Breast Pathology Post-Neoadjuvant Chemotherapy. Megan Troxell, MD/PhD Stanford Pathology
|
|
|
- Thomas Fields
- 6 years ago
- Views:
Transcription

1 Breast Pathology Post-Neoadjuvant Chemotherapy Megan Troxell, MD/PhD Stanford Pathology
2 2 mm
3 Objectives Develop a framework for gross analysis of post-chemotherapy breast specimens. Recognize histologic features of tumor bed and post-chemo carcinoma, including pitfalls Understand reporting schemes, utility and clinical impact of residual tumor burden

4 Neoadjuvant chemotherapy Kummel. BJS 2014; 101: Equivalent long term outcome whether chemotherapy before or after surgery Neoadjuvant: Can assess response/non-response Degree of response: prognostic for survival Response is short term endpoint for clinical trials Tissue collection for research before/during/after Downsize tumor for breast conserving surgery Chemo most efficacious in Her2+ or triple negative tumors, (vs ER+) Now standard of care for locally advanced breast cancer


5 More extensive diagrams Mod Pathol 2015; 28:
6 RCB Prognostic information from degree of pathologic response? Propose RCB as continuous variable: primary tumor dimensions, residual cellularity of tumor bed axillary nodal burden
7 Initial diagnostic pathology Breast Adequate core biopsy essential Caution if limited tumor or extensive DCIS ER, PR, Her2 & other markers % tumor cellularity for some studies Clip placement essential! Hint: core is often ~6 months ago if neoadjuvant Rx Axilla Status impacts local/systemic therapy Routine axillary ultrasound FNA or core bx for clinical, radiologic abnormal nodes Clip!?? Recommended by NCCN 15 Up-front surgical SLN bx not recommended Invalidates ypn & RCB Precludes assessment of nodal response
8 Steps to evaluate post-chemo breast 1. Recognize its post-chemo 2. Identify gross tumor/tumor bed & document size 3. Judiciously sample (map) 4. Assess residual size (largest contiguous and span), cellularity & standard parameters 5. Evaluate lymph nodes 6. Report as per local custom/mandates
 Was the axillary node clipped?")
9 Essential clinical info with specimen At an absolute minimum, the specimen must be clearly marked as post-nast; pre-nast location and size of the tumor must be indicated. (Bossuyt) Was the axillary node clipped?? & five other elements



10 Patterns of residual CA Provenzano Research samples only if grossly obvious residual invasive cancer. (Bossuyt)
11 Specimen sampling CAP: Special attention to finding and evaluating the tumor bed is necessary for these specimens. Provenzano: It is strongly recommended that an image of the sliced specimen be recorded (radiograph, photograph, photocopy, or drawing) and then used as a map for the sections taken, so that the histopathologic findings of any residual disease in the breast can be more easily understood. Bossuyt: Overly exhaustive sampling and histologic evaluation of the entire tumor bed are not required and not as efficient or informative as informed mapping of the specimen.

12 Bossuyt et al. Ann Oncol. 2015;26:
13 Specimen sampling Small specimens: submit entirely, mapped Document if tumor bed at specimen edge (esp if residual scattered ca) Large specimens: guided by pretreatment size & location, mapped Provenzano: full face of pretreatment area every 1 cm If very large, 5 blocks per every 1-2 cm, up to 25 blocks Good clinical judgment on a case-by-case basis RCB: Submit the largest cross-sectional area for histology FDA: at least one block per cm of pre-treatment tumor size, or at least 10 blocks in total (greater of) Sahoo 09: ~1 section/cm of original tumor size Multiple pretreatment lesions: as above & sample between lesions Intervening invasive CA or DCIS? Largest is used for RCB and ypt stage
14 Localizing post-chemo Once you have the slides, document at least one of: 1) Tumor/lesion compatible with findings on prior biopsy -- If abundant tumor, I don t mandate section of biopsy site -- Caution: second occult tumor 2) Tumor bed 3) Biopsy site or clip -- Rarely, minimal histologic evidence -- But clips can migrate, or displace during sectioning.


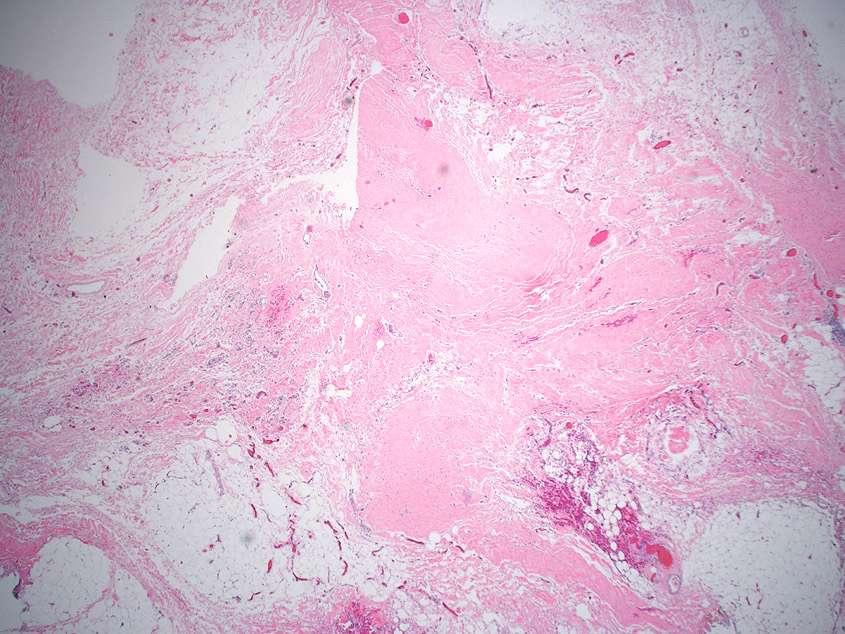
15 Tumor bed Grossly: fibrous rubbery area; here with residual tumor Sahoo & Lester. Surgical Pathology Clinics 2012:5;749 74
16 Mastectomy: clips at 12:00 (or nipple bed) Stitch axillary tail
 Stitch axillary tail Need to know location, size of pre-chemo cancer(s) Any additional lesions on")
17 Section nipple, ink, slice, photo or Xray in order, then map sections taken Mastectomy: clips at 12:00 (or nipple bed) Stitch axillary tail Need to know location, size of pre-chemo cancer(s) Any additional lesions on imaging


")
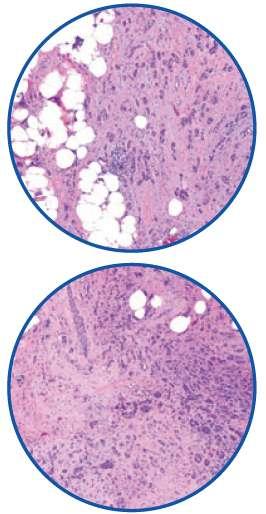
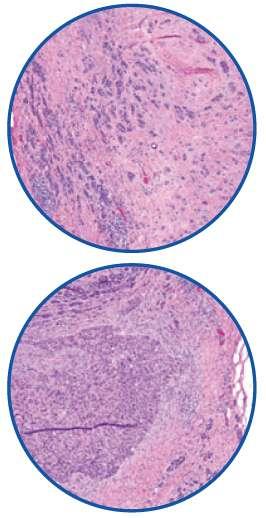
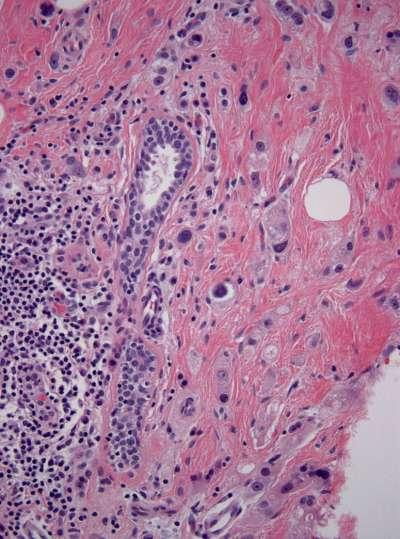
18 Pre-chemo cores heterogeneity, focal geographic necrosis (not shown) Post-chemo Poor response



19 Pre-chemo core Continued Post-chemo tumor bed: DCIS (below) Medial
20

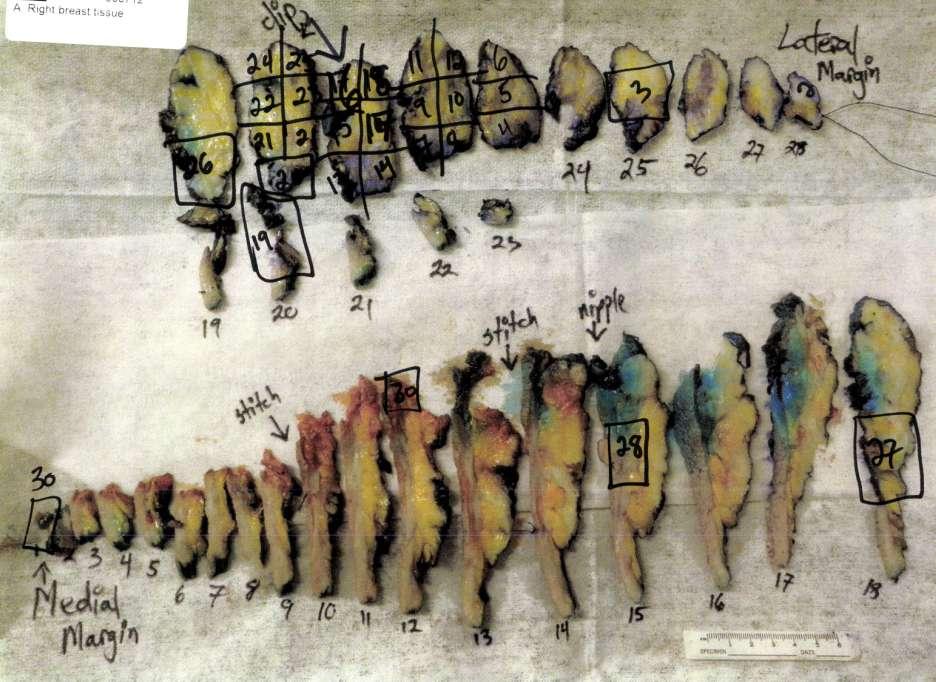
21 Continued Safety pins mark lesions ID ed fresh

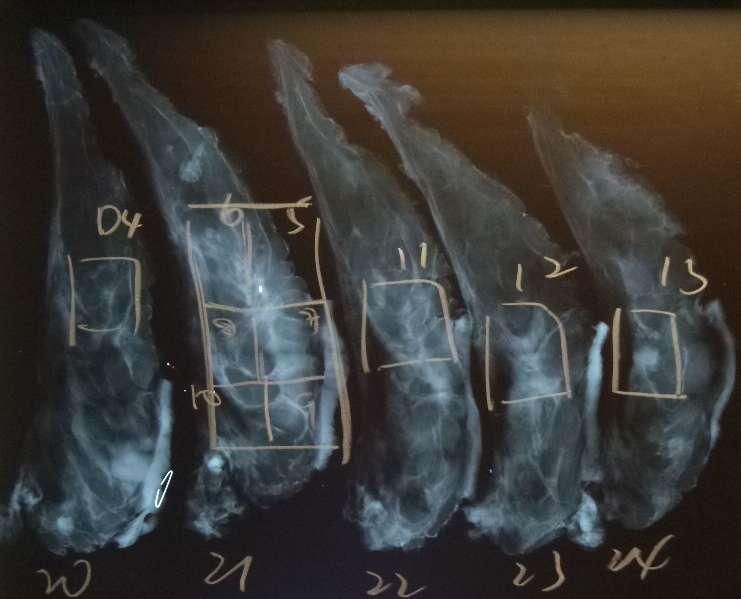
22 Mapped with specimen Xray Also see calcifications
23

24

25 Lumpectomy with 3 clips!
26 What is this in the specimen? Cox. Ann Surg Oncol 2016;23: Gilcrease. AJSP 2016; 40:



27 What is this in the specimen? Savi SCOUT Titanium Encapsulated Radioactive Seed Mango. AJR 2016; 207:W1 W4 Cox. Ann Surg Oncol 2016;23: Gilcrease. AJSP 2016; 40:

28 New wire-loc alternatives Savi SCOUT Radioactive seeds Intraoperative US Magseed Cox. Ann Surg Oncol 2016;23:
29 Gilcrease. AJSP 2016; 40: I 125 localized w/ gamma probe Mayo: 0/2000 MD Anderson: 2/1400 Case 1 Specimen radiograph shows parts of Ti cap in 2 slices!! Case 2: large ossified mass Seed cut with bone saw Titanium cap not damaged Why the &^%$##!! was localization used? If immobilized with forceps, seeds can severed with scalpel blade Use forceps with finesse; no scissors Added recommendations: Know where seed is; use same gamma probe as is used in OR as blade approaches the location of the seed, slow and careful slicing of the tissue Dedicated grossing bench; do not discard anything until seed retrieved
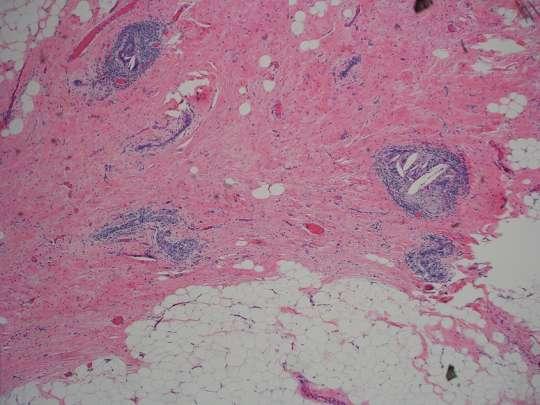
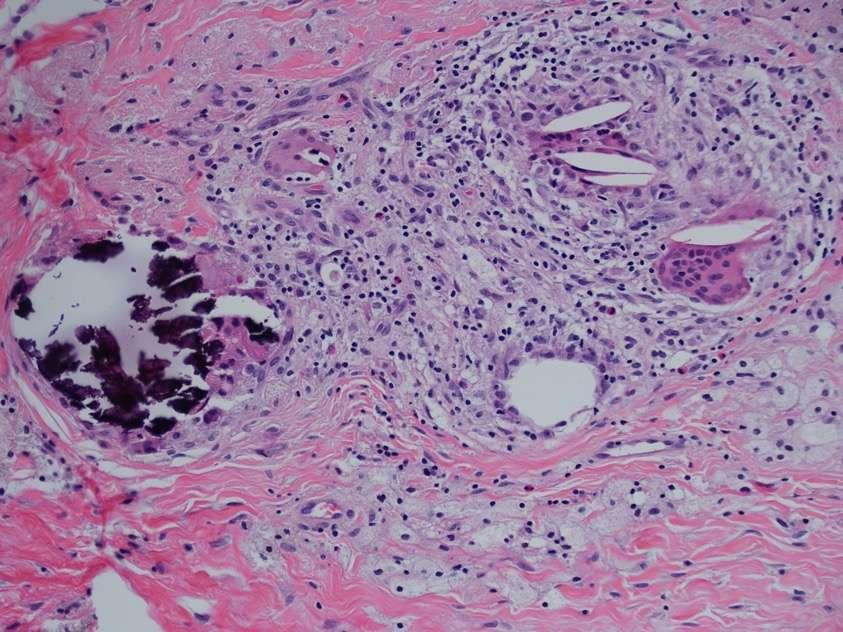
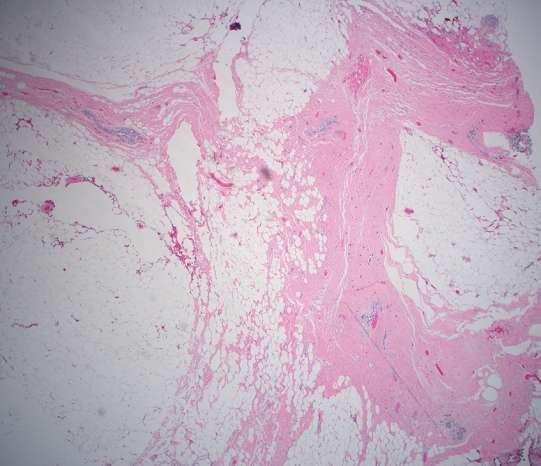
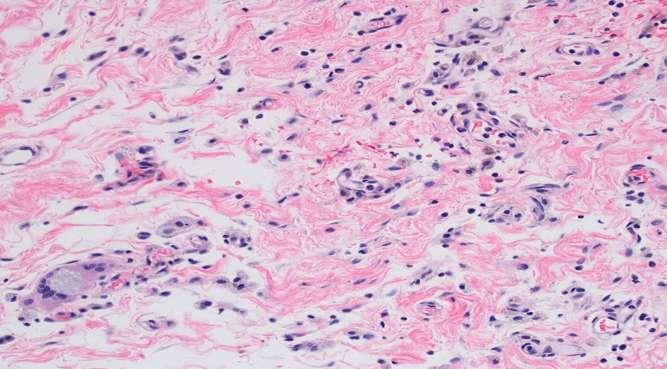
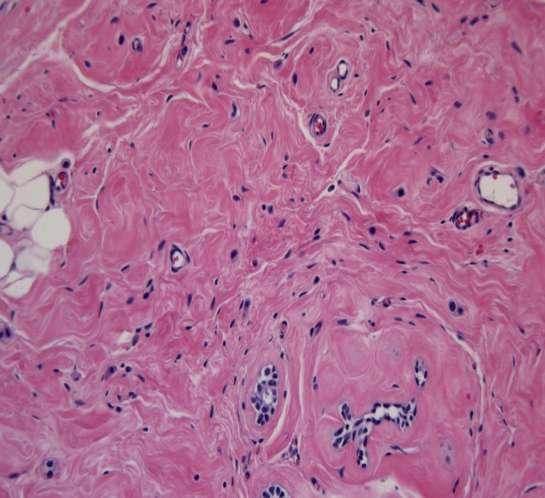
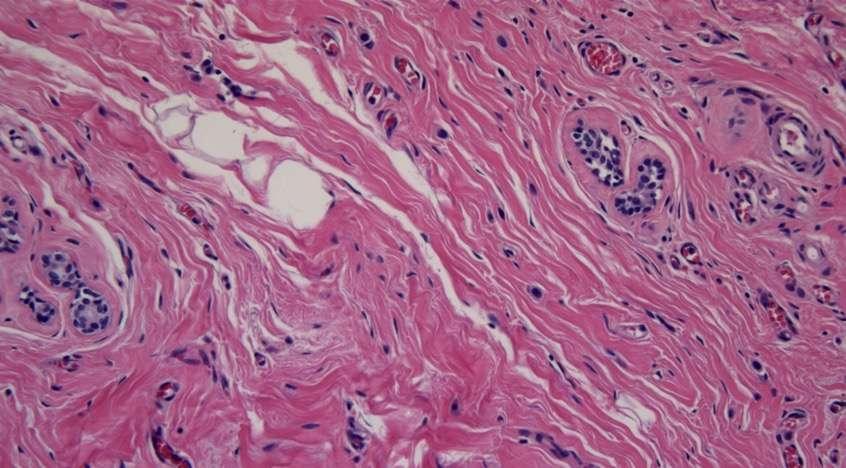
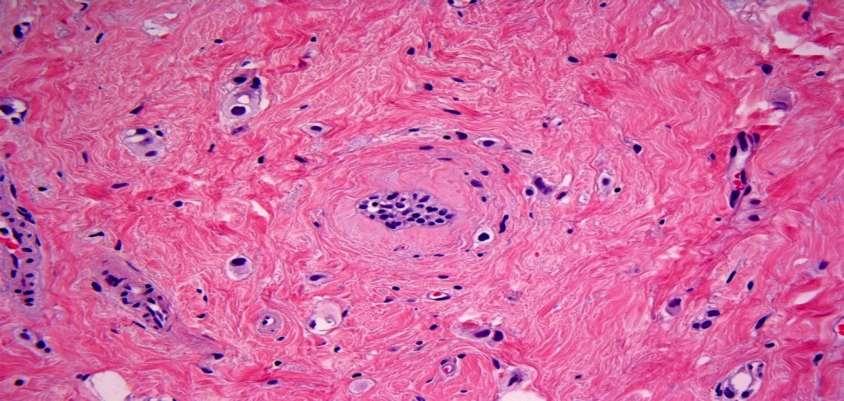
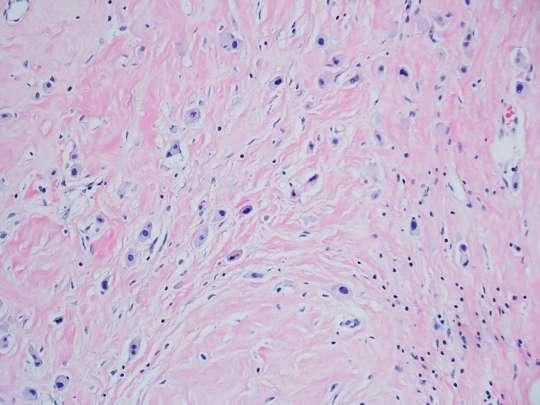
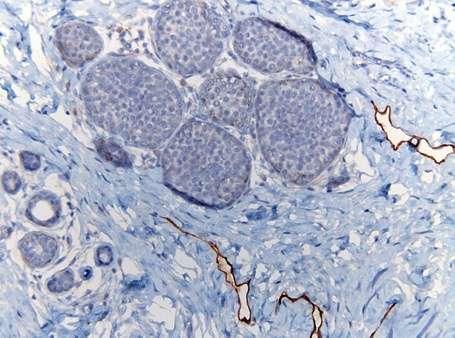
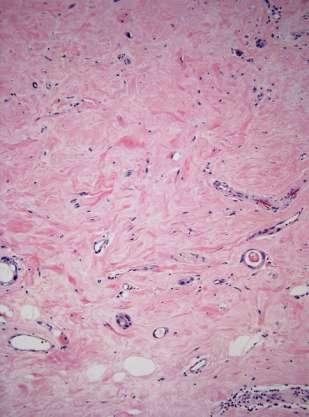
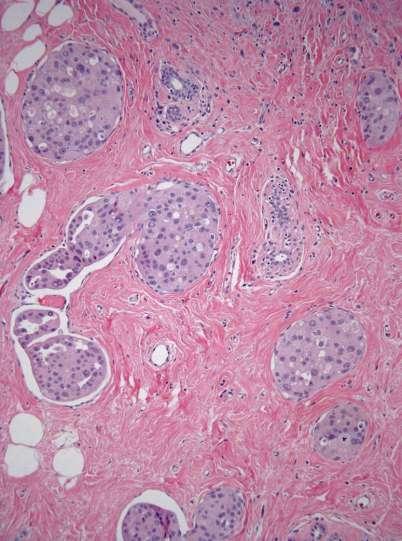
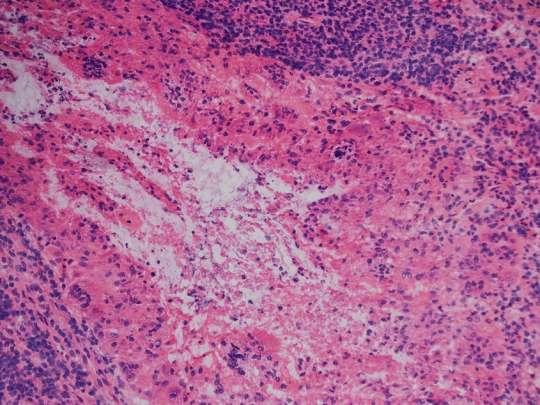
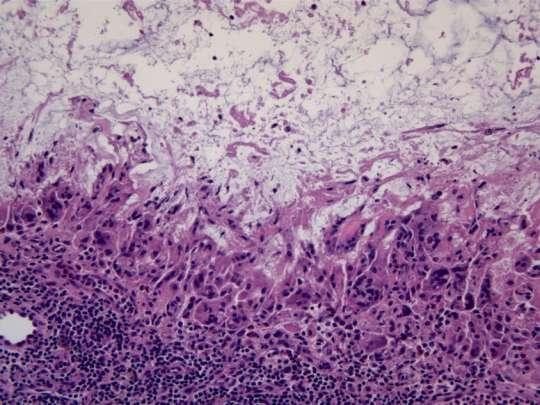
30 Histologic tumor bed Fibrosis +/- elastosis Prominent vessels Fewer to absent normal epithelial structures Inflammation histiocytes, lymphs, giant cells Hemosiderin Calcification Find: 1) Tumor 2) Tumor bed 3) Bx site or clip

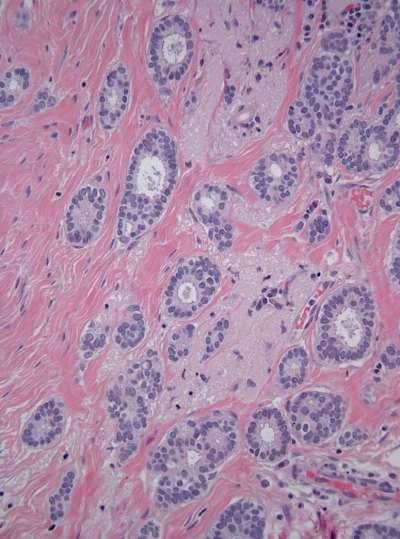
31 Tumor bed: vessels, fibrosis, paucity of normal
32

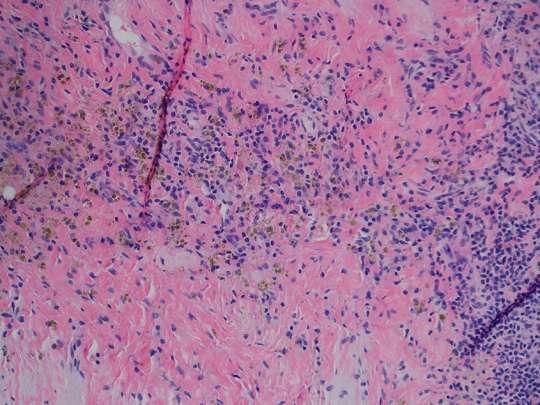
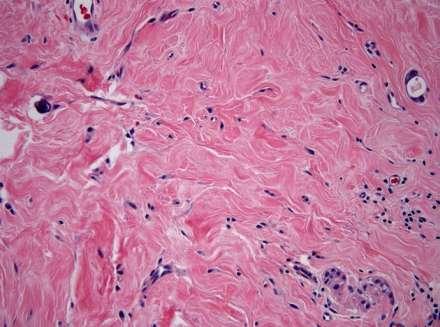
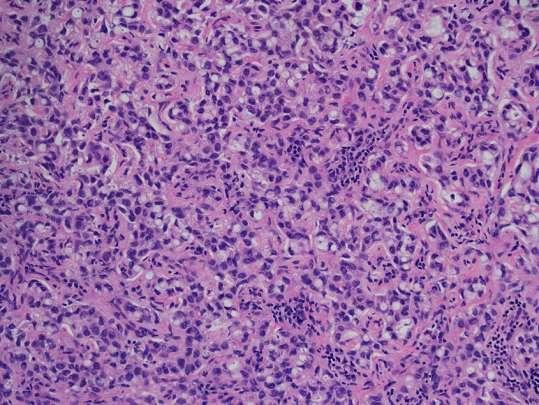
33 Histiocyte rich tumor bed



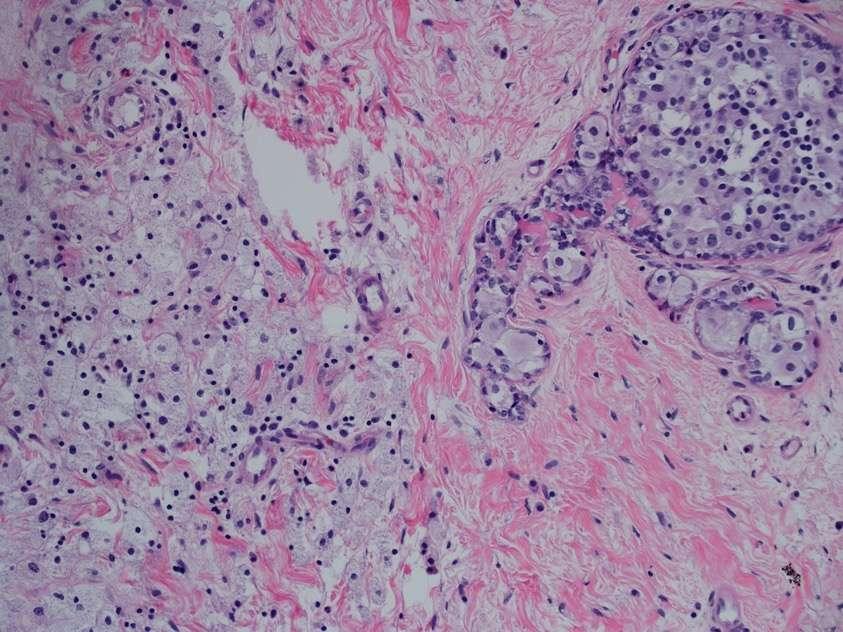
34 Normal breast Edge of tumor bed; same specimen


35 Edge of tumor bed Biopsy site in tumor bed
36


37 Left: parenchymal atrophy post-chemo Below: LCIS unperturbed by chemo
38 Bowtie clip M clip
39


40 Lack of tumor bed stromal change

41 Tumor Bed...

42

 Bx site")
43 History of G3 IDC, triple negative Find: 1) Tumor 2) Tumor bed 3) Bx site or clip
 Tumor")

44 History of G3 IDC, triple negative, prior Find: 1) Tumor 2) Tumor bed 3) Bx site or clip Several foci like this post-chemo



45 Prior axillary LN core biopsy

")
 Bx or")
46 Biopsy site Find: 1) Tumor 2) Tumor bed 3) Bx site or clip

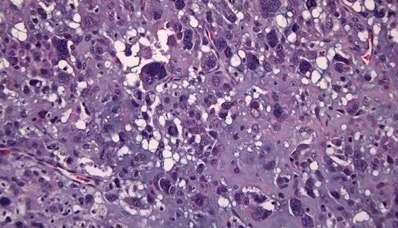
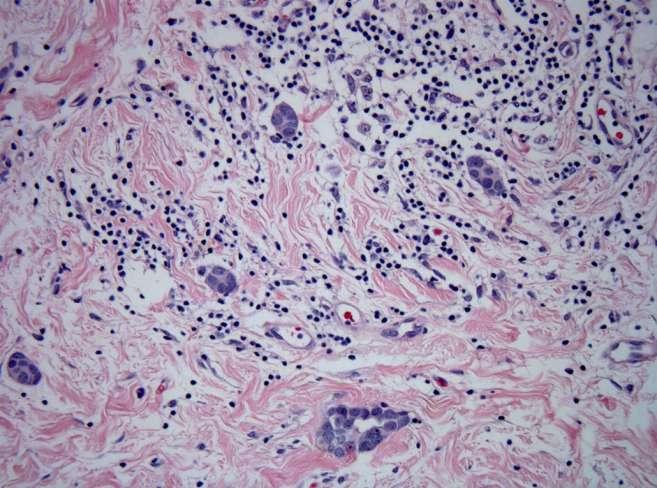
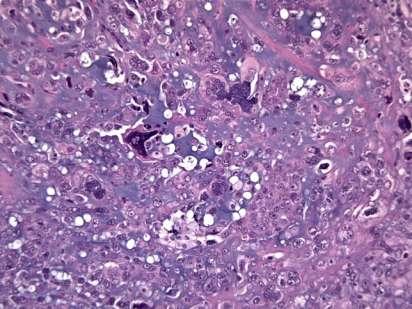
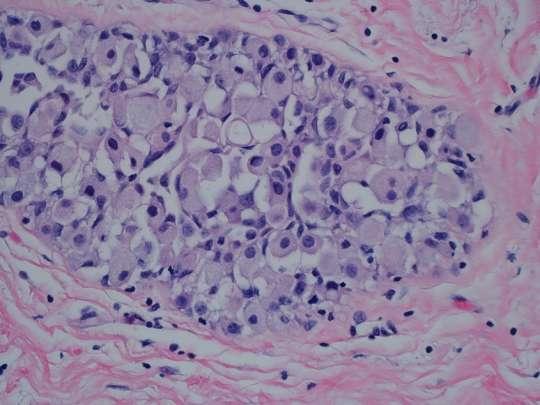
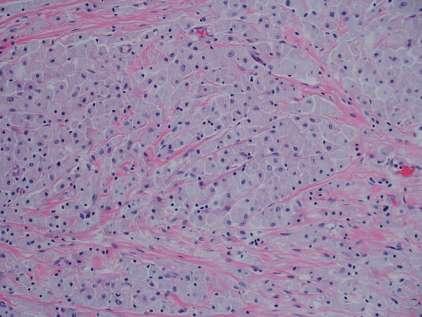
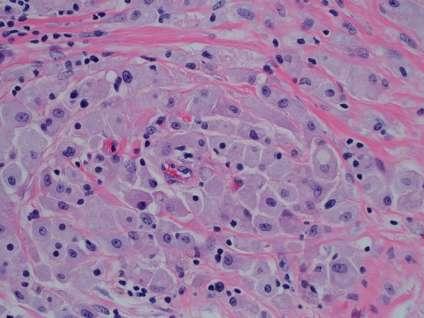
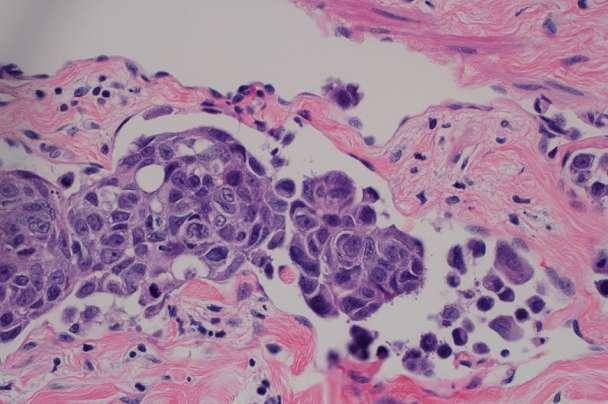
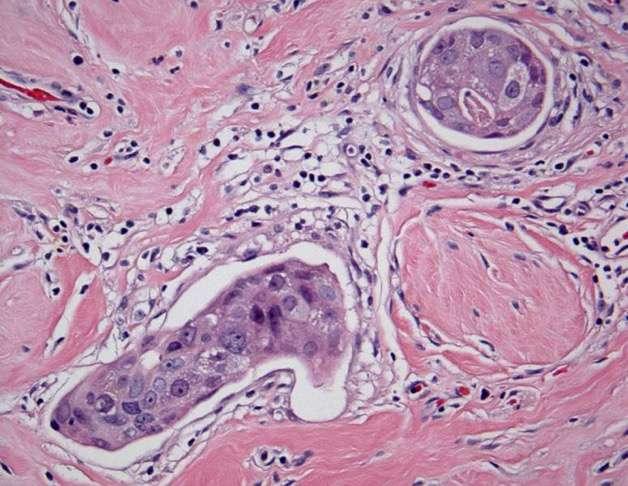
47 Changes in carcinoma histology Histiocytoid appearance Cytoplasmic vacuolization, eosinophilia Nuclear hyperchromasia, pleomorphism Multinucleation Decreased mitotic activity Lobular-like growth pattern Retraction artifact Heterogeneity (selection by chemo?) Expect cellularity to vary across tumor Sahoo, Provenzano
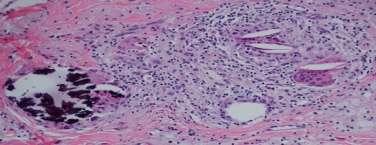
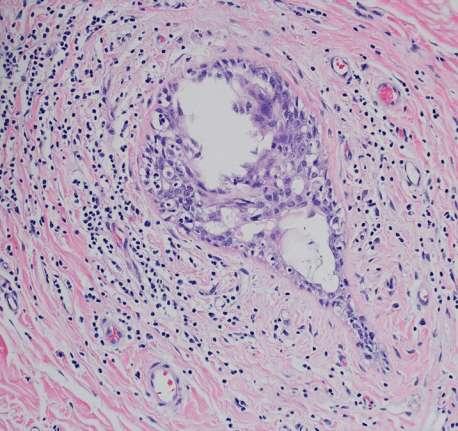
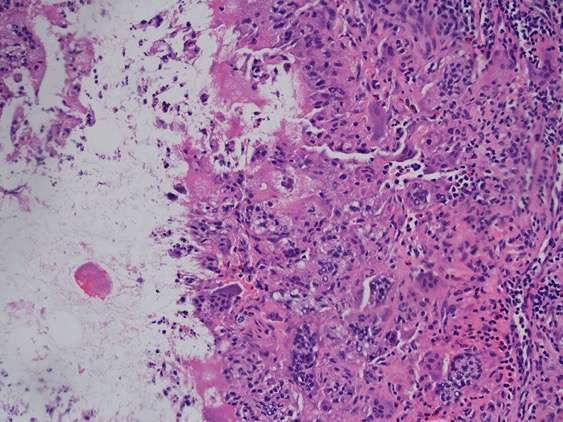
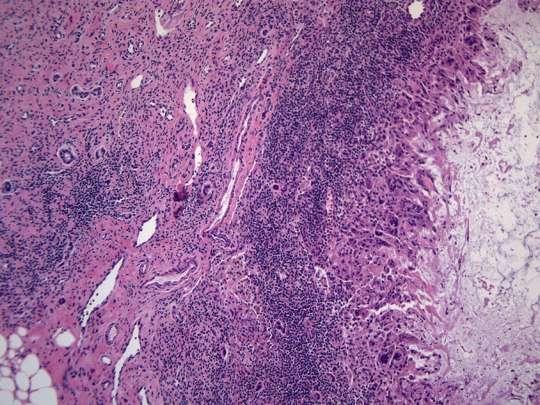
48 Tumor bed & DCIS
49 Tumor bed & DCIS

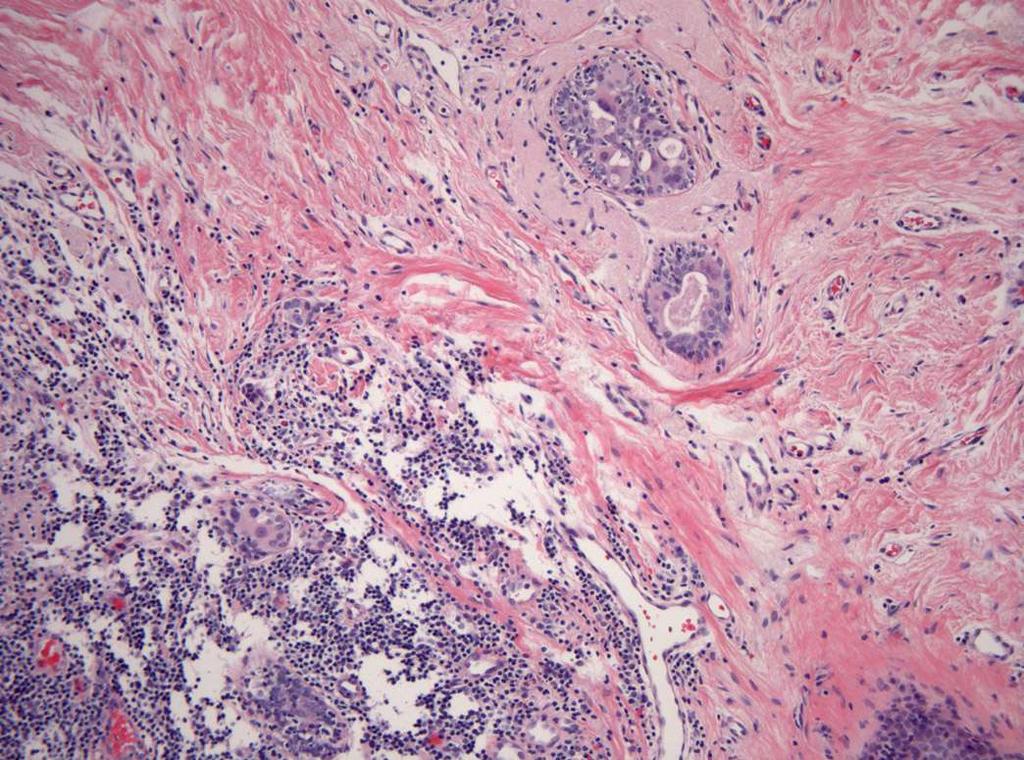
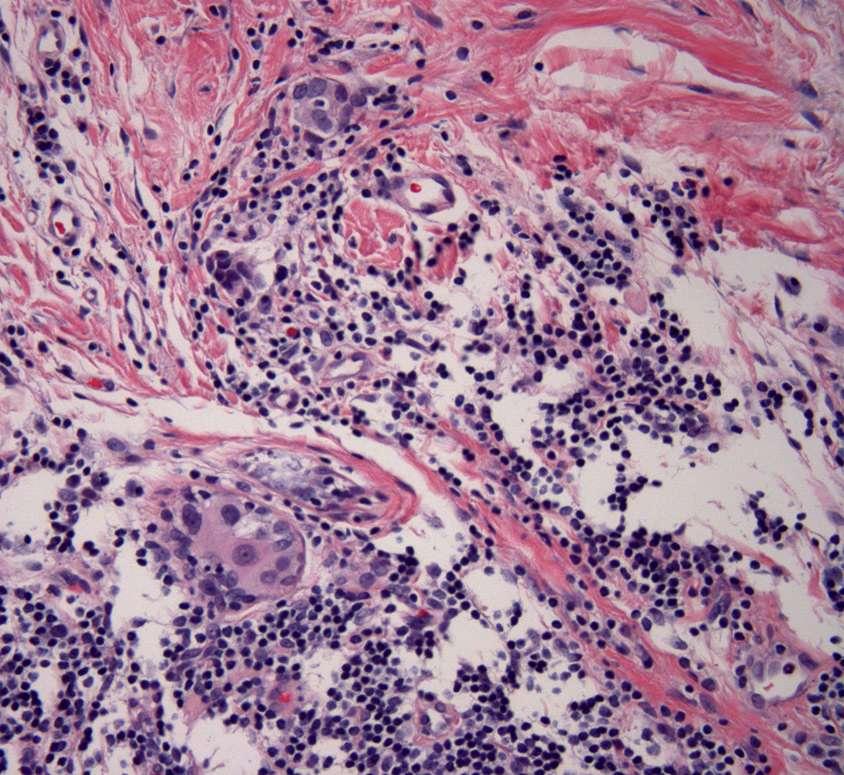
50 Tumor bed & DCIS
51

52

53 Atypia vs. DCIS?
54 Grading post chemo Often increased nuclear pleomorphism Often decreased mitotic rate Should still be graded Nottingham/mSBR/Elston-Ellis Tubules, nuclei, mitosis

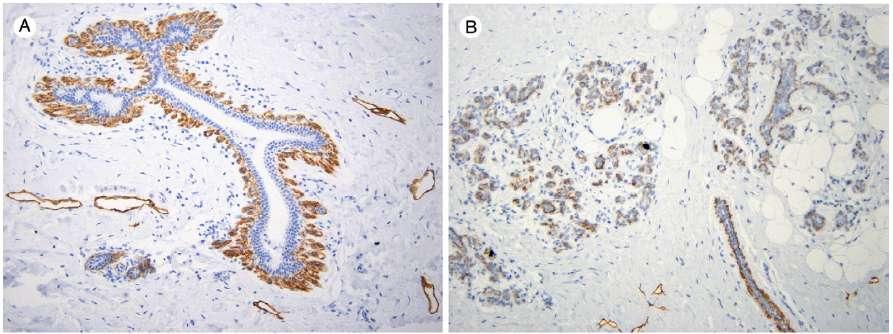
55 Treated carcinoma Metaplasia due to chemotherapy? Squamous elements relatively resistant to chemotherapy?

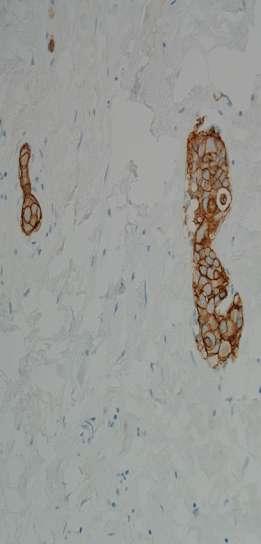
56 Keratin ER
57 Different morphologies across tumor


58 Pre-chemo core Heterogeneity post-chemo
59 Residual histiocytoid IDC & DCIS

60 Dermal tumor Heterogeneous tumor vs. histiocytes?

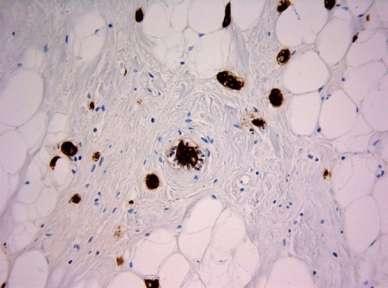
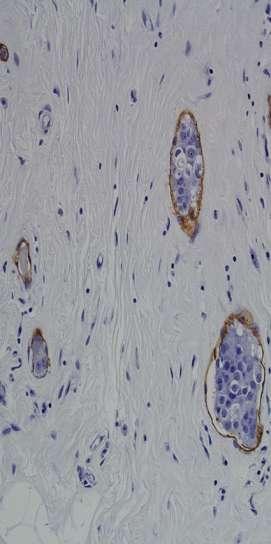
61 Residual invasive carcinoma vs histiocytes?


62 Residual invasive carcinoma vs histiocytes? Keratin



63 Multiple tumors: different chemosensitivity Left: Core bx IDC3, met to LN ER+, PR- Her2+ Right: Post-chemo tumor bed with no residual IDC
64 Same patient Left: Core bx ILC, E-cad negative Right: Post-chemo residual ILC



65 Same patient Chemo response: Her2+ > Triple Neg >> ER+Her2-
66 Post-chemo reporting: CAP (AJCC R) In the Breast No known presurgical therapy No definite response to presurgical therapy in the invasive carcinoma Probable or definite response to presurgical therapy in the invasive ca No residual invasive carcinoma is present in the breast after presurgical therapy In the Lymph Nodes No known presurgical therapy No lymph nodes removed No definite response to presurgical therapy in metastatic carcinoma Probable or definite response to presurgical therapy in metastatic ca No lymph node metastases. Fibrous scarring, possibly related to prior lymph node metastases with pathologic complete response No lymph node metastases and no prominent fibrous scarring in the nodes
67 System Score in breast Correlate w/ core? LN included? B-18 Any treatment effect on invasive No Yes, size met 1 Chevallier Sataloff Presence of invasive with sclerosis, fibrosis Presence of invasive Presence of treatment effect No Yes 1 No Yes +/- TE 2 UICC Product of 2 dimensions No No 3 Miller-Payne Presence of invasive,cellularity Yes No 3 # categories partial AJCC (y) Size of invasive No Yes, # Up to 4 MNPI Size of invasive, grade No Yes, # 3 Pinder % tumor remaining in breast Yes Yes, evidence of response RCB size in 2-dimensions, cellularity No Yes, # & size 4 3
68 RCB Prognostic information from degree of pathologic response? Propose RCB as continuous variable: primary tumor dimensions, residual cellularity of tumor bed, and axillary nodal burden Cohort of 382 patients; 2 different neoadjuvant chemo regimens Validation cohort of 141
69 Residual Cancer Burden (RCB) Tumor size, 2 dimensions % residual invasive cellularity Number of residual involved lymph node Size of largest metastasis
70 Illustrative examples of how residual tumor bed would be defined. Symmans W F et al. JCO 2007;25: by American Society of Clinical Oncology
71 Illustrative examples of how residual tumor bed would be defined. Symmans W F et al. JCO 2007;25: by American Society of Clinical Oncology
 Largest contiguous focus of invasive cancer (B) Use m for scattered foci One")
72 Provenzano Size reporting: difference RCB Largest area of residual invasive cancer (A, span) Does not need to be contiguous Two dimensions Favored by Provenzano AJCC 7th (ypt) Largest contiguous focus of invasive cancer (B) Use m for scattered foci One dimension

73 Residual tumor % cellularity Symmans W F et al. JCO 2007;25: by American Society of Clinical Oncology
74 Residual Cancer Burden (RCB) See website for instructions, helpful diagrams Symmans. Purists include all cancer cellularity, subtract DCIS (I just score invasive)
75 Post-chemo synopsis: example Focality of residual invasion: Span of residual invasion: Size of largest contiguous focus: Average cellularity of invasive carcinoma in tumor bed: Changes consistent with treatment effect: Present as scattered single cells/small clusters. Present as multiple residual foci/masses. Present as single contiguous residual mass/focus. cm x cm cm % Present Indeterminate No definite

76 RCB app/medcalc/index.cfm?pagena me=jsconvert3 Instructions and several helpful downloads (diagrams)
77 Residual LVI Should not be considered pcr Ensure ID & adequate sampling of tumor bed Most patients have other residual disease (LN) Confirm LVI, not DCIS, not retraction artifact (IHC) Don t include in residual invasive cancer size LVI at margin: separately comment Lack of data for current reporting recommendations LVI per Rosen/CAP: Outside the border of the invasive carcinoma Tumor emboli do not conform to the contours of space; invasive with retraction has exactly the same shape. Endothelial cell nuclei should be seen lining the space Lymphatics often adjacent to blood vessels Extensive LVI Provenzano: one or more foci in more than one block Stanford: 3 foci NCCN: not defined Colleoni: focal: one focus of in one tumor block only Moderate: more than one focus in one block Extensive: one or more foci in more than one tumor block

78 LVI with satellite LVI

79 LVI D2-40 Her2

80 Human Pathology. 2008;39: Endothelial markers CD31, CD34, ERG Lymphatic markers LYVE-1, D2-40 (podoplanin)
81


82 Tumor in lymphatics relatively resistant to chemotherapy (as is DCIS)

83 Retrospective study Predominanty AC-4 cycles 14% no residual cancer cells (pcr) 10% DCIS only (pcr) 4% pure IL tumor 3.4% predominantly IL 69% residual IDC IL 3-fold higher risk of death AJSP. 2009;33:256-63

84 Breast Cancer Res Treat 2016; 157: LVI was associated with poorer PFS and OS independent of post-surgical stage/nodal status No pathology review!
85 Axilla post-chemo: controversial Concern for: Lower SLN ID rate Higher false negative Pre-chemo clinical LN neg Pre-chemo LN positive Post-chemo Clinical LN neg Post-chemo Clinical LN neg Post-chemo Clinical LN positive SLN neg SLN & clip neg SLN or clip pos No ALND No ALND??? ALND???
86 Axillary Lymph Nodes Up to 40% of patients convert to node-negative May be more difficult to ID post chemo If so, submit fibrotic & perivascular areas in axilla Handle nodes with standard protocols 2mm gross sections Report with standard protocols #, sizes, ECE AND treatment effect/fibrosis

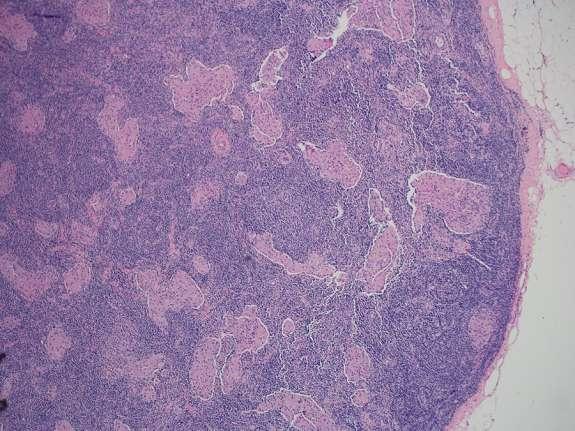
87 SLN: fibrosis, no residual CA

88 SLN: fibrosis, Exclude residual tumor cells
89 Post-chemo SLN: Granulomas?
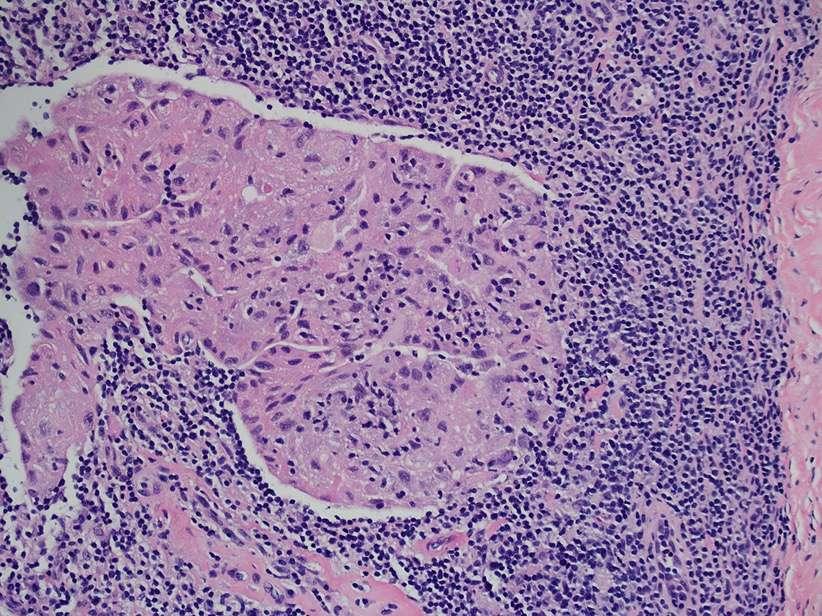

90
91 Post-chemo SLN Germinal center?
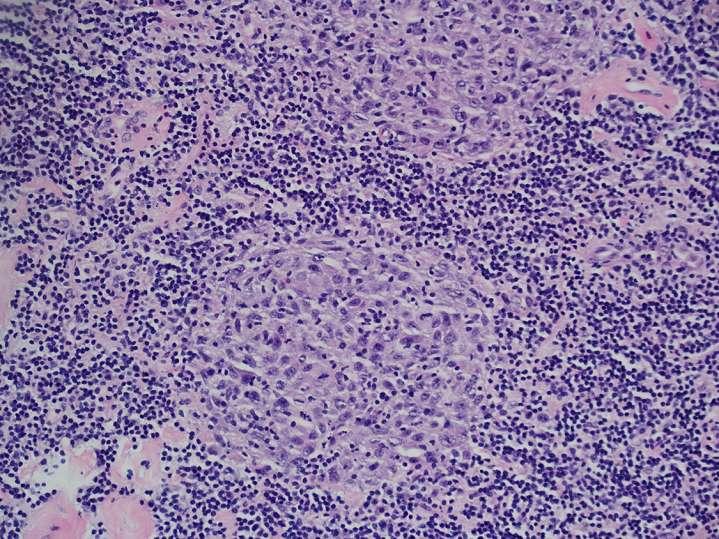

92 Post-chemo SLN Germinal center?

93 SLN FS Both foci cancer?

94 SLN FS How about now?

95 SLN permanents Right: CA Left: clip

96 SLN frozen section

97 SLN Permanents Top: tumor & fibrosis Bottom: clip


98 Another type of clip in SLN In our opinion, it is best to exercise caution.and maintain a low threshold for deferral of the final diagnosis to permanent sections in order to avoid false-positive & unecessary ALND. Brogi. Histopath. 2015;68:
99 LN reporting post chemo AJCC (ypn) Isolated tumor cells reported as node negative (ypn0itc) But not regarded as pcr WHO Isolated tumor cells node positive Provezano (opinion) Any residual disease in LN (mi, itc) should NOT be classified as pcr If no associated fibrosis, report as in adjuvant setting (ypn0itc) If fibrosis, likely macro- or micromet with response Describe in comment Measure entire area, including tumor cells & intervening stroma


100 Different pcr definitions Provenzano, Mod Pathol * Residual LVI? yptis vs. ypt0: --German study Lower DFS but same overall survival --MD Anderson, no difference
101 Complete Pathologic Response (pcr) pcr NOT pcr Insufficien t evidence Comment DCIS X x Definitions vary for DCIS LCIS X LVI X X LVI w/o LN disease very rare LN: macro- & micro- met LN: isolated tumor cells X X From Bossuyt Residual CA in LN worse prognosis irrespective of breast Mi & itc difference significance than adjuvant setting
102 Retesting of biomarkers Provenzano Discordance post-chemo Routine retest not ER: ~15% recommended PR: ~30% Positive ER/PR/Her2 core Her2: 6-9% Consider retest Due to: Negative or equivocal Technical failures result on core Intratumoral heterogeneity Outside biopsy/markers Changes due to therapy Heterogeneous or multiple (?selection) tumors Working group: 6/20 retest No response to therapy routinely



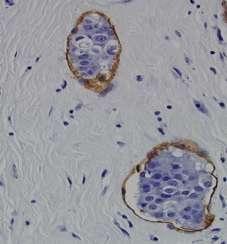
103 Left: Core biopsy Her2+ Right: Tumor bed with fibrosis, lymphs, histiocytes, no tumor
104 Steps to evaluate post-chemo breast 1. Recognize its post-chemo 2. Identify gross tumor/tumor bed & document size 3. Judiciously sample (map) 4. Assess residual size (largest contiguous and span), cellularity & standard parameters 5. Evaluate lymph nodes 6. Report as per local custom/mandates
105 Selected references Provenzano et al. Standardization of pathologic evaluation and reporting of postneoadjuvant specimens in clinical trials of breast cancer: recommendations from an international working group. Modern Pathology (2015) 28, Bossuyt et al. Recommendations for standardized pathological characterization of residual disease for neoadjuvant clinical trials of breast cancer by the BIG-NABCG collaboration. Annals of Oncology 26: , 2015 Lakhani et al eds. WHO Classification of Tumours of the Breast Symmans WF et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy.jco 2007;25: See also on-slide references
106 End
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy
 Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE
 Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Post Neoadjuvant therapy: issues in interpretation
 Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Problems in staging breast carcinoma
 Problems in staging breast carcinoma Primary systemic therapy (PST) of breast carcinoma pathologists tasks Dr. Janina Kulka, 2nd Department of Pathology, Semmelweis University Budapest Austro-Hungarian
Problems in staging breast carcinoma Primary systemic therapy (PST) of breast carcinoma pathologists tasks Dr. Janina Kulka, 2nd Department of Pathology, Semmelweis University Budapest Austro-Hungarian
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Breast Cancer. Pathologic Staging Updates Breast Cancer
 Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Evaluación de la respuesta patológica completa tras tratamiento neoadyuvante en cáncer de mama. José Palacios Calvo Servicio de Anatomía Patológica
 Evaluación de la respuesta patológica completa tras tratamiento neoadyuvante en cáncer de mama José Palacios Calvo Servicio de Anatomía Patológica E-Cadherin HER2 HER2 p63 Pathological Response Pathological
Evaluación de la respuesta patológica completa tras tratamiento neoadyuvante en cáncer de mama José Palacios Calvo Servicio de Anatomía Patológica E-Cadherin HER2 HER2 p63 Pathological Response Pathological
Savitri Krishnamurthy, MD 1
 EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
José Palacios Calvo Servicio de Anatomía Patológica
 Criterios de respuesta patológica con los distintos subtipos de cáncer de mama. Qué cambios se dan en el tejido postquimioterapia y qué dificultades se plantean para evaluar la respuesta? José Palacios
Criterios de respuesta patológica con los distintos subtipos de cáncer de mama. Qué cambios se dan en el tejido postquimioterapia y qué dificultades se plantean para evaluar la respuesta? José Palacios
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Handout for Dr Allison s Lectures on Grossing Breast Specimens:
 Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study
 [ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
[ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Sentinel Lymph Nodes for Breast Carcinoma: A Paradigm Shift. Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology
 Sentinel Lymph Nodes for Breast Carcinoma: A Paradigm Shift Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology Sentinel Lymph Nodes 2014 AJCC 2010 staging Micrometastases Occult metastases
Sentinel Lymph Nodes for Breast Carcinoma: A Paradigm Shift Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology Sentinel Lymph Nodes 2014 AJCC 2010 staging Micrometastases Occult metastases
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Overview of AJCC 8 th Staging in Pathologic Aspects
 Overview of AJCC 8 th Staging in Pathologic Aspects Jee Yeon KIM, M.D.,Ph.D. Department of Pathology, Pusan National University, College of Medicine, Pusan National University Yangsan Hospital, KOREA Major
Overview of AJCC 8 th Staging in Pathologic Aspects Jee Yeon KIM, M.D.,Ph.D. Department of Pathology, Pusan National University, College of Medicine, Pusan National University Yangsan Hospital, KOREA Major
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Sentinel Node Biopsy. Is There Any Role for Axillary Dissection? JCCNB Nov 20, Stephen B. Edge, MD
 Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
Targeting Surgery for Known Axillary Disease. Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center
 Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
RSNA, /radiol Appendix E1. Methods
 RSNA, 2016 10.1148/radiol.2016151097 Appendix E1 Methods US and Near-infrared Data Acquisition Four optical wavelengths (740 nm, 780 nm, 808 nm, and 830 nm) were used to sequentially deliver the light
RSNA, 2016 10.1148/radiol.2016151097 Appendix E1 Methods US and Near-infrared Data Acquisition Four optical wavelengths (740 nm, 780 nm, 808 nm, and 830 nm) were used to sequentially deliver the light
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer. Pathology. AGO e. V. in der DGGG e.v. sowie in der DKG e.v.
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
In Honour of Dr. Neera Patel
 In Honour of Dr. Neera Patel Residual Cancer Burden (RCB) vs Pathologic Complete Response (pcr) as an End-point W. Fraser Symmans, M.D. Professor of Pathology UT M.D. Anderson Cancer Center Pathologic
In Honour of Dr. Neera Patel Residual Cancer Burden (RCB) vs Pathologic Complete Response (pcr) as an End-point W. Fraser Symmans, M.D. Professor of Pathology UT M.D. Anderson Cancer Center Pathologic
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Descriptor Definition Author s notes TNM descriptors Required only if applicable; select all that apply multiple foci of invasive carcinoma
 S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
What to do after pcr in different subtypes?
 What to do after pcr in different subtypes? Luca Moscetti Breast Unit Università degli Studi di Modena e Reggio Emilia Policlinico di Modena, Italy Aims of neoadjuvant therapy in breast cancer Primary
What to do after pcr in different subtypes? Luca Moscetti Breast Unit Università degli Studi di Modena e Reggio Emilia Policlinico di Modena, Italy Aims of neoadjuvant therapy in breast cancer Primary
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY
 EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
Ultrasound or FNA for Predicting Node Positive in Breast Cancer
 Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
Completing the Puzzle AJCC TNM Staging Breast. Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017
 Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
BREAST PATHOLOGY GROSSING GUIDELINES
 THINGS TO CONSIDER: A. Please review ALL imaging and previous biopsies PRIOR to grossing any breast case. a. It may be helpful to draw out your own guide to assist when grossing B. Faxitron your breast
THINGS TO CONSIDER: A. Please review ALL imaging and previous biopsies PRIOR to grossing any breast case. a. It may be helpful to draw out your own guide to assist when grossing B. Faxitron your breast
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Question 1 A. ER-, PR-, HER+ B. ER+, PR+, HER2- C. ER-, PR+, HER2- D. ER-, PR-, HER2- E. ER-, PR+, HER2+
 Triple Negative Breast Cancer Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Question 1 The tumor depicted on the next slide
Triple Negative Breast Cancer Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Question 1 The tumor depicted on the next slide
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Disclosures 5/27/2012. Outline of Talk. Outline of Talk. When Is LCIS Clinically Significant? Classic LCIS. Classic LCIS
 When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
57th Annual HSCP Spring Symposium 4/15/2016
 Pathologic Assessment After Neoadjuvant Therapy W. Fraser Symmans, M.D. Professor of Pathology UT M.D. Anderson Cancer Center Disclosures Nuvera Biosciences, Inc. Co-founder and scientific advisor The
Pathologic Assessment After Neoadjuvant Therapy W. Fraser Symmans, M.D. Professor of Pathology UT M.D. Anderson Cancer Center Disclosures Nuvera Biosciences, Inc. Co-founder and scientific advisor The
PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT
 BREAST CANCER - PATHOLOGY ASSESSMENT") PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT Author: Dr Sally Ann Hales On behalf of the Breast and pathology CNGs Written: March 2005 Reviewed by CNG: June 2009 &
PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT Author: Dr Sally Ann Hales On behalf of the Breast and pathology CNGs Written: March 2005 Reviewed by CNG: June 2009 &
University Journal of Pre and Para Clinical Sciences
 ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA
 + NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA + INTRODUCTION + NEUROENDOCRINE FEATURES IN BREAST CARCINOMA Incidence of 2-5% Seen in various histopathological types of breast carcinoma Seen in both
+ NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA + INTRODUCTION + NEUROENDOCRINE FEATURES IN BREAST CARCINOMA Incidence of 2-5% Seen in various histopathological types of breast carcinoma Seen in both
Newly Diagnosed Breast Cancer: Preoperative Imaging and Localization
 Newly Diagnosed Breast Cancer: Preoperative Imaging and Localization Debra Monticciolo, MD Professor of Radiology Texas A&M University no disclosures Debra Monticciolo, MD Professor of Radiology Texas
Newly Diagnosed Breast Cancer: Preoperative Imaging and Localization Debra Monticciolo, MD Professor of Radiology Texas A&M University no disclosures Debra Monticciolo, MD Professor of Radiology Texas
Reporting of Breast Cancer Do s and Don ts
 Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
Pathology Report Patient Companion Guide
 Pathology Report Patient Companion Guide Breast Cancer - Understanding Your Pathology Report Pathology Reports can be overwhelming. They contain scientific terms that are unfamiliar and might be a bit
Pathology Report Patient Companion Guide Breast Cancer - Understanding Your Pathology Report Pathology Reports can be overwhelming. They contain scientific terms that are unfamiliar and might be a bit
ARROCase - April 2017
 ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Surgical Issues in Neoadjuvant Chemotherapy
 14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
 in Locally Advanced Breast Cancer") Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Financial Disclosure. Learning Objectives. None. To understand the clinical applicability of the NCDB Breast Cancer PUF
 Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!?
 CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
Seventh Edition Staging 2017 Breast
 Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Protocol for the Examination of Specimens from Patients with Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens from Patients with Invasive Carcinoma of the Breast Protocol applies to all invasive carcinomas of the breast, including ductal carcinoma in situ (DCIS) with microinvasion.
Protocol for the Examination of Specimens from Patients with Invasive Carcinoma of the Breast Protocol applies to all invasive carcinomas of the breast, including ductal carcinoma in situ (DCIS) with microinvasion.
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/55957 holds various files of this Leiden University dissertation Author: Dekker T.J.A. Title: Optimizing breast cancer survival models based on conventional
Cover Page The handle http://hdl.handle.net/1887/55957 holds various files of this Leiden University dissertation Author: Dekker T.J.A. Title: Optimizing breast cancer survival models based on conventional
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
What s new in breast pathology? Penny Barnes MD, FRCP(C) May 17, 2016
 May 17, 2016") What s new in breast pathology? Penny Barnes MD, FRCP(C) May 17, 2016 Outline IHC markers of metastatic carcinoma of breast origin Uses and limitations of e-cadherin IHC Breast neoplasms with limited metastatic
What s new in breast pathology? Penny Barnes MD, FRCP(C) May 17, 2016 Outline IHC markers of metastatic carcinoma of breast origin Uses and limitations of e-cadherin IHC Breast neoplasms with limited metastatic
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer
 Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Ines Buccimazza 16 TH UP CONTROVERSIES AND PROBLEMS IN SURGERY SYMPOSIUM
 BILATERAL MASTECTOMY IS NOT ROUTINELY JUSTIFIED IN PATIENTS WITH BILATERAL AXILLARY LYMPHADENOPATHY AND ONLY ONE DETECTABLE PRIMARY BREAST CANCER LESION SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department
BILATERAL MASTECTOMY IS NOT ROUTINELY JUSTIFIED IN PATIENTS WITH BILATERAL AXILLARY LYMPHADENOPATHY AND ONLY ONE DETECTABLE PRIMARY BREAST CANCER LESION SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
What is an Adequate Lumpectomy Margin in 2018?
 What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
Evaluation of the Axilla Post Z-0011 Trial New Paradigm
 Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Donna Plecha, MD 1, Shiyu Bai, BS 2, Helen Patterson 3, Cheryl Thompson, PhD 4, and Robert Shenk, MD 5
 Ann Surg Oncol DOI 10.1245/s10434-015-4527-y ORIGINAL ARTICLE BREAST ONCOLOGY Improving the Accuracy of Axillary Lymph Node Surgery in Breast Cancer with Ultrasound-Guided Wire Localization of Biopsy Proven
Ann Surg Oncol DOI 10.1245/s10434-015-4527-y ORIGINAL ARTICLE BREAST ONCOLOGY Improving the Accuracy of Axillary Lymph Node Surgery in Breast Cancer with Ultrasound-Guided Wire Localization of Biopsy Proven
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Gábor CSERNI. 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged
 Lymphocytes infiltrant la tumeur (TIL) sur micro-biopsies et pièces opératoires Quel impact clinique? Quels moyens de mise en évidence? Comment restituer les résultats? TILs - Clinical impact / Evaluation
Lymphocytes infiltrant la tumeur (TIL) sur micro-biopsies et pièces opératoires Quel impact clinique? Quels moyens de mise en évidence? Comment restituer les résultats? TILs - Clinical impact / Evaluation
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the