Recent Advances and Updated Guidelines in the Management of Chemotherapy-Induced Nausea and Vomiting
|
|
|
- Ashlee Barrett
- 6 years ago
- Views:
Transcription
1 N o v e m b e r w w w. c l i n i c a l a d v a n c e s. c o m V o l u m e 9, I s s u e 1 1, S u p p l e m e n t 2 7 Moderator Discussants Lee S. Schwartzberg, MD, FACP Clinical Oncologist Medical Director The West Clinic Memphis, Tennessee Steven M. Grunberg, MD Professor of Medicine The University of Vermont College of Medicine Burlington, Vermont Mark G. Kris, MD Chief, Thoracic Oncology Memorial Sloan-Kettering Cancer Center New York, New York Recent Advances and Updated Guidelines in the Management of Chemotherapy-Induced Nausea and Vomiting Abstract One of the most dreaded side effects of anticancer treatment, chemotherapy-induced nausea and vomiting (CINV) plays a significant role in cancer patients morbidity and quality of life. The management of CINV has been refined over the past several decades, and CINV can now be addressed with targeted prophylactic medications aimed at inhibiting the molecular pathways involved in emesis, including serotonin receptor antagonists and neurokinin-1 receptor antagonists. Advances in the understanding of the physiology of CINV, coupled with the introduction of several agents that inhibit activation of these receptors, are reflected in current CINV guidelines. These guidelines, which are largely similar, provide recommendations based on expert review of available clinical trial data. Despite the availability of effective prophylaxis, many patients still suffer from CINV. To minimize these side effects, clinicians should ensure widespread adoption and implementation of at least 1 CINV guideline in their practice. Even when the recommendations are followed, a small group of patients continue to experience CINV, often in the form of nausea, for which few treatments are effective. Current and future studies will begin to delineate the specific pathways for the development of nausea, hopefully leading to the identification of novel agents and regimens with improved efficacy in this setting. A CME Activity Approved for 1 AMA PRA Category 1 Credit(s) TM Release Date: November 2011 Expiration Date: November 30, 2012 Estimated time to complete activity: 1 hour Project ID: 8224 Sponsored by the Postgraduate Institute for Medicine S u p p o r t e d t h r o u g h a n e d u c a t i o n a l g r a n t f r o m E i s a i, I n c.
2 Target Audience This activity has been designed to meet the educational needs of hematologists/oncologists and oncologists, radiation oncologists, oncology nurses, and hematology/oncology pharmacy specialists who treat cancer patients undergoing chemotherapy who experience nausea and vomiting as side effects of therapy. Statement of Need/Program Overview Nausea and vomiting can result in serious metabolic derangements, nutritional depletion and anorexia, deterioration of patients physical and mental status, esophageal tears, fractures, wound dehiscence, withdrawal from potentially useful and curative antineoplastic treatment, and degeneration of self-care and functional ability. Despite advances in pharmacologic and nonpharmacologic management, nausea and vomiting remain 2 of the more distressing and feared side effects to cancer patients and their families. Thus, oncologists who treat chemotherapy-induced nausea and vomiting (CINV) need to stay current regarding important findings in the treatment of this condition. This clinical roundtable monograph will include presentations by 3 physicians who will discuss new findings regarding CINV, updates to CINV guidelines, and how these guidelines can be incorporated into clinical practice. These presentations will be followed by a question-and-answer forum in which the 3 physicians will address ancillary points. Educational Objectives After completing this activity, the participant should be better able to: Describe the importance of new study findings and clinical trial data in the natural history of CINV in cancer patients. Assess the results of these new study findings, including updates on guidelines for highly and moderately emetogenic chemotherapy and radiotherapy. Integrate into clinical practice the latest practice methods for treating cancer patients with CINV in an effort to improve current quality of life statistics. Accreditation Statement This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Postgraduate Institute for Medicine (PIM) and Millennium Medical Publishing, Inc. PIM is accredited by the ACCME to provide continuing medical education for physicians. Credit Designation The Postgraduate Institute for Medicine designates this journal-based CME activity for a maximum of 1.0/AMA PRA Category 1 Credit(s) TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Disclosure of Conflicts of Interest PIM assesses conflict of interest with its instructors, planners, managers, and other individuals who are in a position to control the content of continuing medical education (CME) activities. All relevant conflicts of interest that are identified are thoroughly vetted by PIM for fair balance, scientific objectivity of studies utilized in this activity, and patient care recommendations. PIM is committed to providing its learners with high quality CME activities and related materials that promote improvements or quality in healthcare and not a specific proprietary business interest of a commercial interest. The faculty reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity: Disclosures Steven M. Grunberg, MD, has received consulting fees from Helsinn, Merck, SNBL, and Tesaro. He has also received fees for non-cme/ce services and has ownership interest in Merck. Mark G. Kris, MD, has no real or apparent conflicts of interest to report. Lee S. Schwartzberg, MD, FACP, has received consulting fees and fees for non-cme/ce services from Eisai, Inc. The planners and managers reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity: The following PIM planners and managers, Jan Hixon, RN, BSN, MA, Trace Hutchison, PharmD, Julia Kimball, RN, BSN, Samantha Mattiucci, PharmD, Jan Schultz, RN, MSN, CCMEP, and Patricia Staples, MSN, NP-C, CCRN, hereby state that they or their spouse/ life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months. Kay Downer: No real or apparent conflicts of interest to report. Lisa Cockrell, PhD: No real or apparent conflicts of interest to report. Method of Participation There are no fees for participating and receiving CME credit for this activity. During the period November 2011 through November 30, 2012, participants must 1) read the learning objectives and faculty disclosures; 2) study the educational activity; 3) complete the post-test by recording the best answer to each question in the answer key on the evaluation form; 4) complete the evaluation form; and 5) mail or fax the evaluation form with answer key to Postgraduate Institute for Medicine. You may also complete the post-test online at On the navigation menu, click on Find Post-tests by Course and search by project ID Upon successfully completing the post-test and evaluation, your certificate will be made available immediately. A statement of credit wil be issued only upon receipt of a completed activity evaluation form and a completed post-test with a score of 70% or better. Your statement of credit will be mailed to you within three weeks. Media Monograph Disclosure of Unlabeled Use This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. PIM, Millennium Medical Publishing, Inc., and Eisai, Inc., do not recommend the use of any agent outside of the labeled indications. The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of PIM, Millennium Medical Publishing, Inc., and Eisai, Inc. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings. Disclaimer Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient s conditions and possible contraindications or dangers in use, review of any applicable manufacturer s product information, and comparison with recommendations of other authorities. Disclaimer Funding for this monograph has been provided through an educational grant from Eisai, Inc. Support of this monograph does not imply the supporter s agreement with the views expressed herein. Every effort has been made to ensure that drug usage and other information are presented accurately; however, the ultimate responsibility rests with the prescribing physician. Millennium Medical Publishing, Inc., the supporter, and the participants shall not be held responsible for errors or for any consequences arising from the use of information contained herein. Readers are strongly urged to consult any relevant primary literature. No claims or endorsements are made for any drug or compound at present under clinical investigation Millennium Medical Publishing, Inc., 611 Broadway, Suite 310, New York, NY Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.
3 New Findings Regarding Chemotherapy-Induced Nausea and Vomiting in Cancer Patients Steven M. Grunberg, MD Many of the most important advances in our understanding of the natural history of chemotherapy-induced nausea and vomiting (CINV) in cancer patients have occurred during the past 3 decades. Until recently, much of this work focused on unraveling the basic neuropharmacology that defines the emetic reflex. This research led to the development of strategies for inhibiting these pathways and preventing the ultimate consequence of CINV. Dopamine was the first neurotransmitter shown to have an essential role in the CINV pathway. This finding was followed by research establishing the importance of serotonin (5HT) and substance P. Antiemetic drugs targeting these pathways quickly followed, including antidopaminergics, 5HT 3 receptor antagonists, and neurokinin-1 (NK1) receptor antagonists. However, recent work has demonstrated that the pathways involved in the emetic response are not as straightforward as was once believed; no longer is 1 type of neurotransmitter receptor (dopamine, 5HT 3, or NK1) thought to be associated with a particular type of response (acute, delayed, or anticipatory CINV). A continued effort to improve understanding of the physiology underlying the emetic response will hopefully lead to the development of more specific agents to prevent CINV, as well as help physicians to better use existing antiemetic agents in clinical practice. Recently Completed Studies The 5HT 3 receptor has long been recognized as an important target of intervention for prevention of CINV. This recognition led to the development and approval of several 5HT 3 receptor antagonists, including dolasetron, granisetron, ondansetron, and palonosetron. However, researchers did not immediately recognize that these 5HT 3 receptor antagonists differ somewhat in terms of their mechanisms of action and efficacy. The 5HT 3 receptor antagonist palonosetron, a second-generation agent, offers several advantages over older 5HT 3 receptor antagonists. For example, palonosetron has a half-life of nearly 40 hours, making it much more durable compared to the first-generation 5HT 3 agents, which have half-lives of approximately 10 hours. 1 Palonosetron s longer half-life results in prolonged bioavailability, allowing this drug to be effective in both the acute and delayed phases of CINV. Indeed, this benefit was shown by palonosetron s superior ability to prevent delayed emesis caused by both highly and moderately emetogenic chemotherapy agents without an increase in incidence or duration of adverse events. 2-5 Additionally, palonosetron has a higher affinity for the 5HT 3 receptor. 1 Recent work has shown that the increased efficacy of second-generation 5HT 3 receptor antagonists such as palonosetron is not due solely to their longer half-life and higher receptor affinity. This research suggests that palonosetron may have a relatively unique mechanism of action, whereby it undergoes allosteric binding to the 5HT 3 receptor. 6 Other studies suggest that the receptor dynamics are changed when the agent is bound to the receptor; these changes include how rapidly and completely the receptor is internalized. 7 These 2 unique pharmacologic characteristics may explain the increased activity of palonosetron. Another important and relatively recent discovery concerns the NK1 receptor antagonists. Traditionally, 5HT 3 receptor antagonists were used to control CINV during the acute period, while NK1 receptor antagonists were mainly used during the delayed period. Indeed, this strategy has been incorporated into major guidelines. However, research is increasingly revealing that these guidelines reflect an incomplete understanding of antiemetic dynamics. In a study my colleagues and I published in early 2011, we compared 2 schedules of NK1 receptor antagonists to determine their efficacy for preventing both acute and delayed CINV. 8 In this study, 2,322 patients who were receiving cisplatin chemotherapy for the first time were randomized to receive either a single dose of intravenous fosaprepitant on Day 1 or the standard 3-day regimen of oral aprepitant on Days 1 3. All patients were also given ondansetron and dexamethasone. The efficacy of both NK1 receptor antagonist schedules was found to be similar, although readers should note that the study was not specifically designed to assess efficacy during the acute period. The results of this study suggest that NK1 antagonists do not need to be administered over a 3- or 5-day period in order to elicit the desired effect during the delayed period. Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November
4 This finding raises questions about how these agents work and why they continue to work for days after administration. Their continued efficacy could be due to pharmacologic reasons, such as stronger binding of the agent to the target receptor, or due to pharmacodynamic reasons, such as durable receptor occupancy independent of serum levels. Alternatively, this effect may not necessarily be due to either improved pharmacodynamics or pharmacokinetics; instead, efficacy during the delayed phase could be strictly due to prophylactic use of the agent to prevent the NK1 receptors from ever being activated during cisplatin treatment. These and other studies show the importance of reconsidering the pharmacology of existing agents in order to design better drugs in the future. Many of the recent discoveries regarding the mechanism of action and use of existing antiemetic agents will likely affect future updates to CINV guidelines. Future Research Directions Personalized therapy, already a major concept in the field of oncology, may have an important impact in the field of CINV prevention. One potential implementation of personalized therapy is the incorporation of pharmacogenomics, an emerging field that involves studying genetic differences among individuals that alter a drug s pharmacology. For example, pharmacogenomic differences in the cytochrome P450 2D6 (CYP2D6) enzyme pathway have been demonstrated to have an effect on 5HT 3 receptor antagonists. The CYP2D6 pathway is essential for the metabolism of some 5HT 3 receptor antagonists; therefore, changes in CYP2D6 enzyme activity may dramatically alter the efficacy of an agent. For instance, CYP2D6 genotyping can be used to define cancer patients as either rapid or slow metabolizers; those patients who are more rapid metabolizers have an increased risk of having a reduced antiemetic effect. Indeed, patients defined as ultrarapid metabolizers of 5HT 3 receptor antagonists experience a significantly higher frequency of nausea and emesis during the acute period. 9 Separately, researchers have identified mutations in certain 5HT 3 receptor subunits that may explain the lack of efficacy of antiemetic drugs in some patients. 10,11 Interestingly, pharmacogenomics may play a role in explaining why certain antiemetic agents are approved at different doses by regulatory agencies in different countries. For example, both granisetron and palonosetron are approved at different doses in Japan compared with the United States. Traditionally, this difference was attributed to arbitrary decisions made by the different regulatory agencies. However, this difference may actually be due to pharmacogenomic differences between the 2 populations, which may cause variations in the metabolism of the drug that in turn cause the different efficacies observed in clinical studies. Unfortunately, although comparative studies between different populations in different countries might allow the identification of unique treatment results, such studies are difficult to conduct because of the difficulty in controlling for the myriad of factors that vary between populations, including lifestyle, diet, environment, and climate. Shedding more light on the impact of pharmacogenomics in CINV is a longitudinal, prospective, observational study recently conducted at a single hospital in Malaysia, an area of great ethnic diversity. 12 The study population consisted of 158 women with breast cancer who were all treated with similar chemotherapy regimens (cyclophosphamide and 5-fluorouracil plus either epirubicin, adriamycin, or methotrexate). All patients also received the same antiemetic regimen, consisting of a 5HT 3 receptor antagonist plus dexamethasone. Patients were grouped according to ethnic population: Chinese, Malay, or Indian. Interestingly, each ethnic group had a unique response to antiemetic therapy, with Chinese patients experiencing the most CINV symptoms both during acute and delayed periods. This study raises the question of whether differences in the genetic make-up of various ethnic groups could allow for more accurate prediction of how patients will respond to antiemetic therapy or even which medications are necessary to optimally treat a particular patient. In research settings, investigators may be able to observe how different ethnic groups respond to antiemetic regimens and use this information to identify which genes are important for these different responses. Focus on Nausea Traditionally, CINV has been perceived as a single condition, but researchers are increasingly realizing that nausea and vomiting, although related, are in fact 2 very different phenomena. Indeed, nausea will likely become an interesting focus of research in the coming years. Nausea occurs more frequently than emesis, and nausea may actually be of greater clinical significance for patients. 13,14 All of the drugs currently indicated for CINV in the United States were approved based on clinical trials that used complete response as an endpoint. Typically, complete response is defined as the absence of vomiting with no use of rescue medication; it does not include any measurement of nausea. This omission is primarily a reflection of the difficulty involved in measuring nausea, compared to the straightforward method of quantitating emesis (counting vomiting episodes). The typical assumption has been that drugs that are capable of treating vomiting will also be effective for nausea. However, this assumption may not hold true, which could explain 4 Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November 2011
5 why patients still suffer from chemotherapy-induced nausea despite antiemetic interventions. Several recent studies, conducted both in the United States and in other countries, have demonstrated that approximately twice as many patients experience nausea compared with those who experience vomiting; in some populations, this ratio may approach 3:1. In 1 study, the incidence of acute nausea was over 2-fold higher than the incidence of acute vomiting (35% vs 13%). 15 This trend is especially true among young women undergoing treatment for breast cancer, who are particularly prone to experiencing delayed nausea instead of delayed vomiting. This difference in prevalence between nausea and vomiting has caused investigators to conclude that the 2 conditions are discrete phenomena. Currently, the pathways responsible for vomiting are understood much better than the pathways that cause nausea. In order to better devise drugs and strategies aimed at treating nausea itself, future research should be focused on understanding exactly what nausea is and the physiologic pathways that lead to it. Although nausea is typically considered to be a prelude to vomiting, this continuum may not always hold true. Interestingly, many of the medications suggested to have efficacy against nausea such as megestrol, cannabinoids, steroids, and olanzapine are also considered to be remedies for cancer cachexia or appetite stimulants. This observation suggests an interesting way to think about nausea; rather than comparing nausea with vomiting, clinicians may want to start thinking that the opposite of nausea is the presence of a good appetite. Thus, an interesting direction for future research will be to incorporate observations from studies that offer insights into cancer cachexia and cancer anorexia into research on CINV. Summary Although many advances have been made in the past 30 years of research focused on treating and preventing CINV, many gaps in our understanding of these conditions remain. For example, certain factors place a person at greater risk for experiencing increased CINV, including female sex, younger age, and no prior alcohol use. Interestingly, a link has even been suggested between postoperative nausea and vomiting and the stage of a woman s menstrual cycle. However, the reasons why these factors increase the risk of CINV remain undefined. Hormones may be important, and differences in the dopamine reward pathway may help explain why patients who previously used alcohol heavily are less affected by CINV. Acknowledgment Steven M. Grunberg, MD, has received consulting fees from Helsinn, Merck, SNBL, and Tesaro. He has also received fees for non-cme/ce services and has ownership interest in Merck. References 1. Grunberg SM, Koeller JM. Palonosetron: a unique 5-HT3-receptor antagonist for the prevention of chemotherapy-induced emesis. Expert Opin Pharmacother. 2003;4: Eisenberg P, Figueroa-Vadillo J, Zamora R, et al. Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer. 2003;98: Aapro MS, Grunberg SM, Manikhas GM, et al. A phase III, double-blind, randomized trial of palonosetron compared with ondansetron in preventing chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy. Ann Oncol. 2006;17: Gralla R, Lichinitser M, Van Der Vegt S, et al. Palonosetron improves prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy: results of a double-blind randomized phase III trial comparing single doses of palonosetron with ondansetron. Ann Oncol. 2003;14: Saito M, Aogi K, Sekine I, et al. Palonosetron plus dexamethasone versus granisetron plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a double-blind, double-dummy, randomised, comparative phase III trial. Lancet Oncol. 2009;10: Rojas C, Stathis M, Thomas AG, et al. Palonosetron exhibits unique molecular interactions with the 5-HT3 receptor. Anesth Analg. 2008;107: Rojas C, Thomas AG, Alt J, et al. Palonosetron triggers 5-HT(3) receptor internalization and causes prolonged inhibition of receptor function. Eur J Pharmacol. 2010;626: Grunberg S, Chua D, Maru A, et al. Single-dose fosaprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with cisplatin therapy: randomized, double-blind study protocol EASE. J Clin Oncol. 2011;29: Kaiser R, Sezer O, Papies A, et al. Patient-tailored antiemetic treatment with 5-hydroxytryptamine type 3 receptor antagonists according to cytochrome P-450 2D6 genotypes. J Clin Oncol. 2002;20: Tremblay PB, Kaiser R, Sezer O, et al. Variations in the 5-hydroxytryptamine type 3B receptor gene as predictors of the efficacy of antiemetic treatment in cancer patients. J Clin Oncol. 2003;21: Kaiser R, Tremblay PB, Sezer O, Possinger K, Roots I, Brockmöller J. Investigation of the association between 5-HT3A receptor gene polymorphisms and efficiency of antiemetic treatment with 5-HT3 receptor antagonists. Pharmacogenetics. 2004;14: Hassan BA, Yusoff ZB. Genetic polymorphisms in the three Malaysian races effect granisetron clinical antiemetic actions in breast cancer patients receiving chemotherapy. Asian Pac J Cancer Prev. 2011;12: Kurtin SE. Chemotherapy-induced nausea and vomiting: clinical updates. Oncology Pharmacist. 2010;3: mode=embed&layout=http%3a%2f%2fskin.issuu.com%2fv%2flight%2flayout. xml&showflipbtn=true. Accessed October 18, Hesketh PJ. Chemotherapy-induced nausea and vomiting. N Engl J Med. 2008;358: Grunberg SM, Deuson RR, Mavros P, et al. Incidence of chemotherapy-induced nausea and emesis after modern antiemetics. Cancer. 2004;100: Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November
6 Updates to Guidelines on Chemotherapy-Induced Nausea and Vomiting Mark G. Kris, MD Although CINV has been a significant medical issue since the introduction of anticancer chemotherapy, its impact has been dramatically altered over recent decades. This change is mainly due to the introduction of effective antiemetic agents and the use of these agents as prophylactic therapy. Prior to the introduction of effective antiemetic drugs, cancer patients had limited options for the prevention of CINV. Instead, they routinely required hospitalization following chemotherapy administration for care of the ensuing nausea and emesis. Thus, patients developed an expectation that undergoing anticancer chemotherapy would inevitably result in the development of moderate or severe CINV and that this side effect would detract from their lifestyle and reduce their quality of life. Often, CINV made completion of the necessary chemotherapy regimen difficult for patients. Fortunately, advances in our understanding of the underlying biology of CINV have allowed for the development of agents targeted against the pathways important for CINV. This development has resulted in the approval of several drugs to prevent CINV. In general, physicians know that these agents are very effective in the vast majority of chemotherapy patients. However, many physicians incorrectly believe that the problem of CINV is completely solved by these agents. The fallacy of this belief becomes evident when discussing the potential for CINV with a cancer patient who is preparing to undergo chemotherapy. Even with the availability of multiple effective antiemetic agents, most patients still greatly fear CINV. In fact, nausea and emesis rank as the most feared side effects of anticancer chemotherapy. In a survey of patient concerns, 73% of lung cancer patients reported that they would choose their chemotherapy regimen based on its side-effect profile, if they were given that option. 1 Among the side effects listed in this survey, nausea and vomiting were ranked as most important by nearly half (48%) of the respondents. Given these findings, there remains a critical need among cancer patients for treatments and strategies that can address the issue of CINV. To begin to address this problem, oncologists need to recognize the true magnitude and impact of CINV and implement strategies that allow for the most effective use of antiemetic medication to prevent CINV. Studies suggest that CINV remains highly prevalent despite the use of antiemetic agents, occurring in up to 80% of patients receiving chemotherapy. 2 However, clinicians often overlook the prevalence of CINV. 3,4 Healthcare providers also tend to underestimate the impact of CINV on patients, including reductions in daily functioning, hampering of social activities, and interference with employment. 5-7 Role of Guidelines in Clinical Practice To help address the significant needs surrounding CINV, several major groups have produced CINV-specific guidelines. The most prominent of these groups are the American Society of Clinical Oncology (ASCO), the Multinational Association for Supportive Care in Cancer (MASCC), and the National Comprehensive Cancer Network (NCCN) In many cases, the recommendations and overall guidance are similar among the guidelines issued by these 3 groups. To form these guidelines, expert panels carefully reviewed the medical literature, identified the most effective agents available, and codified how these agents could be used most appropriately to prevent CINV resulting from different types of chemotherapy. The implementation of these guidelines into clinical practice not only improves patient outcomes but also lessens the burden on the healthcare system by facilitating more efficient use of resources. 11 One of the main principles shared among these 3 guidelines is the idea that the amount and severity of CINV a patient is likely to experience is mainly determined by the specific chemotherapy regimen being prescribed. To help clinicians better predict the risk of CINV, each guideline has created classification schemes that define the CINV potential of various chemotherapy agents. For intravenous agents, 4 categories have been developed based on the proportion of patients likely to experience acute emesis if no prophylactic antiemetic therapy is administered: high ( 90% of patients), moderate (30 90% of patients), low (10 30% of patients), and minimal (<10% of patients). Readers should note that these definitions only account for the potential of developing acute emesis; they do not consider delayed emesis. Defining the emetogenicity of each chemotherapy agent is important both to provide a framework for choosing an appropriate antiemetic regimen and to better understand the drug s potential for CINV. 12 In most cases when CINV is a significant issue, the offending drug is classified as having either moderate or high emetogenic potential. The quintessential high emetic risk drug is cisplatin, which produces severe emesis. The effects of cisplatin are severe regardless of the dose or administration schedule. Thus, cisplatin-treated patients require opti- 6 Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November 2011
7 mal antiemetic therapy. According to all 3 major guidelines, the best antiemetic regimen for preventing CINV caused by chemotherapy agents with high emetic risk is a triple combination that includes a 5HT 3 receptor antagonist, a corticosteroid, and an NK1 receptor antagonist. Together, these 3 classes of drugs form the cornerstone of antiemetic prophylaxis for all patients receiving high emetic risk chemotherapy. Currently, the preferred agents in this combination include the 5HT 3 receptor antagonist palonosetron, either of the NK1 receptor antagonists aprepitant or fosaprepitant, and the corticosteroid dexamethasone. For chemotherapy agents with moderate emetic risk, the guidelines clearly state that patients should receive a multidrug antiemetic regimen comprised of a 5HT 3 antagonist and dexamethasone. Typically, palonosetron is the preferred 5HT 3 receptor antagonist in this setting. Evidence suggests that the addition of aprepitant is also beneficial for patients receiving moderate emetic risk chemotherapy drugs. Although aprepitant is not yet included as a recommended option for moderate emetic risk agents in any of the guidelines, the literature clearly supports its use in this setting, especially given its favorable safety profile. The currently available antiemetic therapies prevent but do not treat CINV; thus, all 3 guidelines stress the overarching principle of CINV prevention as a primary strategy. Unfortunately, there is no effective treatment for CINV once it has occurred. Additionally, once a patient has experienced CINV, he or she is more likely to suffer from this side effect in subsequent rounds of chemotherapy. 13 Thus, the most effective antiemetic regimens should be administered upfront, either at or near the time of initial chemotherapy administration. Updates to Guidelines Each of the 3 CINV guidelines is regularly updated to incorporate novel clinical data and the availability of newly approved agents. For example, an expert panel recently updated the ASCO guidelines; this update is presently undergoing final review and will be published shortly in the Journal of Clinical Oncology. 14 Of the 3 CINV guidelines, the NCCN guidelines are updated the most frequently; the most recent version was released in July Several important changes were incorporated into this revision. Palonosetron Preferred Among Serotonin Receptor Antagonists One important change in the most recent version of the NCCN guidelines is the identification of palonosetron as the preferred 5HT 3 receptor antagonist. Until recently, the expert panel had been unable to reach a consensus as to whether a particular 5HT 3 receptor antagonist should be recommended over other drugs in this class. However, multiple randomized, phase III clinical trials have been conducted to address this question, and these studies have demonstrated that palonosetron provides higher rates of response for delayed emesis compared to other 5HT 3 receptor antagonists (dolasetron, ondansetron, and granisetron). In a study of 569 patients who received moderately emetogenic chemotherapy, study participants were randomized to receive a single intravenous dose of palonosetron (0.25 mg or 0.75 mg) or dolasetron (100 mg) administered prior to chemotherapy. 15 The primary study endpoint was prevention of acute emesis, which was defined as complete response (no emetic episodes with no rescue medication) during the first 24 hours after chemotherapy. A secondary endpoint assessed the prevention of emesis 2 5 days following chemotherapy. Prevention of acute emesis was achieved at similar rates among the 3 treatment groups (63.0%, 57.1%, and 52.9% for 0.25-mg palonosetron, 0.75-mg palonosetron, and 100-mg dolasetron, respectively), suggesting that either dose of palonosetron was as effective as dolasetron. During the delayed period, however, significantly higher rates of complete response were achieved with both the 0.25 mg and 0.75 mg doses of palonosetron compared to dolasetron (54.0%, 56.6%, and 38.7%, respectively; P=.004 for 0.25-mg palonosetron vs dolasetron; P<.001 for 0.75-mg palonosetron vs dolasetron). In another study, 667 patients who were receiving highly emetogenic chemotherapy were randomized to receive a single intravenous dose of palonosetron (0.25 mg or 0.75 mg) or ondansetron (32 mg) prior to administration of chemotherapy. 16 Again, the study endpoints were complete response during the acute and delayed periods. Both low-dose palonosetron and high-dose palonosetron were as effective as ondansetron for preventing acute emesis (59.2%, 65.5%, and 57.0%, respectively), and both doses of palonosetron were more effective than ondansetron for preventing delayed emesis (45.3%, 48.0%, and 38.9%, respectively). Notably, the addition of dexamethasone, which was done at the investigator s discretion in approximately two-thirds of patients, resulted in significantly higher complete response rates during the delayed period among patients treated with 0.25-mg palonosetron versus those treated with ondansetron (42.0% vs 28.6%; P=.021). In a third study, 570 patients undergoing moderately emetogenic chemotherapy were treated with a single intravenous dose of palonosetron (0.25 mg or 0.75 mg) or ondansetron (32 mg) prior to administration of chemotherapy. 17 In this study, the rates of complete response were significantly higher for 0.25-mg palonosetron compared to ondansetron during both the acute period (81.0% vs 68.6%; P<.01) and the delayed period (74.1% vs 55.1%; P<.01). Although the same trend was observed for the 0.75-mg dose of palonosetron, the differences did not reach statistical significance. Finally, the fourth and largest study involved 1,114 patients who were undergoing treatment with highly emetogenic chemotherapy. 18 Patients were randomized to receive either 0.75 mg palonosetron or Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November
8 40 µg/kg granisetron, both of which were administered prior to chemotherapy. In this trial, dexamethasone was also administered in both treatment arms. The proportion of patients who achieved a complete response during the acute period was similar between the palonosetron and granisetron groups (75.3% vs 73.3%). However, the proportion of patients who achieved a complete response during the delayed period was significantly higher in the palonosetron arm compared to the granisetron arm (56.8% vs 44.5%; P<.0001). Importantly, in addition to its efficacy against emesis, palonosetron also improves symptoms of nausea. Based on the proven efficacy of palonosetron to prevent acute CINV and its greater efficacy for prevention of delayed CINV, the NCCN expert panel recommended palonosetron as the preferred 5HT 3 receptor antagonist. Other Updates Another update to the NCCN CINV guidelines is the inclusion of data from a recent study published by Grunberg and colleagues. 19 In this randomized, double-blind trial, 2,322 patients who were receiving highly emetogenic chemotherapy for the first time were randomized to receive antiemetic therapy consisting of ondansetron, dexamethasone, and either fosaprepitant (150 mg on Day 1) or aprepitant (125 mg on Day 1, 80 mg on Day 2, and 80 mg on Day 3). This study found that a single dose of intravenous fosaprepitant was noninferior to the standard 3-day regimen of oral aprepitant for prevention of delayed CINV. In many practice settings, a single intravenous dose of fosaprepitant would be much easier to administer than the 3-day oral regimen of aprepitant. Furthermore, administration of an intravenous medication helps to ensure that the patient is properly treated, as intravenous administration eliminates the possibility that patients will forget to take the drug. Finally, unlike other 5HT 3 receptor antagonists, fosaprepitant shows no difference in efficacy between men and women. Summary All oncologists should pay close attention to nausea and emesis in cancer patients undergoing chemotherapy treatment, particularly individuals who are receiving drugs that have a moderate or high emetic risk. Clinicians should also stay up-to-date about recent changes in the CINV guidelines, as these guidelines reflect our most current understanding of the development of CINV and optimal strategies for prevention. All healthcare professionals who care for cancer patients undergoing chemotherapy should become very familiar with at least 1 of the CINV guidelines and should incorporate these recommendations into routine patient management. Strict adherence to these guidelines will likely help to reduce the prevalence of this highly troublesome side effect of chemotherapy. Adherence to these guidelines will also help to improve overall quality of care, reduce costs, and more effectively address chemotherapy patients very serious concerns about CINV. Acknowledgment Mark G. Kris, MD, has no real or apparent conflicts of interest to report. References 1. Dubey S, Brown RL, Esmond SL, Bowers BJ, Healy JM, Schiller JH. Patient preferences in choosing chemotherapy regimens for advanced non-small cell lung cancer. J Support Oncol. 2005;3: Nevidjon B, Chaudhary R. Controlling emesis: evolving challenges, novel strategies. J Support Oncol. 2010;8(4 suppl 2): Grunberg SM, Deuson RR, Mavros P, et al. Incidence of chemotherapy-induced nausea and emesis after modern antiemetics. Cancer. 2004;100: Majem M, Moreno ME, Calvo N, et al. Perception of healthcare providers versus patient reported incidence of chemotherapy-induced nausea and vomiting after the addition of NK-1 receptor antagonists. Support Care Cancer Nov 18. Epub ahead of print. 5. Haiderali A, Menditto L, Good M, Teitelbaum A, Wegner J. Impact on daily functioning and indirect/direct costs associated with chemotherapy-induced nausea and vomiting (CINV) in a U.S. population. Support Care Cancer. 2011;19: Lindley CM, Hirsch JD, O Neill CV, Transau MC, Gilbert CS, Osterhaus JT. Quality of life consequences of chemotherapy-induced emesis. Qual Life Res. 1992;1: Decker GM, DeMeyer ES, Kisko DL. Measuring the maintenance of daily life activities using the functional living index-emesis (FLIE) in patients receiving moderately emetogenic chemotherapy. J Support Oncol. 2006;4:35-41, American Society of Clinical Oncology, Kris MG, Hesketh PJ, et al. American Society of Clinical Oncology guideline for antiemetics in oncology: update J Clin Oncol. 2006;24: Roila F, Hesketh PJ, Herrstedt J; Antiemetic Subcommittee of the Multinational Association of Supportive Care in Cancer. Prevention of chemotherapy- and radiotherapy-induced emesis: results of the 2004 Perugia International Antiemetic Consensus Conference. Ann Oncol. 2006;17: National Comprehensive Cancer Network. Antiemesis. Clinical Practice Guidelines in Oncology. Version physician_gls/pdf/antiemesis.pdf. Accessed October 4, Wickham R. Best practice management of CINV in oncology patients: II. Antiemetic guidelines and rationale for use. J Support Oncol. 2010;8(2 suppl 1): Grunberg SM, Warr D, Gralla RJ, et al. Evaluation of new antiemetic agents and definition of antineoplastic agent emetogenicity state of the art. Support Care Cancer. 2011;19(suppl 1):S43-S Nevidjon B, Chaudhary R. Controlling emesis: evolving challenges, novel strategies. J Support Oncol. 2010;8(4 suppl 2): Basch E, Prestrud AA, Hesketh PJ, et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol Sep 26. Epub ahead of print. 15. Eisenberg P, Figueroa-Vadillo J, Zamora R, et al. Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer. 2003;98: Aapro MS, Grunberg SM, Manikhas GM, et al. A phase III, double-blind, randomized trial of palonosetron compared with ondansetron in preventing chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy. Ann Oncol. 2006;17: Gralla R, Lichinitser M, Van Der Vegt S, et al. Palonosetron improves prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy: results of a double-blind randomized phase III trial comparing single doses of palonosetron with ondansetron. Ann Oncol. 2003;14: Saito M, Aogi K, Sekine I, et al. Palonosetron plus dexamethasone versus granisetron plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a double-blind, double-dummy, randomised, comparative phase III trial. Lancet Oncol. 2009;10: Grunberg S, Chua D, Maru A, et al. Single-dose fosaprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with cisplatin therapy: randomized, double-blind study protocol EASE. J Clin Oncol. 2011;29: Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November 2011
9 Incorporating Chemotherapy-Induced Nausea and Vomiting Guidelines Into Clinical Practice Lee S. Schwartzberg, MD, FACP As physicians, we are fortunate to be living in an era in which evidence-based medicine drives many of the guiding principles by which we practice. Not only do we subscribe to evidence-based medicine as the optimal way to manage patients, we now have a number of systems that provide this evidence in accessible, well-referenced ways. In practice, such systems generally take the form of evidence-based guidelines, 3 of which are valuable approaches to the management of CINV. Overall, the recommendations offered by each of these guidelines have more points of similarity than differences. Guidelines from ASCO are periodically updated based on a rigorous evaluation of the evidence that is available to date. 1 The majority of the data considered for the ASCO guidelines is Level 1 evidence, and this evidence is given the most weight. Thus, the ASCO guidelines are considered to be methodologically thorough. However, the rigorous nature of these guidelines makes their development a particularly labor-intensive effort. For this reason, the ASCO guidelines are updated only once every few years, instead of more frequently, even though clinical trial data are continuously being reported. The NCCN also provides guidelines for the management of CINV, and many clinicians rely heavily on them. 2 The NCCN guidelines consider both Level 1 and Level 2 evidence. In addition, the NCCN guidelines take into account the fact that many clinical questions lack the clear evidence needed to form evidence-based recommendations. To address this shortcoming, the NCCN guidelines also take into account the opinions of the expert panel forming the recommendations. Including expert opinions is a good way to provide seamless guidance across all the major decision points in CINV treatment. Another advantage of the NCCN guidelines is that they are updated at least annually and on a more frequent basis as needed to quickly incorporate new results from practice-changing clinical trials. Finally, the MASCC also provides guidelines for the management of CINV. 3 The MASCC was among the first organizations to shed light and real clarity on the management of CINV. MASCC continues to provide recommendations in this area; these recommendations incorporate Level 1 evidence, Level 2 evidence, and expert opinion. In addition to being used in the United States, the MASCC guidelines are often used in European clinical practice as well. Integrating Updates Into Clinical Care Although these guidelines provide clear recommendations for prevention of CINV, patients continue to regard the potential for nausea and emesis as 1 of the most substantial side effects of chemotherapy. Surveys have shown that CINV is the adverse effect about which patients are most apprehensive, and this apprehension results in a great deal of distress and uncertainty at a time when patients are already quite stressed. CINV is thus an important intervention point for clinicians; discussion of CINV should include education about the available prophylactic antiemesis options. Most community oncology practices have a systematic approach to the delivery of chemotherapy. At minimum, this approach generally includes a set of written orders that list all of the chemotherapy agents to be administered, their dosages, and their schedules. Increasingly, a majority of physicians are incorporating electronic medical records into their practice; use of this valuable tool can help to facilitate the best delivery of care. Not only can electronic medical records and associated care plans be easily populated, they can also be conveniently aggregated and reviewed at a later time to assure the quality of care. Additionally, electronic orders can be modified as needed; this flexibility represents a marked improvement over having to make changes to written orders. Supportive care measures, including timing and types of prophylactic antiemesis regimens, can also be included with these medical orders. Adding supportive care measures to existing orders can help to ensure that the correct dosage is administered at the correct time in order to most effectively prevent CINV. For example, intravenous antiemetics such as fosaprepitant, dexamethasone, and palonosetron should be delivered on Day 1 prior to the administration of the chemotherapy to ensure that the patient receives the full dose of the drug and that it is fully bioavailable for prophylaxis. By itself, the discovery that a single intravenous dose of fosaprepitant is noninferior to the 3-day oral regimen of aprepitant is likely to have a significant impact on the Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November
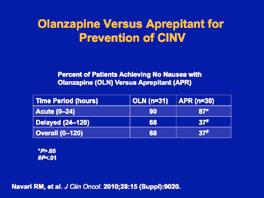
10 CINV field. By receiving an intravenous dose on Day 1, patients avoid the need to self-administer 3 oral pills over 3 days, which may be particularly difficult as patients return to their life at home and are confronted with having to take other prescriptions and deal with other side effects of chemotherapy. When trying to provide the highest quality of care for oncology patients, a goal should be to make consistency a hallmark of treatments. For instance, the same agents should be used in subsequent cycles, when possible. Another important aim is to be sure that side effects are being accurately measured. A variety of tools exist to aid in this endeavor; acute CINV is relatively easy to measure the patient can simply be asked about CINV symptoms on the day of chemotherapy administration but information about delayed CINV may be more difficult to capture. For patients undergoing chemotherapy on a 2 3 week schedule, accurately recalling CINV may be especially hard, as the majority of CINV symptoms occur in the first 5 7 days following chemotherapy. To address this difficulty, a nurse can be assigned to call the patient on Day 2 or 3, at which time he or she can inquire about and document CINV symptoms. Not only does a follow-up call help to ensure that the patient took their Day 2 and Day 3 antiemetic medication correctly, it also gives the nurse an opportunity to verify that the patient has a prescription for breakthrough medication and to initiate the process for prescribing a different medication should it be needed. Future Directions in CINV Prevention Additional research evaluating translation of evidencebased recommendations into the clinic is much needed in CINV. Overall, studies should demonstrate a near 100% translation into practice, as most of the patient populations used in major CINV clinical trials are representative of those patients seen in regular clinical practice. Nonetheless, both published and anecdotal evidence suggests that many clinical practices are not using these rigorous, evidence-based guidelines. The reasons for this shortfall are unclear, but gaps in translating guidelines to clinical practice can be avoided by more systematic use of guidelines across the field. Despite the many advances in the availability of effective prophylactic antiemetic regimens, a residual number of patients continue to experience CINV despite use of these medications. For these patients, nausea symptoms are generally more of an issue than emesis, and symptoms most often affect the individual on or after Day 3. This residual nausea can have a significant impact on quality of life, and it can potentially have a negative impact on healthcare resources as well. Patients with persistent nausea often go back to the clinic for rehydration, and they may even be admitted for treatment. Unfortunately, clinicians still lack effective treatments for chemotherapy-induced nausea. Current guidelines recommend the use of drugs from classes other than those used for prophylaxis. Some of these drugs have sedating effects, which may reduce patient anxiety; however, these agents can be more toxic, and no studies have convincingly demonstrated that they have an established benefit in this setting. New agents such as the atypical antipsychotic olanzapine have shown promise but require further study. For example, results of a phase III trial were reported at the 2010 ASCO Annual Meeting; these data showed that olanzapine was comparable to aprepitant for prevention of CINV in patients receiving highly emetogenic chemotherapy. Notably, olanzapine demonstrated improved control of delayed nausea compared to aprepitant; nausea was avoided in 65% and 38% of patients in each treatment arm, respectively. 4 However, the data are not yet sufficient to support the incorporation of olanzapine into evidence-based guidelines. Acknowledgment Lee S. Schwartzberg, MD, FACP, has received consulting fees and fees for non-cme/ce services from Eisai, Inc. References 1. American Society of Clinical Oncology, Kris MG, Hesketh PJ, et al. American Society of Clinical Oncology guideline for antiemetics in oncology: update J Clin Oncol. 2006;24: National Comprehensive Cancer Network. Antiemesis. Clinical Practice Guidelines in Oncology. Version antiemesis.pdf. Accessed October 4, Roila F, Hesketh PJ, Herrstedt J; Antiemetic Subcommittee of the Multinational Association of Supportive Care in Cancer. Prevention of chemotherapy- and radiotherapy-induced emesis: results of the 2004 Perugia International Antiemetic Consensus Conference. Ann Oncol. 2006;17: Navari RM, Gray SE, Kerr AC. Olanzapine versus aprepitant for the prevention of chemotherapy-induced nausea and vomiting (CINV): a randomized phase III trial. Presented at the 2010 American Society of Clinical Oncology Annual Meeting; June 4 8, 2010; Chicago, Illinois. Abstract Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November 2011
11 Discussion: Ongoing Advances in CINV H&O How current is the pharmacogenomic research on susceptibility to nausea and vomiting? Steven M. Grunberg, MD Most of this research has been conducted within the past decade, and some of the latest breakthroughs have just been published this year. Survey studies on the incidence of acute and delayed nausea and vomiting have been conducted in recent years and have shown a significant incidence of these side effects even in the present era of antiemetic therapy. H&O What opportunities are available for clinicians to learn about the latest research in CINV? Steven M. Grunberg, MD Aside from published literature, scientific meetings provide an excellent opportunity for clinicians to learn about recent advancements. For example, the 2011 Annual Meeting of the MASCC included an entire workshop on nausea. In this workshop, participants discussed ways of better defining chemotherapy-induced nausea and strategies and approaches for managing nausea. One interesting outcome of this discussion was recognition of a particular complication in the field of CINV: Several colloquial terms are commonly used to describe the symptoms of nausea that may not be well defined or consistent. Further complicating this problem, some languages do not even have a term for the word nausea. For example, it is difficult to translate the word into Finnish. H&O Is there a school of thought that says clinicians should focus more on vomiting than nausea? Steven M. Grunberg, MD Traditionally, clinicians have indeed focused more on vomiting than nausea. This trend is partly due to the objective nature of vomiting; in addition, many clinicians have believed that vomiting is the ultimate culmination of nausea. Thus, complete response (no vomiting and no rescue medication) became accepted as the primary endpoint of clinical studies and was used to measure drug efficacy for US Food and Drug Administration (FDA) approvals. Over time, new drugs to treat and prevent CINV were developed specifically to meet this endpoint, thus continuing the emphasis on vomiting. However, nausea in the absence of vomiting is equally troublesome to patients. While vomiting can certainly result in dehydration, nausea can have a similar effect, as a nauseous patient is far less likely to ingest adequate liquids. While nausea should not be overlooked, clinicians should note that vomiting remains an important endpoint. Some episodes of chemotherapy-induced vomiting are incredibly violent. Rarely, extreme vomiting can cause major damage, such as tearing of the esophageal tissue (Boerhaave syndrome). H&O Do you foresee new mechanisms or algorithms being implemented to help clinicians better choose which antiemetic to use and when to use it? Steven M. Grunberg, MD We currently have a number of guidelines on CINV, each of which is slightly different from the others. Some clinicians may ask why these guidelines differ, given that antiemetic agents have been demonstrated to work in particular ways. Much of the difference among guidelines is due to the different goals of each of the guideline committees, including how they analyze the data and what data are considered for inclusion. For guidelines to be incorporated more routinely into clinical practice, we need to better understand obstacles to their use and limitations of the guidelines themselves, including when they should or should not be used. Overall, guidelines should help to point the clinician in the right direction and should be used together with sound clinical judgment, common sense, and evolving knowledge. The NCCN guidelines are perhaps the most frequently updated among all the CINV guidelines. However, only a minority of NCCN recommendations are supported by Level 1 data; the rest are comprised of Level 2 or occasionally Level 3 data. Because the goal of the NCCN guidelines is to be comprehensive in data inclusion and interpretation, these guidelines must include studies other than randomized controlled trials. Another obstacle to optimal implementation of CINV guidelines is physicians learning habits. A recent editorial in The New England Journal of Medicine discussed the value of Level 4 evidence. 1 This editorial concluded that physicians learn intellectually from Level 1 evidence, but Level 4 personal anecdotal evidence has an important impact on physicians actual practice. Studies have shown that institutional support for guideline implementation results only in a temporary increase in their usage, and an Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November
12 expert lecture on antiemetic drugs during grand rounds has little effect on the prescribing habits of physicians. However, when patients are administered a questionnaire on their CINV-related symptoms and these questionnaires are then provided to each patient s own physician, a durable change in CINV guideline implementation can be achieved. This change is likely due to the physicians having a personal reaction to the information, which causes them to be more likely to follow the guidelines. H&O What is the best way to approach CINV prophylaxis for moderately emetogenic chemotherapy? Mark G. Kris, MD Prevention of CINV for moderately emetic chemotherapy is especially difficult because the risk of emesis with these drugs spans such a broad range from 30 90%. Given the relative safety of the antiemetic agents, I err on the side of using more rather than less antiemetic therapy, in order to ensure maximal prophylaxis. In these situations, I typically give all 3 components of the antiemetic regimen, as they are all FDA-approved. Although this approach may mean that the patient must take more pills, patients are generally quite willing to do so if they understand that these pills will help to prevent CINV. H&O Consider a 50-year-old woman with breast cancer who received chemotherapy (anthracycline plus cyclophosphamide). She was given an optimal antiemetic regimen prior to and following chemotherapy treatment, according to guidelines, but she presented 48 hours later complaining of nausea. How should she be managed? Lee S. Schwartzberg, MD, FACP If the patient has taken dexamethasone on Days 2 and 3 but is still experiencing nausea or emesis, she should be given rescue medication. In our practice, we typically rely on compazine first, because it has slightly less sedative effect than phenergan. If the patient continues to have symptoms, we also frequently add a benzodiazepine. In addition to providing rescue medication, clinicians need to question the patient to determine if there is an anxiety component to the CINV. For the second chemotherapy cycle, a more aggressive antiemetic intervention may be needed. For this patient, I would generally use olanzapine as breakthrough medication. As standard practice, all patients are given a prescription for rescue medication at the time of chemotherapy treatment. H&O Which aspects of recent advances in CINV are you most looking forward to incorporating into your own practice? Mark G. Kris, MD One of the things I am particularly excited about is the recognition of palonosetron as the preferred 5HT 3 receptor antagonist. For the first time in many years, we know we can improve control of nausea and emesis simply by prescribing a different medication. The fact that this recognition has been incorporated into guidelines means that it will be widely implemented in clinical practice and will hopefully have a significant impact on many patients. The ability to use a single dose of intravenous fosaprepitant in place of a 3-day regimen of oral aprepitant is also practice-changing. Use of an intravenous medication ensures that the optimal antiemetic will be delivered in the clinic, thus eliminating the risk of the patient forgetting the medication or skipping a dose. Additionally, this change can help us to overcome some of the other barriers to success with the 3-day oral aprepitant regimen, such as issues with reimbursement. Lee S. Schwartzberg, MD, FACP I agree completely. I am also excited about palonosetron s apparent ability to reduce CINV during the delayed period. In many patients, delayed CINV is worse than acute symptoms. Acknowledgment Steven M. Grunberg, MD, has received consulting fees from Helsinn, Merck, SNBL, and Tesaro. He has also received fees for non-cme/ce services and has ownership interest in Merck. Mark G. Kris, MD, has no real or apparent conflicts of interest to report. Lee S. Schwartzberg, MD, FACP, has received consulting fees and fees for non-cme/ce services from Eisai, Inc. Reference 1. Stuebe AM. Becoming a physician: level IV evidence adverse anecdote and clinical practice. N Engl J Med. 2011;365: Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November 2011






13 Slide Library Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November



14 For a free electronic download of these slides, please direct your browser to the following web address: 14 Clinical Advances in Hematology & Oncology Volume 9, Issue 11, Supplement 27 November 2011
Clinical Roundtable Monograph
 Clinical Roundtable Monograph C l i n i c a l A d v a n c e s i n H e m a t o l o g y & O n c o l o g y J a n u a r y 2 0 1 1 Treatment of Chemotherapy-Induced Nausea and Vomiting: A Post-MASCC 2010 Discussion
Clinical Roundtable Monograph C l i n i c a l A d v a n c e s i n H e m a t o l o g y & O n c o l o g y J a n u a r y 2 0 1 1 Treatment of Chemotherapy-Induced Nausea and Vomiting: A Post-MASCC 2010 Discussion
Why Patients Experience Nausea and Vomiting and What to Do About It
 Why Patients Experience Nausea and Vomiting and What to Do About It Rebecca Clark-Snow, RN, BSN, OCN The University of Kansas Cancer Center Westwood, Kansas Multiple Roles for Supportive Care in Cancer
Why Patients Experience Nausea and Vomiting and What to Do About It Rebecca Clark-Snow, RN, BSN, OCN The University of Kansas Cancer Center Westwood, Kansas Multiple Roles for Supportive Care in Cancer
TRANSPARENCY COMMITTEE OPINION. 31 January Date of marketing authorisation: 22 March 2005 (centralised marketing authorisation)
") The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 31 January 2007 ALOXI 250 µg solution for injection B/1 CIP 375,482-8 Applicant: THERABEL LUCIEN PHARMA palonosetron
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 31 January 2007 ALOXI 250 µg solution for injection B/1 CIP 375,482-8 Applicant: THERABEL LUCIEN PHARMA palonosetron
MOLECULAR AND CLINICAL ONCOLOGY 2: , 2014
 MOLECULAR AND CLINICAL ONCOLOGY 2: 375-379, 2014 Palonosetron exhibits higher total control rate compared to first generation serotonin antagonists and improves appetite in delayed phase chemotherapy induced
MOLECULAR AND CLINICAL ONCOLOGY 2: 375-379, 2014 Palonosetron exhibits higher total control rate compared to first generation serotonin antagonists and improves appetite in delayed phase chemotherapy induced
Delayed emesis: moderately emetogenic chemotherapy (single-day chemotherapy regimens only)
") Support Care Cancer (2011) 19 (Suppl 1):S57 S62 DOI 10.1007/s00520-010-1039-y SPECIAL ARTICLE Delayed emesis: moderately emetogenic chemotherapy (single-day chemotherapy regimens only) Fausto Roila & David
Support Care Cancer (2011) 19 (Suppl 1):S57 S62 DOI 10.1007/s00520-010-1039-y SPECIAL ARTICLE Delayed emesis: moderately emetogenic chemotherapy (single-day chemotherapy regimens only) Fausto Roila & David
Clinical Roundtable Monograph
 Clinical Roundtable Monograph Clinical Advances in Hematology & Oncology March 2015 New and Emerging Therapeutic Options for the Management of Chemotherapy-Induced Nausea and Vomiting Discussants Lee S.
Clinical Roundtable Monograph Clinical Advances in Hematology & Oncology March 2015 New and Emerging Therapeutic Options for the Management of Chemotherapy-Induced Nausea and Vomiting Discussants Lee S.
ATTUALITÀ NEL CONTROLLO DELL EMESI
 ATTUALITÀ NEL CONTROLLO DELL EMESI Dr Claudio Lotesoriere Dipartimento di Oncoematologia S.C. di Oncologia Medica P.O. San G. Moscati TARANTO email oncologia.taranto@gmail.com Types of CINV: Definitions
ATTUALITÀ NEL CONTROLLO DELL EMESI Dr Claudio Lotesoriere Dipartimento di Oncoematologia S.C. di Oncologia Medica P.O. San G. Moscati TARANTO email oncologia.taranto@gmail.com Types of CINV: Definitions
Organizing and Overall Meeting Chairs: Richard J. Gralla, MD Fausto Roila, MD Maurizio Tonato, MD
 PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER CONSENSUS CONFERENCE ON ANTIEMETIC THERAPY PERUGIA, March 29-31, 2004 Organizing and Overall Meeting
PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER CONSENSUS CONFERENCE ON ANTIEMETIC THERAPY PERUGIA, March 29-31, 2004 Organizing and Overall Meeting
Management of Nausea and Vomiting
 June 01, 2015 By Rudolph M. Navari, MD, PhD, FACP [1] Although marked progress in controlling chemotherapy-induced emesis has occurred over the past 25 years, nausea and vomiting remain among the most
June 01, 2015 By Rudolph M. Navari, MD, PhD, FACP [1] Although marked progress in controlling chemotherapy-induced emesis has occurred over the past 25 years, nausea and vomiting remain among the most
Clinical Roundtable Monograph
 Clinical Roundtable Monograph Clinical Advances in Hematology & Oncology October 2015 Advances in the Management of Chemotherapy-Induced ausea and Vomiting: ew Data From Recent and Ongoing Trials Discussants
Clinical Roundtable Monograph Clinical Advances in Hematology & Oncology October 2015 Advances in the Management of Chemotherapy-Induced ausea and Vomiting: ew Data From Recent and Ongoing Trials Discussants
CME. The faculty reported the following financial relationships or relationships to
 CME Target Audience This activity has been designed to meet the educational needs of oncologists, hematologists, and oncology nurses involved in the management of cancer patients receiving chemotherapy.
CME Target Audience This activity has been designed to meet the educational needs of oncologists, hematologists, and oncology nurses involved in the management of cancer patients receiving chemotherapy.
Guideline Update on Antiemetics
 Guideline Update on Antiemetics Clinical Practice Guideline Special Announcements Please check www.asco.org/guidelines/antiemetics for current FDA alert(s) and safety announcement(s) on antiemetics 2 Introduction
Guideline Update on Antiemetics Clinical Practice Guideline Special Announcements Please check www.asco.org/guidelines/antiemetics for current FDA alert(s) and safety announcement(s) on antiemetics 2 Introduction
PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER
 June 2004 PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER CONSENSUS CONFERENCE ON ANTIEMETIC THERAPY PERUGIA, March 29-31, 2004 DELAYED EMESIS WORKING
June 2004 PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER CONSENSUS CONFERENCE ON ANTIEMETIC THERAPY PERUGIA, March 29-31, 2004 DELAYED EMESIS WORKING
Using a Simple Diary for Management of Nausea and Vomiting During Chemotherapy
 Using a Simple Diary for Management of Nausea and Vomiting During Chemotherapy Problem identification Nausea and vomiting (N&V) are frequent complications following chemotherapy, even when taking 5-HT3
Using a Simple Diary for Management of Nausea and Vomiting During Chemotherapy Problem identification Nausea and vomiting (N&V) are frequent complications following chemotherapy, even when taking 5-HT3
Management of chemotherapyinduced nausea and vomiting
 p h a r m a c o t h e r a p y Management of induced nausea and vomiting Authors Key words F. Van Ryckeghem and S. Van Belle Antiemetic therapy,, prevention Summary Chemotherapy-induced nausea and vomiting
p h a r m a c o t h e r a p y Management of induced nausea and vomiting Authors Key words F. Van Ryckeghem and S. Van Belle Antiemetic therapy,, prevention Summary Chemotherapy-induced nausea and vomiting
Chemotherapy Induced Nausea and Vomiting
 Chemotherapy Induced Nausea and Vomiting Aminah Jatoi, M.D. Professor of Oncology Mayo Clinic Rochester, Minnesota April 27, 2017 clinical and biologic fundamentals of chemotherapy induced nausea and vomiting
Chemotherapy Induced Nausea and Vomiting Aminah Jatoi, M.D. Professor of Oncology Mayo Clinic Rochester, Minnesota April 27, 2017 clinical and biologic fundamentals of chemotherapy induced nausea and vomiting
Clinical Policy: Ondansetron (Zuplenz) Reference Number: CP.PMN.45 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PMN.45 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Zuplenz) Reference Number: CP.PMN.45 Effective Date: 09.01.06 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Zuplenz) Reference Number: CP.PMN.45 Effective Date: 09.01.06 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Original. Key words : breast cancer, chemotherapy-induced nausea and vomiting, quality of life, Functional Living Index Emesis
 Showa Univ J Med Sci 30 2, 285 296, June 2018 Original The Impact on Quality of Life of Highly Effective Antiemetic Therapy among Breast Cancer Patients Receiving Anthracycline Plus Cyclophosphamide-based
Showa Univ J Med Sci 30 2, 285 296, June 2018 Original The Impact on Quality of Life of Highly Effective Antiemetic Therapy among Breast Cancer Patients Receiving Anthracycline Plus Cyclophosphamide-based
Chemotherapy-induced nausea and vomiting (CINV)
") At a Glance Practical Implications e54 Author Information e57 Full text and PDF 5-HT3 Receptor Antagonist Effects in Cancer Patients With Multiple Risk Factors Original Research Claudio Faria, PharmD,
At a Glance Practical Implications e54 Author Information e57 Full text and PDF 5-HT3 Receptor Antagonist Effects in Cancer Patients With Multiple Risk Factors Original Research Claudio Faria, PharmD,
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Antiemetic Therapy Table of Contents Coverage Policy... 1 General Background... 6 Coding/Billing Information... 8 References... 8 Effective Date... 1/1/2018
Cigna Drug and Biologic Coverage Policy Subject Antiemetic Therapy Table of Contents Coverage Policy... 1 General Background... 6 Coding/Billing Information... 8 References... 8 Effective Date... 1/1/2018
PACIFIC MEDICAL TRAINING Arrhythmia Interpretation
 PACIFIC MEDICAL TRAINING Arrhythmia Interpretation Introduction Activity Summary Target Audience Educational Objectives Nursing Educational Objective Faculty Physician Continuing Medical Education Nursing
PACIFIC MEDICAL TRAINING Arrhythmia Interpretation Introduction Activity Summary Target Audience Educational Objectives Nursing Educational Objective Faculty Physician Continuing Medical Education Nursing
MASCC Guidelines for Antiemetic control: An update
 MASCC / ISOO 17 th International Symposium Supportive Care in Cancer June 30 July 2, 2005 / Geneva, Switzerland MASCC Guidelines for Antiemetic control: An update Sussanne Börjeson, RN, PhD Linköping University,
MASCC / ISOO 17 th International Symposium Supportive Care in Cancer June 30 July 2, 2005 / Geneva, Switzerland MASCC Guidelines for Antiemetic control: An update Sussanne Börjeson, RN, PhD Linköping University,
An Evidence Practice Gap in Antiemetic Prescription with Chemotherapy
 2014 An Evidence Practice Gap in Antiemetic Prescription with Chemotherapy Chepsy C Philip 1*, Biju George 1 1 Department of Clinical Haematology, CMC Vellore, Tamil Nadu, India. ARTICLE INFO Article type:
2014 An Evidence Practice Gap in Antiemetic Prescription with Chemotherapy Chepsy C Philip 1*, Biju George 1 1 Department of Clinical Haematology, CMC Vellore, Tamil Nadu, India. ARTICLE INFO Article type:
Student Project PRACTICE-BASED RESEARCH
 Pharmacist-Driven Management of Chemotherapy Induced Nausea and Vomiting in Hospitalized Adult Oncology Patients. A Retrospective Comparative Study Ramy Elshaboury, PharmD 1 and Kathleen Green, PharmD,
Pharmacist-Driven Management of Chemotherapy Induced Nausea and Vomiting in Hospitalized Adult Oncology Patients. A Retrospective Comparative Study Ramy Elshaboury, PharmD 1 and Kathleen Green, PharmD,
Updates in Chemotherapy-Induced Nausea and Vomiting (CINV) 2017
 2017") Updates in Chemotherapy-Induced Nausea and Vomiting (CINV) 2017 MELISSA C. MACKEY, PHARMD, BCPS, BCOP ONCOLOGY CLINICAL PHARMACIST DUKE UNIVERSITY HOSPITAL AUGUST 5, 2017 Objectives Review risk factors
Updates in Chemotherapy-Induced Nausea and Vomiting (CINV) 2017 MELISSA C. MACKEY, PHARMD, BCPS, BCOP ONCOLOGY CLINICAL PHARMACIST DUKE UNIVERSITY HOSPITAL AUGUST 5, 2017 Objectives Review risk factors
Clinical Policy: Oral Antiemetics (5-HT3 Antagonists) Reference Number: CP.PMN.11 Effective Date: Last Review Date: 05.18
 Reference Number: CP.PMN.11 Effective Date: Last Review Date: 05.18") Clinical Policy: (5-HT3 Antagonists) Reference Number: CP.PMN.11 Effective Date: 09.01.06 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (5-HT3 Antagonists) Reference Number: CP.PMN.11 Effective Date: 09.01.06 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy
David G. Frame, PharmD. he etiology of nausea and vomiting is multifactorial,
 r e v i e w Best Practice Management of CINV in Oncology Patients: I. Physiology and Treatment of CINV Multiple Neurotransmitters and Receptors and the Need for Combination Therapeutic Approaches David
r e v i e w Best Practice Management of CINV in Oncology Patients: I. Physiology and Treatment of CINV Multiple Neurotransmitters and Receptors and the Need for Combination Therapeutic Approaches David
Thalidomide for prevention of chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy
 Thalidomide for prevention of chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy Geng Song, Qian He, Fanfan Li, and Nianfei Wang Department of Oncology, The Second Affiliated
Thalidomide for prevention of chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy Geng Song, Qian He, Fanfan Li, and Nianfei Wang Department of Oncology, The Second Affiliated
Review Article Treatment of Breakthrough and Refractory Chemotherapy-Induced Nausea and Vomiting
 Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 595894, 6 pages http://dx.doi.org/10.1155/2015/595894 Review Article Treatment of Breakthrough and Refractory Chemotherapy-Induced
Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 595894, 6 pages http://dx.doi.org/10.1155/2015/595894 Review Article Treatment of Breakthrough and Refractory Chemotherapy-Induced
PREVENTION OF CHEMOTHERAPY INDUCED NAUSEA AND VOMITING IN ELDERLY CANCER PATIENTS JØRN HERRSTEDT, M.D. COPENHAGEN UNIVERSITY HOSPITAL HERLEV, DENMARK
 PREVENTION OF CHEMOTHERAPY INDUCED NAUSEA AND VOMITING IN ELDERLY CANCER PATIENTS JØRN HERRSTEDT, M.D. COPENHAGEN UNIVERSITY HOSPITAL HERLEV, DENMARK HISTORY OF ANTIEMETICS 1979 A corticosteroid is superior
PREVENTION OF CHEMOTHERAPY INDUCED NAUSEA AND VOMITING IN ELDERLY CANCER PATIENTS JØRN HERRSTEDT, M.D. COPENHAGEN UNIVERSITY HOSPITAL HERLEV, DENMARK HISTORY OF ANTIEMETICS 1979 A corticosteroid is superior
Overview of the neurokinin-1 receptor antagonists
 Editorial Page 1 of 6 Overview of the neurokinin-1 receptor antagonists Rudolph M. avari Division of Hematology Oncology, School of Medicine, University of Alabama Birmingham, Birmingham, AL, USA Correspondence
Editorial Page 1 of 6 Overview of the neurokinin-1 receptor antagonists Rudolph M. avari Division of Hematology Oncology, School of Medicine, University of Alabama Birmingham, Birmingham, AL, USA Correspondence
Clinical Policy: Dolasetron (Anzemet) Reference Number: ERX.NPA.83 Effective Date:
 Reference Number: ERX.NPA.83 Effective Date:") Clinical Policy: (Anzemet) Reference Number: ERX.NPA.83 Effective Date: 09.01.18 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Anzemet) Reference Number: ERX.NPA.83 Effective Date: 09.01.18 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Nausea and Vomiting Team. Outcome: Nausea and Vomiting. Scope of the Problem. Definition: Nausea
 Nausea and Vomiting: The Continuing Battle to Improve Outcomes Jan Tipton, MSN, RN, AOCN Oncology CNS Medical University of Ohio Toledo, Ohio jtipton@meduohio.edu Nausea and Vomiting Team Jan Tipton, MSN,
Nausea and Vomiting: The Continuing Battle to Improve Outcomes Jan Tipton, MSN, RN, AOCN Oncology CNS Medical University of Ohio Toledo, Ohio jtipton@meduohio.edu Nausea and Vomiting Team Jan Tipton, MSN,
Prophylaxis and Management of Chemotherapy-Induced Nausea and Vomiting: A Comparison of How the Experts Practice
 The following is an edited transcript of a CME/CE- certified video series and is intended for informational purposes only. To receive credit for the activity, participants must view the videos online at
The following is an edited transcript of a CME/CE- certified video series and is intended for informational purposes only. To receive credit for the activity, participants must view the videos online at
Drug Name: Aprepitant (Emend ) Manufacturer: Merck & Co., Inc.
 Manufacturer: Merck & Co., Inc.") Drug Name: Aprepitant (Emend ) Manufacturer: Merck & Co., Inc. Pharmacology: Aprepitant (previously known as MK-0839 and L-754030) is a new molecular entity that is the first in a new therapeutic class,
Drug Name: Aprepitant (Emend ) Manufacturer: Merck & Co., Inc. Pharmacology: Aprepitant (previously known as MK-0839 and L-754030) is a new molecular entity that is the first in a new therapeutic class,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Anzemet) Reference Number: CP.PMN.141 Effective Date: 09.01.06 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
Clinical Policy: (Anzemet) Reference Number: CP.PMN.141 Effective Date: 09.01.06 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
Clinical Policy: Nabilone (Cesamet) Reference Number: ERX.NPA.35 Effective Date:
 Reference Number: ERX.NPA.35 Effective Date:") Clinical Policy: (Cesamet) Reference Number: ERX.NPA.35 Effective Date: 09.01.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Cesamet) Reference Number: ERX.NPA.35 Effective Date: 09.01.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
ANTIEMETIC RESEARCH AND PROGRESS: Richard J. Gralla, MD, FACP Professor of Medicine Albert Einstein College of Medicine Bronx, New York
 ANTIEMETIC RESEARCH AND PROGRESS: Richard J. Gralla, MD, FACP Professor of Medicine Albert Einstein College of Medicine Bronx, New York THE FUTURE OF ANTIEMETICS Fausto Roila Medical Oncology, Terni, Italy
ANTIEMETIC RESEARCH AND PROGRESS: Richard J. Gralla, MD, FACP Professor of Medicine Albert Einstein College of Medicine Bronx, New York THE FUTURE OF ANTIEMETICS Fausto Roila Medical Oncology, Terni, Italy
Drug: Aprepitant (Emend ) Date of Review: 4/01/10
 Date of Review: 4/01/10") CAMBRIDGESHIRE JOINT PRESCRIBING GROUP Business Case Evaluation and Recommendation Document Drug: Aprepitant (Emend ) Date of Review: 4/01/10 Business Case Decision and date: DOUBLE RED, 20 January 2010
CAMBRIDGESHIRE JOINT PRESCRIBING GROUP Business Case Evaluation and Recommendation Document Drug: Aprepitant (Emend ) Date of Review: 4/01/10 Business Case Decision and date: DOUBLE RED, 20 January 2010
GUIDELINES FOR ANTIEMETIC USE IN ONCOLOGY SUMMARY CLASSIFICATION
 GUIDELINES FOR ANTIEMETIC USE IN ONCOLOGY SUMMARY More than half of all cancer patients experience nausea or vomiting during the course of their treatment. If nausea or vomiting becomes severe enough,
GUIDELINES FOR ANTIEMETIC USE IN ONCOLOGY SUMMARY More than half of all cancer patients experience nausea or vomiting during the course of their treatment. If nausea or vomiting becomes severe enough,
Drug Therapy Guidelines
 Drug Therapy Guidelines Applicable Medical Benefit Effective: 6/15/18 Pharmacy- Formulary 1 x Next Review: 6/19 Pharmacy- Formulary 2 x Date of Origin: 4/99 Antiemetic Agents: Zofran /ODT (ondansetron/ondansetron
Drug Therapy Guidelines Applicable Medical Benefit Effective: 6/15/18 Pharmacy- Formulary 1 x Next Review: 6/19 Pharmacy- Formulary 2 x Date of Origin: 4/99 Antiemetic Agents: Zofran /ODT (ondansetron/ondansetron
Corporate Medical Policy
 Antiemetic Injection Therapy Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: antiemetic_injection_therapy 5/2015 3/2017 3/2018 3/2017 Description of Procedure
Antiemetic Injection Therapy Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: antiemetic_injection_therapy 5/2015 3/2017 3/2018 3/2017 Description of Procedure
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Cesamet) Reference Number: CP.PMN.160 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Cesamet) Reference Number: CP.PMN.160 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Managing Adverse Events in the Cancer Patient. Learning Objectives. Chemotherapy-Induced Nausea/Vomiting
 Managing Adverse Events in the Cancer Patient Lisa A Thompson, PharmD, BCOP Assistant Professor University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences Learning Objectives Describe
Managing Adverse Events in the Cancer Patient Lisa A Thompson, PharmD, BCOP Assistant Professor University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences Learning Objectives Describe
A C E A C T I V I T Y
 HEAD A C E A C T I V I T Y Jointly sponsored by Robert Michael Educational Institute LLC and Postgraduate Institute for Medicine Supported in part with an educational grant from Celgene CONTENTS Agenda...................................................................................
HEAD A C E A C T I V I T Y Jointly sponsored by Robert Michael Educational Institute LLC and Postgraduate Institute for Medicine Supported in part with an educational grant from Celgene CONTENTS Agenda...................................................................................
Ivyspring International Publisher. Introduction. Journal of Cancer 2017, Vol. 8. Abstract
 1371 Ivyspring International Publisher Research Paper Journal of Cancer 2017; 8(8): 1371-1377. doi: 10.7150/jca.17102 Antiemetic Effectiveness and Cost-Saving of Aprepitant plus Granisetron Is Superior
1371 Ivyspring International Publisher Research Paper Journal of Cancer 2017; 8(8): 1371-1377. doi: 10.7150/jca.17102 Antiemetic Effectiveness and Cost-Saving of Aprepitant plus Granisetron Is Superior
A systemic review and meta analysis of Aprepitant Combination Regimens (ACR) for prevention of Chemotherapy induced Nausea
 for prevention of Chemotherapy induced Nausea") A systemic review and meta analysis of Aprepitant Combination Regimens (ACR) for prevention of Chemotherapy induced Nausea and Vomiting (CINV) in adults Fahad Zubair, PGY 3 UB CHS Internal Medicine Nausea
A systemic review and meta analysis of Aprepitant Combination Regimens (ACR) for prevention of Chemotherapy induced Nausea and Vomiting (CINV) in adults Fahad Zubair, PGY 3 UB CHS Internal Medicine Nausea
ANTIEMETIC GUIDELINES: MASCC/ESMO
 Open Issues for CINV Do we reliably measure that? Do we control nausea optimally? Are guidelines useful for oral therapies related nausea and vomiting? Breakthrough and refractory nausea and vomiting:
Open Issues for CINV Do we reliably measure that? Do we control nausea optimally? Are guidelines useful for oral therapies related nausea and vomiting? Breakthrough and refractory nausea and vomiting:
Patient-Centered Management of Chemotherapy-Induced Nausea and Vomiting
 Clear and accurate communication between patients and health care teams is the key to successfully controlling chemotherapy-induced nausea and vomiting. Roseate Spoonbill_2005. Photograph courtesy of Henry
Clear and accurate communication between patients and health care teams is the key to successfully controlling chemotherapy-induced nausea and vomiting. Roseate Spoonbill_2005. Photograph courtesy of Henry
Richard J. Gralla, MD Medical Director Quality of Life Research Associates New York, NY
 Oncology Consultations Improving the Management of Chemotherapy-Induced Nausea and Vomiting (CINV) A CE-Certified Activity Featuring Consultations With Supported by an educational grant from Eisai. Dannemiller
Oncology Consultations Improving the Management of Chemotherapy-Induced Nausea and Vomiting (CINV) A CE-Certified Activity Featuring Consultations With Supported by an educational grant from Eisai. Dannemiller
Supported by an unrestricted educational grant by Merck & Co.
 Supported by an unrestricted educational grant by Merck & Co. TABLE OF CONTENTS Agenda & Faculty List...2 Course Description...3 Learning Objectives...3 Accreditation Statement & Credit Designation...3
Supported by an unrestricted educational grant by Merck & Co. TABLE OF CONTENTS Agenda & Faculty List...2 Course Description...3 Learning Objectives...3 Accreditation Statement & Credit Designation...3
Research Article. Chemotherapy-induced nausea and vomiting in Portugal: incidence versus healthcare provider estimations and effect on quality of life
 Research Article Chemotherapy-induced nausea and vomiting in Portugal: incidence versus healthcare provider estimations and effect on quality of life Aim: To compare chemotherapy-induced nausea and vomiting
Research Article Chemotherapy-induced nausea and vomiting in Portugal: incidence versus healthcare provider estimations and effect on quality of life Aim: To compare chemotherapy-induced nausea and vomiting
Adherence to guidelines on prophylaxis of chemotherapy-induced nausea and vomiting in the National Cancer Institute, Sudan
 Southern African Journal of Gynaecological Oncology 2017; 9(2):7-11 Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Southern African Journal of Gynaecological Oncology 2017; 9(2):7-11 Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
, Gianluca Ballinari. ) receptor antagonist,
 receptor antagonist,") Leukemia & Lymphoma, March 2014; 55(3): 544 550 2014 Informa UK, Ltd. ISSN: 1042-8194 print / 1029-2403 online DOI: 10.3109/10428194.2013.813498 ORIGINAL ARTICLE: CLINICAL Multicenter phase IV study of
Leukemia & Lymphoma, March 2014; 55(3): 544 550 2014 Informa UK, Ltd. ISSN: 1042-8194 print / 1029-2403 online DOI: 10.3109/10428194.2013.813498 ORIGINAL ARTICLE: CLINICAL Multicenter phase IV study of
MINI-REVIEW. Aprepitant in the Prevention of Vomiting Induced by Moderately and Highly Emetogenic Chemotherapy
 MINI-REVIEW Aprepitant in the Prevention of Vomiting Induced by Moderately and Highly Emetogenic Chemotherapy Shi-Yong Wang 1 *, Zhen-Jun Yang 2, Zhe Zhang 1, Hui Zhang 1 Abstract Chemotherapy is a major
MINI-REVIEW Aprepitant in the Prevention of Vomiting Induced by Moderately and Highly Emetogenic Chemotherapy Shi-Yong Wang 1 *, Zhen-Jun Yang 2, Zhe Zhang 1, Hui Zhang 1 Abstract Chemotherapy is a major
ORIGINAL ARTICLE. Ralph Boccia & Steven Grunberg & Edwin Franco-Gonzales & Edward Rubenstein & Daniel Voisin
 Support Care Cancer (2013) 21:1453 1460 DOI 10.1007/s00520-012-1691-5 ORIGINAL ARTICLE Efficacy of oral palonosetron compared to intravenous palonosetron for the prevention of chemotherapy-induced nausea
Support Care Cancer (2013) 21:1453 1460 DOI 10.1007/s00520-012-1691-5 ORIGINAL ARTICLE Efficacy of oral palonosetron compared to intravenous palonosetron for the prevention of chemotherapy-induced nausea
Effect of chemotherapy-induced nausea on patients quality of life
 Art & science literature review Effect of chemotherapy-induced nausea on patients quality of life Melissa Fitzgerald and Siobhan Murphy discuss ways to manage treatment side effects including non pharmacological
Art & science literature review Effect of chemotherapy-induced nausea on patients quality of life Melissa Fitzgerald and Siobhan Murphy discuss ways to manage treatment side effects including non pharmacological
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT
 DRAFT") European Medicines Agency Evaluation of Medicines for Human Use London, 17 February 2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT GUIDELINE ON NON-CLINICAL AND CLINICAL DEVELOPMENT OF
European Medicines Agency Evaluation of Medicines for Human Use London, 17 February 2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT GUIDELINE ON NON-CLINICAL AND CLINICAL DEVELOPMENT OF
Prevention and Management of cancer disease and of chemo-and radiotherapyinduced nausea and vomiting
 Prevention and Management of cancer disease and of chemo-and radiotherapyinduced nausea and vomiting Focusing on the updated MASCC/ESMO guidelines Karin Jordan Department of Hematology and Oncology, University
Prevention and Management of cancer disease and of chemo-and radiotherapyinduced nausea and vomiting Focusing on the updated MASCC/ESMO guidelines Karin Jordan Department of Hematology and Oncology, University
ANTIEMETICS and FEBRILE NEUTROPENIA. Matti S. Aapro Genolier Switzerland
 ANTIEMETICS and FEBRILE NEUTROPENIA Matti S. Aapro Genolier Switzerland 2010 Multinational Association of Supportive Care in Cancer TM All rights reserved worldwide. Disclosures Collaborations in this
ANTIEMETICS and FEBRILE NEUTROPENIA Matti S. Aapro Genolier Switzerland 2010 Multinational Association of Supportive Care in Cancer TM All rights reserved worldwide. Disclosures Collaborations in this
Conflicts of Interest. Review of Antiemetic Guidelines. Learning Objectives. What is Emesis Anyways? Pharmacy Technician Learning Objectives
 Conflicts of Interest No financial relationships to disclose Review of Antiemetic Guidelines Matthew Fox, PharmD, BCPS, BCOP Clinical Oncology Pharmacist Baptist MD Anderson Jacksonville, Florida October
Conflicts of Interest No financial relationships to disclose Review of Antiemetic Guidelines Matthew Fox, PharmD, BCPS, BCOP Clinical Oncology Pharmacist Baptist MD Anderson Jacksonville, Florida October
Subject: Fosnetupitant-Palonosetron (Akynzeo) IV
 IV") 09-J3000-01 Original Effective Date: 06/15/18 Reviewed: 05/09/18 Revised: 01/01/19 Subject: Fosnetupitant-Palonosetron (Akynzeo) IV THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
09-J3000-01 Original Effective Date: 06/15/18 Reviewed: 05/09/18 Revised: 01/01/19 Subject: Fosnetupitant-Palonosetron (Akynzeo) IV THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
Safety, efficacy, and patient acceptability of singledose fosaprepitant regimen for the prevention of chemotherapy-induced nausea and vomiting
 Patient Preference and Adherence open access to scientific and medical research Open Access Full Text Article Review Safety, efficacy, and patient acceptability of singledose fosaprepitant regimen for
Patient Preference and Adherence open access to scientific and medical research Open Access Full Text Article Review Safety, efficacy, and patient acceptability of singledose fosaprepitant regimen for
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Kytril, Sancuso, Sustol) Reference Number: CP.PMN.74 Effective Date: 11.01.16 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important
Clinical Policy: (Kytril, Sancuso, Sustol) Reference Number: CP.PMN.74 Effective Date: 11.01.16 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important
Can Granisetron Injection Used as Primary Prophylaxis Improve the Control of Nausea and Vomiting with Low- Emetogenic Chemotherapy?
 DOI:http://dx.doi.org/10.7314/APJCP.2013.14.1.469 RESEARCH ARTICLE Can Granisetron Injection Used as Primary Prophylaxis Improve the Control of Nausea and Vomiting with Low- Emetogenic Chemotherapy? Chan
DOI:http://dx.doi.org/10.7314/APJCP.2013.14.1.469 RESEARCH ARTICLE Can Granisetron Injection Used as Primary Prophylaxis Improve the Control of Nausea and Vomiting with Low- Emetogenic Chemotherapy? Chan
Published Ahead of Print on September 26, 2011 as /JCO J Clin Oncol by American Society of Clinical Oncology
 Published Ahead of Print on September 26, 2011 as 10.1200/JCO.2010.34.4614 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.34.4614 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C
Published Ahead of Print on September 26, 2011 as 10.1200/JCO.2010.34.4614 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.34.4614 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C
Managements of Chemotherpay Induded Nausea and Vomiting
 REVIEW ARTICLE Managements of Chemotherpay Induded Nausea and Vomiting Department of Surgery, The Catholic University of Korea Sung Geun Kim 23 24 Sung Geun Kim Korean Journal of Clinical Oncology Summer
REVIEW ARTICLE Managements of Chemotherpay Induded Nausea and Vomiting Department of Surgery, The Catholic University of Korea Sung Geun Kim 23 24 Sung Geun Kim Korean Journal of Clinical Oncology Summer
The MASCC Guidelines Policy
 The MASCC Guidelines Policy Recommendations for MASCC Guideline Construction and the Endorsement of Externally Generated Guidelines Preamble MASCC recognizes that providing supportive care facilitates
The MASCC Guidelines Policy Recommendations for MASCC Guideline Construction and the Endorsement of Externally Generated Guidelines Preamble MASCC recognizes that providing supportive care facilitates
4/26/2016. Disclosure. Institution. Objectives. Background. Background
 Pharmacist-led patient education: the impact of managing chemotherapy-induced nausea and vomiting (CINV) in ambulatory oncology patients Kristyn Gutowski, PharmD, RPh PGY1 Pharmacy Resident St. Vincent
Pharmacist-led patient education: the impact of managing chemotherapy-induced nausea and vomiting (CINV) in ambulatory oncology patients Kristyn Gutowski, PharmD, RPh PGY1 Pharmacy Resident St. Vincent
Prevention of Antineoplastic Medication induced Nausea and Vomiting in Pediatric Cancer Patients
 Prevention of Antineoplastic Medication induced Nausea and Vomiting in Pediatric Cancer Patients Done by :Meznah Zaid Al-Mutairi Pharm.D Candidate PNU University College of Pharmacy Introduction Nausea
Prevention of Antineoplastic Medication induced Nausea and Vomiting in Pediatric Cancer Patients Done by :Meznah Zaid Al-Mutairi Pharm.D Candidate PNU University College of Pharmacy Introduction Nausea
Comparing Different Antiemetic Regimens for Chemotherapy Induced Nausea and Vomiting
 Comparing Different Antiemetic Regimens for Chemotherapy Induced Nausea and Vomiting Sayantani Ghosh, Saugat Dey Corresponding author: Sayantani Ghosh (ghoshsayantani@rediffmail.com) Correspondence concerning
Comparing Different Antiemetic Regimens for Chemotherapy Induced Nausea and Vomiting Sayantani Ghosh, Saugat Dey Corresponding author: Sayantani Ghosh (ghoshsayantani@rediffmail.com) Correspondence concerning
Acute emesis: moderately emetogenic chemotherapy
 Support Care Cancer (2005) 13:97 103 DOI 10.1007/s00520-004-0701-7 R E V I E W R T I C L E Jørn Herrstedt Jim M. Koeller Fausto Roila Paul J. Hesketh David Warr Cynthia Rittenberg Mario Dicato cute emesis:
Support Care Cancer (2005) 13:97 103 DOI 10.1007/s00520-004-0701-7 R E V I E W R T I C L E Jørn Herrstedt Jim M. Koeller Fausto Roila Paul J. Hesketh David Warr Cynthia Rittenberg Mario Dicato cute emesis:
Review Report. (11) Olanzapine Fine Granules 1% "DSEP" (14) Olanzapine OD Tablets 10 mg "DSEP" (17) Olanzapine Tablets 10 mg "Nichi-Iko"
 Olanzapine Fine Granules 1% DSEP (14) Olanzapine OD Tablets 10 mg DSEP (17) Olanzapine Tablets 10 mg Nichi-Iko") Review Report November 13, 2017 Pharmaceuticals and Medical Devices Agency The following are the results of the review of the following pharmaceutical products submitted for marketing approval conducted
Review Report November 13, 2017 Pharmaceuticals and Medical Devices Agency The following are the results of the review of the following pharmaceutical products submitted for marketing approval conducted
Available online at ScienceDirect. journal homepage:
 European Journal of Cancer 57 (2016) 23e30 Available online at www.sciencedirect.com ScienceDirect journal homepage: www.ejcancer.com Original Research Efficacy and safety of rolapitant for prevention
European Journal of Cancer 57 (2016) 23e30 Available online at www.sciencedirect.com ScienceDirect journal homepage: www.ejcancer.com Original Research Efficacy and safety of rolapitant for prevention
Ping-Tsung Chen, MD; Chuang-Chi Liaw, MD
 Original Article 167 Intravenous Ondansetron plus Intravenous Dexamethasone with Different Ondansetron Dosing Schedules during Multiple Cycles of Cisplatin-based Chemotherapy Ping-Tsung Chen, MD; Chuang-Chi
Original Article 167 Intravenous Ondansetron plus Intravenous Dexamethasone with Different Ondansetron Dosing Schedules during Multiple Cycles of Cisplatin-based Chemotherapy Ping-Tsung Chen, MD; Chuang-Chi
Pediatric Trials 23/04/2018. Disclosures. Nausea and Vomiting Control in Adults and Children: Mind the Gap! Learning Objectives
 Nausea and Vomiting Control in Adults and Children: Mind the Gap! Disclosures No relevant conflicts of interest Lee Dupuis, RPh, PhD May 5, 2018 2 Learning Objectives At the end of this presentation, attendees
Nausea and Vomiting Control in Adults and Children: Mind the Gap! Disclosures No relevant conflicts of interest Lee Dupuis, RPh, PhD May 5, 2018 2 Learning Objectives At the end of this presentation, attendees
Chemotherapy-Related Nausea and Vomiting and Treatment-Related Nausea and Vomiting
 CHAPTER 12 Chemotherapy-Related Nausea and Vomiting and Treatment-Related Nausea and Vomiting Elizabeth Blanchard T he ability of chemotherapy to cause nausea and vomiting is legendary and remains a widespread
CHAPTER 12 Chemotherapy-Related Nausea and Vomiting and Treatment-Related Nausea and Vomiting Elizabeth Blanchard T he ability of chemotherapy to cause nausea and vomiting is legendary and remains a widespread
Clinical Policy: Aprepitant (Emend) Reference Number: CP.PMN.19 Effective Date: 11/06 Last Review Date: 08/17
 Reference Number: CP.PMN.19 Effective Date: 11/06 Last Review Date: 08/17") Clinical Policy: (Emend) Reference Number: CP.PMN.19 Effective Date: 11/06 Last Review Date: 08/17 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Emend) Reference Number: CP.PMN.19 Effective Date: 11/06 Last Review Date: 08/17 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Drug Use Criteria: Oral Serotonin 5-HT3 Receptor Antagonists for Nausea and Vomiting
 Texas Vendor Drug Program Drug Use Criteria: Oral Serotonin 5-HT3 Receptor Antagonists for Nausea and Vomiting Publication History Developed September 1996. Revised July 2018; September 2016; June 2015;
Texas Vendor Drug Program Drug Use Criteria: Oral Serotonin 5-HT3 Receptor Antagonists for Nausea and Vomiting Publication History Developed September 1996. Revised July 2018; September 2016; June 2015;
CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING
 CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to the edit Experts Master
CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to the edit Experts Master
Prevention CINV (highly emetogenic) Prevention PONV
 Prevention PONV") Reviews/Evaluations 5-Hydroxytryptamine3 (5-HT3) Receptor Antagonists Generic Name Brand Name Manufacturer Dolasetron Anzemet Aventis Granisetron Kytril Roche Ondansetron Zofran GlaxoSmithKline I. FDA
Reviews/Evaluations 5-Hydroxytryptamine3 (5-HT3) Receptor Antagonists Generic Name Brand Name Manufacturer Dolasetron Anzemet Aventis Granisetron Kytril Roche Ondansetron Zofran GlaxoSmithKline I. FDA
HIV/AIDS in Practice. An Expert Commentary with Myron Cohen, MD. A Clinical Context Report
 HIV/AIDS in Practice An Expert Commentary with Myron Cohen, MD A Clinical Context Report Clinical Context: HIV/AIDS in Practice Expert Commentary Jointly Sponsored by: and Clinical Context: HIV/AIDS in
HIV/AIDS in Practice An Expert Commentary with Myron Cohen, MD A Clinical Context Report Clinical Context: HIV/AIDS in Practice Expert Commentary Jointly Sponsored by: and Clinical Context: HIV/AIDS in
International Symposium on Supportive Care in Cancer, MASCC/ISOO 2013, Berlin, Germany. What was hot at MASCC/ISOO Annual Meeting this year?
 International Symposium on Supportive Care in Cancer, MASCC/ISOO 2013, Berlin, Germany What was hot at MASCC/ISOO Annual Meeting this year? Supportive Care Makes Excellent Cancer Care Possible. This slogan
International Symposium on Supportive Care in Cancer, MASCC/ISOO 2013, Berlin, Germany What was hot at MASCC/ISOO Annual Meeting this year? Supportive Care Makes Excellent Cancer Care Possible. This slogan
Clinical Review Report
 CADTH COMMON DRUG REVIEW Clinical Review Report Netupitant/Palonosetron 300 mg/0.5 mg (Akynzeo) (Purdue Pharma) Indication: In combination with dexamethasone, onceper-cycle treatment for the prevention
CADTH COMMON DRUG REVIEW Clinical Review Report Netupitant/Palonosetron 300 mg/0.5 mg (Akynzeo) (Purdue Pharma) Indication: In combination with dexamethasone, onceper-cycle treatment for the prevention
CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report
 CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report Netupitant/Palonosetron 300 mg/0.5 mg (Akynzeo) (Purdue Pharma) Indication: In combination with dexamethasone, once-percycle treatment for the prevention
CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report Netupitant/Palonosetron 300 mg/0.5 mg (Akynzeo) (Purdue Pharma) Indication: In combination with dexamethasone, once-percycle treatment for the prevention
Cancer Studies Open Access
 Cancer Studies Open Access Received: Sep 16, 2014 Accepted: Oct 10, 2014 Published: Oct 14, 2014 http://dx.doi.org/10.14437/csoa-1-107 Research Hiroshi Ishiguro, Cancer Stud Open Access 2014: 1:2 Prevention
Cancer Studies Open Access Received: Sep 16, 2014 Accepted: Oct 10, 2014 Published: Oct 14, 2014 http://dx.doi.org/10.14437/csoa-1-107 Research Hiroshi Ishiguro, Cancer Stud Open Access 2014: 1:2 Prevention
Prevention of chemotherapy- and radiotherapy-induced emesis: results of the 2004 Perugia International Antiemetic Consensus Conference
 Annals of Oncology 17: 20 28, 2006 doi:10.1093/annonc/mdj078 Published online 28 November 2005 Prevention of chemotherapy- and radiotherapy-induced emesis: results of the 2004 Perugia International Antiemetic
Annals of Oncology 17: 20 28, 2006 doi:10.1093/annonc/mdj078 Published online 28 November 2005 Prevention of chemotherapy- and radiotherapy-induced emesis: results of the 2004 Perugia International Antiemetic
Chemotherapy-induced nausea and vomiting
 Comparison of antiemetic efficacy and safety of palonosetron vs ondansetron in the prevention of chemotherapy-induced nausea and vomiting in children Veerendra Patil, MD, FNB; Harsha Prasada, MD, DCH,
Comparison of antiemetic efficacy and safety of palonosetron vs ondansetron in the prevention of chemotherapy-induced nausea and vomiting in children Veerendra Patil, MD, FNB; Harsha Prasada, MD, DCH,
Subject: NK-1 receptor antagonist injectable therapy (Emend, Cinvanti, Varubi )
") 09-J2000-60 Original Effective Date: 06/15/16 Reviewed: 04/11/18 Revised: 01/01/19 Subject: NK-1 receptor antagonist injectable therapy (Emend, Cinvanti, Varubi ) THIS MEDICAL COVERAGE GUIDELINE IS NOT
09-J2000-60 Original Effective Date: 06/15/16 Reviewed: 04/11/18 Revised: 01/01/19 Subject: NK-1 receptor antagonist injectable therapy (Emend, Cinvanti, Varubi ) THIS MEDICAL COVERAGE GUIDELINE IS NOT
CIC Edizioni Internazionali. Chemotherapy-induced nausea and vomiting: update and future options. Review
 Review Chemotherapy-induced nausea and vomiting: update and future options Umberto Pacetti 1 Silvia Ileana Sara Fattoruso 1 Enzo Veltri 2 1 Operative Unit of Oncology, A. Fiorini Hospital, Terracina, Italy
Review Chemotherapy-induced nausea and vomiting: update and future options Umberto Pacetti 1 Silvia Ileana Sara Fattoruso 1 Enzo Veltri 2 1 Operative Unit of Oncology, A. Fiorini Hospital, Terracina, Italy
CME/CE POSTTEST CME/CE QUESTIONS
 CME/CE POSTTEST CME/CE QUESTIONS Controlling Asthma Severity: Identifying Unmet Needs and Optimizing Therapeutic Options There are no fees for participating in and receiving continuing medical education
CME/CE POSTTEST CME/CE QUESTIONS Controlling Asthma Severity: Identifying Unmet Needs and Optimizing Therapeutic Options There are no fees for participating in and receiving continuing medical education
Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients
 in Adult Cancer Patients") Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients By Zahra Shaghaghi, Pharm-D, BCOP, PhC Prepared for 2018 NMSHP Balloon Fiesta Symposium Goals and Objectives: Describe
Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients By Zahra Shaghaghi, Pharm-D, BCOP, PhC Prepared for 2018 NMSHP Balloon Fiesta Symposium Goals and Objectives: Describe
Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients
 in Adult Cancer Patients") Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients By Zahra Shaghaghi, Pharm-D, BCOP, PhC Prepared for 2018 NMSHP Balloon Fiesta Symposium 1 Goals and Objectives: Describe
Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients By Zahra Shaghaghi, Pharm-D, BCOP, PhC Prepared for 2018 NMSHP Balloon Fiesta Symposium 1 Goals and Objectives: Describe
Comparison of the Control of Nausea and Vomiting among Several Moderately Emetic-Risk Chemotherapy Regimens
 569 Ivyspring International Publisher Research Paper Journal of Cancer 2016; 7(5): 569-575. doi: 10.7150/jca.13637 Comparison of the Control of Nausea and Vomiting among Several Moderately Emetic-Risk
569 Ivyspring International Publisher Research Paper Journal of Cancer 2016; 7(5): 569-575. doi: 10.7150/jca.13637 Comparison of the Control of Nausea and Vomiting among Several Moderately Emetic-Risk
FINAL CDEC RECOMMENDATION
 FINAL CDEC RECOMMENDATION PALONOSETRON CAPSULE (Aloxi Eisai Limited) Indication: Chemotherapy-Induced Nausea and Vomiting Recommendation: The Canadian Drug Expert Committee (CDEC) recommends that oral
FINAL CDEC RECOMMENDATION PALONOSETRON CAPSULE (Aloxi Eisai Limited) Indication: Chemotherapy-Induced Nausea and Vomiting Recommendation: The Canadian Drug Expert Committee (CDEC) recommends that oral
Clinical Policy: Netupitant and Palonosetron (Akynzeo) Reference Number: HIM.PA.113 Effective Date: Last Review Date: 05.
 Reference Number: HIM.PA.113 Effective Date: Last Review Date: 05.") Clinical Policy: (Akynzeo) Reference Number: HIM.PA.113 Effective Date: 05.01.17 Last Review Date: 05.18 Line of Business: HIM Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Akynzeo) Reference Number: HIM.PA.113 Effective Date: 05.01.17 Last Review Date: 05.18 Line of Business: HIM Revision Log See Important Reminder at the end of this policy for important
Class Update with New Drug Evaluation: Antiemetics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
New Cardiovascular Horizons. Tucson. Multidisciplinary Strategies for Optimal Cardiovascular Care. Arizona February 7, 2015
 New Cardiovascular Horizons Tucson Multidisciplinary Strategies for Optimal Cardiovascular Care Arizona February 7, 2015 Chairmen: Miguel Montero-Baker, Salvatore J. Tirrito, Craig M. Walker, Course Directors:
New Cardiovascular Horizons Tucson Multidisciplinary Strategies for Optimal Cardiovascular Care Arizona February 7, 2015 Chairmen: Miguel Montero-Baker, Salvatore J. Tirrito, Craig M. Walker, Course Directors:
clinical practice guidelines
 clinical practice guidelines Annals of Oncology 21 (Supplement 5): v232 v243, 2010 doi:10.1093/annonc/mdq194 Guideline update for MASCC and ESMO in the prevention of chemotherapy- and radiotherapy-induced
clinical practice guidelines Annals of Oncology 21 (Supplement 5): v232 v243, 2010 doi:10.1093/annonc/mdq194 Guideline update for MASCC and ESMO in the prevention of chemotherapy- and radiotherapy-induced