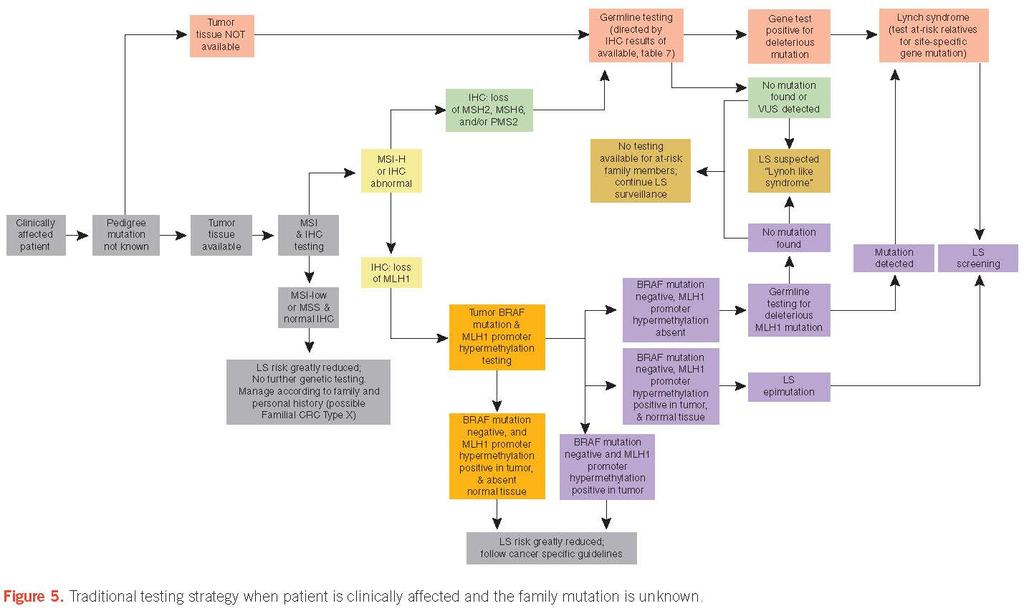
Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer
|
|
|
- Milo Richard
- 6 years ago
- Views:
Transcription
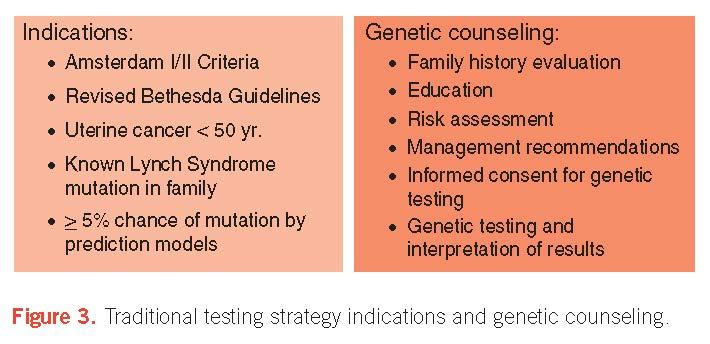
1 s on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer Francis M. Giardiello, MD, 1 John I. Allen, 2 Jennifer E. Axilbund, 1 C. Richard Boland, 3 Carol A. Burke, 4 Randall W. Burt, 5 James M. Church, 4 Jason A. Dominitz, 6,7 David A. Johnson, 8 Tonya Kaltenbach, 9 Theodore R. Levin, 10 David A. Lieberman, 11 Douglas J. Robertson, 12,13 Sapna Syngal, and Douglas K. Rex, 17 1 Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; 2 Yale University School of Medicine, New Haven, Connecticut, USA; 3 Baylor University Medical Center, Dallas, Texas, USA; 4 Cleveland Clinic, Cleveland, Ohio, USA; 5 University of Utah, Salt Lake City, Utah, USA; 6 VA Puget Sound Health Care System, Seattle, Washington, USA; 7 University of Washington, Seattle, Washington, USA; 8 Eastern Virginia Medical School, Norfolk, Virginia, USA; 9 Stanford University, Palo Alto, California, USA; 10 Kaiser Permanente Medical Center, Walnut Creek, California, USA; 11 Oregon Health and Science University, Portland, Oregon, USA; 12 White River Junction VA Medical Center, White River Junction, Vermont, USA; 13 Geisel School of Medicine at Dartmouth, White River Junction, Vermont, USA; 14 Brigham and Women s Hospital, Boston, Massachusetts, USA; 15 Dana Farber Cancer Institute, Boston, Massachusetts, USA; 16 Harvard Medical School, Boston, Massachusetts, USA; 17 Indiana University School of Medicine, Indianapolis, Indiana, USA. Am J Gastroenterol advance online publication, 29 July 2014; doi: /ajg Abstract The Multi-Society Task Force, in collaboration with invited experts, developed guidelines to assist health care providers with the appropriate provision of genetic testing and management of patients at risk for and affected with Lynch syndrome as follows: Figure 1 provides a colorectal cancer risk assessment tool to screen individuals in the office or endoscopy setting; Figure 2 illustrates a strategy for universal screening for Lynch syndrome by tumor testing of patients diagnosed with colorectal cancer; Figures 3 6 provide algorithms for genetic evaluation of affected and at-risk family members of pedigrees with Lynch syndrome; Table 10 provides guidelines for screening at-risk and affected persons with Lynch syndrome; and Table 12 lists the guidelines for the management of patients with Lynch syndrome. A detailed explanation of Lynch syndrome and the methodology utilized to derive these guidelines, as well as an explanation of, and supporting literature for, these guidelines are provided. Introduction Colorectal cancer (CRC) is a major American health problem that ranks as the second leading cause of cancer death after lung cancer. In the United States, approximately 143,000 new cases are diagnosed each year, and 51,000 Americans die annually from this disorder (1). The cause of CRC is multifactorial, with environment and inheritance playing varying roles in different patients (2). Approximately 70 80% of patients with CRC seem to have sporadic disease with no evidence of an inherited disorder. In the remaining 20 30%, a potentially definable inherited component might be causative (3). Lynch syndrome (LS), an autosomal dominant condition, is the most common cause of inherited CRC, accounting for about 3% of newly diagnosed cases of colorectal malignancy (4 8). The eponym Lynch syndrome recognizes Dr Henry T. Lynch, the first author on the original 1966 publication that comprehensively described this condition (9). In the early 1990s, mutation of genes in the DNA mismatch repair (MMR) pathway were implicated as the cause of LS (10 13), and the presence of the mutations now defines the syndrome. Since then,
2 germline testing with increasing sensitivity has been available for patients, as additional genetic discoveries have occurred. When used appropriately, genetic testing for LS can confirm the diagnosis at the molecular level, justify surveillance of at-risk persons, decrease the cost of surveillance by risk stratification, aid in surgical and chemoprevention management, and help in decisions concerning family and career planning. However, when used inappropriately, genetic testing can misinform affected patients with false-negative results and waste patient and societal resources. The goal of this consensus document is to critically analyze the current literature and provide best practice evidence-based recommendations for diagnosis and management strategies to health care providers caring for these patients. Terminology/differential diagnosis HNPCC designates patients and / or families who fulfill the Amsterdam I or II criteria. LS is applied to patients and families in which the genetic basis can be linked to a germline mutation in one of the DNA MMR genes or the EPCAM gene. Lynch-like syndrome describes patients and / or families in which molecular testing demonstrates the presence of MSI and / or abnormalities in the expression of MMR gene proteins on IHC testing of tumor tissue expression, but no pathogenic germline mutation can be found in the patient (e.g., in the absence of a BRAF mutation and / or MLH1 promoter hypermethylation when there is loss of tumor expression of the MLH1 protein). In a recent publication, about half of LLS patients had biallelic somatic mutations of MLH1 or MSH2 to explain the MMR deficient tumors without having causal germline or promotor mutations (68). Table 1. Levels of evidence by national cancer institute levels of evidence for cancer genetic studies Level of evidence Description I Evidence obtained from at least 1 well-designed and wellcontrolled randomized controlled trial that has either: (a) Cancer end point with mortality or incidence, or (b) Intermediate end point II Evidence obtained from well-designed and well-conducted nonrandomized controlled trials that have: (a) Cancer end point (b) Intermediate end point III Evidence obtained from well-designed and well-conducted cohort or case-control studies with: (a) Cancer end point (b) Intermediate end point IV Evidence from descriptive studies with: (a) Cancer end point (b) Intermediate end point V Conclusions from authorities based on clinical experience, descriptive studies and / or expert committees
3 Table 2. Rating of evidence by grades of recommendation, assessment, development, and evaluation methodology Rating of evidence Impact of potential future research Rating of evidence Impact of potential future research A. High quality Very unlikely to change confidence in the estimate of effect B. Moderate Likely to have an important impact on confidence quality and might change estimate of effect C. Low quality Very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate D. Very low quality Any estimate of effect is very uncertain LYNCH SYNDROME CHARACTERISTICS Table 3. Gene-specific cumulative risks of colorectal cancer by age 70 years in Lynch syndrome Gene mutation carriers Risk, % Mean age at diagnosis, y References Sporadic cancer (29) MLH1/MSH2 Male: Female: (17-21,23) MSH6 Male: 22 Female: (17,22) Male and female: 18 PMS2 Male: 20 Female: (25) Table 4. Cumulative risks of extracolorectal cancer by age 70 years in Lynch syndrome Cancer Risk general population, % Risk in LS, % Mean age at diagnosis, y References Endometrium (17 19,21,22,24,25) MLH1/MSH MSH PMS Stomach < (17,40,44 48) Ovary (17,28,39,40,44,46,48) Hepatobiliary tract < (17,28,39,44) Urinary tract < (17,39,40,44,46,48,49) Small bowel < (17,40,44,46,48) Brain/central nervous system < (39,40,44,46) Sebaceous neoplasm <1 1-9 NA (41,42) Pancreas (44,50 52) Prostate (44,48,53,59) Breast (44,48,56,57) NA, Not available.
4 Table 5. Amsterdam I and II criteria for diagnosis of hereditary nonpolyposis colorectal cancer Amsterdam I criteria 1. Three or more relatives with histologically verified colorectal cancer, 1 of which is a first-degree relative of the other two. Familial adenomatous polyposis should be excluded. 2. Two or more generations with colorectal cancer. 3. One or more colorectal cancer cases diagnosed before the age of 50 years. Amsterdam II criteria 1. Three or more relatives with histologically verified HNPCC-associated cancer (colorectal cancer, cancer of the endometrium, small bowel, ureter, or renal pelvis), 1 of which is a first-degree relative of the other 2. Familial adenomatous polyposis should be excluded. 2. Cancer involving at least 2 generations. 3. One or more cancer cases diagnosed before the age of 50 years. Table 6. Revised Bethesda s 1. CRC diagnosed at younger than 50 years. 2. Presence of synchronous or metachronous CRC or other LS-associated tumors. a 3. CRC with MSI-high pathologic-associated features (Crohn-like lymphocytic reaction, mucinous / signet cell differentiation, or medullary growth pattern) diagnosed in an individual younger than 60 years old. 4. Patient with CRC and CRC or LS-associated tumor a diagnosed in at least 1 first-degree relative younger than 50 years old. 5. Patient with CRC and CRC or LS-associated tumor a at any age in 2 first-degree or second-degree relatives. a LS-associated tumors include tumor of the colorectum, endometrium, stomach, ovary, pancreas, ureter, renal pelvis, biliary tract, brain, small bowel, sebaceous glands, and kerotoacanthomas.
5 GENETIC ALTERATIONS Table 7. Sensitivity and specificity for Lynch syndrome utilizing different strategies Sensitivity Specificity (range) (range) Criteria Clinical Amsterdam II criteria Revised Bethesda s Models MMRpredict ( ) 0.82 ( ) 0.98 ( ) 0.77 ( ) References ( 5,6,8,99,100 ) ( 6,7 ) 0.90 ( 5,100 ) ( ) ( ) MMRPro 0.89 ( ) 0.85 ( ) ( 100 ) PREMM1,2, ( ) 0.67 ( ) ( 105 ) Tumor testing MSI 0.85 ( ) IHC 0.83 ( ) 0.90 ( ) 0.89 ( ) ( 107 ) ( 107 ) IDENTIFICATION OF LYNCH SYNDROME

6 GENETIC TESTING Testing for MMR deficiency of newly diagnosed CRC should be performed. This can be done for all CRCs, or CRC diagnosed at age 70 years or younger, and in individuals older than 70 years who have a family history concerning for LS. Analysis can be done by immunohistochemistry (IHC) testing for the MLH1/MSH2/MSH6/PMS2 proteins and/or testing for MSI. Tumors that demonstrate loss of MLH1 should undergo BRAF testing or analysis of MLH1 promoter hypermethylation (Figure 2). To facilitate surgical planning, tumor testing on suspected CRC should be performed on pre-operative biopsy specimens, if possible. This guideline is a strong recommendation, with evidence level III, and GRADE moderate-quality evidence. Individuals who have a personal history of a tumor showing evidence of MMR deficiency (without evidence of MLH1 promoter methylation); uterine cancer diagnosed at younger than age 50 years; a known family MMR gene mutation; fulfill Amsterdam criteria or revised Bethesda guidelines; and / or have a personal risk of 5 % chance of LS based on prediction models should undergo genetic evaluation for LS (Figures 3 6). This guideline is a strong recommendation, with evidence level III, and GRADE moderate-quality evidence.

7

8 LYNCH SYNDROME MANAGEMENT Screening for CRC by colonoscopy is recommended in persons at risk (first-degree relatives of those affected) or affected with LS every 1 to 2 years, beginning between ages years or 2 5 years before the youngest age of diagnosis of CRC in the family if diagnosed before age 25 years. In surveillance of MMR germline mutation-positive patients, consideration should be given to annual colonoscopy. The age of onset and frequency of colonoscopy in this guideline is in agreement with most organizations and authorities (122,131, ). This guideline is a strong recommendation, with evidence level III, and GRADE moderate-quality evidence (Table 10). In carriers of deleterious MSH6 and PMS2 mutations, the risk of CRC is lower and age at diagnosis later (22,25) than in patients with MLH1 and MSH2 mutations. In these affected individuals, consideration could be given to starting screening at age 30 years in MSH6 and 35 years in PMS2 carriers, unless an early-onset cancer exists in a given family. Screening for EC should be offered to women at risk for or affected with LS by pelvic examination and endometrial sampling annually starting at age years (Table 10). The strength of evidence for this guideline is expert consensus level V, GRADE low-quality evidence, and is in concert with other expert opinion (122,137,138). Screening for ovarian cancer should be offered to women at risk for or affected with LS by transvaginal ultrasound annually starting at age years (Table 10). The strength of evidence for this guideline is expert consensus level V and GRADE low-quality evidence. In the absence of data on this issue, several consensus panels have suggested that transvaginal ultrasound for ovarian cancer is a screening consideration in LS (122,137,138).
9 Table 8. Colorectal cancer testing result and additional testing strategies Immunohistochemistry protein expression MSI MLH1 MSH2 MSH6 PMS2 Possible causes Additional tests MSS/MSI-L Sporadic cancer None MSI-H MSI-H NA NA NA NA Germline mutation in MMR or EPCAM genes Sporadic or germline mutation in the MMR or EPCAM genes Consider MLH1, MSH2, then MSH6, PMS2, EPCAM genetic testing Consider IHC to guide germline testing; if IHC is not done germline testing of MLH1, MSH2, MSH6, PMS2, and EPCAM genes MSI-H or NA Sporadic cancer or germline mutation of MLH1 Consider BRAF / MLH1 promoter methylation testing MLH1 genetic + + testing if no BRAF mutation and absent hypermethylation or if testing not done MSI-H or NA Germline mutation MLH1 MLH1 genetic testing MSI-H or NA MSI-H or NA MSI-H or NA MSI-H MSI-L or NA Germline mutation of PMS2, rarely MLH1 Germline mutation of MSH2 or EPCAM, rarely of MSH6 Germline mutation of MSH2 Germline mutation of MSH2 PMS2 genetic testing if negative MLH1 testing Consider MSH2 genetic testing, if negative EPCAM, if negative MSH6 MSH2 genetic testing if negative EPCAM testing MSH6 genetic testing if negative MSH2 testing Note. Adapted from the National Comprehensive Cancer Network Clinical Practice s in Oncology: Colorectal Cancer Screening. Lynch syndrome. Version Available at: (122). MSI-L, microsatellite low; MSI, microsatellite high; MMR, mismatch repair genes (i.e., MLH1, MSH2, MSH6, PMS2); NA, not available; +, protein present in tissue;, protein not present in tissue.
10 Table 10. s for screening at-risk or affected persons with Lynch syndrome Intervention Recommendation Strength of recommendation Colonoscopy Every 1 2 y beginning at age y or 2 5 y younger than youngest age at diagnosis of CRC in family if diagnosis before age 25 y Considerations: Start at age 30 y in MSH6 and 35 in PMS2 families Annual colonoscopy in MMR mutation carriers Strong recommendation: Level of evidence (III): welldesigned and conducted cohort or case-controlled studies from more than 1 group with cancer GRADE rating: moderate Pelvic examination with endometrial sampling Annually beginning at age y Offer to patient: Level of evidence (V): expert consensus GRADE rating: low Transvaginal ultrasound Annually beginning at age y Offer to patient: Level of evidence (V): expert consensus GRADE rating: low EGD with biopsy of the gastric antrum Beginning at age y and subsequent surveillance every 2 3 y can be considered based on patient risk factors Offer to patient: Level of evidence (V): expert consensus GRADE rating: low Urinalysis Annually beginning at age y Consideration: Level of evidence (V): expert consensus GRADE rating: low EGD, esophagogastroduodenoscopy; GRADE, Grades of Recommendation, Assessment, Development, and Evaluation. Hysterectomy and bilateral salpingo-oophorectomy should be recommended to women with LS who have finished childbearing or at age 40 years (Table 12). Patient considerations in this decision could include differences in uterine cancer risk, depending on MMR gene mutation; morbidity of surgery; and the risk of menopausal symptoms, osteoporosis, and cardiac disease if hormone replacement therapy is not given. The strength of evidence for this guideline is observational study level IV and GRADE moderate-quality evidence. This recommendation is in agreement with the Mallorca Group (138). The NCCN recommends considering prophylactic surgery after child bearing is completed (122).
11 Screening for gastric cancer should be considered in persons at risk for or affected with LS by esophagogastroduodenoscopy (EGD) with gastric biopsy of the antrum at age years with treatment of H pylori infection when found. Subsequent, surveillance every 2 3 years can be considered based on individual patient risk factors (Table 10). The strength of evidence for this guideline is expert consensus level V and GRADE low-quality evidence. This guideline is in concert with that of the NCCN (122). The Mallorca group recommends initial screening EGD with biopsy without a recommendation for ongoing surveillance (138). Table 12. s for management of affected persons with Lynch syndrome Intervention Recommendation Strength of recommendation Colectomy with ileorectal anastomosis Hysterectomy and bilateral salpingo-oophorectomy Daily aspirin Patients with colon cancer or colorectal neoplasia not removable by endoscopy Consideration for less extensive surgery in patients older than age y After childbearing or age 40 y Treatment of an individual patient with aspirin is a consideration after discussion of patient-specific risks, benefits, and uncertainties of treatment is conducted Strong recommendation: Level of evidence (III): well-designed and conducted cohort or casecontrolled studies from more than 1 group with cancer GRADE rating: moderate Recommendation: Level of evidence (IV): observation study GRADE rating: moderate Consideration: Level of evidence (I): randomized controlled study GRADE rating: moderate Routine screening of the small intestine is not recommended. This guideline is in concert with the Mallorca group (138), which does not recommend routine screening of the small intestine, but suggests attention to investigation of the distal duodenum and ileum during endoscopic studies. The NCCN suggests capsule endoscopy screening can be considered (122) at 2 3 year intervals beginning at age years. Screening for cancer of the urinary tract should be considered for persons at risk for or affected with LS, with urinalysis annually starting at age years (Table 10). The strength of evidence for this guideline is expert consensus level V and GRADE low-quality evidence. The guideline is in concert with the NCCN (122). The Mallorca group (138) does not recommend routine screening for urinary cancers.
12 Routine screening of the pancreas is not recommended. The benefit of screening for pancreatic cancer with this magnitude of risk is not established. This recommendation is in concert with other societies (122,138). However, an international pancreas consensus panel recommends that MMR gene mutation carriers with 1 affected first degree relative with pancreatic cancer should be considered for screening (156). Routine screening of the prostate and breast cancer is not recommended beyond what is advised for the general population. This recommendation is in concert with other societies (122,138). Colectomy with ileorectal anastomosis is the primary treatment of patients affected with LS with colon cancer or colon neoplasia not removable by endoscopy (Table 12). Consideration for less extensive surgery should be given in patients older than years of age and those with underlying sphincter dysfunction. This guideline is a strong recommendation with level III evidence and GRADE moderatequality evidence. The NCCN (122) and Mallorca group (138) both recommend colectomy with ileorectal anastomosis with no deference to patient age. Growing but not conclusive evidence exists that use of aspirin is beneficial in preventing cancer in LS patients. Treatment of an individual patient with aspirin is a consideration after discussion of patient-specific risks, benefits, and uncertain- ties of treatment is conducted (Table 12). The strength of evidence for this guideline is evidence obtained from at least 1 randomized controlled trial level I and GRADE moderate-quality evidence. This approach is endorsed by the Mallorca group (138) and the NCCN (122).
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer
 Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer Douglas K. Rex, MD, MACG 1, C. Richard Boland, MD 2, Jason A. Dominitz,
Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer Douglas K. Rex, MD, MACG 1, C. Richard Boland, MD 2, Jason A. Dominitz,
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
How common are mutations in the MSH2 gene? 1. Mutations that cause Lynch syndrome are rare found in approximately 1 in 370 individuals.
 The gene is a tumor suppressor gene. Tumor suppressor genes slow down cell division, repair DNA mistakes, or tell cells when to die. When they don't work properly, cells can grow out of control, which
The gene is a tumor suppressor gene. Tumor suppressor genes slow down cell division, repair DNA mistakes, or tell cells when to die. When they don't work properly, cells can grow out of control, which
Hereditary Non Polyposis Colorectal Cancer(HNPCC) From clinic to genetics
 From clinic to genetics") From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Pr
 Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
MSH6 gene. Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Colorectal Cancer (HNPCC) MSH6 Summary Cancer Risk Table
 MSH6 Summary Cancer Risk Table") MSH6 gene Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Colorectal Cancer (HNPCC) MSH6 Summary Cancer Risk Table CANCER Colorectal GENETIC CANCER RISK High Risk Endometrial High Risk
MSH6 gene Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Colorectal Cancer (HNPCC) MSH6 Summary Cancer Risk Table CANCER Colorectal GENETIC CANCER RISK High Risk Endometrial High Risk
Primary Care Approach to Genetic Cancer Syndromes
 Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
MLH1 gene. Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Colorectal Cancer (HNPCC) MLH1 Summary Cancer Risk Table
 MLH1 Summary Cancer Risk Table") MLH1 gene Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Cancer (HNPCC) MLH1 Summary Cancer Risk Table CANCER GENETIC CANCER RISK Endometrial Other MLH1 gene Overview Lynch syndrome 1,
MLH1 gene Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Cancer (HNPCC) MLH1 Summary Cancer Risk Table CANCER GENETIC CANCER RISK Endometrial Other MLH1 gene Overview Lynch syndrome 1,
Lynch Syndrome. Angie Strang, PGY2
 Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
PMS2 gene. Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Colorectal Cancer (HNPCC) PMS2 Summary Cancer Risk Table
 PMS2 Summary Cancer Risk Table") PMS2 gene Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Colorectal Cancer (HNPCC) PMS2 Summary Cancer Risk Table CANCER Colorectal GENETIC CANCER RISK High Risk Endometrial High Risk
PMS2 gene Associated Syndrome Name: Lynch syndrome/hereditary NonPolyposis Colorectal Cancer (HNPCC) PMS2 Summary Cancer Risk Table CANCER Colorectal GENETIC CANCER RISK High Risk Endometrial High Risk
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Universal Screening for Lynch Syndrome
 Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Result Navigator Positive Test Result: MSH6
 Result Navigator Positive Test Result: MSH6 Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
Result Navigator Positive Test Result: MSH6 Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
Yes when meets criteria below. Dean Health Plan covers when Medicare also covers the benefit.
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer
 status in Colorectal Cancer") Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
A Review from the Genetic Counselor s Perspective
 : A Review from the Genetic Counselor s Perspective Erin Sutcliffe, MS, CGC Certified Genetic Counselor Cancer Risk Evaluation Program INTRODUCTION Errors in base pair matching that occur during DNA replication,
: A Review from the Genetic Counselor s Perspective Erin Sutcliffe, MS, CGC Certified Genetic Counselor Cancer Risk Evaluation Program INTRODUCTION Errors in base pair matching that occur during DNA replication,
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Protocols 9-12 MMR mutation carrier guidelines Frequently asked questions
 Protocols 9-12 MMR mutation carrier guidelines Frequently asked questions Last updated: 10/02/2015 Q: Where have the general population cancer risks been taken from? The risk figures for the general population
Protocols 9-12 MMR mutation carrier guidelines Frequently asked questions Last updated: 10/02/2015 Q: Where have the general population cancer risks been taken from? The risk figures for the general population
Lynch Syndrome. A Patient s Guide to Genetic Testing for Lynch Syndrome
 Lynch Syndrome A Patient s Guide to Genetic Testing for Lynch Syndrome What is Lynch Syndrome? Lynch syndrome is an inherited condition that increases your risk of developing colon cancer and other cancers
Lynch Syndrome A Patient s Guide to Genetic Testing for Lynch Syndrome What is Lynch Syndrome? Lynch syndrome is an inherited condition that increases your risk of developing colon cancer and other cancers
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014
 COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By. Magnitude of the Problem. Magnitude of the Problem. Cardinal Features of Lynch Syndrome
 GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
Policy Specific Section: Medical Necessity and Investigational / Experimental. October 14, 1998 March 28, 2014
 Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
National Medical Policy
 National Medical Policy Subject: Policy Number: Genetic Testing for Hereditary Nonpolyposis Colorectal Cancer (HNPCC) (Lynch Syndrome) NMP137 Effective Date*: April 2004 Updated: March 2017 This National
National Medical Policy Subject: Policy Number: Genetic Testing for Hereditary Nonpolyposis Colorectal Cancer (HNPCC) (Lynch Syndrome) NMP137 Effective Date*: April 2004 Updated: March 2017 This National
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 PRACTICE GUIDELINES nature publishing group 223 CME ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Sy nga l, MD, M PH, FAC G 1, 2, 3, R and
PRACTICE GUIDELINES nature publishing group 223 CME ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Sy nga l, MD, M PH, FAC G 1, 2, 3, R and
Genetic Testing for Lynch Syndrome and Inherited Intestinal Polyposis Syndromes
 Genetic Testing for Lynch Syndrome and Inherited Intestinal Polyposis Syndromes Policy Number: 2.04.08 Last Review: 1/2014 Origination: 1/2004 Next Review: 1/2015 Policy Blue Cross and Blue Shield of Kansas
Genetic Testing for Lynch Syndrome and Inherited Intestinal Polyposis Syndromes Policy Number: 2.04.08 Last Review: 1/2014 Origination: 1/2004 Next Review: 1/2015 Policy Blue Cross and Blue Shield of Kansas
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
TumorNext-Lynch. genetic testing for hereditary colorectal or uterine cancer
 TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Genetic Testing for Lynch Syndrome and Other Inherited Page 1 of 34 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Genetic Testing for Lynch Syndrome and Other
Genetic Testing for Lynch Syndrome and Other Inherited Page 1 of 34 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Genetic Testing for Lynch Syndrome and Other
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2018 Origination: 1/2004 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2018 Origination: 1/2004 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas
LYNCH SYNDROME: IN YOUR FACE BUT LOST IN SPACE (MOUNTAIN)!
!") LYNCH SYNDROME: IN YOUR FACE BUT LOST IN SPACE (MOUNTAIN)! Kathryn Singh, MPH, MS, LCGC Associate Clinical Professor Assistant Director, Graduate Program in Genetic Counseling Division of Genetic and Genomic
LYNCH SYNDROME: IN YOUR FACE BUT LOST IN SPACE (MOUNTAIN)! Kathryn Singh, MPH, MS, LCGC Associate Clinical Professor Assistant Director, Graduate Program in Genetic Counseling Division of Genetic and Genomic
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
Prior Authorization. Additional Information:
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Genetic Testing for Lynch Syndrome
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post-test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post-test genetic counseling is
Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association
 Genetic Testing for Inherited Susceptibility to Colon Cancer Page 1 of 24 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Inherited Susceptibility
Genetic Testing for Inherited Susceptibility to Colon Cancer Page 1 of 24 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Inherited Susceptibility
Lynch Syndrome (HNPCC) and MYH-Associated Polyposis (MAP)
 and MYH-Associated Polyposis (MAP)") Lynch Syndrome (HNPCC) and MYH-Associated Polyposis (MAP) A Patient s Guide to risk assessment Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary
Lynch Syndrome (HNPCC) and MYH-Associated Polyposis (MAP) A Patient s Guide to risk assessment Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary
WHAT IS A GENE? CHROMOSOME DNA PROTEIN. A gene is made up of DNA. It carries instructions to make proteins.
 WHAT IS A GENE? CHROMOSOME E GEN DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
WHAT IS A GENE? CHROMOSOME E GEN DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
WELCOME. Taking Care of Your Health. April 30, 8 am to noon
 WELCOME Taking Care of Your Health April 30, 8 am to noon Cancer: Know Your Risk Emily Kuchinsky, MS, CGC, Certified Genetic Counselor Sporadic Cancer Lifetime Probability- Women Family Cluster Risk factors
WELCOME Taking Care of Your Health April 30, 8 am to noon Cancer: Know Your Risk Emily Kuchinsky, MS, CGC, Certified Genetic Counselor Sporadic Cancer Lifetime Probability- Women Family Cluster Risk factors
Genetic Testing for Lynch Syndrome And Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome And Other Inherited Colon Cancer Syndromes Policy Number: Original Effective Date: MM.02.007 09/01/2011 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration
Genetic Testing for Lynch Syndrome And Other Inherited Colon Cancer Syndromes Policy Number: Original Effective Date: MM.02.007 09/01/2011 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration
DIAGNOSTICS ASSESSMENT PROGRAMME Diagnostics consultation document
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE DIAGNOSTICS ASSESSMENT PROGRAMME Diagnostics consultation document Molecular testing strategies for Lynch syndrome in The National Institute for Health
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE DIAGNOSTICS ASSESSMENT PROGRAMME Diagnostics consultation document Molecular testing strategies for Lynch syndrome in The National Institute for Health
Page 1 of 8 TABLE OF CONTENTS
 Page 1 of 8 TABLE OF CONTENTS Patient Evaluation and Recommendation..Page 2 Testing and Follow-up..Page 3 Genetic Counseling Referral Criteria.....Page 4-5 Patient Education..Page 6 Suggested Readings...Page
Page 1 of 8 TABLE OF CONTENTS Patient Evaluation and Recommendation..Page 2 Testing and Follow-up..Page 3 Genetic Counseling Referral Criteria.....Page 4-5 Patient Education..Page 6 Suggested Readings...Page
Tumori eredofamiliari: sorveglianza di donne ad alto rischio
 Tumori eredofamiliari: sorveglianza di donne ad alto rischio 14/01/2018 Dott Matteo Generali AUSL Modena Carpi U.O. Ostetricia e Ginecologia Screening for gynaecologic cancer in genetically predisposed
Tumori eredofamiliari: sorveglianza di donne ad alto rischio 14/01/2018 Dott Matteo Generali AUSL Modena Carpi U.O. Ostetricia e Ginecologia Screening for gynaecologic cancer in genetically predisposed
Genetic Testing for Inherited Susceptibility to Colon Cancer; Including Microsatellite Instability Testing. Original Policy Date
 MP 2.04.06 Genetic Testing for Inherited Susceptibility to Colon Cancer; Including Microsatellite Instability Testing Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review
MP 2.04.06 Genetic Testing for Inherited Susceptibility to Colon Cancer; Including Microsatellite Instability Testing Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Section 2.0 Medicine Subsection 2.04 Pathology/Laboratory
 2.04.08 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Section 2.0 Medicine Subsection 2.04 Pathology/Laboratory Effective Date January 30, 2015 Original Policy Date October
2.04.08 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Section 2.0 Medicine Subsection 2.04 Pathology/Laboratory Effective Date January 30, 2015 Original Policy Date October
Objectives. Case Study #1 1/28/14. A Collaborative Practice Approach to Genetic Testing in Cancer: Translating Science Into Clinical Practice
 A Collaborative Practice Approach to Genetic Testing in Cancer: Translating Science Into Clinical Practice Heather Hampel, MS, CGC Associate Director, Division of Human Genetics Professor, Department of
A Collaborative Practice Approach to Genetic Testing in Cancer: Translating Science Into Clinical Practice Heather Hampel, MS, CGC Associate Director, Division of Human Genetics Professor, Department of
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Update from the 2011 symposium: MOH testing criteria
 Update from the 2011 symposium: MOH testing criteria Melyssa Aronson, MS, (C)CGC Zane Cohen Centre for Digestive Disease May 26, 2017 Criteria Working Group 2011 Symposium Concerns expressed: Last revised
Update from the 2011 symposium: MOH testing criteria Melyssa Aronson, MS, (C)CGC Zane Cohen Centre for Digestive Disease May 26, 2017 Criteria Working Group 2011 Symposium Concerns expressed: Last revised
Importance of Family History in Gynecologic Cancer Prevention. Objectives. Genetic Counselors. Angela Thompson, MS, CGC
 Importance of Family History in Gynecologic Cancer Prevention Angela Thompson, MS, CGC Genetic Counselor Froedtert & The Medical College of Wisconsin Objectives Introduce role of genetic counselor Discuss
Importance of Family History in Gynecologic Cancer Prevention Angela Thompson, MS, CGC Genetic Counselor Froedtert & The Medical College of Wisconsin Objectives Introduce role of genetic counselor Discuss
The Whys OAP Annual Meeting CCO Symposium September 20. Immunohistochemical Assessment Dr. Terence Colgan Mount Sinai Hospital, Toronto
 Immunohistochemical Assessment of Mismatch Repair Proteins in Endometrial Cancer: The Whys and How Terence J. Colgan, MD Head of Gynaecological Pathology, Mount Sinai Hospital, University of Toronto, Toronto.
Immunohistochemical Assessment of Mismatch Repair Proteins in Endometrial Cancer: The Whys and How Terence J. Colgan, MD Head of Gynaecological Pathology, Mount Sinai Hospital, University of Toronto, Toronto.
Colorectal Cancer Syndromes. Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago
 Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
FAMILIAL COLORECTAL CANCER. Lyn Schofield Manager Familial Cancer Registry
 FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
WHAT IS A GENE? CHROMOSOME DNA PROTEIN. A gene is made up of DNA. It carries instructions to make proteins.
 WHAT IS A GENE? CHROMOSOME GENE DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
WHAT IS A GENE? CHROMOSOME GENE DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
Hereditary Colorectal Cancer
 A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer testing is right for
A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer testing is right for
MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER. POLICY NUMBER: CATEGORY: Laboratory Test
 MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER POLICY NUMBER: 2.02.11 CATEGORY: Laboratory Test EFFECTIVE DATE: 09/16/99 REVISED DATE: 04/19/01, 05/16/02, 06/19/03,
MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER POLICY NUMBER: 2.02.11 CATEGORY: Laboratory Test EFFECTIVE DATE: 09/16/99 REVISED DATE: 04/19/01, 05/16/02, 06/19/03,
Genetic Counseling: Dealing with Uncertainty. Kathy J. Helzlsouer, MD, MHS Epidemiology and Genomics Research Program, DCCPS, NCI August 17, 2017
 Genetic Counseling: Dealing with Uncertainty Kathy J. Helzlsouer, MD, MHS Epidemiology and Genomics Research Program, DCCPS, NCI August 17, 2017 2 Multiple Paths to Genetic Counseling/Testing Family history
Genetic Counseling: Dealing with Uncertainty Kathy J. Helzlsouer, MD, MHS Epidemiology and Genomics Research Program, DCCPS, NCI August 17, 2017 2 Multiple Paths to Genetic Counseling/Testing Family history
Hereditary Cancer Syndromes
 Hereditary Cancer Syndromes Nicoleta Voian, MD, MPH Director Clinical Genetics Service Roswell Park Cancer Institute Nicoleta.Voian@Roswellpark.org February 28, 2017 Common Genetics Terms Gene: A hereditary
Hereditary Cancer Syndromes Nicoleta Voian, MD, MPH Director Clinical Genetics Service Roswell Park Cancer Institute Nicoleta.Voian@Roswellpark.org February 28, 2017 Common Genetics Terms Gene: A hereditary
A Patient s Guide to risk assessment. Hereditary Colorectal Cancer
 A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
Diagnostics guidance Published: 22 February 2017 nice.org.uk/guidance/dg27
 Molecular testing strategies for Lynch syndrome in people with colorectal cancer Diagnostics guidance Published: 22 February 2017 nice.org.uk/guidance/dg27 NICE 2018. All rights reserved. Subject to Notice
Molecular testing strategies for Lynch syndrome in people with colorectal cancer Diagnostics guidance Published: 22 February 2017 nice.org.uk/guidance/dg27 NICE 2018. All rights reserved. Subject to Notice
Resource impact report: Molecular testing strategies for Lynch syndrome in people with colorectal cancer (DG27)
") Putting NICE guidance into practice Resource impact report: Molecular testing strategies for Lynch syndrome in people with colorectal cancer (DG27) Published: February 2017 Summary Molecular testing strategies
Putting NICE guidance into practice Resource impact report: Molecular testing strategies for Lynch syndrome in people with colorectal cancer (DG27) Published: February 2017 Summary Molecular testing strategies
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management. Dr. med. Henrik Csaba Horváth PhD
 Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Assessment of Universal Mismatch repair (MMR) or Microsatellite Instability (MSI) testing in colorectal cancers.
 or Microsatellite Instability (MSI) testing in colorectal cancers.") Assessment of Universal Mismatch repair (MMR) or Microsatellite Instability (MSI) testing in colorectal cancers. Soheila Hamidpour MD, Madhusudhana S MD. MMR deficient colorectal tumors can be present
Assessment of Universal Mismatch repair (MMR) or Microsatellite Instability (MSI) testing in colorectal cancers. Soheila Hamidpour MD, Madhusudhana S MD. MMR deficient colorectal tumors can be present
Caring for Patients at Risk for Hereditary Colorectal Cancer
 February 05, 2007 By Karen Greco, PhD, RN, ANP [1] About 6% of colorectal cancers are caused by genetic mutations associated with hereditary colorectal cancer syndromes. The most common hereditary cancer
February 05, 2007 By Karen Greco, PhD, RN, ANP [1] About 6% of colorectal cancers are caused by genetic mutations associated with hereditary colorectal cancer syndromes. The most common hereditary cancer
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: Original Effective Date: MM.02.007 09/01/2011 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: Original Effective Date: MM.02.007 09/01/2011 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_colon_cancer 5/2004 8/2017 8/2018 8/2017 Description of Procedure or Service Genetic
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_colon_cancer 5/2004 8/2017 8/2018 8/2017 Description of Procedure or Service Genetic
Lynch syndrome. 9 October 2015 Masato Yozu Middlemore Hospital, Auckland, New Zealand
 Lynch syndrome 9 October 2015 Masato Yozu Middlemore Hospital, Auckland, New Zealand History of Lynch syndrome Aldred ScoO Warthin, MD, PhD (1866-1931) The father of cancer geneycs (JAMA. 2005;294(17):2195-2202)
Lynch syndrome 9 October 2015 Masato Yozu Middlemore Hospital, Auckland, New Zealand History of Lynch syndrome Aldred ScoO Warthin, MD, PhD (1866-1931) The father of cancer geneycs (JAMA. 2005;294(17):2195-2202)
GI Screening/Surveillance in Lynch Syndrome
 GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
Understanding and Managing Lynch Syndrome
 Understanding and Managing Lynch Syndrome Princess Margaret For women who may have Lynch syndrome and their family members Please visit the UHN Patient Education website for more health information: www.uhnpatienteducation.ca
Understanding and Managing Lynch Syndrome Princess Margaret For women who may have Lynch syndrome and their family members Please visit the UHN Patient Education website for more health information: www.uhnpatienteducation.ca
Hereditary Cancer Update: What do GPOs need to know?
 Hereditary Cancer Update: What do GPOs need to know? Mary McCullum, RN, MSN, CON(C) Nurse Educator, Hereditary Cancer Program BC Cancer Agency October 1, 2016 Conflict of Interest Disclosure Nothing to
Hereditary Cancer Update: What do GPOs need to know? Mary McCullum, RN, MSN, CON(C) Nurse Educator, Hereditary Cancer Program BC Cancer Agency October 1, 2016 Conflict of Interest Disclosure Nothing to
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Colorectal cancer Chapelle, J Clin Oncol, 2010
 Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Measure Description. Denominator Statement
 CMS ID/CMS QCDR ID: CAP 18 Title: Mismatch Repair (MMR) or Microsatellite Instability (MSI) Biomarker Testing to Inform Clinical Management and Treatment Decisions in Patients with Primary or Metastatic
CMS ID/CMS QCDR ID: CAP 18 Title: Mismatch Repair (MMR) or Microsatellite Instability (MSI) Biomarker Testing to Inform Clinical Management and Treatment Decisions in Patients with Primary or Metastatic
The Next Generation of Hereditary Cancer Testing
 The Next Generation of Hereditary Cancer Testing Why Genetic Testing? Cancers can appear to run in families. Often this is due to shared environmental or lifestyle patterns, such as tobacco use. However,
The Next Generation of Hereditary Cancer Testing Why Genetic Testing? Cancers can appear to run in families. Often this is due to shared environmental or lifestyle patterns, such as tobacco use. However,
The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
 The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove Research Institute Happy Lynch Syndrome Awareness Day March 22, 2016 Thanks to the Lynch Syndrome
The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove Research Institute Happy Lynch Syndrome Awareness Day March 22, 2016 Thanks to the Lynch Syndrome
FACT SHEET 49. What is meant by a family history of bowel cancer? What is bowel cancer? What causes bowel cancer?
 Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
Incidence and Clinical Characteristics of Colonic and Extra Colonic Lynch Syndrome Manifestations in Uruguayan Mismatch Repair Carriers
 Research Article imedpub Journals http://www.imedpub.com/ Colorectal Cancer: Open Access ISSN 47-9943 07 Vol.3 No.:6 DOI: 0.767/47-9943.00036 Incidence and Clinical Characteristics of Colonic and Extra
Research Article imedpub Journals http://www.imedpub.com/ Colorectal Cancer: Open Access ISSN 47-9943 07 Vol.3 No.:6 DOI: 0.767/47-9943.00036 Incidence and Clinical Characteristics of Colonic and Extra
GI EMERGENCIES Acute Abdominal Pain
 GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Lynch Syndrome (HNPCC) and MYH-Associated Polyposis (MAP)
 and MYH-Associated Polyposis (MAP)") Lynch Syndrome (HNPCC) and MYH-Associated Polyposis (MAP) A Patient s Guide to risk assessment Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary
Lynch Syndrome (HNPCC) and MYH-Associated Polyposis (MAP) A Patient s Guide to risk assessment Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary
Genetic Determinants, Risk Assessment and Management
 Genetic Determinants, Risk Assessment and Management Rachel Rando, MS, CGC Genetic Counselor Hunterdon Regional Cancer Center Flemington, NJ I have no disclosures. Acknowledgements: Staff of Hunterdon
Genetic Determinants, Risk Assessment and Management Rachel Rando, MS, CGC Genetic Counselor Hunterdon Regional Cancer Center Flemington, NJ I have no disclosures. Acknowledgements: Staff of Hunterdon
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Understanding Your Genetic Test Result. Positive for a Deleterious Mutation or Suspected Deleterious
 Understanding Your Genetic Test Result Positive for a Deleterious Mutation or Suspected Deleterious This workbook is designed to help you understand the results of your genetic test and is best reviewed
Understanding Your Genetic Test Result Positive for a Deleterious Mutation or Suspected Deleterious This workbook is designed to help you understand the results of your genetic test and is best reviewed
A Patient s Guide to Hereditary Cancer. Is Hereditary Cancer Testing Right for You?
 A Patient s Guide to Hereditary Cancer Is Hereditary Cancer Testing Right for You? What is Hereditary Cancer? Most cancers occur in people who do not have a strong family history of that cancer. This is
A Patient s Guide to Hereditary Cancer Is Hereditary Cancer Testing Right for You? What is Hereditary Cancer? Most cancers occur in people who do not have a strong family history of that cancer. This is
Management of higher risk of colorectal cancer. Huw Thomas
 Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Case Study. Overview. Deleterious MLH1 mutation detected on sequencing 10/16/2014
 The Role of Next Generation Sequencing for Hereditary Cancer Syndromes: A Focus on Endometrial Cancer Laura J. Tafe, MD Assistant Professor of Pathology Assistant Director, Molecular Pathology Dartmouth-Hitchcock
The Role of Next Generation Sequencing for Hereditary Cancer Syndromes: A Focus on Endometrial Cancer Laura J. Tafe, MD Assistant Professor of Pathology Assistant Director, Molecular Pathology Dartmouth-Hitchcock
Pancreatic non-functioning neuroendocrine tumor: a new entity genetically related to Lynch syndrome
 Case Report Pancreatic non-functioning neuroendocrine tumor: a new entity genetically related to Lynch syndrome Anna Serracant Barrera 1, Sheila Serra Pla 1, Carmen María Blázquez Maña 2, Rubén Carrera
Case Report Pancreatic non-functioning neuroendocrine tumor: a new entity genetically related to Lynch syndrome Anna Serracant Barrera 1, Sheila Serra Pla 1, Carmen María Blázquez Maña 2, Rubén Carrera
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD
 Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania
 Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania Aging Family history Early menarche Late menopause Nulliparity Estrogen / Progesterone use after menopause More than two alcoholic
Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania Aging Family history Early menarche Late menopause Nulliparity Estrogen / Progesterone use after menopause More than two alcoholic
Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management
 CLINICAL AND SYSTEMATIC S 1509 CME Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management Pr iyan ka Kant h, M D, M S 1, Jade Grimmett, MS2, 3, Mar j an C hampi ne,
CLINICAL AND SYSTEMATIC S 1509 CME Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management Pr iyan ka Kant h, M D, M S 1, Jade Grimmett, MS2, 3, Mar j an C hampi ne,
Information for You and Your Family
 Information for You and Your Family What is Prevention? Cancer prevention is action taken to lower the chance of getting cancer. In 2017, more than 1.6 million people will be diagnosed with cancer in the
Information for You and Your Family What is Prevention? Cancer prevention is action taken to lower the chance of getting cancer. In 2017, more than 1.6 million people will be diagnosed with cancer in the
GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer
 GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer Causes of Hereditary Ovarian and Uterine Cancer uterine cancer ovarian cancer Sporadic 75-90% Sporadic 70-80% Hereditary, 5% Lynch syndrome
GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer Causes of Hereditary Ovarian and Uterine Cancer uterine cancer ovarian cancer Sporadic 75-90% Sporadic 70-80% Hereditary, 5% Lynch syndrome