The Role of Radiation in the Management of Gynecologic Cancers. Scott Glaser, MD
|
|
|
- Lionel Dean
- 5 years ago
- Views:
Transcription
1 The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD
2 Nothing to disclose DISCLOSURE
3 Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical Cancer Post-operative for early stage Definitive for locally advanced Vaginal Cancer Vulvar Cancer Ovarian Cancer
4 Endometrial Cancer Most common presenting symptom is post-menopausal bleeding Ultrasound performed and demonstrates thickened endometrial stripe (>4mm) Endometrial biopsy performed If positive, complete work-up and proceed to surgery
5 Endometrial Cancer Surgically managed disease Total hysterectomy with regional lymph node evaluation is the first step in management Growing role of SLNBx Staging largely dependent upon surgical findings Risk of recurrence is dependent upon stage and histology Guides adjuvant therapy recommendations

6 Endometrial Cancer

7 Endometrial Cancer Epithelial Type 1 (AKA Endometrioid adenocarcinoma): Most common histology is endometrioid adenocarcinoma ~80% of endometrial cancer Type 2 (serous, clear cell, carcinosarcoma [MMMT])


8 Endometrial Cancer <5% >10-40% >15% if deep invasion + Gr2-3
9 Endometrial Cancer Stage 1 What are the most common sites of recurrence: Vaginal cuff 10% (~75% of LRR) Pelvic lymph nodes 4% Distant 7%
10 Endometrial Cancer Stage 1 How can we reduce this risk? Portec 1 GOG 99 Portec 2
11 Endometrial Cancer Stage 1 What predicts for locoregional recurrence? GOG 99 (had LN dissection) Portec 1 (No LN dissection) Outer 1/3 myometrial invasion Outer 1/2 myometrial invasion Grade 2 or 3 Grade 3 LVSI Age >60 Patients classified as High-Intermediate Risk if: GOG: Age> RF, Age RF, Age<50 and 3 RF Portec: 2/3 Risk Factors 20-25% risk of LRR in HIR group
12 Endometrial Cancer Stage 1 PORTEC 1 & GOG 99 Post Op pelvic EBRT vs Obs Intermediate Risk decreased LRR from 12-14% to 3-4% High-Intermediate Risk Decreased LRR from 18-26% to 5-6% Low-Intermediate Risk Decreased LRR from 5-6% to 2% Site of locoregional relapse ~75% vaginal
13 Endometrial Cancer Stage 1 Portec 2 Phase III Randomized Trial EBRT vs VBT Population H-I Risk Patients Primary endpoint vaginal relapse Non-inferiority

14 Endometrial Cancer What is vaginal brachytherapy?

15 Endometrial Cancer
16 Endometrial Cancer Vaginal Brachytherapy Acute Toxicity Gastrointestinal - 12% grade 1 or 2 Late Toxicity Gastrointestinal - <1% grade 3 Vaginal atrophy 2% grade 3 Most studies describe late toxicity rate of 1-5% Do all patients need radiation? Sorbe et al, (Int J Gynecol Cancer, 2009) N=645, IA G1-2, Randomized VBT or Obs Vaginal recurrence rate of 3.1% vs. 1.2% (NS)
17 Endometrial Cancer Primary Risk Factors Age >60, LVSI, and/or large tumor size Risk Group Observation VBT Authors Recommendation Non-invasive, Gr 1-2 Non-invasive Gr Low 0-2% [5,67] + Low 0-2% [5,67] 0-1% Observation 0-1% Observation <1/2 MMI - Low-Int 3-4% 0-2% Observation Gr 1-2 [3,4,7,22] [22,30] OR Referral to radiation oncology <1/2 MMI, Gr Low-Int 5-6% [3,4,7] 0-2% Referral to radiation oncology OR [22,30] non-invasive Gr 3 +/- >1/2 MMI, Gr Int 8-10% 0-3% VBT OR [3,4,7] [18,29] <1/2 MMI, Gr 3 - >1/2 MMI, Gr 1-2 OR + High-Int 13-19% [3,4,7] 2-3% [28,29] VBT, but consider EBRT based on risk factors & nodal dissection <1/2 MMI, Gr 3 +
18 Endometrial Cancer
19 Endometrial Cancer Stage 2 Stage II Stage II Rare presentation Data limited primary to retrospective reviews Brachy or EBRT both reasonable depending on grade and extent of disease
20 Endometrial Cancer Stage 2 Harkenrider et al. (Int J Radiat Oncol Biol Phys, 2018) Multi-institutional analysis (7 institutions) Endometrioid Type Stage II treated with Adjuvant Vaginal Brachytherapy alone (N=92) Median follow up 39.0 months Surgery 98% had total hysterectomy, 2% radical hysterectomy 88% had pelvic lymph nodes removed 90% G1-2 98% had microscopic cervical involvement 5 year vaginal and pelvic failure rate 2.6% and 4.2%, respectively 5 year risk of distant failure was 7.2%
21 Endometrial Cancer Stage 3 Stage IIIA-B Similar to stage II, relatively rare with individualized therapy Stage IIIC (LN+) Historically managed with combination of radiation (EBRT +/- brachytherapy) and/or chemotherapy GOG 122: Chemo alone better than EBRT alone Recent trials have sought to better define the role of both chemotherapy and radiotherapy Portec 3: RT+/- Chemo GOG 258: Chemo +/- RT
22 Endometrial Cancer Stage 3 Portec patients with FIGO II-III endometrial or I-III Serous/Clear Randomized to RT or Chemo-RT (concurrent Cis, Adj Carbo/taxol x4)
23 Endometrial Cancer All Pts Stage III
24 Endometrial Cancer Stage 3 GOG 258 (ASCO 2017) 733 pts, stage III-IVa endometrioid, stage I-II serous/clear Randomized to Chemo (Carbo/Taxol x6) or Chemo-RT (concurrent Cis, Adj Carbo/taxol x4) 5-yr outcomes Vaginal Recurrence 7% vs 3% Pelvic/PA Recurrence 19% vs 10% Distant Recurrence 21% vs 27% Awaiting Final Publication

25 Endometrial Cancer How is EBRT delivered?

26 Endometrial Cancer
27 Endometrial Cancer Medically Inoperable Radiation can offer long term cure Brachytherapy alone for small/superficial tumors EBRT + Brachy for larger/deeper tumors



28 Endometrial Cancer

29 Cervical Cancer Present with abnormal pap smear or vaginal bleeding Very strong association with HPV Vaccine against HPV available Pelvic exam demonstrates cervical dysplasia or mass
30 Cervical Cancer Biopsy performed Cervical cancer is staged clinically goal is to have staging applied similarly in developing world still, PET/CT and MRI of the pelvis are routinely part of work-up and help guide treatment decisions in the developed world Staging

31 Cervical Cancer
32 Cervical Cancer Early Stage (IA, IB1, IIA1) Surgery typically indicated Extent of surgery dependent upon stage and size Small tumors may be amenable to fertility sparing procedure Larger tumors require hysterectomy with extent dependent upon size/stage Adjuvant therapy dependent upon surgical findings Locally Advanced (1B2, IIA2, IIB or higher, LN+) Non-operative management preferred External Beam Radiation with Concurrent Chemotherapy followed by Brachytherapy (Internal Radiation)
; OS NS Consider for adeno or with 1 RF, had large reduction in recurrence (8% vs.")
33 Cervical Cancer Early Stage GOG 92 (Sedlis) Early stage, intermediate risk: LVSI Deep 1/3 stromal invasion >4cm tumor Stage IB tx d with rad hyst, LN-, margin- 2 factors Obs vs WP Gy RT improved LC (79 86%); OS NS Consider for adeno or with 1 RF, had large reduction in recurrence (8% vs. 44%)
34 Cervical Cancer Early Stage GOG 109 (Peters) Early stage, high risk: + Margin + LN + Parametria IA2-IIA w/ LN+, +margin or +parametria after RH/PLND WP 49.3/29 (1.7/fx, 45 PA if common iliac +) +/- cis/5fu q3wk x4c (2 concurrent, 2 adjuvant) CRT improved OS (71 81%) vs. RT CRT improved LC (79 91%) vs. RT
35 Cervical Cancer Early Stage How is adjuvant RT given? Pelvic EBRT very similar to endometrial cancer Brachytherapy not routinely performed
36 Cervical Cancer Higher Stage Landoni Trial N=469 with IB or IIA cervical CA RCT EBRT+LDR vs. Surgery Surgery: class III radhys +/- adj XRT if high-risk (pt2b+, <3mm safe cervical stroma, cut-through, or +LN) RT: Gy in Gy/fx to pelvis and intracavitary brachy (pt A Gy) Outcomes same: 5y OS 83%, DFS 74%, recurrence ~25% Gr 2-3 toxicity worse with S: 28% (vs. 12% RT) 54% of IB1 and 84% of IB2 needed RT (in S arm) Maybe IB2 should just get CRT
37 Cervical Cancer How is radiation performed for locally advanced cervical cancer? 45 Gy of EBRT in 25 fractions Involved lymph nodes treated to Gy in 25 fractions EBRT is combined with concurrent chemo Most commonly weekly Cisplatin Toward the end of EBRT brachytherapy is initiated Goal of finishing all treatment in less than 8 weeks Improves control rates
38 Cervical Cancer What are the types of brachytherapy used for cervical cancer? Intracavitary vs interstitial Depends on extent of disease Intracavitary applicators include Tandem and ovoids Ring and tandem Indications for interstitial Extensive lateral spread of tumor (>2-3 cm from midline at time of brachytherapy) Distal vaginal involvement Anatomic inability to place intracavitary applicator


39 Cervical Cancer

40 Cervical Cancer Radiotherapy and Oncology, Volume 78, Issue 1, January 2006, Pages 67-77


41 Cervical Cancer


42 Cervical Cancer How is intracavitary brachytherapy preformed? Conscious sedation or general anesthesia for insertion Paracervical block (local anesthesia) Ultrasound guidance for tandem placement Time from applicator insertion to treatment delivery is about 3-4 hours

43 Cervical Cancer





44 Cervical Cancer
45 Cervical Cancer How is interstitial brachytherapy preformed? OR with general anesthesia and epidural Patient admitted to hospital for 2-3 nights Needles stay in place for 2.5 days Five fractions of radiation One on day of procedure, two per day the next two days Applicator comes out in radiation department after 5 th fraction Epidural is discontinued Patient discharged

46 Cervical Cancer

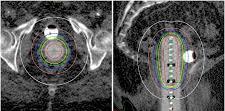
47 Cervical Cancer Needle placement is iterative process done with CT guided adjustment Pre adjustment Post adjustment


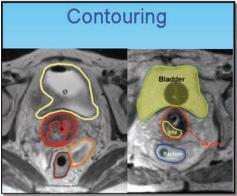
48 Cervical Cancer Contouring Target and organs at risk (OAR)
49 Cervical Cancer Date 11/21/17 11/30/17 12/03/17 12/07/17 12/10/17 External Beam Dose Prescribed Dose Pt.A Bladder 0.1cc Dose Bladder 1cc Dose Bladder 2cc Dose Dose Bladder 5cc Dose Rectum 0.1cc Dose Rectum 1cc Dose Rectum 2cc Dose Rectum 5cc Dose Sigmoid 0.1cc Dose Sigmoid 1cc Dose Sigmoid 2cc Dose Sigmoid 5cc Dose HR CTV D IR CTV D GTV D

50 Cervical Cancer Hybrid Intracavitary Interstitial Applicators Bulky disease, especially residual medial parametria and asymmetric disease
51 Vaginal Cancer Primary cancer of the vagina is rare (2% of gyn cancer) Majority are squamous cell Cannot involve vulva or cervix By definition if a cancer involves both the vagina and either the vulva or the cervix, it is treated as a cervical cancer or a vulvar cancer, not a vaginal cancer More common than primary vaginal cancer is vaginal recurrence of other gynecological cancers Most commonly endometrial cancer Salvage rate 50%
52 Vaginal Cancer Treatment Surgery can be considered for small superficial lesions Most frequently treated with definitive radiation +/- chemo
53 Vaginal Cancer 193 patients from
54 Vaginal Cancer
55 Vaginal Cancer

56 Vaginal Cancer

57 Vaginal Cancer



58 Vaginal Cancer
59 Vulvar Cancer Presents as vulvar mass/lesion Primary risk factors include HPV and Lichen Sclerosis Management Upfront surgical management for small tumors (< 4cm) not involving critical structures Partial vulvectomy and lymph node evaluation (SLNBx typically) Adjuvant RT based on pathological risk factors Neoadjuvant Chemo-RT for borderline resectable tumors Definitive Chemo-RT for unresectable tumors.
60 Vulvar Cancer FIGO Staging IA: <2cm AND <1.0mm stromal invasion IB: larger, but still in vulva/perineum II: Distal 1/3 urethra, vaginal, or anal involvement III: LN positive, NO relation to T stage N1 IIIA, N2 IIIB, but ECE = IIIC IVA: Fixed/ulcerated LN, or more extensive locally
61 Vulvar Cancer - Postop Heaps (1990) SM >=8mm = 0% RR SM < 8mm = 48% RR Other predictors for recurrence: DOI >9mm Tumor thickness > 1cm Infiltrative (rather than pushing border) LVI+ Increased keratin >10mm Indications for adjuvant RT to primary Close margins <8mm Tumor Size DOI > 5-9mm + LVSI For Lymph nodes: If LNs not evaluated SLN+ After LND+, if >1 LN+, >2 5mm metastasis, or ECE >=20% ratio of ipsilateral LN+ Consider chemotherapy
62 Vulvar Cancer - Postop Faul, 1997, retrospective 62 pts w/ <8mm margin, 31 tx w/ RT to vulva LR in 58% of observed, 16% of RT group Viswanathan, 2013, retrospective 205 pts, margin status re-quantified Negative >1=cm (34%), close <1cm (56%), positive (10%) All treated with RT to Vulva +/- inguinal nodes, 2D Highest risk with margins <=5mm Radiation dose >=56Gy had lower relapse risk than <=50.4Gy
63 Vulvar Cancer Post op GOG 37 Adjuvant RT for LN+ Ipsilateral Pelvic LN dissection vs B/L inguinal/pelvic RT 45-50Gy No RT to vulva Radiation Improved: 2-yrs OS 54 vs 68%, Groin failures 24 vs 5% (SS) Vulvar recurrence similar (9%) Subset analyses Worse survival with surgery if cn+ or >=2LNs No difference between RT and PLND if single LN+
64 Vulvar Cancer - Advanced GOG 205 Phase II Unresectable T3/T4, any N, 58 pts 1.8Gy/fx qd w/ weekly cisplatin, followed by resection N0 - RT to primary (groin at discretion of MD) N+ - Vulva, inguinofemoral, lower pelvic LNs ccr in 37/58 (64%) 29 had PCR (78% of ccr, 50% of total) GOG 279 Ongoing, increase RT dose to 64 Gy and add Gemcitabine
65 Vulvar Cancer GRONISS-V II Prospective study currently in progress < 4cm confined to Vulva Initial Protocol If SLNB-, no further therapy If SLNB+, randomized to: Adjuvant RT (w/ chemo at discretion) Completion of superficial and deep inguinofemoral LND Interim safety monitoring showed high rate of in-field groin failures (20% in macromets, 2% in micromets) Protocol changed to mandate dissection followed by adjuvant RT in all LN dz > 2mm size Micromets still randomized
66 Ovarian Cancer Radiation is not typically used in ovarian cancer Treatment consists primarily of surgery and chemotherapy In rare case, radiation is considered Pelvic/periaortic LN recurrence/persistence despite systemic therapy in the absence of other metastatic disease Data

67 Ovarian Cancer 102 patients with epithelial ovarian cancer treated with RT to a dose of 45 Gy or more 50% nodal recurrence, 50% extranodal
68 Ovarian Cancer
69 Ovarian Cancer
70 Conclusions In early stage endometrioid adenocarcinoma, the most common site of recurrence is the vaginal cuff forming the rationale for vaginal cuff brachytherapy For locally advanced cervical cancer, the preferred treatment is non-operative, including EBRT with concurrent chemotherapy followed by brachytherapy Adjuvant radiation therapy for node positive vulvar cancer improves both locoregional control and overall survival Radiation therapy is not commonly used in ovarian cancer
71 Thank You
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Janjira Petsuksiri, M.D
 GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
17 th ESO-ESMO Masterclass in clinical Oncology
 17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
receive adjuvant chemotherapy
 Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
ESGO-ESTRO-ESP Cervical Cancer Clinical Practice Guidelines Management of early stages: algorithms focusing on the histological data
 ESGO-ESTRO-ESP Cervical Cancer Clinical Practice Guidelines Management of early stages: algorithms focusing on the histological data David Cibula Gynecologic Oncology Centre General University Hospital
ESGO-ESTRO-ESP Cervical Cancer Clinical Practice Guidelines Management of early stages: algorithms focusing on the histological data David Cibula Gynecologic Oncology Centre General University Hospital
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Advances in Gynecologic Brachytherapy
 Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Basics of Cervix Cancer Brachytherapy
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre)
") ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Staging. Carcinoma confined to the corpus. Carcinoma confined to the endometrium. Less than ½ myometrial invasion. Greater than ½ myometrial invasion
 5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
ARRO Case: Early-stage Endometrial Cancer
 ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Risk group criteria for tailoring adjuvant treatment in patients with endometrial cancer : a validation study of the GOG criteria
 Risk group criteria for tailoring adjuvant treatment in patients with endometrial cancer : a validation study of the GOG criteria Suk-Joon Chang, MD, Hee-Sug Ryu MD Gynecologic Cancer Center Department
Risk group criteria for tailoring adjuvant treatment in patients with endometrial cancer : a validation study of the GOG criteria Suk-Joon Chang, MD, Hee-Sug Ryu MD Gynecologic Cancer Center Department
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Interstitial Brachytherapy. Low dose rate brachytherapy. Brachytherapy alone cures some cervical cancer. Learning Objectives
 Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Endometrial Cancer. Incidence. Types 3/25/2019
 Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva Malignant melanoma sho
 Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
Quimio Radioterapia en Cancer de Cervix
 Quimio Radioterapia en Cancer de Cervix HIGINIA R. CÁRDENES PROFESSOR RADIATION ONCOLOGY CLINICAL DIRECTOR SCHNECK CANCER CENTER Worldwide incidence of cervical cancer 2014, 12.360 cases Global incidence
Quimio Radioterapia en Cancer de Cervix HIGINIA R. CÁRDENES PROFESSOR RADIATION ONCOLOGY CLINICAL DIRECTOR SCHNECK CANCER CENTER Worldwide incidence of cervical cancer 2014, 12.360 cases Global incidence
University of Kentucky. Markey Cancer Center
 University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
Management of high risk early cervical cancer - a view of surgeon Dan DY Kim, M.D., Ph.D.
 Management of high risk early cervical cancer - a view of surgeon Dan DY Kim, M.D., Ph.D. Department of Obstetrics and Gynecology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea
Management of high risk early cervical cancer - a view of surgeon Dan DY Kim, M.D., Ph.D. Department of Obstetrics and Gynecology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea
Patterns of Care in Patients with Cervical Cancer:
 Patterns of Care in Patients with Cervical Cancer: Power and Pitfalls of Claims-Based Analysis Grace Smith, MD, PhD, MPH Resident, PGY-5 Department of Radiation Oncology, MD Anderson Cancer Center Acknowledgments
Patterns of Care in Patients with Cervical Cancer: Power and Pitfalls of Claims-Based Analysis Grace Smith, MD, PhD, MPH Resident, PGY-5 Department of Radiation Oncology, MD Anderson Cancer Center Acknowledgments
surgical staging g in early endometrial cancer
 Risk adapted d approach to surgical staging g in early endometrial cancer Leon Massuger University Medical Centre St Radboud Nijmegen, The Netherlands Doing nodes Yes Yes Yes No No No 1957---------------------------
Risk adapted d approach to surgical staging g in early endometrial cancer Leon Massuger University Medical Centre St Radboud Nijmegen, The Netherlands Doing nodes Yes Yes Yes No No No 1957---------------------------
GCIG Rare Tumour Brainstorming Day
 GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
A phase II study of weekly paclitaxel and cisplatin followed by radical hysterectomy in stages IB2 and IIA2 cervical cancer AGOG14-001/TGOG1008
 A phase II study of weekly paclitaxel and cisplatin followed by radical hysterectomy in stages IB2 and IIA2 cervical cancer AGOG14-001/TGOG1008 NCT02432365 Chyong-Huey Lai, MD On behalf of Principal investigator
A phase II study of weekly paclitaxel and cisplatin followed by radical hysterectomy in stages IB2 and IIA2 cervical cancer AGOG14-001/TGOG1008 NCT02432365 Chyong-Huey Lai, MD On behalf of Principal investigator
PET/CT in Gynaecological Cancers. Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp
 PET/CT in Gynaecological Cancers Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp Cervix cancer Outline of this talk Initial staging Treatment monitoring/guidance
PET/CT in Gynaecological Cancers Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp Cervix cancer Outline of this talk Initial staging Treatment monitoring/guidance
New Cancer Cases By Site Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3%
 Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Algorithms for management of Cervical cancer
 Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
Gynecological Cancers in Primary Care
 Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer
 THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
NAACCR Webinar Series /7/17
 COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Linking DVH-parameters to clinical outcome. Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria
 Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
ENDOMETRIAL CANCER. Endometrial cancer is a great concern in UPDATE. For personal use only. Copyright Dowden Health Media
 For mass reproduction, content licensing and permissions contact Dowden Health Media. UPDATE ENDOMETRIAL CANCER Are lymphadenectomy and external-beam radiotherapy valuable in women who have an endometrial
For mass reproduction, content licensing and permissions contact Dowden Health Media. UPDATE ENDOMETRIAL CANCER Are lymphadenectomy and external-beam radiotherapy valuable in women who have an endometrial
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
EMBRACE- Studien Analysen und Perspektiven
 EMBRACE- Studien Analysen und Perspektiven Alina Sturdza EMBRACE study group Outline Historical development of GEC ESTRO Gyn Group Historical development of the MRI compatible applicators Presentation
EMBRACE- Studien Analysen und Perspektiven Alina Sturdza EMBRACE study group Outline Historical development of GEC ESTRO Gyn Group Historical development of the MRI compatible applicators Presentation
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Study Title The SACS trial - Phase II Study of Adjuvant Therapy in CarcinoSarcoma of the Uterus
 Study Title The SACS trial - Phase II Study of Adjuvant Therapy in CarcinoSarcoma of the Uterus Investigators Dr Bronwyn King, Peter MacCallum Cancer Centre Dr Linda Mileshkin, Peter MacCallum Cancer Centre
Study Title The SACS trial - Phase II Study of Adjuvant Therapy in CarcinoSarcoma of the Uterus Investigators Dr Bronwyn King, Peter MacCallum Cancer Centre Dr Linda Mileshkin, Peter MacCallum Cancer Centre
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Case Scenario 1. History
 History Case Scenario 1 A 53 year old white female presented to her primary care physician with post-menopausal vaginal bleeding. The patient is not a smoker and does not use alcohol. She has no family
History Case Scenario 1 A 53 year old white female presented to her primary care physician with post-menopausal vaginal bleeding. The patient is not a smoker and does not use alcohol. She has no family
GCIG Cervix Committee: Chicago, USA May 30th Satoru Sagae (JGOG) Bradley Monk (GOG)
 Bradley Monk (GOG)") GCIG Cervix Committee: Chicago, USA May 30th 2013 Satoru Sagae (JGOG) Bradley Monk (GOG) Conflict of Interest Disclosures CURRENT ACTIVE/NEAR ACTIVATION RANDOMIZED TRIALS WITH GCIG PARTICIPATION: Wellcome
GCIG Cervix Committee: Chicago, USA May 30th 2013 Satoru Sagae (JGOG) Bradley Monk (GOG) Conflict of Interest Disclosures CURRENT ACTIVE/NEAR ACTIVATION RANDOMIZED TRIALS WITH GCIG PARTICIPATION: Wellcome
Type I. Type II. Excess estrogen Lynch Endometrioid adenocarcinoma PTEN. High grade More aggressive Serous, Clear Cell p53
 Type I Excess estrogen Lynch Endometrioid adenocarcinoma PTEN Type II High grade More aggressive Serous, Clear Cell p53 Stage I IA IB Stage II Stage III IIIA IIIB IIIC IIIC1 IIIC2 Stage IV IVA IVB nodes
Type I Excess estrogen Lynch Endometrioid adenocarcinoma PTEN Type II High grade More aggressive Serous, Clear Cell p53 Stage I IA IB Stage II Stage III IIIA IIIB IIIC IIIC1 IIIC2 Stage IV IVA IVB nodes
3/25/2019. Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates
 Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates") J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
Cervical Cancer: 2018 FIGO Staging
 Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
Challenging Cases in Cervical Cancer: Parametrial Boosting. Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin
 Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
Gynecologic Cancer InterGroup Cervix Cancer Research Network. The SHAPE Trial
 Gynecologic Cancer InterGroup Cervix Cancer Research Network The SHAPE Trial Comparing radical hysterectomy and pelvic node dissection against simple hysterectomy and pelvic node dissection in patients
Gynecologic Cancer InterGroup Cervix Cancer Research Network The SHAPE Trial Comparing radical hysterectomy and pelvic node dissection against simple hysterectomy and pelvic node dissection in patients
Correlation of intermediate risk factors with prognostic factors in patients with early cervical cancer
 대한부인종양콜포스코피학회제 24 차학술대회 Correlation of intermediate risk factors with prognostic factors in patients with early cervical cancer Seoul National University Bundang Hospital Eun Jung Soh, M.D. Cervical cancer
대한부인종양콜포스코피학회제 24 차학술대회 Correlation of intermediate risk factors with prognostic factors in patients with early cervical cancer Seoul National University Bundang Hospital Eun Jung Soh, M.D. Cervical cancer
Outline - MRI - CT - US. - Combinations of imaging modalities for treatment planning
 Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
SLN Mapping in Cervical Cancer. Memorial Sloan Kettering Cancer Center New York, USA
 Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK
 Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
HYPERTHERMIA in CERVIX and VAGINA CANCER. J. van der Zee
 HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix
HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix
3/25/2019. J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse
 J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
New NCCN Guidelines for Vulvar Cancer
 New NCCN Guidelines for Vulvar Cancer Benjamin E. Greer, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance Vulvar Cancer Objectives: 1) Overview of vulvar carcinoma and FIGO staging.
New NCCN Guidelines for Vulvar Cancer Benjamin E. Greer, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance Vulvar Cancer Objectives: 1) Overview of vulvar carcinoma and FIGO staging.
Endometrial Cancer. Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines
 Gynecological Cancer Treatment Guidelines") Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
Rochester Minnesota Mayo Clinic
 Are There Still Indications for Lymphadenectomy in Endometrial Cancer? A Mariani Mayo Clinic Rochester - MN USA Rochester Minnesota Mayo Clinic 1 Endometrial Cancer Lymphadenectomy Yes or No? Endometrial
Are There Still Indications for Lymphadenectomy in Endometrial Cancer? A Mariani Mayo Clinic Rochester - MN USA Rochester Minnesota Mayo Clinic 1 Endometrial Cancer Lymphadenectomy Yes or No? Endometrial
Chapter 8 Adenocarcinoma
 Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Gynecologic Malignancies. Kristen D Starbuck 4/20/18
 Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
Radiotherapy of Gynecological Malignancies
 Radiotherapy of Gynecological Malignancies Felipe A. Calvo Hospital General Universitario Gregorio Marañon Madrid, Spain ESO-ESMO Latin-American Masterclass Bogotá, Colombia April 2016 Radiotherapy of
Radiotherapy of Gynecological Malignancies Felipe A. Calvo Hospital General Universitario Gregorio Marañon Madrid, Spain ESO-ESMO Latin-American Masterclass Bogotá, Colombia April 2016 Radiotherapy of
Recent Advances and current status of radiotherapy for cervix cancer
 Recent Advances and current status of radiotherapy for cervix cancer Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 24, 2017 Recent
Recent Advances and current status of radiotherapy for cervix cancer Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 24, 2017 Recent
Role of Surgery in Cervical Cancer & Research Questions
 Role of Surgery in Cervical Cancer & Research Questions Arb-aroon Lertkhachonsuk, M.D., Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Role of surgery in cervical cancer
Role of Surgery in Cervical Cancer & Research Questions Arb-aroon Lertkhachonsuk, M.D., Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Role of surgery in cervical cancer
INTRODUCTION PATIENT. J. Radiat. Res., 52, (2011)
") J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
Chapter 5 Stage III and IVa disease
 Page 55 Chapter 5 Stage III and IVa disease Overview Concurrent chemoradiotherapy (CCRT) is recommended for stage III and IVa disease. Recommended regimen for the chemotherapy portion generally include
Page 55 Chapter 5 Stage III and IVa disease Overview Concurrent chemoradiotherapy (CCRT) is recommended for stage III and IVa disease. Recommended regimen for the chemotherapy portion generally include
Uterus Malignancies /5/15
 Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
CARCINOMA CERVIX. Dr. PREETHI REDDY. B. M S OBG II yr POST GRADUATE.
 CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
Evolving Treatment Strategies for Cervical Cancer
 Evolving Treatment Strategies for Cervical Cancer Nadeem Abu-Rustum, MD Memorial Sloan Kettering Cancer Center Evolving Treatment Strategies 1. Surgery 2. Radiation 3. Chemotherapy Incidence of cervix
Evolving Treatment Strategies for Cervical Cancer Nadeem Abu-Rustum, MD Memorial Sloan Kettering Cancer Center Evolving Treatment Strategies 1. Surgery 2. Radiation 3. Chemotherapy Incidence of cervix
Should the Optimal Adjuvant Treatment for Patients With Early-Stage Endometrial Cancer With High-Intermediate Risk Factors Depend on Tumor Grade?
 ORIGINAL STUDY Should the Optimal Adjuvant Treatment for Patients With Early-Stage Endometrial Cancer With High-Intermediate Risk Factors Depend on Tumor Grade? Chunyan Lan, MD,* Xin Huang, MD,* Qidan
ORIGINAL STUDY Should the Optimal Adjuvant Treatment for Patients With Early-Stage Endometrial Cancer With High-Intermediate Risk Factors Depend on Tumor Grade? Chunyan Lan, MD,* Xin Huang, MD,* Qidan
MSRO35-01 MSRO35-02 MSRO MSRO35 BOOST: Gynecology Integrated Science and Practice (ISP) Session. Participants. Sub-Events
 Session. Participants. Sub-Events") MSRO35 BOOST: Gynecology Integrated Science and Practice (ISP) Session Multisession Courses RO OI GU AMA PRA Category 1 Credits : 1.50 ARRT Category A+ Credits: 1.50 Tue, Dec 2 10:30 AM - 12:00 PM Location:
MSRO35 BOOST: Gynecology Integrated Science and Practice (ISP) Session Multisession Courses RO OI GU AMA PRA Category 1 Credits : 1.50 ARRT Category A+ Credits: 1.50 Tue, Dec 2 10:30 AM - 12:00 PM Location:
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
ROLE OF RADIOTHERAPY IN CERVICAL AND ENDOMETRIAL CANCER
 ROLE OF RADIOTHERAPY IN CERVICAL AND ENDOMETRIAL CANCER Vesna Plesinac Karapandzic Instutute of Oncology and Radiology of Serbia ESO BELGRADE 2017 Introduction Radiotherapy (RT) in gynaecological cancer
ROLE OF RADIOTHERAPY IN CERVICAL AND ENDOMETRIAL CANCER Vesna Plesinac Karapandzic Instutute of Oncology and Radiology of Serbia ESO BELGRADE 2017 Introduction Radiotherapy (RT) in gynaecological cancer
University Cooperation Platform
 Starting a Brachytherapy Program in Government Controlled Healthcare Systems Razvan Galalae, MD, PhD Associate Professor, Medical Faculty, Christian Albrecht University Kiel, Germany, and Head of Radiotherapy
Starting a Brachytherapy Program in Government Controlled Healthcare Systems Razvan Galalae, MD, PhD Associate Professor, Medical Faculty, Christian Albrecht University Kiel, Germany, and Head of Radiotherapy
Invasive Cervical Cancer: Squamous Cell, Adenocarcinoma, Adenosquamous
 Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
2016 Uterine Cancer Annual Report
 2016 Uterine Cancer Annual Report Overview At Carolinas HealthCare System s Levine Cancer Institute, we offer comprehensive care focused on using the latest technology and innovative techniques in the
2016 Uterine Cancer Annual Report Overview At Carolinas HealthCare System s Levine Cancer Institute, we offer comprehensive care focused on using the latest technology and innovative techniques in the
Management of Cervical Cancer in Resource Limited Settings
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD MPH MS Professor, Gynecologic Oncology Icahn School of Medicine at Mount Sinai New York NY 84% of incidence and death occur in
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD MPH MS Professor, Gynecologic Oncology Icahn School of Medicine at Mount Sinai New York NY 84% of incidence and death occur in
GCIG Cervix Committee: Chicago William Small Jr. Satoru Sagae Bradley Monk
 GCIG Cervix Committee: Chicago 2012 William Small Jr. Satoru Sagae Bradley Monk Conflict of Interest Disclosures Closed Trials GOG 240 and Active Trials Gynecologic Oncology Group Cervical Cancer Update
GCIG Cervix Committee: Chicago 2012 William Small Jr. Satoru Sagae Bradley Monk Conflict of Interest Disclosures Closed Trials GOG 240 and Active Trials Gynecologic Oncology Group Cervical Cancer Update