Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO?
|
|
|
- Anthony Blair
- 5 years ago
- Views:
Transcription
1 Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO? Axel Grothey Professor of Oncology Minnesota -> Tennessee



2 The Luxury of So Many Options... How Do We Personalize? Patient X Patient Y PD-1 mab Patient Z
3 What influences treatment choices in mcrc? Patient characteristics Molecular characteristics Comorbidities Age Prior adjuvant treatment Performance status 1L 2L RAS MSI-high BRAF HER2 Tumor characteristics 3L Patient preference Tumor burden Resectability 4L Quality of life Toxicity profile Tumor location Therapy tailored according to individual patient needs
4 Key points in the medical management of mcrc We can cure some patients with limited metastatic disease Collaboration within a MDT essential For the majority of patients the treatment goal is to extend life and maintain quality of life as long as possible Patients benefit from access to all active agents Sequential therapy. It is a marathon, not a sprint We have biomarkers who identify cancers which do NOT respond to certain therapies, i.e. EGFR mabs Routine testing for extended RAS/ BRAF mutations, now also HER-2 Biomarkers that select patients FOR a specific therapy are emerging MMR/ MSI-H for immunotherapy, HER-2 and BRAF for targeted approaches
5 Key Points To Consider Outcome is not driven by first-line therapy for the majority of patients Importance of subsequent lines of therapy Continuum of care We have refined the patient population which benefits from EGFR mabs Better benefit-risk ratio Some patients need special treatment approaches MSI-H cancers BRAF mutated CRC (V600E vs non-v600e) HER-2 overexpressors
6 Proportional Impact on Magnitude of OS Benefit Achieved Across Lines of Therapy 1 L FOLFOX/XELOX ± bevacizumab 2 L 3/4 L FOLFIRI ± cetuximab b FOLFOX4 ± panitumumab a FOLFOX ± bevacizumab FOLFIRI ± panitumumab a CT ± continued bevacizumab FOLFIRI ± aflibercept Regorafenib vs placebo TAS102 vs placebo Not for RAS MT Not for RAS MT a KRAS WT subset; P value = not significant. b KRAS WT subset; P value = significant. 1. Saltz LB, et al. J Clin Oncol. 2008;26(12): ; 2. Douillard, J-Y, et al. J Clin Oncol. 2010;28(31): ; 3. Van Cutsem E, et al. J Clin Oncol. 2011;29(15): ; 4. Van Cutsem E, et al. J Clin Oncol. 2012;30(28): ; 5. Bennouna J, et al. Lancet Oncol. 2013;14(1):29-37; 6. Giantonio BJ, et al. J Clin Oncol. 2007;25(12) ; 7. Peeters M, et al. J Clin Oncol. 2010;28: ; 8. Grothey A, et al. Lancet. 2013;381: Van Cutsem E, et al. ESMO HR for OS Median OS improvement, months 3.5 b 4.2 a a
7 Although OS Continues to Improve, PFS Has Been Mostly Stable With First-line Therapy in the Chemo-Biologic Era PFS 15 OS Months 1. Hurwitz H, et al. N Engl J Med. 2004;350(23): ; 2. Saltz LB, et al. J Clin Oncol. 2008;26(12): ; 3. Bokemeyer C, et al. Ann Oncol. 2011;22(7): ; 4. Van Cutsem E, et al. J Clin Oncol. 2011;29(15): ; 5. Douillard JY, et al. N Engl J Med. 2013;369(11): ; 6. Heinemann V, et al. J Clin Oncol. 2013;(suppl 31):abstract LBA3506; 7. Falcone A, et al. J Clin Oncol. 2013;(suppl 31):abstract 3505.


8 The Key Question: First-Line Choice of Biologics BEV vs EGFR mabs Bevacizumab VS Cetuximab Panitumumab
9 Key Points on anti-vegf Therapy Duration of VEGF-inhibition matters More cytostatic than cytotoxic MoA Treatment to progression Maintenance strategies Treatment beyond progression Clinical synergism between fluoropyrimidine + bevacizumab Three positive phase III trials for prolonged VEGF inhibition beyond progression No compelling arguments for aflibercept or ramucirumab over bevacizumab
10 VEGFi Beyond PD - Phase III Trials Agent Bevacizumab Ziv-aflibercept Ramucirumab Study TML VELOUR RAISE 1 st Line Tx Chemo+BEV FP-Oxali+/- BEV FP-Oxali+BEV Chemo-BEV Chemo FOLFIRI + AFL FOLFIRI + PL FOLFIRI + RAM FOLFIRI + PL N pts mos (mos) HR 0.81 p= HR 0.82 p= HR 0.84 p=0.022 mpfs (mos) HR 0.68 p< HR 0.76 p= HR 0.79 p= RR (%) FP = fluoropyrimidine Bennouna et al., Lancet Oncol 2012 van Cutsem et al., JCO 2012 Tabernero et al., Lancet Oncol 2015
11 Key Points To Consider Outcome is not driven by first-line therapy for the majority of patients Importance of subsequent lines of therapy Continuum of care We have refined the patient population which benefits from EGFR mabs Better benefit-risk ratio Some patients need special treatment approaches MSI-H cancers BRAF mutated CRC (V600E vs non-v600e) HER-2 overexpressors
12 The Perfect Candidate for First-Line EGFR mabs Negative selection (mutually exclusive) KRAS/ NRAS/ HRAS exon 2, 3, 4 wild-type - 55% No BRAF V600E mutation - 8% (No HER-2 amplification -2.5%)

13 Bettington, et al Histopathology, 2013
14 Same Data: Different Perspectives RAS/ RAF wt Treatment recommendations Location primary ESMO NCCN Left Right EGFR mabs are Standard of Care in first-line EGFR mabs can be considered in first line if response is goal No clear preference for EGFR mabs or BEV in first line No EGFR mabs in first line and potentially not in any line
15 Metastatic Colorectal Cancer: Does Side Matter? Study Patients, N Line of Tx Molecular Selection Treatment Outcom e Right Left O Dwyer, et al. J Clin Oncol (E2290) N = st None 5-FU variations OS (mo) Brulé, et al. Eur J Cancer (CO.17) N = rd / 4 th KRAS WT BSC vs BSC + CET PFS (mo)

16 FIRE-3: Effect of Location on PFS and OS Heinemann, et al. ASCO 2014
17 CRYSTAL: FOLFIRI +/- Cetuximab L R PFS OS L R Tejpar et al., JAMA Oncol 2016
18 FIRE-3 Tejpar et al., JAMA Oncol 2016
19 OS and PFS by Sidedness in PRIME OS PFS Boeck, et al. Ann Oncol 2017
20 CALGB/SWOG 80405: OS by Tumor Location (RAS WT) % Event Free Cetux (n=173 vs 71) Bev (n=152 vs 78) OS (95% CI), Months Left 39.3 ( ) 32.6 ( ) Right 13.6 ( ) 29.2 ( ) HR (95% CI) 0.55 ( ) 0.88 ( ) P Value* Time From Study Entry, Months *Adjusted for biologic, protocol CT, prior adjuvant therapy, prior RT, age, sex, synchronous disease, in place primary, liver metastases. Venook A, et al. Presented at: ESMO
21 The Perfect Candidate for First-Line EGFR mabs Negative selection (mutually exclusive) KRAS/ NRAS/ HRAS exon 2, 3, 4 wild-type - 55% No BRAF V600E mutation - 8% (No HER-2 amplification -2.5%) Further exclusion criteria (not mutually exclusive) Right-sided cancers 30% (Low EGFR ligand expression 60%)
22 The Truth on Sidedness RAS/ RAF wt Location primary Left Right Treatment recommendations ESMO NCCN AG EGFR mabs are Standard of Care in first-line EGFR mabs can be considered in first line if response is goal No clear preference for EGFR mabs or BEV in first line No EGFR mabs in first line and potentially not in any line EGFR mabs are preferred, BEV can be used in select patients in first line No EGFR mabs in first line (if RR is goal, consider triplet), but allow EGFR mabs in later line
23 The Truth on Sidedness RAS/ RAF wt Location primary Left Right Treatment recommendations ESMO NCCN AG EGFR mabs are Standard of Care in first-line EGFR mabs can be considered in first line if response is goal No clear preference for EGFR mabs or BEV in first line No EGFR mabs in first line and potentially not in any line EGFR mabs are preferred, BEV can be used in select patients in first line No EGFR mabs in first line (if RR is goal, consider triplet), but allow EGFR mabs in later line
24 Sidedness and Tumor Response Based on published / presented results, not individual patient data. Mix of first- and second-line trials, with or without BEV P=0.089 Arnold et al., Ann Oncol 2017
25 Primary Tumor Location and Potential Treatments Anti-PD1 Right-sided MSI-H Left-sided Bev + Triplet CT BRAF MT HER2+ HER2-targeted agents KRAS MT KRAS WT AREG/EREG Bevacizumab + CT Anti-EGFRs + CT Bufill JA. Ann Intern Med. 1990;113: ; Missiaglia E, et al. ASCO Abstract 3526; Brule SY, et al. ASCO Abstract 3528; The Cancer Genome Atlas Network. Nature :61-70; Bendardaf R, et al. Anticancer Res. 2008;28:
26 Hallmarks of Cancer Acquired Capabilities for Tumor Growth and Progression Deregulating cellular energetics Resisting cell death Sustaining proliferative signaling Evading growth suppressors Avoiding immune destruction Enabling replicative immortality Interaction with outside world e.g. microbiome Genome instability & mutation Inducing angiogenesis Tumorpromoting inflammation Activating invasion & metastasis Hanahan D, et al. Cell. 2011;144:
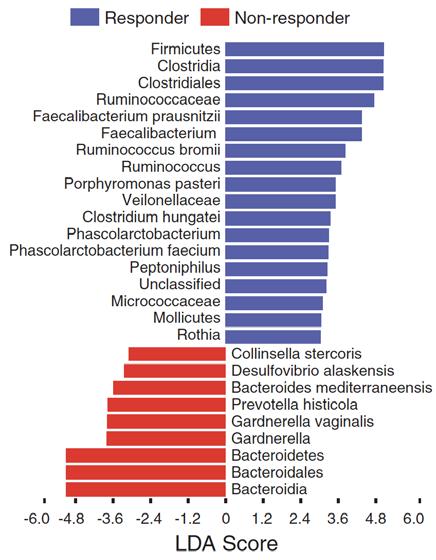
27 Gopalakrishnan et al., Science 359, (2018)
 Key findings: - Fusobacterium nucleatum commonly found in CRC tiss - 80% concordance between")
28 Bullman et al., Science 358, (2017) Key findings: - Fusobacterium nucleatum commonly found in CRC tiss - 80% concordance between FN colonization in primary an - FN also found in Xenografts - Antibiotic therapy reduced tu and proliferation index
29 Cell Line PDX Key findings: - Fusobacterium nucleatum commonly found in CRC tiss - 80% concordance between - FN also found in Xenografts - Antibiotic therapy reduced tu and proliferation index Bullman et al., Science 358, (2017)
30 Key Points To Consider Outcome is not driven by first-line therapy for the majority of patients Importance of subsequent lines of therapy Continuum of care We have refined the patient population which benefits from EGFR mabs Better benefit-risk ratio Some patients need special treatment approaches MSI-H cancers BRAF mutated CRC (V600E vs non-v600e) HER-2 overexpressors

 with MSI-H")

31 Mismatch Repair Deficiency (MMR-D): Unique Biological Subgroup of Colon Cancer IHC for MMR protein status MLH1+ MLH1- MSH2- MSH2+ Thus, IHC for MMR proteins PCR on and tumor PCR for MSI detect two manifestations of the same DNA for tumor MSI biology: (microsatellite MMR-D is synonymous instability) with MSI-H MMR-P is synonymous with MSI-L/MSS Imai and Yamamoto. Carcinogenesis 2008 Umetani, Annals of Surgical Oncology 2000 Rosen et al. Modern Pathology (2006) 19,

32 Hypermutation and Immuno-Oncology In CRC, MSI-H is associated with increases in immune infiltration and expression of immune checkpoint regulators 1,2 MSI-H is also associated with increased number of mutations per tumor Tumor mutations produce tumor-specific neoantigens, which when expressed on the tumor cell surface, are a target for T cells May improve response to immunotherapy Elevated neoantigen load in CRC is associated with improved survival 2 1. Llosa NJ, et al. Cancer Discov. 2015;5: Giannakis M, et al. Cell Reports. 2016;15:
33 Change from baseline SLD (%) MSI-high tumors are responsive to PD-1 inhibitors Pembrolizumab (KEYNOTE 016, phase II) 1,* 365 MMR-proficient CRC MMR-deficient CRC 730 Change from baseline (%) Nivolumab ± ipilimumab (CheckMate-142, phase II) 2 Nivolumab 3mg/kg Off treatment Nivolumab treatment ongoing 1st occurrence of new lesion CR or PR % change truncated to 100 Nivolumab 3mg/kg + ipilimumab 1mg/kg Time (weeks) Change from baseline (%) Time (weeks) Off treatment Nivolumab + ipilimumab treatment ongoing 1st occurrence of new lesion CR or PR Change from baseline SLD (%) MMR-proficient CRC MMR-deficient CRC Best reduction from baseline in target lesion (%) % change truncated to 100% 56% of patients with reduction ** * *** * ** * ** Best reduction from baseline in target lesion (%) % of patients with reduction * * * * * * * * * *Lynch Syndrome (yes/no/unknown): MMR-deficient CRC = 54/7/39; MMR-proficient CRC = 0/100/0 1. Le et al. ASCO 2016; 2.Overman et al. ASCO 2016
34 Recent FDA Approvals May 23, 2017: Pembrolizumab is indicated for the treatment of adult and pediatric patients with unresectable or metastatic solid tumors that have been identified as having a biomarker referred to as microsatellite instability-high (MSI-H) or mismatch repair deficient (MMR-D). This indication covers patients with solid tumors that have progressed following prior treatment and who have no satisfactory alternative treatment options and patients with colorectal cancer that has progressed following treatment with certain chemotherapy drugs. July 31, 2017: Nivolumab gained accelerated approval for the treatment of patients 12 years and older with mismatch repair deficient (MMR-D) or microsatellite instability high (MSI-H) metastatic colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan.
35 BRAF Mutations in CRC EGF BRAF is primary effector of KRAS signaling BRAF mutations: Occur most frequently in exon 15 (V600E) Found in 4%-14% of patients with CRC Mutually exclusive with KRAS mutations Yarden. Nat Rev Mol Cell Biol. 2001; Di Nicolantonio. J Clin Oncol. 2008; Artale. J Clin Oncol Tumor Cell Tumor cell proliferation and survival P P P P Ras Raf MEK Erk
 BRAF wildtype BRAF mut Tejpar et al, ASCO 2010 Roth et al.")
36 PETACC-3: Survival after relapse according to BRAF mutation status Median OS: BRAF mut: 7.49 m BRAF wt: 25.2 m (p = 1.9e-11) BRAF wildtype BRAF mut Tejpar et al, ASCO 2010 Roth et al. JCO 2010
37 FOLFOXIRI + BEV in BRAF V600E mut mcrc FOLFOXIRI +BEV FOLFIRI +BEV Loupakis et al., NEJM 2014
38 Rationale for combined BRAF and EGFR blockade EGFR RAS BRAF mut MEK ERK 1 Hong et al Cancer Disc 16
 + Irinotecan 60% 40% 20% HR = 0.48 (95% CI 0.31 0.75) P = 0.001 48% cross-over 0% 0 3 6 8 10 12 14 Months after randomization Kopetz et al.")
39 S1406: PFS Cetux+Irino +/- Vemurafenib 100% 80% N Events Median 95% Conf Int Cetuximab + Irinotecan ( ) Vemurafenib + Cetuximab ( ) + Irinotecan 60% 40% 20% HR = 0.48 (95% CI ) P = % cross-over 0% Months after randomization Kopetz et al., ASCO 2017
 N Median 95% CI")
 + Irinotecan HR = 0.73 (95% CI 0.45 1.17) P=0.")
40 100% 20% 0% -30% -100% 100% S1406: RR/OS Cetux+Irino +/- Vemurafenib Cetuximab + Irinotecan DCR 22% 4% Vemurafenib + Cetuximab + Irinotecan OS (mos) N Median 95% CI Cetuximab + Irinotecan ( ) Vemurafenib + Cetuximab ( ) + Irinotecan HR = 0.73 (95% CI ) P= % 16% 0% -30% -100% DCR 67% Kopetz et al., ASCO 2017
, then 250 mg/m 2 QW R 1:1:1 Triplet therapy ENCO + BINI + CETUX n=205 Doublet Therapy ENCO + CETUX n=205 Control Arm FOLFIRI +")
. Van Cutsem et al., ESMO GI 2018")
41 BEACON CRC Phase 3 Study Design 1 Safety Lead-in Completed Phase 3 Currently Enrolling ENCO 300 mg QD + BINI 45 mg BID + CETUX 400 mg/m 2 (initial), then 250 mg/m 2 QW R 1:1:1 Triplet therapy ENCO + BINI + CETUX n=205 Doublet Therapy ENCO + CETUX n=205 Control Arm FOLFIRI + CETUX, or IRI + CETUX n=205 Disease progression Disease progression Disease progression Continued follow-up for evaluation of OS N=30 1. Clinicaltrials.gov/ct2/show/NCT ; (February 2018). Van Cutsem et al., ESMO GI 2018
42 BEACON SLI: Confirmed Best Overall Response CONFIRMED BEST OVERALL RESPONSE* PATIENTS (N=29) ORR (CR + PR) 14 (48%) (95% CI 29% 67%) CR 3 (10%) PR 11 (38%) SD 13 (45%) PD 0 Not evaluable for response 2 (7%) ORR for patients with 1 and 2 prior regimens were 62% and 31% respectively 43% of responders have response 6 months Median DOR: 5.5 mo (95% CI, 4.1 NR) Median PFS: 8.0 months *Local assessed confirmed responses per RECIST 1.1 Patients with BRAF V600E mutations. Non-responders per intent-to-treat analysis. Van Cutsem et al., ESMO GI 2018
 -100 26 1 17 2 16 9 14 7 8 13 28 25 24 23 27 15 12 4* 22 21 19 20 18 11 6* 10 3 5* Patients *Patients with lymph node disease with decreases in short axis dimensions consistent with")
43 Best Percentage Change in Tumor Measurements from Baseline Best % Change from Baseline Cetuximab + Irinotecan from SWOG S Partial Response (n=11) Complete Response (n=3) * * * Patients *Patients with lymph node disease with decreases in short axis dimensions consistent with RECIST 1.1 defined Complete Response. One patient had no baseline sum of longest diameters and is not presented. 1. Kopetz S, et al. J Clin Oncol. 2017;35:Abstr 3505, with permission. Van Cutsem et al., ESMO GI 2018
44 BEACON SLI: Overall Survival year OS rate: 62% 80 Overall survival (%) Survival Rate 1 Prior Regimen 2 Prior Regimens 6 mo 88% 85% 12 mo 63% 62% Median OS: Not reached Data fully mature through 12.6 months 10 0 Patients at risk Patients with BRAF V600 mutation (N=29) Censored patients Time (mo) Van Cutsem et al., ESMO GI 2018
 2 3 K = 0.85 Int J Cancer 03 FISH: 4 (3%) Ooi et al. Mod Pathol 04 244 IHC: 8 (3%) FISH: 8 (3%) 2 6 100% Marx et al.")
 1 HER2 amplification enriched in KRAS, NRAS, BRAF, and PIK3CA WT tumors 2 1Siena et al.")
45 HER-2 Amplification in CRC Study HER2 overexpression N Positive and amplification Rate IHC is seen 2+ in a IHC3+ distinct subset FISH of Concordance mcrc Nathanson et al. 139 IHC: 5 (4%) 2 3 K = 0.85 Int J Cancer 03 FISH: 4 (3%) Ooi et al. Mod Pathol IHC: 8 (3%) FISH: 8 (3%) % Marx et al. Human Path IHC: 39 (3%) FISH: 36 (3%) % SummaryIHC Good 5.3% HER2 amplification seen in HERACLES Study (screened = 836) 1 HER2 amplification enriched in KRAS, NRAS, BRAF, and PIK3CA WT tumors 2 1Siena et al. GI ASCO Bertotti et al. Cancer Discovery 2011;1: Kuwada et al. Int. J. Cancer: 109, (2004)

46 HERACLES: Trastuzumab + Lapatinib Patients histologically diagnosed with metastatic CRC not amenable to surgery HER2+, KRAS exon 2 WT Prior fluoropyrimidines, irinotecan, oxaliplatin, cetuximab, or panitumumab; prior bevacizumab, aflibercept or regorafenib allowed but not mandatory PS 0-1 Therapy with Trastuzumab IV 4 mg/kg load and then 2 mg/qw Lapatinib po 1000 mg/qd (Enrolled n=24; evaluable n=23) PD Primary endpoint: ORR (RECIST 1.1 with central independent radiological review) Secondary endpoints: TTP, safety Translational: HER2 ctdna in plasma (ddpcr); HER2 ectodomain in serum (ELISA); NGS in tissue and plasma in de novo resistant patients and upon PD ddpcr=droplet Digital PCR; NGS=next-generation sequencing. Sartore-Bianchi, et al. Lancet Oncol 2016
47 HERACLES: Trastuzumab + Lapatinib Best Response (RECIST 1:1 by Central Rev) N % Responses (PR + CR) 8 30 Complete response 1 4 Partial response 7 26 Stable disease 4 mos 8 30 Stable disease <4 mos 4 15 Progressive disease % DCR Total Primary endpoint met in advance with 8/27 objective responses (as per protocol, 6/27 needed to declare the study positive) Sartore-Bianchi, et al. Lancet Oncol 2016
48 HERACLES: Responses Sartore-Bianchi, et al. Lancet Oncol 2016


49 MyPathway: Trastuzumab + Pertuzumab in HER-2 pos CRC N = 31, RR 42% Hurwitz et al., ASCO GI 2017
50 HER-2 Amplification in CRC Resistance marker for EGFR antibodies Defines patients who are candidates for HER-2 targeted therapy
51 Median Survival Increases With Increased Lines of Therapy Median OS, months SEER Medicare Database Analysis for mcrc ( ; N = 5,129) 6.8 HR = 0.398* HR = 0.604* 11.9 HR = 0.364* Total lines of therapy Patients should be exposed to all active and approved agents during their treatment *P <.001. HR, hazard ratio; SEER, Surveillance, Epidemiology, and End Results. Hanna N, et al. J Clin Oncol. 2014;32(suppl 3):abstract 559.
52 NCCN and ESMO mcrc Guidelines 1L 2L 3L 4L RAS mutation Chemo + anti-vegf Chemo + anti-vegf REGORAFENIB or TAS-102 Other anticancer therapy, BSC, or clinical trial RAS wild type Chemo + anti-vegf Chemo + anti-egfr REGORAFENIB or TAS-102 Other anticancer therapy, BSC, or clinical trial Left-sided cancers only per NCCN RAS wild type Chemo + anti-egfr Chemo + anti-vegf REGORAFENIB or TAS-102 Other anticancer therapy, BSC, or clinical trial RAS wild type Chemo + anti-vegf Chemo + anti-vegf Chemo + anti-egfr REGORAFENIB or TAS-102 Other anticancer therapy, BSC, or clinical trial BSC, best supportive care; EGFR, epidermal growth factor receptor; ESMO, European Society for Medical Oncology; NCCN, National Comprehensive Cancer Network; VEGF, vascular endothelial growth factor. Figure adapted from NCCN Clinical Practice Guidelines. Colon cancer. V2.2017; NCCN Clinical Practice Guidelines. Rectal cancer. V3.2017; Van Cutsem E, et al. Ann Oncol. 2016;27(8):

53 Regorafenib Studies Design CORRECT 1 and CONCUR 2 Phase III Trials R A N D O Regorafenib + BSC 160 mg orally once daily 3 weeks on, 1 week off Multicenter, randomized, doubleblind, placebo-controlled, phase III 2:1 randomization mcrc after standard therapy M I Z A T I O N 2 : 1 Placebo + BSC 3 weeks on, 1 week off Trial populations CORRECT global outside of Asia CONCUR Asia Grothey A, Van Cutsem E, et al. Lancet. 2013;381(9863): ; Li J, et al. Lancet Oncol. 2015;16(6):
54 Patient Eligibility for Regorafenib Phase III Trials CORRECT 1 CONCUR 2 Disease progression during/within 3 months after last administration of or intolerance to approved standard therapies, which had to include (if licensed) Fluoropyrimidine, oxaliplatin, irinotecan Bevacizumab Cetuximab or panitumumab (if KRAS wildtype) Age 18 years Adenocarcinoma of the colon or rectum ECOG performance status 0 1 Measurable or nonmeasurable disease Adequate bone marrow, liver, and renal function Signed informed consent Disease progression during/within 3 months after the last standard therapies (or within 6 months of stopping adjuvant oxaliplatin) or have stopped standard treatment because of unacceptable toxicity Prior anti-vegf or anti-egfr targeted therapy allowed, but not mandatory Asian adults 18 years of age Grothey A, Van Cutsem E, et al. Lancet. 2013;381(9863): ; Li J, et al. Lancet Oncol. 2015;16(6):
55 52% of Patients in CORRECT and 61% in CONCUR Received 3 or Fewer Prior Therapies for mcrc Regorafenib 160 CORRECT 1 mg + BSC (n = 505) Prior therapies for metastatic disease* Placebo + BSC (n = 255) 3 52% 53% 4 49% 47% Prior targeted therapy Any 100% 100% Trial Geography Global Regorafenib 160 CONCUR 2 mg + BSC (n = 136) Prior therapies for metastatic disease* Placebo + BSC (n = 68) 3 62% 60% 4 38% 40% Prior targeted therapy Any 59% 62% Trial Geography Asia *Previous therapies included fluoropyrimidines, oxaliplatin, irinotecan, and bevacizumab, and if KRAS wildtype, anti-egfr. Five patients on placebo (2%) and 16 patients on regorafenib (3%) had received only 1 prior therapy for metastatic disease. In CONCUR, some patients did not have access to targeted therapies; in contrast, all patients in CORRECT had received bevacizumab, and an anti-egfr agent had been utilized for all KRAS wildtype cases. Grothey A, Van Cutsem E, et al. Lancet. 2013;381(9863): ; Li J, et al. Lancet Oncol. 2015;16(6):
56 Significant Improvements in OS with Regorafenib in 2 Randomized Phase III Trials: CORRECT and CONCUR Overall survival (%) Number at risk Regorafenib Placebo 6.4 months OS with regorafenib Median OS (95% CI): Regorafenib 6.4 months ( ) Placebo 5.0 months ( ) HR = 0.77, 95% Cl: ; P = Months after randomization Regorafenib 160 mg Placebo 7 3 Overall survival (%) 100 Number at risk Regorafenib Placebo Median OS (95% CI): Regorafenib 8.8 months ( ) Placebo 6.3 months ( ) HR = 0.55, 95% Cl: ; P = months OS with regorafenib Months after randomization Regorafenib Placebo Censored patients CORRECT 1 : 23% reduction in the risk of death (primary endpoint) CONCUR 2 : 45% reduction in the risk of death (primary endpoint) 1. Grothey A, Van Cutsem E, et al. Lancet. 2013;381(9863): ; 2. Li J, et al. Lancet Oncol. 2015;16(6):
57 Drug-Related Treatment-Emergent Adverse Events Occurring in 10% of Patients Adverse Event, % Regorafenib (n = 500) Placebo (n = 253) All grades Grade 3 Grade 4 All grades Grade 3 Grade 4 Hand-foot skin reaction Fatigue Hypertension Diarrhea Rash/desquamation Anorexia Mucositis, oral Thrombocytopenia Fever Nausea Bleeding Voice changes Weight loss *Grade 5 drug-related AEs: 1.0% in regorafenib arm vs 0% in placebo arm Grothey A, Van Cutsem E, et al. Lancet. 2013;381:
58 Phase II ReDOS Study: Overview A1: 80 mg/d increasing to 160 mg/d (pre-emptive clobetasol) Patients with previously treated mcrc (N=123) R 1:1:1:1 A2: 80 mg/d increasing to 160 mg/d (reactive clobetasol) B1: Start at 160 mg/d (pre-emptive clobetasol) Primary Endpoint: % of patients who completed 2 cycles and initiated a 3 rd B1: Start at 160 mg/d (reactive clobetasol) Other endpoints: OS, PFS, TTP OS, overall survival; PFS, progression-free survival; TTP, time-to-progression. Data on File, ACCRU.
59 Phase II ReDOS Study: Percentage of Patients Starting Cycle 3 (primary endpoint) Percentage of patients a Fisher s exact test (1-sided) 43 P=.0281 a 24 Escalating Category Standard 1 dose dose Data on File, ACCRU.
60 Phase II ReDOS Study: OS (secondary endpoint) HR, hazard ratio; KM est, Kaplan-Meier estimate; OS, overall survival. Data on File, ACCRU.
61 TAS-102 Global Randomized Phase III study RECOURSE: Refractory Colorectal Cancer Study (NCT ) Metastatic colorectal cancer (mcrc) 2 or more prior regimens Refractory / Intolerable fluoropyrimidine irinotecan oxaliplatin bevacizumab anti-egfr if wild-type KRAS ECOG PS 0-1 Age 18 (target sample size: 800) R A N D O M I Z A T I O N 2:1 TAS BSC (n = 534) 35 mg/m 2 b.i.d. p.o. d1-5, 8-12 q4wks Placebo + BSC (n = 266) d1-5, 8-12 q4wks Endpoints Primary: OS Secondary: PFS, Safety, Tolerability, TTF, ORR, DCR, DoR, Subgroup by KRAS (OS and PFS) Treatment continuation until progression, intolerant toxicity or patient refusal Multicenter, randomized, double-blind, placebo-controlled, phase III Stratification: KRAS status, time from diagnosis of metastatic disease, geographical region Sites: 13 countries, 114 sites Enrollment: June 2012 to October 2013 Mayer et al., NEJM 2015
62 Survival Distribution function TAS-102 Overall Survival TAS-102 N=534 Placebo N=266 Events # (%) 364 (68) 210 (79) HR (95% CI) 0.68 ( ) Stratified Log-rank test p< Median OS, months Alive at, % Median follow-up: 8.4 months 6 months months Months from Randomization N at Risk: TAS Placebo Mayer et al., NEJM 2015
63 Mayer R and Van Cutsem E, et al. N Engl J Med. 2015;372: RECOURSE: OS Subgroup Analyses Favors TAS-102 Favors Placebo Subgroup Events / N HR (95% CI) For Internal Educational Use Only. Not for External Distribution. All patients 574 / ( ) ECOG Performance Status / ( ) / ( ) Primary Tumor Site Colon Rectal Number of Prior Regimens 2 3 >4 _ 361 / ( ) 213 / ( ) 106 / ( ) 137 / ( ) 331 / ( ) Prior Use of Regorafenib Use 94 / ( ) Not Use 480 / ( ) Refractory to Fluoropyrimidine Part of last prior regimen 329 / ( ) Hazard Ratio: TAS-102 versus Placebo (95% CI)
64 Why Regorafenib before TAS-102? Patients benefit from access to all active agents, i.e. Regorafenib AND TAS-102 Regorafenib appears to provide more benefit in less pretreated patients Regorafenib should not be used in PS2+ patients Do not let PS deteriorate before Regorafenib Side-effects can be managed Cytotoxic therapy (e.g. TAS-102) can be active after Regorafenib We have data on TAS-102 after Regorafenib Riechelmann R, Grothey A. Lancet Oncol. 2015
65 Conclusions Survival of patients with mcrc has significantly improved in the last decade Survival gains are not driven by advances in first-line therapy, but by incremental additions of effects of subsequent treatment lines In spite of advances in molecular profiling, sidedness is currently an independent prognostic (and for EGFR mabs, predictive) factor in mcrc Subgroups of patients are being identified which warrant a specific treatment intervention Regorafenib and TAS-102 are later-line treatment options
66 2018: A classical case of mcrc 3 months preterminal phase 3 months rechallenge 5 months first-line induction 3 months third line 3 months break 4 months second line OS 30 months 6 months maintenance 3 months reintroduction (or treatment beyond progression) Courtesy: Alberto Sobrero
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer
 Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression
 Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
AIOM GIOVANI Perugia, Luglio 2017
 AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux
 Michel Ducreux") Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO
 Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer. Objectives
 Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer Michael S. Lee, MD Assistant Professor of Medicine University of North Carolina Objectives Discuss important clinicopathologic
Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer Michael S. Lee, MD Assistant Professor of Medicine University of North Carolina Objectives Discuss important clinicopathologic
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Colon cancer: Highlights. Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano
 Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
Colon cancer: ASCO poster review. Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome
 Colon cancer: ASCO poster review Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome a.destefano@istitutotumori.na.it 255 poster examined: my selection Clinical Practice Translational &
Colon cancer: ASCO poster review Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome a.destefano@istitutotumori.na.it 255 poster examined: my selection Clinical Practice Translational &
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Colorectal Cancer in the Coming Years: What Can We Expect?
 Colorectal Cancer in the Coming Years: What Can We Expect? Clara Montagut, MD, PhD Hospital Universitari del Mar, Barcelona, Spain Memorial Sloan Kettering Cancer Center, New York, United States What Are
Colorectal Cancer in the Coming Years: What Can We Expect? Clara Montagut, MD, PhD Hospital Universitari del Mar, Barcelona, Spain Memorial Sloan Kettering Cancer Center, New York, United States What Are
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
First line treatment in metastatic colorectal cancer
 First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Colon Cancer ASCO Poster Review
 Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
JY Douillard MD, PhD Professor of Medical Oncology
 Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria
 IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
Colon Cancer: State of the Art
 Colon Cancer: State of the Art Heinz-Josef Lenz Professor of Medicine and Preventive Medicine Associate Director, Clinical Research J Terrence Lanni Chair in Cancer Research Co-Director, USC Center for
Colon Cancer: State of the Art Heinz-Josef Lenz Professor of Medicine and Preventive Medicine Associate Director, Clinical Research J Terrence Lanni Chair in Cancer Research Co-Director, USC Center for
Colorectal Cancer in 2017: From Biology to the Clinics. Rodrigo Dienstmann
 Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
What to do after 1st-line failure in mcrc?
 What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO. CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS?
 INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
Treatment of Advanced Colorectal Cancer
 Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Kolorektalni karcinom- novosti u liječenju. PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić
 Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
Eric Van Cutsem University Hospitals Leuven, Belgium
 BEACON CRC Study Safety Lead-in: Assessment of the BRAF Inhibitor Encorafenib + MEK Inhibitor Binimetinib + Anti Epidermal Growth Factor Receptor Antibody Cetuximab for BRAF V600E Metastatic Colorectal
BEACON CRC Study Safety Lead-in: Assessment of the BRAF Inhibitor Encorafenib + MEK Inhibitor Binimetinib + Anti Epidermal Growth Factor Receptor Antibody Cetuximab for BRAF V600E Metastatic Colorectal
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC
 Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
Management of Patients with Colorectal Cancer
 Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Fighting a Smarter War On Colon Cancer:
 Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Daniele Santini University Campus Bio-Medico Rome, Italy
 Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
MANAGEMENT OF ADVANCED COLORECTAL CANCER
 MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
La strategia terapeutica del carcinoma del colon metastatico
 Dalla Capecitabina al TAS-102 Milano, 29 settembre 2016 La strategia terapeutica del carcinoma del colon metastatico Gianluca Masi U.O. di Oncologia Medica Universitaria Azienda Ospedaliero-Universitaria
Dalla Capecitabina al TAS-102 Milano, 29 settembre 2016 La strategia terapeutica del carcinoma del colon metastatico Gianluca Masi U.O. di Oncologia Medica Universitaria Azienda Ospedaliero-Universitaria
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD
 Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018
 ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Ashita Waterston Beatson West of Scotland Cancer Centre
 Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
The ESMO consensus conference on metastatic colorectal cancer
 ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
What to do after 1 st line failure?
 ESMO Preceptorship Programme Colorectal Cancer Singapore 20-22 nd 2016 JY Douillard MD PhD ESMO CMO What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy
ESMO Preceptorship Programme Colorectal Cancer Singapore 20-22 nd 2016 JY Douillard MD PhD ESMO CMO What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy
COMETS: COlorectal MEtastatic Two Sequences
 COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
The left versus right colon cancer story What is the truth?
 The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Toxicity by Age Group. Old Factor 1: Age. Disclosures. Predicting survival in metastatic colorectal cancer. Personalized Medicine - Decision Tools -
 Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy?
 Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142
 Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
COLORECTAL CANCER: STATE OF THE ART
 COLORECTAL CANCER: STATE OF THE ART Andrés Cervantes Professor of Medicine DECLARATION OF INTERESTS Consulting and advisory services, speaking or writing engagements, public presentations Merck Serono
COLORECTAL CANCER: STATE OF THE ART Andrés Cervantes Professor of Medicine DECLARATION OF INTERESTS Consulting and advisory services, speaking or writing engagements, public presentations Merck Serono
Colorectal Cancer: Novel Insights
 Colorectal Cancer: Novel Insights Richard Kim M.D. Associate Professor Service Chief of Medical Oncology Department of Gastrointestinal Oncology Moffitt Cancer Center Tampa, FL Richard Kim, MD Colorectal
Colorectal Cancer: Novel Insights Richard Kim M.D. Associate Professor Service Chief of Medical Oncology Department of Gastrointestinal Oncology Moffitt Cancer Center Tampa, FL Richard Kim, MD Colorectal
Antiangiogenic therapy in GI cancer: current status and future directions
 Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Adjuvant treatment Colon Cancer
 ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
Medical Therapy of Colorectal Cancer in the Biomarker Era
 Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
ReDOS Trial Background
 Regorafenib Dose Optimization Study (ReDos) A Phase II Randomized Study of Lower Dose Regorafenib Compared to Standard Dose Regorafenib in Patients With Refractory Metastatic Colorectal Cancer (mcrc) Abstract
Regorafenib Dose Optimization Study (ReDos) A Phase II Randomized Study of Lower Dose Regorafenib Compared to Standard Dose Regorafenib in Patients With Refractory Metastatic Colorectal Cancer (mcrc) Abstract
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos?
 Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
Abetter understanding of the tumor biology of colorectal cancer has led to. Beyond the second line
 Beyond the second line of the care continuum in metastatic colorectal cancer In first-line treatment, a deep response on the tumor load is the primary aim to improve patient prognosis; however, in later
Beyond the second line of the care continuum in metastatic colorectal cancer In first-line treatment, a deep response on the tumor load is the primary aim to improve patient prognosis; however, in later
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES
 CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT?
 DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
XXV Corso Nazionale TSLB: evoluzione o ri(e)voluzione?
voluzione?") XXV Corso Nazionale TSLB: evoluzione o ri(e)voluzione? Marcatori predittivi di efficacia nel carcinoma del colon: DESTRO verso SINISTRO conta? Dott. Matteo Clavarezza S.C. Oncologia Medica RAS metastatic
XXV Corso Nazionale TSLB: evoluzione o ri(e)voluzione? Marcatori predittivi di efficacia nel carcinoma del colon: DESTRO verso SINISTRO conta? Dott. Matteo Clavarezza S.C. Oncologia Medica RAS metastatic
What s New? Dr. Barbara Melosky
 Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
HeavilyTreated mcrc..whats next?
 ESMO Preceptorship Programme Gastrointestinal Cancer 20-22 October 2016,Singapore Dr Surendra Pal Chaudhary Dept of Medical Oncology Dr BR Ambedkar Instituite Rotary Cancer Hospital All India Institute
ESMO Preceptorship Programme Gastrointestinal Cancer 20-22 October 2016,Singapore Dr Surendra Pal Chaudhary Dept of Medical Oncology Dr BR Ambedkar Instituite Rotary Cancer Hospital All India Institute
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer. Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center
 Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups. Chemotherapy and targeted agents in 1st line
 ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
New Options in Metastatic Colorectal Cancer. Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka
 New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
Optimizing Sequencing Beyond Disease Progression After Second-Line Therapy in Metastatic Colorectal Cancer
 Optimizing Sequencing Beyond Disease Progression After Second-Line Therapy in Metastatic Colorectal Cancer Kabir Mody, MD, and Tanios Bekaii-Saab, MD Abstract Colorectal cancer (CRC) remains a significant
Optimizing Sequencing Beyond Disease Progression After Second-Line Therapy in Metastatic Colorectal Cancer Kabir Mody, MD, and Tanios Bekaii-Saab, MD Abstract Colorectal cancer (CRC) remains a significant
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Axel Grothey West Cancer Center University of Tennessee, Germantown, TN, USA
 Updated Results of the BEACON CRC Safety Lead-in: Encorafenib (ENCO) + binimetinib (BINI) + cetuximab (CETUX) for BRAFV600E-mutant metastatic colorectal cancer (mcrc) Axel Grothey West Cancer Center University
Updated Results of the BEACON CRC Safety Lead-in: Encorafenib (ENCO) + binimetinib (BINI) + cetuximab (CETUX) for BRAFV600E-mutant metastatic colorectal cancer (mcrc) Axel Grothey West Cancer Center University
ADVANCES IN COLON CANCER
 ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
How to treat a patient with metastatic CRC? Towards personalized treatment strategies
 How to treat a patient with metastatic CRC? Towards personalized treatment strategies Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Progress in the treatment
How to treat a patient with metastatic CRC? Towards personalized treatment strategies Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Progress in the treatment
My name is Dr. David Ilson, Professor of Medicine at Memorial Sloan Kettering Cancer Center and Weill Cornell Medical Center in New York, New York.
 Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
State of the Art Colorectal Cancer (CRC) Marc Peeters, MD, PhD Antwerp University Hospital Edegem, Belgium
 Marc Peeters, MD, PhD Antwerp University Hospital Edegem, Belgium") State of the Art Colorectal Cancer (CRC) Marc Peeters, MD, PhD Antwerp University Hospital Edegem, Belgium Objectives 02 Review current approaches for the management of CRC Discuss current challenges/unmet
State of the Art Colorectal Cancer (CRC) Marc Peeters, MD, PhD Antwerp University Hospital Edegem, Belgium Objectives 02 Review current approaches for the management of CRC Discuss current challenges/unmet
Microsatellite instability and other molecular markers: how useful are they?
 Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
What to do after 1 st line failure?
 ESMO Preceptorship Programme Colorectal Cancer BARCELONA NOVEMBER, 25-26, 2016 What to do after 1 st line failure? Andrés Cervantes Professor of Medicine mcrc: Howtomaximizesurvival? Improving 1st line
ESMO Preceptorship Programme Colorectal Cancer BARCELONA NOVEMBER, 25-26, 2016 What to do after 1 st line failure? Andrés Cervantes Professor of Medicine mcrc: Howtomaximizesurvival? Improving 1st line
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)
 in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)") Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology