Conflict of Interest Disclosure. Anita L. Nelson, MD. Principles Underlying Screening Recommendations. Learning Objectives
|
|
|
- Candice Elliott
- 6 years ago
- Views:
Transcription

1 Advanced Colposcopy Conflict of Interest Disclosure Anita L. Nelson, MD Anita L. Nelson, MD Professor OB-GYN David Geffen School of Medicine at UCLA CFHC s 2014 Women s Health Update Berkeley, CA May 20, 2014 Grants/ Research Honoraria/ Speakers Bureau Consultant/ Advisory Board Bayer, Merck, Pfizer, Teva Actavis, Bayer, Merck, Pfizer, Teva Agile, Bayer, ContraMed, Medicus, Merck, Teva Anita L. Nelson, MD 2 Learning Objectives At the end of this presentation, the participant will be able to: Outline routine screening recommendations for women of different ages. Explain the principles underlying the differences between younger and older women in recommendations for management of biopsy-proven dysplasia. Describe the upcoming new terminology that is expected to replace the current CIN nomenclature. Outline the evaluation needed for abnormal cytologic test results and for dysplasia. Anita L. Nelson, MD 3 Principles Underlying Screening Recommendations Virtually every sexually active person will be exposed to HPV Most HPV infections are transient High risk-hpv infections take longer (> 24 months) than low risk HPV Significant cervical dysplasia is caused by persistent HPV infection Anita L. Nelson, MD 4 Cervical Cancer Anita L. Nelson, MD 5 U.S. Incidence of Cervical Cancer In US in 2014: 12,360 new cases 4,020 deaths 70% reduction due to Pap smear screening Cervical cancer is disease of economically disadvantaged--elderly, minorities and low socioeconomic status Types of cervical carcinoma: Squamous 85% Adenocarcinoma 15% Anita L. Nelson, MD 6 1
 First Lesion Immune Response About 9 mo Active Growth (3-6 Mo.")
2 Risk Factors For Cervical Dysplasia and Cancer: Multiple Sexual Partners Natural Course of HPV Infection Number of Sexual Partners Relative Risk Without Smoking Relative Risk With Smoking Anita L. Nelson, MD 7 I N F E C T I O N Incubation (1-8 Mo.) First Lesion Immune Response About 9 mo Active Growth (3-6 Mo.) Host Late Stage Containment (3-6 Mo.) Sustained clinical remission Persistent or recurrent disease Anita L. Nelson, MD 8 Prevalence of Minor Precursors, Major Precursors, and Invasive Cancer Screening Recommendations Age/Condition < > 65 After hysterectomy No Screening Screening Cytology alone Q 3 years HPV and cytology co-testing Q 5 years OR No screening following adequate prior negative screening No screening if no prior CIN 2 in prior 20 years Anita L. Nelson, MD 9 ACOG Bulletin no Obstet Gynecol. 2013;122(6): Anita L. Nelson, MD 10 Cervical Cancer: Impact of Screening: Remaining Gaps About 50% of US cervical cancers occur in: Women never screened Another 10% US cervical cancers Women not screened in past 5 years Screening fails Low resource, medically underserved regions rates 7 times higher Socioeconomic, geographic and/or racial disparities Saslow D, et al. Am J Clin Pathol. 2012;137: Anita L. Nelson, MD 11 Accuracy of Colposcopically-Directed Punch Biopsies: Meta-analysis 7,873 pairs of punch biopsy and excisional biopsies when excisional biopsy done immediately following punch biopsy 1 Sensitivity 81.4% Specificity 63.3% Norwegian study 24% with negative biopsies found to have CIN 2 on follow-up biopsy 2 Single punch biopsy/leep pairs in colposcopically diagnosed CIN 1 failed to detect 71.4% of CIN 2 1. Underwood M, et al. BJOG. 2012;119(11): Moss EL, et al. J Low Genit Tract Dis. 2012;16(4): Anita L. Nelson, MD 12 2
3 Contributions of ECC 13,115 colposcopic examinations with guided biopsy ECC increased diagnosis of CIN2+ by 1.01% 99 ECC procedures needed to identify one new case of CIN2+ ECC most valuable in: Women 46 years old High grade CIN, HSIL Most of these women need excisional biopsy regardless of ECC Gage JC, et al. Am J Obstet Gynecol. 2010;203(5):481.e1-9. Anita L. Nelson, MD 13 Random Cervical Biopsy and ECC in Low Risk Populations 4 quadrant random biopsies and ECC routinely added to colposcopically directed biopsies 4,677 women had colposcopy 295 CIN 3 61 (20.7%) diagnosed on random biopsy ± ECC Random biopsies increase yield ECC not helpful in women < 25 years Pretorius RG, et al. J Low Genit Tract Dis. 2012;16(4): Anita L. Nelson, MD 14 Revised Terminology for Cervical Histopathology Consensus conference: Lower Anogenital Squamous Terminology (LAST) 35 organizations Uniform 2-tier terminology for all HPV-related squamous diseases Vulva, vagina, cervix, penis, perianus, and anus 2-tier classification similar to cytology results Low-grade SIL (IN) High-grade SIL (IN) Replaces CIN 1, CIN 2, CIN 3 Waxman AG, et al. Obstet & Gynecol. 2012;120(6): Anita L. Nelson, MD 15 Revised Terminology for Cervical Histopathology Problems with prior CIN 2 Poor reproducibility Agreement in only 13-43% of cases Not clear clinical meaning Usually combined with CIN 3 Many represent mixture of cells Intermediate diagnosis of CIN 2 now resolved into either high or low grade SIL Waxman AG, et al. Obstet & Gynecol. 2012;120(6): Anita L. Nelson, MD 16 Use of Adjunctive Tests to Sort CIN 2 Use of p16 INK4a (p16) immunohistochemical stain to determine if high or low grade lesion Overexpression of P16 occurs in squamous cells Cell cycle regulator (retinoblastoma protein)(prb) inactivated by E7 oncoprotein of high-risk HPV Positive p16 immunostaining of squamous cells throughout epithelium correlates well with HSIL If CIN 2 lesion seen on hematoxylin and eosin dyes P16 HSIL (histology) P16 LSIL (histology) Waxman AG, et al. Obstet & Gynecol. 2012;120(6): Anita L. Nelson, MD 17 Lost to Follow-Up Low-Income Colposcopy Clinic Compliance was defined as 1 return visit within 3-14 months 54% appropriately timed repeat testing 46% failed to return within 14 months 45% of women with CIN 2 or 3 did not return Risk factors: Referral from outside clinic, self or government funds, Spanish speaking, unmarried Chase DM, et al. J Low Genit Tract Dis. 2012;16(4): Anita L. Nelson, MD 18 3
4 Recurrence Rates After Treatment for CIN 1, 2, 3 37,142 women treated for CIN 1, 2, or 3 diagnosed in Recurrence rates depend on grade of CIN, treatment used and woman s age In first 6 year after treatment, rate of CIN 2,3 5.6% for original CIN 1 9.3% for original CIN % for original CIN 3 After 6 years, annual recurrence rates were <1% Melnikov J, et al. J Natl Cancer Inst. 2009;20(101): Anita L. Nelson, MD 19 Alternative Screening Methods High risk HPV testing of urine sample 1 Concordance with cervical cytology 80% Sensitivity for HSIL 100% Specificity for HSIL 80% Positive predictive value 91% Blind vaginal swabs for HR-HPV 2 Acceptable yield of endocervical cells Self swabbing for cytology and HR-HPV samples 1. Alameda F, et al. J Low Genit Tract Dis. 2007;11(1): Kavoussi SK, et al. J Womens Health. 2009;18(1): Anita L. Nelson, MD 20 Future Developments: Cervical Adenocarcinoma HPV 16, 18 account for: 70% squamous cell carcinoma 80% adenocarcinoma HPV test-based screening may be more effective than cytology-based screening for adenocarcinoma HPV 77.8% vs. PAP 17.4% HPV-related adenocarcinoma detected earlier by HPV-tests Adegple O, et al. J Womens Health. 2012;21(10): Anita L. Nelson, MD 21 Vaccine for Cervical Dysplasia Cancer Treatment: Early Promise 10-25% of women with high grade dysplasia clear themselves Tend to have higher levels of T cells against HPV genes E6 and E7 New vaccine designed to trigger production of these T cells 14 of 18 women responded for 2 years T cells functional Inserts specific DNA into patient s cells using electroporation Anita L. Nelson, MD 22 Treatment CIN 2-3 Topical Imiquimod: 16 Week Trial Randomized, double-blind, placebo-controlled phase 2 trial self-applied vaginal imiquimod vs. placebo: Imiquimod Placebo Reduced to CIN 1 73% 39% Complete remission 47% 14% HPV clearance 60% 14% Complete remission HPV-16 47% 0 Microinvasive 0 5% Erythema 37% Erosion 30% Severe edema 13% Grimm C, et al. Obstet & Gynecol. 2012;120(1): Anita L. Nelson, MD 23 Value of ECC and Random Biopsy Retrospective analysis of 550 patients undergoing colposcopy Women with CIN 2 on colposcopy 42.1% single 1-quadrant lesion 101 patients with no visible lesion; CIN 2 found 26 patients on ECC only 11 patients ECC + random biopsy 63% of ASC-US on pap and no colposcopic lesion had on CIN 2 on random biopsy Patients with no visible lesions were 4 times more likely to have CIN 2 Diedrich JT, et al. J Low Genit Tract Dis. 2012;S11. Anita L. Nelson, MD 24 4


5 ECC in Low Grade Cytology (LSIL or ASC-US + HPV) Improves Detection High Grade Disease 374 patients; 75 women CIN 2 16 ECC with high grade dysplasia 12 high grade had ectocervical dysplasia 4 on ECC alone 4 in 374 = 1 in 93.5 Screen to find 1 case 4 in 16-25% of cases Rose JD, et al. Am J Obstet Gynecol. 2012;doi: Anita L. Nelson, MD 25 ECC in Low Grade Cytology Improve Detection High Grade Disease Conclusion: Routine ECC at time of satisfactory colposcopy for low grade abnormality with a visible lesion does not significantly improve the diagnosis of high grade dysplasia Rose JD, et al. Am J Obstet Gynecol. 2012;doi: Anita L. Nelson, MD 26 Pain Control (VAS) with Cervical Biopsy Forced Coughing vs 1% Lidocaine Injection Speculum Insertion Local Anesthetic Injection 1.4 (0-6) Cervical Biopsy Forced Coughing P Value 95% CI for Difference 1.7 (0-7.5) 1.4 (0-6.9) to (0-7.1) 1.9 (0-8.5) to 1.3 Overall Score 2.3 (0-9) 3.0 (0-8.5) to 1.5 Time needed (min) 7.0 (5-15) 5.0 (3-8) < to -1.6 Schmid BC, et al. Am J Obstet Gynecol. 2008;199(6):641.e1-3. Anita L. Nelson, MD 27 Role Of Primary LLETZ Therapy Look and LEEP Reserved for HSIL in Adults Pap smear Histology No dysplasia CIN 1 CIN 2/3 Microinvasive All grades 32.5% 26.5% 40.5% 0.5% CIN % CIN 2,3 63.9% Alvarez: Gynecol Oncology Anita L. Nelson, MD 28 Photodynamic Therapy 19&cHash=742ddca6d83d090bfeb4b64383ba1678 Anita L. Nelson, MD 29 Anita L. Nelson, MD 30 5




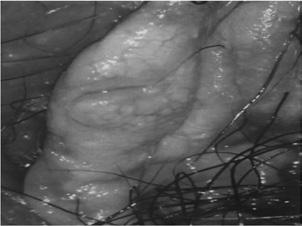
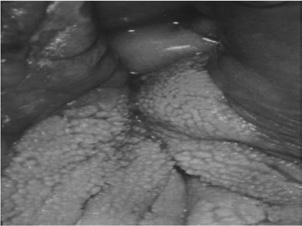
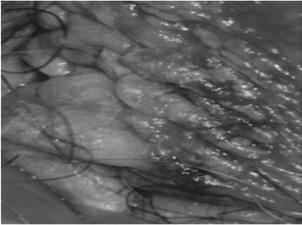
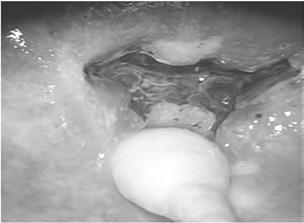
6 Anita L. Nelson, MD 31 Anita L. Nelson, MD year old, obese G 5 P 4 Ab woman referred in for abnormal pap smear. After challenging placement of the speculum, this is what you can see. Anita L. Nelson, MD 34 Anita L. Nelson, MD 35 What tricks do you have to improve visualization of her cervix? Anita L. Nelson, MD 36 Anita L. Nelson, MD 37 6





7 CN is a 21 year old G 3 P 0 Ab 3 woman whose pap smear returns ASC-US. She had coarche at age 13 and has had 6 lifetime partners. At age 14, she had EGW that required multiple treatments with TCA and cryotherapy to eradicate. She wants you to test to see if she has HPV. How do you manage her? Anita L. Nelson, MD 38 Anita L. Nelson, MD 39 ASC-US or LSIL Age Anita L. Nelson, MD 40 Anita L. Nelson, MD 41 Anita L. Nelson, MD 42 Anita L. Nelson, MD 43 7


8 So young, but so worrisome, 21 year old with history of sexual debut 2 years ago has HSIL on her first pap. Anita L. Nelson, MD 44 Anita L. Nelson, MD 45 More Worrisome? Would you be more worried if you learned that she had been sexually abused at age 12 and has not been able to have sexual relations since then? Anita L. Nelson, MD 46 Anita L. Nelson, MD 47 A 67 year old G 7 P 7 woman who has never had a pap smear test is referred for well woman care. She denies any recent abnormal bleeding, vaginal discharge or sexual contact for last 12 years. She has never smoked tobacco or consumed alcohol. What examinations and tests should she have to evaluate for pelvic organ carcinoma? A. No tests B. Cytology test C. Cytology test + HP-HPV test D. Colposcopy Conditions for Discontinuation for Cervical Cytology Discontinuation 3 consecutive normal pap smears with satisfactory samples in last 10 years No abnormal tests in that time frame No CIN2 in last 20 years Anita L. Nelson, MD 48 Anita L. Nelson, MD 49 8



9 What would you do if your examination revealed a 5 mm cervical polyp? What would you do if you found an exophytic lesion on the anterior lip of her cervix? Anita L. Nelson, MD 50 Anita L. Nelson, MD 51 A 29 year old woman with LSIL on pap smear. No previously abnormal pap smears. New sex partner 9 months ago. No HPV test was done. What should we do next. Management of Women with Low-Grade LSIL A. HPV testing B. Colposcopy C. Repeat testing in 12 months Anita L. Nelson, MD 52 Anita L. Nelson, MD 53 Anita L. Nelson, MD 54 Anita L. Nelson, MD 55 9




10 Anita L. Nelson, MD 56 Anita L. Nelson, MD 57 If colposcopy failed to identify any suspicious lesions and her ECC is negative, which of the following is recommended? No Lesion or CIN 1 Proceeded by Lesser Abnormalities A. Repeat colposcopy with blind biopsies B. Repeat pap every 6 months X 2 C. Cotesting at 12 months D. Look and LEEP Anita L. Nelson, MD 58 Anita L. Nelson, MD year old woman with pap smear with ASC-H underwent colposcopy. No lesions were seen on inspection of the cervix and ECC showed no dysplasia. Would you do A. Repeat pap in 6 and 12 months B. Co-testing at 6 and 12 months C. Repeat colposcopy, on cervix and vagina with blind cervical biopsies D. Other Anita L. Nelson, MD 60 Anita L. Nelson, MD 61 10

11 No Lesions or CIN 1 Preceded by ASC-H or HSIL What if Leukoplakia Found? Anita L. Nelson, MD 62 Anita L. Nelson, MD 63 What if Noncervical Lesions Were Seen? Anita L. Nelson, MD 64 Anita L. Nelson, MD 65 Now What? A 23 year old woman with repeat pap smear with LSIL. At age 21 she had LSIL on pap smear. Her colposcopy exam at the time was reported as being satisfactory and a cervical biopsy showed CIN1. Last year her pap smear was ASC-US, so repeat pap was done this year. Now what do we do? Anita L. Nelson, MD 66 Anita L. Nelson, MD 67 11




12 Women Age With No Lesions Or CIN 1 Anita L. Nelson, MD 68 Anita L. Nelson, MD 69 What if... Her next biopsy returns as CIN1 again? How long can this watch and wait process go on? Why? Anita L. Nelson, MD 70 Anita L. Nelson, MD 71 Climbing Higher, Higher A 52 year old woman with HSIL after years without any screening. Colposcopic exam was unsatisfactory. Biopsy was CIN1 and ECC was negative. What are your treatment options? Choose all the apply A. Cytology at 6 and 12 months B. Co-testing at 12 and 24 months C. Diagnostic excision procedure D. Review cytology, histological and colposcopic findings Anita L. Nelson, MD 72 Anita L. Nelson, MD 73 12



13 No Lesions or CIN 1 Preceded by ASC-H or HSIL Climbing Higher, Higher What if her ECC were inadequate? What would your options be then? Check all the apply: A. Cytology at 6 and 12 months B. Co-testing at 12 and 24 months C. Diagnostic excision procedure D. Review cytology, histological and colposcopic findings Anita L. Nelson, MD 74 Anita L. Nelson, MD 75 More About ECCs A 22 year old with ASC-H has CIN1 biopsy and ECC with CIN1. What are her treatment options? Check all that apply. A. Cytology at 6 and 12 months B. Cytology and colposcopy every 6 months x 4 a. Biopsy if high grade lesion persists for > 1 year C. Cytology, colposcopy and ECC every 6 months x 4 a. Biopsy if high grade lesion persists for > 1 year Anita L. Nelson, MD 76 Anita L. Nelson, MD 77 Young Woman Again: Border Cases A 24 year old woman has a pap smear with LSIL. The following year, her pap smear is LSIL again. Now what do you do? Management of Women with Atypical Squamous Cells A. Repeat cytology in 1 year B. Colposcopy Anita L. Nelson, MD 78 Anita L. Nelson, MD 79 13


14 Management of Women with Low-Grade LSIL Oops! A 47 year old woman presents with HSIL. Her colposcopy was not satisfactory. A diagnostic LEEP cone was performed as was an ECC above the LEEP site. Hemostasis was challenging. Her remaining cervical length is 2.5 cm. Her ECC was unsatisfactory. What are your treatment options? Check all that apply: A. Cytology at 6 and 12 months B. Co-testing at 12 and 24 months C. Cytology and ECC at 4-6 months D. Repeat diagnostic excisional procedure E. Hysterectomy Anita L. Nelson, MD 80 Anita L. Nelson, MD 81 Anita L. Nelson, MD 82 Anita L. Nelson, MD 83 A 32 year old woman G3P2 at 8 weeks gestational age reports she has missed her paps since her last pregnancy 4 years ago. She says she was told her pap was not normal, but they would look into the problem after she delivered. She figured it probably was not very serious because they never got back to her. Her pap is now HSIL. A. What are your options? B. What is the purpose of your evaluation? C. What are your challenges? D. What tests are you allowed to perform? Anita L. Nelson, MD 84 Anita L. Nelson, MD 85 14



:346-55. Anita L.")
15 Colposcopic Principles in Pregnancy Limit biopsy to lesions suspicious for CIN2, 3 or cancer Biopsy not linked to fetal loss or preterm labor ECC is contraindicated in pregnancy CIN2 or CIN3 on biopsy rarely progress to invasive cancer during first months of pregnancy Re-evaluation during pregnancy may prompt needless intervention Observation until postpartum period safe and reasonable provided cancer has been ruled out Anita L. Nelson, MD 86 Management of ASC-US Pregnant women > 20 years Reflex HR-HPV testing Repeat cytology Colposcopy may be deferred until at least 6 weeks postpartum If colposcopy done, biopsy only lesions suspicious for invasive carcinoma Wright TC Jr, et al. Am J Obstet Gynecol. 2007;197(4): Anita L. Nelson, MD 87 Anita L. Nelson, MD 88 Anita L. Nelson, MD 89 Anita L. Nelson, MD 90 Anita L. Nelson, MD 91 15




16 Management of LSIL in Pregnant Woman > 20 Years Colposcopy is preferred Biopsy only lesions suspicious for invasive disease ECC unacceptable If no high grade lesions seen, repeat evaluation 6 weeks postpartum If high grade lesion seen, repeating colposcopy periodically until delivery may be helpful Deferring colposcopy until 6 weeks postpartum is acceptable Wright TC Jr, et al. Am J Obstet Gynecol. 2007;197(4): Anita L. Nelson, MD 92 Anita L. Nelson, MD 93 Anita L. Nelson, MD 94 Anita L. Nelson, MD 95 Anita L. Nelson, MD 96 Anita L. Nelson, MD 97 16


17 Management of HSIL in Pregnancy Colposcopy necessary to rule out invasive disease Biopsy lesions with features that can not confidentially exclude invasive disease Endocervical curettage not acceptable If colposcopy satisfactory and no invasive disease Repeat colposcopy and cytology in 8-12 weeks Anticipate vaginal delivery Repeat full evaluation at 8-12 weeks postpartum If lesion resolved, repeat 2 tests Q 6 months for 2 years Anita L. Nelson, MD 98 Anita L. Nelson, MD 99 Anita L. Nelson, MD 100 Anita L. Nelson, MD 101 Management of HSIL in Pregnancy If colposcopy not satisfactory Repeat colposcopy periodically until Satisfactory or GA of 28 weeks, when can consider cone biopsy Anita L. Nelson, MD 102 Details of Management of Abnormal Cytology Tests During Pregnancy AGC and AIS Colposcopy recommended Cervical biopsy of suspicious lesions HR-HPV testing preferred at time of colposcopy for AGC-NOS Endocervical cuttage and endometrial biopsy are unacceptable Postpartum re-evaluation at 6 weeks Wright TC Jr, et al. Am J Obstet Gynecol. 2007;197(4): Anita L. Nelson, MD
:137-48. Anita L.")


18 Physiologic Effects of Pregnancy Colposcopic Challenges Cervical mucus obscures visualization Cervical hyperemia Gland prominence Eversion of columnar epithelium SCJ difficult to visualize early Everts later Fleury AC, et al. Minerca Ginecol. 2012;64(2): Anita L. Nelson, MD 104 Management of CIN or AIS During Pregnancy: Considerations Risk of progression of CIN 2,3 to invasive cancer during pregnancy is minimal Rate of regression postpartum is relatively high Treatment of CIN during pregnancy is associated with Complications-bleeding, infection, abortion High rate of recurrence/persistence CIN and AIS should not affect route of delivery Wright TC, et al. Am J Obstet Gynecol. 2007;197(4): Anita L. Nelson, MD 105 Natural History Dysplasia in Pregnancy 65 women followed postpartum Remission 40.0% Partial remission 4.6% Persistence 26.2% Progression 3.0% 4.4% miscarried 71.1% Delivered vaginally Henes M, et al. Anticancer Res. 2013;3(2): Anita L. Nelson, MD 106 Anita L. Nelson, MD 107 Anita L. Nelson, MD 108 Anita L. Nelson, MD



19 Anita L. Nelson, MD 110 Anita L. Nelson, MD 111 Anita L. Nelson, MD 112 Anita L. Nelson, MD 113 Anita L. Nelson, MD 114 Anita L. Nelson, MD
20 Colposcopy Indicated For... Ablation or Excision for... ASC-US + HPV women over 25 LSIL women over 25 ASC-H women all ages HSIL women all ages AGC (with ECC +/- EMB) AIS (with ECC +/- EMB) Histology of CIN2, CIN3, CIN2, 3 with adequate colposcopy Anita L. Nelson, MD 116 Anita L. Nelson, MD 117 Repeat Co-Testing for: HPV and cytology in 30 years Negative colposcopy in HPV ASC-US CIN1 in women < 25 years with lesser abnormalcies pap Repeat co-testing in 3 years ASC-US with HPV Follow-up negative co-testing, negative colposcopy in HPV, ASC-US Treatment CIN1 Unacceptable Pregnant women Women years Anita L. Nelson, MD 118 Anita L. Nelson, MD 119 Repeat Cytology Only Diagnostic Excision Procedure Repeat cytology in 12 months Women ASC-US LSIL HSIL with inadequate colposcopy Except in pregnancy Except in women Anita L. Nelson, MD 120 Anita L. Nelson, MD


21 Anita L. Nelson, MD 122 Anita L. Nelson, MD 123 Anita L. Nelson, MD
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests
 ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two
 Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$
*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$") !"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
Management Algorithms for Abnormal Cervical Cytology and Colposcopy
 Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Case Based Problems. Recommended Guidelines. Workshop: Case Management of Abnormal Pap Smears and Colposcopies. Disclosure
 Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines
 Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Cervical Cancer 4/27/2016
 Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Eradicating Mortality from Cervical Cancer
 Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
The society for lower genital tract disorders since 1964.
 The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
I have no financial interests to disclose.
 Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics I have no financial interests
Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics I have no financial interests
Management of Abnormal Cervical Cytology and Histology
 Management of Abnormal Cervical Cytology and Histology Assoc. Prof. Gökhan Tulunay Etlik Zübeyde Hanım Women s Diseases Teaching & Research Hospital Gynecologic Oncology Clinic Universally accepted guideline
Management of Abnormal Cervical Cytology and Histology Assoc. Prof. Gökhan Tulunay Etlik Zübeyde Hanım Women s Diseases Teaching & Research Hospital Gynecologic Oncology Clinic Universally accepted guideline
Dysplasia: layer of the cervical CIN. Intraepithelial Neoplasia. p16 immunostaining. 1, Cervical. Higher-risk, requires CIN.
 CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
HPV and Cervical Cancer, Screening and Prevention. John Ragsdale, MD July 12, 2018 CME Lecture Series
 HPV and Cervical Cancer, Screening and Prevention John Ragsdale, MD July 12, 2018 CME Lecture Series We have come a long Way Prevalence HPV in Young Adults in U.S HPV genotypes 55-60% of All cancers 20%
HPV and Cervical Cancer, Screening and Prevention John Ragsdale, MD July 12, 2018 CME Lecture Series We have come a long Way Prevalence HPV in Young Adults in U.S HPV genotypes 55-60% of All cancers 20%
Making Sense of Cervical Cancer Screening
 Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
No Disclosures. Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results. Objectives 5/9/2016
 Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
Cervical Cancer Screening Update. Melissa Hartman, DO Women s Health
 Cervical Cancer Screening Update Melissa Hartman, DO Women s Health Previous Cervical Cancer Screening Organization Recommendation ACS (2011) ACP (2008) NCI (2003) Age 21 or 3 years after first intercourse
Cervical Cancer Screening Update Melissa Hartman, DO Women s Health Previous Cervical Cancer Screening Organization Recommendation ACS (2011) ACP (2008) NCI (2003) Age 21 or 3 years after first intercourse
Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches.
 Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches. Fadi W. Abdul-Karim MD MEd. Professor of Pathology. Vice chair for education. Robert Tomsich Pathology and Lab Med
Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches. Fadi W. Abdul-Karim MD MEd. Professor of Pathology. Vice chair for education. Robert Tomsich Pathology and Lab Med
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary
 Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
Samuel B. Wolf, D.O., F.A.C.O.G. Emerald Coast Obstetrics and Gynecology Panama City Florida
 Making sense of the new Pap smear screening guidelines. Samuel B. Wolf, D.O., F.A.C.O.G. Emerald Coast Obstetrics and Gynecology Panama City Florida Case 17 year old G1P0010 with first sexual encounter
Making sense of the new Pap smear screening guidelines. Samuel B. Wolf, D.O., F.A.C.O.G. Emerald Coast Obstetrics and Gynecology Panama City Florida Case 17 year old G1P0010 with first sexual encounter
Management that provides continuity of care for women
 Management that provides continuity of care for women If women are diagnosed with reproductive tract infection, prompt treatment should be instituted according to the WHO guidelines. Though it may be preferred
Management that provides continuity of care for women If women are diagnosed with reproductive tract infection, prompt treatment should be instituted according to the WHO guidelines. Though it may be preferred
Becoming a colposcopist: Colposcope case studies
 Becoming a colposcopist: Colposcope case studies Seon-Kyung Lee, M.D. Department of Obstetrics and Gynecology College of Medicine, Kyung Hee University Value of Colposcopy Cytology is an effective screening
Becoming a colposcopist: Colposcope case studies Seon-Kyung Lee, M.D. Department of Obstetrics and Gynecology College of Medicine, Kyung Hee University Value of Colposcopy Cytology is an effective screening
Cervical Cancer Screening Guidelines Update
 Frontier AIDS Education and Training Center Cervical Cancer Screening Guidelines Update Hillary Liss, MD Harborview Medical Center, Madison and Adult Medicine Clinics Frontier AETC, Medical Program Director
Frontier AIDS Education and Training Center Cervical Cancer Screening Guidelines Update Hillary Liss, MD Harborview Medical Center, Madison and Adult Medicine Clinics Frontier AETC, Medical Program Director
Managament of Abnormal Cervical Cytology and Histology
 Managament of Abnormal Cervical Cytology and Histology Ali Ayhan, M.D Başkent University Faculty of Medicine Department of Gynecology and Obstetrics Division of Gynecologic Oncology Abnormal Cytologic
Managament of Abnormal Cervical Cytology and Histology Ali Ayhan, M.D Başkent University Faculty of Medicine Department of Gynecology and Obstetrics Division of Gynecologic Oncology Abnormal Cytologic
Over-diagnoses in Cytopathology: Is histology the gold standard?
 Over-diagnoses in Cytopathology: Is histology the gold standard? Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M. Darragh,
Over-diagnoses in Cytopathology: Is histology the gold standard? Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M. Darragh,
SESSION J4. What's Next? Managing Abnormal PAPs in 2014
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
Treatment of Cervical Intraepithelial Neoplasia. Case. How would you manage this woman?
 Treatment of Cervical Intraepithelial Neoplasia Karen Smith-McCune Professor, Department of Obstetrics, Gynecology and Reproductive Sciences I have no conflicts of interest Case How would you manage this
Treatment of Cervical Intraepithelial Neoplasia Karen Smith-McCune Professor, Department of Obstetrics, Gynecology and Reproductive Sciences I have no conflicts of interest Case How would you manage this
Cervical Cancer Screening. David Quinlan December 2013
 Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Cervical Cancer Screening
 Todd R. Jenkins, MD, MSHA Senior Vice Chair Director, Division of Women s Reproductive Healthcare Learning Objectives Describe the etiology, natural history, and usage of the human papillomavirus (HPV)
Todd R. Jenkins, MD, MSHA Senior Vice Chair Director, Division of Women s Reproductive Healthcare Learning Objectives Describe the etiology, natural history, and usage of the human papillomavirus (HPV)
I have no financial interests in any product I will discuss today.
 Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Colposcopy. Attila L Major, MD, PhD
 Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Objectives. I have no financial interests in any product I will discuss today. Cervical Cancer Screening Guidelines: Updates and Controversies
 Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Your Colposcopy Visit
 Introduction Welcome to the colposcopy clinic. This booklet tells you about. The colposcopy examination.. Tests that are done in the colposcopy clinic.. What these tests look for Take a few minutes to
Introduction Welcome to the colposcopy clinic. This booklet tells you about. The colposcopy examination.. Tests that are done in the colposcopy clinic.. What these tests look for Take a few minutes to
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 09/5/95 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 09/5/95 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines. June 2013
 Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D.
 Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D. 27 May, 2014 London, England Faculty Disclosure X No, nothing to disclose Yes, please specify
Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D. 27 May, 2014 London, England Faculty Disclosure X No, nothing to disclose Yes, please specify
Cervical Dysplasia and HPV
 Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
SOGC / SCC Clinical Practice Guideline
 SOGC / SCC Clinical Practice Guideline Colposcopic Management of Abnormal Cervical Cancer Screening and Histology These Clinical Practice Guidelines have been prepared and approved by the Executive and
SOGC / SCC Clinical Practice Guideline Colposcopic Management of Abnormal Cervical Cancer Screening and Histology These Clinical Practice Guidelines have been prepared and approved by the Executive and
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT
 PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0 / 0 / 6 ANY MISSING OR INCOMPLETE TEST RESULTS
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0 / 0 / 6 ANY MISSING OR INCOMPLETE TEST RESULTS
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0/0/0 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0/0/0 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
Cervical Conization. 1
 Cervical Conization www.zohrehyousefi.com 1 Cone Biopsy is a surgical procedure with removal of a cone shaped portion of the cervix The extent of involvement of epithelium on the ectocervix has been clearly
Cervical Conization www.zohrehyousefi.com 1 Cone Biopsy is a surgical procedure with removal of a cone shaped portion of the cervix The extent of involvement of epithelium on the ectocervix has been clearly
Running head: EVIDENCE-BASED MEDICINE TWO-STEP DISCREPANCY
 Evidence-Based Medicine Two-Step Discrepancy 1 Running head: EVIDENCE-BASED MEDICINE TWO-STEP DISCREPANCY Evidence-Based Medicine Two-Step Discrepancy Julie Nelson Texas Woman s University Philosophy of
Evidence-Based Medicine Two-Step Discrepancy 1 Running head: EVIDENCE-BASED MEDICINE TWO-STEP DISCREPANCY Evidence-Based Medicine Two-Step Discrepancy Julie Nelson Texas Woman s University Philosophy of
Chapter 10: Pap Test Results
 Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
Introduction to Colposcopy
 Introduction to Colposcopy Papanicolaou smear (Pap smear) screening test Colposcopy diagnostic test Introduction to Colposcopy Acetic acid and Lugol s iodine applied Cervix examined under magnification
Introduction to Colposcopy Papanicolaou smear (Pap smear) screening test Colposcopy diagnostic test Introduction to Colposcopy Acetic acid and Lugol s iodine applied Cervix examined under magnification
Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages years
 Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages 21-39 years Michelle I. Silver, PhD, ScM Cancer Prevention Fellow National Cancer Institute Division of Cancer
Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages 21-39 years Michelle I. Silver, PhD, ScM Cancer Prevention Fellow National Cancer Institute Division of Cancer
Cervical Screening for Dysplasia and Cancer in Patients with HIV
 Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 08/5/94 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 08/5/94 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
9/18/2008. Cervical Cancer Prevention for Adolescent Populations Garcia. Faculty disclosure. Objectives. HPV Positivity by Age (UK)
") Faculty disclosure Cervical Cancer Prevention for Francisco, MD, MPH Associate Professor Obstetrics & Gynecology Mexican American Studies Public Health Francisco, MD, MPH has no financial affiliations
Faculty disclosure Cervical Cancer Prevention for Francisco, MD, MPH Associate Professor Obstetrics & Gynecology Mexican American Studies Public Health Francisco, MD, MPH has no financial affiliations
Cervical Cancer Screening
 Cervical Cancer Screening MEGAN CHENEY, MD MPH MEDICAL DIRECTOR, THE WOMEN S CENTER ASSISTANT DIRECTOR, BGSMC OBGYN RESIDENCY PROGRAM SECTION CHIEF, THE WOMEN S HEALTH INSTITUTE Objectives Understand proper
Cervical Cancer Screening MEGAN CHENEY, MD MPH MEDICAL DIRECTOR, THE WOMEN S CENTER ASSISTANT DIRECTOR, BGSMC OBGYN RESIDENCY PROGRAM SECTION CHIEF, THE WOMEN S HEALTH INSTITUTE Objectives Understand proper
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES TREATMENT FORM FORM L16
 WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES TREATMENT FORM FORM L16 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 05/01/95 ANY MISSING OR INCOMPLETE TEST RESULTS
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES TREATMENT FORM FORM L16 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 05/01/95 ANY MISSING OR INCOMPLETE TEST RESULTS
Human Papillomavirus (HPV) and Cervical Cancer Prevention
 and Cervical Cancer Prevention") Human Papillomavirus (HPV) and Cervical Cancer Prevention MOA Autumn Convention November 3, 2017 David J Boes, DO, FACOOG (Dist.) Associate Professor, MSU-COM 1 Disclosures None relative to this presentation
Human Papillomavirus (HPV) and Cervical Cancer Prevention MOA Autumn Convention November 3, 2017 David J Boes, DO, FACOOG (Dist.) Associate Professor, MSU-COM 1 Disclosures None relative to this presentation
VIN/VAIN O C T O B E R 3 RD J M O R G A N
 VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
Human Papillomavirus
 Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
BC Cancer Cervix Screening 2015 Program Results. February 2018
 BC Cancer Cervix Screening 2015 Program Results BC Cancer Cervix Screening 2015 Program Results 2 Table of Contents BC Cancer Cervix Screening 2015 Program Results... 1 Table of Contents... 2 Program Overview...
BC Cancer Cervix Screening 2015 Program Results BC Cancer Cervix Screening 2015 Program Results 2 Table of Contents BC Cancer Cervix Screening 2015 Program Results... 1 Table of Contents... 2 Program Overview...
Associate Professor of Gyn. & Obs., Department of Gynecology and Obstetrics, Tehran University of Medical Sciences, Iran.
 Assessment of Visual Inspection with Acetic Acid (VIA) as a Screening Test for Cervical Neoplasia in Comparison with Cytologic Screening in Imam Khomeini Hospital F. Ghaemmaghami, MD Associate Professor
Assessment of Visual Inspection with Acetic Acid (VIA) as a Screening Test for Cervical Neoplasia in Comparison with Cytologic Screening in Imam Khomeini Hospital F. Ghaemmaghami, MD Associate Professor
Cervical Testing and Results Management. An Evidenced-Based Approach April 22nd, Debora Bear, MSN, MPH
 Cervical Testing and Results Management An Evidenced-Based Approach April 22nd, 2010 Debora Bear, MSN, MPH Assistant Medical Director for Planned Parenthood of New Mexico, Inc. Burden of cervical cancer
Cervical Testing and Results Management An Evidenced-Based Approach April 22nd, 2010 Debora Bear, MSN, MPH Assistant Medical Director for Planned Parenthood of New Mexico, Inc. Burden of cervical cancer
Update on Cervical Cancer Screening. Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014
 Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Update on Cervical Cancer Screening
 Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Understanding Your Pap Test Results
 Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
Update on HPV Testing. Robert Schlaberg, M.D., Dr. med., M.P.H. Assistant Professor, University of Utah Medical Director, ARUP Laboratories
 Update on HPV Testing Robert Schlaberg, M.D., Dr. med., M.P.H. Assistant Professor, University of Utah Medical Director, ARUP Laboratories Disclosures In accordance with ACCME guidelines, any individual
Update on HPV Testing Robert Schlaberg, M.D., Dr. med., M.P.H. Assistant Professor, University of Utah Medical Director, ARUP Laboratories Disclosures In accordance with ACCME guidelines, any individual
Disclosures. Learning objectives. George F. Sawaya, MD. I have nothing to disclose.
 Well Woman Visits in 2018: How Should We Approach Cervical Cancer Screening and Routine Pelvic Examinations? George F. Sawaya, MD Disclosures I have nothing to disclose. Professor, Obstetrics, Gynecology
Well Woman Visits in 2018: How Should We Approach Cervical Cancer Screening and Routine Pelvic Examinations? George F. Sawaya, MD Disclosures I have nothing to disclose. Professor, Obstetrics, Gynecology
 1 Cervical Cancer Prevention and Screening: Update 2010 Michael S. Policar, MD, MPH Clinical Professor of Ob, Gyn, and RS UCSF School of Medicine policarm@obgyn.ucsf.edu No commercial disclosures for this
1 Cervical Cancer Prevention and Screening: Update 2010 Michael S. Policar, MD, MPH Clinical Professor of Ob, Gyn, and RS UCSF School of Medicine policarm@obgyn.ucsf.edu No commercial disclosures for this
HKCOG GUIDELINES NUMBER 3 (revised November 2002) published by The Hong Kong College of Obstetricians and Gynaecologists
 published by The Hong Kong College of Obstetricians and Gynaecologists") HKCOG Guidelines Guidelines on the Management of An Abnormal Cervical Smear Number 3 revised November 2002 published by The Hong Kong College of Obstetricians and Gynaecologists A Foundation College of
HKCOG Guidelines Guidelines on the Management of An Abnormal Cervical Smear Number 3 revised November 2002 published by The Hong Kong College of Obstetricians and Gynaecologists A Foundation College of
An Update on Cervical Cancer Screening Recommendations and on the DOH BCC Program
 An Update on Cervical Cancer Screening Recommendations and on the DOH BCC Program Susan Baum, MD, MPH NM Nurse Practitioner Council Annual Conference April 20, 2012 I have no commercial relationships related
An Update on Cervical Cancer Screening Recommendations and on the DOH BCC Program Susan Baum, MD, MPH NM Nurse Practitioner Council Annual Conference April 20, 2012 I have no commercial relationships related
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA
 Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal
 Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
Cuid d Fheidhmeannacht na Seirbhíse Sláinte. Part of the Health Service Executive. CS/PR/PM-20 Rev 2 ISBN Programme Report 2014/2015
 Programme Report 2014/2015 Contents Summary points 2 Introduction to the statistics 2014/2015 3 Part 1 Cervical screening activity 3 Programme coverage 4 Laboratory turnaround time 7 Notification of results
Programme Report 2014/2015 Contents Summary points 2 Introduction to the statistics 2014/2015 3 Part 1 Cervical screening activity 3 Programme coverage 4 Laboratory turnaround time 7 Notification of results
Goals. In the News. Primary HPV Screening 3/9/2015. Your PAP and HPV Update Primary HPV Testing- Screening Intervals- HPV Vaccine Updates-
 Your PAP and HPV Update 2015 Connie Mao, MD University of Washington Goals Primary HPV Testing- Is it time to stop doing pap smears? Screening Intervals- Should patients have a choice? HPV Vaccine Updates-
Your PAP and HPV Update 2015 Connie Mao, MD University of Washington Goals Primary HPV Testing- Is it time to stop doing pap smears? Screening Intervals- Should patients have a choice? HPV Vaccine Updates-
CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN)
") CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN) The cervix constitutes the lower third of the uterus. It is in two parts, the endocervix and the ectocervix. Ectocervix is covered with squamous epithelium. Endocervix
CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN) The cervix constitutes the lower third of the uterus. It is in two parts, the endocervix and the ectocervix. Ectocervix is covered with squamous epithelium. Endocervix
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma
 Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
What is a Pap Smear and What do the results mean? Maria E Daheri RN Cervical Nurse Case Harris Health System
 What is a Pap Smear and What do the results mean? Maria E Daheri RN Cervical Nurse Case Manager @ Harris Health System What is a Pap Smear and when is it recommended? Pap smear The Pap smear is a screening
What is a Pap Smear and What do the results mean? Maria E Daheri RN Cervical Nurse Case Manager @ Harris Health System What is a Pap Smear and when is it recommended? Pap smear The Pap smear is a screening
News. Laboratory NEW GUIDELINES DEMONSTRATE GREATER ROLE FOR HPV TESTING IN CERVICAL CANCER SCREENING TIMOTHY UPHOFF, PHD, DABMG, MLS (ASCP) CM
 CM") Laboratory News Inside This Issue NEW GUIDELINES DEMONSTRATE GREATER ROLE FOR HPV TESTING IN CERVICAL CANCER SCREENING...1 NEW HPV TEST METHODOLOGY PROVIDES BETTER SPECIFICITY FOR CERVICAL CANCER...4 BEYOND
Laboratory News Inside This Issue NEW GUIDELINES DEMONSTRATE GREATER ROLE FOR HPV TESTING IN CERVICAL CANCER SCREENING...1 NEW HPV TEST METHODOLOGY PROVIDES BETTER SPECIFICITY FOR CERVICAL CANCER...4 BEYOND
The LAST Guidelines in Clinical Practice. Implementing Recommendations for p16 Use
 AJCP / Original Article The LAST Guidelines in Clinical Practice Implementing Recommendations for p16 Use Lani K. Clinton, MD, PhD, 1,2 Kyle Miyazaki, 1 Asia Ayabe, 1 James Davis, PhD, 2 Pamela Tauchi-Nishi,
AJCP / Original Article The LAST Guidelines in Clinical Practice Implementing Recommendations for p16 Use Lani K. Clinton, MD, PhD, 1,2 Kyle Miyazaki, 1 Asia Ayabe, 1 James Davis, PhD, 2 Pamela Tauchi-Nishi,
COLPOSCOPY MADE EASY AND SIMPLE
 COLPOSCOPY MADE EASY AND SIMPLE Burton Brodsky M.D. Husband, father of four kids Chief of gynecology University of Toledo Assistant residency director University of Toledo Associate professor university
COLPOSCOPY MADE EASY AND SIMPLE Burton Brodsky M.D. Husband, father of four kids Chief of gynecology University of Toledo Assistant residency director University of Toledo Associate professor university
Sydney Gynaecology Oncology Group, Sydney Cancer Centre, Royal Prince Alfred Hospital, Camperdown, New South Wales, Australia
 bs_bs_banner doi:10.1111/jog.12545 J. Obstet. Gynaecol. Res. Vol. 41, No. 3: 440 444, March 2015 Abnormal cervicovaginal cytology, unsatisfactory colposcopy and the use of vaginal estrogen cream: An observational
bs_bs_banner doi:10.1111/jog.12545 J. Obstet. Gynaecol. Res. Vol. 41, No. 3: 440 444, March 2015 Abnormal cervicovaginal cytology, unsatisfactory colposcopy and the use of vaginal estrogen cream: An observational
Human Papillomavirus. Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita
 Human Papillomavirus Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita What is Genital HPV Infection Human papillomavirus is
Human Papillomavirus Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita What is Genital HPV Infection Human papillomavirus is
CPC on Cervical Pathology
 CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
The new Cervical Screening Test for Australian women: Louise Farrell
 The new Cervical Screening Test for Australian women: Louise Farrell Outline and explain the changes to the National Cervical Screening Program due to commence in Dec 2017 LEARNING OBJECTIVES FOR TODAY
The new Cervical Screening Test for Australian women: Louise Farrell Outline and explain the changes to the National Cervical Screening Program due to commence in Dec 2017 LEARNING OBJECTIVES FOR TODAY
Cervical Precancer: Evaluation and Management
 TAJ June 2002; Volume 15 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Review fam Cervical Precancer: Evaluation and Management SM Khodeza Nahar Begum 1 Abstract Carcinoma of
TAJ June 2002; Volume 15 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Review fam Cervical Precancer: Evaluation and Management SM Khodeza Nahar Begum 1 Abstract Carcinoma of
Manitoba Cervical Cancer Screening Program. Operations & Statistical Report and 2006
 anitoba Cervical Cancer Screening Program Operations & Statistical Report 2005 and 2006 1 MCCSP 2005-2006 Report ANITOBA CERVICAL CANCER SCREENING PROGRAM 2005 and 2006 Operations & Statistical Report
anitoba Cervical Cancer Screening Program Operations & Statistical Report 2005 and 2006 1 MCCSP 2005-2006 Report ANITOBA CERVICAL CANCER SCREENING PROGRAM 2005 and 2006 Operations & Statistical Report
Jean Anderson, MD Catherine Sewell, MD, MPH
 Jean Anderson, MD Catherine Sewell, MD, MPH To review diagnosis and management of HPV disease in the setting of HIV infection and address controversies HIV-infected women have: higher prevalence and incidence
Jean Anderson, MD Catherine Sewell, MD, MPH To review diagnosis and management of HPV disease in the setting of HIV infection and address controversies HIV-infected women have: higher prevalence and incidence
Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination. Dr Stella Heley Senior Liaison Physician Victorian Cytology Service
 Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination Dr Stella Heley Senior Liaison Physician Victorian Cytology Service Victorian Cytology Service Dr Stella Heley Dr Siobhan Bourke
Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination Dr Stella Heley Senior Liaison Physician Victorian Cytology Service Victorian Cytology Service Dr Stella Heley Dr Siobhan Bourke
HPV infections and potential outcomes
 CONTENTS Preface by Silvia de Sanjosé... 33 Preface by Jacob Bornstein... 37 Author s note... 39 Acknowledgments... 45 CHAPTER 1 HPV infections and potential outcomes HPV: What it is, where it is and what
CONTENTS Preface by Silvia de Sanjosé... 33 Preface by Jacob Bornstein... 37 Author s note... 39 Acknowledgments... 45 CHAPTER 1 HPV infections and potential outcomes HPV: What it is, where it is and what
Human Papillomaviruses and Cancer: Questions and Answers. Key Points. 1. What are human papillomaviruses, and how are they transmitted?
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Human Papillomaviruses
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Human Papillomaviruses
Lauren O Sullivan, D.O. February 19, 2015
 Lauren O Sullivan, D.O. February 19, 2015 1. Review basics of Pap smear, cervical dysplasia/cancer and HPV infection. 2. Review 2012 updated screening guidelines. 3. Discuss how and where to find updated
Lauren O Sullivan, D.O. February 19, 2015 1. Review basics of Pap smear, cervical dysplasia/cancer and HPV infection. 2. Review 2012 updated screening guidelines. 3. Discuss how and where to find updated
He Said, She Said: HPV and the FDA. Audrey P Garrett, MD, MPH June 6, 2014
 He Said, She Said: HPV and the FDA Audrey P Garrett, MD, MPH June 6, 2014 Disclosure Speaker for Merck Gardasil Speaker for Hologic Thin Prep and Cervista Cervical Cancer Screening: 21 st century Dr. Papanicolaou
He Said, She Said: HPV and the FDA Audrey P Garrett, MD, MPH June 6, 2014 Disclosure Speaker for Merck Gardasil Speaker for Hologic Thin Prep and Cervista Cervical Cancer Screening: 21 st century Dr. Papanicolaou
Name of Policy: Speculoscopy
 Name of Policy: Speculoscopy Policy #: 095 Latest Review Date: September 2011 Category: Medicine/OB Gyn Policy Grade: C Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Speculoscopy Policy #: 095 Latest Review Date: September 2011 Category: Medicine/OB Gyn Policy Grade: C Background/Definitions: As a general rule, benefits are payable under Blue Cross
Focus. A case. I have no conflicts of interest. HPV Vaccination: Science and Practice. Collaborative effort with Karen Smith-McCune, MD, PhD 2/19/2010
 HPV Vaccination: Science and Practice George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics Director, Colposcopy Clinic,
HPV Vaccination: Science and Practice George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics Director, Colposcopy Clinic,
Cervical Cancer Prevention in the 21 st Century Changing Paradigms
 Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
10/31/2017. Disclosures. I. Background: History 1,4. Cervical Cancer Screening and HPV
 Cervical Cancer and Disclosures I have no conflicts of interest to disclose Slides courtesy of : Dr. Sarah Morgan Sukhpreet S. Multani, MD St. Vincent Women s Clinical Assistant Professor, Marian University
Cervical Cancer and Disclosures I have no conflicts of interest to disclose Slides courtesy of : Dr. Sarah Morgan Sukhpreet S. Multani, MD St. Vincent Women s Clinical Assistant Professor, Marian University
Human Papillomavirus (HPV) in Patients with HIV.
 in Patients with HIV.") Human Papillomavirus (HPV) in Patients with HIV www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS residents with HIV who are screened for HPV-related dysplasia and managed effectively.
Human Papillomavirus (HPV) in Patients with HIV www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS residents with HIV who are screened for HPV-related dysplasia and managed effectively.
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Twenty-first refresher course. Chan Kit Sheung
 Twenty-first refresher course Chan Kit Sheung 7-5-2015 Case 1 Case 1, 29y old, G3P2, referred from MCHC Cervical smear on 27-9-2013: LGSIL, defaulted appointment Cervical smear in 12/2014: negative Colposcopy
Twenty-first refresher course Chan Kit Sheung 7-5-2015 Case 1 Case 1, 29y old, G3P2, referred from MCHC Cervical smear on 27-9-2013: LGSIL, defaulted appointment Cervical smear in 12/2014: negative Colposcopy
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics Treatment of Cervical Precancerous Lesions using Thermocoagulation(Cold Coagulation) and Cryotherapy General Principles All high grade CIN should be
International Federation of Gynecology and Obstetrics Treatment of Cervical Precancerous Lesions using Thermocoagulation(Cold Coagulation) and Cryotherapy General Principles All high grade CIN should be
Proposed new national cervical screening program. Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns
 Proposed new national cervical screening program Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns www.drelizabethjackson.com Cervical cancer in Australia 12th most common cancer affecting Australian
Proposed new national cervical screening program Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns www.drelizabethjackson.com Cervical cancer in Australia 12th most common cancer affecting Australian
GLANDULAR LESIONS PITFALLS IN MANAGEMENT. Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016
 GLANDULAR LESIONS PITFALLS IN MANAGEMENT Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016 Introduction Cervical glandular lesions are much less common than squamous lesion Incidence
GLANDULAR LESIONS PITFALLS IN MANAGEMENT Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016 Introduction Cervical glandular lesions are much less common than squamous lesion Incidence
Understand Your Results
 Understand Your Results The Pap test takes little time and may save your life. This simple screening test checks for cell changes in the cervix, the opening of the uterus. If your Pap results were abnormal,
Understand Your Results The Pap test takes little time and may save your life. This simple screening test checks for cell changes in the cervix, the opening of the uterus. If your Pap results were abnormal,