TB Intensive Houston, Texas October 15-17, 2013
|
|
|
- Darlene Blake
- 6 years ago
- Views:
Transcription
1 TB Intensive Houston, Texas October 15-17, 2013 Nontuberculous Mycobacterial Lung Disease David Griffith, MD October 15, 2013 David Griffith, MD has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1
2 Nontuberculous Mycobacterial Lung Disease David Griffith, M.D Professor of Medicine University of Texas Health Center, Tyler NTM Incidence and Prevalence Why it is difficult to know the exact incidence and prevalence of NTM disease Not all NTM isolates are pathogenic, some isolates represent specimen contamination M. gordonae NTM in tap water (MAC, M kansasii, M simiae, M abscessus, M xenopi) Even pathogenic NTM are not always associated with progressive disease NOT ALL NTM ISOLATED ARE CLINICALLY SIGNIFICANT 2
3 NTM Disease Prevalence Winthrop et al NTM pulmonary disease more common than TB MAC the predominant isolate (RGM 2 nd ) The prevalence of NTM pulmonary disease rose with age and in females A positive respiratory culture for a non- M. gordonae NTM signified NTM pulmonary disease in approximately 50% of patients NTM epidemiology possible in small populations with closed laboratory systems Isolation prevalence a fair predictor Evidence for environmental transmission of NTM to humans Opportunistic pathogens enriched in showerhead biofilms Feazel et al. PNAS 2009, 106; MAC genetic sequences found in 20% of 45 showerheads from 9 cities Mycobacterium avium in a shower linked to pulmonary disease Falkinham et al. J Water and Health 2008, 6: 209. Hypersensitivity pneumonitis reaction to Mycobacterium avium in household water Marras et al. Chest 2005, 127;
4 Nontuberculous Mycobacterial infections and antitumor necrosis factor-factor therapy Winthrop et al, 2009: 15: 1556 Data from U.S. FDA Med-watch database 105 reports met NTM disease criteria 65% female, X age = 62, majority with RA All available TNF-α blockers implicated MAC most common NTM implicated 44% extrapulmonary disease, 9% died time of reporting TNF-α blockers are clearly an important predisposing factor for serious, sometimes fatal, NTM infection. Diversity of NTM Pulmonary Disease Associated with disseminated disease and immune suppression HIV Defects in IFNγ and IL-12 pathways Tumor necrosis factor α blockers Tuberculosis-like disease Disease associated with nodules/bronchiectasis Disease associated with genetic airway abnormalities and abnormal airways clearance (cystic fibrosis, primary ciliary dyskinesia) Esophageal motility disorders Hypersensitivity-like lung disease 4
5 An Official ATS/IDSA Statement: Diagnosis, Treatment and Prevention of Nontuberculous Mycobacterial Diseases American Journal of Respiratory and Critical Care Medicine 2007, 175; Diagnosis of NTM Lung Disease Minimum Evaluation Compatible Symptoms Radiographic Evaluation Chest radiograph (cavitary disease) or, HRCT of chest (nodular/bronchiectatic disease) Microbiologic Evaluation 3 or more sputum for AFB analysis Bronchoscopic evaluation Exclusion of other diagnoses (TB) 5
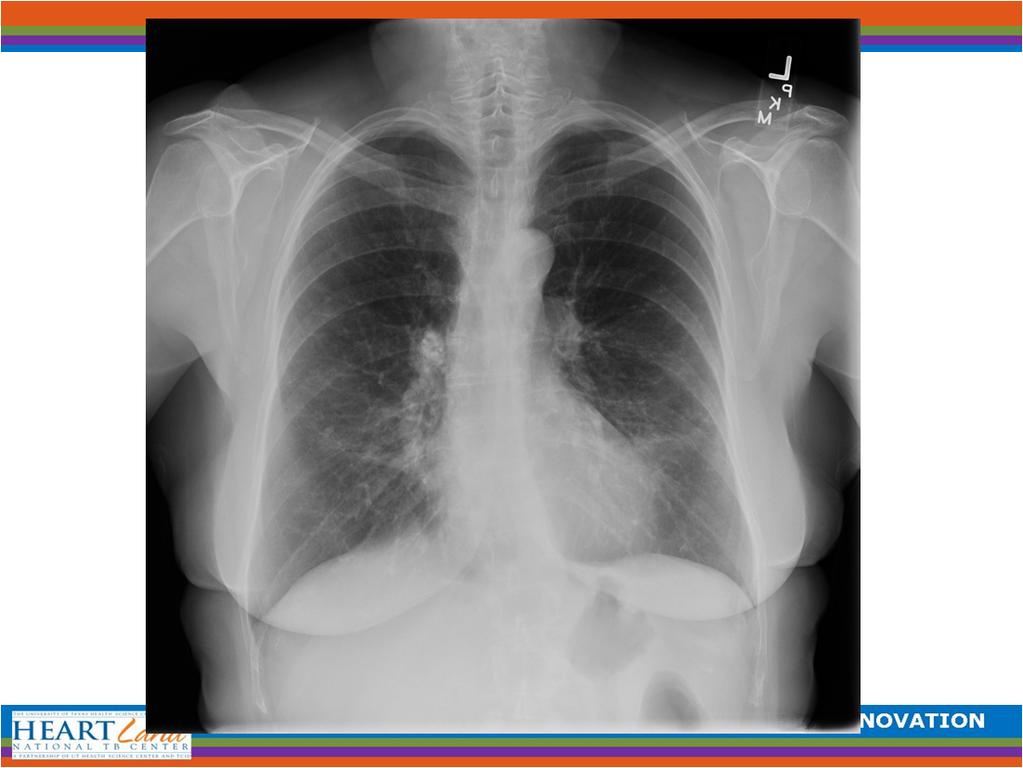
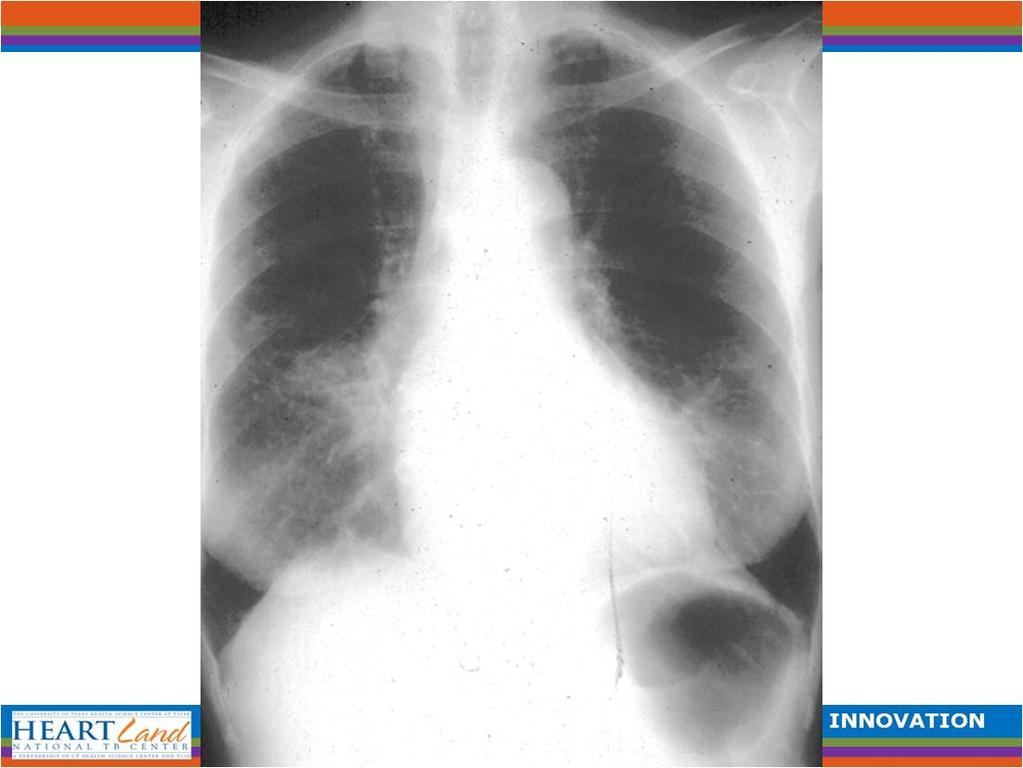
6 Is it TB or NTM Disease? NTM Disease Indolent, Milder Symptoms Thin walled cavities Contiguous spread > Pleural reaction Pleural effusion rare Frequent nodules/bronchiect asis Tuberculosis Rapidly Progressive Severe Symptoms Variable cavity shape Bronchogenic spread < Pleural reaction Pleural effusion common N/B disease unusual Is there any one radiographic finding or combination of findings that distinguishes NTM disease from TB? NO 6
7 Clinically distinguishing NTM disease from TB Scenario #1 35 yo male from Mexico History of TB in family Several months cough, sweats, weight loss (+) PPD CXR: apical cavitary consolidation 1 st sputum AFB culture (+) for MAC Clinically distinguishing NTM disease from TB Scenario #1: Pulmonary MAC disease unusual in a 35 yo male Multiple risk factors for TB Clinical presentation typical for TB Patient subsequently grew multiple (+) cultures for M. tuberculosis Empiric therapy for TB ok in this setting, may occur frequently 7

8 Clinically distinguishing NTM disease from TB Scenario #1a: 78 yo man with remote history of smoking who developed fatigue, mild weight loss and cough in 1/13 QFT +, started on 4 drugs CT scan showed nodules and bronchiectasis Sputum AFB culture + for M. abscessus Referred for treatment of M. abscessus Clinically distinguishing NTM disease from TB 8

9 Clinically distinguishing NTM disease from TB Clinically distinguishing NTM disease from TB Sputum culture + for: Klebsiella Serratia Enterobacter Mycobacterium abscessus Mycobacterium avium complex And.. 9
10 Clinically distinguishing NTM disease from TB AFB FLUOROCHROME STAIN Final NEGATIVE 7H11 CULTURE Preliminary Organism 1 M. TUBERCULOSIS CX 17 COLONIES AFB BROTH CULTURE Preliminary POSITIVE FOR AFB 09/27/13 Organism 1 M.TUBERCULOSIS COMPLEX PROBE+ MTB PROBE RESULT: PROBE POSITIVE FOR MTB CX MAC PROBE RESULT: PROBE NEGATIVE FOR MAC 10/03/ Clinically distinguishing NTM disease from TB What is the take-home from this case? I m not sure.. Don t assume anything, don t take shortcuts Stuff happens, maybe there is no other take-home message 10
11 Clinically distinguishing NTM disease from TB Scenario #2: Patient with established diagnosis of TB on antituberculosis therapy Sputum AFB culture (+) for NTM (especially MAC) during course of TB therapy Does therapy need to be altered? Nontuberulous mycobacteria isolated during the treatment of pulmonary tuberculosis Jun et al, 2009; 103: patients with tuberculosis: 68 (7.1%) had NTM isolated during TB therapy 71% had only one positive NTM culture Only two patients (3%) both with M. abscessus isolates were felt to have progressive NTM disease after completion of TB therapy Progressive NTM disease rare after completion of TB therapy but patients require follow-up after completion of TB therapy, especially with isolation of M. abscessus. 11
12 Nontuberulous mycobacteria isolated during the treatment of pulmonary tuberculosis Huang et al. Repir Med 2009, 103; TB patients in Taiwan over 6 year period 2.3% with multiple and 5% with single NTM isolates More likely to have cavitation on CXR Kendall et al. IJTLD 2010, 14; TB patients in Oregon over 1 year 14% with NTM in sputum More likely to have cavitation on CXR Damaraju et al IJTLD 2013, 17; TB patients from Canada in one year - 11% NTM co-isolation (MAC 55%, xenopi 18%) - 23% went on to have 2 NTM + cultures NO longterm followup in any study M. Abscessus recovered during treatment for Mycobacterium avium complex (MAC) lung disease Griffith et al 2013 presented at ERS, Barcelona 53/190 (28%) patients with MAC and M. abscessus Total AFB cultures obtained: 40 ± 19 32/53 (60%) with one M. abscessus isolate More likely to have > 1 water-borne NTM isolated No difference in bronchiectasis-related bacteria isolated 21/53 (40%) with > 1 M abscessus isolate Mean number + culture for M abscessus 15 ± 11 Treated for M abscessus disease 11/21 (52%) Mean duration of followup 47 ± 32 months 12
13 Clinically distinguishing NTM disease from TB Scenario #2: Therapy does not need to be altered NTM in sputum will complicate therapy especially if specimens also AFB smear (+) Complete therapy for TB then evaluate significance of NTM isolate In our experience, most patients do not have progressive NTM disease in this setting but followup required to know Clinically distinguishing NTM disease from TB Scenario #3: Patient with established NTM disease and multiple AFB culture (+) specimens for NTM While on therapy for NTM disease, AFB culture (+) specimen for M. tuberculosis Does this patient have NTM disease and TB? 13
14 14
15 Clinically distinguishing NTM disease from TB 66 yo female with longstanding MAC lung disease Unresponsive microbiologically to MAC medication Patient s son, living in household, diagnosed with tuberculosis Patient with M. tuberculosis isolate, same genotype as her son s isolate. Clinically distinguishing NTM disease from TB Scenario #3: Very rare occurrence In our experience, (+) AFB culture for M. tuberculosis usually due to specimen contamination Need genotyping of M. tuberculosis isolate to exclude specimen contamination May need to treat TB pending evaluation 15
16 Clinically distinguishing NTM disease from TB What do you do with the elderly female patient who has a clinical course and radiographic changes characteristic of nodular/bronchiectatic MAC disease and a sputum smear (+) for AFB? Start antituberculosis therapy or wait for culture results? Start antituberculosis therapy in most cases ATS Diagnostic Guidelines for NTM Lung Disease More than 160 NTM species with a spectrum of virulence for humans NTM lung disease diagnostic criteria are based on experience with common and well-described respiratory pathogens such as Mycobacterium avium complex, M. kansasii and M. abscessus It is extremely unlikely that a single set of diagnostic criteria would be useful or accurate for all NTM species in all clinical circumstances. 16
17 Diagnosis of NTM Lung Disease: Microbiologic Criteria sputum results: 2 positive cultures regardless of AFB smear results Single available bronchial wash or lavage: One positive culture regardless of smear results Tissue biopsy: Compatible histopathology and (+) culture Compatible histopathology and (+) sputum or bronchial wash culture ATS DIAGNOSTIC GUIDELINES FOR NTM LUNG DISEASE Under diagnosis Untreated disease Over diagnosis Drug toxicity Usually enough time for a careful assessment of patients with bronchiectasis and possible NTM disease 17
18 Diagnosis of NTM Lung Disease: Microbiologic Criteria A single positive culture from any source (sputum or bronchoscopy) is is regarded as indeterminate for diagnosis of NTM lung disease: Frequent contaminants, M. gordonae, M. terrae complex, M. mucogenicum NTM species known to be present in tap water, M. simiae, M. lentiflavum, M. abscessus, M. kansasii, M. xenopi Diagnostic Criteria for NTM Lung Disease PATIENTS WHO ARE SUSPECTED OF HAVING NTM LUNG DISEASE BUT DO NOT MEET THE DIAGNOSTIC CRITERIA SHOULD BE FOLLOWED UNTIL THE DIAGNOSIS IS FIRMLY ESTABLISHED OR EXCLUDED. 18
19 NTM Diagnostic Guidelines Current diagnostic guidelines are inadequate, but will continue to evolve Diagnostic evaluation influenced by: The virulence of the isolated NTM: M. kansasii, M. gordonae The host (immune suppression, airway abnormalities, body morphotype): MAC, M. mucogenicum, M. abscessus The clinical source (setting) of the organism: blood, soft tissue, sputum It is imperative that clinicians evaluating patients with NTM lung disease are familiar with characteristics of individual NTM species. Factors Influencing the Decision to Treat NTM Lung Disease MAKING THE DIAGNOSIS OF NTM LUNG DISEASE DOES NOT, PER SE, NECESSITATE THE INSTITUTION OF THERAPY. The decision to initiate treatment for patients with NTM lung disease is ultimately a decision based on risk/benefit analysis taking into account patient symptoms, radiographic findings (progression) and microbiologic results vs. the adverse effects of multiple potentially toxic and relatively weak drugs. 19
20 Mycobacterium avium complex (MAC) Lung Disease AKA Mycobacterium aviumintracellulare (MAI) disease State of the Art: Nontuberculous Mycobacteria and Associated Diseases (Wolinsky, ARRD 1979;119: 107) Chronic pulmonary disease resembling TB represents the most important clinical problem associated with NTM The average case of M kansasii or MAI disease would be a 48-year-old man with long-standing lung disease with a 3-month history of increasingly productive cough, night sweats, a low-grade fever, and moderate weight loss. The chest roentgenogram shows fibrosis and a thin-walled cavity in the right upper lobe. 20
21 M. avium Complex (MAC) Lung Disease Clinical presentations: Fibronodular cavitary or "tuberculosis" type <50% cases Heavy smoker, male predominance, alcoholism, onset <60 years age Diagnosed initially as TB suspects 21
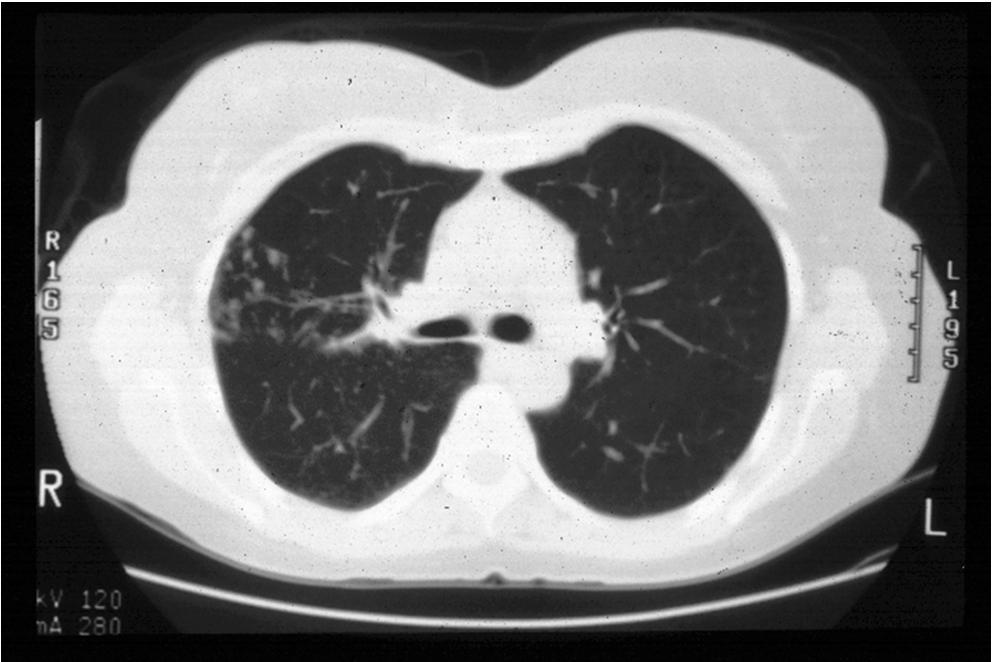
22 MAC Lung Disease with Nodules and Bronchiectasis: Clinical Features > 50% / cases 80% of patients are women 95% of patients are Caucasian 60% are lifelong non-smokers, no alcohol mean age is 70 years most have no serious underlying disease Nodular/Bronchiectasis MAC Lung Disease: Radiographic Features Predominantly involve RML and lingula Cavities are unusual (typically in mid lung) On CT or HRCT have: a) Cylindrical bronchiectasis and/or b) Small nodules <5mm usually in the same lung segments c) Rarely neither Radiographic progression is usually slow (years) 22

23 23
24 24

25 Nontuberculous Mycobacterial Diseases: Pulmonary Disease Usual clinical presentation: chronic cough ( recurrent pneumonia ), debilitating fatigue, weight loss, fever, hemoptysis Variable disease progression: frequent bronchiectasis- related symptoms Prevalence:?1/3-500 women over age 65? Most common cause of cough and abnormal chest radiograph in this population 25
26 Pathogenesis of NTM Lung Disease Kim et al. AJRCCM 2008, 178; 1066 Characteristic morphotype (body habitus) in 63 patients with NTM lung disease evaluated at the NIH: BMI significantly lower and height significantly greater than matched controls High rates of scoliosis (51%), pectus excavatum (11%) and mitral valve prolapse (9%), CFTR mutations (36%) No recognized immune defects (cell mediated dysfunction or cytokine pathway abnormalities) Pathophysiologic consequences of this constellation of findings currently unknown. Does not explain disease in majority of patients Pathogenesis of NTM Lung Disease Bronchiectasis and pulmonary NTM infection inextricably linked 20% of cystic fibrosis patients and 15% of primary ciliary dyskinesia patients have NTM recovered from respiratory specimens difficult to determine clinical significance, effect on prognosis, MAC vs M. abscessus Strongly suggests, at least for some patients, a predisposing alteration in airway surface defenses 26


27 27
28 Therapy of MAC Lung Disease New ATS NTM Guidelines Cavitary disease: macrolide/emb/rifamycin ± injectable: DAILY Nodular/bronchiectatic disease: macrolide/emb/rifamycin: INTERMITTENT* Severe or previously treated disease: macrolide/emb/rifamycin/injectable: DAILY Duration: 12 months sputum culture negativity while on therapy *Not indicated for severe and/or cavitary disease Treatment of NTM Lung Disease Controversies in the treatment of patients with NTM lung disease Role of in vitro susceptibility testing Consequences of ineffective therapy: Diminishing treatment response with successive treatment efforts Disease Relapse vs Reinfection Increasing numbers of patients receiving therapy for NTM (MAC) lung disease magnify these controversies 28
29 In Vitro Susceptibility Testing M. tuberculosis The ideal for mycobacterial response to therapy INH and Rifampin Highly active bacteriocidal drugs Achievable blood levels X MIC s of susceptible organisms Penetrate all tissues Clear association between MIC and resistance EMB and PZA: not all TB drugs are created equal 29
30 PULMONARY DISEASE CAUSED BY MAC IN HIV- NEGATIVE PATIENTS: FIVE-YEAR FOLLOW-UP OF PATIENTS RECEIVING STANDARDISED TREATMENT (BTS Int J Tuberc Lung Dis 2002; 6: 628) 75 patients with MAC lung disease 40 (53%) M, 46 (61%) cavitation 37 RE vs 38 REH for 24 mos PULMONARY DISEASE CAUSED BY MAC IN HIV- NEGATIVE PATIENTS: FIVE-YEAR FOLLOW-UP OF PATIENTS RECEIVING STANDARDISED TREATMENT (BTS Int J Tuberc Lung Dis 2002; 6: 628) 23 (31%) patients alive and cured 21 (28%) treatment failures/relapses MAC Susceptibility: 14%R, 32%E, 0%H No correlation between in vitro resistance and treatment failure/relapse 30
31 MAC and In Vitro Susceptibility Testing (Kobashi et al. J Infect Chemother 2006, 12; 195) 52 patients with pulmonary MAC treated with Rmp, Emb, Clari, and Stm No relationship between clinical response and MICs for Rmp, Emb and Stm (similar findings BTS study IJTLD 2002, 6; 628) Clinical efficacy did correlate with clari MICs pulmonary and dissmeminated disease (AJRCCM 1994; 149:1335, CID 1996; 23:983, Ann Int Med, 1994, 121; 905, CID 1999; 28: 1080, Respir Med 2007, 101; 130) Macrolides for MAC Disease: Summary Treatment success correlates with in vitro MIC (susceptible < 8 μg/ml, intermediate 16 μg/ml, resistant > 32 μg/ml Disease progression/relapse associated with MIC > 32 μg/ml There are no drugs, other than the macrolides for which there is a correlation between in vitro susceptibility (MIC) and in vivo response for disseminated or pulmonary MAC disease. 31
32 Macrolides for MAC Disease: Summary The designation of susceptible must be used with caution for all drugs other than macrolides in MAC disease. In vitro susceptibility tests for most drugs do not predict who will respond and who will fail therapy. MAC In Vitro Susceptibility Testing: 2007 NTM Guidelines Clarithromycin susceptibility testing only is recommended for new MAC isolates Clarithromycin is the class agent for macrolide susceptibility testing No other drugs are recommended for susceptibility testing of new MAC isolates Clarithormycin susceptibility should be performed for MAC isolates from patients who fail macrolide therapy 32
33 Nontuberculous mycobacteria for which there is not an established correlation between in vitro susceptibility and in vivo response M. malmoense M. scrofulaceum M. simiae M. xenopi M. abscessus M. immunogenum Etc. NTM for which there is an established correlation between in vitro susceptibility and in vivo response M. kansasii M. marinum M. szulgai M. fortuitum (except macrolides) 33
34 Consequences of Macrolide Resistance Possible Risk Factors for the Development of Macrolide Resistance (Griffith et al 2006 Am J Resp Crit Care Med) Macrolide Monotherapy: 28/51 (55%) Macrolide plus quinolone: 11/51 (22%) Combined, regimens without ethambutol: 39/51 (76%) Other risk factors: 12/51 (23%) No difference in macrolide resistance based on macrolide (azi or clari) or dosing interval (daily or intermittent) 34
35 Macrolide Resistant MAC Lung Disease: Response to Therapy Sputum conversion after macrolide resistance:11/14 (77%) p= in patients who had both injectable therapy and surgery. Sputum conversion after macrolide resistance 2/37 (5%) in patients without both injectable therapy and surgery. No difference in response between cavitary and nodular disease Macrolide Resistant MAC Lung Disease: Response to Therapy Of the patients who failed therapy, the one year mortality was 13/38 (34%), two year mortality was 17/38 (45%) Of the patients whose sputum converted to negative, the one and two year mortality was 0/13, (0%) 35
36 MAC Reinfection Significance of Multiple (+) Sputum Cultures After Months (-) Cultures on Rx: 1. Occurs in the setting of nodular bronchiectasis 2. May be seen at any time during therapy or after stopping therapy 3. Approximately 90% will be new infections, and often involve multiple strains 4. Reinfection isolates usually macrolide susceptible 5. True clinical/microbiologic relapses are unusual 36
37 State of the Art: Nontuberculous Mycobacteria and Associated Diseases (Wolinsky, ARRD 1979;119: 107) Proper management requires greater expertise than is needed for treatment of TB, first, to decide who needs to be treated, and second, to determine which drug regimens to use. MAC: Hypersensitivity-Like Lung Disease Clinically, radiographically, histologically resembles hypersensitivity lung disease (subacute onset) Associated with standing water sources ( hot tub lung ) Infectious, inflammatory,?both Identical MAC genotypes recovered from water source, patient Inconsistent attention to manufacturers recommended specifications for hot tub maintenance procedures 37

38 MAC: Hypersensitivity-Like Lung Disease ( Hot tub lung ) (Hanak et al Respir Med 2006, 100; 610) Prognosis generally excellent: most patients recover spontaneously Most benefit gained by removing patient from antigen exposure Steroids may hasten symptomatic/physiologic recovery MAC antimicrobials of unclear benefit 38
39 M. kansasii Clinical presentation, in vitro susceptibilities and response to medications similar to M. tuberculosis Rifampin, INH, Ethambutol effective Multiple medications with activity against M. kansasii: clari, azi, moxi, sulfa, strep, etc. Expect treatment for cure Intrinsic Macrolide Resistance in Rapidly Growing Mycobacteria The primary mechanism of acquired clinically significant macrolide resistance for some mycobacteria (especially RGM) is the presence of an erm gene All isolates of M. abscessus, M. fortuitum (and several other RGM, but not M. chelonae) contain an inducible erm gene. Novel erm gene in M. tuberculosis. 39
40 Intrinsic Macrolide Resistance in Rapidly Growing Mycobacteria Bottom line for M. abscessus and M. fortuitum Macrolides should not be used as monotherapy No empiric macrolide therapy for M. fortuitum cryptic resistance difficult (impossible) to detect in the laboratory macrolides should be used with caution with MIC >4mcg/L (for M. fortuitum) Kevin Nash USC, Richard Wallace and Barbara Elliott UTHSCT (JAC 2005, 55; 170 and AAC 2006, 50; 3476, AAC 2009, 53; 1367) Mycobacterium abscessus LUNG DISEASE 1. Female, non-smokers, 60 years or older 2. Mid and lower lung field nodules/bronchiectasis 3. Lung disease resembles, non-cavitary Mycobacterium avium complex (MAC) lung disease 4. No consistently identified immune defect (unusual pathogen in AIDS) 40
41 Treatment of M. abscessus Lung Disease Macrolide: value uncertain, no other oral agents of proven value Amikacin mg/kg 3-5X/week Cefoxitin 8-12g/day in divided doses Imipenem 500 mg 2-4X/day Tigecycline mg/day There is no predictably or reliably effective medical treatment strategy for M. abscessus lung disease Healthcare Associated NTM Disease NTM transmission in the healthcare setting most frequently linked to exposure to tap (municipal) water (MAC, M. kansasii, M. simiae, M. xenopi, M. fortuitum, M. abscessus) Even with potent disinfectants, NTM organisms can persist on equipment or devices. 41


42 42
43 Healthcare Associated NTM Disease Infections and Pseudoinfections: median sternotomy, liposuction, LASIK, catheters (IV and peritoneal), prosthetic heart valves, prosthetic joints, ocular lenses, pedicures, etc. Complete avoidance of tap water for specimen collection, instrument cleaning and wound cleaning is absolutely necessary! 43
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 Nontuberculosis Mycobacterial Lung Disease David Griffith, MD August 8, 2012 David Griffith, MD has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 Nontuberculosis Mycobacterial Lung Disease David Griffith, MD August 8, 2012 David Griffith, MD has the following disclosures to make: No conflict of interests
Nontuberculous Mycobacteria
 Nontuberculous Mycobacteria Epidemiology and Clinical Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health &
Nontuberculous Mycobacteria Epidemiology and Clinical Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health &
How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients?
 Lung Disease Patients?") How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients? David E. Griffith, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Potential COI Statement I was a
How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients? David E. Griffith, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Potential COI Statement I was a
Nontuberculous Mycobacterial Lung Disease
 Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
2018 Vindico Medical Education. Non-tuberculous Mycobacteria: Circumventing Difficulties in Diagnosis and Treatment
 Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
NTM AND BRONCHIECTASIS (BXSIS): THE CHICKEN AND THE EGG
: THE CHICKEN AND THE EGG") REMINGTON WINTER COURSE IN ID VAIL, CO FEBRUARY, 2010 NONTUBERCULOSIS MYCOBACTERIA AND BRONCHIECTASIS: Revised 1/28/10 10:31 AM- CQ MICHAEL D. ISEMAN, MD OR In some cases NTMs invade pre-existing BXSIS
REMINGTON WINTER COURSE IN ID VAIL, CO FEBRUARY, 2010 NONTUBERCULOSIS MYCOBACTERIA AND BRONCHIECTASIS: Revised 1/28/10 10:31 AM- CQ MICHAEL D. ISEMAN, MD OR In some cases NTMs invade pre-existing BXSIS
Nontuberculous Mycobacteria (NTM)
") Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Slowly Growing Nontuberculous Mycobacterial Infections
 Slowly Growing Nontuberculous Mycobacterial Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Advisory Board Horizon, Johnson and Johnson, Otsuka and Spero
Slowly Growing Nontuberculous Mycobacterial Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Advisory Board Horizon, Johnson and Johnson, Otsuka and Spero
NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW.
 INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW.") NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW. K. Clay 1, K. Bhatt 1, D. Burns 1, J. Evans 2, S. Gardiner 2, EG. Smith 2, P. Hawkey 2,
NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW. K. Clay 1, K. Bhatt 1, D. Burns 1, J. Evans 2, S. Gardiner 2, EG. Smith 2, P. Hawkey 2,
Shannon Kasperbauer, M.D. National Jewish Health University of Colorado Health Sciences Center. Property of Presenter. Not for Reproduction
 Shannon Kasperbauer, M.D. National Jewish Health University of Colorado Health Sciences Center Consultant: Johnson and Johnson Speaker/consultant: Insmed Examine characteristics of the RGM Define the main
Shannon Kasperbauer, M.D. National Jewish Health University of Colorado Health Sciences Center Consultant: Johnson and Johnson Speaker/consultant: Insmed Examine characteristics of the RGM Define the main
Diagnostic Evaluation of NTM and Bronchiectasis
 Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Nontuberculous Mycobacteria: Ubiquitous Environmental Pathogens for Predisposed Hosts
 Nontuberculous Mycobacteria: Ubiquitous Environmental Pathogens for Predisposed Hosts History, Epidemiology, Spectrum of Disease Diagnosis, Treatment and Predictors of Treatment Outcome James L. Cook,
Nontuberculous Mycobacteria: Ubiquitous Environmental Pathogens for Predisposed Hosts History, Epidemiology, Spectrum of Disease Diagnosis, Treatment and Predictors of Treatment Outcome James L. Cook,
Nontuberculous Mycobacteria (NTM) in Patients with Cystic Fibrosis
 in Patients with Cystic Fibrosis") Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Mycobacteriosisok. Somoskövi Ákos
 Mycobacteriosisok Somoskövi Ákos Phylogenetic position of the MTBC and NTM within the genus Mycobacteria Gutierrez and Somoskovi 2014 Encyclopedia of Human Biology Increased identification of NTMs Plethora
Mycobacteriosisok Somoskövi Ákos Phylogenetic position of the MTBC and NTM within the genus Mycobacteria Gutierrez and Somoskovi 2014 Encyclopedia of Human Biology Increased identification of NTMs Plethora
Pulmonary Non Tuberculous Mycobacteria Infections
 Non Tuberculous Mycobacteria Pulmonary Non Tuberculous Mycobacteria Infections Jorge Murillo, MD, FIDSA, FACP Associate Professor at FIU Herbert Wertheim College of Medicine Infectious Disease Consultant
Non Tuberculous Mycobacteria Pulmonary Non Tuberculous Mycobacteria Infections Jorge Murillo, MD, FIDSA, FACP Associate Professor at FIU Herbert Wertheim College of Medicine Infectious Disease Consultant
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Mycobacterial Infections in HIV. H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine
 Mycobacterial Infections in HIV H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine Learning Objectives List the most common mycobacterial infections
Mycobacterial Infections in HIV H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine Learning Objectives List the most common mycobacterial infections
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review
 Showa Univ J Med Sci 28 4, 373 377, December 2016 Case Report Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review Makoto HAYASHI 1, Satoshi MATSUKURA 1,
Showa Univ J Med Sci 28 4, 373 377, December 2016 Case Report Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review Makoto HAYASHI 1, Satoshi MATSUKURA 1,
AFB Identification Texas Approach
 AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
Canadian Tuberculosis Standards
 Canadian Tuberculosis Standards 7 th Edition Chapter 11: Nontuberculous Mycobacteria To promote and protect the health of Canadians through leadership, partnership, innovation and action in public health.
Canadian Tuberculosis Standards 7 th Edition Chapter 11: Nontuberculous Mycobacteria To promote and protect the health of Canadians through leadership, partnership, innovation and action in public health.
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Bronchiectasis and Nontuberculous Mycobacterial Disease
 Bronchiectasis and Nontuberculous Mycobacterial Disease David E. Griffith, MD a, *, Timothy R. Aksamit, MD b KEYWORDS Nontuberculous mycobacteria Bronchiectasis Mycobacterium avium complex Mycobacterium
Bronchiectasis and Nontuberculous Mycobacterial Disease David E. Griffith, MD a, *, Timothy R. Aksamit, MD b KEYWORDS Nontuberculous mycobacteria Bronchiectasis Mycobacterium avium complex Mycobacterium
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Infection With the Mycobacterium avium Complex in Patients Without Predisposing Conditons A Case Report and Literature Review
 BJID 2005; 9 (April) 173 Infection With the Mycobacterium avium Complex in Patients Without Predisposing Conditons A Case Report and Literature Review Andrea Barral Martins 1, Eliana Dias Matos 2,3 and
BJID 2005; 9 (April) 173 Infection With the Mycobacterium avium Complex in Patients Without Predisposing Conditons A Case Report and Literature Review Andrea Barral Martins 1, Eliana Dias Matos 2,3 and
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI Page 1 Page 2 nontuberculous mycobacteria ntm nontuberculous mycobacteria ntm pdf nontuberculous mycobacteria ntm patients and those
DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI Page 1 Page 2 nontuberculous mycobacteria ntm nontuberculous mycobacteria ntm pdf nontuberculous mycobacteria ntm patients and those
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
NTM Lecture Series. Challenging Cases: Part 1. Property of Presenter
 NTM Lecture Series Challenging Cases: Part 1 Dr. Wendi Kay Drummond DO, MPH Assistant Professor of Medicine Division of Mycobacterial and Infectious Diseases Department of Medicine September 27, 2018 Disclosures
NTM Lecture Series Challenging Cases: Part 1 Dr. Wendi Kay Drummond DO, MPH Assistant Professor of Medicine Division of Mycobacterial and Infectious Diseases Department of Medicine September 27, 2018 Disclosures
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
The Epidemiology of NTM
 The Epidemiology of NTM Jennifer Adjemian, PhD Deputy Chief, Epidemiology Unit Commander, US Public Health Service National Institute of Allergy and Infectious Diseases National Institutes of Health Presentation
The Epidemiology of NTM Jennifer Adjemian, PhD Deputy Chief, Epidemiology Unit Commander, US Public Health Service National Institute of Allergy and Infectious Diseases National Institutes of Health Presentation
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
When Can Isolation Be Discontinued?
 When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
Transmission and Pathogenesis of Tuberculosis
 Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Associate Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Associate Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Profile of Tuberculosis Infection among Current HIV+ Patients at the Philippine General Hospital
 Profile of Tuberculosis Infection among Current HIV+ Patients at the Albert B. Albay Jr., MD Jemylyn Garcia, MD Joel Santiaguel, MD UP- TB in the Philippines 6 th leading cause of morbidity and mortality
Profile of Tuberculosis Infection among Current HIV+ Patients at the Albert B. Albay Jr., MD Jemylyn Garcia, MD Joel Santiaguel, MD UP- TB in the Philippines 6 th leading cause of morbidity and mortality
How To Assess Severity and Prognosis
 How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Transmission and Pathogenesis of Tuberculosis. Transmission and Pathogenesis of Tuberculosis. Mycobacteria. Introduction to the pathogen Transmission
 Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Assistant Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Assistant Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Nontuberculous Mycobacteria
 Nontuberculous Mycobacteria When antibiotics are not enough a surgical approach John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief Section of General Thoracic Surgery University
Nontuberculous Mycobacteria When antibiotics are not enough a surgical approach John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief Section of General Thoracic Surgery University
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Implication of species change of Nontuberculous Mycobacteria during or after treatment
 Lee et al. BMC Pulmonary Medicine (2017) 17:213 DOI 10.1186/s12890-017-0539-7 RESEARCH ARTICLE Open Access Implication of species change of Nontuberculous Mycobacteria during or after Jong Sik Lee 1, Jong
Lee et al. BMC Pulmonary Medicine (2017) 17:213 DOI 10.1186/s12890-017-0539-7 RESEARCH ARTICLE Open Access Implication of species change of Nontuberculous Mycobacteria during or after Jong Sik Lee 1, Jong
Nontuberculous mycobacteria isolated during the treatment of pulmonary tuberculosis
 Respiratory Medicine (2009) 103, 1936e1940 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed Nontuberculous mycobacteria isolated during the treatment of pulmonary tuberculosis
Respiratory Medicine (2009) 103, 1936e1940 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed Nontuberculous mycobacteria isolated during the treatment of pulmonary tuberculosis
Appendix C. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Geographical distribution and clinical relevance of nontuberculous mycobacteria in Croatia
 Geographical distribution and clinical relevance of nontuberculous mycobacteria in Croatia M. Jankovic 1, M. Samarzija 1, I. Sabol 2, M. Jakopovic 1, V. Katalinic Jankovic 3, LJ. Zmak 3, B. Ticac 4, A.
Geographical distribution and clinical relevance of nontuberculous mycobacteria in Croatia M. Jankovic 1, M. Samarzija 1, I. Sabol 2, M. Jakopovic 1, V. Katalinic Jankovic 3, LJ. Zmak 3, B. Ticac 4, A.
Standardized Case Definition for Extrapulmonary Nontuberculous Mycobacteria Infections
 Operational Guidance for Position Statement 17 ID 07: Standardized Case Definition for Extrapulmonary Nontuberculous Mycobacteria Infections Submission Date: April 28, 2017 Committee: Infectious Disease
Operational Guidance for Position Statement 17 ID 07: Standardized Case Definition for Extrapulmonary Nontuberculous Mycobacteria Infections Submission Date: April 28, 2017 Committee: Infectious Disease
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Novel Therapies for NTM
 NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
Peritoneal dialysis associated peritonitis secondary to Mycobacterium fortuitum
 Case Reports Peritoneal dialysis associated peritonitis secondary to Mycobacterium fortuitum Paula McKenzie MD, David Sotello MD, Kunal Parekh MD, Kristen Fuhrmann PharmD, Richard Winn MD Abstract We report
Case Reports Peritoneal dialysis associated peritonitis secondary to Mycobacterium fortuitum Paula McKenzie MD, David Sotello MD, Kunal Parekh MD, Kristen Fuhrmann PharmD, Richard Winn MD Abstract We report
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Nontuberculous mycobacterial infections
 Chapter 8 Nontuberculous mycobacterial infections C.L. Daley Summary Nontuberculous mycobacteria (NTM) represent a large group of bacteria that have been isolated from environmental sources. When NTM are
Chapter 8 Nontuberculous mycobacterial infections C.L. Daley Summary Nontuberculous mycobacteria (NTM) represent a large group of bacteria that have been isolated from environmental sources. When NTM are
Serodiagnosis of Mycobacterium avium complex pulmonary disease in the USA
 ORIGINAL ARTICLE PULMONARY INFECTIONS Serodiagnosis of Mycobacterium avium complex pulmonary disease in the USA Seigo Kitada 1, Adrah Levin 2, Melissa Hiserote 3, Ron J. Harbeck 3, Chris A. Czaja 2,4,
ORIGINAL ARTICLE PULMONARY INFECTIONS Serodiagnosis of Mycobacterium avium complex pulmonary disease in the USA Seigo Kitada 1, Adrah Levin 2, Melissa Hiserote 3, Ron J. Harbeck 3, Chris A. Czaja 2,4,
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Nontuberculous Mycobacteria and Heater-Cooler Devices: A CDC Update
 National Center for Emerging and Zoonotic Infectious Diseases Nontuberculous Mycobacteria and Heater-Cooler Devices: A CDC Update Kiran Perkins, MD, MPH Medical Officer Division of Healthcare Quality Promotion
National Center for Emerging and Zoonotic Infectious Diseases Nontuberculous Mycobacteria and Heater-Cooler Devices: A CDC Update Kiran Perkins, MD, MPH Medical Officer Division of Healthcare Quality Promotion
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Mycobacterium fortuitum,
 2009 177 Mycobacterium fortuitum 1 1) 2) 3) 1) 1) 4) 4) 5) 2) 1) 1) 2) 3) 4) 5) 21 3 16 21 7 1 Mycobacterium fortuitum 1 39 BHI 2 Ziehl Neelsen M. fortuitum MIC CPFX 0.2 mg/ml, MINO 0.78 mg/ml, CAM 100
2009 177 Mycobacterium fortuitum 1 1) 2) 3) 1) 1) 4) 4) 5) 2) 1) 1) 2) 3) 4) 5) 21 3 16 21 7 1 Mycobacterium fortuitum 1 39 BHI 2 Ziehl Neelsen M. fortuitum MIC CPFX 0.2 mg/ml, MINO 0.78 mg/ml, CAM 100
WELCOME. Lab Talk: What a Nurse Hears. April 18, NTNC Annual Meeting Lab Talk: What a Nurse Hears
 Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Nontuberculous mycobacteria isolated from pulmonary specimens between 2004 and 2009: causative agent or not?
 NEW MICROBIOLOGICA, 33, 399-403, 2010 Nontuberculous mycobacteria isolated from pulmonary specimens between 2004 and 2009: causative agent or not? Can Bicmen 1, Meral Coskun 1, Ayriz T. Gunduz 1, Gunes
NEW MICROBIOLOGICA, 33, 399-403, 2010 Nontuberculous mycobacteria isolated from pulmonary specimens between 2004 and 2009: causative agent or not? Can Bicmen 1, Meral Coskun 1, Ayriz T. Gunduz 1, Gunes
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
Cardiovascular Center Grand Rounds. December 15, 2016
 Cardiovascular Center Grand Rounds December 15, 2016 Agenda Overview of Heater-Cooler Device Issue NTM Infection Incidence Chronology of Events and Communications Risk Management Implications Q&A NTM Grand
Cardiovascular Center Grand Rounds December 15, 2016 Agenda Overview of Heater-Cooler Device Issue NTM Infection Incidence Chronology of Events and Communications Risk Management Implications Q&A NTM Grand
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2