Gastrointestinal bleeding and life threating conditions in surgery
|
|
|
- Ethel O’Connor’
- 5 years ago
- Views:
Transcription
1 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery
2 Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts for more than 80% of acute bleeding) Lower intestinal hemorrhage distal to the Treitz ligament
3 Gastrointestinal hemorrhage Acute bleeding blood loss exeeds 500 ml Chronic bleeding blood loss 50 ml/day Occult bleeding is not apparent to the patient until presentation with symptoms related to the anemia.
4 Upper Gastrointestinal hemorrhage
5 Upper Gastrointestinal hemorrhage Acute gastrointestinal hemorrhage may range from trivial to massive and can originate from virtually any region of the gastrointestinal tract, including the pancreas, liver and biliary tree.

6 Upper Gastrointestinal hemorrhage Most patients with an acute hemorrhage stop bleeding spontaneously. However, in almost 15% of cases, major bleeding persists, requiring emergent resuscitation, evaluation and treatment. Improvement of the management of these patients, primarily by early endoscopy and directed therapy, has significantly reduced the lenght of hospitalization. Despite this, the mortality rate remains graeter than 5% and is significantly higher in those patients initially hospitalized for other reasons.
7 Acute Gastrointestinal hemorrhage In patients with GI bleeding, several fundamental principles of initial evaluation and management must be followed.
8 Acute Gastrointestinal hemorrhage Initial assesment and resuscitation Assess airway, breathing, and circulation (ABCs) Assess magnitude of bleeding Initiate appropriate monitoring Laboratory evaluation History and exam Identify risk factors Previous surgery Medications Localize bleeding Nasogastric tube aspirate Endoscopy Other studies as needed Initiate therapy Pharmacologic, Endoscopic Angiographic Surgical
9 Upper Gastrointestinal hemorrhage 80-85% - stop bleeding spontaneously 15-20% - endoscopic treatment 15% - endoscopically treated requires surgery 70% urgency procedure 30% planned procedure
10 Upper Gastrointestinal hemorrhage Symptoms: Coffee-ground vomit refers to the vomiting of black material which is assumed to be blood; it implies that bleeding has ceased or has been relatively modest. Melaena: black tarry stools, usually due to acute UGIB but occasionally bleeding from the small bowel or right side of the colon. Haematemesis: bright red haematemesis usually implies active haemorrhage. Patients presenting with haematemesis have a higher mortality than those presenting with melaena alone. Haematochezia: passage of fresh or altered blood per rectum, usually due to colonic bleeding but occasionally due to profuse upper gastrointestinal or small bowel bleeding. Abdominal pain, epigastric pain Weakness Loss of blood: shock, syncope, presyncope
11 Acute Upper Gastrointestinal hemorrhage Aetiology Peptic ulcer Oesophagitis Gastritis/erosions Erosive duodenitis Varices Portal hypertensive gastropathy Malignancy Mallory-Weiss tear Vascular malformation
12 Acute Upper Gastrointestinal hemorrhage PUD peptic ulcer disease still represent the most frequent cause of upper GI hemorrhage accounting for about 40 % of all cases. About 10 to 15% of patients with peptic ulcer disease develop bleeding. bleeding develops as a consequence of acid-peptic erosion of the mucosal surface. Although chronic blood loss is common with any ulcer, significant bleeding typically results when there is involvement of an artery, either of the submucosa or, with penetration of the ulcer, an even larger vessel. although duodenal ulcers are more common than gastric ulcer, gastric ulcers bleed more commonly; as a result, in most series the relative proportions are nearly equal. The most significant hemorrhage occurs when duodenal or gastric ulcers penetrate into branches of the gastroduodenal artery or left gastric artery, respectively.

13 Acute Upper Gastrointestinal hemorrhage
 and regimens for eradication of Helicobacter pylori.")
14 Acute Upper Gastrointestinal hemorrhage The incidence of uncomplicated peptic ulcer has declined dramatically. This recent change has been attributed to better medical therapy, including proton pump inhibitors (PPI s) and regimens for eradication of Helicobacter pylori. The need for operation for perforated peptic ulcer disease has declined as well, surgical intervention for bleeding peptic ulcer disease has remained relatively stable
15 Acute Upper Gastrointestinal hemorrhage Endoscopic therapy is instituted if bleeding is active or, when bleeding has already stopped, if there is a significant risk for rebleeding. The ability to predict the risk for rebleeding permits prophylactic therapy, closer monitoring and earlier detection of hemorrhage in a high-risk patients. The forest classification was developed in an attempt to assess the risk based are on endoscopic findings, and to stratify the patients into low, intermediate and high-risk groups.

16 Acute Upper Gastrointestinal hemorrhage
17 Acute Upper Gastrointestinal hemorrhage PUD Medical management - PPI - Eradication H. pylori PUD Endoscopic Management: - epinephrine injection - heater probes and coagulation - aplication of hemoclips

18 Acute Upper Gastrointestinal hemorrhage Rebleeding - Second attempt
19 Acute Upper Gastrointestinal hemorrhage Surgical management 10% of patients with bleeding still require surgical intervention
20 Acute Upper Gastrointestinal hemorrhage Indications for surgery in gastrointestinal hemorrhage: - Hemodynamic instability despite vigorous resuscitation (>6 units tranasfusion) - Failure of endoscopic techniques to arrest hemorrhage - Recurrent hemorrhage after initial stabilization (with up to two attempts st obtaining endoscopic hemostasis) - Shock associated with recurrent hemorrhage - Continued slow bleeding with a transfusion requirement exceeding 3 units/day
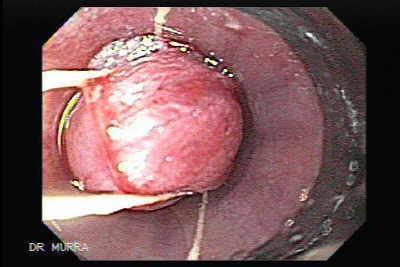
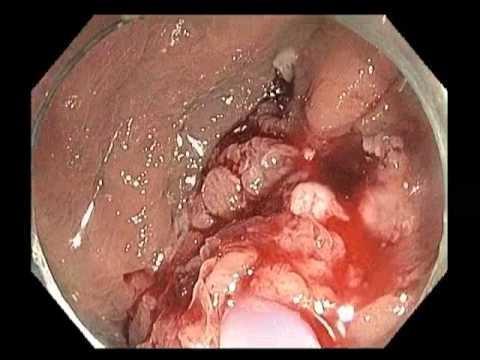
21 Acute Upper Gastrointestinal hemorrhage In Mallory-Weiss syndrome lacerations are longitudinal tears in the esophagus at the esophagogastric junction, attributed to episodes of excessive vomiting in the setting of toxic gastritis, with failure of lower esophageal sphincter relaxation.

22 Acute Upper Gastrointestinal hemorrhage Mallory-Weiss syndrome

23 Acute Upper Gastrointestinal hemorrhage
24 Acute Upper Gastrointestinal hemorrhage Rare causes include: Dieulafoy's lesion (a vascular malformation of the proximal stomach). Angiodysplasia. Haemobilia (bleeding from the gallbladder or biliary tree). Pancreatic pseudocyst and pseudo-aneurysm. Aortoenteric fistula. Bleeding diathesis. Ehlers-Danlos syndrome. Pseudoxanthoma elasticum. Gastric antral vascular ectasia. Osler-Weber-Rendu syndrome.

25 Upper Gastrointestinal hemorrhage Dieulafoy s Leasin are vascular malformationes found primarilyalong the lesser curve of stomach within 6 cm of the gastroesophageal junction.

26 Acute Upper Gastrointestinal hemorrhage Gastric antral Vascular ectasia also known as water melon stomach
27 Acute Upper Gastrointestinal hemorrhage Malignancy: Malignancies of the upper GI tract are usually associated with chronic anemia or hemoccult-positive stool, rather than episodes of significant hemorrhage
28 Acute Upper Gastrointestinal hemorrhage Aortoenteric fistula Primary aortoduodenal fistulas are rare lesions developing up to 1% of aortic graft cases. They typically develop in the setting of a previous abdominal aneurysm repair. Hemorrhage in this situation is often massive and fatal unless immediate surgical intervention is undertaken.
; or witnessed haematemesis or haematochezia (suspected continued bleeding); or haemodynamic disturbance (systolic blood pressure <100 mm Hg, pulse 100 beats per minute); or liver")
29 Acute Upper Gastrointestinal hemorrhage Hospital admission Consider for admission and early endoscopy (and calculation of full Rockall score) if: aged 60 years (all patients who are aged >70 years should be admitted); or witnessed haematemesis or haematochezia (suspected continued bleeding); or haemodynamic disturbance (systolic blood pressure <100 mm Hg, pulse 100 beats per minute); or liver disease or known varices.
30 Acute Upper Gastrointestinal hemorrhage Resuscitation and initial management Shocked patients should receive prompt volume replacement. It has been demonstrated that early and aggressive resuscitation reduces mortality in UGIB Correct fluid losses (place two wide-bore cannulae and also send bloods at the same time). Either colloid or crystalloid solutions may be used to achieve volume restoration prior to administering blood products; red cell transfusion should be considered after loss of 30% of the circulating volume. Transfuse patients with massive bleeding with blood, platelets and clotting factors in line with local protocols for managing massive bleeding. Major haemorrhage protocols should be in place. Decisions on blood transfusion should be based on the full clinical picture; over-transfusion may be as damaging as under-transfusion. Platelet transfusions should not be offered to patients who are not actively bleeding and are haemodynamically stable. Platelet transfusions should be offered to patients who are actively bleeding and have a platelet count of less than 50 x 10 9 /litre. Fresh frozen plasma should be used for patients who have either a fibrinogen level of less than 1 g/litre, or a prothrombin time (INR) or activated partial thromboplastin time greater than 1.5 times normal. Prothrombin complex concentrate should be used for patients who are taking warfarin and actively bleeding. Recombinant factor Vlla should not be used except when all other methods have failed. Proton pump inhibitors (PPIs) should not be used prior to diagnosis by endoscopy in patients presenting with acute UGIB.
31 Rockall Numerical Risk Scoring System assessment of bleeding risk Age Score 0: Age less than 60 years Score 1: Age 60 to 79 years Score 2: Age 80 years or older Shock symptoms Score 0: Shock absent, normal Heart Rate and Blood Pressure Score 1: Heart Rate 100 or higher Score 2: Systolic Blood Pressure <100 mmhg (and Heart Rate 100 or higher) Comorbidity Score 0: None Score 2: CHF, CAD or other major comorbidity Score 3: Renal Failure, liver failure or metastatic cancer Endoscopic diagnosis Score 0: No lesion and no stigmata of recent Hemorrhage (or Mallory-Weiss tear) Score 1: All other Upper Gastrointestinal Bleeding causes (except upper gastrointestinal cancer) Score 2: Upper gastrointestinal tract cancer Stigmata of recent Gastrointestinal Bleeding Score 0: No stigmata or dark spot only Score 3: Blood in upper GI tract, adherent clot, visible vessel, or actively bleeding or spurting vessel
32 Upper Gastrointestinal hemorrhage Interpretation: Total cummulative score Score 0 to 2 Rebleeding rate: 3.5 to 5.3% Mortality: 0 to 0.2% Score 3 Rebleeding rate: 11.2% Mortality: 2.9% Score 4 Rebleeding rate: 14.1% Mortality: 5.3% Score 5 Rebleeding rate: 24.1% Mortality: 10.8% Score 6 Rebleeding rate: 32.9% Mortality: 17.3% Score 7 Rebleeding rate: 43.8% Mortality: 27% Score 8 or higher Rebleeding rate: 41.8% Mortality: 41.1%
33 Upper Gastrointestinal hemorrhage Endoscopy is now the method of choice for controlling active peptic-ulcer related UGIB. Endoscopic therapy should only be delivered to actively bleeding lesions, nonbleeding visible vessels and, when technically possible, to ulcers with an adherent blood clot. Black or red spots or a clean ulcer base with oozing do not merit endoscopic intervention since these lesions have an excellent prognosis without intervention. [ Adrenaline (epinephrine) should not be used as monotherapy for the endoscopic treatment of non-variceal UGIB. For the endoscopic treatment of non-variceal UGIB, one of the following should be used: A mechanical method (eg clips) with or without adrenaline (epinephrine). Thermal coagulation with adrenaline (epinephrine). Fibrin or thrombin with adrenaline (epinephrine). Interventional radiology should be offered to unstable patients who re-bleed after endoscopic treatment. Refer urgently for surgery if interventional radiology is not immediately available.
34 Upper Gastrointestinal hemorrhage Monitoring of ill patient puls Arterial pressure OCŻ diuresis - 50 ml/h
35 Upper Gastrointestinal hemorrhage IPP 80 mg-bolus; followed by continuous intravenous infusion 8mg/h/24h/3 days;
36 Upper Gastrointestinal hemorrhage Monitoring: Allgöwer rate = puls / systolic blood pressure = 0,5 healthy = 1,0 potentially shock > 1,5 shoc
37 Upper Gastrointestinal hemorrhage Surgery
38 A. Bochenek Anatomia człowieka, Tom III
39 A. Bochenek Anatomia człowieka, Tom III
40 Duodenal ulcer Exposure of the bleeding site, longitudinal duodenotomy or duodenal pyloromiotomy is performed, typically suture ligation suffices. Pyloroplasty combined with with truncl vagotomy is the most frequentlu used operation
41 Gastric ulcer Hemigastrectomy with anastomosis BI or BII, vagotomy Exposure of the bleeding site, gastrotomy is performed - typically suture ligation is asociated with 30% rebleeding Gastric ulcer resection
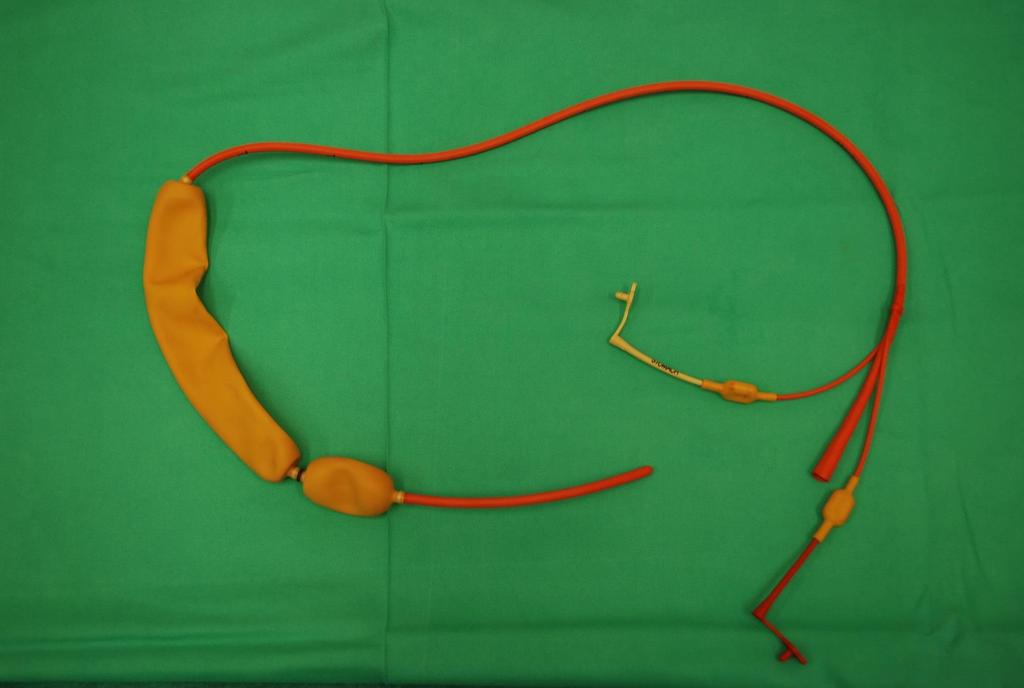
42 Upper Gastrointestinal hemorrhage Management of variceal bleeding [ Terlipressin should be offered to patients with suspected variceal bleeding at presentation. Treatment should be stopped after definitive haemostasis has been achieved, or after five days, unless there is another indication for its use. Prophylactic antibiotic therapy should be offered at presentation to patients with suspected or confirmed variceal bleeding. Balloon tamponade should be considered as a temporary salvage treatment for uncontrolled variceal haemorrhage.
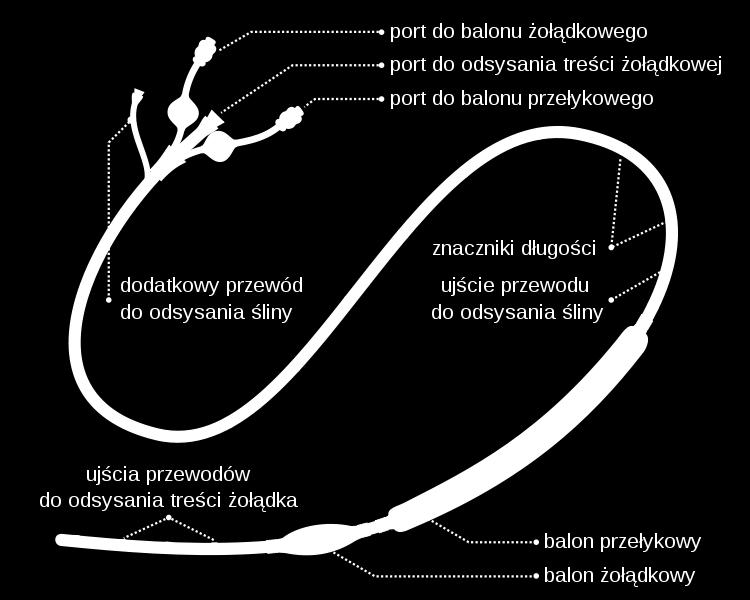
43 Sonda Sengstakena-Blakemorea
44
45 Upper Gastrointestinal hemorrhage Oesophageal varices: Band ligation should be used for patients with UGIB from oesophageal varices. NICE recommends that there is sufficient evidence to show that stent insertion is effective for selected patients with oesophageal varices in whom other methods of treatment have failed to control bleeding. Transjugular intrahepatic portosystemic shunts (TIPS) should be considered if bleeding from oesophageal varices is not controlled by band ligation. Gastric varices: Endoscopic injection of N-butyl-2-cyanoacrylate should be offered to patients with UGIB from gastric varices. TIPS should be offered if bleeding from gastric varices is not controlled by endoscopic injection of N-butyl-2-cyanoacrylate.
46
47 Upper Gastrointestinal hemorrhage Sengstaken-Blakemore probe (1950) Introducing into the lumen of the gastrointestinal tract Gastric baloon filling: 200 ml liquid / air Oesophageal baloon filling: air mmhg Traction 250 g Surgery: Tanner s procedure, Sugiura procedure
48 Lower intestinal hemorrhage

49 Lower intestinal hemorrhage Lower intestinal hemorrhage distal to the Treitz ligament
50 Lower intestinal hemorrhage Stool mixed with blood degree is higher, more high is source of bleeding. Blood on the surface of the stool bleeding from the final part of the gastrointestinal tract laboratory blood tests weakness, shortness of breath
51 Lower intestinal hemorrhage Medical history Clinical examination + per rectum Diagnostic Treatment
52 Lower intestinal hemorrhage Adults to 25 years - Ulcerative colitis - Crohn s disease - Colon polyps - Hemorroidal disease
53 Lower intestinal hemorrhage Adults to 60 years Diverticular disease Ulcerative colitis Crohn s disease Colon polyps Hemorrhoids
54 Lower intestinal hemorrhage Adults above 60 years Angiodysplasia Diverticular disease Colon cancer Colon polyps Hemorrhoids
55 Lower intestinal hemorrhage Diagnostic Clinical exam + per rectum Endoscopy (recto, colonoscopy) Abdominal US Abdomen CT, virtual colonoscopy Contrast of the colon Scyntygraphy


56 Lower intestinal hemorrhage Crohn disease Bleeding from diverticula

57 Colon polyps


58 Lower intestinal hemorrhage Colon cancer Colon cancer


59 Lower intestinal hemorrhage Hemorroids bleeding
60 Lower intestinal hemorrhage Hemorrhage treatment is to locate it s source and removing it (np. hemorroidectomy, gastrectomy, polypectomy itd.); or / and conservative treatment with taking into accout comorbidities.
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Clinical guideline Published: 13 June 2012 nice.org.uk/guidance/cg141
 Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
CLINICAL VIGNETTE 2015; 1:3
 CLINICAL VIGNETTE 2015; 1:3 UPPER GASTRO INTESTINAL BLEEDING Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers
CLINICAL VIGNETTE 2015; 1:3 UPPER GASTRO INTESTINAL BLEEDING Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
Emergency - Upper gastrointestinal haemorrhage
 Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Guidelines for the Management of Upper gastrointestinal bleeding
 Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
CrackCast Episode 30 GI Bleeding
 CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine -
 Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
Scottish Medicines Consortium
 Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Upper GI Bleeds. AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM
 Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient
 Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
Management of acute upper gastrointestinal bleeding
 1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
James Irwin Gastroenterology Department Palmerston North Hospital. Acute Medicine Meeting Hutt Hospital. June 21, 2015
 The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Blood and guts.. Haemodynamics / resuscitation. Haemodynamics / resuscitation. Blood and guts. Dr Jonathan Hoare
 Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding
 ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
Managing acute upper gastrointestinal bleeding in the acute assessment unit
 Clinical Medicine, Vol, No : 589 59 Managing acute upper gastrointestinal bleeding in the acute assessment unit Lotte Dinesen, SpR in gastroenterology; Martin Benson, consultant gastroenterologist and
Clinical Medicine, Vol, No : 589 59 Managing acute upper gastrointestinal bleeding in the acute assessment unit Lotte Dinesen, SpR in gastroenterology; Martin Benson, consultant gastroenterologist and
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital ABSTRACT
 Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Gastrointestinal bleeding definitions (I)
") definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
A cute upper gastrointestinal haemorrhage is
 399 BEST PRACTICE Management of haematemesis and melaena K Palmer... Acute upper gastrointestinal bleeding is a common medical emergency which carries hospital mortality in excess of 10%. The most important
399 BEST PRACTICE Management of haematemesis and melaena K Palmer... Acute upper gastrointestinal bleeding is a common medical emergency which carries hospital mortality in excess of 10%. The most important
Note No nausea or vomiting before collapse increases the risk of an arrhythmia. A
 174 40 TACHYCARDIAS SYMPTOMS AND SIGNS Think about cardiac arrhythmias in patients with: palpitations D dyspnoea B chest pain D dizziness or syncope D cardiac arrest. D Ask about: any nausea or vomiting
174 40 TACHYCARDIAS SYMPTOMS AND SIGNS Think about cardiac arrhythmias in patients with: palpitations D dyspnoea B chest pain D dizziness or syncope D cardiac arrest. D Ask about: any nausea or vomiting
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
9/10/2012. Chapter 44. Learning Objectives. Learning Objectives (Cont d) Bleeding
 Bleeding") Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Multidisciplinary management strategies for acute non-variceal upper gastrointestinal bleeding
 Review Multidisciplinary management strategies for acute non-variceal upper gastrointestinal bleeding Y. Lu 1, R. Loffroy 3,J.Y.W.Lau 4 and A. Barkun 1,2 1 Division of Gastroenterology and 2 Department
Review Multidisciplinary management strategies for acute non-variceal upper gastrointestinal bleeding Y. Lu 1, R. Loffroy 3,J.Y.W.Lau 4 and A. Barkun 1,2 1 Division of Gastroenterology and 2 Department
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap. Simon McPherson, Vascular Interventional Radiologist, Leeds
 Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Picking up their Pieces: Emergency Management of GI Bleeds
 Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Approach to upper gastrointestinal bleeding
 Approach to upper gastrointestinal bleeding Upper GI bleeding is the most common complication of peptic ulceration and portal hypertension. S R Thomson, ChM, FRCS (Edin&Eng) Professor and Head of Department,
Approach to upper gastrointestinal bleeding Upper GI bleeding is the most common complication of peptic ulceration and portal hypertension. S R Thomson, ChM, FRCS (Edin&Eng) Professor and Head of Department,
Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding
 in high risk peptic ulcer bleeding") ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
New Techniques. Incidence of Peptic Ulcer. Changing. Contents - with an emphasis on peptic ulcer bleeding. Cause of death in peptic ulcer bleeding
 Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Dyspepsia and upper gastrointestinal bleeding. Dr. Wayne H.C. Hu 胡興正
 Dyspepsia and upper gastrointestinal bleeding Dr. Wayne H.C. Hu 胡興正 25 year old medical student Occasional smoker and drinker. About to take final examinations. 3 week history of epigastric bloating. Worse
Dyspepsia and upper gastrointestinal bleeding Dr. Wayne H.C. Hu 胡興正 25 year old medical student Occasional smoker and drinker. About to take final examinations. 3 week history of epigastric bloating. Worse
Gastrointestinal bleed- what saves life?
 Gastrointestinal bleed- what saves life? Prof Sauid Ishaq Gastroenterologist, DGH BCU, SGU and Fudan University Physician Associates conference Friday 16 February 2018 Reality What is the mortality of
Gastrointestinal bleed- what saves life? Prof Sauid Ishaq Gastroenterologist, DGH BCU, SGU and Fudan University Physician Associates conference Friday 16 February 2018 Reality What is the mortality of
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Management of acute upper GI bleeding
 BJA Education, 17 (4): 117 123 (2017) Matrix reference 1A01, 2A05, 3C00 doi: 10.1093/bjaed/mkw054 Advance Access Publication Date: 10 December 2016 Management of acute upper GI bleeding Ingi Adel Salah
BJA Education, 17 (4): 117 123 (2017) Matrix reference 1A01, 2A05, 3C00 doi: 10.1093/bjaed/mkw054 Advance Access Publication Date: 10 December 2016 Management of acute upper GI bleeding Ingi Adel Salah
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding.
 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
UPPER AND LOWER GASTROINTESTINAL BLEEDING. Prof. G. Zuliani
 UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
Shou Jiang Tang, MD, FASGE. Director of Endoscopic Research Professor in Medicine
 Shou Jiang Tang, MD, FASGE Director of Endoscopic Research Professor in Medicine Through-the-scope clipping devices Over-the-scope clipping devices First reported clipping device Hayshi T, Yonezawa M,
Shou Jiang Tang, MD, FASGE Director of Endoscopic Research Professor in Medicine Through-the-scope clipping devices Over-the-scope clipping devices First reported clipping device Hayshi T, Yonezawa M,
GASTROINTESTINAL HEMORRHAGE
 Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
Improved risk assessment in upper GI bleeding
 EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
Risk assessment in UGIB: recent PCI & ACS. Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass
 Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Portogram shows opacification of gastroesophageal varices.
 Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A Retrospective Study
 Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
CHAPTER 30 Gastrointestinal Bleeding
 CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
Internet Journal of Medical Update
 Internet Journal of Medical Update. 2017 July;12(2):4-9. doi: 10.4314/ijmu.v12i2.2 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work A clinical study
Internet Journal of Medical Update. 2017 July;12(2):4-9. doi: 10.4314/ijmu.v12i2.2 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work A clinical study
Acute Gastrointestinal Haemorrhage. Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield
 Acute Gastrointestinal Haemorrhage Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield Scope of Talk Introduction Upper GI haemorrhage-non variceal - Pathology/ risk stratification/management
Acute Gastrointestinal Haemorrhage Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield Scope of Talk Introduction Upper GI haemorrhage-non variceal - Pathology/ risk stratification/management
Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication
 Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
haemorrhage in a tropical country
 Archives of Emergency Medicine, 1991, 8, 169-176 The management of upper gastrointestinal haemorrhage in a tropical country T. H. S. G. RAO, G. K. PANDE, P. SAHNI & S. NUNDY Department of Gastrointestinal
Archives of Emergency Medicine, 1991, 8, 169-176 The management of upper gastrointestinal haemorrhage in a tropical country T. H. S. G. RAO, G. K. PANDE, P. SAHNI & S. NUNDY Department of Gastrointestinal
Spectrum of upper gastrointestinal bleed in patients with cirrhosis of liver
 Journal of College of Medical Sciences-Nepal, Vol-13, No 3, July-Sept 017 ISSN: 2091-0657 (Print); 2091-0673 (Online) Open Access Spectrum of upper gastrointestinal bleed in patients with cirrhosis of
Journal of College of Medical Sciences-Nepal, Vol-13, No 3, July-Sept 017 ISSN: 2091-0657 (Print); 2091-0673 (Online) Open Access Spectrum of upper gastrointestinal bleed in patients with cirrhosis of
T he aim of a scheduled second endoscopy is to detect and
 1403 STOMACH Effect of scheduled second therapeutic endoscopy on peptic ulcer rebleeding: a prospective randomised trial P W Y Chiu, C Y W Lam, S W Lee, K H Kwong, S H Lam, D T Y Lee, S P Y Kwok... See
1403 STOMACH Effect of scheduled second therapeutic endoscopy on peptic ulcer rebleeding: a prospective randomised trial P W Y Chiu, C Y W Lam, S W Lee, K H Kwong, S H Lam, D T Y Lee, S P Y Kwok... See
Perforated peptic ulcers. Dr V. Roudnitsky KCH
 Perforated peptic ulcers Dr V. Roudnitsky KCH Peptic ulcer disease Peptic ulcers are focal defects in the gastric or duodenal mucosa that extend into the submucosa or deeper Caused by an imbalance between
Perforated peptic ulcers Dr V. Roudnitsky KCH Peptic ulcer disease Peptic ulcers are focal defects in the gastric or duodenal mucosa that extend into the submucosa or deeper Caused by an imbalance between
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding
 ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING
 Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Nothing to disclose. Annually ~ 300,000 hospitalizations and ~ 20,000 deaths in US*
 Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
UNC HOSPITALS CHAPEL HILL, NORTH CAROLINA REQUEST AND AUTHORIZATION FOR UPPER GASTROINTESTINAL ENDOSCOPY AND BIOPSY MIM#180
 UNC HOSPITALS CHAPEL HILL, NORTH CAROLINA 27514 REQUEST AND AUTHORIZATION FOR UPPER GASTROINTESTINAL ENDOSCOPY AND BIOPSY MIM#180 I request and authorize and/or associates or assistants of his/her choice
UNC HOSPITALS CHAPEL HILL, NORTH CAROLINA 27514 REQUEST AND AUTHORIZATION FOR UPPER GASTROINTESTINAL ENDOSCOPY AND BIOPSY MIM#180 I request and authorize and/or associates or assistants of his/her choice
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures