patients.
33 General Principles patients currently prescribed oral anticoagulant drugs. Warfarin is the most frequently prescribed Most commonly associated with medication errors in primary and secondary care. Most common drugs involved in errors resulting in claims against NHS Trusts. NPSA recommendations in March 2007
34 Studies showing cancer link to PE The Olmsted County analysis by Silverstein et al The Multiple Environmental and Genetic Assessment of risk factors for venous thrombosis (MEGA) study Sallah et al Ambrus et al
35 Choice of anticoagulation Recurrent VTE occurs in 27% of patients despite a therapeutic INR Current recommendations support use of Low Molecular Weight Heparin as first line for initial and long term management of cancer associated thrombosis Lee -Treatment of Venous Thromboembolism in cancer patients -2009
36 Warfarin Vs Heparin CLOT study LMWH vs. Oral Anticoagulant Therapy by Lee et al Primary Outcome- Recurrent VTE Secondary Outcome Clinical Bleeding, Death
37 Warfarin is generally inferior to therapeutic LMWH for treatment of VTE in patients with cancer (grade A, level Ib) BJH Meyer et al showed that an initial treatment with full-dose enoxaparin, followed by a half dose, significantly reduces the haemorrhagic risk compared with oral anticoagulants without influencing the risk of recurrence.
38 LMWH vs Unfractionated Heparin (UFH) LMWH is likely to be superior to UFH in the initial treatment of VTE in patients with cancer. Need for more trials to better address this research question in cancer patients. Cochrane Review in 2007 (LMWH)
39 Survival Benefit Existing evidence does not suggest a mortality benefit from oral anticoagulation in patients with cancer. Survival benefit of heparin in cancer patients (Hypothesis Direct effect on tumour and excess thrombin production) Patients with small cell lung cancer Heparin might be particularly beneficial in cancer patients with limited cancer or a longer life expectancy.
40 Venous Thromboembolism Prophylaxis
41 Surgical Prophylaxis evidence Bergqvist et al. & Rasmussen et al. Dalteparin good VTE prophylactic effect No increased risk bleeding for cancer patients Two agents have shown efficacy and safety for VTE prophylaxis in cancer patients under a certain set of clinical conditions: dalteparin and enoxaparin for abdominal or pelvic surgery for malignancy
42 Prophylaxis in Medical patients Three major studies: PREVENT- Dalteparin (14% had cancer) ARTEMIS-Fondaparinux (5% had cancer) MEDENOX- Enoxoparin (5% had cancer)
43 Mismetti and colleagues Meta-analysis (2000) Seven trials comparing a prophylactic heparin treatment to a control in medical patients. Four studies evaluated UFH Three studies evaluated a LMWH A significant decrease in DVT and in clinical PE were observed with heparins as compared to control (risk reductions of 56% and 58% respectively, p in both cases), without significant difference in the incidence of major bleeding or deaths
44 There is no data available on the numbers of cancer patients needed to treat to prevent one VTE. The appropriateness of generalising these studies to palliative care patients is uncertain. There are no studies to date examining the efficacy of using thrombo prophylaxis within this group.
45 Comparisons among anticoagulant agents ENOXACAN study Enoxaparin is as safe and effective as UFH in preventing VTE in major elective surgery for abdominal or pelvic malignancy. McLeod Both heparin and enoxaparin provide highly safe and effective prophylaxis in colorectal cancer surgery patients. Among LMWH products, the current literature does not indicate that any single LMWH has been shown as superior to any other
46 ACCP guidelines from 2005 The guidelines have provided 1A evidence-based recommendations therapy for LMWH or UFH in only high-risk patients, with cancer patients undergoing surgery considered to be most significant. Hospitalized cancer patients have also been considered to be at high risk of DVT,and 1A recommendations include prophylaxis with LMWH (dalteparin or enoxaparin) or low-dose UFH 3 times daily
47 ACCP guidelines from 2005 In the event that there is a contraindication to pharmacological thromboprophylaxis, consider non-pharmacological treatments. Non-pharmacological strategies include graduated compression stockings, intermittent pneumatic compression, leg elevation and early mobilization.
48 Mechanical prophylaxis No randomized clinical trials have evaluated mechanical methods of prophylaxis in general medical patients. These measures should be considered as alternative methods when contraindications to anticoagulants exist (Geerts et al 2004)
49 Nice Guidance on Mechanical Prophylaxis Mechanical methods have been proven to be effective in surgical patients and do not to add the risk of bleeding. Large study in stroke patients did not show any beneficial effect of stockings in stroke patients but did show an increase in skin complications associated with their use
50 Gap between theory and practise Heterogeneity of clinical studies, selected populations, concern about bleeding, and the lack of a clear clinical benefit are some of the reasons Only few trials were conducted using symptomatic VTE and/or mortality as the primary end point. Asymptomatic DVT, however, were the great majority of events detected during the studies
51 Patients Attitudes (Qualitative study) Low molecular weight heparin is acceptable to inpatients with advanced cancer receiving palliative care and has a positive impact on overall quality of life. Antiembolic stockings are an unacceptable intervention in this patient group. Guidelines on thromboprophylaxis are urgently needed for palliative care inpatient units and hospices. S I R Noble, senior lecturer in palliative medicine,1 A Nelson, palliative care research coordinator,2 C Turner, specialist registrar,3 and I G Finlay, professor of palliative medicine4
52 NICE guidance 2010 Decisions should be made on an individual basis with consideration of risk and burden of treatment. On initiation of therapy, a clinical plan should be made to review the appropriateness of treatment if there is felt to be a sufficient potential benefit from treatment. The treatment choice is LMWH in a once daily dose. There is a lack of evidence to support long term primary prophylaxis in patients with cancer.
53 Using antiplatelet therapy as a convenient prophylactic two for one. Not recommended because the protective effective of aspirin against VTE is insufficient Consider offering temporary inferior vena caval filters to patients who are at very high risk of VTE (such as patients with a previous VTE event or an active malignancy) and for whom mechanical and pharmacological VTE prophylaxis are contraindicated.
54
55
56 Calvary, Bethlehem Guidance Thrombopropylaxis should be considered in previously ambulatory patients, admitted to the inpatient facility with acute change in their condition and mobility. This may include infection, hypercalcemia, recent spinal cord compression, post operative or recent functional decline with restorative care as the goal. Need to take account of the patient s prognosis and the potential effect on quality of life to avoid inappropriate treatment.
57 Pan Birmingham Cancer Network As a part of the holistic assessment all patients should have their risk of VTE assessed to decide whether they may benefit from anticoagulation with LMWH, to reduce the risk of symptomatic and life limiting VTE. These guidelines are aimed at palliative patients admitted to a hospice or hospital
58 Consideration of primary prophylaxis in palliative care patients for VTE should keep at its centre the focus of high quality symptom control At present there are insufficient studies to support treating all cancer inpatients with primary prophylaxis for VTE

59

60

61

62
63 Audit Results Dr Richard Latten Specialist Registrar in Palliative Medicine Royal Liverpool University Hospital & Marie Curie Hospice Liverpool
64 Audit Method Prospective case-note audit 1 month data collection period (Jan/Feb 2010) Audit forms distributed to ICN leads Cascaded down to individual units
65 Settings represented Hospital Hospice Community Not Documented
66 Speciality completing forms Medical Nursing Other Not Documented
67 Data sets by location
68 Age Range >81



69 Gender Balance Not Documented 7% Male 38% Female 55%
70 Primary Diagnosis
71 Metastases Bone Liver Lung Peritoneal Other
72 When was anticoagulation started? During this admission Already taking Not Doc.
73 Specialty Commencing Pall Care Surical Medical Oncology Don't Know Not Doc.
74 Is indication documented? Yes No No data
75 Indications documented
76 Is intended duration documented? Yes No No data
77 Type of anticoagulation Warfarin LMWH No data

78 Heparin results
79 Type of LMWH Enoxaparin (Clexane) Dalteparin (Fragmin) Tinzaparin (Innohep)
80 FBC monitoring Yes No n/a No Data 0 Pre-Treatment After 1 week Every 4 weeks
81 Renal Function pre-heparin Yes No n/a No Data
82 Weight documentation Yes No n/a No Data 0 Pre-treatment Subsequent Assessment

83 Warfarin Results
84 Target INR documentation Yes No No Data
85 Recent INR documentation Yes No No Data
86 Current warfarin dose documentation Yes No No Data
87 Standard anticoagulation booklet Yes No No Data
88 Responsible clinician documented Yes No No Data
89 Venous Thromboembolism prophylaxis
90 Unit VTE prophylaxis policy? Yes No Don't know No Data
91 Proposed updates to standards & guidelines Dr Helen Emms Consultant in Palliative Medicine St John s Hospice Wirral
92 Overview of proposed changes General Principles Some information previously in guidelines moved to general principles section Guidelines Split into 2 sections 1. Venous Thrombo-Embolism Prophylaxis 2. Therapeutic anticoagulation Standards 2 potential new standards
93 Explanation of colours Red = proposed new or changed text Green = no change in wording but altered position Strikethrough = proposed text moved or removed
94 Moved to General Principles It is important for the clinician to decide whether anticoagulation is appropriate on an individual patient basis. Decisions surrounding the use of anticoagulation in patients with advanced cancer should be discussed with a senior physician. Prophylactic and therapeutic anticoagulation should be kept under regular review as continuation may not be appropriate in certain circumstances e.g. if the patient is in the dying phase.
95 Moved to General Principles Poor INR control may subject the patient to an increased risk of bleeding without adequately treating the venous thrombosis. Low Molecular Weight Heparin (LMWH) is an alternative to warfarin in palliative care patients and can be used for prophylaxis of venous thromboembolism (VTE) in high-risk patients.
96 Moved to General Principles There are a number of Low Molecular Weight Heparins available. They include Dalteparin, Enoxaparin and Tinzaparin. Choice will vary according to local policies/formulary. They are all given using a once-daily administration schedule via the subcutaneous route. There may be clinical situations (e.g. Acute Coronary Syndromes) where a split twice-daily dose schedule gives better symptom control. The risk of heparin-induced thrombocytopenia is low with LMWH but may occur after 5-10 days. Platelet counts should be measured just before commencing treatment with heparin. Regular monitoring of the platelet count is recommended if it is given for longer than 4 days. If there is a 50% reduction of the platelet count, heparin should be stopped.
97 Moved to General Principles Renal function should be checked prior to, and during treatment with LMWH. Renal impairment may require dose adjustment. Inhibition of aldosterone secretion by heparin can result in hyperkalaemia. Patients with diabetes mellitus, chronic renal failure, acidosis, raised plasma potassium or those taking potassium-sparing drugs seem to be more susceptible. The risk appears to increase with the duration of therapy. Plasma potassium concentration should be measured in patients at risk of hyperkalaemia before starting LMWH. It should then be monitored at regular intervals, especially if the heparin is to be continued for longer than 7 days.
98 Moved to General Principles Contraindications to treatment with LMWH are listed in Table 3.4. Table 3.4 Contraindications when considering the use of treatment with LMWH Acute bacterial endocarditis Haemophilia and other haemorrhagic disorders History of heparin-induced thrombocytopenia Known hypersensitivity to heparin or LMWH After major trauma Peptic ulcer Recent cerebral haemorrhage Recent injury or surgery to central nervous system / eyes/ ears Severe hypertension Severe liver disease (including oesophageal varices) Spinal or epidural anaesthesia Thrombocytopenia
99 Guidelines Venous Thrombo-Embolism (VTE) prophylaxis The appropriateness of VTE prophylaxis for palliative care patients should be made on an individual patient basis, including consideration of the stage of the patient s illness. [Level 4] Palliative care patients in the dying phase of their illness (e.g. supported by an end-of-life care pathway) should not be routinely given pharmacological or mechanical VTE prophylaxis. [Level 4]
100 Qualitative research has shown the acceptability of VTE prophylaxis with LMWH to patients and a desire to be involved in the decision making process. The views of the patient, their families, carers and the multi-disciplinary team looking after the patient should be taken into account when making decisions regarding the provision of VTE prophylaxis. [Level 4] The potential benefit of reducing VTE events should be balanced with the potential harms of bleeding and the qualitative aspects of receiving VTE prophylaxis. Assess all patients for risk of bleeding before offering pharmacological VTE prophylaxis. [Level 4]
101 For patients in whom pharmacological prophylaxis is contraindicated, consider whether mechanical VTE prophylaxis is appropriate. Potential options include: antiembolism stockings, foot impulse devices and intermittent pneumatic compression devices. [Level 4] The National Institute for Heath and Clinical Excellence (NICE) gives guidance regarding the assessment and provision of VTE prophylaxis for patients admitted to hospital. ( Aspects are summarised in figures 1-4 below: All decisions regarding the provision of VTE prophylaxis should be reviewed at regular intervals. [Level 4]
102

103
104
105
106 Guidelines General management of suspected Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE) Figure 3.1 illustrates some general guidelines regarding the investigation and management of thrombo-embolic disease. [Level 4]
107
108 Aims, duration and choice of therapeutic anticoagulation In some patients LMWH may be a better choice for patients than warfarin. Possible clinical indications for use of LMWH include: Treatment of thromboembolic disease e.g. DVT / PE whilst warfarin therapy is being initiated. Heparin treatment is usually temporary and is stopped when adequate anticoagulation with warfarin is achieved i.e. INR >2. 13 [Level 4] Long term treatment of thromboembolic disease where warfarin therapy is not appropriate e.g. liver disease, unstable INR, difficult venepuncture (see Figure 3.1). 5 [Level 4] Extension of the thrombus despite the use of warfarin. [Level 1+]
109 All LMWH treatment doses are calculated according to the weight of the patient. Drug doses are available in the BNF. [Level 3] For patients requiring long-term therapy with LMWH, monitoring anti-factor Xa activity levels may be advisable and it is best to seek advice from the local haematologist. This especially applies especially to patients who are under or over-weight, those with renal impairment and those at risk of bleeding. [Level 4]
110 Table 3.1 illustrates: The suggested duration of treatment for patients on warfarin and LMWH, and The target INR for patients on warfarin. [Level 4] Anticoagulation may be stopped abruptly when the duration of therapy is completed. [Level 2]

111
112 Advice on the management of bleeding and /or high INR Guidelines are given in Table 3.2. [Level 3] If the INR is outside the target range, check for bleeding, haematuria or significant bruising. [Level 3]

113
114 Standards 1. The following information should be documented in the case notes: [Grade D] All patients on anticoagulation - Indication for anticoagulation Patients commencing warfarin - Target INR Patients commencing on LMWH - Weight (kg) - Intended duration of treatment - Daily warfarin dose and INR when checked (inpatients) - Renal function - Platelet count
115 2. The full blood count, urea and electrolytes should be checked as follows: [Grade C] - Prior to commencing treatment with LMWH. - Seven days after starting treatment with LMWH. - Every 4 weeks during treatment with LMWH (if appropriate) 3. If there is a 50% reduction of the platelet count, heparin should be stopped. [Grade D] 4. All patients receiving anticoagulation should be issued with the standard anticoagulation booklet. [Grade D] 5. For patients on warfarin, clinician responsibility for both INR monitoring and patient follow-up should be clearly documented in the case notes and the patient-held anticoagulation booklet. [Grade D]
116 6. The need for VTE prophylaxis should be considered in all patients and the decision, with reasoning, documented in the case notes. [Grade D]
Supra-Regional Audit Anticoagulation in Palliative Care. 4 th March Denise Farrance
 Supra-Regional Audit Anticoagulation in Palliative Care 4 th March 2010 Dr Helen Emms Dr Carolyn Watt Denise Farrance Dr Richard Latten Dr Leslie Johnny Overview Review of current standard & guidelines
Supra-Regional Audit Anticoagulation in Palliative Care 4 th March 2010 Dr Helen Emms Dr Carolyn Watt Denise Farrance Dr Richard Latten Dr Leslie Johnny Overview Review of current standard & guidelines
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales
 John Fletcher Wound Care Association of New South Wales") Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Anticoagulation for prevention of venous thromboembolism
 Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Venous Thrombo-Embolism. John de Vos Consultant Haematologist RSCH
 Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Chapter 1 Introduction
 Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins
 Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
THROMBOTIC DISORDERS: The Final Frontier
 THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Venothromboembolism prophylaxis: Trauma and Orthopaedics Clinical guideline, V2
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
NICE Guidance: Venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital 1
 in patients admitted to hospital 1") The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
Venous thromboembolism - reducing the risk
 Venous thromboembolism - reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital NICE guideline Draft for consultation,
Venous thromboembolism - reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital NICE guideline Draft for consultation,
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Title Use and monitoring of Low Molecular Weight Heparins (LMWHs) in community hospitals and community nursing Clinical Guidelines
 in community hospitals and community nursing Clinical Guidelines") Document Control Title Use and monitoring of Low Molecular Weight Heparins (LMWHs) in community hospitals and community nursing Clinical Guidelines Author Team Directorate Medical Date Version Status Issued
Document Control Title Use and monitoring of Low Molecular Weight Heparins (LMWHs) in community hospitals and community nursing Clinical Guidelines Author Team Directorate Medical Date Version Status Issued
Primary Exam Physiology lecture 5. Haemostasis
 Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
Venous thromboembolism: reducing the risk
 Issue date: January 2010 Venous thromboembolism: reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital This guideline
Issue date: January 2010 Venous thromboembolism: reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital This guideline
New v1.0 Date: December 2015 Patricia Wain - Associate Director Physical Care. Kenny Laing - Deputy Director of Nursing
 Clinical Venous Thromboembolism: Standing Operating Procedure Document Control Summary Status: Version: Author/Title: Owner/Title: New v1.0 Date: December 2015 Patricia Wain - Associate Director Physical
Clinical Venous Thromboembolism: Standing Operating Procedure Document Control Summary Status: Version: Author/Title: Owner/Title: New v1.0 Date: December 2015 Patricia Wain - Associate Director Physical
GUIDELINE FOR THROMBOPROPHYLAXIS IN ADULT (18 YEARS AND OLDER) IN GENERAL MEDICAL PATIENTS AND INPATIENTS UNDERGOING SURGERY
 IN GENERAL MEDICAL PATIENTS AND INPATIENTS UNDERGOING SURGERY") GUIDELINE FOR THROMBOPROPHYLAXIS IN ADULT (18 YEARS AND OLDER) IN GENERAL MEDICAL PATIENTS AND INPATIENTS UNDERGOING SURGERY SEE SEPARATE GUIDELINES FOR THROMBOPROPHYLAXIS IN OBSTETRICS This guidance does
GUIDELINE FOR THROMBOPROPHYLAXIS IN ADULT (18 YEARS AND OLDER) IN GENERAL MEDICAL PATIENTS AND INPATIENTS UNDERGOING SURGERY SEE SEPARATE GUIDELINES FOR THROMBOPROPHYLAXIS IN OBSTETRICS This guidance does
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY
 THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
Venous Thromboembolism Prophylaxis: Checked!
 Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
These are guidelines only and can be deviated from if it is thought to be in the patient s best interest.
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
Venous Thromboembolism National Hospital Inpatient Quality Measures
 Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
Venous Thromboembolism. Prevention
 Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
*Corresponding Author:
 Audit of venous thromboembolism prophylaxis administered to general surgical patients undergoing elective and emergency operations at National Hospital, Sri Lanka *Migara Seneviratne 1, Asanka Hemachandra
Audit of venous thromboembolism prophylaxis administered to general surgical patients undergoing elective and emergency operations at National Hospital, Sri Lanka *Migara Seneviratne 1, Asanka Hemachandra
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Single Technology Appraisal (STA)
") Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
VTE Prevention Guidelines (Venous Thromboembolism) (Venous Thromboembolism)
 (Venous Thromboembolism)") VTE Prevention Guidelines (Venous Thromboembolism) (Venous Thromboembolism) When using this document please ensure that the version you are using is the most up to date either by checking on the Trust
VTE Prevention Guidelines (Venous Thromboembolism) (Venous Thromboembolism) When using this document please ensure that the version you are using is the most up to date either by checking on the Trust
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Venous Thromboembolism Policy (VTE)
") Venous Thromboembolism Policy (VTE) DOCUMENT CONTROL: Version: 2 Ratified by: Clinical Effectiveness Committee Date ratified: 5 November 2013 Name of originator/author: Modern Matron St John s Hospice
Venous Thromboembolism Policy (VTE) DOCUMENT CONTROL: Version: 2 Ratified by: Clinical Effectiveness Committee Date ratified: 5 November 2013 Name of originator/author: Modern Matron St John s Hospice
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge
 in hospital and after discharge") Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
incidence of cancer-associated thrombosis (CAT) is further increased by additional risk factors such as chemotherapeutic 2
 is further increased by additional risk factors such as chemotherapeutic 2") CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
Warfarin in Adults : Guidelines for the use of. These guidelines apply to all patients commenced or continuing on warfarin
 Warfarin in Adults : Guidelines for the use of Document Type: Clinical Guideline Clinical Lead: Ian Neilly Author/s: Ian Neilly/Paul Barbieri Directorate: Haematology Approved by Haematology Specialty
Warfarin in Adults : Guidelines for the use of Document Type: Clinical Guideline Clinical Lead: Ian Neilly Author/s: Ian Neilly/Paul Barbieri Directorate: Haematology Approved by Haematology Specialty
Venous Thromboembolism (VTE) Prevention and Treatment of VTE in Patients Admitted to Hospital
 Prevention and Treatment of VTE in Patients Admitted to Hospital") Please Note: This policy is currently under review and is still fit for purpose. Venous Thromboembolism (VTE) Prevention and Treatment of VTE in Patients Admitted to Hospital This procedural document supersedes
Please Note: This policy is currently under review and is still fit for purpose. Venous Thromboembolism (VTE) Prevention and Treatment of VTE in Patients Admitted to Hospital This procedural document supersedes
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement. Marilyn Szekendi, PhD, RN
 Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Medicines Management Group
 Title SHARED CARE PROTOCOL for Extended Treatment of symptomatic VTE and prevention of its recurrence in Cancer Patients with Solid and Haematological Tumours Scope: Dalteparin (Fragmin ) may be considered
Title SHARED CARE PROTOCOL for Extended Treatment of symptomatic VTE and prevention of its recurrence in Cancer Patients with Solid and Haematological Tumours Scope: Dalteparin (Fragmin ) may be considered
Fatal P.E. Historic 1-2% Current %
 Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
DENOMINATOR: All surgical patients aged 18 years and older undergoing procedures for which VTE prophylaxis is indicated in all patients
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
Venous Thromboembolism Policy (VTE)
") Venous Thromboembolism Policy (VTE) DOCUMENT CONTROL: Version: v3 Ratified by: Clinical Quality Group Date ratified: 2 February 2016 Name of originator/author: Modern Matron St John s Hospice Name of responsible
Venous Thromboembolism Policy (VTE) DOCUMENT CONTROL: Version: v3 Ratified by: Clinical Quality Group Date ratified: 2 February 2016 Name of originator/author: Modern Matron St John s Hospice Name of responsible
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
Anticoagulation. MPharm Programme & OSPAP Programme. Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics
 MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
4/23/2009. September 15, 2008
 The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Single Technology Appraisal (STA)
") Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Clinical Policy: Dalteparin (Fragmin) Reference Number: ERX.SPA.207 Effective Date:
 Reference Number: ERX.SPA.207 Effective Date:") Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015
 Clinical Practice Guideline August 2015") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H
 Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H Authors' objectives To systematically review the incidence of deep vein
Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H Authors' objectives To systematically review the incidence of deep vein
Prevention and treatment of venous thromboembolic disease
 REVIEW Prevention and treatment of venous thromboembolic disease SUSAN McNEILL AND CATHERINE BAGOT Awareness of the risk factors for venous thromboembolic (VTE) disease and timely administration of thromboprophylaxis
REVIEW Prevention and treatment of venous thromboembolic disease SUSAN McNEILL AND CATHERINE BAGOT Awareness of the risk factors for venous thromboembolic (VTE) disease and timely administration of thromboprophylaxis
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
National Institute for Health and Clinical Excellence Health Technology Appraisal
 National Institute for Health and Clinical Excellence Health Technology Appraisal Rivaroxaban for the prevention of venous thromboembolism after elective orthopaedic surgery of the lower limbs Comment
National Institute for Health and Clinical Excellence Health Technology Appraisal Rivaroxaban for the prevention of venous thromboembolism after elective orthopaedic surgery of the lower limbs Comment
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 66 of 593
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES:
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
AN AUDIT: THROMBOPROPHYLAXIS FOR TOTAL HIP REPLACEMENT PATIENTS AT NORTHWICK PARK AND CENTRAL MIDDLESEX HOSPITALS
 The West London Medical Journal 2010 Vol 2 No 4 pp 19-24 AN AUDIT: THROMBOPROPHYLAXIS FOR TOTAL HIP REPLACEMENT PATIENTS AT NORTHWICK PARK AND CENTRAL MIDDLESEX HOSPITALS Soneji ND Agni NR Acharya MN Anjari
The West London Medical Journal 2010 Vol 2 No 4 pp 19-24 AN AUDIT: THROMBOPROPHYLAXIS FOR TOTAL HIP REPLACEMENT PATIENTS AT NORTHWICK PARK AND CENTRAL MIDDLESEX HOSPITALS Soneji ND Agni NR Acharya MN Anjari
Anticoagulants. Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT
 Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Are guidelines for anticoagulation useful in cancer patients?
 Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Venous Thromboembolism (VTE)
") Venous Thromboembolism (VTE) Nursing A guide for patients and carers Contents Why do blood clots form in veins?... 1 How common is a deep vein thrombosis (DVT) or pulmonary embolus (PE)?... 2 How are DVTs/
Venous Thromboembolism (VTE) Nursing A guide for patients and carers Contents Why do blood clots form in veins?... 1 How common is a deep vein thrombosis (DVT) or pulmonary embolus (PE)?... 2 How are DVTs/
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Drug Class Review Newer Oral Anticoagulant Drugs
 Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Blood Thinner Agent. Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy
 Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
TRANSPARENCY COMMITTEE OPINION. 18 April 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
Prevention of Venous Thromboembolism
 Prevention of Venous Thromboembolism Reference No: P_CS_05 Version 2.4 Ratified by: LCHS Trust Board Date ratified: 27 th January 2015 Name of originator / author: Medical Director Name of responsible
Prevention of Venous Thromboembolism Reference No: P_CS_05 Version 2.4 Ratified by: LCHS Trust Board Date ratified: 27 th January 2015 Name of originator / author: Medical Director Name of responsible
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Factor Xa Inhibition in the Management of Venous Thromboembolism: Important Safety Information. Important Safety Information (cont d)
") Factor Xa Inhibition in the Management of Venous Thromboembolism: The Role of Fondaparinux WARNING: SPINAL/EPIDURAL HEMATOMAS Epidural or spinal hematomas may occur in patients who are anticoagulated with
Factor Xa Inhibition in the Management of Venous Thromboembolism: The Role of Fondaparinux WARNING: SPINAL/EPIDURAL HEMATOMAS Epidural or spinal hematomas may occur in patients who are anticoagulated with
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS
 EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY
 EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients
 4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Deep Vein Thrombosis
 Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS
 Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS Please note that newer oral anticoagulants e.g. rivaroxaban, dabigatran and apixiban should be only be considered in patients with
Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS Please note that newer oral anticoagulants e.g. rivaroxaban, dabigatran and apixiban should be only be considered in patients with
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Handbook for Venous Thromboembolism
 Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Xarelto (rivaroxaban) Prescriber Guide
 Prescriber Guide") Xarelto (rivaroxaban) Prescriber Guide October 2018 PP-XAR-IE-0031 Contents Patient Alert Card 4 Dosing Recommendations 4 Stroke prevention in adult patients with non-valvular atrial fibrillation 4 Patients
Xarelto (rivaroxaban) Prescriber Guide October 2018 PP-XAR-IE-0031 Contents Patient Alert Card 4 Dosing Recommendations 4 Stroke prevention in adult patients with non-valvular atrial fibrillation 4 Patients
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Getting Started Kit VENOUS THROMBOEMBOLISM PREVENTION. Section 2: Evidence-Based Appropriate VTE Prophylaxis
 Reducing Harm Improving Healthcare Protecting Canadians VENOUS THROMBOEMBOLISM PREVENTION Getting Started Kit Section 2: Evidence-Based Appropriate VTE Prophylaxis January 2017 www.patientsafetyinstitute.ca
Reducing Harm Improving Healthcare Protecting Canadians VENOUS THROMBOEMBOLISM PREVENTION Getting Started Kit Section 2: Evidence-Based Appropriate VTE Prophylaxis January 2017 www.patientsafetyinstitute.ca
NICE guideline Published: 21 March 2018 nice.org.uk/guidance/ng89
 Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism NICE guideline Published: 21 March 2018 nice.org.uk/guidance/ng89 NICE 2018. All rights
Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism NICE guideline Published: 21 March 2018 nice.org.uk/guidance/ng89 NICE 2018. All rights
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get