NTM Lecture Series. Challenging Cases: Part 1. Property of Presenter
|
|
|
- Buddy Summers
- 5 years ago
- Views:
Transcription
1 NTM Lecture Series Challenging Cases: Part 1 Dr. Wendi Kay Drummond DO, MPH Assistant Professor of Medicine Division of Mycobacterial and Infectious Diseases Department of Medicine September 27, 2018
2 Disclosures No relevant financial disclosures to report.
3 Objectives Discuss the presentation and clinical evaluation of a complicated case in an immune compromised host Review some common drug reactions associated with antibiotics used to treat NTM infections and management of these drug reactions Discuss indications for surgical intervention in complex pulmonary mycobacterial infection
4 Case 1: Outpatient clinic evaluation Mr. E. is a 53 year old Vietnamese male who presented to the NJH outpatient ID clinic for evaluation in June He first presented for care in the October 2013 with new onset dry cough, shortness of breath, weakness, fever and a 30 lb weight loss. He was subsequently hospitalized. No significant PMH or pertinent exposures other than sauna use at the gym
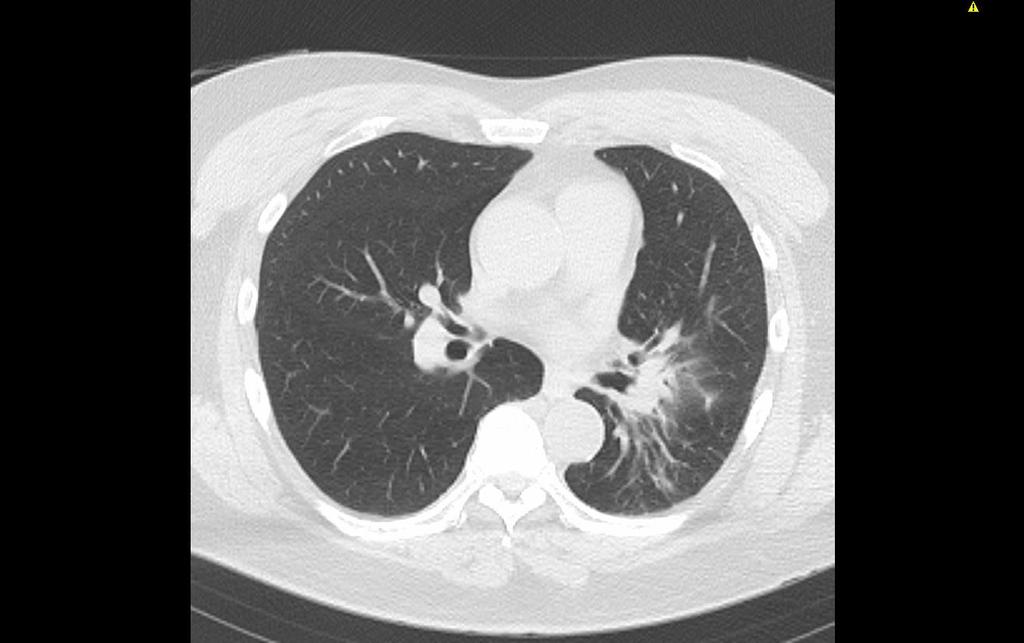
5 Case 1 CTA Chest 10/29/13: Round mass versus infiltrate in the inferior left hilum, superior segment left lower lobe (5.3x5.1cm) Mediastinal lymphadenopathy, left tracheobronchial angle Addendum: Left supraclavicular lymphadenopathy. The appearance is suspicious for advanced bronchogenic carcinoma.

6 CT Chest 11/4/13 (status post bronchoscopy 11/1/13)
7 Pathology, Lymph Node Biopsy: Nonnecrotizing granulomas, negative stains Left supraclavicular lymph node biopsy 11/1/13: Special stains negative for any organisms. Pathology notable for Non-necrotizing granulomas. Bronchoscopy with BAL 11/1/13: Brushing with rare mildly atypical cells favoring reactive change. AFB and GMS stains negative for pathogens. Left upper lung bronchus biopsy: No evidence of maligancy. Bronchial wall with severe mixed inflammation and scattered multinucleated giant cells. Histology most concerning for infectious process.
8 Pathology: Lung Biopsy, granulomatous inflammation, stains negative CT-guided needle lung biopsy 11/6/13: Left lung parenchyma with multinucleated giant cells, moderately chronic inflammation and scarring. Comment: The granulomatous inflammation and chronic inflammation is most concerning for an infectious process. All AFB and GMS stains are negative for organisms. The histology would be somewhat atypical for sarcoid.
9 Clinical Course: Started on treatment for sarcoidosis with steroids Mr. E was treated for community acquired versus post-obstructive pneumonia Based on the results of the biopsy, he was treated for sarcoidosis and was started on prednisone 60 mg daily with a taper 11/13/13-12/9/14 with some improvement in his pulmonary symptoms. Off of steroids, developed night sweats, abdominal pain and bilateral hip pain Admitted to a local hospital on 1/30/14 with worsening productive cough, progressive shortness of breath, fevers (Tmax 39) Hospitalized from 1/30/14-7/24/14
10 Clinical Course The bronchoscopy specimen (BAL) from 11/1/13 subsequently grew Mycobacterium avium intracellulare (reported 11/11/13) The left lung biopsy from 11/6/13 was smear negative, culture positive for Mycobacterium avium intracellulare (reported 11/18/13) He developed bone pain in his upper and lower extremities with abnormal imaging suggestive of osteomyelitis and persistent fevers.
11 DIAGNOSIS: Disseminated MAC Bone marrow biopsies notable for granulomas Positive cultures for MAC from multiple sites (blood, bone, lung, bone marrow) Bony involvement including lesions in his skull, thoracic spine, ribs, bilateral femurs, bilateral humerii, requiring IM rods (left humerus, bilateral femurs)
12 Therapeutics Once MAC was diagnosed, he was started on therapy with azithromycin, rifampin, ethambutol M/W/F, transitioned to daily therapy one month later Amikacin (IV) added 1 month later He was discharged on oral azithromycin, rifampin, ethambutol, and ciprofloxacin
13 Past Medical History Disseminated Mycobacterium avium complex disease History of L pulmonary mass CKD (Cr 1.5) (amikacin associated nephrotoxicity) Hearing loss (amikacin associated ototoxicity) Aspiration GERD Osteomyelitis of the long bones (bilateral femurs, humerii), ribs, spine, skull involvement Pancreatitis Globus pallidus infarct Left ulnar mononeuropathy Cognitive delay
14 Immmunology Evaluation IFNγR1 expression: 8.0 (>2.1): indicating normal receptor expression IL-12RB1: expression is PRESENT (normal) Th1/Th17 assay: IFNg and IL17 CD4 Cells by Flow. Showed appropriate IFN-gamma production by CD4 T cells. IFN gamma auto-antibody: PRESENT
15
16 Disseminated NTM Infections Occurs most in immunocompromised hosts Uncommon in persons not infected with the human immunodeficiency virus (HIV) Tumor necrosis factoralpha antagonists (TNFa) Organ transplant recipients Untreated AIDS Mendelian Susceptibility to Mycobacterial Diseases (MSMD) MAC is the most common cause of disseminated NTM The respiratory and GI tracts are the usual portal of entry for dissemination Bacteremia
17 Clinical Features of Disseminated NTM Infections Fever, weight loss, sweating, diarrhea, generalized lymphadenopathy, generalized cutaneous lesions, diffuse abdominal tenderness, hepatosplenomegaly Signs and symptoms typically reflect major sites of infection: bone marrow, lungs, GI tract, skin lesions, multifocal osteomyelitis Disease severity and age of onset depends on the part of the pathway affected In our patient, disseminated disease including pulmonary involvement, lymph node involvement, with multifocal osteomyelitis Anti-IFN-gamma autoantibodies in Disseminated Nontuberculous Mycobacterial Infections. J Immunol 2005; 175: They described the clinical features of 6 patients with IFN gamma autoantibodies and DMAC 4/6 with cutaneous disease 4/6 with involvement of the cervical LN 4/6 with pulmonary involvement 3/6 with bony involvement 1/6 with appendix, retropharyngeal, parapharyngeal, prevertebral
18 Clinical Evaluation Biopsy of tissue of clinical concern (lymph node, lung biopsy, skin biospy/i&d, bone marrow biopsy) AFB blood cultures (more than 90% of patients with disseminated MAC have positive blood cultures) Imaging Laboratory evaluation CBC with dif, CMP, CRP, ESR HIV antibody test, Lymphocyte subsets Sputum evaluation (minimum of 3)
19 Mendelian Susceptibility to Mycobacterial Disease Rare syndrome Mutations in 7 different genes identified Predisposition to disseminated infections by weakly virulent mycobacteria Nontuberculous mycobacteria (NTM) Bacillus Calmette-Guerin (BCG) vaccine Disseminated Mycobacterium bovis More virulent M. tuberculosis Salmonella (50% patients) Intracellular pathogens Nocardia, Listeria, Klebsiella, Leishmania Viruses (HHV8, VZV, CMV) Histoplasma, Coccidiodes Holland, Steven and Wu, Un-In. Lancet Infectious Disease 2015.
20 Auto-antibodies against IFN-γ Anti-cytokine autoantibodies are increasingly recognized as having a role in disease pathogenesis IgG antibodies that inhibit IFN gamma binding and downstream STAT1 phosphorylation and GAF formation Usually have normal CD4+ T cells, monocytes numbers, IFNGR and IL-12 receptor expression Holland, Steven and Wu, Un-In. Lancet Infectious Disease 2015.


21 Auto-antibodies against IFN-γ Acquired, adult onset immunodeficiency (median age of 50 years) Increased susceptibility to non-tb mycobacterial and other opportunistic infections. Most common in Asia-born Asian patients. Outside Asia, more common in women, otherwise affects both sexes equally. Not associated with tuberculosis, even in TB endemic region. Slide courtesy of Neha Dunn
22 Case 2: Mycobacterium abscessus pulmonary infection 65 year old female with a history of ulcerative colitis s/p total proctocolectomy with ileostomy (1989); breast cancer, s/p lumpectomy, chemotherapy and radiation therapy to the right lung (upper chest) Diagnosed with bronchiectasis in 2003 in the context of multiple episodes bronchitis Had a sputum specimen positive for Mycobacterium abscessus in 2004, but no treatment was initiated
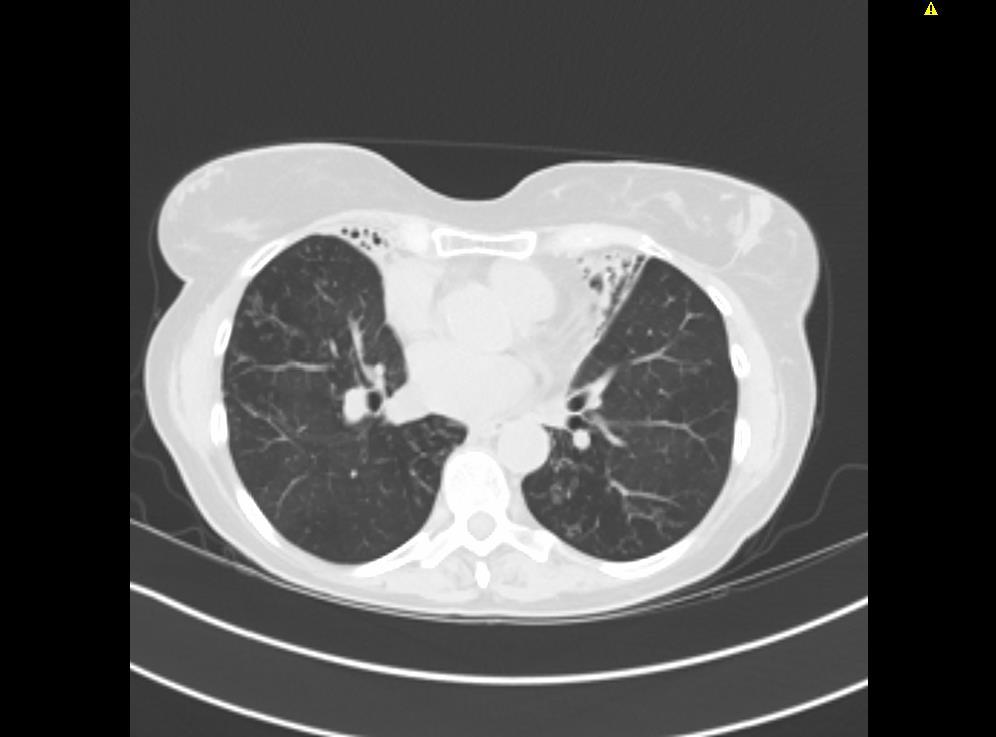
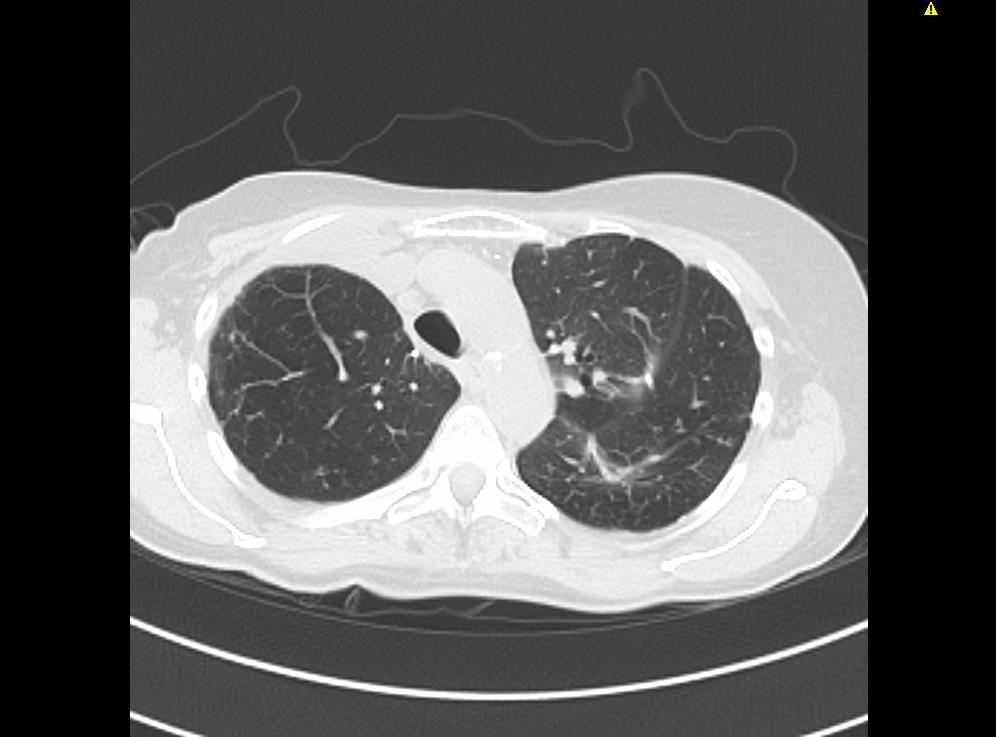
23 Case 2: Diagnosed with cavitary disease : CT scan of the chest demonstrated a right upper lobe cavitary lesion; isolated culture positive for Mycobacterium chelonae 2013: Bronchoscopy with BAL positive for M. abscessus; follow up CT with evidence of persistent cavitary disease. Progression of cavitary disease over the next year and half on serial CT scans
24 Case 2: Progression of cavitary disease HRCT Chest: Cavitary disease in the right upper lobe which had mildly progressed since prior study comparison of 12/12/ dominant cavities within the right upper lobe measuring 2.2 x 2.8 cm and 2.4 x 3.1 cm. Previously noted small cavity in the posterior aspect of the right upper lobe that has filled in, though the underlying cavity is still present. Small cavity in the left upper lobe, which has increased slightly measuring 1.1 compared to 0.9. Increased volume loss within the right upper lobe, moderate bronchiectasis noticed within the pericardiac portions of the lungs, pronounced within the right middle lobe and lingula with volume loss

25
26 Case 2: ADU Evaluation Bronchiectasis likely due to ulcerative colitis +/- reflux and aspiration; radiation pneumonitis in right lung Surgical evaluation: Recommendations for right upper lobe (RUL) and right middle lobe (RML) lobectomy and lingulectomy based on local disease, complicated cavitary disease
27 12/2014
28 Clinical Course Microbiology: Mycobacterium abscessus Cefoxitin intermediate with an MIC of 32 Amikacin intermediate with an MIC of 8 Ciprofloxacin intermediate resistance with an MIC of 2, Moxifloxacin resistant with an MIC of 4 Clarithromycin susceptible with an MIC of less than 0.25, Azithromycin susceptible with an MIC of less than 16 Linezolid intermediate with an MIC of 8 Tigecycline susceptible with an MIC of less than 0.25 Clofazimine susceptible with an MIC of less than 0.05
29 Management of side effects 3 Drug therapy initiated Imipenem developed fever and elevated LFTs IV amikacin developed tinnitus and hearing loss 4 weeks into therapy Azithromycin Clofazimine added when received by the patient 12 weeks of IV therapy prior to lingulectomy
30 Post operative course Lingulectomy 4/30/2015 (Uncomplicated) Right Upper and Middle Lobe Lobectomy 7/28/16 (intraoperative culture positive for 10 colonies of M. abscessus) Post operative course complicated by a wound infection (Right) Suspected secondary to M. abscessus, although serial wound cultures negative Wound completely healed 6 months later (managed by a wound care specialist)
31 8/2016
32 Adjuvant Surgical Resection for NTM Lung Disease Treatment success rates for medical therapy alone: 45-50% MAC, 25-30% M. abscessus Disease localized to one lung or localized disease Ability to tolerate surgery Appropriate pre and post operative antimicrobial therapy Segmentectomy, lobectomy, bilobectomy, pneumonectomy Jarand, et al. CID, 2011
33 Indications for Pulmonary Resection Poor response to medical therapy/treatment failure Limit progression of disease Persistent cavitary lesions Severe focal bronchiectasis Massive hemoptysis/other complications Relief of symptoms Intractable cough Severe and/or recurrent hemoptysis
34 Patient Outcomes Review of outcomes in patients with M. abscessus who underwent adjunctive surgical resection 107 patients over 7 years Comparison of patients on medical therapy versus medical therapy + surgical treatment More surgical than medical patients converted to culture negative and remained so at a year Jarand et al. CID, 2011
35 References Honda JR, Knight V, Chan ED. Pathogenesis and Risk Factors for Nontuberculous Mycobacterial Lung Disease. Clin Chest Med 36 (2015) 1-11 Winthrop KL, McNelley E, Kendall B et al. Pulmonary nontuberculous mycobacterial disease prevalence and clinical features: an emerging public health disease. Am J Respir Crit Care Med 2010; 182: Griffith DE, Aksamit T, Brown-Elliott BA et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 175: Patel SY, Brown M et al. Anti-IFN-gamma autoantibodies in Disseminated Nontuberculous Mycobacterial Infections. J Immunol 2005; 175: Lai CC, Lee LN, et al. Emergence of disseminated infections due to nontuberculous mycobacteria in non-hiv infection patients, including immunocompetent and immunocompromised patients in a university hospital in Taiwan. J Infect Aug; 53(2):77-84 Jarand J, Levin A, Zhang L, Huitt G, Mitchell J, Daley C. Clinical and Microbiologic Outcomes in Patients Receiving Treatment for Mycobacterium abscessus Pulmonary Disease. CID 2011;52:
NTM Lecture Series. Challenging Cases: Part 2. Property of Presenter
 NTM Lecture Series Challenging Cases: Part 2 Dr. Wendi Kay Drummond DO, MPH Assistant Professor of Medicine Division of Mycobacterial and Infectious Diseases Department of Medicine October 20, 2017 Disclosures
NTM Lecture Series Challenging Cases: Part 2 Dr. Wendi Kay Drummond DO, MPH Assistant Professor of Medicine Division of Mycobacterial and Infectious Diseases Department of Medicine October 20, 2017 Disclosures
Nontuberculous Mycobacterial Lung Disease
 Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
2018 Vindico Medical Education. Non-tuberculous Mycobacteria: Circumventing Difficulties in Diagnosis and Treatment
 Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Nontuberculous Mycobacteria
 Nontuberculous Mycobacteria When antibiotics are not enough a surgical approach John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief Section of General Thoracic Surgery University
Nontuberculous Mycobacteria When antibiotics are not enough a surgical approach John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief Section of General Thoracic Surgery University
Diagnostic Evaluation of NTM and Bronchiectasis
 Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients?
 Lung Disease Patients?") How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients? David E. Griffith, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Potential COI Statement I was a
How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients? David E. Griffith, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Potential COI Statement I was a
Nontuberculous Mycobacteria
 Nontuberculous Mycobacteria Epidemiology and Clinical Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health &
Nontuberculous Mycobacteria Epidemiology and Clinical Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health &
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Nontuberculous Mycobacteria (NTM) in Patients with Cystic Fibrosis
 in Patients with Cystic Fibrosis") Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
Pathologic Findings of Surgically Resected Nontuberculous Mycobacterial Pulmonary Infection
 The Korean Journal of Pathology 2010; 44: 56-62 DOI: 10.4132/KoreanJPathol.2010.44.1.56 Pathologic Findings of Surgically Resected Nontuberculous Mycobacterial Pulmonary Infection Hye-Jong Song Jung Suk
The Korean Journal of Pathology 2010; 44: 56-62 DOI: 10.4132/KoreanJPathol.2010.44.1.56 Pathologic Findings of Surgically Resected Nontuberculous Mycobacterial Pulmonary Infection Hye-Jong Song Jung Suk
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review
 Showa Univ J Med Sci 28 4, 373 377, December 2016 Case Report Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review Makoto HAYASHI 1, Satoshi MATSUKURA 1,
Showa Univ J Med Sci 28 4, 373 377, December 2016 Case Report Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review Makoto HAYASHI 1, Satoshi MATSUKURA 1,
Nontuberculous Mycobacteria (NTM)
") Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
AIDS. 1) Mycobacterium avium MRI (T2WI) HTLV-1 AIDS. Key words: Mycobacterium avium AIDS. Mycobacterium. complex MAC M. avium M.
 Mycobacterium avium MRI (T2WI) HTLV-1 AIDS. Key words: Mycobacterium avium AIDS. Mycobacterium. complex MAC M. avium M.") 2008 193 AIDS Mycobacterium avium 1) 2) 3) 4) 4) 3) 3) 3) 5) 1) 6) 1) 2) 3) 4) 5) 6) 20 1 30 20 6 13 46 MRI (T2WI) MRI 5 Mycobacterium avium M. avium HIV HTLV-1 AIDS AIDS Key words: Mycobacterium avium
2008 193 AIDS Mycobacterium avium 1) 2) 3) 4) 4) 3) 3) 3) 5) 1) 6) 1) 2) 3) 4) 5) 6) 20 1 30 20 6 13 46 MRI (T2WI) MRI 5 Mycobacterium avium M. avium HIV HTLV-1 AIDS AIDS Key words: Mycobacterium avium
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Mycobacterium abscessus Lung Disease in a Patient with Kartagener Syndrome
 CASE REPORT http://dx.doi.org/10.4046/trd.2014.77.3.136 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2014;77:136-140 Mycobacterium abscessus Lung Disease in a Patient with Kartagener Syndrome
CASE REPORT http://dx.doi.org/10.4046/trd.2014.77.3.136 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2014;77:136-140 Mycobacterium abscessus Lung Disease in a Patient with Kartagener Syndrome
Slowly Growing Nontuberculous Mycobacterial Infections
 Slowly Growing Nontuberculous Mycobacterial Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Advisory Board Horizon, Johnson and Johnson, Otsuka and Spero
Slowly Growing Nontuberculous Mycobacterial Infections Charles L. Daley, MD National Jewish Health University of Colorado, Denver Disclosures Advisory Board Horizon, Johnson and Johnson, Otsuka and Spero
Shannon Kasperbauer, M.D. National Jewish Health University of Colorado Health Sciences Center. Property of Presenter. Not for Reproduction
 Shannon Kasperbauer, M.D. National Jewish Health University of Colorado Health Sciences Center Consultant: Johnson and Johnson Speaker/consultant: Insmed Examine characteristics of the RGM Define the main
Shannon Kasperbauer, M.D. National Jewish Health University of Colorado Health Sciences Center Consultant: Johnson and Johnson Speaker/consultant: Insmed Examine characteristics of the RGM Define the main
Cardiovascular Center Grand Rounds. December 15, 2016
 Cardiovascular Center Grand Rounds December 15, 2016 Agenda Overview of Heater-Cooler Device Issue NTM Infection Incidence Chronology of Events and Communications Risk Management Implications Q&A NTM Grand
Cardiovascular Center Grand Rounds December 15, 2016 Agenda Overview of Heater-Cooler Device Issue NTM Infection Incidence Chronology of Events and Communications Risk Management Implications Q&A NTM Grand
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 Nontuberculosis Mycobacterial Lung Disease David Griffith, MD August 8, 2012 David Griffith, MD has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 Nontuberculosis Mycobacterial Lung Disease David Griffith, MD August 8, 2012 David Griffith, MD has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
2/18/19. Case 1. Question
 Case 1 Which of the following can present with granulomatous inflammation? A. Sarcoidosis B. Necrobiotic xanthogranulma C. Atypical mycobacterial infection D. Foreign Body Reaction E. All of the above
Case 1 Which of the following can present with granulomatous inflammation? A. Sarcoidosis B. Necrobiotic xanthogranulma C. Atypical mycobacterial infection D. Foreign Body Reaction E. All of the above
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Mycobacterial Infections in HIV. H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine
 Mycobacterial Infections in HIV H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine Learning Objectives List the most common mycobacterial infections
Mycobacterial Infections in HIV H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine Learning Objectives List the most common mycobacterial infections
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Using Xpert to discontinue airborne isolation The Consensus Statement
 Using Xpert to discontinue airborne isolation The Consensus Statement Neha Shah, MD MPH Tuberculosis Control California Department of Public Health Centers for Disease Control and Prevention NAR February
Using Xpert to discontinue airborne isolation The Consensus Statement Neha Shah, MD MPH Tuberculosis Control California Department of Public Health Centers for Disease Control and Prevention NAR February
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Nontuberculous Mycobacterial Lung Disease David Griffith, MD October 15, 2013 David Griffith, MD has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Nontuberculous Mycobacterial Lung Disease David Griffith, MD October 15, 2013 David Griffith, MD has the following disclosures to make: No conflict of interests
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis)
") Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Management of Drug-resistant Tuberculosis (DR-TB)
") Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Clinical Manifestations of HIV
 HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Implication of species change of Nontuberculous Mycobacteria during or after treatment
 Lee et al. BMC Pulmonary Medicine (2017) 17:213 DOI 10.1186/s12890-017-0539-7 RESEARCH ARTICLE Open Access Implication of species change of Nontuberculous Mycobacteria during or after Jong Sik Lee 1, Jong
Lee et al. BMC Pulmonary Medicine (2017) 17:213 DOI 10.1186/s12890-017-0539-7 RESEARCH ARTICLE Open Access Implication of species change of Nontuberculous Mycobacteria during or after Jong Sik Lee 1, Jong
ACCME/Disclosures. Two Patients and a Caveat 4/13/2016. Patient #1: 13 y/o boy with IPEX syndrome; s/p BMT
 Two Patients and a Caveat The Use and Misuse of Molecular Methods in Mycobacterial Infections Gary W. Procop, MD Director, Molecular Microbiology Infectious Disease Pathologist Cleveland Clinic ACCME/Disclosures
Two Patients and a Caveat The Use and Misuse of Molecular Methods in Mycobacterial Infections Gary W. Procop, MD Director, Molecular Microbiology Infectious Disease Pathologist Cleveland Clinic ACCME/Disclosures
Geographical distribution and clinical relevance of nontuberculous mycobacteria in Croatia
 Geographical distribution and clinical relevance of nontuberculous mycobacteria in Croatia M. Jankovic 1, M. Samarzija 1, I. Sabol 2, M. Jakopovic 1, V. Katalinic Jankovic 3, LJ. Zmak 3, B. Ticac 4, A.
Geographical distribution and clinical relevance of nontuberculous mycobacteria in Croatia M. Jankovic 1, M. Samarzija 1, I. Sabol 2, M. Jakopovic 1, V. Katalinic Jankovic 3, LJ. Zmak 3, B. Ticac 4, A.
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
A Vietnamese woman with a 2-week history of cough
 Delphine Natali 1, Hai Tran Pham 1, Hung Nguyen The 2 delphinenatali@gmail.com Case report A Vietnamese woman with a 2-week history of cough A 52-year-old nonsmoker Vietnamese woman without any past medical
Delphine Natali 1, Hai Tran Pham 1, Hung Nguyen The 2 delphinenatali@gmail.com Case report A Vietnamese woman with a 2-week history of cough A 52-year-old nonsmoker Vietnamese woman without any past medical
Mycobacterium fortuitum,
 2009 177 Mycobacterium fortuitum 1 1) 2) 3) 1) 1) 4) 4) 5) 2) 1) 1) 2) 3) 4) 5) 21 3 16 21 7 1 Mycobacterium fortuitum 1 39 BHI 2 Ziehl Neelsen M. fortuitum MIC CPFX 0.2 mg/ml, MINO 0.78 mg/ml, CAM 100
2009 177 Mycobacterium fortuitum 1 1) 2) 3) 1) 1) 4) 4) 5) 2) 1) 1) 2) 3) 4) 5) 21 3 16 21 7 1 Mycobacterium fortuitum 1 39 BHI 2 Ziehl Neelsen M. fortuitum MIC CPFX 0.2 mg/ml, MINO 0.78 mg/ml, CAM 100
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI Page 1 Page 2 nontuberculous mycobacteria ntm nontuberculous mycobacteria ntm pdf nontuberculous mycobacteria ntm patients and those
DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI Page 1 Page 2 nontuberculous mycobacteria ntm nontuberculous mycobacteria ntm pdf nontuberculous mycobacteria ntm patients and those
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW.
 INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW.") NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW. K. Clay 1, K. Bhatt 1, D. Burns 1, J. Evans 2, S. Gardiner 2, EG. Smith 2, P. Hawkey 2,
NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW. K. Clay 1, K. Bhatt 1, D. Burns 1, J. Evans 2, S. Gardiner 2, EG. Smith 2, P. Hawkey 2,
Appendix C. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Slide 120, Lobar Pneumonia. Slide 120, Lobar Pneumonia. Slide 172, Interstitial Pneumonia. Slide 172, Interstitial Pneumonia. 53 Year-Old Smoker
 Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical and Pathologic Features of Mycobacterium fortuitum Infections. An Emerging Pathogen in Patients With AIDS
 Microbiology and Infectious Disease/ MYCOBACTERIUM FORTUITUM INFECTION IN PATIENTS WITH AIDS Clinical and Pathologic Features of Mycobacterium fortuitum Infections An Emerging Pathogen in Patients With
Microbiology and Infectious Disease/ MYCOBACTERIUM FORTUITUM INFECTION IN PATIENTS WITH AIDS Clinical and Pathologic Features of Mycobacterium fortuitum Infections An Emerging Pathogen in Patients With
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
A CASE OF RECURRENT TUBERCULOSIS -LAVANYA DR. S. BALASUBRAMANIAN S UNIT SR. CONSULTANT KKCTH
 A CASE OF RECURRENT TUBERCULOSIS -LAVANYA DR. S. BALASUBRAMANIAN S UNIT SR. CONSULTANT KKCTH PRESENTING COMPLAINTS 8 year old boy 3 o consanguineous marriage low grade fever and swelling left parotid area
A CASE OF RECURRENT TUBERCULOSIS -LAVANYA DR. S. BALASUBRAMANIAN S UNIT SR. CONSULTANT KKCTH PRESENTING COMPLAINTS 8 year old boy 3 o consanguineous marriage low grade fever and swelling left parotid area
Refractory Bacteremia and Osteomyelitis Resulting in Fatal. Bacteremic Pneumonia with Multiorgan Failure Caused by
 JCM Accepts, published online ahead of print on 2 September 2009 J. Clin. Microbiol. doi:10.1128/jcm.00627-09 Copyright 2009, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 2 September 2009 J. Clin. Microbiol. doi:10.1128/jcm.00627-09 Copyright 2009, American Society for Microbiology and/or the Listed Authors/Institutions. All
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Original Article Tree-in-bud pattern of chest CT images for diagnosis of Mycobacterium abscesses
 Int J Clin Exp Med 2015;8(10):18705-18712 www.ijcem.com /ISSN:1940-5901/IJCEM0013538 Original Article Tree-in-bud pattern of chest CT images for diagnosis of Mycobacterium Haiqing Chu 1, Bing Li 1, Lan
Int J Clin Exp Med 2015;8(10):18705-18712 www.ijcem.com /ISSN:1940-5901/IJCEM0013538 Original Article Tree-in-bud pattern of chest CT images for diagnosis of Mycobacterium Haiqing Chu 1, Bing Li 1, Lan
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Novel Therapies for NTM
 NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Surgery for MDR/XDR Tuberculosis
 Surgery for MDR/XDR Tuberculosis John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief, General Thoracic Surgery Department of Surgery University of Colorado School of Medicine
Surgery for MDR/XDR Tuberculosis John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief, General Thoracic Surgery Department of Surgery University of Colorado School of Medicine
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Nontuberculous Mycobacteria: Ubiquitous Environmental Pathogens for Predisposed Hosts
 Nontuberculous Mycobacteria: Ubiquitous Environmental Pathogens for Predisposed Hosts History, Epidemiology, Spectrum of Disease Diagnosis, Treatment and Predictors of Treatment Outcome James L. Cook,
Nontuberculous Mycobacteria: Ubiquitous Environmental Pathogens for Predisposed Hosts History, Epidemiology, Spectrum of Disease Diagnosis, Treatment and Predictors of Treatment Outcome James L. Cook,
Property of Presenter. Not for Reproduction DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS
 DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
Lung cancer in patients with chronic empyema
 Lung cancer in patients with chronic empyema Poster No.: P-0025 Congress: ESTI 2015 Type: Scientific Poster Authors: Y. Lee, C.-K. Park; Guri/KR Keywords: Neoplasia, Biopsy, PET-CT, CT, Thorax, Lung DOI:
Lung cancer in patients with chronic empyema Poster No.: P-0025 Congress: ESTI 2015 Type: Scientific Poster Authors: Y. Lee, C.-K. Park; Guri/KR Keywords: Neoplasia, Biopsy, PET-CT, CT, Thorax, Lung DOI:
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Myositis and Your Lungs
 Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Ryo Takahashi 1,2,3, Taiki Fujiwara 1,2, Hisami Yamakawa 1,2. Introduction
 Case Report Completion pneumonectomy after fenestration for empyema due to nontuberculous mycobacteriosis associated with destroyed lung as a result of cancer surgery Ryo Takahashi 1,2,3, Taiki Fujiwara
Case Report Completion pneumonectomy after fenestration for empyema due to nontuberculous mycobacteriosis associated with destroyed lung as a result of cancer surgery Ryo Takahashi 1,2,3, Taiki Fujiwara