Metastatic Colorectal Cancer. Update 2015
|
|
|
- Arron Black
- 5 years ago
- Views:
Transcription

1 Metastatic Colorectal Cancer Update 2015 A/Prof Jeremy Shapiro GI Medical Oncologist Cabrini Hospital, Melbourne 1

2 Not all pts with metastatic CRC are equal
3 1 st consideration can patient be cured by resection of metasatic disease? 3
4 Metastatic colorectal cancer Unresectable 66% 48% Resectable --- Best supportive care --- 5FU --- Resectable liver mets % Colon Cancer Collaborative Group, BMJ 2000 and Adam, Ann Surg 2004
5 Liver resection can cure some pts Refs Colon Ca Collab. Group, BMJ 2000 / Tournigand, JCO 2004 / Adam, Ann Surg % --- BSC FU --- FOLFIRI/FOLFOX6 --- FOLFOX6/FOLFIRI --- resectable 40 30% years
6 Is metastatic disease resectable? Full CT staging, PET +/- liver MRI And if it is, is pt fit enough for surgery? sometimes, I can make the call. 20 % pts suitable, 50 % clearly not Perhaps 30% or so unsure => Best to assess all pts with liver limited disease in MDT.. NB Bilobar disease, not necessarily a contra-indication
7 2 nd consideration understanding what you can/ can t do with chemo
8
9 Pts diagnosed with met CRC in can t be cured with chemo alone - can expect (on average) to live about 2.5 years % chance of living beyond 5 years
10 Managing Colorectal Cancer in the clinic Traditional Same treatment for all Limited options Treating doctor only 2015 Individualised treatment plan Large treatment menu Multi-disciplinary care
11 CRC Menu Chemotherapy 5FU Capecitabine Raltitrexed S1 Oxaliplatin Irinotecan Mitomycin C Primary tumour Leave in situ Stent Surgery Radiotherapy Biologic agents Bevacizumab Cetuximab Panitumumab Aflibercept Ramucirumab Supportive Symptom control Palliative services Clinical trial Surgery Liver Lung Peritonectomy Liver directed therapy Sirt RFA DC beads FUDR (HAI) Biomarkers
12 All pts suitable for Rx should have a RAS test at diagnosis of metastases (altho RAS test will not necessarily determine initial Rx..)
13 RAS a new predictive biomarker -a gene that encodes one of the proteins in the epidermal growth factor receptor (EGFR) signaling pathway -important in the development and progression of cancer - 40% CRC pts have a KRAS exon 2 mutation and don t benefit from EGFR-ab Rx - ** another 10-15% have a NRAS or rare type of KRAS mutation => Near perfect negative predictor of resistance
 ~40% Douillard JY. ASCO 2013. Abstract 3620; Oliner KS. ASCO 2013. Abstract 3511.")
14 Distribution of mutations in mcrc KRAS mt (non exon 2 KRAS mt) & NRAS mt ~10% RAS wt ~50% KRAS mt (exon 2) ~40% Douillard JY. ASCO Abstract 3620; Oliner KS. ASCO Abstract 3511.
15 KRAS testing A revolution in the clinical care of met CRC pts % met CRC pts being KRAS tested in USA (n=1188) Before EGFR inhibitor treatment At any time during clinical care Webster J Cancer Epidemiol Biomarkers Prev 2013
16 Which chemotherapy? Disease factors Curative v Non-curative Symptoms Burden of metastatic disease Clinical course - ie pace of disease
17 Which chemotherapy? Patient factors Age Performance Status Co-morbidities Patient wishes
18 Which chemo? Cure Aggressive Rx Rapid PD / Significant Sx Aggressive Rx No cure / no rapid PD or signif Sx (majority) Can use milder approaches
19 First line therapy



20 systemic therapy cards Additional Australian (PBS) Rules: - Can substitute X card in place of F - Must play B at start or not at all - A can not be played at all - Can only play C after O or I has been played - Only some players are given the C or P cards and they are interchangeable - New cards cannot be used without lengthy application to rules committees
21 First line therapy Non-intensive initial approach (suitable for > 50% but in practice used less often)
 irinotecan capecitabine + oxaliplatin 0.2 Sequential (Arm A) p = 0.")
22 Overall survival CAIRO study: median overall survival 1.0 sequential Rx 16.3 m ( ) combination Rx 17.4 m ( ) st line sequential capecitabine Randomisation combination capecitabine + irinotecan nd line Combination (Arm B) irinotecan capecitabine + oxaliplatin 0.2 Sequential (Arm A) p = rd line capecitabine + oxaliplatin n = Months from randomisation Koopman et al. Lancet 2007
23 Oral Capecitabine 5FU pro-drug, with equivalent efficacy usually well tolerated Patients like the freedom! (no IV / can travel) still need regular monitoring Especially in initial stages as dose is adjusted Side effects slowly accumulate with each course Dose delays between cycles often required Compliance issues
24 Cape + Bev better than Cape Cape best option for most monotherapy pts can still use IV 5FU schedules if you want Concerned re compliance Unable to swallow/absorb talblets Troublesome HF syndrome adding Bev increases RR, PFS and possibly OS

25 AVEX Phase III Study Design Patients Previously untreated mcrc Age 70 yr Adjuvant chemo if >6 mo prior Not optimal candidates for irinotecan or oxaliplatin No cardiovascular disease, recent aspirin/nsaid use, or full-dose anticoagulants or thrombolytics N=280 Capecitabine 1000 mg/m2 BID days Bev 7.5 mg/kg day 1 every 3 weeks 1:1 Randomization Capecitabine 1000 mg/m2 BID days 1-14 every 3 weeks Treat to progression Cunningham et al: The Lancet Oncology, Volume 14, Issue 11, Pages , October 2013

26 AVEX: Progression-Free Survival Cunningham et al: The Lancet Oncology, Volume 14, Issue 11, Pages , October 2013
27 AVEX: Outcomes by Age years years 80 years Cape + Bev (n=55) Cape (n=46) Cape + Bev (n=57) Cape (n=66) Cape + Bev (n=28) Cape (n=28) Median PFS, mos PFS HR (P value) 0.52 (p<0.001) 0.60 (p=0.016) 0.36 (p=0.003) Median OS, mos OS HR (P value) 0.91 (p=0.55) 0.79 (p=0.37) 0.62 (p=0.24) Best ORR, % ORR P value Grade 3 AEs, % Saunders M. ESMO Abstract O-0030.
28 Proportion not progressed AGITG MAX: Bev increases PFS Capecitabine + Bevacizumab + Mitomycin C Median PFS C: 5.7 months CB: 8.5 months CBM: 8.4 months 0.6 Capecitabine Capecitabine + Bevacizumab Hazard ratios C vs CB: 0.63, P<0.001 C vs CBM: 0.59, P< Months from randomisation 24 Tebbutt, MAX AGITG study ESMO 2009
29 First line therapy More intensive initial approach
30 Oxaliplatin and Irinotecan are the most active drugs, and are similar in efficacy (when used optimally in 1st-line advanced disease)
31 Equivalent survival if both drugs combined with infusional 5FU in 1 st line Colucci et al. JCO Aug 2005 Tournigand et al. JCO 2004 RR 31% v 34% (NS) RR (1 st line) 56% v 54% (NS) TTP 7 m v 7 m (NS) TTP (1 st line) 8 m v 8.5 m (NS) Med survival 14 m v 15 m (NS) Med survival 21.5 m v 20.6 m (NS)
32 Capecitabine can replace 5FU doublet backbone Overall Survival XELOX v FOLFOX Cassidy ASCO 2007
33 order not important, as long as all the active drugs are used
34 Best survival if exposed to all active agents Median OS (mos) p = Patients With Three Drugs (%) 11 phase III trials: 5,768 patients OS (mos) = (% 3 drugs x 0.1); R^2 =.85 1st-line therapy Infusional 5-FU/LV + irinotecan Infusional 5-FU/LV + oxaliplatin Bolus 5-FU/LV + irinotecan Irinotecan + oxaliplatin Bolus 5-FU/LV LV/5-FU2 FOLFOXIRI CAIRO-1 Grothey & Sargent, 2005; Falcone et al., 2007; Koopman et al., 2007.

35 Oxaliplatin Mode of action Oxaliplatin causes inter- and intra-strand cross-links in DNA, inhibiting DNA synthesis and cell proliferation Lesions per Mbp Monoadducts Interstrand Protein cross-links Breaks Oxaliplatin Cisplatin

36 Irinotecan Mode of action Irinotecan is a topoisomerase I inhibitor, this causes DNA double strand breaks and S-phase specific cytotoxicity

37 5-Fluorouracil (5-FU) Mode of action 5-FU inhibits thymidylate synthase (TS) and the synthesis of thymidine nucleotides required for DNA replication It prevents cell division and is S-phase specific
38 Folfiri FOLFOX v FOLFIRI: different toxicity profiles nausea, diarrhoea, mucositis, alopecia fatigue Mild-moderate cytopenias low rates of hospital admission Folfox neurotoxicity is the major toxicity and is usually dose-limiting fatigue Mild-moderate cytopenias low rates of hospital admission
39 Biologic agents VEGF-ab (bevacizumab / aflibercept / ramucirumab) EGFR-ab (cetuximab / panitumumab)


")
 (Tumour cell intravasation)")
 Stages at")

40 Angiogenesis is critical for tumour growth, development, and spread Pre-malignant stage Malignant tumour Tumour growth Vascular invasion Dormant micrometastasis Overt metastasis (Avascular tumour) (Angiogenic switch) (Vascularised tumour) (Tumour cell intravasation) (Seeding in distant organs) (Secondary angiogenesis) Stages at which angiogenesis plays a role in tumour progression Adapted from Poon RT-P, et al. J Clin Oncol 2001;19:
 Avastin (bevacizumab) PI. October 2006; 2. Presta et al. Cancer Res. 1997;57:4593.")
41 Bevacizumab (Avastin ) Blocks VEGF a key mediator in angiogenesis Recombinant humanized monoclonal IgG 1 antibody Half-life is approximately 20 days (range, 11 to 50 days) Avastin (bevacizumab) PI. October 2006; 2. Presta et al. Cancer Res. 1997;57:4593.
42 Proportion surviving Bevacizumab Increases OS in 1st-line mcrc HR=0.66, P= Med OS : 15.6 v 20.3 months 0.2 IFL + placebo IFL + bevacizumab survival (mo) Hurwitz et al. NEJM 2004
43 Proportion of patients NO16966: Bev did not significantly improve OS 1.0 XELOX / FOLFOX4 + Bev XELOX / FOLFOX4 + Placebo HR=0.89 [ ] p= Time [months] Cassidy JCO 2008
44 Several studies now reported, and ALL show some benefit BUT - not as effective as we had initially thought - not as toxic as we had feared - costly - no sub-group identified that derive greater (or lesser) benefit - Doesn t work as monotherapy



45 Aflibercept VEGFR-1 VEGFR-2 IgG Fc Aflibercept Soluble fusion protein Consists of portion of extracellular domains of human VEGF receptors 1 and 2 fused to human IgG1 Fc portion Binds all VEGF-A isoforms, VEGF-B and PlGF High affinity: binds VEGF-A and PlGF more tightly than native receptors Half-life in humans ~17 days

 - Prior bevacizumab (Y/N)")

46 VELOUR Study (World GI and ESMO 2011) R A N 600 Aflibercept 4 mg/kg IV, day 1 + FOLFIRI q2 weeks Metastatic CRC with PD post oxaliplatin Stratification factors: - ECOG PS (0 vs 1 vs 2) - Prior bevacizumab (Y/N) D O M I Z E 1:1 600 Placebo IV, day 1 + FOLFIRI q2 weeks Primary endpoint: OS Sample size: HR 0.8, 90% power and a 2-sided type I error 0.05
47 Overall Survival - ITT Population Cut-off date = February 7, 2011; Median follow-up = months

48 Ramucirumab RAISE (n=1072) : Ph3: FOLFIRI + Ramucirumab/Placebo Med OS 13.3 v 11.7m HR 0.84 p=.02 Med PFS 5.7 v 4.5m HR 0.79 p <.05 Gr 3 toxicity increase: Neut 38 v 23%, HPT 11%v 3%
49 Adding EGFRab to chemo (in RAS WT patients only) Refractory pts work best in this setting either as monotherapy (OS benefit) (often given with irinotecan based on an old phii study in pts unselected for KRAS) Second line improves RR and PFS in all studies but not OS (? cross over effect) First line more consistent improvement in RR cf Bevacizumab -? a better debulker Generally improves PFS v doublet alone Crystal and PRIME studies +ve for OS (modest in KRAS popn) but also 2 ve studies (COIN, NORDIC) (?oxali?cape)
50 OS estimate OS estimate Crystal 1 st line: all RAS: Cetuximab improves OS Overall patient population (ITT) Cetuximab + FOLFIRI (n=599) FOLFIRI (n=599) HR 0.88 p= Months RAS wt population Cetuximab + FOLFIRI (n=178) FOLFIRI (n=189) 28.4 HR 0.69 p= Months Adapted from Van Cutsem E, et al. J Clin Oncol 2011 and Ciardiello F, et al. ASCO 2014 (#3506)
 => greater OS benefit (Post removal 17% pts with mnras) HR 0.78 medos 26.0 v 20.")
51 Prime (FOLFOX+/-Pan) all RAS WT HR 0.83 med OS 23.9 v 19.7 p=.07 OS BENEFIT months RAS WT (both) => greater OS benefit (Post removal 17% pts with mnras) HR 0.78 medos 26.0 v 20.2 p=.04 OS BENEFIT months
 RAS")

52 Prime (FOLFOX+/-Pan) mutant (all) RAS Mutant RAS pts may be harmed by Panitumumab
53
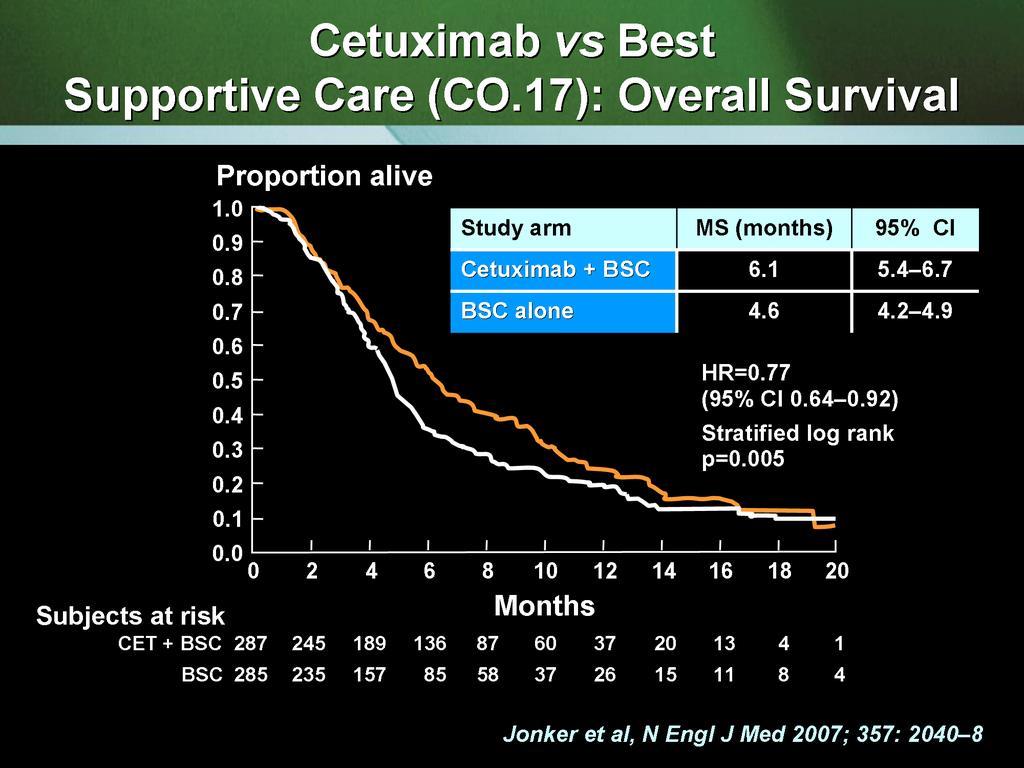
54 1 NCIC CTG C0.17: Overall survival in K-ras Mutant patients Study arm MS (months) 95% CI 0.8 Cetuximab + BSC BSC alone Proportion Alive HR % CI (0.70,1.37) Log rank p-value: Cetuximab BSC Cetuximab BSC Time from Randomisation (Months)
 Log rank p-value: <0.0001 0.")
55 1 NCIC CTG C0.17: Overall survival in K- ras Wild-Type patients Study arm MS (months) 95% CI Proportion Alive Cetuximab + BSC BSC alone HR % CI (0.41,0.74) Log rank p-value: < Cetuximab BSC Time from Randomisation (Months) Cetuximab BSC
56 Biologics - toxicity Bevacizumab Cetuximab/Panitumumab Hypertension gr3/4 (10-15%) Proteinuria gr3 (0-2%) Arterial thrombosis (2-3%) wound healing (1-2%) Bleeding (1-2%) GI perforation (1-2%) acne-form rash (>70%) paronychia Dyspnoea - rare Infusion reaction (0-3%) No effects on wound healing/bleeding reported Long half life


57 EGFr Inhibitor-mediated Skin Toxicity
58 Proportion Alive CO17: Suvival by Worst Grade of Rash Grade HR 95%CI p-value 2+ vs (0.22, 0.50) < vs (0.40, 0.93) vs (0.41, 0.72) < Grade n Median Survival mo mo mo 20 0 Landmark-type analysis excluding all pts dying within 28 days of entry 90% experienced rash by 29 days, Median time to rash = 10 days Months 18
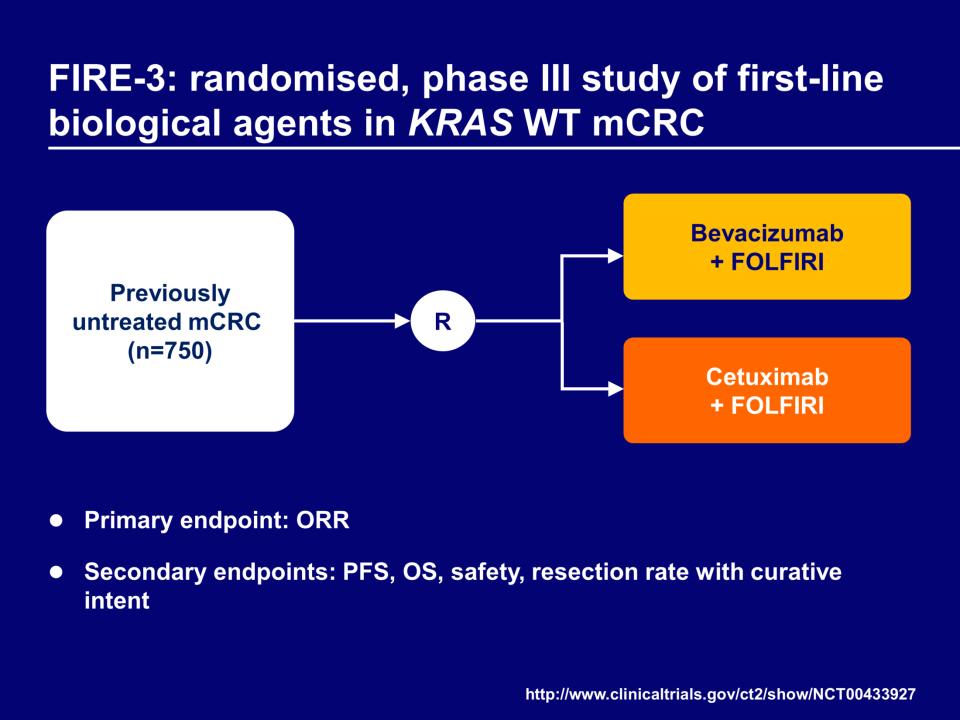
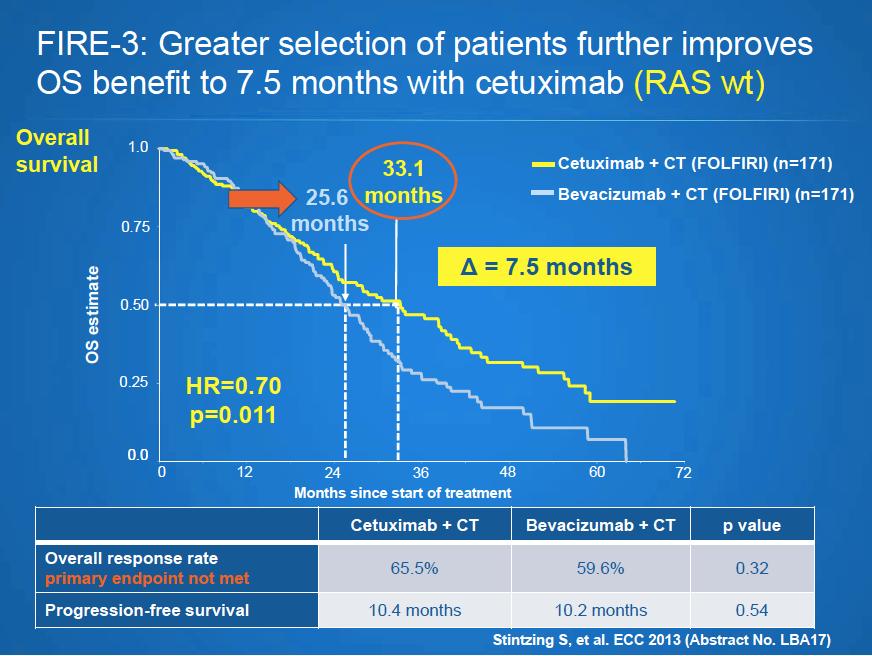
59 head to head comparison (only in the 40-50% of pts all RAS WT)
60
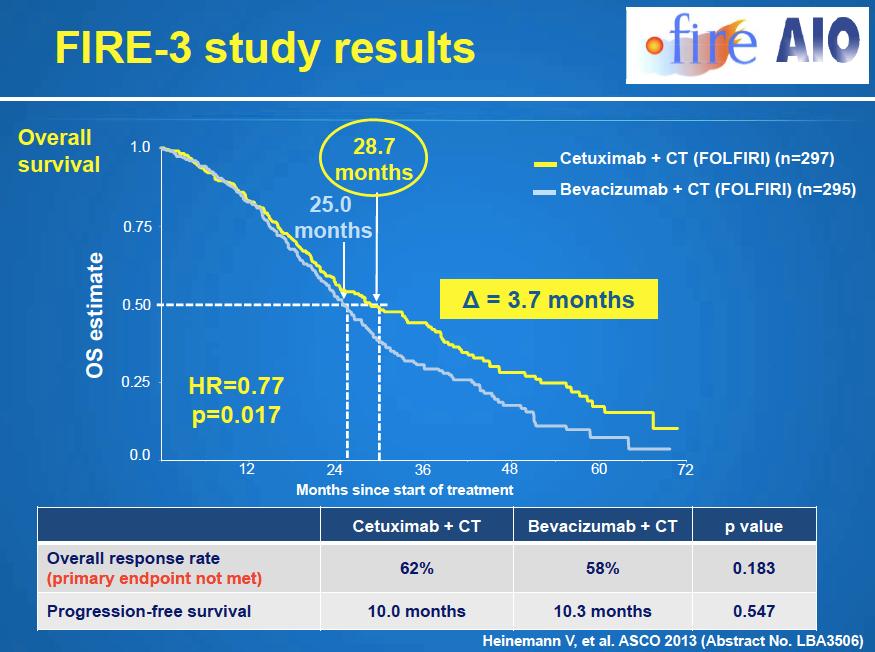
61 Primary Endpoint of FIRE-3: Overall Response Rate Endpoint FOLFIRI + Cetuximab FOLFIRI + Bevacizumab OR P Value ORR, intent-to-treat (ITT) population (N=592) 62.0% 58.0% 1.18 ( ) Complete response 4.4% 1.4% Partial response 57.6% 56.6% Stable disease 17.5% 28.8% Progressive disease 7.1% 5.4% Not evaluable 13.1% 7.8% ORR, Evaluable (N=526) 72.2% 63.1% 1.52 ( ) Heinemann V. ASCO Abstract LBA3506.

62 FIRE-3: Progression Free Survival Stintzing S. ASCO Abstract LBA3506
63
64
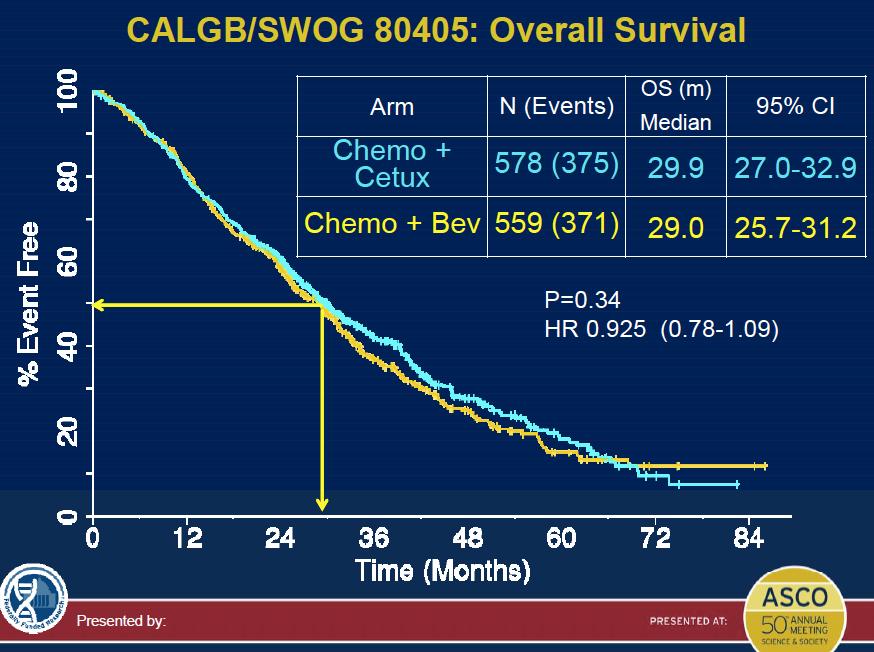
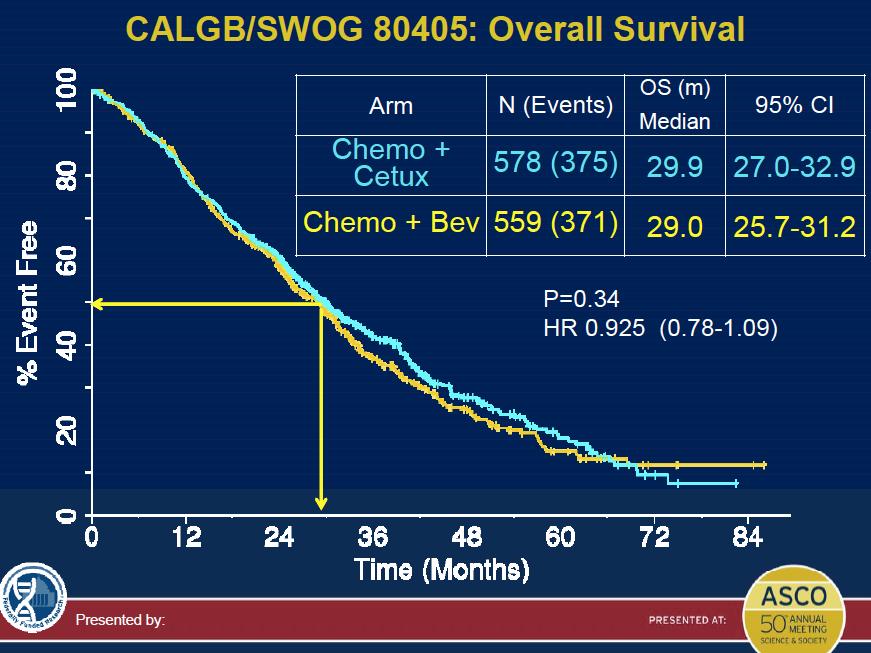
65 This data rocked GI oncology in 2013/ 2014 Was it true? How could a drug not increase RR (primary end point), or PFS, yet increase OS..?? large US trial (80405) eagerly anticipated
66
67
68
69 PBS Logistics 2015 PBS reimbursement dictates order of use: => Bevacizumab then Cetuximab/Panitumumab Bev PBS funded only for 1 st line Cetux/Pan PBS funded only after progression (RAS WT only) Bevacizumab not funded if given after Cetuximab
70 First line therapy Even more intensive initial approach FOLFOXIRI +/- biologics
71 Even more intensive Advantages Most like to induce a rapid and more dramatic responses Rapid symptom relief Longer disease control conversion therapy unresectable to resectable
72 Even more intensive Disadvantages Toxicity Played all cards upfront?? salvage Not clear that this will result in OS advantage
73 FOLFIRI vs FOLFOXIRI: GONO STUDY FOLFIRI (122 pts) FOLFOXIRI (122 pts) P value RR 34% 60% < R0 surgery 6% 15% Liver only 12% 36% mpfs (mos) mos (mos) A. Falcone et al. JCO 2007 and ASCO 2007
74 FOLFIRI vs FOLFOXIRI: GONO STUDY Largely ignored! (TOXICITY CONCERNS) Gr 3-4 toxicity Triplet % Doublet % neutropenia diarrhoea vomiting 7 2 Neuro (gr 2/3) 20 0 => DOUBLET + BIOLOGICS PREFERRED IF AVAILABLE A. Falcone et al. JCO 2007 and ASCO 2007
75 Since 3 drugs are better than 2... How about 4??...? Triple chemo with one biologic? Doublet chemo with 2 biologics
 5-FU/LV + Bev (Maintenance) 1:1 Randomization FOLFOXIRI + Bev (up to 12 cycles) 5-FU/LV + Bev (Maintenance) Treat to progression Falcone A. ASCO 2013. Abstract 3505.")
76 TRIBE Phase III Study ( 4 v 3 drugs) Patients Unresectable mcrc No prior mcrc treatment Adjuvant oxali-containing chemotherapy allowed if >12 mo between tx and relapse FOLFIRI + Bev (up to 12 cycles) 5-FU/LV + Bev (Maintenance) 1:1 Randomization FOLFOXIRI + Bev (up to 12 cycles) 5-FU/LV + Bev (Maintenance) Treat to progression Falcone A. ASCO Abstract 3505.
77 TRIBE: PFS (ITT Population) Falcone A. ASCO Abstract 3505.
78 TRIBE: Secondary Endpoint (OS) Falcone A. ASCO Abstract 3505.

79
80 Combination EGF and VEGF Abs. Seemed a good idea...pre-clinical rationale, clinical data (BOND2)... But PACCE (2007) Increased toxicity Inferior PFS Phase III ChemoBev +/- panitumumab in arm with chemo and doublet antibody trend to worse OS at interim analysis => TRIAL STOPPED CAIRO 2 (2008) Phase III XeloxBev +/- cetuximab Increased toxicity in arm with chemo and doublet antibody Inferior PFS 9.6 v 10.7 m [p=0.018]
81 Maintenance therapy
82 Chemotherapy Free Intervals - CFIs OPTIMOX 1 (JCO 06) - Similar outcomes - arm2 better tolerated FOLFOX7 x 6 FOLFOX4 until progression 5FU FOLFOX7 OPTIMOX 2 (ASCO 07) - inferior outcome in arm2 - (av break 4 mths?too long) FOLFOX7 x 6 FOLFOX7 x 6 5FU FOLFOX7 FOLFOX7 GISCAD (ASCO 06) - Similar outcomes - Less toxicity - 2 months on/off Irinotecan - continuous Irinotecan Irinotecan Irinotecan Irinotecan

 CR PR SD R Observation")


83 Koopman, et al. ASCO 2013 CAIRO3: maintenance bev+cape v observation PFS1 PFS2 Arm A Previously untreated mcrc (n=558) bevacizumab + XELOX (x6) CR PR SD R Observation bevacizumab + capecitabine PD1 PD1 bevacizumab + XELOX bevacizumab + XELOX PD2 PD2 Arm B Primary endpoint: PFS after re-introduction = PFS2 Capecitabine 625 mg /m2 bd continuously (Bev 7.5 mg/kg q3 wks) Upon PD1, only 75% in ARM A and 47% arm B received XELOXbev
84 PFS1 estimate CAIRO3: PFS1 significantly improved with maintenance Maintenance Observation Median PFS1, months Stratified HR (95% CI) 0.44 ( ) p< Adjusted* HR 0.41 p < Time (months) Observation Maintenance *Adjusted for covariates with imbalances at baseline; Koopman, et al. ASCO 2013
85 PFS2 estimate CAIRO3: PFS2 (1 o end point) improved with maintenance Maintenance Observation Median PFS2, months Stratified HR (95% CI) 0.81 ( ) p=0.028 Adjusted* HR 0.77 p= Time (months) Observation Maintenance *Adjusted for covariates with imbalances at baseline; Koopman, et al. ASCO 2013
86 OS estimate CAIRO3: OS improved* with maintenance bevacizumab (preliminary analysis) Maintenance Observation Median OS, months Stratified HR (95% CI) 0.87 ( ) p=0.156 Adjusted* HR 0.80 p= Time (months) Observation Maintenance *Adjusted for covariates with imbalances at baseline; Koopman, et al. ASCO 2013
87 CAIRO3: safety profile during observation/ maintenance Grade 3/4 adverse event, % Observation (n=279) Maintenance (n=279) Hypertension Neutropenia 0 2 Thrombocytopenia 0 1 Diarrhoea 1 3 Vomiting Nausea 0 2 Hand-foot syndrome 0 22 Neurotoxicity 5 10 GI perforation 0 1 Venous thromboembolic events 2 3 Fatigue 2 4 Red box indicates a difference in incidence between treatment arms of 5% NB also - no drop off in % pts receiving all 4/5 drugs - reassuring
88 Maintenance therapy No significant survival benefit can t be too dogmatic! Does delay progression modestly (CAIR03 HR 0.44) If having breaks, need to monitor closely A FP + bev is optimal. (No role Bev mono) however 22% gr3+ HF syndrome is unacceptable Which subgroup benefit most from this approach??
89 Second line therapy? chemo + antivegf (more bev/aflib/ram?)? chemo + EGFR (WT)? chemo alone
90 Decision 1 is more systemic Rx needed? Progression may be very slow? continue to observe Sometimes non-systemic Rx is appropriate Radiotherapy for local PD Liver directed therapy
91 Decision 2: which chemo backbone? Change doublet Restart 1 st line Rx if did not progress on Rx. (if Optimoxing, or if on a chemo-break)
92 Decision 3: to add a biologic? Continue Bevacizumab Beyond Progression New data re aflibercept/ramucurimab to consider too Switch from Bev to EGFRab if WT (or vice versa) Chemo alone, (keep EGFRab in reserve for 3 rd line) NB If FOLFIRI alone in 1 st line => FOLFOX + Bev (e3200 data, but not PBS)
93 What about using EGFR Abs in second line
94 2 nd line regimens -EGFRAb Increased RR and PFS when C-Mab / P-Mab added to Irinotecan-based chemo EPIC trial - cetux Sobrero JCO trial - p mab Peeters ESMO 2009 BUT no survival benefit (? due to crossover)
95 ECCO 2011: PICCOLO: efficacy data KRAS WT Irinotecan (n=230) Irinotecan + panitumumab (n=230) Median OS (months) HR (95% CI) 0.91 ( ) p value 0.44 Median PFS (months) HR (95% CI) 0.78 ( ) p value 0.01 ORR (%) p value < Seymour, et al. ECCO-ESMO 2011 (abstract 6007)
96 ECCO 2011: PICCOLO trial Irinotecan +/- P mab in 2 nd line adv CRC Again no overall survival benefit with EGFR in 2 nd line but Not due to crossover only 6% in this study => Strengthens argument to hold EGFRAb for 3 rd line - delay toxicity - use where survival benefit clearly documented
97




98 Proportion of pts receiving Rx diminishes with subsequent lines 1st line 2nd line 3rd line
99 Refractory patients No significant advances for several years now modest benefit at best: Regorafenib/TAS102 several ve phase III trials: Brivanib, BBI Don t always need to rush into next line of Rx consider liver directed Rx if suitable.. consider Rx breaks if asymptomatic/slow paced

 Regorafenib VEGFR1 13 ± 0.")
 Inhibition of proliferation KIT PDGFR RET")

 PDGFR-β 22 ± 3 (2) FGFR1 202 ± 18 (6)")
 RAF-1 2.5 ± 0.")

100 Regorafenib (BAY ), an oral multikinase inhibitor targeting multiple tumor pathways 1-3 Biochemical activity Regorafenib IC 50 mean ± SD nmol/l (n) Regorafenib VEGFR1 13 ± 0.4 (2) Murine VEGFR2 4.2 ± 1.6 (10) Inhibition of proliferation KIT PDGFR RET Inhibition of tumor microenvironment signaling PDGFR-β FGFR Inhibition of neoangiogenesis VEGFR1-3 TIE2 Murine VEGFR3 46 ± 10 (4) TIE2 311 ± 46 (4) PDGFR-β 22 ± 3 (2) FGFR1 202 ± 18 (6) KIT 7 ± 2 (4) RET 1.5 ± 0.7 (2) RAF ± 0.6 (4) B-RAF 28 ± 10 (6) B-RAF V600E 19 ± 6 (6) 1. Wilhelm SM et al. Int J Cancer Mross K et al. Clin Cancer Research Strumberg D et al. Expert Opin Invest Drugs 2012.

101 Overall survival (primary endpoint) Primary endpoint met prespecified stopping criteria at interim analysis (1-sided p< at approximately 74% of events required for final analysis)
102 Drug-related treatment-emergent adverse events occurring in 10% of patients Adverse event, % All grades Regorafenib N=500 Grade 3 Grade 4 Grade 5* All grades Grade 3 Placebo N=253 Grade 4 Hand-foot skin reaction Fatigue Hypertension Diarrhea Rash / desquamation Anorexia Mucositis, oral Thrombocytopenia Fever Nausea Bleeding Voice changes Weight loss * Grade 5 drug-related AEs: 1.0% in regorafenib arm vs 0% in placebo arm Grade 5*

103 What about SIR Spheres? ASX: post SIRFLOX press release 17/3/15
104 Conclusions (1) consider if your stage IV pt could be resectable Even if not, med OS 2.5 yrs, 15% > 5 years. A large array of treatment options now available Early review of these patients in MDM setting
105 Conclusions (2) Treatment Goal Treatment Intensity Develop chemo strategy (cure v palliative v decide in 3months) (aggressive v mono v observ) (OPTIMOX/?maintenance/?CFI) Determine biologic strategy


106 Play your systemic therapy cards cleverly know when to hold them..
 study MONO V COMBO cetux cetux +")
107 For RAS WT pts refractory to Irinotecan.. The Irinotecan Cetuximab Evaluation and the Cetuximab Response Evaluation Among Mutants (ICE CREAM) study MONO V COMBO cetux cetux + irino Study recruitment 89/100, g13d arm closed WT arm : all RAS WT now acceptable for study entry..
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer
 Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
First line treatment in metastatic colorectal cancer
 First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
What s New? Dr. Barbara Melosky
 Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Antiangiogenic therapy in GI cancer: current status and future directions
 Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC)
") 1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC) Role of the VEGF Pathway in Oncogenesis The Role of Angiogenesis in Cancer Somatic mutation Small avascular tumor Tumor secretion of
1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC) Role of the VEGF Pathway in Oncogenesis The Role of Angiogenesis in Cancer Somatic mutation Small avascular tumor Tumor secretion of
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Advances in Chemotherapy of Colorectal Cancer
 Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos?
 Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms
 21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
JY Douillard MD, PhD Professor of Medical Oncology
 Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical modulation, Oral fluoropyrimidines, Developmentof combination chemotherapy
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
What to do after 1st-line failure in mcrc?
 What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
Fighting a Smarter War On Colon Cancer:
 Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
AIOM GIOVANI Perugia, Luglio 2017
 AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
Understanding predictive and prognostic markers
 Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression
 Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy?
 Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Targeted therapies in colorectal cancer: the dos, don ts, and future directions
 Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER
 RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
The role of Maintenance treatment Appropriate endpoints according to ESMO consensus
 ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
The ESMO consensus conference on metastatic colorectal cancer
 ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
Ashita Waterston Beatson West of Scotland Cancer Centre
 Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Toxicity by Age Group. Old Factor 1: Age. Disclosures. Predicting survival in metastatic colorectal cancer. Personalized Medicine - Decision Tools -
 Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Medical Therapy of Colorectal Cancer in the Biomarker Era
 Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
What to do after 1 st line failure?
 ESMO Preceptorship Programme Colorectal Cancer Singapore 20-22 nd 2016 JY Douillard MD PhD ESMO CMO What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy
ESMO Preceptorship Programme Colorectal Cancer Singapore 20-22 nd 2016 JY Douillard MD PhD ESMO CMO What to do after 1 st line failure? mcrc: How to maximize survival? Improving 1st line therapy efficacy
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Recent advances in treatment of metastatic colorectal cancer
 Recent advances in treatment of metastatic colorectal cancer Clin. Invest. (2012) 2(11), 1109 1122 Metastatic colorectal cancer is the second leading cause of cancer-related death in the Western population.
Recent advances in treatment of metastatic colorectal cancer Clin. Invest. (2012) 2(11), 1109 1122 Metastatic colorectal cancer is the second leading cause of cancer-related death in the Western population.
RAS and BRAF in metastatic colorectal cancer management
 Review Article RAS and BRAF in metastatic colorectal cancer management Jun Gong 1, May Cho 1, Marwan Fakih 2 1 Department of Medical Oncology, City of Hope National Medical Center, Duarte, CA, USA; 2 Medical
Review Article RAS and BRAF in metastatic colorectal cancer management Jun Gong 1, May Cho 1, Marwan Fakih 2 1 Department of Medical Oncology, City of Hope National Medical Center, Duarte, CA, USA; 2 Medical
Jonathan Dickinson, LCL Xeloda
 Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Colorectal Cancer Update Dr. Barb Melosky
 Colorectal Cancer Update 2017 Dr. Barb Melosky bmelosky@bccancer.bc.ca Disclosure Research Support/P.I. Honoraria/Advisory Board Bayer Roche, Amgen, Bayer, Lilly Objectives 1) Demonstrate knowledge of
Colorectal Cancer Update 2017 Dr. Barb Melosky bmelosky@bccancer.bc.ca Disclosure Research Support/P.I. Honoraria/Advisory Board Bayer Roche, Amgen, Bayer, Lilly Objectives 1) Demonstrate knowledge of
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer. Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center
 Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
La strategia terapeutica del carcinoma del colon metastatico
 Dalla Capecitabina al TAS-102 Milano, 29 settembre 2016 La strategia terapeutica del carcinoma del colon metastatico Gianluca Masi U.O. di Oncologia Medica Universitaria Azienda Ospedaliero-Universitaria
Dalla Capecitabina al TAS-102 Milano, 29 settembre 2016 La strategia terapeutica del carcinoma del colon metastatico Gianluca Masi U.O. di Oncologia Medica Universitaria Azienda Ospedaliero-Universitaria
Tobias Engel Ayer Botrel 1,2*, Luciana Gontijo de Oliveira Clark 1, Luciano Paladini 1 and Otávio Augusto C. Clark 1
 Botrel et al. BMC Cancer (2016) 16:677 DOI 10.1186/s12885-016-2734-y RESEARCH ARTICLE Open Access Efficacy and safety of bevacizumab plus chemotherapy compared to chemotherapy alone in previously untreated
Botrel et al. BMC Cancer (2016) 16:677 DOI 10.1186/s12885-016-2734-y RESEARCH ARTICLE Open Access Efficacy and safety of bevacizumab plus chemotherapy compared to chemotherapy alone in previously untreated
Università degli Studi di Pisa Facoltà di Medicina e Chirurgia Scuola di Specializzazione in Oncologia
 Università degli Studi di Pisa Facoltà di Medicina e Chirurgia Scuola di Specializzazione in Oncologia Tesi di Specializzazione EZH2 polymorphisms and outcome of metastatic colorectal cancer patients Candidato:
Università degli Studi di Pisa Facoltà di Medicina e Chirurgia Scuola di Specializzazione in Oncologia Tesi di Specializzazione EZH2 polymorphisms and outcome of metastatic colorectal cancer patients Candidato:
P < vs. 5FU/LV LD 0% 60.0% 3.6 months P < P = 0.113
 in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD
 Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)
 in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)") Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO
 Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Tumors in the Randomized German AIO study KRK-0306
 FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer
 Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
New Options in Metastatic Colorectal Cancer. Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka
 New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER
 THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER Cathy Eng, M.D., F.A.C.P. Associate Professor Associate Medical Director, Colorectal Center Dept of GI Medical Oncology November 5, 2010
THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER Cathy Eng, M.D., F.A.C.P. Associate Professor Associate Medical Director, Colorectal Center Dept of GI Medical Oncology November 5, 2010
GI SLIDE DECK. Selected abstracts from: 31 May 4 Jun 2013 Chicago, USA ASCO Annual Meeting. 27 Sep 1 Oct 2013 Amsterdam, Netherlands ESMO-ECCO
 GI SLIDE DECK 31 May 4 Jun 2013 Chicago, USA ASCO Annual Meeting 2013 Selected abstracts from: 3 Jul 6 Jul 2013 Barcelona, Spain WCGIC 27 Sep 1 Oct 2013 Amsterdam, Netherlands ESMO-ECCO Supported by Eli
GI SLIDE DECK 31 May 4 Jun 2013 Chicago, USA ASCO Annual Meeting 2013 Selected abstracts from: 3 Jul 6 Jul 2013 Barcelona, Spain WCGIC 27 Sep 1 Oct 2013 Amsterdam, Netherlands ESMO-ECCO Supported by Eli
Adjuvant treatment Colon Cancer
 ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux
 Michel Ducreux") Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
MANAGEMENT OF ADVANCED COLORECTAL CANCER
 MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
COMETS: COlorectal MEtastatic Two Sequences
 COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Colon cancer: Highlights. Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano
 Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Role of SIRT Beyond First Line Therapy in Colorectal Cancer. Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore
 Role of SIRT Beyond First Line Therapy in Colorectal Cancer Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore MILESTONES IN THE TREATMENT OF COLON CANCER SIR-Spheres microspheres
Role of SIRT Beyond First Line Therapy in Colorectal Cancer Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore MILESTONES IN THE TREATMENT OF COLON CANCER SIR-Spheres microspheres
Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto
 Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
MEET ROY*: A PATIENT WITH LIVER-LIMITED mcrc
 MEET ROY*: A PATIENT WITH LIVER-LIMITED mcrc * A hypothetical case study of a patient eligible for first-line mcrc therapy. mcrc = metastatic colorectal cancer. WHAT CLINICAL CHARACTERISTICS AFFECT YOUR
MEET ROY*: A PATIENT WITH LIVER-LIMITED mcrc * A hypothetical case study of a patient eligible for first-line mcrc therapy. mcrc = metastatic colorectal cancer. WHAT CLINICAL CHARACTERISTICS AFFECT YOUR
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
Bevacizumab is currently licensed for the following indication relevant for this NICE review:
 Roche Executive Summary Context Bevacizumab (Avastin) is a humanized (93% human) murine monoclonal antibody which binds to and neutralizes VEGF, a powerful pro-angiogenic glycoprotein produced by both
Roche Executive Summary Context Bevacizumab (Avastin) is a humanized (93% human) murine monoclonal antibody which binds to and neutralizes VEGF, a powerful pro-angiogenic glycoprotein produced by both
Strategy for the treatment of metastatic CRC through the lines
 Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
Optimizing Sequencing Beyond Disease Progression After Second-Line Therapy in Metastatic Colorectal Cancer
 Optimizing Sequencing Beyond Disease Progression After Second-Line Therapy in Metastatic Colorectal Cancer Kabir Mody, MD, and Tanios Bekaii-Saab, MD Abstract Colorectal cancer (CRC) remains a significant
Optimizing Sequencing Beyond Disease Progression After Second-Line Therapy in Metastatic Colorectal Cancer Kabir Mody, MD, and Tanios Bekaii-Saab, MD Abstract Colorectal cancer (CRC) remains a significant
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
SIR-Spheres: Des essais cliniques à la pratique courante
 SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
OVERALL CLINICAL BENEFIT
 cetuximab plus FOLFIRI to convert unresectable liver metastatses to resectable, perc confirmed that neither the FIRE-3 study nor the CRYSTAL study were designed to assess resectability and, in the absence
cetuximab plus FOLFIRI to convert unresectable liver metastatses to resectable, perc confirmed that neither the FIRE-3 study nor the CRYSTAL study were designed to assess resectability and, in the absence
Panitumumab: The KRAS Story. Chrissie Fletcher, MSc. BSc. CStat. CSci. Director Biostatistics, Amgen Ltd
 Panitumumab: The KRAS Story Chrissie Fletcher, MSc. BSc. CStat. CSci. Director Biostatistics, Amgen Ltd Clinical Background: panitumumab in mcrc Panitumumab is a fully human IgG2 monoclonal antibody directed
Panitumumab: The KRAS Story Chrissie Fletcher, MSc. BSc. CStat. CSci. Director Biostatistics, Amgen Ltd Clinical Background: panitumumab in mcrc Panitumumab is a fully human IgG2 monoclonal antibody directed
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
COLORECTAL CANCER. Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program
 COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
Advances in the Management of Colorectal Cancer
 Advances in the Management of Colorectal Cancer Dr Ashraf Wadee Medical Oncologist Charlotte Maxeke Johannesburg Academic Hospital and Wits Donald Gordon Medical Colorectal Cancer: Background 3 rd most
Advances in the Management of Colorectal Cancer Dr Ashraf Wadee Medical Oncologist Charlotte Maxeke Johannesburg Academic Hospital and Wits Donald Gordon Medical Colorectal Cancer: Background 3 rd most
Opinion 17 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 October 2012 VECTIBIX 20 mg/ml, concentrate for solution for infusion B/1 vial of 5 ml (CIP code: 3400957181857)
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 October 2012 VECTIBIX 20 mg/ml, concentrate for solution for infusion B/1 vial of 5 ml (CIP code: 3400957181857)
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage. Dr Lee-Ann Jones
 Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre)
") Metastatic Esophagogastric Cancer Summary Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
Metastatic Esophagogastric Cancer Summary Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES
 CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία. Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018
 Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
ADVANCES IN COLON CANCER
 ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
Management of Patients with Colorectal Cancer
 Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Angiogenesis and tumor growth
 Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
The treatment of metastatic colorectal cancer in 2007
 The treatment of metastatic colorectal cancer in 2007 Prof Eric Van Cutsem, MD, PhD Gastrointestinal Oncology Unit University Hospital Gasthuisberg Leuven - Belgium CRC is a major health concern Life-time
The treatment of metastatic colorectal cancer in 2007 Prof Eric Van Cutsem, MD, PhD Gastrointestinal Oncology Unit University Hospital Gasthuisberg Leuven - Belgium CRC is a major health concern Life-time
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
Malignant pleural Mesothelioma: A Year In Review
 Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second
Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second