Welcome to CAP s Hot Topics in Pathology Webinar Series sponsored by the Personalized Health Care Committee
|
|
|
- Abigayle Long
- 5 years ago
- Views:
Transcription
1 Welcome to CAP s Hot Topics in Pathology Webinar Series sponsored by the Personalized Health Care Committee This webinar on Molecular Markers in Breast Cancer is presented by David G. Hicks, MD, FCAP. Your host is Jill Kaufman, PhD. For comments about this webinar or suggestions for upcoming webinars, please contact Jill Kaufman at jkaufma@cap.org THE WEBINAR WILL BEGIN MOMENTARILY. ENJOY!

2 David G. Hicks, MD, FCAP Professor of Pathology and Laboratory Medicine, University of Rochester School of Medicine Director of Surgical Pathology at the University of Rochester Medical Center Current research interests focus on the molecular genetic profiling of clinical samples from patients with cancer Authored or co-authored over 140 peer reviewed articles Member of the CAP s Breast Pathology Certificate Program Work Group and Breast Predictive Factors Testing Program Group 2013 College of American Pathologists. All rights reserved. 2



3 Hot Topics in Pathology Breast Cancer and Molecular David G. Hicks, MD, FCAP March 20, 2013 cap.org v. #
4 Disclaimer The College does not permit reproduction of any substantial portion of the material in this Webinar without its written authorization. The College hereby authorizes attendees of the CAP Webinar to use the pdf presentation solely for educational purposes within their own institutions. The College prohibits use of the material in the Webinar and any unauthorized use of the College s name or logo in connection with promotional efforts by marketers of laboratory equipment, reagents, materials, or services. Opinions expressed by the speaker are the speaker s own and do not necessarily reflect an endorsement by CAP of any organizations, equipment, reagents, materials or services used by participating laboratories College of American Pathologists. All rights reserved. 4
5 Disclosure Professor of Pathology Director of the Surgical Pathology Unit University of Rochester Medical Center Member of the Speakers Bureau Honorarium, Genentech Bio-Oncology 5
6 Changing Role of the Pathologist: Diagnosis and Therapeutic Decisions for Breast Cancer Patients Traditional role Establish morphologic diagnosis of malignancy Infiltrating carcinoma (ductal vs lobular) Tumor grade (SBR) Anatomic extent (size, lymph node status) Breast cancer markers (ER, PR, HER2) Challenges and Opportunities Ensure biologic quality of tissue sample Ensure accurate and reliable ER and HER2 results Guide assay selection per clinical setting Help interpret, and integrate breast cancer marker testing into clinical morphologic context for each patient Role: inform on therapeutic decision Surgical planning Adjuvant endocrine Rx Adjuvant chemotherapy Adjuvant XRT Neoadjuvant therapy Targeted therapies Increasingly, treatment based on an evaluation of tumor biology ER=estrogen receptor; PR=progesterone receptor; SBR=Scarff-Bloom-Richardson tumor grade; TK=tyrosine kinase; XRT=X-ray therapy. Hicks DG et al. Arch Pathol Lab Med. 2008;132: Hoff ER et al. Am J Clin Pathol. 2002;117:
7 Is Molecular/Biological Profiling the Future of Breast Cancer Diagnosis? The Answer is YES! Role of molecular in clinical practice still evolving o What is the most practical, relevant, cost-effective, & broadly applicable ancillary testing that can help determine prognosis? Can this approach be reliably used to guide the selection of beneficial treatment regimens? Can some patients be spared the cost and morbidity of treatments that will be ineffective? What is the level of evidence that the testing strategy can reliably answer these question? Does the test results correlate with the patients clinical profile?
8 Breast Cancer: Clinical, Morphologic and Molecular Heterogeneity Factors used to stratify patient s to understand diversity/predict behavior Age/menopausal status Tumor size/tumor burden Histologic features: type, grade, LVI, necrosis, margin status Lymph node status Immunophenotype: ER, PR, HER2 Proliferation Genomic gains and losses Gene expression profiling QRTPCR profiling Clinical Utility Classify patient s (subsets) Predict outcome Predict treatment response
9 Breast Cancer Management: Decisions on Adjuvant Therapy Based on Risk Assessment Weigh background level - risk of recurrence against benefits & burdens of adjuvant therapy Patient factors (clinically validated) o Age, menopausal status and co-morbidities Tumor-related factors (clinically validated) o Tumor size, grade, LN, LVI Factors are robust prognostic markers, weaker in predicting for Rx response
 T1 = up to 2.0cm T2 = 2.1-5.")

10 Tumor Size/Burden (Measure Greatest Diameter X3) Firm gritty mass with irregular infiltrating borders DFS vs Tumor Size (pt stage) T1 = up to 2.0cm T2 = cm T3 = >5cm T4 = chest wall invasion For node (-)patients: tumor size next most significant prognostic factor used for adjuvant treatment decisions Cancer 1989;63: , Br J Cancer 1984;49:
 Nodal stage Nodal involvement N0 Negative")

11 Lymph Node Status: Correlation with Recurrence & Survival Classic ILC, LN involvement DFS vs LN status (pn stage) Nodal stage Nodal involvement N0 Negative lymph nodes 82.8% N1 1 3 positive nodes 73% N2 4 9 positive nodes 45.7% N3 10 or more positive nodes 5 year survival 28.4% Cancer 1983;52: , JAMA 1996;276:


:403-410, J Clin Pathol.")
12 Histologic Grade (Elston & Ellis modification of SBR) Correlate with Prognosis in Breast Cancer msbr 1 msbr 2 msbr 3 Modified SBR Grade 3-5: Grade I - Well 6-7: Grade II - Moderate 8-9: Grade III Poor Significantly correlates with DFS & OS Histopathology. 1991;19(5): , J Clin Pathol Feb;55(2):88-92, J Clin Oncol. 2007;25(10):




13 GEP: Genomic Grade Index HG1 HG2 HG3 Challenge clinical relevance intermediate grade Low Risk Recurrence High Risk Recurrence Sotiriou, C. et al. J. Natl. Cancer Inst :








14 High Grade Breast Neoplasia Pathway: Aggressive Clinical Course +17q12 +11q13 +6p21-p25 Poor Prognosis Similar DNA changes GEP High Grade Pre-invasive/precursor lesion Invasive disease Normal Breast Similar DNA changes GEP +1q -16q Low Grade Breast Neoplasia Pathway: Indolent Clinical Course Good Prognosis Biomarkers useful for individual risk prediction? Low Grade
15 Guiding Treatment Decisions: Predicted Benefit from Systemic Adjuvant Therapy What criterion must be met to justify the use of endocrine therapy? Any ER staining by IHC (>1% ER+ invasive tumor) What criterion must be met to justify the use of anti-her2 therapy? ASCO/CAP HER2+ - IHC: >30% intense complete membrane staining, FISH: HER2/CEP17 >2.2 What criterion must be met to justify the use of chemotherapy? HER2+ disease = chemo + HER2-targeted therapy Triple negative = chemo ER+/HER2 negative variable indication, based on biology + risk Treatment thresholds are based on disease biology, tumor characteristics and estimated risk for recurrence
16 Chemo/Endocrine Therapy Decision Making in ER+/HER2- Breast Cancer (St. Gallen's) Pathologic Features ER & PR Relative indication for chemotherapy Low expression of ER & PR (or ER[+]/PR[-]) Factors not useful for decision Relative indication for endocrine therapy alone High expression of ER & PR Histologic grade Grade 3 Grade 2 Grade 1 Proliferation High (Ki-67 >20%) Borderline (10-20%) Low (Ki-67 <10%) Nodal status Positive (4 or more) Positive (1-3 nodes) Negative LVI Presence (especially extensive) +/- Absence Tumor size (pt) > 5 cm cm < 1-2 cm *Validated multigene assays may be an adjunct to high-quality pathologic phenotyping if doubt about the indications for chemotherapy persist after consideration of all pathologic factors Multigene assay* High risk score Intermediate Low risk score Goldhirsch Annals of Oncology, 20: (2009)
17 New Approaches to an Old Problem: Prognosis, Risk, Genomic Profiling & Multigene Assays State-of-the-art molecular technology can be used to analyze global genomic changes in clinical breast cancer samples Genomic activity in early breast cancer Refine breast cancer classification Assess prognosis Assess response to therapy Garber. Science. 2004;303:
18 Two Complementary RNA Analysis Methods: Study of Gene Expression in Clinical Samples DNA Arrays (Chips) RT-PCR Assay (e.g., Genomic Health) Unfixed, frozen tissue (high quality RNA) 1000s of genes Limited dynamic range and difficult to control Fixed paraffin or unfixed tissue 10s-100s of genes Wide dynamic range, high sensitivity, specificity, reproducibility Cronin et al. Am J Pathol. 2004;164:35-42, Karsten et al. Nucleic Acids Res. 2002; 30(2):E4.
 Unfixed, frozen tissue 1000s of genes Limited dynamic range")

19 RNA Analysis Methods: Study of gene expression in clinical samples DNA Arrays (Chips) Unfixed, frozen tissue 1000s of genes Limited dynamic range and difficult to control Generates huge data sets,? Analysis? Cronin et al. Am J Pathol. 2004;164:35-42, Karsten et al. Nucleic Acids Res. 2002; 30(2):E4.

20 Gene Expression Profiling of Breast Cancer: Types of Analysis Unsupervised Cluster Analysis o Sorts tumors into related clusters based upon similarities in gene expression profiles o Dendrograms illustrate the degree of relatedness o Sorts tumors into groups of imputed biologic significance o? Clinical informative? Ramaswamy and Golub JCO 20:1932,2001 Class Discovery




21 Molecular Classification Gene Expression Profiling Basal, HER2 over-expression, Luminal A, Luminal B, ER+ ER- HER2 Lum B BLC erbb2 over-expressing Luminal B Type High proliferation index Basal Type CK5/6,17 & EGFR expression Lum A Luminal A Type Estrogen receptor positive Prognostic Significance Perou, Sorlie et al, 1999, 2000, 2001, 2003
22 Unsupervised Analysis of Breast Cancer Gene Expression Profiles (Intrinsic Molecular Subtypes) Identify reproducible, biologically distinct subgroups of breast cancers o Validated across multiple patient cohorts o Significantly different outcomes between subtypes o Differences in likelihood/patterns of recurrence o Added to our understanding of breast cancer biology/diversity Established drug targets (ER, HER2) and proliferation gene help define subgroups o Closely correlates with conventional histologic classification and IHC phenotypes of breast cancer Proc Natl Acad Sci USA 100: , 2003

23 Gene Expression Profiling of Breast Cancer: Types of Analysis Supervised Analysis o Initial step is to separate tumors into groups e.g., relapsed vs. not o Compare signatures of groups o Identify genes identifying tumor as belonging to one group or the other o Multiple tests leads to many false positives o Validation is necessary Ramaswamy and Golub JCO 20:1932,2001 Class Prediction

24 70-Gene Prognostic Signature Assay Developed Netherlands Cancer Institute Requires fresh/frozen tumor Matched BC cases with good & bad outcome - Node (-), tumors <5cm, <55 years age 70 prognosis classifier genes developed dichotomized to good or bad signature Independent predict outcome Classifier validated in 295 patients with breast cancer Nature. 2002;415: , N Eng J Med. 2002;347:
25 Probability Patients Would Remain Free of Distant Metastases & Probability of OS According to Whether They Had Good-Prognosis or Poor-Prognosis Signature Overall Good vs. Poor HR=5.1 All Pts All Pts Node - HR=5.5 Node - Node + Node + van de Vijver, M. J. et al. N Engl J Med 2002;347:
 Fixed paraffin or unfixed tissue 10s-100s of genes Wide dynamic range, high sensitivity, specificity, reproducibility Cronin et al.")
26 RNA Analysis Methods: Study of Gene Expression in Clinical Samples FFPE RT-PCR Assay (e.g., Genomic Health) Fixed paraffin or unfixed tissue 10s-100s of genes Wide dynamic range, high sensitivity, specificity, reproducibility Cronin et al. Am J Pathol. 2004;164:35-42, Karsten et al. Nucleic Acids Res. 2002; 30(2):E4.









27 Oncotype DX Technology: Candidate Gene Selection Approach From ~40,000 genes: Develop RTPCR FFPE Test candidates in 3 studies 250 cancer-related candidate genes 21 final gene set with algorithm Calculate Recurrence Score (RS) *Sources include: van't Veer et al. Nature. 2002;415: Sorlie et al. PNAS. 2001;98: Ramaswamy et al. Nat Genetics. 2003;33: Gruvberger et al. Cancer Res. 2001;61:
28 PROLIFERATION Ki-67 STK15 Survivin Cyclin B1 MYBL2 INVASION Stromolysin 3 Cathepsin L2 HER2 GRB7 HER2 Oncotype DX: 21 Gene Recurrence Score (RS) Assay 16 Cancer and 5 Reference Genes From 3 Studies ESTROGEN ER The RS recurrence = x score HER2 defined Group as: Score PR RS= x HER2 Group Score Bcl x ER Proliferation Group Score Group Score SCUBE x Proliferation Invasion Group Group Score Score x Invasion CD68 Group Score GSTM1 BAG x CD68 GSTM x GSTM1 BAG1 CD x BAG1 Scaled 0 to 100 REFERENCE Beta-actin GAPDH RPLPO GUS TFRC Coefficient x Expression Level Category Low risk Int risk High risk RS < 18 RS 18 and < 31 RS 31 Best RT-PCR performance and most robust predictors RS (0 100)
: 6.8% 10-year recurrence risk (95% CI, 4-9.6%) o Intermediate RS (19-30): 14.3% 10-year recurrence risk (95% CI, 8.3-20.3%) o High RS (31-100): 30.")
29 Clinical Data Supporting the Oncotype DX: 21 Gene Recurrence Score Validation study (NSABP B14): ER(+)/node(-) breast cancer treated with tamoxifen (Tam = benefit) o Prospective, randomized clinical trial o Low RS (0-18): 6.8% 10-year recurrence risk (95% CI, 4-9.6%) o Intermediate RS (19-30): 14.3% 10-year recurrence risk (95% CI, %) o High RS (31-100): 30.5% 10-year recurrence risk (95% CI, %) 21 gene score validated as prognostic marker for ER(+)/Node (-) patient s treated with Tam
: ER(+)/node(-) breast cancer randomized to Tam alone versus CMF + Tam")


30 Clinical Data Supporting Oncotype DX: 21 Gene Recurrence Score Validation study ( NSABP B20): ER(+)/node(-) breast cancer randomized to Tam alone versus CMF + Tam (modest benefit from + chemotherapy) o Substantial benefit from + chemo for high RS HR=0.26; 95% CI, o No benefit from + chemo for low RS HR=1.31; 95% CI, o Uncertain benefit from chemo for intermediate RS Very few cases and small number of events 21 gene score validated as predictive marker for chemotherapy benefit (CMF) ER(+)/node(-)

31 Performance of individual genes and gene clusters in predicting recurrence HER2 Group



32 B-14 Results DRFS, Multivariate Analysis Analysis without Recurrence Score Variable P Value Hazard Ratio Analysis with Recurrence Score P Value Hazard Ratio Age at surgery Clinical tumor size Tumor grade Moderately differentiated Poorly differentiated < < HER2 amplification Estrogen-receptor protein fmol/mg fmol/mg > 200 fmol/mg Recurrence Score < Only RS and poor tumor grade are independently associated with recurrence Paik et al. N Engl J Med. 2004;351:

 Both morphology & gene expression appears to track biologic characteristics which impact clinical")
33 Histopathologic Variables Predict Oncotype DX Recurrence Score R = 0.59 P<0.01 R = 0.58 P<0.01 RS - significantly correlated with tubule formation, nuclear grade, mitotic count, ER IHC score, PR IHC score & HER2 (Flanagan MB, et al. Mod Pathol. 2008) Both morphology & gene expression appears to track biologic characteristics which impact clinical behavior and outcome in breast cancer Results should correlate with one another
 Altered gene expression Altered protein expression Altered morphology Clinical Behavior Therapeutic")
34 Can GEP data be translated into IHC markers that are clinically useful and have therapeutic implications??? DNA errors (copy # changes) Altered gene expression Altered protein expression Altered morphology Clinical Behavior Therapeutic responsiveness Tumor Phenotype?



")






35 Lum A Lum B HER2-Like Basal-Like ER ER HER2 CK5 KI67 KI67 60% ER (-) Classic HER2 40% ER(+) Luminal HER2 High-Grade Ki-67-high Most Triple-Negative [ER(-), PR(-), HER2(-)] CK5/6 and/or EGFR(+) High-Grade Ki-67-high
36 Luminal A Subtype of Breast Cancer
37 Luminal A Breast Tumors: Characteristic Features Demonstrate higher level of expression of ER and ER related genes o Lower histologic grade o Lower levels of proliferation related genes o HER2 negative More indolent clinical course o May experience late recurrences Better prognosis compared with Lum-B and other subtypes



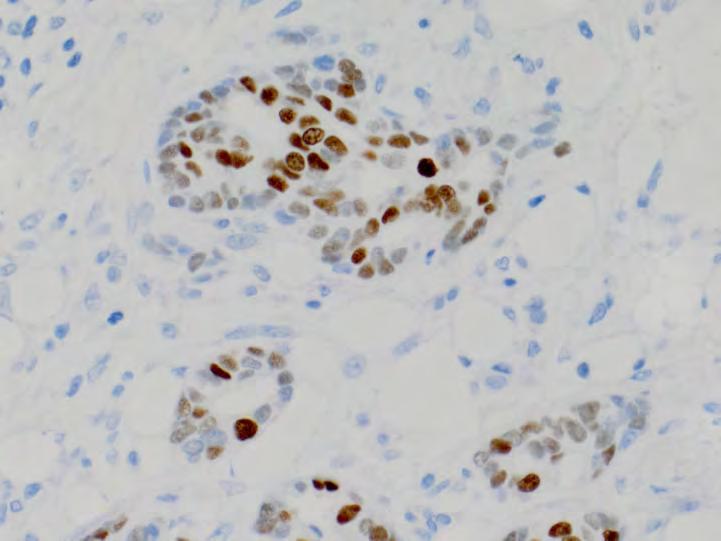
38 ER+ Breast Cancer (Luminal A) ER KI67
39 Luminal A Breast tumors Implications for therapy o Good prognosis o Respond well to endocrine therapy o May be adequately treated with hormonal therapy alone o Little if any benefit from adjuvant and neoadjuvant chemotherapy o Typically low recurrence score by 21 gene assay (Oncotype Dx)
40 Luminal B Subtype of Breast Cancer
41 Luminal-B Breast Tumors: Characteristic Features Lower levels of ER expression and ER-related genes o May be PR negative o May over-express GFR (HER2 & EGFR) Higher histologic grade More aggressive clinical course, worse prognosis o More likely lymph node positive Higher expression of proliferation related genes o KI-67 proliferation index may be useful in separating Lum B from Lum A tumors




42 ER+ Breast Cancer (Luminal-B) ER KI67






43 ER+/HER2+ Breast Cancer (Luminal-B/Luminal-HER2) ER HER2 KI67
44 Luminal-B/Luminal HER2 Breast Tumors Implication for therapy o Aggressive clinical course o May be less likely to respond to tamoxifen o More likely to benefit from chemotherapy added to endocrine treatment o Typically - high recurrence score by Oncotype Dx o Similar benefit from Herceptin+chemo compared with HER2+/ER- tumors in adjuvant clinical trials
45 IHC Classification and Prognosis Univariate survival by breast cancer subtype among 943 patients with lymph node-negative, hormone receptor-positive breast cancer who received no adjuvant systemic therapy Luminal A = ER+, and/or PR+, HER2-, Ki-67<14% Luminal B = ER+, and/or PR+, HER2-, Ki-67>14% Luminal HER2 = ER+, and/or PR+, HER2+ Cheang, J. Natl. Cancer Inst :
46 IHC Classification and Prediction Univariate survival by breast cancer subtype among 976 patients with hormone receptorpositive breast cancer who received tamoxifen as their sole adjuvant systemic therapy Luminal A = ER+, and/or PR+, HER2-, Ki-67<14% Luminal B = ER+, and/or PR+, HER2-, Ki-67>14% Luminal HER2 = ER+, and/or PR+, HER2+ Cheang, J. Natl. Cancer Inst :

47 HER2-Enriched Subtype of Breast Cancer
48 HER2+ Breast Tumors: Characteristic Features HER2+ breast tumors by GEP are ER negative o Over-expression of other genes in HER2-amplicon (GRB7, TOP2A) o High proliferative index o More likely to harbor p53 mutations o Higher histologic grade o Younger age at presentation Aggressive clinical course, poor prognosis
49 HER2+ Breast Tumors Implications for therapy o Good response to trastuzumab therapy (adjuvant and metastatic) in combination with chemotherapy o More likely to show pcr to neo-adjuvant chemotherapy + trastuzumab compared with other subtypes o More likely to respond to anthracyclines May be explain by co-amplification of TOP2A
50 Basal Subtype of Breast Cancer ( Basal-like Carcinoma)
51 Basal Subtype Breast Tumors GEP reminiscent of normal myoepithelial cells o Lack of expression of ER and related genes o Low expression of HER2, o High expression of basal cytokeratins (CK5,6,14,17) o High expression of proliferation-related genes, GFR (EGFR) Aggressive clinical course, poor prognosis o Increase likelihood of early systemic recurrence o Visceral recurrence & brain mets more likely than other subtypes Hereditary breast cancer o BRCA1 mutation generally develop basal-like breast tumors




52 Basal-Like Carcinoma: Morphologic Features & Immunophenotype (TNBC) EGFR CK 5/6
53 Basal Subtype Breast Tumors Implications for therapy o No role for endocrine therapy or trastuzumab o Aggressive clinical course = combination cytotoxic chemotherapy Absence or impaired BRCA1 function- o BRCA1 regulated repair of DNA damage (homologous recombination) o Cell lacking BRCA1 function prone to replication errors and genomic instability initiating oncogenic events o Cells dependent on less reliable mechanisms for DNA repair o Hypersensitivity to DNA damaging agents (loss of DNA repair)
54 Therapeutic Strategies in Investigation for Basal subtype breast cancer Targeting aberrant DNA repair o Platinum agents o PARP inhibitors (AZD2281; BSI-201) o Trabectedin (DNA transcription inhibitor) Antiangiogenesis o Bevacizumab o Sunitinib EGFR targeting o Cetuximab o Erlotinib Epigenetic modifications o Trichostatin A o Butyrate o Vorinostat Src inhibitor o Dasatinib Eur J Cancer Dec;44(18):
 Patient Samples (RNA) Breast Cancer Genes")

55 Translation of Gene Expression Data into 5 Reagent IHC Test for ER+/N0 Breast Cancer Patients to Determine Prognosis: Mammostrat (Applied Genomics/Clairent) Patient Samples (RNA) Breast Cancer Genes Patient Samples (paraffin blocks) Raise Poly/Monoclonal Antibodies Help predict likelihood of recurrence & likelihood of benefit from adjuvant chemo J Clin Oncol 2006 ; 24 : , Clin Cancer Res. 2008;20:




56 Five Monoclonal Immunohistochemical Assay P53 - NDRG1 - SLC7A5 - CEACAM5 - HTF9C Cox Model selects 5 antibody reagents: SLC7A5 * P53 *1.12 Low < 0 + NDRG1 *1.06 Moderate > 0 + HTF9C *0.72 High > CEACAM * = Risk Index SLC7A5 amino acid transport P53 cell cycle control NDRG1 stress/hypoxia response protein HTF9C methyl transferase gene family homology CEACAM5 embryonic expressed protein Potential to help predict likelihood of recurrence & likelihood of benefit from adjuvant chemotherapy J Clin Oncol 2006 ; 24 : , Clin Cancer Res. 2008;20:
57 NSABP B14 & B20 ER+, node negative tamoxifen-treatment arms combined NSABP/AGI B14 & B20 TAM-Treated Patients Team trial: cumulative risk of distant recurrence by Mammostrat risk index All patients Proportion of Free from Recurrence GMB=0 GMB=1 GMB=2 Log-rank test: p=0.001 Tam followed by exemestane Time in Years Clin Cancer Res. 2008;20: Low risk = 7.6% Distant recurrence at 10yrs exemestane alone High risk = 20.9% Distant recurrence at 10yrs p=0.003 Bartlett J M et al. JCO 2012;30: Bartlett et al, BCR 2010
58 IHC Approach for Profiling Breast Cancer Advantages o Wide availability o Cost/TAT o Morphologic confirmation of tissue Disadvantages o Susceptibility to preanalytic variables o Qualitative evaluation and readout Needs: o Establish optimal antibody reagents/panels o Correlation of results with outcome/response o Standardized tissue handling/fixation protocols o Standarized assay procedures, controls, criterion for interpretation o Quantitative results (image analysis)

59 Take Home Message: Intrinsic Properties of Breast Cancer & Clinical Course: Proliferation is Critically Important! Intrinsic Biologic Properties of Tumor Patient Tumor Burden Wound signature Genomic Grade Index Tumor Size & Nodal Status 70 gene signature 76 gene signature High Tumor Proliferation Aggressive Clinical Course Poor Prognosis 21 gene recurrence score Intrinsic Molecular Classification Proliferation genes common driving force in prognostic signatures Tumor burden independently associated with prognosis Sotiriou and Paccart, 2007
60 Risk Assessment and Acceptance of Tumor Markers: Balance of Carrots and Sticks Intrinsic Molecular Classification Technical validation Genomic Grade Index Rapid Clinical Acceptance Patient and clinician desire Financial and academic benefits 70 gene signature 76 gene signature 21 gene recurrence score IHC antibody panels Validated Clinical Utility LOE I studies Financial burden Low Payoff Clinical validation

 Tumor Burden Molecular")


61 Take Home Message: Integration of Profiling/Molecular Testing into Treatment Planning Clinical Presentation Proliferation and Differentiation (Grade) Tumor Burden Molecular results must correlate with clinical & pathologic features Does this all Make sense? Discordance with clinical or pathologic findings must be reconciled prior to treatment decisions Pathologist s are perfectly position to do integrate these results 61
62 Next in the Hot Topics in Pathology Webinar Series Transforming the Diagnostic Evaluation of Inherited Disorders with Next-Generation Sequencing Tuesday, April 23, 10:00-11:00 AM Central o Karl V Voelkerding, MD, FCAP The commercial introduction of next-generation sequencing (NGS) in 2005 ushered in a new era in biomedical research. Now eight years later, NGS is being increasingly applied as a molecular diagnostic tool in fields as diverse as oncology, infectious diseases and inherited disorders. This presentation will highlight how NGS is transforming the diagnostic evaluation of inherited disorders. Emphasized will be the growing adoption of NGS as a methodological approach for performing multi-gene panel and exome sequencing. Multi-gene panels are being employed in a variety of inherited disorders wherein mutations in any one of several genes can result in phenotypic overlap. Exome sequencing is being leveraged to identify causal and candidate genes in patients with undiagnosed disorders. For both of these use case scenarios, the presentation will address technical, bioinformatics and reporting considerations and challenges. As a powerful new diagnostic modality, NGS offers unique practice opportunities for pathologists in the emerging era of genomic medicine. Register by going to College of American Pathologists. All rights reserved. 62
63 Access Archived Webinars-View Recording & Download Presentation PDF go to Archived Webinars on Getting Started and Taking Next Steps in Molecular Pathology The Why, What, and How of Identifying Patients at Risk for Hereditary Cancer Syndromes in Surgical Pathology Practice (Alexis Carter, MD, FCAP) Molecular Tests and Pathology Practice: What Every Community Pathologist Should Know/Clinical Requests for Molecular Tests (Alexis B Carter, MD, FCAP) How to Build and Fund a Viable Molecular Lab (Frederick Kiechle, MD, PhD, FCAP) Cancer: The Critical Role of Pathology in Personalized Health Care (Eric Walk, MD, FCAP) Archived Webinars on Genomic Analysis, Large Molecular Panels, Exome, Genome Whole Genome Analysis as a Universal Diagnostic: A Pathologist s Perspective (Mark Boguski MD, PhD, FCAP) Clinical Use of Whole Genomic and Whole Exome Today(Paula North, MD, FCAP and David Bick MD) Next-Generation Sequencing for the Clinical Laboratory (Karl V. Voelkerding, MD, FCAP) Next-Generation Sequencing: Just Another Lab Test (John Pfeifer, MD, FCAP) 2011 College of American Pathologists. All rights reserved. 63
64 Access Archived Webinars-View Recording & Download Presentation PDF go to Archived Webinars on Organ Based Pathology Molecular Diagnosis for Colorectal Cancer Patients (Antonia R. Sepulveda MD, PhD, FCAP) Molecular Testing Guidelines for Selection of EGFR and ALK Tynsine Karnase Inhibitors in Non-Small Cell Lung Cancer (Neal I Lindeman, MD, FCAP and Marc Ladanyi, MD, FCAP) Molecular Diagnostics of Lung Cancer (John Iafrate, MD, PhD) Molecular Testing and Hematopathologic Conditions (David Czuchlewski, MD, and Mohammad Vasef, MD, FCAP) Molecular Genetics of Pancreatic Neoplasms (Ralph Hruban, MD) 2012 College of American Pathologists. All rights reserved. 64
65 CAP Learning Molecular Markers in Breast Cancer Course Archives Applied - Metaplastic Breast Carcinoma and Mimickers (SAM eligible) CME/SAM 1.0 Archives Applied - Molecular Pathology of Breast Cancer (SAM eligible) CME/SAM 1.0 Learning Objectives -Identify the key morphologic features for diagnosing metaplastic carcinomas with low-grade spindle cell morphology. -Recognize the most useful pathologic and immunohistochemical features in the differential diagnosis of metaplastic carcinoma. -Identify key diagnostic features in core biopsy samples for the diagnosis of metaplastic carcinoma. -Recognize the four groups of spindle cell lesions to consider when evaluating atypical spindle cell proliferation in the breast. Identify challenges in the diagnosis of metaplastic carcinomas. -Recognize the challenges of making an accurate morphologic classification of breast carcinoma. -Recognize the advantages of brightfield in situ hybridization methods over fluorescence in situ hybridization (FISH) detection methods. -Differentiate the most commonly recognized molecular subtypes of breast carcinoma. -Identify the advantages and disadvantages of array-based comparative genomic hybridization (acgh) in classifying breast neoplasms. -Identify the advantages and disadvantages of matrix-assisted laser desorption/ionization (MALDI) imaging mass spectrometry for investigating breast neoplasms College of American Pathologists. All rights reserved. 65
66 CAP Learning Molecular Markers in Breast Cancer Course BPF Testing Self Study (SAM eligible) CME/SAM 2.5 ER IHC Test Interpretation Accuracy (SAM eligible) CME/SAM 2.0 HER2 IHC Test Interpretation Accuracy (SAM eligible) CME/SAM 2.0 Use of Immunohistochemistry in the Diagnosis of Breast Lesions (SAM eligible) CME/SAM 1.5 Learning Objectives -Explain the ASCO-CAP ER/PR Testing Guidelines and their implications for lab procedures, test results and patient care. -Explain the ASCO-CAP HER2 Testing Guidelines and their implications for lab procedures, test results and patient care. -Determine if the assay and tissue sample are appropriately matched per the ASCO/CAP Guidelines. -Explain the biology of fixation interactions with assay performance. -Explain the potential use of molecular analysis in patient care decisions. -Plan and perform a proper ER IHC test validation. -Accurately perform and interpret ER IHC tests, including the proper evaluation of appropriate controls and test tissues. -Evaluate and integrate ER staining patterns with clinical and morphologic findings. -Identify the relationship and impact of ER IHC test results on patient treatment. -Plan and perform a proper HER2 IHC test validation in accordance with ASCO- CAP guidelines for HER2 testing. -Accurately perform and interpret HER2 IHC tests, including the proper evaluation of appropriate controls and test tissues. -Evaluate and integrate HER2 staining patterns with clinical and morphologic findings to help improve concordance with HER2 FISH results. -Identify the relationship and impact of HER2 IHC test results on patient treatment. -Interpret commonly used immunohistochemical studies. -Recognize potential interpretative pitfalls. -Utilize correlative morphologic features to avoid misdiagnosis College of American Pathologists. All rights reserved. 66
67 CAP Learning Molecular Markers in Breast Cancer Course Validation of ER and PgR IHC Assays (SAM eligible) CME/SAM 1.5 HER2 FISH Test Interpretation Accuracy (SAM eligible) CME/SAM 1.5 BPFT Reporting (SAM eligible) CME/SAM 1.5 Learning Objectives -Distinguish between validation and verification of an ER/PgR assay and when each is required. -Describe an appropriate sample set for an ER/PgR assay validation or verification study. -Identify appropriate test conditions and requirements for an ER/PgR assay validation or verification study. -Accurately interpret HER2 FISH tests. -Correct for HER2 FISH interpretative errors. -Recognize the relationship between HER2 FISH test results and patient treatment. -Apply the ASCO-CAP ER/PR and HER2 Guideline criteria to all reports in a standardized manner. -Create consistent, standardized and integrated reports. -Remediate inconsistent data and provide a resolution in an integrated report. -Create patient friendly reports. -Use formatting techniques to create clear and understandable reports College of American Pathologists. All rights reserved. 67


68 CAP Learning Portal CAP Learning Portal The CAP Learning Portal includes content and tools designed to support the learning needs of pathologists. A user must login to cap.org in order to access the portal. In the portal, you will find: o o o o o Learning Options search/catalog Competency Model for Pathologists Personal Progress Check My Learning Plan Help Center (Guides, Video, FAQs) Benefits Increase effectiveness to plan and manage learning Increase efficiency to target learning needs and identify premium learning solutions Increase satisfaction with learning solutions that meet specific learner needs Increase capability to maintain professional certifications 2013 College of American Pathologists. All rights reserved. 68

69 To learn more For more details and to register for/access educational offerings: 1. Log in to the cap.org website 2. Click on the Learning Portal tab. 3. Click on the Browse Our Learning Catalog tab 4. Type your desired topic in the Search box or make a selection from the list provided. A list of available learning options displays 2013 College of American Pathologists. All rights reserved. 69
70 A New CAP Tool- Short Presentations On Emerging Concepts (SPECs) Pathology SPECs are: o o short PowerPoint presentations, created for pathologists, focused on selected diseases where molecular tests play a key role in patient management. valuable resource for your discussions with Tumor Boards or other physician colleagues. Now Available: Emerging Concepts in the Workup of Colorectal Cancer Emerging Concepts in Therapeutic Guidance for Metastatic Melanoma Emerging Concepts in the Diagnosis and Workup of Thyroid Cancer Emerging Concepts in Colorectal Cancer Hereditary Non-Polyposis Cancer (Lynch Syndrome) Emerging Concepts in the Workup of Polycythemia and Thrombocythemia: JAK2 To register, go to the CAP Member tab on cap.org. You do not need to be a member to utilize this free tool College of American Pathologists. All rights reserved. 70

71 A New CAP Tool-Pathology Resource Guides The CAP has created the Pathology Resource Guides, a new tool to assist pathologists in understanding key emering technologies. These Resource Guides are a new CAP member benefit available at no charge. Molecular Diagnostic (small panel, single gene) Genomic Analysis (large molecular panels, exome, genome) Digital Pathology In Vivo Microscopy Register through the CAP member tab. You will receive periodic updates for two years. Questions? Contact capguides@cap.org College of American Pathologists. All rights reserved. 71

72

73 CAP 2013 Policy Meeting

74 2012 College of American Pathologists. All rights reserved.
75 THANK YOU! Thank you for attending our webinar Molecular Markers in Breast Cancer by David G Hicks, MD, FCAP. For comments about this webinar or suggestions for upcoming webinars, please contact Jill Kaufman, PhD, Director of Personalized Health Care at jkaufma@cap.org NOTE: There is no CME/CE credit available for today s free webinar. 75
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Molecular Characterization of Breast Cancer: The Clinical Significance
 Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013
 Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
30 years of progress in cancer research
 Breast Cancer Molecular Knowledge Integrated in Clinical Practice Personalized Medicine Laura J. Esserman UCSF Comprehensive Cancer Center Retreat Breast Cancer Management Advances 80-90s 1) Screening
Breast Cancer Molecular Knowledge Integrated in Clinical Practice Personalized Medicine Laura J. Esserman UCSF Comprehensive Cancer Center Retreat Breast Cancer Management Advances 80-90s 1) Screening
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
Genomic Profiling of Tumors and Loco-Regional Recurrence
 1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
She counts on your breast cancer expertise at the most vulnerable time of her life.
 HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
The Oncotype DX Assay A Genomic Approach to Breast Cancer
 The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
Breast cancer classification: beyond the intrinsic molecular subtypes
 Breast cancer classification: beyond the intrinsic molecular subtypes Britta Weigelt, PhD Signal Transduction Laboratory CRUK London Research Institute Summary Breast cancer heterogeneity Molecular classification
Breast cancer classification: beyond the intrinsic molecular subtypes Britta Weigelt, PhD Signal Transduction Laboratory CRUK London Research Institute Summary Breast cancer heterogeneity Molecular classification
Rationale For & Design of TAILORx. Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York
 Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Morphological and Molecular Typing of breast Cancer
 Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
BREAST CANCER. Dawn Hershman, MD MS. Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center.
 BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors)
") Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer
 Node Positive Breast Cancer") Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Modern classification of breast cancer-should we stick with morphology or convert to molecular profiles?
 Modern classification of breast cancer-should we stick with morphology or convert to molecular profiles? Ian Ellis Professor of Cancer Pathology Molecular Medical Sciences University of Nottingham Dept
Modern classification of breast cancer-should we stick with morphology or convert to molecular profiles? Ian Ellis Professor of Cancer Pathology Molecular Medical Sciences University of Nottingham Dept
Harmesh Naik, MD. Hope Cancer Clinic
 Harmesh Naik, MD. Hope Cancer Clinic A brief review of adjuvant therapy of breast cancer Summarize selected new developments in adjuvant therapy of breast cancer Discussion is limited to early stage breast
Harmesh Naik, MD. Hope Cancer Clinic A brief review of adjuvant therapy of breast cancer Summarize selected new developments in adjuvant therapy of breast cancer Discussion is limited to early stage breast
Immunohistochemical classification of breast tumours
 Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
Bradley M Turner MD, MPH, MHA. Assistant Professor University of Rochester Department of Pathology and Laboratory Medicine
 Bradley M Turner MD, MPH, MHA Assistant Professor University of Rochester Department of Pathology and Laboratory Medicine My real job!!! I have nothing to disclose although Oncotype Dx year end revenues
Bradley M Turner MD, MPH, MHA Assistant Professor University of Rochester Department of Pathology and Laboratory Medicine My real job!!! I have nothing to disclose although Oncotype Dx year end revenues
The Current Status and the Future Prospects of Multigene testing in Europe
 The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
Carcinome du sein Biologie moléculaire. Thomas McKee Service de Pathologie Clinique Genève
 Carcinome du sein Biologie moléculaire Thomas McKee Service de Pathologie Clinique Genève Pathology Diagnostic Prognostic information Predictive information The information provided depends on the available
Carcinome du sein Biologie moléculaire Thomas McKee Service de Pathologie Clinique Genève Pathology Diagnostic Prognostic information Predictive information The information provided depends on the available
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER
 OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
A new way of looking at breast cancer tumour biology
 A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
Harmesh Naik, MD. Hope Cancer Clinic PERSONALIZED CANCER TREATMENT USING LATEST IN MOLECULAR BIOLOGY
 Harmesh Naik, MD. Hope Cancer Clinic PERSONALIZED CANCER TREATMENT USING LATEST IN MOLECULAR BIOLOGY A NEW GENE A DAY.WHILE YOU ARE ENJOYING MORNING COFFEE From cancer.gov GOALS FOR THE CME TODAY A brief
Harmesh Naik, MD. Hope Cancer Clinic PERSONALIZED CANCER TREATMENT USING LATEST IN MOLECULAR BIOLOGY A NEW GENE A DAY.WHILE YOU ARE ENJOYING MORNING COFFEE From cancer.gov GOALS FOR THE CME TODAY A brief
Question 1 A. ER-, PR-, HER+ B. ER+, PR+, HER2- C. ER-, PR+, HER2- D. ER-, PR-, HER2- E. ER-, PR+, HER2+
 Triple Negative Breast Cancer Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Question 1 The tumor depicted on the next slide
Triple Negative Breast Cancer Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Question 1 The tumor depicted on the next slide
Adjuvan Chemotherapy in Breast Cancer
 Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Profili di espressione genica
 Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
10/15/2012. Biologic Subtypes of TNBC. Topics. Topics. Histopathology Molecular pathology Clinical relevance
 Biologic Subtypes of TNBC Andrea L. Richardson M.D. Ph.D. Brigham and Women s Hospital Dana-Farber Cancer Institute Harvard Medical School Boston, MA Topics Histopathology Molecular pathology Clinical
Biologic Subtypes of TNBC Andrea L. Richardson M.D. Ph.D. Brigham and Women s Hospital Dana-Farber Cancer Institute Harvard Medical School Boston, MA Topics Histopathology Molecular pathology Clinical
Molecular classification of breast cancer implications for pathologists. Sarah E Pinder
 Molecular classification of breast cancer implications for pathologists Sarah E Pinder Courtesy of CW Elston Histological types Breast Cancer Special Types 17 morphological special types 25-30% of all
Molecular classification of breast cancer implications for pathologists Sarah E Pinder Courtesy of CW Elston Histological types Breast Cancer Special Types 17 morphological special types 25-30% of all
Seigo Nakamura,M.D.,Ph.D.
 Seigo Nakamura,M.D.,Ph.D. Professor of Surgery Director of Breast Center Showa University Hospital Chairman of the board of directors Japan Breast Cancer Society Inhibition of Estrogen-Dependent Growth
Seigo Nakamura,M.D.,Ph.D. Professor of Surgery Director of Breast Center Showa University Hospital Chairman of the board of directors Japan Breast Cancer Society Inhibition of Estrogen-Dependent Growth
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
FAQs for UK Pathology Departments
 FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
RNA preparation from extracted paraffin cores:
 Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Breast Cancer Heterogeneity
 Breast Cancer Heterogeneity Session 2: 8:15 AM 9:00 AM Molecular Subsets and Molecular Diagnostics in Breast Cancer ER + subtypes ER-negative subtypes Lisa A. Carey, MD University of North Carolina Lineberger
Breast Cancer Heterogeneity Session 2: 8:15 AM 9:00 AM Molecular Subsets and Molecular Diagnostics in Breast Cancer ER + subtypes ER-negative subtypes Lisa A. Carey, MD University of North Carolina Lineberger
TAILORx: Established and Potential Implications for Clinical Practice
 TAILORx: Established and Potential Implications for Clinical Practice Joseph A. Sparano, MD Study Chair, TAILORx Vice-Chair, ECOG-ACRIN Cancer Research Group Hello Healthcare Summit Berlin, Germany March
TAILORx: Established and Potential Implications for Clinical Practice Joseph A. Sparano, MD Study Chair, TAILORx Vice-Chair, ECOG-ACRIN Cancer Research Group Hello Healthcare Summit Berlin, Germany March
Reporting of Breast Cancer Do s and Don ts
 Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX
 High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX Test: An Independent Quality Assurance Study DAVID J DABBS, MD Professor and Chief of Pathology
High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX Test: An Independent Quality Assurance Study DAVID J DABBS, MD Professor and Chief of Pathology
THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE. Dr Husam Marashi 03/02/2017
 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE Dr Husam Marashi 03/02/2017 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER TODAY S TALK: CENTRE EXPERIENCE
THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE Dr Husam Marashi 03/02/2017 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER TODAY S TALK: CENTRE EXPERIENCE
Luminal A and B Where are we? (or lost in translation?)
") Luminal A and B Where are we? (or lost in translation?) Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam How to determine adjuvant or neoadjuvant treatment for
Luminal A and B Where are we? (or lost in translation?) Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam How to determine adjuvant or neoadjuvant treatment for
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
ISPOR 4 th Asia Pacific Conference IP2 Gilberto de Lima Lopes
 Health Economic Considerations for Personalized Medicine in Asia: Using Genomic Profiling to Guide Treatment Decisions in Early Breast Cancer Gilberto de Lima Lopes, Jr., M.D., M.B.A Assistant Director
Health Economic Considerations for Personalized Medicine in Asia: Using Genomic Profiling to Guide Treatment Decisions in Early Breast Cancer Gilberto de Lima Lopes, Jr., M.D., M.B.A Assistant Director
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI
 Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
FISH mcgh Karyotyping ISH RT-PCR. Expression arrays RNA. Tissue microarrays Protein arrays MS. Protein IHC
 Classification of Breast Cancer in the Molecular Era Susan J. Done University Health Network, Toronto Why classify? Prognosis Prediction of response to therapy Pathogenesis Invasive breast cancer can have
Classification of Breast Cancer in the Molecular Era Susan J. Done University Health Network, Toronto Why classify? Prognosis Prediction of response to therapy Pathogenesis Invasive breast cancer can have
Adjuvant endocrine therapy (essentials in ER positive early breast cancer)
") Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
The TAILORx Trial: A review of the data and implications for practice
 The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
Reliable Evaluation of Prognostic & Predictive Genomic Tests
 Reliable Evaluation of Prognostic & Predictive Genomic Tests Richard Simon, D.Sc. Chief, Biometric Research Branch National Cancer Institute http://brb.nci.nih.gov Different Kinds of Biomarkers Prognostic
Reliable Evaluation of Prognostic & Predictive Genomic Tests Richard Simon, D.Sc. Chief, Biometric Research Branch National Cancer Institute http://brb.nci.nih.gov Different Kinds of Biomarkers Prognostic
Making Understanding Molecular Profiles Less Painful. Presenter Disclosure Information
 Welcome to Master Class for Oncologists Miami, FL December 18, 2009 Session 1: 1:00 PM - 1:45 PM Towards Personalized Medicine in Breast Cancer: Understanding Molecular Subtypes and the Role of Diagnostics
Welcome to Master Class for Oncologists Miami, FL December 18, 2009 Session 1: 1:00 PM - 1:45 PM Towards Personalized Medicine in Breast Cancer: Understanding Molecular Subtypes and the Role of Diagnostics
Present Role of Immunohistochemistry in the. Subtypes. Beppe Viale European Institute of Oncology University of Milan Milan-Italy
 Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
Post Neoadjuvant therapy: issues in interpretation
 Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón
 Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
Oncotype DX reveals the underlying biology that changes treatment decisions 37% of the time
 Oncotype DX reveals the underlying biology that changes treatment decisions 37% of the time Even when treatment decisions based on traditional measures seem conclusive, Oncotype DX can lead to a different
Oncotype DX reveals the underlying biology that changes treatment decisions 37% of the time Even when treatment decisions based on traditional measures seem conclusive, Oncotype DX can lead to a different
Intro to Cancer Therapeutics
 An Intro to Cancer Therapeutics Christopher R. Chitambar, MD Professor of Medicine Division of Hematology & Oncology Froedtert and Medical College of Wisconsin Clinical Cancer Center cchitamb@mcw.edu Intro
An Intro to Cancer Therapeutics Christopher R. Chitambar, MD Professor of Medicine Division of Hematology & Oncology Froedtert and Medical College of Wisconsin Clinical Cancer Center cchitamb@mcw.edu Intro
Biologic Subtypes and Prognos5c Factors. Claudine Isaacs, MD Georgetown University
 Biologic Subtypes and Prognos5c Factors Claudine Isaacs, MD Georgetown University Prognos5c Factor Defini5on Predicts outcome in absence of systemic therapy Thus tell us when (not how) to treat a pa5ent
Biologic Subtypes and Prognos5c Factors Claudine Isaacs, MD Georgetown University Prognos5c Factor Defini5on Predicts outcome in absence of systemic therapy Thus tell us when (not how) to treat a pa5ent
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
The Latest Research: Hormonal Therapies
 The Latest Research: Hormonal Therapies Sameer Gupta, M.D., M.P.H 9/29/2018 Attending Physician, Hematology/Oncology Bryn Mawr Hospital Clinical Assistant Professor, Jefferson Medical College Disclosures
The Latest Research: Hormonal Therapies Sameer Gupta, M.D., M.P.H 9/29/2018 Attending Physician, Hematology/Oncology Bryn Mawr Hospital Clinical Assistant Professor, Jefferson Medical College Disclosures
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions
 1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
Breast cancer pathology
 Breast cancer pathology Giancarlo Pruneri, M.D. National Cancer Institute (INT) Milan University of Milan, School of Medicine Giancarlo.Pruneri@unimi.it Currently accepted prognostic/predictive parameters
Breast cancer pathology Giancarlo Pruneri, M.D. National Cancer Institute (INT) Milan University of Milan, School of Medicine Giancarlo.Pruneri@unimi.it Currently accepted prognostic/predictive parameters
Breast Cancer: Who Gets It? Who Survives? The Latest Information
 Breast Cancer: Who Gets It? Who Survives? The Latest Information James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine
Breast Cancer: Who Gets It? Who Survives? The Latest Information James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine
Genomic platforms in breast cancer
 Genomic platforms in breast cancer Prof. Miguel Martín Instituto de Investigación Sanitaria Hospital Gregorio Marañón Universidad Complutense Madrid mmartin@geicam.org Disclosure Dr. Martin has received
Genomic platforms in breast cancer Prof. Miguel Martín Instituto de Investigación Sanitaria Hospital Gregorio Marañón Universidad Complutense Madrid mmartin@geicam.org Disclosure Dr. Martin has received
Kathy Albain, MD. Chemotherapy in Luminal Breast Cancer: Who Benefits? Loyola University Chicago Stritch School of Medicine
 Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Session thématisée Les Innovations diagnostiques en cancérologie
 10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer
10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer
Understanding and Optimizing Treatment of Triple Negative Breast Cancer
 Understanding and Optimizing Treatment of Triple Negative Breast Cancer Edith Peterson Mitchell, MD, FACP Clinical Professor of Medicine and Medical Oncology Program Leader, Gastrointestinal Oncology Department
Understanding and Optimizing Treatment of Triple Negative Breast Cancer Edith Peterson Mitchell, MD, FACP Clinical Professor of Medicine and Medical Oncology Program Leader, Gastrointestinal Oncology Department
Evolution of Pathology
 1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Clinical Next Generation Sequencing: Just Another Lab Test
 Hot Topics in Pathology Series Clinical Next Generation Sequencing: Just Another Lab Test The presentation will start momentarily! cap.org v. # Hot Topics in Pathology Series Clinical Next Generation Sequencing:
Hot Topics in Pathology Series Clinical Next Generation Sequencing: Just Another Lab Test The presentation will start momentarily! cap.org v. # Hot Topics in Pathology Series Clinical Next Generation Sequencing:
Comparison of prognostic signatures for ER positive breast cancer in TransATAC:
 Comparison of prognostic signatures for ER positive breast cancer in TransATAC: EndoPredict, a high performance test in node negative and node positive disease Ivana Sestak, PhD Centre for Cancer Prevention
Comparison of prognostic signatures for ER positive breast cancer in TransATAC: EndoPredict, a high performance test in node negative and node positive disease Ivana Sestak, PhD Centre for Cancer Prevention
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
MammaPrint, the story of the 70-gene profile
 MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany
 Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany Triple-Negative Breast Cancer (TNBC) 2018 Presentation Outline The molecular heterogeneity
Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany Triple-Negative Breast Cancer (TNBC) 2018 Presentation Outline The molecular heterogeneity
GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN
 GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN Adam Brufsky, MD, PhD Professor of Medicine Associate Chief, Hematology-Oncology Associate Director, Clinical Investigation University
GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN Adam Brufsky, MD, PhD Professor of Medicine Associate Chief, Hematology-Oncology Associate Director, Clinical Investigation University
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology
 XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
HER2 status assessment in breast cancer. Marc van de Vijver Academic Medical Centre (AMC), Amsterdam
, Amsterdam") HER2 status assessment in breast cancer Marc van de Vijver Academic Medical Centre (AMC), Amsterdam 13e Bossche Mamma Congres 17 th June 2015 Modern cancer therapies are based on sophisticated molecular
HER2 status assessment in breast cancer Marc van de Vijver Academic Medical Centre (AMC), Amsterdam 13e Bossche Mamma Congres 17 th June 2015 Modern cancer therapies are based on sophisticated molecular
Session II: Academic Research in Breast Cancer: Challenges and Opportunities Robert L. Comis, MD ECOG-ACRIN Group Co-Chair
 Session II: Academic Research in Breast Cancer: Challenges and Opportunities Robert L. Comis, MD ECOG-ACRIN Group Co-Chair Symposium: Innovation in Breast Cancer 2014 Madrid, Spain February 21, 2014 Cancer
Session II: Academic Research in Breast Cancer: Challenges and Opportunities Robert L. Comis, MD ECOG-ACRIN Group Co-Chair Symposium: Innovation in Breast Cancer 2014 Madrid, Spain February 21, 2014 Cancer
Low ER+ Breast Cancer. Is This a Distinct Group? Nika C. Gloyeske, MD, David J. Dabbs, MD, and Rohit Bhargava, MD ABSTRACT
 Low ER+ Breast Cancer Is This a Distinct Group? Nika C. Gloyeske, MD, David J. Dabbs, MD, and Rohit Bhargava, MD From the Magee-Womens Hospital of University of Pittsburgh Medical Center, Pittsburgh, PA.
Low ER+ Breast Cancer Is This a Distinct Group? Nika C. Gloyeske, MD, David J. Dabbs, MD, and Rohit Bhargava, MD From the Magee-Womens Hospital of University of Pittsburgh Medical Center, Pittsburgh, PA.
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
patients in the era of
 Communicating with cancer patients in the era of personalized medicine September 9 th, 2017 Gerald Prager, M.D. Comprehensive Cancer Center Vienna Medical University of Vienna, Austria Gerald Prager, M.D.
Communicating with cancer patients in the era of personalized medicine September 9 th, 2017 Gerald Prager, M.D. Comprehensive Cancer Center Vienna Medical University of Vienna, Austria Gerald Prager, M.D.
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer. California Technology Assessment Forum
 As a Guide for the Management of Early Stage Breast Cancer. California Technology Assessment Forum") TITLE: The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department
TITLE: The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department
Janet E. Dancey NCIC CTG NEW INVESTIGATOR CLINICAL TRIALS COURSE. August 9-12, 2011 Donald Gordon Centre, Queen s University, Kingston, Ontario
 Janet E. Dancey NCIC CTG NEW INVESTIGATOR CLINICAL TRIALS COURSE August 9-12, 2011 Donald Gordon Centre, Queen s University, Kingston, Ontario Session: Correlative Studies in Phase III Trials Title: Design
Janet E. Dancey NCIC CTG NEW INVESTIGATOR CLINICAL TRIALS COURSE August 9-12, 2011 Donald Gordon Centre, Queen s University, Kingston, Ontario Session: Correlative Studies in Phase III Trials Title: Design
Postoperative Adjuvant Chemotherapies. Stefan Aebi Luzerner Kantonsspital
 Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/55957 holds various files of this Leiden University dissertation Author: Dekker T.J.A. Title: Optimizing breast cancer survival models based on conventional
Cover Page The handle http://hdl.handle.net/1887/55957 holds various files of this Leiden University dissertation Author: Dekker T.J.A. Title: Optimizing breast cancer survival models based on conventional
Personalized Treatment of DCIS
 Global Breast Cancer Conference 2016 [The Shilla Hotel, Jeju] Symposium 1 : DCIS - What s New? (14:40-15:50) Personalized Treatment of DCIS 2016. 4. 28. Breast Division, Department of Surgery Sungkyunkwan
Global Breast Cancer Conference 2016 [The Shilla Hotel, Jeju] Symposium 1 : DCIS - What s New? (14:40-15:50) Personalized Treatment of DCIS 2016. 4. 28. Breast Division, Department of Surgery Sungkyunkwan
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival