La strategia terapeutica del carcinoma del colon metastatico
|
|
|
- Cleopatra Dalton
- 5 years ago
- Views:
Transcription


1 Dalla Capecitabina al TAS-102 Milano, 29 settembre 2016 La strategia terapeutica del carcinoma del colon metastatico Gianluca Masi U.O. di Oncologia Medica Universitaria Azienda Ospedaliero-Universitaria Pisana Istituto Toscano Tumori
2 MCRC: KEY POINTS FOR A WINNING STRATEGY 1. MULTI-DISCIPLINARY ASSESSMENT Opportunity & timing for resect primary T Opportunity & timing for resect sites of M 2. CHOICE OF FIRST-LINE TREATMENT Set chemo-intensity (mono, doublet, triplet) Pick the best biological partner (anti-vegf vs anti-egfr) 3. ASSURE THE BEST CONTINUUM OF CARE Maintenance, Re-inducion, Re-challenge Second-line, Third-line,

3 Examples of treatment strategies in MCRC TREAT UNTILL PD AND SWITHC («old fashioned») Treatment 1 PD Treatment 2 PD Treatment 3 CHEMO HOLIDAYS AND SWITHC AT PD Treatment 1 PD Treatment 2 PD Treatment 3 SWITHC AT PD AND RECHALLENGE Treatment 1 PD Treatment 2 PD Treatment 1 CHEMO HOLIDAYS AND REINTRODUCTION AT PD Treatment 1 PD Treatment 1 PD Treatment 2 MAINTENANCE AND REINTRODUCTION AT PD Treatment 1 Maintenance PD Treatment 1 PD Tr 2
4 MCRC: CHOOSE THE FIRST-LINE THERAPY RESECATBILITY of MTS Easy, Border-line, Potentially CLINICAL PRESENTATION Sites of Mts & Burden Symptoms Side of Primary T (!?) MOLECULAR PROFILE RAS, RAF MSI (?), HER2 (?), THE PATIENT Comorbidities Expectations,


5 Upfront treatment is still a crucial step to Achieve disease control Allow further interventions (surgery and other systemic treatments)
6 The funnel effect PATIENTS 1st line 2nd line 3rd line 4th line 5th line
7 The funnel effect in the case of disease control/response 1st line 2nd line 3rd line 4th line 5th line PATIENTS

8 The funnel effect in the case of initial PD 1st line 2nd line 3rd line PATIENTS PD, progressive disease
9 What are our best evidenced-based options in first-line? Less intense Fluoropyrimidine + BV Doublets (FOLFOX, XELOX or FOLFIRI) + BV Doublets (FOLFOX or FOLFIRI) + anti-egfr More intense Triplet (FOLFOXIRI) + BV
10 What are our best evidenced-based options in first-line? Less intense Fluoropyrimidine + BV Doublets (FOLFOX, XELOX or FOLFIRI) + BV More intense Triplet (FOLFOXIRI) + BV
11 The AVEX study Capecitabine + BV 280 mcrc pts 1st line mcrc AGE >70 yrs R Stratification factors: ECOG PS (0 1 vs 2) Geographic region Capecitabine Key inclusion criteria ECOG PS 0 2 Prior adjuvant chemotherapy allowed if completed >6 month before inclusion Not optimal candidates for a combination chemotherapy with irinotecan or oxaliplatin Cunningham D. et al, Lancet Oncol 13
12 AVEX - Progression Free Survival Cunningham D. et al, Lancet Oncol 13
13 . The TASCO 1 trial
14 The TASCO 1 trial TAS-102 Twice a day 35 mg/m² orally BEVACIZUMAB 5 mg/kg IV 28-day cycle OR CAPECITABINE Twice a day 1250mg/m² orally BEVACIZUMAB 7.5 mg/kg IV 21-day cycle
15 What are our best evidenced-based options in first-line? Less intense Fluoropyrimidine + BV Doublets (FOLFOX, XELOX or FOLFIRI) + BV More intense Triplet (FOLFOXIRI) + BV
 5-FU/LV + bev PD INDUCTION MAINTENANCE Primary Endpoint: PFS Loupakis et al.")
16 TRIBE Study Design FOLFIRI + bev (up to 12 cycles) 5-FU/LV + bev 508 mcrc pts 1st line unresectable stratified by center PS 0/1-2 adjuvant CT R FOLFOXIRI + bev (up to 12 cycles) 5-FU/LV + bev PD INDUCTION MAINTENANCE Primary Endpoint: PFS Loupakis et al., NEJM 2014
17 Primary endpoint: PFS FOLFIRI + bev, median PFS : 9.7 mos FOLFOXIRI + bev, median PFS : 12.1 mos HR: 0.75 [ ] p=0.003 Loupakis et al., NEJM 2014
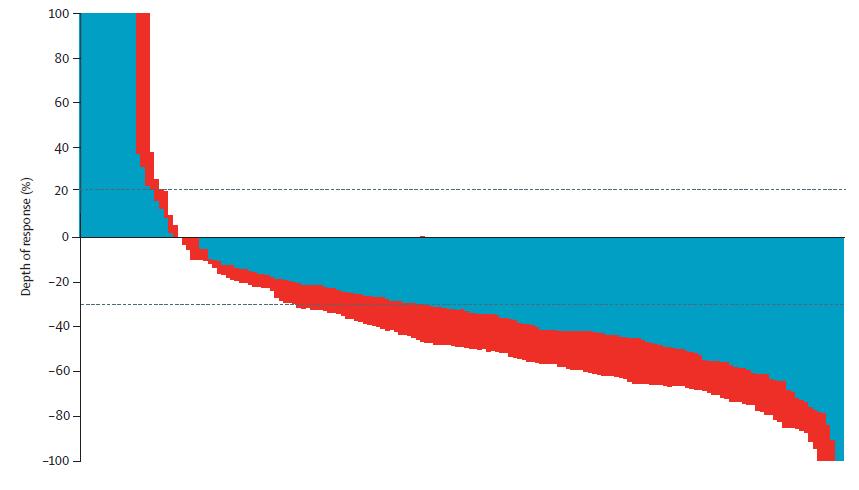
 60 FOLFOXIRI + bevacizumab 40 (43.4%) 20 0-20 -40 51.9% 62.")
18 TRIBE: FOLFOXIRI + bev improves RECIST response, ETS and DoR RECIST Response: 53% vs 65 % p=0.006 Tumour shrinkage 20% at 8 wks Depth of response FOLFIRI + bevacizumab FOLFOXIRI + bevacizumab 80 FOLFIRI + bevacizumab (37.8%) 60 FOLFOXIRI + bevacizumab 40 (43.4%) % 62.7% P =.003 P =.025 Loupakis F, et al. N Engl J Med. 2014;23;371(17): Cremolini C, et al. Ann Oncol. 2015;26(6):
19 TRIBE: Updated OS results Median follow-up: 48.1 mos FOLFIRI + bev, median OS: 25.8 mos FOLFOXIRI + bev, median OS: 29.8 mos HR: 0.80 [ ] P = year OS rate 24.9% vs 12.4% Cremolini C, et al. Lancet Oncol 2015
20 TRIBE in molecular subgroups - OS RAS and BRAF wild-type arm A RAS mutant arm A BRAF mutant arm A RAS and BRAF wild-type arm B RAS mutant arm B BRAF mutant arm B Median OS 41.7 months 33.5 months 27.3 months 23.9 months 19.0 months 10.7 months Cremolini et al, Lancet Oncol 15


21 Decision drivers for FOLFOXIRI FOLFOXIRI plus bev appropriateness
 + BV Doublets (FOLFOX or FOLFIRI)")
22 What are our best evidenced-based options in first-line? Less intense Fluoropyrimidine + BV Doublets (FOLFOX, XELOX or FOLFIRI) + BV Doublets (FOLFOX or FOLFIRI) + anti-egfr More intense Triplet (FOLFOXIRI) + BV
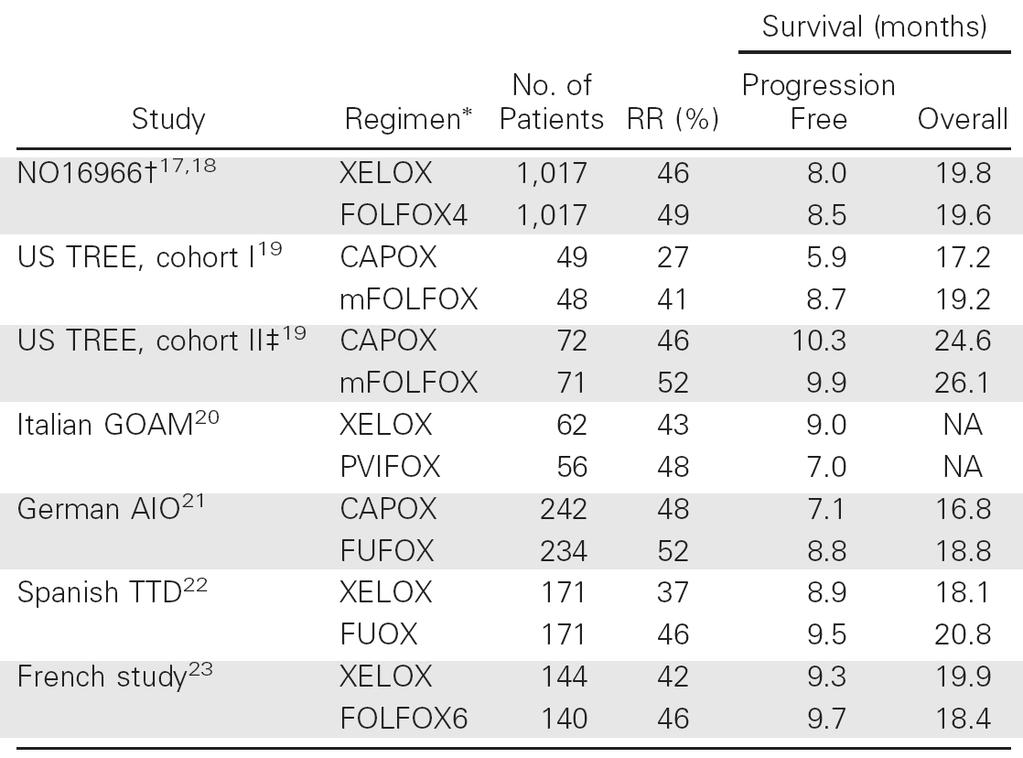
23 Capecitabine + Oxaliplatin vs 5FU + Oxaliplatin N RR PFS OS German AIO CapOx % FUFOX % Spanish TTD Xelox % FUOX % NO16966 Xelox 350 n.a FOLFOX 351 n.a
24
25 6 randomized trials (N=3494) Decreased RR (OR= 0.85, p=0.02) Equivalent PFS (HR= 1.04, p=0.17) Equivalent OS (HR= 1.04, p=0.41)
26 NO16966 study design Recruitment June 2003 May 2004 Recruitment Feb 2004 Feb 2005 XELOX N=317 FOLFOX4 N=317 XELOX + placebo N=350 FOLFOX4 + placebo N=351 XELOX + bevacizumab N=350 FOLFOX4 + bevacizumab N=350 Initial 2-arm open-label study (N=634) Protocol amended to 2x2 placebocontrolled design after bevacizumab phase III data 1 became available (N=1401) Saltz et al, JCO 2009
27 PFS estimate PFS chemotherapy + bevacizumab superiority: XELOX and FOLFOX subgroups Months Months XELOX+placebo N=350; 270 events XELOX+bevacizumab N=350; 258 events XELOX subgroup HR = 0.77 [97.5% CI ] (ITT) p = FOLFOX+placebo N=351; 277 events FOLFOX+bevacizumab N=349; 255 events FOLFOX subgroup HR = 0.89 [97.5% CI ] (ITT) p = Saltz et al, JCO 2009

28 Maughan et al, ESMO 2009
29 Maughan et al, ESMO 2009
30 Capecitabine + Irinotecan vs 5FU + Irinotecan EORTC CAPIRI vs FOLFIRI: suspended due to occurrence of 6 treatment related deaths in the CAPIRI arm BICC-C CAPIRI vs FOLFIRI: efficacy safety CAIRO-1 CAPIRI: is safe Oral chemotherapy needs ACTIVE management!!!

31
32
33 WHICH BIOLOGIC IN FIRST-LINE? Direct comparisons anti-egfrs vs bev FIRE-3 CALGB C80405 PEAK




34 Phase III study design FOLFIRI + Cetuximab mcrc 1st-line therapy KRAS wild-type N= 592 Randomize 1:1 Cetuximab: 400 mg/m 2 i.v. 120min initial dose 250 mg/m 2 i.v. 60min q 1w FOLFIRI + Bevacizumab Bevacizumab: 5 mg/kg i.v min q 2w Key inclusion criteria Patients 18 years with histologically confirmed diagnosis of mcrc ECOG PS 0-2 prior adjuvant chemotherapy allowed if completed >6 month before inclusion Amendment in October 2008 to include only KRAS wildtype patients 150 active centers in Germany and Austria FOLFIRI: 5-FU: 400 mg/m 2 (i.v. bolus); folinic acid: 400mg/m 2 irinotecan: 180 mg/m 2 5-FU: 2,400 mg/m 2 (i.v. 46h)
35 Probability of survival Progression-free survival Events n/n (%) FOLFIRI + Cetuximab 250/297 (84.2%) FOLFIRI + Bevacizumab 242/295 (82.0%) Median (months) 95% CI HR 1.06 (95% CI ) Log-rank p= numbers at risk months since start of treatment
36 Probability of survival Overall survival Events n/n (%) FOLFIRI + Cetuximab 158/297 (53.2%) FOLFIRI + Bevacizumab 185/295 (62.7%) Median (months) 95% CI HR 0.77 (95% CI: ) Log-rank p= numbers at risk months since start of treatment
37 Probability of survival Overall survival RAS* wild-type * KRAS and NRAS exon 2, 3 and 4 wild-type Events n/n (%) FOLFIRI + Cetuximab 91/171 (53.2%) FOLFIRI + Bevacizumab 110/171 (64.3%) Median (months) 95% CI HR 0.70 (95% CI: ) p (log-rank)= No. at risk months since start of treatment Adapted from Heinemann V, et al. ECCO-ESMO 2013
38 CALGB/SWOG 80405: FINAL DESIGN mcrc 1st-line KRAS wild type (codons 12,13) FOLFIRI or FOLFOX MD choice Chemo + Cetuximab Chemo + Bevacizumab N = Endpoint: Overall Survival
39 CALGB/SWOG 80405: Overall Survival Arm Chemo + Cetux N (Events) OS (m) Median 95% CI 578 (375) Chemo + Bev 559 (371) P=0.34 HR ( ) Presented by: Venook A
40 CALGB 80405: Overall Survival By Arm (All RAS Wild Type Patients) Arm Chemo + Bev Chemo + Cetux N (Events) 256 (178) 270 (177) Median (95% CI) 31.2 ( ) 32.0 ( ) HR (95% CI) 0.9 ( ) p 0.40 Lenz HJ et al, ESMO 2014


41
42
43 OS
44 PFS
45 RR
46 Main troubles with H-H comparison trials PEAK Phase II random Primary EP (PFS): negative FIRE-3 Primary EP (RR): negative Data interpretation CALGB/SWOG N. pts analyzed Data quality
47 FIRE-3: possible explanations for OS Choice and duration of 2nd line therapy Change in tumor biology during 1st line therapy OS Depth of response
48 Early Tumor Shrinkage & Deepness of Response Lethal tumor load OS Baseline tumor load ETS ETS ETS predicts sensitivity ETS predicts the potential DpR DpR predicts OS DpR (smallest tumor size) Time under treatment ETS: early tumor shrinkage 1,2 DpR: depth of response 3 At least 20% decrease (shrinkage) in the sum of the longest diameter compared with baseline at week 8 Percentage of tumor shrinkage observed at the smallest tumor size compared with baseline adapted from Mansmann et al, ASCO GI 2013 abstract #427
49
50

51 Courtesy :Andrea Sartore Bianchi AIOM 2015

52 PFS 2nd = First-line FOLFIRI+CET = First-line FOLFIRI+BEV OS 2nd
53 COMETS: Study design Study conducted in 11 centres in Italy PFS BEV + FOLFIRI (n=110) PD Randomise 1:1 Irinotecan/ CETUXIMAB FOLFOX FOLFOX Irinotecan/ CETUXIMAB 101 events were required to achieve a power of 80% of detecting a HR of 0.57 in favour of one of the two sequences, translating in an increase of median overall PFS from 4 to 7 months, with a type I error of 5%, two-sided, using the Mantel-Cox version of the log-rank test. 110 assessable patients were needed to reach the target number of events. Primary endpoint Secondary endpoints Progression-free survival (PFS) Overall survival (OS) from randomisation; PFS 2 and 3 line; Overall response rate Safety Clinicaltrials.gov: NCT Research Funding Source: AIFA (Agenzia Italiana del Farmaco) Code FARM 6XB38F Cascinu S., Labianca R. et al. ECC 2015
54 Efficacy data according to arm Arma A CETUX/CPT (55 patients) Arm B FOLFOX (55 patients) Hazard ratio (95% CI) Response rate (%) 19/52 (37%) 30/53 (57%) p= 0.05 Fisher exact test Overall median PFS (months) HR 0.83 ( ); p= 0.37 Overall median survival (months) HR 0.79 ( ); p= 0.26 Arm A: Cetuximab/irinotecan followed by FOLFOX Arm B: FOLFOX followed by Cetuximab/irinotecan Adapted: Cascinu S., Labianca R. et al. ECC 2015

55 X Colon?? RIGHT LEFT
56 Metastatic Colorectal Cancer: Does Side Matter? PUBLICATION (Study) Patients N Molecular Selection Treatment OUTCOME RIGHT LEFT O Dwyer JCO, 2001 (E2290) Brule, Eur J Can, 2015 (CO.17) Loupakis, JNCI, 2015 N = 1120 NONE 5FU VARIATIONS OS (MOS) N =399 KRAS wt BSC v. BSC + CET N = 2053 NONE FOLFIRI/BEV FUOX/BEV IFL/BEV PFS (MOS) OS (MOS)
 (95% CI) 33.3 (31.4-35.7) 1.55 19.4 (1.32-1.82) (16.7-23.6) p < 0.")
57 80405: Overall Survival by Sidedness Side N (Events) Left 732 (550) Right 293 (242) Median HR (95% CI) (95% CI) 33.3 ( ) ( ) ( ) p < Left Right Presented by:
58 Right versus Left and Bevacizumab AVF2017g : p for interaction OS=0.38; PFS=0.59 NO16966 : p for interaction OS=0.29; PFS=0.62


59 Right versus Left and anti-egfr: OS in FIRE-3 FOLFIRI+cetuximab FOLFIRI+bevacizumab Heinemann et al., ASCO 14
60 Impact of primary tumor location on Overall Survival and Progression Free Survival in patients with metastatic colorectal cancer: Analysis of CALGB/SWOG (Alliance) A Venook, D Niedzwiecki, F Innocenti, B Fruth, C Greene, BH O Neil, J Shaw, J Atkins, LE Horvath, B Polite, JA Meyerhardt, EM O Reilly, R Goldberg, HS Hochster, CD Blanke, R Schilsky, RJ Mayer, M Bertagnolli, HJ Lenz for SWOG and the ALLIANCE
61 Patient Characteristics by Tumor Side, (KRAS wt) RIGHT-SIDED (N = 293) LEFT-SIDED (N = 732) TOTAL* (N = 1137) P Age (mean) < Gender (M %) 54.9% 65.0 % 62.1% Synchronous Stage IV 86.9% 76.0% 79.3% Prior Adjuvant 10.6% 15.7% 14.2% 0.03 FOLFOX / FOLFIRI 74.4 / / / Primary in place 19.2% 29.6% 26.6% Pattern mets: liver only liver mets extra-hepatic 27.5% 40.5% 32.0 % 32.1% 43.2% 24.7% 30.9% 42.8% 28.5% *Transverse colon 66 (excluded from analysis); unknown - 46 **Test of any liver metastases versus extrahepatic 0.02**
62 80405: OS by Sidedness (Bevacizumab) Median Side N (Events) HR(95% CI) p (95% CI) 31.4 Left 356 (280) 1.32 ( ) 0.01 ( ) 24.2 Right 150 (121) ( ) Right Left Presented by:
 1.87 (32.6-40.3) <0.0001 (1.48-2.32) 16.7 Right 143 (121) (13.1-19.")
63 80405: OS by Sidedness (Cetuximab) Median HR Side N (Events) p (95% CI) (95% CI) 36.0 Left 376 (270) 1.87 ( ) < ( ) 16.7 Right 143 (121) ( ) Right Left Presented by:
 36.0 (32.6-40.3) 24.2 (17.9-30.3) 16.7 (13.1-19.")
64 80405: Overall Survival by Sidedness and Biologic 31.4 ( ) 36.0 ( ) 24.2 ( ) 16.7 ( ) Presented by:

65 MIDGUT Bettington, et al. Histopathology HINDGUT Bettington, et al Histopathology, 2013

66

67

68
69 Which is the best strategy in mcrc? RAS WT (and BRAF WT) pts have a MAJOR benefit from anti-egfr moabs Maintenance & Treatment Beyond PD maximize the benefit of BEVA WHAT IS THE NEED OF A RAPID & DEEP RESPONSE??? WHAT IS THE CHANCE TO RECEIVE A THIRD-LINE THERAPY???
70 Which variables to consider in the choice of second-line? Patient clinical characteristics Patient preferences Performance status Age Comorbidities Prior adjuvant treatment Expectations Toxicity profile First-line related factors Which chemo Which biologic Which response Tolerance Residual toxicities Drug free-interval Tumour Molecular characteristics Tumour clinical characteristics RAS BRAF Tumour burden Resectability Related symptoms Aggressiveness

71


72
73 Targeted agents in second line MCRC COMBINATION STUDY RR PFS OS Bevacizumab + IRI or LOHP-based CT (E3200) TML BEPYP NO YES YES Aflibercept + FOLFIRI VELOUR YES YES YES Ramucirumab + FOLFIRI RAISE NO YES YES Cetuximab + IRI EPIC Panitumumab + IRI PICCOLO Panitumumab + FOLFIRI 181 YES YES NO
74 Anti-angiogenic agents in 2nd line Bevacizumab Aflibercept Ramucirumab FDA and EMA approved VEGF-A PlGF VEGF-B VEGF-A VEGFR-2
75 Bevacizumab beyond progression: TML trial 2 nd line chemo 820 mcrc pts progressed to a 1st line chemo plus Beva* R Primary Endpoint: Overall survival 2 nd line chemo + BEV * progressed up to 3 months after discontinuing 1st-line bevacizumab switched chemo Bennouna et al, Lancet Oncol 2013
76 Bevacizumab Beyond Progression: TML trial - OS Bennouna, Lancet Oncol 2013
77 Anti-angiogenic agents in 2nd line Bevacizumab Aflibercept Ramucirumab FDA and EMA approved VEGF-A PlGF VEGF-B VEGF-A VEGFR-2
78 Aflibercept: VELOUR trial 1226 mcrc pts progressed to a 1st line oxaliplatin-based therapy* Primary Endpoint: Overall survival R 2 nd line FOLFIRI 2 nd line FOLFIRI+afl * 1 st -line bev allowed and administered in 30% of pts Van Cutsem et al, J Clin Oncol 2012
79 VELOUR trial: Primary endpoint met (OS) Van Cutsem et al, J Clin Oncol 12

80 VELOUR trial: PFS & Response Rate
81 Anti-angiogenic agents in 2nd line Bevacizumab Aflibercept Ramucirumab VEGF-A PlGF VEGF-B VEGF-A VEGFR-2
82 Ramucirumab: RAISE trial 1072 mcrc pts progressed to a 1st line therapy with oxaliplatin, fluoropyrimidine and BEV R 2 nd line FOLFIRI 2 nd line FOLFIRI+ram Primary Endpoint: Overall survival Tabernero et al, Lancet Oncol 2015
83 RAISE trial: OS results Tabernero et al, Lancet Oncol 2015
84 Angiogenesis inhibition in second line Bevacizumab Aflibercept Ramucirumab Study TML E3200 VELOUR RAISE mos HR 0.81* 0.75* 0.82* 0.84* mpfs HR 0.68* 0.61* 0.76* 0.79* RR (%) * * * p< % prior Beva NO prior Beva 30% prior Beva 100% prior Beva Bennouna Lancet Oncol Giantonio JCO Van Cutsem JCO 2012 Tabernero Lancet Oncol 2015
85 Can toxicity profile help us? G3/4 adverse events, % Chemo + bevacizumab TML FOLFIRI + aflibercept VELOUR FOLFIRI + ramucirumab RAISE Diarrhea 10% 19% 19% 11% Stomatitis 3% 14% 11% 4% Neutropenia 16% 37% 20% 38% Hypertension 2% 19% 16% 11% Venous thromboembolism 5% 8% 7% 3% Arterial thromboembolism 2% 2% 2% <1% ITT Prior Bev 100% prior Bev 100% prior Bev population subgroup Adapted from: Bennouna et al, Lancet Oncol 2012; Tabernero et al, Eur J Cancer 2014; Van Cutsem et al, J Clin Oncol 2012; Tabernero et al, Lancet Oncol 2015
86 Bevacizumab Beyond PD: alternatives??? Anti EGFR EPIC, J Clin Oncol 2008 PICCOLO, Lancet Oncol 2013 Pmab 181, Ann Oncol 2014 No Formal Evidence of Survival Benefit Cross over (activity in third-line) Re-think on the basis of extended molecular selection
87 Panitumumab in 2nd line: 181 trial 1186 mcrc pts progressed to a 1st line fluoropyrimidine-based therapy R 2 nd line FOLFIRI 2 nd line FOLFIRI+Pan Primary Endpoints: Overall survival and Progression-free Survival, by KRAS status Peeters et al, JCO 2010
88 181 trial: OS and PFS results in RAS wt population OVERALL SURVIVAL PROGRESSION-FREE SURVIVAL 34% of patients assigned to FOLFIRI eventually received anti-egfr Peeters et al, Clin Cancer Res 2015

89 In the Event that Tumor Shrinkage Is Needed Study: ORR and Depth of response Peeters et al, Clin Cancer Res 2015
90 Anti-EGFR moabs in second line Cetuximab Panitumumab Study EPIC PICCOLO mos HR (p=0.08) 0.92 mpfs NA NA HR 0.69* 0.70* 0.68* RR (%) 16.4* * * 12.3 * p<0.05 No molecular selection RAS wt all-wt (RAS, BRAF, PIK3CA) Sobrero JCO 2008 Peeters Clin Cancer Res Seymour Lancet Oncol
91 Which Biologic After CT+Bev? Bevacizumab both after Oxa-based and CPT-based 1 st line and with FOLFIRI or FOLFOX or XELOX Aflibercept only after oxa-based 1 st -line and only with FOLFIRI Ramucirumab only after oxa-based+beva 1 st -line and only with FOLFIRI Anti-EGFRs only RAS WT; only with CPT-based CT; mainly if shrinkage is needed
92 Third and further-line treatments
93 Well established «salvage» options Anti-EGFR (pani, cet +/- irinotecan) In RAS wt pts not previously treated with anti-egfr Chemo Rechallenge No prospective evidences Carefully consider previous benefit and toxicity REGORAFENIB TAS-102
94 Regorafenib: indication and approval mcrc pts, pretreated or not considered candidates for available tx 27 September August August 2015

95 CORRECT trial Study design mcrc pts treated with all standard tx PD during or 3 months after last tx R 1:2 N= 760 Placebo + BSC N= 255 Regorafenib + BSC Stratification by Prior BV Time from diagnosis of mets Geographical region N= 505 Primary end-point: OS Grothey et al, Lancet 2013


96 CORRECT trial: Patients characteristics Grothey et al, Lancet 2013
97 CORRECT trial Primary end-point MET Regorafenib mos = 6.4 mos Placebo mos = 5.0 mos HR=0.77 (95%CI ) p= Grothey et al, Lancet 2013
98 CONCUR trial Outcome Results Regorafenib mos = 8.8 mos Placebo mos = 6.3 mos HR=0.55 (95%CI ) p= Regorafenib mpfs = 3.2 mos Placebo mpfs = 1.7 mos HR= % CI p< HR=0.31 (95%CI ) p< Li et al, Lancet Oncol 2015
99 Regorafenib: safety profile G 3 Adverse event % Rego (n=505) CORRECT CONCUR CONSIGN Placebo (n=255) Rego (n=136) Placebo (n=68) Rego (2872) HFS 17 < Fatigue Hypertension Diarrhea Rash <5 Bilirubin increase Grothey et al, Lancet 2013 Li et al, Lancet Oncol 2015 Van Cutsem et al, WCGIC 2015
100 AEs and dose modifications: CORRECT and CONCUR Rego (n=505) CORRECT Placebo (n=255) Rego (n=136) CONCUR Placebo (n=68) G 3 AE Treatment modification* *interruption, delay, dose reduction Grothey et al, Lancet 2013 Li et al, Lancet Oncol 2015





101 TAS-102: indication and approval mcrc pts, pretreated or not considered candidates for available tx 22 September April 2016 Pending





102 TAS-102: mechanism of action TPase FTY (inactive form) TPI TAS-102 FTD + TPI Molar ratio = 1:0.5 FTD:Trifluorothymidine TPI:Tipiracil-HCl FTD F 3 TMP F 3 TDP F 3 TTP Inhibition of tumor growth DNA dysfunction FTD incorporation into DNA 15mg tablet 20mg tablet
103 RECOURSE trial Study design mcrc pts treated with 2 tx lines refractory to all standard tx* R 1 : 2 N= 800 Placebo + BSC N= 266 TAS 102+ BSC N= 534 About 20% rego-pretreated Primary end-point: OS *PD during or 3 months after all active drugs Mayer et al, NEJM 2015
104 Recourse trial Primary end-point OS MET TAS-102 mos = 7.1 mos Placebo mos = 5.3 mos HR=0.68 (95%CI ) p<0.001 Mayer et al, NEJM 2015
105 Survival distribution function Recourse trial updated OS Trifluridine/tipiracil (N=534) Placebo (N=266) Median OS (months) Stratified log-rank test: p< HR: 0.69, 95% CI [0.59, 0.81] Alive at 12 months, % No. at Risk: Months from randomization Trifluridine/tipiracil Placebo Carried out at 89% of events (138 additional events) Cut off October 8th, 2014: 712 events Mayer R, et al. ASCO GI 2016 Abstract 634
106 Recourse trial subgroup analysis OS Subgroup Favours trifluridine/tipiracil Favours placebo Events / N HR (95% CI) All patients 574 / ( ) KRAS status Wild type Mutant Time since diagnosis of first metastasis <18 months 18 months Geographic region Japan US, Europe & Australia Age <65 years 65 years Gender Male Female ECOG performance status 0 1 Primary tumor site Colon Rectum Number of prior regimens Prior use of regorafenib Yes No 280 / / / / / / / / / / / / / / / / / / / ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) Refractory to fluoropyrimidine part of last prior regimen 329 / ( ) Hazard ratio: Trifluridine/tipiracil vs. placebo (95% CI) Mayer RJ, Van Cutsem E, et al. N Engl J Med. 2015;372:
107 Recourse trial RR & DCR Disease control rate Response rate 60% 50% 40% 30% 20% 10% 0% 44% p< % Trifluridine/tipiracil Placebo Trifluridine/tipiracil (N=112) % Placebo (N=57) % CR 0 0 PR SD ORR (%) Mayer RJ, Van Cutsem E, et al. N Engl J Med. 2015;372:
108 REGO vs TAS Efficacy CORRECT RECOURSE Rego (n=500) Placebo (n=253) TAS-102 (534) Placebo (266) mpfs HR mos HR
109 RECOURSE trial Safety profile Lab abnormalities, % TAS-102 (n=533) Placebo (n=265) All Gr Gr 3 All Gr Gr 3 Leukopenia Anemia Neutropenia <1 0 Thrombocytopenia <1 TAS-102 (n=533) Placebo (n=265) Adverse events, % All Gr Gr 3 All Gr Gr 3 Febrile neutropenia Adapted from Mayer et al, NEJM 2015
110 REGO vs TAS: how can we choose? Toxicity profile Previous treatments toxicities Previous treatments efficacy Biomarkers??? COST!!!
111 Recourse trial: Subgroup analysis for OS Mayer et al, NEJM 2015
112 Mayer et al, N Eng J Med 2015 Clinical selection in advanced lines is essential CORRECT Grothey et al, Lancet 2013 RECOURSE TAS-102 mpfs = 2.0 mos Placebo mpfs = 1.7 mos HR= 0.48 (95%CI ) p<0.001
113 How can I optimize the tx of my MCRC pt? Use a comprehensive & carefull approach (clinical & molecular) Plan a strategy Modulate therapy Assess & re-think the strategy DON T BE DOGMATIC, BUT RATHER PRAGMATIC!


114 Grazie per l attenzione! alfredo.falcone@med.unipi.it
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
AIOM GIOVANI Perugia, Luglio 2017
 AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression
 Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
First line treatment in metastatic colorectal cancer
 First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
What to do after 1 st line failure?
 ESMO Preceptorship Programme Colorectal Cancer BARCELONA NOVEMBER, 25-26, 2016 What to do after 1 st line failure? Andrés Cervantes Professor of Medicine mcrc: Howtomaximizesurvival? Improving 1st line
ESMO Preceptorship Programme Colorectal Cancer BARCELONA NOVEMBER, 25-26, 2016 What to do after 1 st line failure? Andrés Cervantes Professor of Medicine mcrc: Howtomaximizesurvival? Improving 1st line
What to do after 1st-line failure in mcrc?
 What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
COMETS: COlorectal MEtastatic Two Sequences
 COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria
 IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
Toxicity by Age Group. Old Factor 1: Age. Disclosures. Predicting survival in metastatic colorectal cancer. Personalized Medicine - Decision Tools -
 Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon cancer: Highlights. Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano
 Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD
 Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
What to do after 1 st line failure?
 ESMO Preceptorship Programme Colorectal Cancer Singapore 20-22 nd 2016 JY Douillard MD PhD ESMO CMO What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy
ESMO Preceptorship Programme Colorectal Cancer Singapore 20-22 nd 2016 JY Douillard MD PhD ESMO CMO What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy
The left versus right colon cancer story What is the truth?
 The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups. Chemotherapy and targeted agents in 1st line
 ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
Fighting a Smarter War On Colon Cancer:
 Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux
 Michel Ducreux") Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
The ESMO consensus conference on metastatic colorectal cancer
 ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC)
") 1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC) Role of the VEGF Pathway in Oncogenesis The Role of Angiogenesis in Cancer Somatic mutation Small avascular tumor Tumor secretion of
1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC) Role of the VEGF Pathway in Oncogenesis The Role of Angiogenesis in Cancer Somatic mutation Small avascular tumor Tumor secretion of
NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO
 Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Medical Therapy of Colorectal Cancer in the Biomarker Era
 Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms
 21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
Antiangiogenic therapy in GI cancer: current status and future directions
 Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Advances in Chemotherapy of Colorectal Cancer
 Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos?
 Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO?
 Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO? Axel Grothey Professor of Oncology Minnesota -> Tennessee The Luxury of So Many Options...
Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO? Axel Grothey Professor of Oncology Minnesota -> Tennessee The Luxury of So Many Options...
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy?
 Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Colon cancer: ASCO poster review. Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome
 Colon cancer: ASCO poster review Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome a.destefano@istitutotumori.na.it 255 poster examined: my selection Clinical Practice Translational &
Colon cancer: ASCO poster review Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome a.destefano@istitutotumori.na.it 255 poster examined: my selection Clinical Practice Translational &
What s New? Dr. Barbara Melosky
 Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
MEETING SUMMARY ASCO GI, SATURDAY JANUARY 17 TH 2015
 Supported by an Independent Educa1onal Grant from MEETING SUMMARY ASCO GI, SATURDAY JANUARY 17 TH 2015 BY DR. GUILLEM ARGILES, BARCELONA, SPAIN Cancers of the Lower GI Tract RAISE: A RANDOMIZED, DOUBLE-BLIND,
Supported by an Independent Educa1onal Grant from MEETING SUMMARY ASCO GI, SATURDAY JANUARY 17 TH 2015 BY DR. GUILLEM ARGILES, BARCELONA, SPAIN Cancers of the Lower GI Tract RAISE: A RANDOMIZED, DOUBLE-BLIND,
Tumors in the Randomized German AIO study KRK-0306
 FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
Ashita Waterston Beatson West of Scotland Cancer Centre
 Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer
 Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
JY Douillard MD, PhD Professor of Medical Oncology
 Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
What to do after 1 st line failure?
 ESMO Preceptorship Programme Colorectal Cancer Valencia 21 st May 2016 What to do after 1 st line failure? Andrés Cervantes ESMO Preceptorship Programme Colorectal Cancer Valencia 21 th May 2016 Dirk Arnold,
ESMO Preceptorship Programme Colorectal Cancer Valencia 21 st May 2016 What to do after 1 st line failure? Andrés Cervantes ESMO Preceptorship Programme Colorectal Cancer Valencia 21 th May 2016 Dirk Arnold,
Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon
 Convegno Nazionale AIOM Giovani 2018 News in Oncology Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon Daniele Rossini U.O. di Oncologia Medica
Convegno Nazionale AIOM Giovani 2018 News in Oncology Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon Daniele Rossini U.O. di Oncologia Medica
Metastatic Colorectal Cancer. Update 2015
 Metastatic Colorectal Cancer Update 2015 A/Prof Jeremy Shapiro GI Medical Oncologist Cabrini Hospital, Melbourne 1 Not all pts with metastatic CRC are equal 1 st consideration can patient be cured by resection
Metastatic Colorectal Cancer Update 2015 A/Prof Jeremy Shapiro GI Medical Oncologist Cabrini Hospital, Melbourne 1 Not all pts with metastatic CRC are equal 1 st consideration can patient be cured by resection
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Kolorektalni karcinom- novosti u liječenju. PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić
 Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER
 RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
MANAGEMENT OF ADVANCED COLORECTAL CANCER
 MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
Targeted therapies in colorectal cancer: the dos, don ts, and future directions
 Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT?
 DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
La strategia terapeutica per il trattamento del carcinoma del colon-retto metastatico
 VI Corso Nazionale Eventi Formativi AIOM-SIAPEC Roma,15 Giugno 2016 La strategia terapeutica per il trattamento del carcinoma del colon-retto metastatico Francesco Di Costanzo Direttore SC Oncologia Medica
VI Corso Nazionale Eventi Formativi AIOM-SIAPEC Roma,15 Giugno 2016 La strategia terapeutica per il trattamento del carcinoma del colon-retto metastatico Francesco Di Costanzo Direttore SC Oncologia Medica
GI SLIDE DECK. Selected abstracts from: 31 May 4 Jun 2013 Chicago, USA ASCO Annual Meeting. 27 Sep 1 Oct 2013 Amsterdam, Netherlands ESMO-ECCO
 GI SLIDE DECK 31 May 4 Jun 2013 Chicago, USA ASCO Annual Meeting 2013 Selected abstracts from: 3 Jul 6 Jul 2013 Barcelona, Spain WCGIC 27 Sep 1 Oct 2013 Amsterdam, Netherlands ESMO-ECCO Supported by Eli
GI SLIDE DECK 31 May 4 Jun 2013 Chicago, USA ASCO Annual Meeting 2013 Selected abstracts from: 3 Jul 6 Jul 2013 Barcelona, Spain WCGIC 27 Sep 1 Oct 2013 Amsterdam, Netherlands ESMO-ECCO Supported by Eli
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
What comes after 1 st line?
 ESMO Preceptorship Programme Colorectal Cancer Valencia 12-13 May 2017 Dirk Arnold Instituto CUF de Oncologia, Lisbon, Portugal What comes after 1 st line? DISCLOSURES Advisory role Bayer, Boehringer,
ESMO Preceptorship Programme Colorectal Cancer Valencia 12-13 May 2017 Dirk Arnold Instituto CUF de Oncologia, Lisbon, Portugal What comes after 1 st line? DISCLOSURES Advisory role Bayer, Boehringer,
/m 2 Oxaliplatin 85 1 Q2W 1-3 Leucovorin Q2W 5-FU Q2W 5-FU Q2W
 癌症診療指引33 Adjuvant therapy of colon cancer mfolfox6 Oxaliplatin 85 1 Q2W 1-3 FOLFOX4 Oxaliplatin 85 1 Q2W 9 Leucovorin 200 1-2 Q2W 5-FU 400 1-2 Q2W 5-FU 600 1-2 Q2W FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin
癌症診療指引33 Adjuvant therapy of colon cancer mfolfox6 Oxaliplatin 85 1 Q2W 1-3 FOLFOX4 Oxaliplatin 85 1 Q2W 9 Leucovorin 200 1-2 Q2W 5-FU 400 1-2 Q2W 5-FU 600 1-2 Q2W FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin
COLORECTAL CANCER: STATE OF THE ART
 COLORECTAL CANCER: STATE OF THE ART Andrés Cervantes Professor of Medicine DECLARATION OF INTERESTS Consulting and advisory services, speaking or writing engagements, public presentations Merck Serono
COLORECTAL CANCER: STATE OF THE ART Andrés Cervantes Professor of Medicine DECLARATION OF INTERESTS Consulting and advisory services, speaking or writing engagements, public presentations Merck Serono
Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical modulation, Oral fluoropyrimidines, Developmentof combination chemotherapy
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
Incorporating biologics in the management of older patients with metastatic colorectal cancer
 Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)
 in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)") Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage. Dr Lee-Ann Jones
 Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
New Options in Metastatic Colorectal Cancer. Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka
 New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
THE BEST OF ESMO 2016
 THE BEST OF ESMO 2016 Colorectal cancer Pr Julien TAIEB, Sorbonne Paris Cité and Paris Descartes University Georges Pompidou European Hospital Paris, FRANCE esmo.org DISCLOSURES JT has received research
THE BEST OF ESMO 2016 Colorectal cancer Pr Julien TAIEB, Sorbonne Paris Cité and Paris Descartes University Georges Pompidou European Hospital Paris, FRANCE esmo.org DISCLOSURES JT has received research
The role of Maintenance treatment Appropriate endpoints according to ESMO consensus
 ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
Annals of Oncology Advance Access published January 18, 2015
 Annals of Oncology Advance Access published January 18, 2015 1 Continuation or reintroduction of bevacizumab beyond progression to first-line therapy in metastatic colorectal cancer: final results of the
Annals of Oncology Advance Access published January 18, 2015 1 Continuation or reintroduction of bevacizumab beyond progression to first-line therapy in metastatic colorectal cancer: final results of the
Treating Liver Limited or Oligometastatic CRC
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Treating Liver Limited or Oligometastatic CRC Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Treating Liver Limited or Oligometastatic CRC Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
How to treat a patient with metastatic CRC? Towards personalized treatment strategies
 How to treat a patient with metastatic CRC? Towards personalized treatment strategies Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Progress in the treatment
How to treat a patient with metastatic CRC? Towards personalized treatment strategies Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Progress in the treatment
Colon Cancer ASCO Poster Review
 Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
What to do after 1 st line failure?
 ESMO Preceptorship Programme Colorectal Cancer Prague July 6-7 th 2016 JY Douillard MD PhD What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy- and selecting
ESMO Preceptorship Programme Colorectal Cancer Prague July 6-7 th 2016 JY Douillard MD PhD What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy- and selecting
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
Management of Patients with Colorectal Cancer
 Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC
 Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
Unresectable or boarderline resectable (Groupp 1) chemotherpy +/- targeted agents
 chemotherpy +/- targeted agents") ESMO Preceptorship Program 27.-28. March Singapore Unresectable or boarderline resectable (Groupp 1) chemotherpy +/- targeted agents Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West
ESMO Preceptorship Program 27.-28. March Singapore Unresectable or boarderline resectable (Groupp 1) chemotherpy +/- targeted agents Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West
Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto
 Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
Traitement de 2ème ligne du cancer colorectal métastatique : nouvelles données cliniques en 2018
 GR DIG 2017 Traitement de 2ème ligne du cancer colorectal métastatique : nouvelles données cliniques en 2018 9 décembre 2017 Benoist Chibaudel Oncologie Médicale Institut Hospitalier Franco-Britannique,
GR DIG 2017 Traitement de 2ème ligne du cancer colorectal métastatique : nouvelles données cliniques en 2018 9 décembre 2017 Benoist Chibaudel Oncologie Médicale Institut Hospitalier Franco-Britannique,
Clinical Spotlight in Metastatic Colorectal Cancer
 2015 European Oncology Congress Clinical Spotlight in Metastatic Colorectal Cancer Featured Research: ESMO Consensus on Metastatic CRC 2015 TRIBE: Cremolini C, et al. Lancet Oncol. 2015 Aug 28. [Epub ahead
2015 European Oncology Congress Clinical Spotlight in Metastatic Colorectal Cancer Featured Research: ESMO Consensus on Metastatic CRC 2015 TRIBE: Cremolini C, et al. Lancet Oncol. 2015 Aug 28. [Epub ahead
RAS and BRAF in metastatic colorectal cancer management
 Review Article RAS and BRAF in metastatic colorectal cancer management Jun Gong 1, May Cho 1, Marwan Fakih 2 1 Department of Medical Oncology, City of Hope National Medical Center, Duarte, CA, USA; 2 Medical
Review Article RAS and BRAF in metastatic colorectal cancer management Jun Gong 1, May Cho 1, Marwan Fakih 2 1 Department of Medical Oncology, City of Hope National Medical Center, Duarte, CA, USA; 2 Medical
Supplementary Online Content
 Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced
Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Adjuvant treatment Colon Cancer
 ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
療指引 34 Adjuvant Therapy of Colon Cancer
 療指引 34 Adjuvant Therapy of Colon Cancer mfolfox6 Oxaliplatin 85 1 Q2W 1~3, 10 FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin 500 1,8,15,22,29,35 Q8W 5-FU 500 1,8,15,22,29,35 Q8W Capecitabine Capecitabine
療指引 34 Adjuvant Therapy of Colon Cancer mfolfox6 Oxaliplatin 85 1 Q2W 1~3, 10 FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin 500 1,8,15,22,29,35 Q8W 5-FU 500 1,8,15,22,29,35 Q8W Capecitabine Capecitabine
Daniele Santini University Campus Bio-Medico Rome, Italy
 Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
XXV Corso Nazionale TSLB: evoluzione o ri(e)voluzione?
voluzione?") XXV Corso Nazionale TSLB: evoluzione o ri(e)voluzione? Marcatori predittivi di efficacia nel carcinoma del colon: DESTRO verso SINISTRO conta? Dott. Matteo Clavarezza S.C. Oncologia Medica RAS metastatic
XXV Corso Nazionale TSLB: evoluzione o ri(e)voluzione? Marcatori predittivi di efficacia nel carcinoma del colon: DESTRO verso SINISTRO conta? Dott. Matteo Clavarezza S.C. Oncologia Medica RAS metastatic
Evaluation of SIRFLOX Study Results. Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany
 Evaluation of SIRLX Study Results Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany ESM Guideline: Response is a Goal of Treatment Performance Status of the
Evaluation of SIRLX Study Results Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany ESM Guideline: Response is a Goal of Treatment Performance Status of the
P < vs. 5FU/LV LD 0% 60.0% 3.6 months P < P = 0.113
 in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES
 CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli