Better Outcomes for Lung Cancer in Family Practice. AProf Jeff Garrett Respiratory Physician
|
|
|
- Oliver Stokes
- 6 years ago
- Views:
Transcription

1 Better Outcomes for Lung Cancer in Family Practice AProf Jeff Garrett Respiratory Physician
2 Lung Cancer Leading cause of cancer death in NZ overall Maori have especially poor lung cancer outcomes 19% cancer deaths in NZ ~1500 deaths annually

3 5yr Relative Survival (NZ)
4
5 Lung cancer 5 year Survival NZ




6 Identification of Barriers to the Early Diagnosis of Lung Cancer and Description of Best Practice Solutions Wendy Stevens, Jeff Garrett, Chris Lewis, Denise Aitken et al Cancer Trials New Zealand, the University of Auckland 6 September Funded by a Health Research Council of New Zealand & District Health Boards New Zealand Grant
7 Our Barriers to Early Diagnosis 1. Presentation/Attendance Barriers 2. Identification Barriers 3. Waiting Time Barriers 4. Information Barriers
8 Survival & Stage 5 year survival strongly related to stage at diagnosis NSCLC Stage I/II >50% (73% with surgery) III 15% IV 3% Worldwide, poor survival outcomes from lung cancer are largely attributed to late presentation Currently majority present with advanced disease Audits (2004 & 2008) in the Northern Region NZ >70% have incurable disease at diagnosis (IIIB/IV NSCLC; extensive SCLC) Unaware symptoms serious Nihilistic attitudes death sentence nothing can be done
9 Clinical Management Findings from Audits (2004 & 2008) in Northern Region Low investigation rates in 1 0 care 65% CXR prior to 2 0 care (98% Canada) 11% chest CT prior to 2 0 care (56% Canada) - poor GP access to CTs High proportion (44%) present acutely to 2 0 care (UK 21%); Only 26% GP referred to Respiratory Specialist!!! (UK 45%)
10 Clinical Management cont Lower treatment rates (curative & palliative intent) in NZ Surgical resection rate (2004 audit): Overall NZ 14% 20-24% (USA, Europe) I/II NSCLC NZ 49% 65-84% (72% Australia) Any anticancer treatment : NZ 50% 68-75% OS Palliative Radiation Rx NZ 40% 72% OS
11 Summary of the clinical standards for the management of lung cancer services 1. Timely access to services Standard 1: Patients requiring active treatment shall start treatment within 62 calendar days of receipt of referral by secondary care. Standard 2: Patients with clinical and/or radiological signs and symptoms suggestive of lung cancer should be seen by a specialist with an interest in respiratory medicine within 14 calendar days of receipt of referral by secondary care. Standard 3: Chest x-ray should be performed for all patients with symptoms suggestive of lung cancer and should be reported back to the referrer within 7 calendar days (immediately) of receipt of referral by the radiology service provider. 2. Communication and referral Standard 4: Formal referral pathway and required information should be agreed between primary, secondary and tertiary care. Communications between health care providers should include patient s name, date of birth, National Health Index (NHI) and should ideally be electronic. 3. Data collection Standard 5: All patients with lung cancer should be entered into a lung cancer database. 4. Investigations Standard 6: CT should be performed before a bronchoscopy. Standard 7: All cancer centres should have timely access to endobronchial ultrasound (EBUS). Standard 8: Staging PET-CT should be performed in patients with suspected or confirmed non-small cell lung cancer suitable for potentially radical treatment with the exception of peripheral T1aN0 tumours.
12 Summary of the clinical standards for the management of lung cancer services cont 5. Multidisciplinary care Standard 9: All patients with lung cancer should be discussed at a multidisciplinary meeting. 6. Smoking cessation Standard 10: All current smokers and their family/whānau should be offered smoking cessation advice and support to quit where appropriate. 7. Care coordination Standard 11: All patients with suspected lung cancer should have a nominated single point of contact, ideally a cancer nurse, to provide psychosocial support, information and coordination of a patient s journey. Contact will be made with the patient within 7 calendar days of the initial assessment with a specialist. 8. Palliative care Standard 12: Patients, who cannot be offered curative treatment, as well as those with significant symptom burden, should be offered early access to palliative care services. 9. Active anticancer treatment There is no specific standard for active anticancer treatment. However timely active anticancer treatment is important and is incorporated in the 62 calendar day wait time target between receipt of referral and start of treatment (see Standard 1). 10. Follow-up Standard 13: All patients and their general practitioners should be given written information regarding a follow-up plan (including frequency of visits, required tests if needed and with which designated service) together with a nominated point of contact if there is a clinical concern.
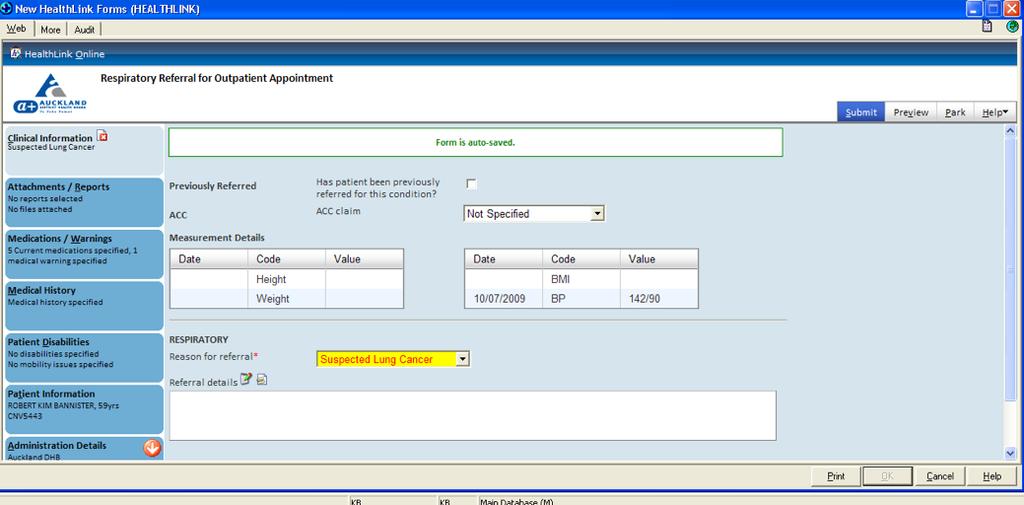
13

14 When you click on Help Referral Guidelines
15 Lung Cancer Pathway Lung cancer Primary Care Indicator two (best practise 14 days) Urgent referral with highsuspicion of cancer CT First specialist assessment Indicator three (best practise 31 days) Decision-to-treat First cancer treatment Indicator one (best practise 62 days) Includes diagnostics, surgical & nonsurgical treatments All cancers by tumour stream
16 Lung cancer Pathway High Suspicion Lung Cancer Referral CT Respiratory FSA (< 14 days) CT report Bronchoscopy CT-FNA Biopsy extra thoracic lesion Bronchoscopy report (< 3 days) ~35% non diagnostic CT-FNA report (<1-3 days) Biopsy report (< 3 days) ~65% diagnostic TMDM (< 14 days after FSA) When there is a high suspicion of cancer ensure that you complete Referral to Respiratory Referral to CT


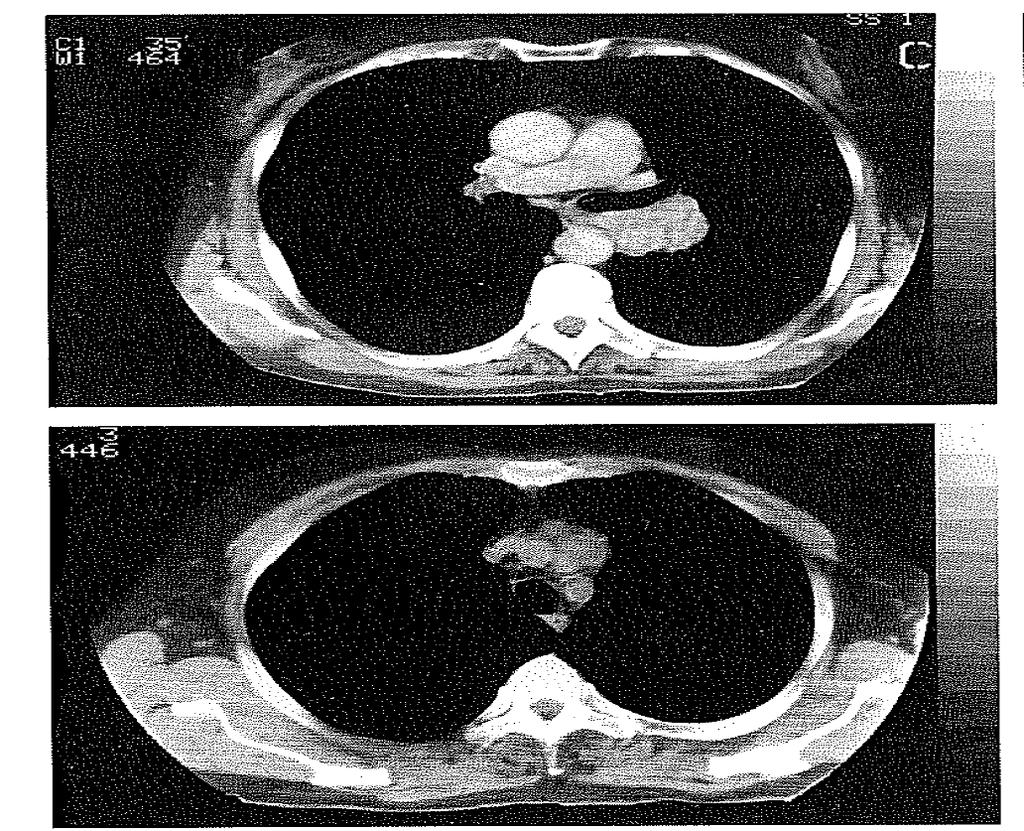
17 Fig 10. Pancost s tumour. There is a mass at the left apex on the frontal view. Close inspection shows destruction of the posterior half of the second rib and part of the third rib. CT section through the tumour shows its proximity to the posterior ends of the ribs and partial destruction of the ribs and adjacent vertebral body.
18
19 Profile of a Patient that should be referred urgently for a chest x-ray Unexplained haemoptysis OR Any of the following unexplained, persistent (lasting more than 3 weeks or less than 3 weeks in people with known risk factors) symptoms and signs: Chest and/or shoulder pain Shortness of breath /cough Weight loss/loss of appetite Abnormal chest signs (eg fixed wheeze, focal signs) Hoarseness Finger clubbing Cervical and/or supraclavicular lymphadenopathy Features suggestive of metastasis from a lung cancer (e.g., in brain, bone, liver or skin)
20 Background Why don t we screen for lung cancer? If you screen 1000 patients for lung cancer, you Find 9 stage 1 lung cancers Find 235 false positive lung nodules, (determined by further tests or follow up) Perform 4 thoracotomies for benign disease Risk of over-diagnosis of cancers that would never have become clinically apparent We need to be smarter at selecting patients with the highest risk of lung cancer, to reduce false positives Gopal et al. J Thorac Oncol 2010; 5:
21 NLST: Screening with CT vs CXR improves survival, but cost effectiveness data is awaited
 Emphysema/COPD (20-30% of smokers) Lancet Oncology")
22 Hypothesis: COPD and lung cancer genetic overlap? Lung Cancer (10-15% of smokers) Emphysema/COPD (20-30% of smokers) Lancet Oncology 2011; 12; July, 623. Young & Hopkins

23 Risk Profile Cigarettes Lung Cancer Emphysema/COPD
24 Palliative Care
25 Useful Website Guide
26 Key Take Home Messages Prevent lung cancer Ask about smoking status; offer support to quit Recognition of lung cancer Pts with emphysema at highest risk (+FH/PH cancer) Persistent cough (longer than 3 weeks) not responding to treatment most common symptom Low threshold for ordering Chest Xray Order CT chest at time of specialist referral (sputums/bloods) DHBs are now required to see and treat your patient quickly; most are already doing so
27 Lung Cancer Survival Rates

28 Faster Cancer Treatment Indicator Report
29 Northern Region DHBs Northland Waitemata Auckland Counties Manukau 1. Timely access to services 1) Patients requiring active treatment should start treatment within 62 calendar days of secondary care receiving a referral. 2) Patients with clinical and/or radiological signs and symptoms suggestive of lung cancer should be seen by a specialist with an interest in respiratory medicine within 14 calendar days of secondary care receiving a referral. 3) Chest X-rays should be performed for all patients with symptoms suggestive of lung cancer and should be reported back to the referrer within seven calendar days of the radiology service provider receiving a referral. 93% 57% 65% 63% 68% 72% 84% 69% 2. Communication and referral 4) The formal referral pathway and required information should be agreed between primary, secondary and tertiary care. Communications between health care providers include the patient s name, date of birth, NHI number, ethnicity and contact details, and are ideally electronic. Key: Meets standard or expected performance level (at least 75%) Partially achieved, needs improvement or performance level is between 50% and 74% Does not meet standard or performance level is below 50% Inadequate information available
30 Northern Region DHBs Northland Waitemata Auckland Counties Manukau 3. Data Collection 5) All patients with lung cancer should be entered into a lung cancer database. 4. Investigations 6) Computed tomography (CT) should be performed before a bronchoscopy. 7) All cancer centres should have timely access to endobronchial ultrasound (EBUS). 8) Staging PET-CT should be performed in patients with suspected or confirmed non-smallcell lung cancer suitable for potentially radical treatment, with the exception of peripheral T1aN0 tumours. Key: Meets standard or expected performance level (at least 75%) Partially achieved, needs improvement or performance level is between 50% and 74% Does not meet standard or performance level is below 50% Inadequate information available
31 Northern Region DHBs Northland Waitemata Auckland Counties Manukau 5. Multidisciplinary care 9) All patients with lung cancer should be discussed at a multidisciplinary meeting. 6. Smoking cessation 10) All current smokers and their family/whanau should be offered smoking cessation advice and support to quit, where appropriate. 7. Care co-ordination 11) All patients with suspected lung cancer should have a nominated single point of contact, ideally a nurse who specialises in cancer care, to provide psychosocial support, information and co-ordination of a patient s cancer journey. Contact will be made with the patient within seven calendar days of the initial assessment with a specialist. 98% 96% 95% 95% Key: Meets standard or expected performance level (at least 75%) Partially achieved, needs improvement or performance level is between 50% and 74% Does not meet standard or performance level is below 50% Inadequate information available
32 Northern Region DHBs Northland Waitemata Auckland Counties Manukau 8. Palliative care 12) Patients who cannot be offered curative treatment, as well as those with a significant symptom burden, should be offered early access to palliative care services. 9. Active anti-cancer treatment There is no specific standard for active anticancer treatment. However, timely active anticancer treatment is important and is incorporated in the 31 day wait time indicator between decision to treatment and start of treatment. 10. Follow-up 13) All patients and their general practitioners should be given written information regarding a follow up plan (including frequency of visits, tests required and with which designated service), together with a nominated point of contact if there is a clinical concern. Key: Meets standard or expected performance level (at least 75%) Partially achieved, needs improvement or performance level is between 50% and 74% Does not meet standard or performance level is below 50% Inadequate information available 93% 68% 74% 63%
Dr Greg Frazer. Respiratory Physician Christchurch Hospital Christchurch. 15:10-15:35 Primary and Secondary Healthcare Interface Supported by:
 Dr Greg Frazer Respiratory Physician Christchurch Hospital Christchurch 15:10-15:35 Primary and Secondary Healthcare Interface Supported by: Primary and Secondary Healthcare Interface How Working Together
Dr Greg Frazer Respiratory Physician Christchurch Hospital Christchurch 15:10-15:35 Primary and Secondary Healthcare Interface Supported by: Primary and Secondary Healthcare Interface How Working Together
Clinical Audit Report
 Clinical Audit Report The Lung Cancer Pathway from Initial Presentation to Healthcare Services until Diagnosis (Auckland & Lakes Regions) Identification of Barriers to the Early Diagnosis of People with
Clinical Audit Report The Lung Cancer Pathway from Initial Presentation to Healthcare Services until Diagnosis (Auckland & Lakes Regions) Identification of Barriers to the Early Diagnosis of People with
Investigating Symptoms of Lung Cancer An evidence based Guide for general practitioners
 Medicine, Nursing and Health Sciences Investigating Symptoms of Lung Cancer An evidence based Guide for general practitioners Dr Kay Jones Professor Danielle Mazza Dr Samantha Chakraborty Prof essor Ian
Medicine, Nursing and Health Sciences Investigating Symptoms of Lung Cancer An evidence based Guide for general practitioners Dr Kay Jones Professor Danielle Mazza Dr Samantha Chakraborty Prof essor Ian
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Resources for health professionals (3) Risk Factors (5) Initial investigations (8) Red Flag (9) Diagnosis and staging (12)
 Risk Factors (5) Initial investigations (8) Red Flag (9) Diagnosis and staging (12)") Lung Cancer Care map information (1) Resources for patients, families and carers (2) Resources for health professionals (3) Aboriginal and Torres Strait Islander Health (4) Risk Factors (5) Red Flag (7)
Lung Cancer Care map information (1) Resources for patients, families and carers (2) Resources for health professionals (3) Aboriginal and Torres Strait Islander Health (4) Risk Factors (5) Red Flag (7)
National Optimal Lung Cancer Pathway
 National Optimal Lung Cancer Pathway This document was produced by the Lung Clinical Expert Group 2017 Document Title: National Optimal Lung Cancer Pathway and Implementation Guide Date of issue: August
National Optimal Lung Cancer Pathway This document was produced by the Lung Clinical Expert Group 2017 Document Title: National Optimal Lung Cancer Pathway and Implementation Guide Date of issue: August
MANAGING LUNG CANCER GP CME South Roland Meyer Respiratory Physician, Southern DHB
 MANAGING LUNG CANCER GP CME South 19.8.12 Roland Meyer Respiratory Physician, Southern DHB 137R.00 137S.00 It takes years to be detectable 27 tumor doublings for 1cm Spirometry to identify those at risk
MANAGING LUNG CANCER GP CME South 19.8.12 Roland Meyer Respiratory Physician, Southern DHB 137R.00 137S.00 It takes years to be detectable 27 tumor doublings for 1cm Spirometry to identify those at risk
Faster Cancer Treatment Indicators: Use cases
 Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
NICE Quality Standards and COF
 NICE Quality Standards and COF David Baldwin Consultant Respiratory Physician NUH Hon Senior Lecturer Nottingham University Clinical lead NICE lung cancer GL Chair NICE QS Topic Expert Group Quality Standards
NICE Quality Standards and COF David Baldwin Consultant Respiratory Physician NUH Hon Senior Lecturer Nottingham University Clinical lead NICE lung cancer GL Chair NICE QS Topic Expert Group Quality Standards
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
National Optimal Lung Cancer Pathways. Dr Sadia Anwar Nottingham University Hospitals NHS Trust Clinical Lead for Lung Cancer
 National Optimal Lung Cancer Pathways Dr Sadia Anwar ttingham University Hospitals NHS Trust Clinical Lead for Lung Cancer Overview How NOLCP evolved How it relates to national guidance Pathways Implementation
National Optimal Lung Cancer Pathways Dr Sadia Anwar ttingham University Hospitals NHS Trust Clinical Lead for Lung Cancer Overview How NOLCP evolved How it relates to national guidance Pathways Implementation
Lung Cancer Case Study
 Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
LUNG CANCER SCREENING: LUNG CANCER SCREENING: THE TIME HAS COME LUNG CANCER: A NATIONAL EPIDEMIC
 : THE TIME HAS COME Physician Leader, Lung Cancer Multi-Disciplinary Program Fletcher Allen Health Care Annual Meeting Montpelier, VT - April 25, 2014 Gerald S. Davis, MD Professor of Medicine University
: THE TIME HAS COME Physician Leader, Lung Cancer Multi-Disciplinary Program Fletcher Allen Health Care Annual Meeting Montpelier, VT - April 25, 2014 Gerald S. Davis, MD Professor of Medicine University
There are a number of national guidelines and performance standards which support the implementation of a straight to CT pathway.
 December 2015 CONTENTS Contents... 2 1 Introduction... 3 2 Case for Change... 3 3 Evidence... 3 3.1 National and regional policy... 3 3.2 Local audit... 4 4 Supporting Work Initiatives... 5 4.1 Identification
December 2015 CONTENTS Contents... 2 1 Introduction... 3 2 Case for Change... 3 3 Evidence... 3 3.1 National and regional policy... 3 3.2 Local audit... 4 4 Supporting Work Initiatives... 5 4.1 Identification
ACE Programme SOMERSET INTEGRATED LUNG CANCER PATHWAY. Phases One and Two Final Report
 ACE Programme SOMERSET INTEGRATED LUNG CANCER PATHWAY Phases One and Two Final Report July 2017 Introduction This paper presents the learning and actions that have been generated from phase One and Two
ACE Programme SOMERSET INTEGRATED LUNG CANCER PATHWAY Phases One and Two Final Report July 2017 Introduction This paper presents the learning and actions that have been generated from phase One and Two
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Ambulatory lung biopsy: a new model for the NHS. Dr Sam Hare Barnet Hospital Royal Free London NHS Trust
 Ambulatory lung biopsy: a new model for the NHS Dr Sam Hare Barnet Hospital Royal Free London NHS Trust Lung cancer Leading cause of UK cancer mortality UK: 2 nd lowest European survival rate 62-day RTT
Ambulatory lung biopsy: a new model for the NHS Dr Sam Hare Barnet Hospital Royal Free London NHS Trust Lung cancer Leading cause of UK cancer mortality UK: 2 nd lowest European survival rate 62-day RTT
Lung cancer forms in tissues of the lung, usually in the cells lining air passages.
 Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM)
") SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
LCA Lung Clinical Forum. 21 st October 2014
 LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
National Cancer Programme. Work Plan 2015/16
 National Cancer Programme Work Plan 2015/16 Citation: Ministry of Health. 2015. National Cancer Programme: Work plan 2015/16. Wellington: Ministry of Health. Published in October 2015 by the Ministry of
National Cancer Programme Work Plan 2015/16 Citation: Ministry of Health. 2015. National Cancer Programme: Work plan 2015/16. Wellington: Ministry of Health. Published in October 2015 by the Ministry of
Days. Visits, Tests and Procedures
 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 SURGICAL, MED ONC OR
01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 SURGICAL, MED ONC OR
National Cancer Programme. Work Plan 2014/15
 National Cancer Programme Work Plan 2014/15 Citation: Ministry of Health. 2014. National Cancer Programme: Work Plan 2014/15. Wellington: Ministry of Health. Published in December 2014 by the Ministry
National Cancer Programme Work Plan 2014/15 Citation: Ministry of Health. 2014. National Cancer Programme: Work Plan 2014/15. Wellington: Ministry of Health. Published in December 2014 by the Ministry
Better community respiratory care. Dr Roland Meyer Respiratory Physician Southern DHB August 2010
 Better community respiratory care Dr Roland Meyer Respiratory Physician Southern DHB August 2010 Integration : What is needed? Raise profile of disease Strong management in primary care Good communication
Better community respiratory care Dr Roland Meyer Respiratory Physician Southern DHB August 2010 Integration : What is needed? Raise profile of disease Strong management in primary care Good communication
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
A community based intervention for rural Maori at risk of lung cancer
 A community based intervention for rural Maori at risk of lung cancer Ross Lawrenson, Jacquie Kidd, Chunhuan Lao, Rawiri Keenan, Anna Rolleston, Brendan Hokowhitu, Denise Aitken, Janice Wong Background
A community based intervention for rural Maori at risk of lung cancer Ross Lawrenson, Jacquie Kidd, Chunhuan Lao, Rawiri Keenan, Anna Rolleston, Brendan Hokowhitu, Denise Aitken, Janice Wong Background
Lung health and you. Looking after your lungs and steps to stay well.
 Lung health and you Looking after your lungs and steps to stay well www.roycastle.org Staying well Your lungs supply oxygenated blood to your heart and other vital organs. Your lungs can be damaged by
Lung health and you Looking after your lungs and steps to stay well www.roycastle.org Staying well Your lungs supply oxygenated blood to your heart and other vital organs. Your lungs can be damaged by
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD. November 18, 2017
 Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Information for. Patients with an Abnormal Lung X-ray
 Information for Patients with an Abnormal Lung X-ray Some of the materials in this resource were adapted with permission from: Understanding Lung Cancer, Juravinski Cancer Centre, Hamilton Health Sciences,
Information for Patients with an Abnormal Lung X-ray Some of the materials in this resource were adapted with permission from: Understanding Lung Cancer, Juravinski Cancer Centre, Hamilton Health Sciences,
Screening for Lung Cancer - State of the Art
 Screening for Lung Cancer - State of the Art Rohit Kumar, MD Assistant Professor of Medicine Fox Chase Cancer Center Temple University School of Medicine Philadelphia, PA Objectives Review current evidence
Screening for Lung Cancer - State of the Art Rohit Kumar, MD Assistant Professor of Medicine Fox Chase Cancer Center Temple University School of Medicine Philadelphia, PA Objectives Review current evidence
Lung Cancer and the Cancer Alliance DR JAMES RAMSAY
 Lung Cancer and the Cancer Alliance DR JAMES RAMSAY Background Lung cancer is the second commonest cancer in the UK (37,000 new cases in England each year). Commonest cause of cancer death (28,500 people
Lung Cancer and the Cancer Alliance DR JAMES RAMSAY Background Lung cancer is the second commonest cancer in the UK (37,000 new cases in England each year). Commonest cause of cancer death (28,500 people
None
 2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
Lung cancer case finding in COPD using low-dose CT
 Lung cancer case finding in COPD using low-dose CT The South Tyneside Model Part of: South Tyneside and Sunderland Healthcare Group Ross T., Fuller E. Lung cancer Largest cause of cancer-related death
Lung cancer case finding in COPD using low-dose CT The South Tyneside Model Part of: South Tyneside and Sunderland Healthcare Group Ross T., Fuller E. Lung cancer Largest cause of cancer-related death
Lung Cancer Screening: To Screen or Not to Screen?
 Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer
: Targeting Lung Cancer") Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
Lung Cancer: Diagnosis, Staging and Treatment
 PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer starts in your cells. Cells are the building blocks of your tissues. Tissues make up the organs of your
PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer starts in your cells. Cells are the building blocks of your tissues. Tissues make up the organs of your
Christine Argento, MD Interventional Pulmonology Emory University
 Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
How can we facilitate cross-boundary working in Greater Manchester?
 How can we facilitate cross-boundary working in Greater Manchester? Emma Halkyard Nurse Clinician Cross boundary working: where are we now? Our patients are complex Our pathways are complex Our treatments
How can we facilitate cross-boundary working in Greater Manchester? Emma Halkyard Nurse Clinician Cross boundary working: where are we now? Our patients are complex Our pathways are complex Our treatments
2016 Public Reporting of Outcomes Standard 1.12
 2016 Public Reporting of Outcomes Standard 1.12 Roland Matthews MD, Director GCCE Sheryl Gabram MD, Deputy Director GCCE Pooja Mishra FACHE, Executive Director GCCE Top 5 Primary Sites 250 200 150 100
2016 Public Reporting of Outcomes Standard 1.12 Roland Matthews MD, Director GCCE Sheryl Gabram MD, Deputy Director GCCE Pooja Mishra FACHE, Executive Director GCCE Top 5 Primary Sites 250 200 150 100
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM)
") SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician GMCN ROYAL WOLVERHAMPTON HOSPITALS The Royal Wolverhampton Hospitals Trust Lung MDT (11-2C-1) - 2011/12 Dr Angela Morgan
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician GMCN ROYAL WOLVERHAMPTON HOSPITALS The Royal Wolverhampton Hospitals Trust Lung MDT (11-2C-1) - 2011/12 Dr Angela Morgan
Early Detection of Lung Cancer
 UK Data Archive Study Number 6647 - National Awareness and Early Diagnosis Initiative: Cancer Awareness Measure, Doncaster, 2008: Special Licence Access Early Detection of Lung Cancer Information for General
UK Data Archive Study Number 6647 - National Awareness and Early Diagnosis Initiative: Cancer Awareness Measure, Doncaster, 2008: Special Licence Access Early Detection of Lung Cancer Information for General
Guide to Understanding Lung Cancer
 Guide to Understanding Lung Cancer Lung cancer is the second most common cancer overall for men and women in the U.S., with an estimated 222,500 new cases in 2017. However, lung cancer is the most common
Guide to Understanding Lung Cancer Lung cancer is the second most common cancer overall for men and women in the U.S., with an estimated 222,500 new cases in 2017. However, lung cancer is the most common
Clinical Advice to Cancer Alliances for the Commissioning of the whole Lung Cancer Pathway
 Clinical Advice to Cancer Alliances for the Commissioning of the whole Lung Cancer Pathway This document was produced by the Lung Cancer Clinical Expert August 2017 Document Title: Clinical Advice to Cancer
Clinical Advice to Cancer Alliances for the Commissioning of the whole Lung Cancer Pathway This document was produced by the Lung Cancer Clinical Expert August 2017 Document Title: Clinical Advice to Cancer
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Lung Cancer Imaging Guidelines: Integration with the Lung Cancer Diagnosis and Staging Clinical Pathway
 Lung Cancer Imaging Guidelines: Integration with the Lung Cancer Diagnosis and Staging Clinical Pathway Cancer Imaging Guidance L-1 Version 1 January 2014 Cancer Imaging Program Cancer Care Ontario Page
Lung Cancer Imaging Guidelines: Integration with the Lung Cancer Diagnosis and Staging Clinical Pathway Cancer Imaging Guidance L-1 Version 1 January 2014 Cancer Imaging Program Cancer Care Ontario Page
Diagnosing Cancer in Grampian An Academic GP s Perspective
 Diagnosing Cancer in Grampian An Academic GP s Perspective Dr Peter Murchie Academic Primary Care, Research Group Hilton Edinburgh Carlton 6 th September 2018 A sense of perspective? Douglas Adams The
Diagnosing Cancer in Grampian An Academic GP s Perspective Dr Peter Murchie Academic Primary Care, Research Group Hilton Edinburgh Carlton 6 th September 2018 A sense of perspective? Douglas Adams The
Small Cell Lung Cancer
 Small Cell Lung Cancer Small cell lung cancer (SCLC) affects 15% of all lung cancer patients. SCLC is the most aggressive type of lung cancer. It may be treated with chemotherapy and radiation. SCLC has
Small Cell Lung Cancer Small cell lung cancer (SCLC) affects 15% of all lung cancer patients. SCLC is the most aggressive type of lung cancer. It may be treated with chemotherapy and radiation. SCLC has
GCE AS/A level 1661/01-A APPLIED SCIENCE UNIT 1
 GCE AS/A level 1661/01-A APPLIED SCIENCE UNIT 1 S16-1661-01A Pre-release Article for Examination in May 2016 1661 01A001 CJ*(S16-1661-01A) 2 Information for Teachers The pre-release article is intended
GCE AS/A level 1661/01-A APPLIED SCIENCE UNIT 1 S16-1661-01A Pre-release Article for Examination in May 2016 1661 01A001 CJ*(S16-1661-01A) 2 Information for Teachers The pre-release article is intended
Urgent referral for suspected cancer in Scotland
 270 Oncology Urgent referral for suspected cancer in Scotland Cancer is a common problem, but an individual GP may only see about seven to eight new cases of cancer per annum (although they will see many
270 Oncology Urgent referral for suspected cancer in Scotland Cancer is a common problem, but an individual GP may only see about seven to eight new cases of cancer per annum (although they will see many
The Management of Lung Cancer. Pathway of Care. Kent & Medway Cancer Collaborative
 Kent & Medway Cancer Collaborative The Management of Lung Cancer Pathway of Care Publication date April 2014 Expected review date April 2016 Version number 5.0 Version status Final/Published Table of Contents
Kent & Medway Cancer Collaborative The Management of Lung Cancer Pathway of Care Publication date April 2014 Expected review date April 2016 Version number 5.0 Version status Final/Published Table of Contents
North of England Cancer Network. NECN Lung Cancer Clinical Guidelines
 North of England Cancer Network Lung Cancer Clinical Guidelines Lung NSSG on behalf of NECN Document Information Title: NECN Lung Cancer Clinical Guidelines Author: Lung NSSG Members Circulation List:
North of England Cancer Network Lung Cancer Clinical Guidelines Lung NSSG on behalf of NECN Document Information Title: NECN Lung Cancer Clinical Guidelines Author: Lung NSSG Members Circulation List:
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Early Detection of Lung Cancer. Amsterdam March 5 th 2010
 Early Detection of Lung Cancer Amsterdam March 5 th 2010 Rob J van Klaveren, MD, PhD Dept. of Pulmonology Erasmus MC Rotterdam, the Netherlands Early Detection and Screening - Questions to be addressed
Early Detection of Lung Cancer Amsterdam March 5 th 2010 Rob J van Klaveren, MD, PhD Dept. of Pulmonology Erasmus MC Rotterdam, the Netherlands Early Detection and Screening - Questions to be addressed
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Screening for Lung Cancer
 Screening for Lung Cancer 15 ΜΑΡΤΙΟΥ 2014 Ioannis Gkiozos Pulmonologist Oncology Unit G P General & Chest Diseases Hospital Sotiria Despite advances in therapy, 5-year survival rates of Lung Cancer Remains
Screening for Lung Cancer 15 ΜΑΡΤΙΟΥ 2014 Ioannis Gkiozos Pulmonologist Oncology Unit G P General & Chest Diseases Hospital Sotiria Despite advances in therapy, 5-year survival rates of Lung Cancer Remains
Lung Cancer Screening: Evidence and current recommendations
 Lung Cancer Screening: Evidence and current recommendations 20 th March 2018 Dr Annette McWilliams Fiona Stanley Hospital University of Western Australia WA Cancer & Palliative Care Network I have no financial
Lung Cancer Screening: Evidence and current recommendations 20 th March 2018 Dr Annette McWilliams Fiona Stanley Hospital University of Western Australia WA Cancer & Palliative Care Network I have no financial
Disclosures. Overview. Selection the most accurate statement: Updates in Lung Cancer Screening 5/26/17. No Financial Disclosures
 Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Streamlining the lung diagnostic pathway (A87)
") Streamlining the lung diagnostic pathway (A87) Crawley CCG with Surrey and Sussex Healthcare NHS Trust Evaluation January 2017 Summary A new Straight-to-CT pathway for patients with an abnormal CXR result
Streamlining the lung diagnostic pathway (A87) Crawley CCG with Surrey and Sussex Healthcare NHS Trust Evaluation January 2017 Summary A new Straight-to-CT pathway for patients with an abnormal CXR result
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Tongue cancer. Patient information
 What is cancer? The human body is made up of billions of cells. In healthy people, cells grow, divide and die. New cells constantly replace old ones in an orderly way. This process ensures each part of
What is cancer? The human body is made up of billions of cells. In healthy people, cells grow, divide and die. New cells constantly replace old ones in an orderly way. This process ensures each part of
Ghosts in the Machine: Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand
 Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Will CT screening reduce overall lung cancer mortality? Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH
 Will CT screening reduce overall lung cancer mortality? Heidi Roberts MD FRCP(C) Heidi Roberts, MD, FRCP(C) Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH Screening - Requirements
Will CT screening reduce overall lung cancer mortality? Heidi Roberts MD FRCP(C) Heidi Roberts, MD, FRCP(C) Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH Screening - Requirements
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
Lung Cancer Screening:
 Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
Effectiveness of the Get Checked diabetes programme
 Effectiveness of the Get Checked diabetes programme This is an independent report published under section 21 of the Public Audit Act 2001. September 2010 ISBN 978-0-478-32675-8 (online) 2 Contents Auditor-General
Effectiveness of the Get Checked diabetes programme This is an independent report published under section 21 of the Public Audit Act 2001. September 2010 ISBN 978-0-478-32675-8 (online) 2 Contents Auditor-General
Referral of Suspected Lung Cancer by Family Physicians and Other Primary Care Providers
 Evidence-Based Series 24-2 IN REVIEW Referral of Suspected Lung Cancer by Family Physicians and Other Primary Care Providers L. Del Giudice, S. Young, E. Vella, M. Ash, P. Bansal, A. Robinson, R. Skrastins,
Evidence-Based Series 24-2 IN REVIEW Referral of Suspected Lung Cancer by Family Physicians and Other Primary Care Providers L. Del Giudice, S. Young, E. Vella, M. Ash, P. Bansal, A. Robinson, R. Skrastins,
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Supporting information for the Report on National Gynaecological Oncology Service Provision Models
 Discussion document Supporting information for the Report on National Gynaecological Oncology Service Provision Models Sub Group of the National Gynaecological Cancer Working Group 26 November 2013 For
Discussion document Supporting information for the Report on National Gynaecological Oncology Service Provision Models Sub Group of the National Gynaecological Cancer Working Group 26 November 2013 For
LUNGS? YOU GET THESE YOUR GUIDE TO YEARLY LUNG CANCER SCREENING CHECKED REGULARLY. WHAT ABOUT YOUR. Think. Screen. Know.
 YOU GET THESE CHECKED REGULARLY. WHAT ABOUT YOUR LUNGS? YOUR GUIDE TO YEARLY LUNG CANCER SCREENING WHAT YOU SHOULD KNOW BEFORE, DURING, AND AFTER Think. Screen. Know. Talk to your doctor. TABLE OF CONTENTS
YOU GET THESE CHECKED REGULARLY. WHAT ABOUT YOUR LUNGS? YOUR GUIDE TO YEARLY LUNG CANCER SCREENING WHAT YOU SHOULD KNOW BEFORE, DURING, AND AFTER Think. Screen. Know. Talk to your doctor. TABLE OF CONTENTS
Evaluation of Cancer Outcomes Barwon South West Registry
 Evaluation of Cancer Outcomes Barwon South West Registry Data Request Form Applicant details Applicant name: Position: Email: Project start date: Date: Telephone: Project completion date: Project details
Evaluation of Cancer Outcomes Barwon South West Registry Data Request Form Applicant details Applicant name: Position: Email: Project start date: Date: Telephone: Project completion date: Project details
Improving diagnostic pathways for patients with vague symptoms
 Improving diagnostic pathways for patients with vague symptoms Executive summary Accelerate, Coordinate, Evaluate (ACE) Programme An early diagnosis of cancer initiative supported by: NHS England, Cancer
Improving diagnostic pathways for patients with vague symptoms Executive summary Accelerate, Coordinate, Evaluate (ACE) Programme An early diagnosis of cancer initiative supported by: NHS England, Cancer
Pulmonary Nodules. Michael Morris, MD
 Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
The Maine Lung Cancer Coalition. Working Together to Reduce Lung Cancer in Maine
 The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center
 You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
Report to Waikato Medical Research Foundation
 Report to Waikato Medical Research Foundation Understanding the importance of tumour biology and socio-demographic difference in cancer stage at diagnosis using the Midland Lung Cancer Register Ross Lawrenson
Report to Waikato Medical Research Foundation Understanding the importance of tumour biology and socio-demographic difference in cancer stage at diagnosis using the Midland Lung Cancer Register Ross Lawrenson
Lung Cancer Screening
 Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
Single Suspected Cancer Pathway Definitions pathway start date
 Single Suspected Cancer Pathway Definitions pathway start date Date: March 2018 Version: 1.2.1 Wales Cancer Owner: Network and Welsh Government Status Published 1 P a g e Purpose of Document This document
Single Suspected Cancer Pathway Definitions pathway start date Date: March 2018 Version: 1.2.1 Wales Cancer Owner: Network and Welsh Government Status Published 1 P a g e Purpose of Document This document
A Comprehensive Cancer Center Designated by the National Cancer Institute
 N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
SHARED DECISION MAKING AND LUNG CANCER SCREENING
 SHARED DECISION MAKING AND LUNG CANCER SCREENING DISCLOSURES Cathleen E. Morrow, MD None William C. Black, MD No financial disclosure Co-investigator for NLST Member of the ACR Lung-RADS Screening Registry
SHARED DECISION MAKING AND LUNG CANCER SCREENING DISCLOSURES Cathleen E. Morrow, MD None William C. Black, MD No financial disclosure Co-investigator for NLST Member of the ACR Lung-RADS Screening Registry
LOOKING BACK FROM THE
 The Clerk s tale EARLY DIAGNOSIS: LOOKING BACK FROM THE ONCOLOGY CLINIC Peter Johnson Professor of Medical Oncology, University of Southampton Chief Clinician, Cancer Research UK A 47 year-old lady Diabetic
The Clerk s tale EARLY DIAGNOSIS: LOOKING BACK FROM THE ONCOLOGY CLINIC Peter Johnson Professor of Medical Oncology, University of Southampton Chief Clinician, Cancer Research UK A 47 year-old lady Diabetic
Lung Cancer Screening: To screen or not to screen?
 Lung Cancer Screening: To screen or not to screen? Dan J. Raz, M.D. Co Director, Lung Cancer Screening Program Co Director, LungCancer and Thoracic OncologyProgram Assistant Professor, Thoracic Surgery
Lung Cancer Screening: To screen or not to screen? Dan J. Raz, M.D. Co Director, Lung Cancer Screening Program Co Director, LungCancer and Thoracic OncologyProgram Assistant Professor, Thoracic Surgery
The RAPID Programme Rapid Access to Pulmonary Investigation & Diagnosis
 Patient Experience National Network Awards (PENNA) The RAPID Programme 2016-2019 Rapid Access to Pulmonary Investigation & Diagnosis Kath Hewitt Lead Clinical Nurse Specialist Ailsa Rowlands Programme
Patient Experience National Network Awards (PENNA) The RAPID Programme 2016-2019 Rapid Access to Pulmonary Investigation & Diagnosis Kath Hewitt Lead Clinical Nurse Specialist Ailsa Rowlands Programme
Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services. Cancer of Unknown Primary Network Site Specific Group. Clinical Guidelines
 Cancer Services. Cancer of Unknown Primary Network Site Specific Group. Clinical Guidelines") Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services Cancer of Unknown Primary Network Site Specific Group Revision due: April 2019 Page 1 of 11 VERSION CONTROL THIS IS A CONTROLLED DOCUMENT.
Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services Cancer of Unknown Primary Network Site Specific Group Revision due: April 2019 Page 1 of 11 VERSION CONTROL THIS IS A CONTROLLED DOCUMENT.
SCREENING FOR EARLY LUNG CANCER. Pang Yong Kek
 SCREENING FOR EARLY LUNG CANCER Pang Yong Kek Lecture Outline Why performing screening? How to improve early detection? Benefits and Risks of screening Challenges in screening Conclusion Why Performing
SCREENING FOR EARLY LUNG CANCER Pang Yong Kek Lecture Outline Why performing screening? How to improve early detection? Benefits and Risks of screening Challenges in screening Conclusion Why Performing
Tests Your Pulmonologist Might Order. Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Lung cancer is the leading cause of cancer death in New
 ORIGINAL ARTICLE Lung Cancer in New Zealand: Patterns of Secondary Care and Implications for Survival Wendy Stevens, MBBS,* Graham Stevens, MD, FRANZCR,* John Kolbe, MBBS, FRACP, and Brian Cox, MB, ChB,
ORIGINAL ARTICLE Lung Cancer in New Zealand: Patterns of Secondary Care and Implications for Survival Wendy Stevens, MBBS,* Graham Stevens, MD, FRANZCR,* John Kolbe, MBBS, FRACP, and Brian Cox, MB, ChB,
REFERRAL GUIDELINES RESPIRATORY
 REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Lung cancer. The diagnosis and treatment of lung cancer. Issued: April NICE clinical guideline 121. guidance.nice.org.
 Lung cancer The diagnosis and treatment of lung cancer Issued: April 2011 NICE clinical guideline 121 guidance.nice.org.uk/cg121 NICE has accredited the process used by the Centre for Clinical Practice
Lung cancer The diagnosis and treatment of lung cancer Issued: April 2011 NICE clinical guideline 121 guidance.nice.org.uk/cg121 NICE has accredited the process used by the Centre for Clinical Practice
Professor John K Field PhD, FRCPath University of Liverpool Cancer Research Centre, UK.
 Professor John K Field PhD, FRCPath University of Liverpool Cancer Research Centre, UK. J.K.Field@liv.ac.uk 1.8 million new cases in 2012 Bender Nature Outlook 2014 Probability of survival: ALL participants
Professor John K Field PhD, FRCPath University of Liverpool Cancer Research Centre, UK. J.K.Field@liv.ac.uk 1.8 million new cases in 2012 Bender Nature Outlook 2014 Probability of survival: ALL participants
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Screening for Lung Cancer: New Guidelines, Old Problems
 Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
Current Approach to Screening for Lung Cancer. James R Jett M.D.
 Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Staging Issues: Lung Cancer & Mesothelioma. Mick Peake Clinical Lead, NCIN Chair, Lung SSCRG
 Staging Issues: Lung Cancer & Mesothelioma Mick Peake Clinical Lead, NCIN Chair, Lung SSCRG Staging systems Non-Small Cell Lung Cancer (>85%): UICC TNM v6 used until 1.1.10 transition since then to v7
Staging Issues: Lung Cancer & Mesothelioma Mick Peake Clinical Lead, NCIN Chair, Lung SSCRG Staging systems Non-Small Cell Lung Cancer (>85%): UICC TNM v6 used until 1.1.10 transition since then to v7
Lung Cancer Screening
 Lung Cancer Screening Steven Leh, MD, FCCP Diplomat of the American Association for Bronchology and Interventional Pulmonology Aurora Medical Group Pulmonary and Sleep Medicine February 10, 2018 Disclosures
Lung Cancer Screening Steven Leh, MD, FCCP Diplomat of the American Association for Bronchology and Interventional Pulmonology Aurora Medical Group Pulmonary and Sleep Medicine February 10, 2018 Disclosures
Lung Cancer Screening: Benefits and limitations to its Implementation
 Lung Cancer Screening: Benefits and limitations to its Implementation Rolando Sanchez, MD Clinical Assistant Professor Pulmonary-Critical Care Medicine University of Iowa Lung cancer - Epidemiology Cancer
Lung Cancer Screening: Benefits and limitations to its Implementation Rolando Sanchez, MD Clinical Assistant Professor Pulmonary-Critical Care Medicine University of Iowa Lung cancer - Epidemiology Cancer
The European Board of Urology
 Page 1 of 15 The European Board of Urology Sub-specialty certification application: Prostate cancer, A - General information A1 - APPLICATION IDENTIFICATION 1a. Application code blank 1b. EBU internal
Page 1 of 15 The European Board of Urology Sub-specialty certification application: Prostate cancer, A - General information A1 - APPLICATION IDENTIFICATION 1a. Application code blank 1b. EBU internal