Colorectal Cancer Update Dr. Barb Melosky
|
|
|
- Evelyn Mathews
- 6 years ago
- Views:
Transcription


1 Colorectal Cancer Update 2017 Dr. Barb Melosky
2 Disclosure Research Support/P.I. Honoraria/Advisory Board Bayer Roche, Amgen, Bayer, Lilly
 Summarize the management of adjuvant and metastatic")
3 Objectives 1) Demonstrate knowledge of the epidemiology of colorectal cancer 2) Relate the importance of staging in treatment decisions 3) Summarize the management of adjuvant and metastatic therapies
4 Definitions

5 The Colorectum... Peritoneal Reflection
6 Side also matters! RIGHT LEFT

7 Colorectal Cancer Third most common cancer in men and women alike Lifetime probability 1 in 17
8 BC Incidence Rates - Colorectal Cancer Males Females
9 Survival with Colorectal Cancer BC Men BC Women
10 Colorectal Cancer (CRC) Sporadic (average risk) (65% 85%) Rare syndromes (<0.1%) HNPCC (5%) Family history (10% 30%) FAP (1%)

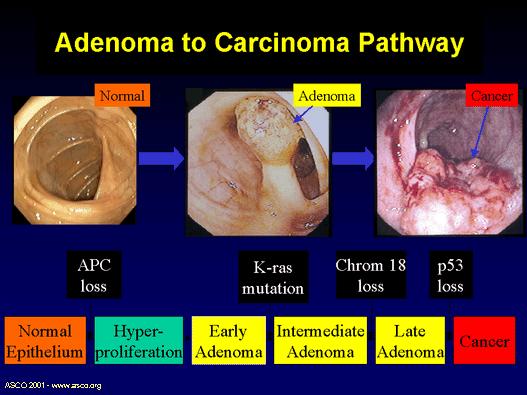
11 Who is at risk? Males=Females Risk increases with age Average age at diagnosis is yrs Industrialized nations Most cancers start as polyps - precancerous growths
12
13 Fecal Immunochemical Test
14 Colon Screening in BC Colon Check Pilot Program Funding from Ministry of Health in July 2008 Screening began in January 2009 in Penticton; Powell River (September 2009) and Vancouver core (April 2010) Approximately 20,000 screened Provincial Colon Screening Program Announced in November 2012 by Ministry of Health FIT covered by MSP on April 1, 2013 Program rolled out in province wide November 15,
15 Colon Screening Program Overview Target Population Men & Women age Screening Test Patient obtains requisition for screening from health care provider Fecal immunochemical test (FIT) for average risk Screening colonoscopy for higher than average risk FIT Specimens are returned to the lab for processing and reporting Results Results mailed to both patient and health care provider Reminder Mailed to patient and health care provider when time to rescreen
16 Colon Screening Policy Risk Average Risk Higher than Average Risk Screening Recommendation Fecal immunochemical test (FIT) is recommended every two years for people who do not have a personal history of adenomas or a significant family history of colon cancer. Colonoscopy is recommended every five years for people with at least one of the following: One first degree relative (mother, father, sister, brother, daughter or son) with colon cancer diagnosed under the age of 60; or, Two or more first degree relatives with colon cancer diagnosed at any age; or, A personal history of adenomas.
17 Early Program Statistics 45% of eligible patients who have had a FIT have been registered Over 91,000 FITs have been completed through the program Over 22,000 patients have been referred to colonoscopy to investigate an abnormal FIT or for primary screening in higher risk individuals.


18 Early Program Statistics Of the 1,483 patients with an abnormal FIT results that have had their colonoscopy and have pathology results available for review: 34% had a normal colonoscopy 16% had other pathology such as hyperplastic polyps 25% had low risk pre-cancerous polyps 24% had high risk pre-cancerous polyps 1% had cancer.
19 Staging

20 Staging 4 stages Stage I Cancer has grown thru the mucosa up to the muscular layer Stage II Cancer has spread into muscularis propria but not into lymph nodes Stage III Cancer has spread into lymph nodes but not to other parts of the body Stage IV Cancer has metastasized to distant organs
 (T 3 N 0 ) (T 4 N 0 ) (T 1 2 N 1 ) (T 3 4 N 1 ) (T any N 2 ) (M 1 ) O Connell et al.")
21 5-Year Relative Survival By AJCC Stage Percentage of Patients (%) Stage I Stage Stage Stage Stage Stage Stage IV IIA IIB IIIA IIIB IIIC (T 1 2 N 0 ) (T 3 N 0 ) (T 4 N 0 ) (T 1 2 N 1 ) (T 3 4 N 1 ) (T any N 2 ) (M 1 ) O Connell et al., 2004.
 N 0 No regional lymph node metastases N 1 Metastases in 1 3 regional lymph nodes N 2")
22 AJCCv6 TNM Staging Definitions AJCC v7 Effective Jan 2010 Primary tumor (T) T is Carcinoma in situ T 1 Tumor invades submucosa T 2 Tumor invades muscularis propria T 3 Tumor invades through muscularis propria or subserosa T 4 Tumor directly invades other organs or structures Regional lymph nodes (N) N 0 No regional lymph node metastases N 1 Metastases in 1 3 regional lymph nodes N 2 Metastases in 4 or more regional lymph nodes Distant metastases (M) M 0 No distant metastases M 1 Distant metastases T4a: perf. visceral peritoneum T4b: invasion of organs N1a: 1 N+ N1b: 2-3 N+ AJCC = American Joint Committee on Cancer. National Comprehensive Cancer Network (NCCN), 2008; Greene et al., N2a: 4-6 N+ N2b: >7 N+
23 AJCC v7 Stage II Stage III Gunderson et al, JCO 2009


24 AJCC v7 Stage II Stage III Gunderson et al, JCO 2009
25 Adjuvant Treatment for Colon Cancer

26 CRC Demographics and Presentation 12.2% stage I 18.6% stage IV 24.5% stage II 32.6% stage III
27 The Evolution of Adjuvant Therapy FU/Levamisole 12 months >observation FU/LV 12 months > than observation FU/LV > than 5-FU/Levamisole months = 12 months FOLFOX > 5FU/LV 2004 Capecitabine = 5FU/LV No role for Irinotecan confirmed CAPOX better that 5FU/LV 2010 Role of biological agents negative Avastin /Cetuximab
28 Moertel N Engl J Med 1990 Intergroup FU + Levamisole Stage III Colon n = 930 Levamisole No Adjuvant Rx 52 weeks
29 Intergroup 0035 OS 16% absolute reduction Moertel, C. G. et. al. Ann Intern Med 1995;122:

30 BCCA Adjuvant Chemotherapy Stage lll: N1+ FOLFOX / CAPOX Capecitabine: Elderly or Unfit Stage ll High Risk T4: FOLFOX Low Risk: Capecitabine If treatment deemed necessary / Rule out MSI
31 MOSAIC: Study Design n=2246 Completely resected colon cancer Stage II, 40%; Stage III, 60% (n=1123) R (n=1123) FOLFOX4 (LV5FU2 + oxaliplatin 85 mg/m²) LV5FU2
32 MOSAIC 6-yr DFS: ASCO p= % Probability Events FOLFOX4 304/1123 (27.1%) LV5FU2 360/1123 (32.1%) HR [95% CI]: 0.80 [ ] FOLFOX4 LV5FU Disease-free survival (months)
33 Disease-free Survival: Stage II and Stage III Patients 1.0 Probability p=0.258 p= % 7.5% HR [95% CI] p-value Stage II 0.84 [ ] Stage III 0.78 [ ] FOLFOX4 stage II LV5FU2 stage II FOLFOX4 stage III LV5FU2 stage III Months
34 XELOXA Trial 1.0 CAPOX 5-FU/LV CAPOX (6 months) capecitabine 1000mg/m 2 bid d1 14 oxaliplatin130mg/m 2 d HR=0.80 (95% CI: ) p= Years
35 BCCA Adjuvant Chemotherapy Stage lll: N1+ FOLFOX/ CAPOX Capecitabine: Elderly or Unfit Stage ll High Risk T4: FOLFOX Low Risk: Capecitabine if treatment deemed necessary (R/O MSI)

36 X-ACT: Unfit CAPECITABINE 1 250mg/m 2 BID, d1 14, q21d

37 BCCA Adjuvant Chemotherapy Stage lll: N1+ FOLFOX CAPOX (XELOX): Funding October Capecitabine: Elderly or Unfit Stage ll High Risk T4: FOLFOX Low Risk: Capecitabine if treatment deemed necessary (R/O MSI)
38 MOSAIC: DFS High-risk Stage II Probability FOLFOX4 n=286 LV5FU2 n=290 HR: 0.74; (CI): % ASCO criteria T4 tumour with adherence to or invasion of local organs Bowel obstruction at presentation Perforation at tumour site Poorly differentiated tumour histology 0 6 Peritumoural lymphovascular involvement Questionable surgical Disease-free margin survival (months) <12 nodes examined

39 Microsatelite Instability - Colon cancer Tumors: Poorly differentiated, Signet-ring-cell, Lymphocytic infiltration, near diploid Right sided, Female, Early stage, Better prognosis Malignant cells resistant to 5-FU 1,2 1 Carethers, 1999; 2 Arnold 2003


40 Overall Survival stage II MSI Treatment 5FU N = 55 N = 47 Untreated 93% Treated 75% 5 yr OS HR: 3.15 ( ) p=0.03

41 What happened to the biologics? EGFR Monoclonal Antibodies Panitumumab, Cetuximab VEGF Monoclonal Antibodies Bevacizumab ALL NEGATIVE!!!
42 Future in Adjuvant? New drugs?
43 IDEA International Duration Evaluation in Adjuvant Worldwide effort to address Duration 6 vs 3 months R 3 mos 6 mos Group-specific question e.g. +/- BEV +/- Celecoxib +/- Agents X/Y/Z FOLFOX or XELOX

44 Adjuvant Treatment for Rectal Cancer


45




46 Radiation and Surgery Surgery vs Radiation and Surgery 5 Y OS 62 vs 63% Pre-op 46% reduced LRR Post-op 37% reduced LRR Total Mesorectal Excision established as the superior surgery 1970s 1980s 1990s 2000s 2001: Radiation reduces Loco Regional Relapse (LRR) even when TME is done. CCCG Lancet 2001; Kapitejn NEJM 2001

47 Radiation Preoperative preferred: Short or Long Course Short: The tumour doesn t need to be smaller 5 days treatment followed within a week by surgery. Chemotherapy after if necessary Long: The tumour needs to be made smaller before surgery: 5 radiation treatments/week for 5 weeks with capecitabine followed 4-6 weeks later by surgery Chemotherapy after if necessary
48 Rectal Cancer : Short Course XRT Radiation 1 week 6-8 weeks Chemo Surgery N: Pathology N1 FOLFOX 6 months N0 Cape 6 months 1 week


49 Rectal Cancer: Long Course Chemoradiation 5 weeks 6 weeks 6-8 weeks Chemo Surgery N: Imaging N1 FOLFOX 4 months N0 Cape 4 months

50 Surveillance CEA every 3 months for 3 yrs and then every 6 months for another 2 yrs = 5 years Imaging chest abdomen and pelvis yearly for 5 years Why?.. Liver/ lung lesions may be cured with surgery

51 Regional Treatment Strategies 5 year survival 30-35% following resection of oligo- hepatic metastases
52 Metastatic Colorectal Carcinoma

53 Lines of Therapy Today BCCA First Line FOLFIRI + Bevacizumab Capecitabine PS 2 Second Line FOLFOX Third Line Ras WT: Panitumumab or Cetuximab

54 5FU the Drug of Choice for over 60 Years! Nature, March 30, 1957
55 First Line FOLFOX or FOLFIRI?
56
57
58
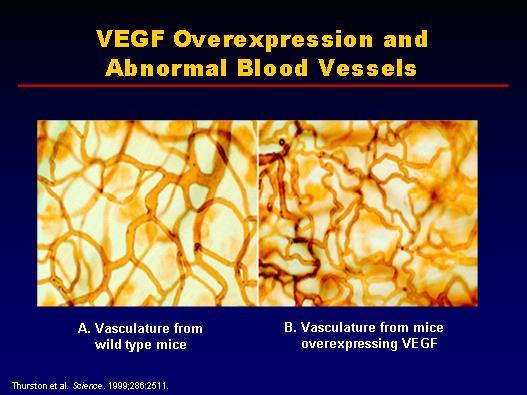
59 Why add the bevacizumab?
60
61 IFL and Avastin: OS 1.0 HR=0.66 (95% CI: ) p<0.001 Estimated probability IFL + Avastin IFL + placebo Months ITT population Hurwitz et al. NEJM 2004
62 66 PFS HR = 0.83 [97.5% CI ] (ITT) p = PFS estimate Months FOLFOX+placebo/XELOX+placebo N=701; 547 events FOLFOX+bevacizumab/XELOX+bevacizumab N=699; 513 events Saltz et al., JCO 2008

63 How long do you treat for in first line? Drug Holidays or Treatment to Progression?
64 OPTIMOX 2 6 FOLFOX FOLFOX 5FU/LV 6 FOLFOX FOLFOX Maindrault-Goebel et al, ASCO 2006
65 OPTIMOX 2: OS Maintenance P = CFI 26 months 19 months 0. 4 OS 7 months 0. 2 Lesson from OPTIMOX2: 0. 0 Complete chemo free intervals may not be ideal months Maindrault-Goebel et al, ASCO 2007
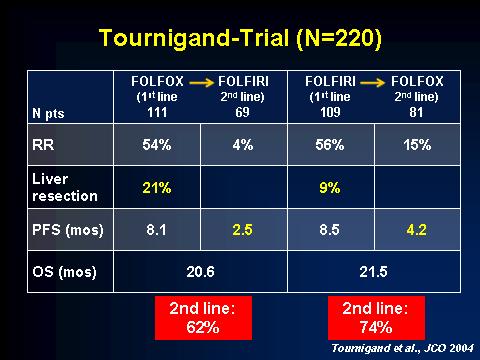
66 Second Line? What ever you didn t use first line
 FOLFOXIRI CAIRO 2007")
67 Concept of All-3-Drugs 11 Phase III Trials, 5768 Patients Median OS (mo) First-Line Therapy Infusional 5-FU/LV + irinotecan Infusional 5-FU/LV + oxaliplatin Bolus 5-FU/LV + irinotecan Irinotecan + oxaliplatin Bolus 5-FU/LV LV5FU Patients with 3 drugs (%) FOLFOXIRI CAIRO 2007

68 Third LIne Ras Wild Type: EGFR Inhibitors
69 Panitumumab Cetuximab EGFR (Epidermal Growth Factor Receptor) Cell Membrane TK P TK P STATs PI3 kinase KRas Akt P PTEN MAPK/ERK Angiogenesis Apoptosis Proliferation Invasion & metastasis
70 KRAS WT THIRD LINE

71 KRAS WT THIRD LINE PRESENTATION NAME AND/OR DESCRIPTION
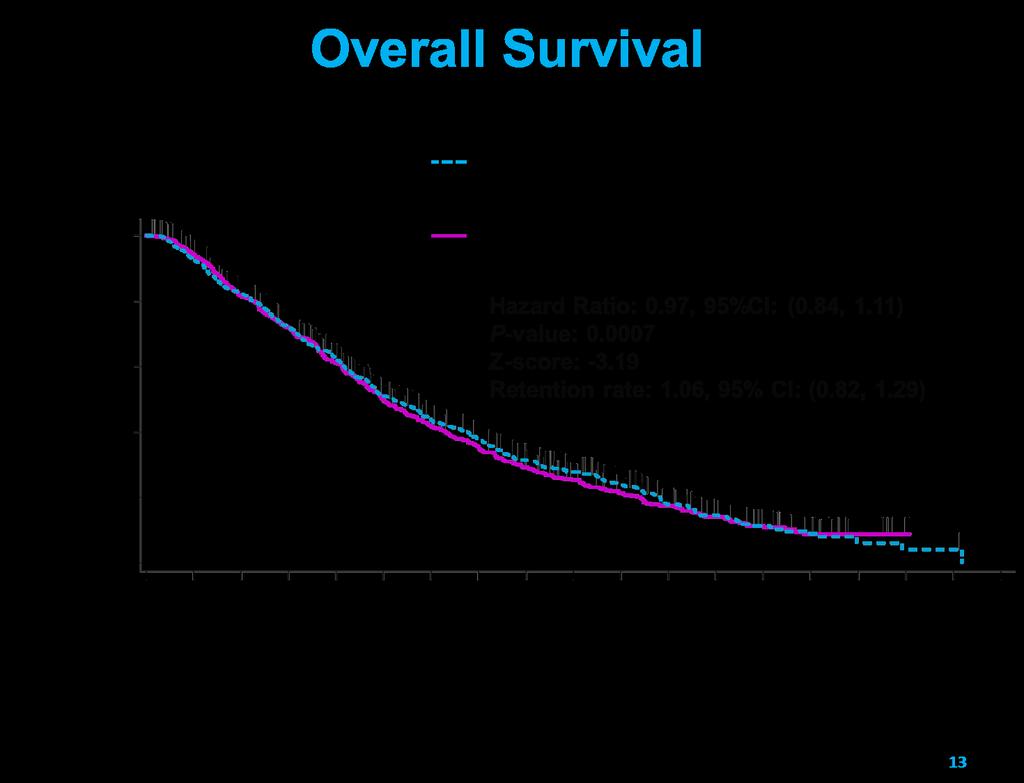
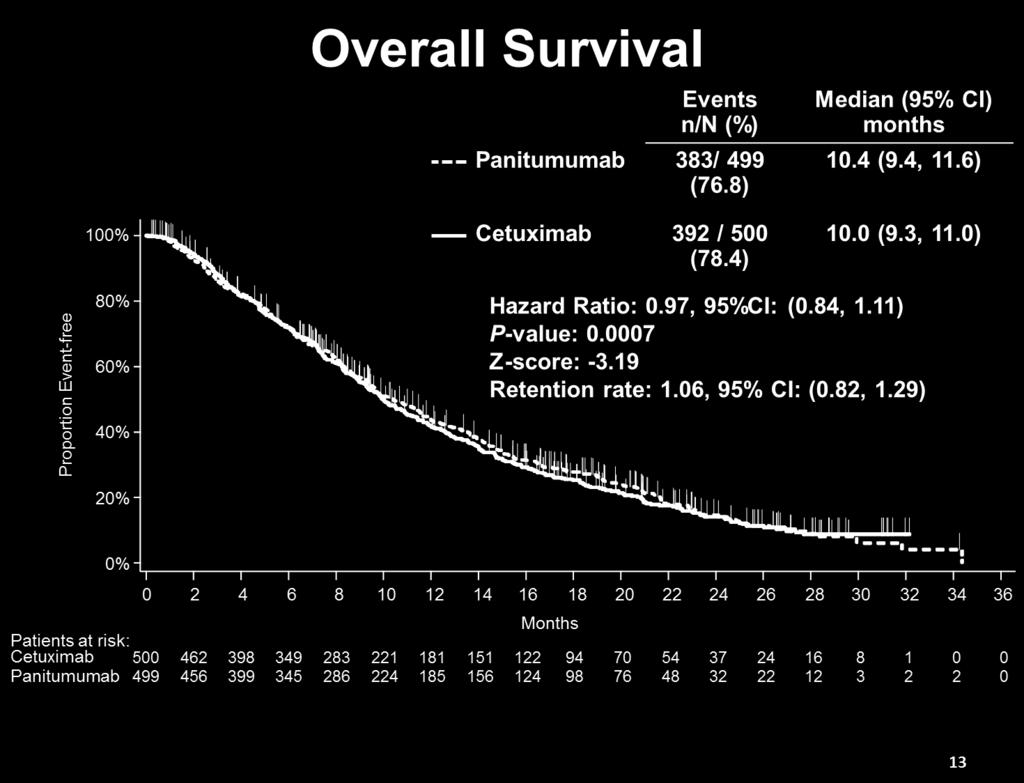
72 ASPECTT
73 BIOMARKER KRAS mcrc: Approximately 60% KS WT vs 40% KRAS MT KRAS exon 2 wild-type subset EXON 2 KRAS mt
74 Other RAS Mutations KRAS EXON 1 EXON 2 EXON 3 EXON NRAS EXON 1 EXON 2 EXON 3 EXON

75 BEST BIOLOGIC FIRST LINE? FIRE VEGF MoA EGFR MoA
76 FIRE 3 Previously untreated patients with mcrc WT KRAS N= 592 R FOLFIRI and bevacizumab N=295 FOLFIRI, and cetuximab N=297 PRIMARY OBJECTIVE : RR by RECIST
![FIRE 3 [TITLE]](/docs-images/78/76933348/images/77-0.jpg "RR ITT: 62%")

77 FIRE 3 [TITLE] RR ITT: 62% Cetuximab vs 58% Bevacizumab P=.183

78 CALGB/SWOG 80405: <br /> FINAL DESIGN
 Presented By Alan Venook at 2014 ASCO Annual")
79 CALGB/SWOG 80405: Progression-Free Survival<br />(Investigator Determined) Presented By Alan Venook at 2014 ASCO Annual Meeting
80 Anything New? New drugs: Regorafenib



81 Regorafenib inhibits multiple cell-signaling kinases: Angiogenic VEGFR1 3, TIE2 Stromal PDGFR-β, FGFR Oncogenic KIT, PDGFR, RET Regorafenib Wilhelm SM et al. Int J Cancer 2011





82 CORRECT mcrc after standard therapy R A N D O M I Z AT Regorafenib + BSC 160 mg orally once daily 3 weeks on, 1 week off 2 : 1 Primary Endpoint: OS I O N Placebo + BSC 3 weeks on, 1 week off

83 Overall survival Survival distribution function Placebo N=255 Regorafenib N=505 Regorafenib Median 6.4 mos 5.0 mos Hazard ratio: 0.77 p-value: Days from randomization 6 weeks Placebo

84 Response Best response, % Regorafenib N=505 Placebo N=255 Complete response 0 0 Partial response Stable disease Progressive disease Disease control rate, %* *DCR = PR + SD; p<
85 Anything New? MSI Tumors: IO works!!

86 Histology of MSI Cancers Presented By Luis Diaz at 2017 Gastrointestinal Cancers Symposium
87
88 Pembrolizumab 100 MMR-proficient CRC % Change from Baseline SLD MSI colon MMR-deficient CRC MMR-deficient non-crc -100 Le DT, et al. J Clin Oncol. 2015;33(Suppl): Abstract LBA100.
89 PFS OS
90 Left vs Right Anything New?
91 Yes, Side does matter RIGHT LEFT
92 Yes, Side does matter MSI-H BRAF-mut KRAS wt HER2+ AREG/EREG

93 OS by sidedness: CALGB and FIRE FIRE-3 RIGHT SIDE: BEV DID BETTER Venook, ASCO 2016

94 OS by sidedness: CALGB and FIRE FIRE-3 LEFT SIDE: CETUX DID BETTER Venook, ASCO 2016
95 BEST BIOLOGIC FIRST LINE? COMING SOON VEGF MoA RIGHT EGFR MoA LEFT (RAS WT)
96 Conclusion

97 BCCA Adjuvant Chemotherapy Stage lll: N1+ FOLFOX/ CAPOX Capecitabine: Elderly or Unfit Stage ll High Risk T4: FOLFOX Low Risk: Capecitabine if treatment deemed necessary (R/O MSI)
98 BCCA Metastatic Colorectal Carcinoma First Line FOLFIRI + Bevacizumab Capecitabine PS 2 Second Line FOLFOX or FOLFIRI Third Line Ras WT: Panitumumab or Cetuximab

99 BCCA Metastatic Colorectal Carcinoma Regorafenib: Not approved MSI Tumors: Find a trial Anti- EGFR vs VEGF RAS M+: Anti EGFR does not work Pretty soon: Left RAS WT: Anti- EGFR Right : Anti- VEGF
100 9 months Slide months Presented By Alan Venook at 2014 ASCO Annual Meeting
101 Thank you
What s New? Dr. Barbara Melosky
 Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Disclosures. Clinical and molecular features to guide adjuvant therapy. Personalized Medicine - Decision Tools -
 Disclosures Clinical and molecular features to guide adjuvant therapy Daniel Sargent Professor of Biostatistics & Oncology Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis
Disclosures Clinical and molecular features to guide adjuvant therapy Daniel Sargent Professor of Biostatistics & Oncology Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Medical Therapy of Colorectal Cancer in the Biomarker Era
 Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer
 THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer SANJAY GOEL, M.D., M.S. PROFESSOR OF MEDICINE ALBERT EINSTEIN COLLEGE OF MEDICINE MONTEFIORE MEDICAL CENTER DEPT. OF ONCOLOGY JUN 22,
THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer SANJAY GOEL, M.D., M.S. PROFESSOR OF MEDICINE ALBERT EINSTEIN COLLEGE OF MEDICINE MONTEFIORE MEDICAL CENTER DEPT. OF ONCOLOGY JUN 22,
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
Toxicity by Age Group. Old Factor 1: Age. Disclosures. Predicting survival in metastatic colorectal cancer. Personalized Medicine - Decision Tools -
 Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
First line treatment in metastatic colorectal cancer
 First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
High risk stage II colon cancer
 High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
COLORECTAL CANCER. Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program
 COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Adjuvant treatment Colon Cancer
 ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
Advances in Chemotherapy of Colorectal Cancer
 Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
JY Douillard MD, PhD Professor of Medical Oncology
 Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER
 THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER Cathy Eng, M.D., F.A.C.P. Associate Professor Associate Medical Director, Colorectal Center Dept of GI Medical Oncology November 5, 2010
THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER Cathy Eng, M.D., F.A.C.P. Associate Professor Associate Medical Director, Colorectal Center Dept of GI Medical Oncology November 5, 2010
Treatment of Advanced Colorectal Cancer
 Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage. Dr Lee-Ann Jones
 Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
A Brief Overview of Screening and Management of Colorectal Cancer
 A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
Ashita Waterston Beatson West of Scotland Cancer Centre
 Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms
 21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
Progress towards an individualized approach to therapy: colorectal cancer
 Progress towards an individualized approach to therapy: colorectal cancer Alan P. Venook, M.D. University of California, SF GIST: PET change after 4 weeks imatinib Multiple liver and upper abdominal 18
Progress towards an individualized approach to therapy: colorectal cancer Alan P. Venook, M.D. University of California, SF GIST: PET change after 4 weeks imatinib Multiple liver and upper abdominal 18
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist
 ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES
 CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
CHEMOTHERAPY FOR COLON CANCER OUTLINE OF TODAY S TALK. Colon Cancer Epidemiology 11/6/2012 GATRA/GCCR FALL CONFERENCE NOVEMBER 14 16, 2012
 CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
Where are we in 2013?
 The Use of Gene Profile Testing in the Adjuvant Therapy of Stages II & III Colon Cancer: Where are we in 2013? Howard S. Hochster, MD Professor of Medicine, Yale School of Medicine Associate Director,
The Use of Gene Profile Testing in the Adjuvant Therapy of Stages II & III Colon Cancer: Where are we in 2013? Howard S. Hochster, MD Professor of Medicine, Yale School of Medicine Associate Director,
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer. Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center
 Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany
 MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory boards for AMGEN, ROCHE I Speaker
MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory boards for AMGEN, ROCHE I Speaker
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression
 Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Microsatellite instability and other molecular markers: how useful are they?
 Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
MANAGEMENT OF ADVANCED COLORECTAL CANCER
 MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer -
 International Society of Geriatric Oncology Lisbon October 23 rd 25t h 2014 Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer - Claus-Henning Köhne Klinik für Onkologie
International Society of Geriatric Oncology Lisbon October 23 rd 25t h 2014 Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer - Claus-Henning Köhne Klinik für Onkologie
2014/2015 FCDS Educational Webcast Series
 2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
Adjuvant therapies for large bowel cancer Wasantha Rathnayake, MD
 LEADING ARTICLE Adjuvant therapies for large bowel cancer Wasantha Rathnayake, MD Consultant Clinical Oncologist, National Cancer Institute, Maharagama, Sri Lanka. Key words: Large bowel; Cancer; Adjuvant
LEADING ARTICLE Adjuvant therapies for large bowel cancer Wasantha Rathnayake, MD Consultant Clinical Oncologist, National Cancer Institute, Maharagama, Sri Lanka. Key words: Large bowel; Cancer; Adjuvant
Disclosure. Nothing to Disclose Will not be discussing off label use of any of the medications
 Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Colon, Rectum, and Appendix
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix. Presentation Outline. Overview Tumor Characteristics
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
ADVANCES IN COLON CANCER
 ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
THE BEST OF ESMO 2016
 THE BEST OF ESMO 2016 Colorectal cancer Pr Julien TAIEB, Sorbonne Paris Cité and Paris Descartes University Georges Pompidou European Hospital Paris, FRANCE esmo.org DISCLOSURES JT has received research
THE BEST OF ESMO 2016 Colorectal cancer Pr Julien TAIEB, Sorbonne Paris Cité and Paris Descartes University Georges Pompidou European Hospital Paris, FRANCE esmo.org DISCLOSURES JT has received research
Jonathan Dickinson, LCL Xeloda
 Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Fighting a Smarter War On Colon Cancer:
 Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC
 Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
The left versus right colon cancer story What is the truth?
 The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
Incorporating biologics in the management of older patients with metastatic colorectal cancer
 Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
AIOM GIOVANI Perugia, Luglio 2017
 AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study
 Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study Henaine AM; Chahine G; Massoud M; Salameh P; Awada S; Lahoud N; El
Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study Henaine AM; Chahine G; Massoud M; Salameh P; Awada S; Lahoud N; El
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT?
 DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
Progress and Challenges in the Adjuvant Treatment of Stage II & III Colon Cancer
 Progress and Challenges in the Adjuvant Treatment of Stage II & III Colon Cancer Professor Eva Segelov Monash Health and Monash University (with thanks to A/P Jeremy Shapiro) Melbourne, Australia Apr 2017
Progress and Challenges in the Adjuvant Treatment of Stage II & III Colon Cancer Professor Eva Segelov Monash Health and Monash University (with thanks to A/P Jeremy Shapiro) Melbourne, Australia Apr 2017
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
The role of Maintenance treatment Appropriate endpoints according to ESMO consensus
 ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
Introduction. Why Do MSI/MMR Analysis?
 Clinical Significance Of MSI, KRAS, & EGFR Pathway In Colorectal Carcinoma UCSF & Stanford Current Issues In Anatomic Pathology Introduction Microsatellite instability and mismatch repair protein deficiency
Clinical Significance Of MSI, KRAS, & EGFR Pathway In Colorectal Carcinoma UCSF & Stanford Current Issues In Anatomic Pathology Introduction Microsatellite instability and mismatch repair protein deficiency
Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical modulation, Oral fluoropyrimidines, Developmentof combination chemotherapy
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
Metastatic Colorectal Cancer. Update 2015
 Metastatic Colorectal Cancer Update 2015 A/Prof Jeremy Shapiro GI Medical Oncologist Cabrini Hospital, Melbourne 1 Not all pts with metastatic CRC are equal 1 st consideration can patient be cured by resection
Metastatic Colorectal Cancer Update 2015 A/Prof Jeremy Shapiro GI Medical Oncologist Cabrini Hospital, Melbourne 1 Not all pts with metastatic CRC are equal 1 st consideration can patient be cured by resection
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Thoracic and head/neck oncology new developments
 Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Colorectal Cancer Therapy and Associated Toxicity
 Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
Strategy for the treatment of metastatic CRC through the lines
 Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
Understanding predictive and prognostic markers
 Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
Recent Advances in Gastrointestinal Cancers
 Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO. CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS?
 INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
Targeted therapies in colorectal cancer: the dos, don ts, and future directions
 Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
Heather Wakelee, M.D.
 Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Sponsored by Educational Grant Support from Adjuvant (Post-Operative) Lung Cancer Chemotherapy Heather Wakelee, M.D.
Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Sponsored by Educational Grant Support from Adjuvant (Post-Operative) Lung Cancer Chemotherapy Heather Wakelee, M.D.
Current Status of Adjuvant Therapy for Colorectal Cancer
 Review Article [1] May 01, 2004 By Michael J. O connell, MD [2] Adjuvant therapy with chemotherapy and/or radiation therapy in addition to surgery improves outcome for patients with high-risk carcinomas
Review Article [1] May 01, 2004 By Michael J. O connell, MD [2] Adjuvant therapy with chemotherapy and/or radiation therapy in addition to surgery improves outcome for patients with high-risk carcinomas
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER
 RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
Colorectal Cancer Treatment
 Colorectal Cancer Treatment Syed Husain, MD, FACS, FASCRS Assistant Professor of Surgery Department of Surgery Division of Colon and Rectal Surgery The Ohio State University Wexner Medical Center Introduction
Colorectal Cancer Treatment Syed Husain, MD, FACS, FASCRS Assistant Professor of Surgery Department of Surgery Division of Colon and Rectal Surgery The Ohio State University Wexner Medical Center Introduction
Supplementary Online Content
 Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced
Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced