Endoscopic band ligation (EBL) is the most effective and
|
|
|
- Mercy Gibson
- 5 years ago
- Views:
Transcription
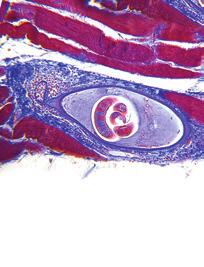
1 CURRENT ENDOSCOPIC PRACTICES THE EXPERTS SPEAK Endoscopic band ligation for nonvariceal bleeding: A review Sergio Zepeda-Gómez MD 1, Norman E Marcon MD FRCPC 2 Endoscopic band ligation (EBL) is the most effective and accepted treatment for acute esophageal variceal bleeding (1). EBL is an easy and safe method to achieve hemostasis for gastrointestinal (GI) bleeding, in contrast to other endoscopic therapies (thermal, mechanical, injection). The use of EBL for other types of bleeding in the GI tract has been published mostly as case report series (Table 1). In the present review, we describe the results of published studies that have evaluated different options for EBL in the setting of nonvariceal bleeding. VASCULAR LESIONS IN THE GI TRACT Vascular malformations may cause chronic blood loss or acute GI hemorrhage. These lesions, often called angiodysplasias or vascular ectasias, are single or multiple bright red round spots of variable diameter with uniform or slightly irregular margins. These can present independently or in association with other conditions such as radiation injury, collagen vascular disease, chronic renal failure, cirrhosis or hereditary hemorrhagic telangiectasia, and they account for 1% to 5% of all causes of GI bleeding reported (2) (Figure 1). Treatment of vascular lesions with EBL has been reported to be effective. Wong et al (3) described two patients with GI bleeding secondary to gastric angiodysplasia successfully treated with EBL, one of them previously treated with pure ethanol injection. Furthermore, Abi-Hanna et al (4) described 10 patients with vascular lesions in the stomach and duodenum successfully treated with EBL. Four of the patients had previous endoscopic therapy and four had active bleeding at the time of ligation therapy. No rebleeding was observed at a mean follow-up time of six months. In another prospective study that evaluated treatment of vascular lesions in the small bowel (5), a cohort of patients with upper GI bleeding were investigated and 14 patients with angiodysplasias were identified. These lesions were located in the duodenal bulb (n=5), the second portion of the duodenum (n=8) and the third portion of the duodenum (n=1). All patients were treated with EBL and hemostasis was achieved in a single endoscopic session. No patients had further bleeding at 40 days of follow-up. DIEULAFOY LESION A Dieulafoy lesion (DL) is a large-calibre, tortuous artery that is located in the submucosa in close contact with the mucosa. The erosion of the mucosa and arterial wall can initiate massive bleeding. The majority of these lesions are located in the gastric fundus. DLs represent approximately 0.3% to 6% of all causes of GI bleeding (6). Several reports and series on endoscopic treatment for DLs have been published. Most DLs have been treated by thermal or injection methods, or hemoclipping (7-12). The initial success rate reported for hemostasis with these methods was 84% and 90% in two different studies that included 26 and 40 patients, respectively (7,8). The first use of EBL for the treatment of a gastric DL was reported in 1994 (13). Since then, there has been a trend to treat these lesions with EBL (Figures 2 and 3). The majority of the reported cases responded immediately after one session of EBL and usually only one band per lesion was sufficient. Effective EBL of a bleeding rectal DL that was previously treated with hemoclips has also been reported (14). Although most DLs are located in the stomach, esophageal and duodenal DLs have been successfully treated with EBL (15,16). From all the cases reviewed, we found only one case of rebleeding after 24 h of therapy with EBL a shallow ulcer at the site of banding was seen and adrenaline 1:10,000 was injected with no further rebleeding at 12 months follow-up (4). There was only one reported case (17) of fatal rebleeding after EBL for a DL located at the gastric cardia in a patient with previous failed endoscopic treatments (injection and thermal probe coagulation). Two rubber bands had to be applied because of a large-size lesion and a delayed massive rebleeding occurred (after 33 days of EBL treatment). A diagnostic upper endoscopy was not performed, nor was an autopsy to confirm the cause of death. In a retrospective study, Mumtaz et al (18) analyzed the outcomes of patients with DL who were treated with EBL compared with thermal-injection therapy. Twenty-three patients were included in the study (14 patients in the EBL group). Active hemostasis was achieved in 100% of cases in both groups but early rebleeding occurred in one 1 Department of Gastrointestinal Endoscopy, Instituto Nacional de Ciencias Médicas y Nutrición, Mexico City, Mexico; 2 The Centre for Advanced Therapeutic Endoscopy and Endoscopic Oncology, St Michael s Hospital, Toronto, Ontario Correspondence and reprints: Dr Norman E Marcon, Division of Gastroenterology, University of Toronto, St Michael s Hospital, 30 Bond Street, Toronto, Ontario M5B 1W8. Telephone , fax , norman.marcon@utoronto.ca Received for publication July 23, Accepted August 11, Pulsus Group Inc. All rights reserved Can J Gastroenterol Vol 22 No 9 September 2008
2 TABLE 1 Different options for endoscopic band ligation in nonvariceal bleeding Vascular lesions in the gastrointestinal tract Dieulafoy lesion Mallory-Weiss tear Gastric antral vascular ectasia Postpolypectomy bleeding Rubber bleb nevus syndrome Colonic diverticular bleeding patient in the thermal-injection therapy group. The authors concluded that EBL is as effective as injection with or without thermal therapy in the treatment of DL. In a prospective, randomized trial (19) comparing EBL with hemoclip placement for bleeding DL, 26 patients were enrolled, 13 in each group. One rubber band was applied for each EBL case and the median number of hemoclips needed was one. Primary hemostasis was achieved in all patients with one case of rebleeding in each group. No complications were reported. The authors concluded that there were no differences in the efficacy or safety between EBL and hemoclips for the treatment of DL. MALLORY-WEISS TEAR Mallory-Weiss tears (MWTs) are lacerations at or near the esophagogastric junction that may cause acute GI bleeding. These lacerations are secondary to sudden elevations in abdominal pressure, usually after retching or vomiting. The first cases of successful treatment of MWTs with EBL were reported in 1998, one after previous failed endoscopic treatment with adrenaline injection (3,4). Another patient (20) with bleeding secondary to an MWT was successfully treated with EBL. In this case, a 75-year-old man presented with hematemesis after severe retching during a gastroscopy. The bleeding stopped immediately after the release of one rubber band at the site of the mucosal tear. Gunay et al (21) reported four patients with bleeding MWTs that were successfully treated with EBL. All patients achieved complete hemostasis and no rebleeding was observed. In a prospective, randomized trial comparing EBL with adrenaline injection for bleeding MWTs (22), 34 patients were enrolled; 17 patients underwent EBL and 17 underwent adrenaline injection. One to two rubber bands were applied in the EBL group and the mean volume of adrenaline required in the second group was 18 ml. Primary hemostasis was achieved in all cases in the EBL group and in 16 cases in the adrenaline group, with no rebleeding or major complications in either group. The authors concluded that there was no difference in the efficacy or safety of EBL versus adrenaline injection for the treatment of bleeding MWTs. A case series also described the usefulness of EBL for bleeding MWTs (23). Thirty-seven patients were prospectively treated with EBL. Thirty-six patients achieved complete hemostasis after the first session, while the remaining patient had severe liver failure with coagulopathy. No complications were reported. The authors concluded that EBL is an effective and safe procedure for treating bleeding MWTs. Finally, a recently published prospective, randomized study compared EBL with endoscopic hemoclip placement (EHP) in actively bleeding MWTs (24). Forty-one patients were included and 20 were treated with EBL. Primary hemostasis was achieved in all patients. Two patients in the EBL group and one in the EHP group had recurrent bleeding and were treated with a second session of the same endoscopic modality. Secondary hemostasis was achieved in all patients. There were no complications, and no differences in hospital stay or transfusion requirements between the two groups. The authors concluded that EBL and EHP are equally effective and safe for the treatment of actively bleeding MWTs. POSTPOLYPECTOMY BLEEDING The occurrence of bleeding after endoscopic polypectomy is seen in approximately 2% of cases, and there are several therapies to achieve hemostasis. These include hemoclips, argon plasma coagulation (APC), heater probe and adrenaline injection. The use of EBL for the treatment of postpolypectomy bleeding (PPB) in the colon was first described in Slivka et al (25) reported the case of a 70-year-old patient with multiple comorbidities and bleeding from three polypectomy stalks two at the hepatic flexure and one at the sigmoid colon. He was treated first with electrocautery and adrenaline injection, but rebleeding occurred. EBL was performed and immediate hemostasis was observed with no further rebleeding. In another case report (26), a patient s bleeding immediately after polypectomy was controlled with EBL after unsuccessful treatment with adrenaline injection. Since then, there have been several reports of successful EBL for the treatment of PPB. One rubber band is usually required and hemostasis is achieved immediately (Figures 4 and 5). No complications of this procedure have been reported (27). No trials comparing this therapy with other modalities for PPB have been reported. GASTRIC ANTRAL VASCULAR ECTASIA Gastric antral vascular ectasia (GAVE) or watermelon stomach is characterized by red, angiomatous, ectatic lesions in the gastric antrum that can be associated with GI hemorrhage at endoscopic examination (28). There are two kinds of patterns identified. The first pattern is multiple red stripes, which are often raised and radiate to the pylorus. The etiology is unknown in the majority of patients but sometimes it is associated with autoimmune or connective tissue diseases. The second pattern is more diffuse lesions with a pattern of small, flat spots, primarily in the antrum. This is usually associated with portal hypertension (29). GAVE can account for approximately 3.9% of cases of obscure GI bleeding (30). Endoscopic treatment is now the preferred therapy in the majority of cases. Surgical therapy consisting of antrectomy is effective but its application is limited by the high surgical risk of most patients and the morbidity related to the procedure. Various endoscopic treatment modalities have been used for GAVE. These include monopolar electrocoagulation, heater probe, cryotherapy and APC (31-36). Currently, APC is the most frequent endoscopic modality used for the treatment of GAVE. The treatment time and number of sessions needed to complete eradication of lesions depends on the pattern (the diffuse type takes longer to eradicate), the extent and number of lesions, and the circumstances of treatment (active bleeding takes more sessions than elective therapy). On average, two to four treatment sessions are needed to achieve complete eradication with APC. Two recent reports have described Can J Gastroenterol Vol 22 No 9 September
 Spurting Dieulafoy ulcer controlled with rubber band ligation anemia and an episode of hematemesis.")


3 11319_Zepeda-Gomez_experts.qxd 29/08/2008 9:21 AM Page 750 Figure 1) Multiple angiodysplasias in a patient with hereditary hemorrhagic telangiectasia. Muliple lesions were ligated Figure 2) Spurting Dieulafoy ulcer controlled with rubber band ligation anemia and an episode of hematemesis. An upper endoscopy revealed a type 1 GAVE, and EBL of the ectasias was performed because APC was not available. Six bands were deployed from the stripes of the pylorus to a more proximal location. Further endoscopies revealed partial resolution of the lesions and a second session of EBL was performed six months later, applying another six bands that targeted the residual areas of GAVE. No complications were observed during or after the procedure. The hemoglobin level stabilized and subsequent endoscopic examinations after two and six months showed complete resolution of GAVE. The patient remained asymptomatic after 16 months of follow-up. In another case report (38), a 55-year-old woman with a history of melena and severe anemia had been treated with APC on two occasions for GAVE. She was treated with EBL as a salvage therapy. In the first session, five bands were applied and in the second (two weeks later), 11 bands were deployed. There was clinical and endoscopic improvement, and the reported adverse effects after EBL were epigastric pain controlled by oral analgesics (not specified) and ulcers at the site of treatment, which healed completely. After 15 months of follow-up, she remained stable. Figure 3) Nonbleeding Dieulafoy ulcer the use of EBL for the treatment of GAVE. In the first report (37), a 53-year-old man was evaluated for iron deficiency 750 OTHER CAUSES OF GI BLEEDING There was one report (39) of the use of EBL for rubber bleb nevus syndrome in a 15-year-old boy with hematemesis and four elevated bluish lesions in the antrum. Two treatment sessions were performed and no further bleeding was documented. Can J Gastroenterol Vol 22 No 9 September 2008
. There were no complications or rebleeding during a 12-month follow-up period.")

4 Figure 5) Stalk of polyp ligated with control of bleeding Figure 4) Spurting stalk after a polypectomy in the sigmoid colon Colonic diverticular bleeding has been reported to be effectively treated by EBL in four patients (40). There were no complications or rebleeding during a 12-month follow-up period. CONCLUSIONS EBL is increasingly being used as a primary therapy for nonvariceal bleeding lesions in the GI tract. It has been shown to be an easy and safe method with a high rate of success. It is at least equally effective as the previous standard methods such as hemoclipping, injection of adrenaline or sclerosants, and thermal therapy. There is more information in patients with vascular malformations, Dieulafoy lesions and MWTs, but recent studies have also shown promising results for the treatment of GAVE and PPB. EBL could be a primary or alternative method for the treatment of nonvariceal bleeding lesions of the GI tract. REFERENCES 1. Laine L, Cook D. Endoscopic ligation compared with sclerotherapy for treatment of esophageal variceal bleeding. A meta-analysis. Ann Intern Med 1995;123: Karnam US, Barkin J. Vascular malformations of the small intestine. Curr Treat Options Gastroenterol 2001;4: Wong RM, Ota S, Katoh A, et al. Endoscopic ligation for non-esophageal variceal upper gastrointestinal hemorrhage. Endoscopy 1998;30: Abi-Hanna D, Williams S, Gillespie P, Bourke M. Endoscopic band ligation for non-variceal non-ulcer gastrointestinal hemorrhage. Gastrointest Endosc 1998;48: Junquera F, Brullet E, Campo R, Calvet X, Puig-Diví V, Vergara M. Usefulness of endoscopic band ligation for bleeding small bowel vascular lesions. Gastrointest Endosc 2003;58: Pointner R, Schwab G, Königsrainer A, Dietze O. Endoscopic treatment of Dieulafoy s disease. Gastroenterology 1988;94: Parra-Blanco A, Takahashi H, Mendez Jerez PV, et al. Endoscopic management of Dieulafoy lesions of the stomach: A case study of 26 patients. Endoscopy 1997;29: Schmulewitz N, Baillie J. Dieulafoy lesions: A review of 6 years of experience at a tertiary referral center. Am J Gastroenterol 2001;96: Yilmaz M, Ozütemiz O, Karasu Z, et al. Endoscopic injection therapy of bleeding Dieulafoy lesion of the stomach. Hepatogastroenterology 2005;52: Sone Y, Kumada T, Toyoda H, Hisanaga Y, Kiriyama S, Tanikawa M. Endoscopic management and follow-up of Dieulafoy lesion in the upper gastrointestinal tract. Endoscopy 2005;37: Cheng CL, Liu NJ, Lee CS, et al. Endoscopic management of Dieulafoy lesions in acute nonvariceal upper gastrointestinal bleeding. Dig Dis Sci 2004;49: Norton ID, Petersen BT, Sorbi D, Balm RK, Alexander GL, Gostout CJ. Management and long-term prognosis of Dieulafoy lesion. Gastrointest Endosc 1999;50: Brown GR, Harford WV, Jones WF. Endoscopic band ligation of an actively bleeding Dieulafoy lesion. Gastrointest Endosc 1994;40: Yoshikumi Y, Mashima H, Suzuki J, et al. A case of rectal Dieulafoy s ulcer and successful endoscopic band ligation. Can J Gastroenterol 2006;20: Hurlstone DP. Successful endoscopic band ligation of duodenal Dieulafoy s lesions. Further large controlled studies required. Scan J Gastroenterol 2002;37: Soetikno RM, Piper J, Montes H, Ukomadu C, Carr-Locke DL. Use of endoscopic band ligation to treat a Dieulafoy s lesion of the esophagus. Endoscopy 2000;32:S Chen YY, Su WW, Soon MS, Yen HH. Delayed fatal hemorrhage after endoscopic band ligation for gastric Dieulafoy s lesion. Gastrointest Endosc 2005;62: Mumtaz R, Shaukat M, Ramirez F. Outcomes of endoscopic treatment of gastroduodenal Dieulafoy s lesion with rubber band ligation and thermal/injection therapy. J Clin Gastroenterol 2003;36: Park CH, Joo YE, Kim HS, Choi SK, Rew JS, Kim SJ. A prospective, randomized trial of endoscopic band ligation versus endoscopic hemoclip placement for bleeding gastric Dieulafoy s lesions. Endoscopy 2004;36: Myung SJ, Kim HR, Moon YS. Severe Mallory-Weiss tear after endoscopy treated by endoscopic band ligation. Gastrointest Endosc 2000;52: Gunay K, Cabioglu N, Barbaros U, Taviloglu K, Ertekin C. Endoscopic ligation for patients with actively bleeding Mallory- Weiss tears. Surg Endosc 2001;15: Park CH, Min SW, Sohn YH, et al. A prospective, randomized trial of endoscopic band ligation vs epinephrine injection for actively bleeding Mallory-Weiss syndrome. Gastrointest Endosc 2004;60: Higuchi N, Akahoshi K, Sumida Y, et al. Endoscopic band ligation therapy for upper gastrointestinal bleeding related to Mallory-Weiss syndrome. Surg Endosc 2006;20: Cho YS, Chae HS, Kim HK, et al. Endoscopic band ligation and endoscopic hemoclip placement for patients with Mallory-Weiss syndrome and active bleeding. World J Gastroenterol 2008;14: Slivka A, Parsons W, Carr-Locke D. Endoscopic band ligation for treatment of post-polypectomy hemorrhage. Gastrointest Endosc 1994;40: Smith RE, Doull J. Treatment of colonic post-polypectomy bleeding site by endoscopic band ligation. Gastrointest Endosc 1994;40: Can J Gastroenterol Vol 22 No 9 September
5 27. Pfaffenbach B, Adamek RJ, Wegener M. Endoscopic band ligation for treatment of post-polypectomy bleeding. Z Gastroenterol 1996;34: Jensen DM, Chaves DM, Grund K. Endoscopic diagnosis and treatment of watermelon stomach. Endoscopy 2004;36: Ito M, Uchida Y, Kamono S, et al. Clinical comparisons between two subsets of gastric antral vascular ectasia. Gastrointest Endosc 2001;53: Kovacs TO, Jensen DM. Recent advances in the endoscopic diagnosis and treatment of upper gastrointestinal, small intestinal, and colonic bleeding. Med Clin N Am 2002;86: Cugia L, Carta M, Dore MP, et al. The watermelon stomach: Successful treatment by monopolar electrocoagulation and endoscopic injection of polidocanol. J Clin Gastroenterol 2000;31: Petrini JL, Johnston JH. Heat probe treatment for antral vascular ectasia. Gastrointest Endosc 1989;35: Kantsevoy SV, Cruz-Correa MR, Vaughn CA, et al. Endoscopic cryotherapy for the treatment of bleeding mucosal vascular lesions of the GI tract: A pilot study. Gastrointest Endosc 2003;57: Probst A, Scheudbel R, Wienbeck M. Treatment of watermelon stomach (GAVE syndrome) by means of endoscopic argon plasma coagulation (APC): Long-term outcome. Gastroenterology 2001;39: Chaves DM, Baba ER, Sakai P, et al. The argon beam plasma coagulation (ABPC) for treatment of gastric antral vascular ectasia (watermelon stomach). Endoscopy 1991;31(Suppl 1):E Grund KE, Straub T, Farin G. New haemostatic techniques: Argon plasma coagulation. Bailliere s Best Pract Res Clin Gastroenterol 1999;13: Sinha S, Udawat H, Varma S, et al. Watermelon stomach treated with endoscopic band ligation. Gastrointest Endosc 2006;64: Kumar R, Mohindra S, Pruthi HS. Endoscopic band ligation: A novel therapy for bleeding gastric antral vascular ectasia. Endoscopy 2007;39:E56-E Nijhawan S, Kumar D, Joshi A, et al. Endoscopic band ligation for non-variceal bleed. Indian J Gastroenterol 2004;23: Farrell JJ, Graeme-Cook F, Kelsey PB. Treatment of bleeding colonic diverticula by endoscopic band ligation: An in-vivo and ex-vivo pilot study. Endoscopy 2003;35: Can J Gastroenterol Vol 22 No 9 September 2008











6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Endoscopic Management of Vascular Lesions of the GI tract
 Endoscopic Management of Vascular Lesions of the GI tract Lake Louise, June 2014 Sergio Zepeda Gómez MD Assistant Professor Division of Gastroenterology University of Alberta, Edmonton Best Practice &
Endoscopic Management of Vascular Lesions of the GI tract Lake Louise, June 2014 Sergio Zepeda Gómez MD Assistant Professor Division of Gastroenterology University of Alberta, Edmonton Best Practice &
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Portal Hypertensive Gastropathy and Gastric Antral Vascular Ectasia
 Portal Hypertensive Gastropathy and Gastric Antral Vascular Ectasia Andrés Cárdenas, MD, MMSc,PhD,AGAF, FAASLD GI/Liver Unit - Hospital Clinic Institut de Malalties Digestives i Metaboliques University
Portal Hypertensive Gastropathy and Gastric Antral Vascular Ectasia Andrés Cárdenas, MD, MMSc,PhD,AGAF, FAASLD GI/Liver Unit - Hospital Clinic Institut de Malalties Digestives i Metaboliques University
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Stem Cell 2017;8(2)
") Endoscopic Band Ligation versus Argon Plasma Coagulation in Treatment of Gastric Antral Vascular Ectasia Tarek El-Mahdy Korah, MD; Elsayed Ibrahim Elshayeb, MD; Mohamed Hamdy Badr, MD; Ezzat Mohamed Abdalla,
Endoscopic Band Ligation versus Argon Plasma Coagulation in Treatment of Gastric Antral Vascular Ectasia Tarek El-Mahdy Korah, MD; Elsayed Ibrahim Elshayeb, MD; Mohamed Hamdy Badr, MD; Ezzat Mohamed Abdalla,
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital ABSTRACT
 Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Risk Factors for Dieulafoy Lesions in the Upper Gastrointestinal Tract
 ORIGINAL ARTICLE Clin Endosc 2015;48:228-233 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2015.48.3.228 Open Access Risk Factors for Dieulafoy Lesions in the Upper Gastrointestinal
ORIGINAL ARTICLE Clin Endosc 2015;48:228-233 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2015.48.3.228 Open Access Risk Factors for Dieulafoy Lesions in the Upper Gastrointestinal
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Shou Jiang Tang, MD, FASGE. Director of Endoscopic Research Professor in Medicine
 Shou Jiang Tang, MD, FASGE Director of Endoscopic Research Professor in Medicine Through-the-scope clipping devices Over-the-scope clipping devices First reported clipping device Hayshi T, Yonezawa M,
Shou Jiang Tang, MD, FASGE Director of Endoscopic Research Professor in Medicine Through-the-scope clipping devices Over-the-scope clipping devices First reported clipping device Hayshi T, Yonezawa M,
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
EndoClot PHS A medical application on 74 patients march 2013
 EndoClot PHS A medical application on 74 patients march 2013 EndoClot PHS as a new method to achieve hemostasis of gastrointestinal bleeding Evaluation of a medical application involving 74 patients. Introduction
EndoClot PHS A medical application on 74 patients march 2013 EndoClot PHS as a new method to achieve hemostasis of gastrointestinal bleeding Evaluation of a medical application involving 74 patients. Introduction
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding
 in high risk peptic ulcer bleeding") ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING
 Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding.
 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper Gastrointestinal Manifestations in Chronic Renal Failure Through Upper Gastrointestinal Endoscopy
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/249 Upper Gastrointestinal Manifestations in Chronic Renal Failure Through Upper Gastrointestinal Endoscopy Madavaram
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/249 Upper Gastrointestinal Manifestations in Chronic Renal Failure Through Upper Gastrointestinal Endoscopy Madavaram
Epidemiology and Treatment of Colonic Angiodysplasia; a Population-Based Study. Naomi G. Diggs, MD Lisa L. Strate, MD MPH March 2, 2010
 Epidemiology and Treatment of Colonic Angiodysplasia; a Population-Based Study. Naomi G. Diggs, MD Lisa L. Strate, MD MPH March 2, 2010 Background Angiodysplasia is an important cause of occult and acute
Epidemiology and Treatment of Colonic Angiodysplasia; a Population-Based Study. Naomi G. Diggs, MD Lisa L. Strate, MD MPH March 2, 2010 Background Angiodysplasia is an important cause of occult and acute
Introduction E266. Introduction and study aims Gastric antral vascular ectasia
 Radiofrequency ablation (RFA) vs. argon plasma coagulation (APC) for the management of gastric antral vascular ectasia (GAVE) in patients with and without cirrhosis: results from a retrospective analysis
Radiofrequency ablation (RFA) vs. argon plasma coagulation (APC) for the management of gastric antral vascular ectasia (GAVE) in patients with and without cirrhosis: results from a retrospective analysis
Therapeutic Endoscopy for Nonvariceal Gastrointestinal Bleeding
 Journal of Pediatric Gastroenterology and Nutrition 45:157 171 # 2007 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology,
Journal of Pediatric Gastroenterology and Nutrition 45:157 171 # 2007 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology,
Case Report Features of the Atrophic Corpus Mucosa in Three Cases of Autoimmune Gastritis Revealed by Magnifying Endoscopy
 Volume 2012, Article ID 368160, 4 pages doi:10.1155/2012/368160 Case Report Features of the Atrophic Corpus Mucosa in Three Cases of Autoimmune Gastritis Revealed by Magnifying Endoscopy Kazuyoshi Yagi,
Volume 2012, Article ID 368160, 4 pages doi:10.1155/2012/368160 Case Report Features of the Atrophic Corpus Mucosa in Three Cases of Autoimmune Gastritis Revealed by Magnifying Endoscopy Kazuyoshi Yagi,
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Original Article INTRODUCTION
 Original Article Endoscopic treatment for high risk bleeding peptic ulcers: A randomized, controlled trial of epinephrine alone with epinephrine plus fresh Mahsa Khodadoostan, Mohammad Karami Horestani,
Original Article Endoscopic treatment for high risk bleeding peptic ulcers: A randomized, controlled trial of epinephrine alone with epinephrine plus fresh Mahsa Khodadoostan, Mohammad Karami Horestani,
The New England Journal of Medicine URGENT COLONOSCOPY FOR THE DIAGNOSIS AND TREATMENT OF SEVERE DIVERTICULAR HEMORRHAGE
 URGENT COLONOSCOPY FOR THE DIAGNOSIS AND OF SEVERE DIVERTICULAR HEMORRHAGE DENNIS M. JENSEN, M.D., GUSTAVO A. MACHICADO, M.D., ROME JUTABHA, M.D., AND THOMAS O.G. KOVACS, M.D. ABSTRACT Background Although
URGENT COLONOSCOPY FOR THE DIAGNOSIS AND OF SEVERE DIVERTICULAR HEMORRHAGE DENNIS M. JENSEN, M.D., GUSTAVO A. MACHICADO, M.D., ROME JUTABHA, M.D., AND THOMAS O.G. KOVACS, M.D. ABSTRACT Background Although
New Techniques. Incidence of Peptic Ulcer. Changing. Contents - with an emphasis on peptic ulcer bleeding. Cause of death in peptic ulcer bleeding
 Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:151 158 Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy SATOSHI SHINOZAKI, HIRONORI YAMAMOTO,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:151 158 Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy SATOSHI SHINOZAKI, HIRONORI YAMAMOTO,
Research Article Endoscopic and Pathologic Changes of the Upper Gastrointestinal Tract in Crohn s Disease
 BioMed Research International, Article ID 610767, 6 pages http://dx.doi.org/10.1155/2014/610767 Research Article Endoscopic and Pathologic Changes of the Upper Gastrointestinal Tract in Crohn s Disease
BioMed Research International, Article ID 610767, 6 pages http://dx.doi.org/10.1155/2014/610767 Research Article Endoscopic and Pathologic Changes of the Upper Gastrointestinal Tract in Crohn s Disease
Role of Malabsorptive Endoscopic Procedures in Obesity Treatment
 FOCUSED REVIEW SERIES: Roles of Bariatric Endoscopy in Obesity Treatment Clin Endosc 2017;50:26-30 https://doi.org/10.5946/ce.2017.004 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Role of Malabsorptive
FOCUSED REVIEW SERIES: Roles of Bariatric Endoscopy in Obesity Treatment Clin Endosc 2017;50:26-30 https://doi.org/10.5946/ce.2017.004 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Role of Malabsorptive
Eugenia Lauret, Jesús Herrero, Lorena Blanco, Olegario Castaño, Maria Rodriguez, Isabel Pérez, Verónica Alvarez, Adolfo Suárez, and Luis Rodrigo
 Gastroenterology Research and ractice Volume 2013, Article ID 584540, 5 pages http://dx.doi.org/10.1155/2013/584540 Clinical Study Epidemiological Clinical Features and Evolution of Gastroduodenal Ulcer
Gastroenterology Research and ractice Volume 2013, Article ID 584540, 5 pages http://dx.doi.org/10.1155/2013/584540 Clinical Study Epidemiological Clinical Features and Evolution of Gastroduodenal Ulcer
Endoscopic band ligation for colonic diverticular bleeding: possibility of standardization
 E233 Endoscopic band ligation for colonic diverticular bleeding: possibility of standardization Authors Institution Yuto Shimamura, Naoki Ishii, Fumio Omata, Noriatsu Imamura, Takeshi Okamoto, Mai Ego,
E233 Endoscopic band ligation for colonic diverticular bleeding: possibility of standardization Authors Institution Yuto Shimamura, Naoki Ishii, Fumio Omata, Noriatsu Imamura, Takeshi Okamoto, Mai Ego,
Case Report Familial Abdominal and Intestinal Lipomatosis Presenting with Upper GI Bleeding
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 123723, 4 pages http://dx.doi.org/10.1155/2015/123723 Case Report Familial Abdominal and Intestinal Lipomatosis Presenting with Upper GI
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 123723, 4 pages http://dx.doi.org/10.1155/2015/123723 Case Report Familial Abdominal and Intestinal Lipomatosis Presenting with Upper GI
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Aetiology Of Upper Gastrointestinal Bleeding In North- Eastern Nigeria: A Retrospective Endoscopic Study
 ISPUB.COM The Internet Journal of Third World Medicine Volume 8 Number 2 Aetiology Of Upper Gastrointestinal Bleeding In North- Eastern Nigeria: A Retrospective Endoscopic S Mustapha, N Ajayi, A Shehu
ISPUB.COM The Internet Journal of Third World Medicine Volume 8 Number 2 Aetiology Of Upper Gastrointestinal Bleeding In North- Eastern Nigeria: A Retrospective Endoscopic S Mustapha, N Ajayi, A Shehu
Clinical Outcomes of Endoscopic Hemostasis for Bleeding in Patients with Unresectable Advanced Gastric Cancer
 J Gastric Cancer. 2017 Dec;17(4):374-383 pissn 2093-582X eissn 2093-5641 Original Article Clinical Outcomes of Endoscopic Hemostasis for Bleeding in Patients with Unresectable Advanced Gastric Cancer 2,*
J Gastric Cancer. 2017 Dec;17(4):374-383 pissn 2093-582X eissn 2093-5641 Original Article Clinical Outcomes of Endoscopic Hemostasis for Bleeding in Patients with Unresectable Advanced Gastric Cancer 2,*
True obscure causes hemobilia, hemosuccus pancreaticus, vasculitis
 Endoscopic Techniques for Small Bowel Imaging Going Where No Man Has Gone Before! Jonathan A. Leighton, MD, FACG, FASGE Mayo Clinic in Arizona 2014 ACG Governors/ASGE Best Practices Course January 2014
Endoscopic Techniques for Small Bowel Imaging Going Where No Man Has Gone Before! Jonathan A. Leighton, MD, FACG, FASGE Mayo Clinic in Arizona 2014 ACG Governors/ASGE Best Practices Course January 2014
Dieulafoy. A Dieulafoy-like Lesion of the Rectum as a Cause of Massive Lower G-I Bleeding. A report of two cases
 19 3 Dieulafoy = Abstract = A Dieulafoy-like Lesion of the Rectum as a Cause of Massive Lower G-I Bleeding A report of two cases Ki Hyun Seo, M.D., Il Kwun Chung, M.D., In Seob Chung, M.D. Jin Woo Lee,
19 3 Dieulafoy = Abstract = A Dieulafoy-like Lesion of the Rectum as a Cause of Massive Lower G-I Bleeding A report of two cases Ki Hyun Seo, M.D., Il Kwun Chung, M.D., In Seob Chung, M.D. Jin Woo Lee,
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Clinical Application of AIMS65 Scores to Predict Outcomes in Patients with Upper Gastrointestinal Hemorrhage
 ORIGINAL ARTICLE Clin Endosc 2015;48:380-384 http://dx.doi.org/10.5946/ce.2015.48.5.380 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Clinical Application of AIMS65 Scores to Predict Outcomes
ORIGINAL ARTICLE Clin Endosc 2015;48:380-384 http://dx.doi.org/10.5946/ce.2015.48.5.380 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Clinical Application of AIMS65 Scores to Predict Outcomes
Hemostatic powder application for control of acute upper gastrointestinal bleeding in patients with gastric malignancy
 Original article Hemostatic powder application for control of acute upper gastrointestinal bleeding in patients with gastric malignancy Authors Yeong Jin Kim, Jun Chul Park, Eun Hye Kim, Sung Kwan Shin,
Original article Hemostatic powder application for control of acute upper gastrointestinal bleeding in patients with gastric malignancy Authors Yeong Jin Kim, Jun Chul Park, Eun Hye Kim, Sung Kwan Shin,
Comparison of the Effectiveness of Interventional Endoscopy in Bleeding Peptic Ulcer Disease according to the Timing of Endoscopy
 Gut and Liver, Vol. 3, No. 4, December 2009, pp. 266-270 original article Comparison of the Effectiveness of Interventional Endoscopy in Bleeding Peptic Ulcer Disease according to the Timing of Endoscopy
Gut and Liver, Vol. 3, No. 4, December 2009, pp. 266-270 original article Comparison of the Effectiveness of Interventional Endoscopy in Bleeding Peptic Ulcer Disease according to the Timing of Endoscopy
R. J. L. F. Loffeld, 1 P. E. P. Dekkers, 2 and M. Flens Introduction
 ISRN Gastroenterology Volume 213, Article ID 87138, 5 pages http://dx.doi.org/1.1155/213/87138 Research Article The Incidence of Colorectal Cancer Is Decreasing in the Older Age Cohorts in the Zaanstreek
ISRN Gastroenterology Volume 213, Article ID 87138, 5 pages http://dx.doi.org/1.1155/213/87138 Research Article The Incidence of Colorectal Cancer Is Decreasing in the Older Age Cohorts in the Zaanstreek
Systematic Review of the Predictors of Recurrent Hemorrhage After Endoscopic Hemostatic Therapy for Bleeding Peptic Ulcers
 American Journal of Gastroenterology ISSN 0002-9270 C 2008 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2008.02070.x Published by Blackwell Publishing CLINICAL REVIEWS Systematic Review of
American Journal of Gastroenterology ISSN 0002-9270 C 2008 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2008.02070.x Published by Blackwell Publishing CLINICAL REVIEWS Systematic Review of
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding
 ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Endoscopic Resection of Subepithelial Tumors
 REVIEW Clin Endosc ;45:240-244 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce..45.3.240 Open Access Endoscopic Resection of Subepithelial Tumors Gwang Ha Kim Department of Internal
REVIEW Clin Endosc ;45:240-244 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce..45.3.240 Open Access Endoscopic Resection of Subepithelial Tumors Gwang Ha Kim Department of Internal
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Supplementary Online Content
 Supplementary Online Content Guimarães PO, Krishnamoorthy A, Kaltenbach LA, et al. Accuracy of medical claims for identifying cardiovascular and bleeding events after myocardial infarction: a secondary
Supplementary Online Content Guimarães PO, Krishnamoorthy A, Kaltenbach LA, et al. Accuracy of medical claims for identifying cardiovascular and bleeding events after myocardial infarction: a secondary
Endoscopic Management of Tumor Bleeding from Inoperable Gastric Cancer
 FOCUSED REVIEW SERIES: Endoscopic Management of Upper Gastrointestinal Bleeding Clin Endosc 2015;48:121-127 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2015.48.2.121 Open
FOCUSED REVIEW SERIES: Endoscopic Management of Upper Gastrointestinal Bleeding Clin Endosc 2015;48:121-127 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2015.48.2.121 Open
Comparison of adrenaline injection and bipolar electrocoagulation for the arrest of peptic ulcer bleeding
 Gut 1999;44:715 719 715 Division of Gastroenterology, Department of Medicine, Veterans General Hospital, Taipei, Taiwan, Republic of China H-J Lin G-Y Tseng C-L Perng F-Y Lee F-Y Chang S-D Lee Correspondence
Gut 1999;44:715 719 715 Division of Gastroenterology, Department of Medicine, Veterans General Hospital, Taipei, Taiwan, Republic of China H-J Lin G-Y Tseng C-L Perng F-Y Lee F-Y Chang S-D Lee Correspondence
Over the Scope Clips for Treatment of Acute Nonvariceal Gastrointestinal Bleeding in Children Are Safe and Effective. What Is New
 ORIGINAL ARTICLE: GASTROENTEROLOGY Over the Scope Clips for Treatment of Acute Nonvariceal Gastrointestinal Bleeding in Children Are Safe and Effective Paul Tran, Joshua Carroll, y Bradley A. Barth, y
ORIGINAL ARTICLE: GASTROENTEROLOGY Over the Scope Clips for Treatment of Acute Nonvariceal Gastrointestinal Bleeding in Children Are Safe and Effective Paul Tran, Joshua Carroll, y Bradley A. Barth, y
Risk factors of the rebleeding according to the patterns of nonvariceal upper gastrointestinal bleeding
 Gastrointestinal Tract Risk factors of the rebleeding according to the patterns of nonvariceal upper gastrointestinal bleeding Ji Hyung Nam 1, Tae Joo Jeon 2, Jae Hee Cho 3, Jae Hak Kim 1 1 Department
Gastrointestinal Tract Risk factors of the rebleeding according to the patterns of nonvariceal upper gastrointestinal bleeding Ji Hyung Nam 1, Tae Joo Jeon 2, Jae Hee Cho 3, Jae Hak Kim 1 1 Department
Research Article Small Bowel Endoscopy Diagnostic Yield and Reasons of Obscure GI Bleeding in Chinese Patients
 Gastroenterology Research and Practice, Article ID 437693, 5 pages http://dx.doi.org/10.1155/2014/437693 Research Article Small Bowel Endoscopy Diagnostic Yield and Reasons of Obscure GI Bleeding in Chinese
Gastroenterology Research and Practice, Article ID 437693, 5 pages http://dx.doi.org/10.1155/2014/437693 Research Article Small Bowel Endoscopy Diagnostic Yield and Reasons of Obscure GI Bleeding in Chinese
Evaluation and Management of Gastrointestinal Bleeding Part 2: Lower and Obscure Gastrointestinal Bleeding
 Evaluation and Management of Gastrointestinal Bleeding Part 2: Lower and Obscure Gastrointestinal Bleeding Edward Lung, MD, MPH ABSTRACT This article, the second in a 2-part series, provides information
Evaluation and Management of Gastrointestinal Bleeding Part 2: Lower and Obscure Gastrointestinal Bleeding Edward Lung, MD, MPH ABSTRACT This article, the second in a 2-part series, provides information
2nd INTERNATIONAL SYMPOSIUM ON LASER SURGERY. laser Phototherapy in Man Using Argon and Neodymium:YAG Lasers
 2nd INTERNATIONAL SYMPOSIUM ON LASER SURGERY laser Phototherapy in Man Using Argon and Neodymium:YAG Lasers R.M. Dwyer, M. Bass and E. Van Stryland ~ Department of Medicine, University of California Los
2nd INTERNATIONAL SYMPOSIUM ON LASER SURGERY laser Phototherapy in Man Using Argon and Neodymium:YAG Lasers R.M. Dwyer, M. Bass and E. Van Stryland ~ Department of Medicine, University of California Los
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A Retrospective Study
 Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Endoclips vs large or small-volume epinephrine in peptic ulcer recurrent bleeding
 Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v18.i18.2219 World J Gastroenterol 2012 May 14; 18(18): 2219-2224 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v18.i18.2219 World J Gastroenterol 2012 May 14; 18(18): 2219-2224 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
REFERRAL GUIDELINES: ENDOSCOPY
 Outpatient Referral Guidelines Page 1 REFERRAL GUIDELINES: Referrals for endoscopy must be made using the Essential Referral Content Gastrointestinal Endoscopy Referral Form Please fax the completed referral
Outpatient Referral Guidelines Page 1 REFERRAL GUIDELINES: Referrals for endoscopy must be made using the Essential Referral Content Gastrointestinal Endoscopy Referral Form Please fax the completed referral
Fluoroscopy-Guided Endoscopic Removal of Foreign Bodies
 CASE REPORT Clin Endosc 2017;50:197-201 https://doi.org/10.5946/ce.2016.085 Print ISSN 2234-2400 / On-line ISSN 2234-2443 Open Access Fluoroscopy-Guided Endoscopic Removal of Foreign odies Junhwan Kim
CASE REPORT Clin Endosc 2017;50:197-201 https://doi.org/10.5946/ce.2016.085 Print ISSN 2234-2400 / On-line ISSN 2234-2443 Open Access Fluoroscopy-Guided Endoscopic Removal of Foreign odies Junhwan Kim
Internet Journal of Medical Update
 Internet Journal of Medical Update. 2017 July;12(2):4-9. doi: 10.4314/ijmu.v12i2.2 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work A clinical study
Internet Journal of Medical Update. 2017 July;12(2):4-9. doi: 10.4314/ijmu.v12i2.2 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work A clinical study
Upper Gastrointestinal Bleeding Among Saudis: Etiology And Prevalence The Riyadh Central Hospital Experience
 Upper Gastrointestinal Bleeding Among Saudis: Etiology And Prevalence The Riyadh Central Hospital Experience Mohammed Al-Mofarreh, Facharzt; Yisa M. Fakunle, MD, FRCP (London); Mohammed Al-Moagel, Facharzt
Upper Gastrointestinal Bleeding Among Saudis: Etiology And Prevalence The Riyadh Central Hospital Experience Mohammed Al-Mofarreh, Facharzt; Yisa M. Fakunle, MD, FRCP (London); Mohammed Al-Moagel, Facharzt
Clinical outcome of acute nonvariceal upper gastrointestinal bleeding after hours: the role of urgent endoscopy
 ORIGINAL ARTICLE Korean J Intern Med 2016;31:470-478 Clinical outcome of acute nonvariceal upper gastrointestinal bleeding after hours: the role of urgent endoscopy Dong-Won Ahn 1,2,*, Young Soo Park 1,3,*,
ORIGINAL ARTICLE Korean J Intern Med 2016;31:470-478 Clinical outcome of acute nonvariceal upper gastrointestinal bleeding after hours: the role of urgent endoscopy Dong-Won Ahn 1,2,*, Young Soo Park 1,3,*,
UPPER GASTROINTESTINAL BLEEDING; ENDOSCOPIC FINDINGS IN PATIENTS
 The Professional Medical Journal DOI: 10.17957/TPMJ/17.3711 ORIGINAL PROF-3711 UPPER GASTROINTESTINAL BLEEDING; ENDOSCOPIC FINDINGS IN PATIENTS 2. MBBS, FCPS (Med) Assistant Professor of Medicine Independent
The Professional Medical Journal DOI: 10.17957/TPMJ/17.3711 ORIGINAL PROF-3711 UPPER GASTROINTESTINAL BLEEDING; ENDOSCOPIC FINDINGS IN PATIENTS 2. MBBS, FCPS (Med) Assistant Professor of Medicine Independent
Three Year Old Male with Multiple Dieulafoy Lesions Treated with Epinephrine Injections via Therapeutic Endoscopy
 pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2016.19.4.276 Pediatr Gastroenterol Hepatol Nutr 2016 December 19(4):276-280 Case Report PGHN Three Year Old Male with Multiple Dieulafoy
pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2016.19.4.276 Pediatr Gastroenterol Hepatol Nutr 2016 December 19(4):276-280 Case Report PGHN Three Year Old Male with Multiple Dieulafoy
Histological Value of Duodenal Biopsies
 Case Study TheScientificWorldJOURNAL (2005) 5, 396 400 ISSN 1537-744X; DOI 10.1100/tsw.2005.44 Histological Value of Duodenal Biopsies Limci Gupta and B. Hamid Countess of Chester Hospital NHS Foundation
Case Study TheScientificWorldJOURNAL (2005) 5, 396 400 ISSN 1537-744X; DOI 10.1100/tsw.2005.44 Histological Value of Duodenal Biopsies Limci Gupta and B. Hamid Countess of Chester Hospital NHS Foundation
Nonvariceal Upper Gastrointestinal Bleeding
 Nonvariceal Upper Gastrointestinal Bleeding Stephen R. Rotman and John R. Saltzman 2 Introduction Upper gastrointestinal bleeding (UGIB) is defined as bleeding in the gastrointestinal tract originating
Nonvariceal Upper Gastrointestinal Bleeding Stephen R. Rotman and John R. Saltzman 2 Introduction Upper gastrointestinal bleeding (UGIB) is defined as bleeding in the gastrointestinal tract originating
Eisuke Nomura, Hisatada Hiraoka, and Hiroya Sakai. 1. Introduction. 2. Case Report
 Case Reports in Orthopedics Volume 2016, Article ID 1026861, 5 pages http://dx.doi.org/10.1155/2016/1026861 Case Report Spontaneous Recurrent Hemarthrosis of the Knee: A Report of Two Cases with a Source
Case Reports in Orthopedics Volume 2016, Article ID 1026861, 5 pages http://dx.doi.org/10.1155/2016/1026861 Case Report Spontaneous Recurrent Hemarthrosis of the Knee: A Report of Two Cases with a Source
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Impact of a bleeding care pathway in the management of acute upper gastrointestinal bleeding
 Indian J Gastroenterol (March April 2011) 30(2):72 77 DOI 10.1007/s12664-011-0089-5 ORIGINAL ARTICLE Impact of a bleeding care pathway in the management of acute upper gastrointestinal bleeding Khalid
Indian J Gastroenterol (March April 2011) 30(2):72 77 DOI 10.1007/s12664-011-0089-5 ORIGINAL ARTICLE Impact of a bleeding care pathway in the management of acute upper gastrointestinal bleeding Khalid
James Irwin Gastroenterology Department Palmerston North Hospital. Acute Medicine Meeting Hutt Hospital. June 21, 2015
 The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper Intestinal Obstruction
 Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Improved risk assessment in upper GI bleeding
 EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine -
 Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
YES NO UNKNOWN. Stage I: Rule-Out Dashboard ACTIONABILITY PENETRANCE SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS. YES ( 1 of above)
") Stage I: Rule-Out Dashboard GENE/GENE PANEL: SMAD4, BMPR1A DISORDER: Juvenile Polyposis Syndrome HGNC ID: 6670, 1076 OMIM ID: 174900, 175050 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource,
Stage I: Rule-Out Dashboard GENE/GENE PANEL: SMAD4, BMPR1A DISORDER: Juvenile Polyposis Syndrome HGNC ID: 6670, 1076 OMIM ID: 174900, 175050 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource,
25/11/ / upper G.I. bleeding sources 20/ lower G.I. bleeding sources. scaricato da 1
 U.S.L. AVEZZANO - SULMONA Ospedale SS Filippo e Nicola U.O. ENDOSCOPIA DIGESTIVA (Direttore Dott. Antonio Sedici) double-balloon balloon enteroscopy new gold standard for small-bowel imaging? A. Sedici
U.S.L. AVEZZANO - SULMONA Ospedale SS Filippo e Nicola U.O. ENDOSCOPIA DIGESTIVA (Direttore Dott. Antonio Sedici) double-balloon balloon enteroscopy new gold standard for small-bowel imaging? A. Sedici
Original Article. Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome
 Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
Experience in the use of argon plasma in gastrointestinal tract lesions in two institutions in Bogotá
 Original articles Experience in the use of argon plasma in gastrointestinal tract lesions in two institutions in Bogotá Cañadas Raúl, MD, 1 Serrano Carlos, MD, 1 Hani Albis, MD, 1 Galiano María T, MD,
Original articles Experience in the use of argon plasma in gastrointestinal tract lesions in two institutions in Bogotá Cañadas Raúl, MD, 1 Serrano Carlos, MD, 1 Hani Albis, MD, 1 Galiano María T, MD,