BTKi in MCL. Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK
|
|
|
- Annice Quinn
- 6 years ago
- Views:
Transcription
1 BTKi in MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK
2 2 Table of Various Treatment for R/R MCL Treatment Study or Literature Reference Ibrutinib PCYC CA Bortezomib Fischer 2006 Goy 2009 N ORR CR Median DOR (months) Median PFS (months) Median OS (months) % 21% Not reached 155 a 33% 8% Lenalidomide Goy % 8% Temsirolimus b Hess % 2% CR=complete response; DOR= duration of response; ORR=overall response rate; OS=overall survival; PFS= progression-free survival. a Of the 155 patients enrolled, 141 were assessable for response. b Results are presented for temsirolimus 175/75 mg dose group. Campo & Rule Blood 2015 Jan 1;125(1):48-55
3 3 Table of Various Treatment for R/R MCL Treatment Study or Literature Reference Ibrutinib PCYC CA Bortezomib Fischer 2006 Goy 2009 N ORR CR Median DOR (months) Median PFS (months) Median OS (months) % 21% Not reached 155 a 33% 8% Lenalidomide Goy % 8% Temsirolimus b Hess % 2% Acalabrutinib Wang % 40% Not reached Not reached CR=complete response; DOR= duration of response; ORR=overall response rate; OS=overall survival; PFS= progression-free survival. a Of the 155 patients enrolled, 141 were assessable for response. Not reached b Results are presented for temsirolimus 175/75 mg dose group.
4 IBRUTINIB
5 Overall Survival Outcomes in Patients With Mantle-Cell Lymphoma Treated With Ibrutinib: A Pooled Analysis of 370 Patients From 3 International Open-Label Studies Simon Rule, 1 Martin Dreyling, 2 Georg Hess, 3 Rebecca Auer, 4 Brad Kahl, 5 Nora Cavazos, 6 Black Liu, 7 Fong Clow, 6 Jenna Goldberg, 8 Darrin Beaupre, 6 Jessica Vermeulen, 9 Mark Wildgust, 8 and Michael Wang 10 1 Derriford Hospital, Plymouth, UK; 2 Klinikum der Universität München, Munich, Germany; 3 University Medical School of the Johannes Gutenberg University, Mainz, Germany; 4 St. Bartholomew's Hospital, Barts Health NHS Trust, London, UK; 5 Washington University School of Medicine, St. Louis, MO, USA; 6 Pharmacyclics, Sunnyvale, CA, USA; 7 Janssen China Research & Development, Shanghai, China; 8 Janssen Research & Development, Raritan, NJ, USA; 9 Janssen Research & Development, Leiden, The Netherlands; 10 The University of Texas MD Anderson Cancer Center, Houston, TX, USA
6 Median 3.5-year follow-up of ibrutinib treatment in patients with relapsed/refractory MCL: A pooled analysis - Patient disposition Study, n (%) PCYC-1104 SPARK RAY Discontinuation rates due to AEs at time of primary analysis (median follow-up): PCYC-1104 (15.3 months): 7% SPARK (14.9 months): 7% RAY (20 months): 6% Total (Pooled) (N = 370) Patients rolled over to CAN3001, n (%) 87 (23.5) Median duration of follow-up, months (range) 41.1 ( ) Treatment discontinuation, n (%) AE Disease progression Death Other* 316 (85.4) 37 (10.0) 218 (58.9) 19 (5.1) 42 (11.4) *Includes: alternative access to ibrutinib (n = 1); physician decision (n = 14); withdrawal of consent (n = 24); other reasons (n = 3). Rule et al., ASH 2017 (abstract 151, oral presentation)

7 Pooled MCL Analysis: Improvement in Response Rates Over Time CR PR 80 ORR (%) PR, par3al response Months 7 N = 370
8 Pooled MCL Analysis: PFS and OS by Prior Lines of Therapy (1, 2, 3) 1.00 PFS 1.00 OS Propor1on surviving without progression Propor1on alive Censored Months line (n = 99) 2 lines (n = 109) Months 3 lines (n = 162)! Patients who had received only 1 prior line of therapy had the longest PFS and OS; 2-year PFS and OS were 57% and 68%, respectively Rule et al ASH 2015 oral presentation 8
9 Ibrutinib in MCL: PFS and OS by prior line of therapy PFS OS Median 33.6 mo ( ) Median NR (36.0-NE) Median 8.4 mo ( ) Median 22.5 mo ( ) Median PFS overall (95% CI): 13.0 ( ) months Median OS overall (95% CI): 26.7 ( ) months Median PFS was nearly 3 years in patients with 1 prior line of therapy Patients censored from OS analysis upon study discontinuation. CI, confidence interval; NE, not estimable. Rule et al., ASH 2017 (abstract 151, oral presentation)
10 Pooled MCL Analysis: PFS by Baseline Patient Characteristics HR (95% CI) p value * * * * 10
11 Pooled MCL Analysis: OS by Baseline Patient Characteristics HR (95% CI) p value * * * * * Significant in univariate analysis Significant in mul3variate analysis 11
12 Pooled MCL Analysis: PFS and OS by Blastoid Histology Propor1on surviving without progression months PFS* months Propor1on alive months OS* Median OS, not reached 2-year OS, ~ 55% + Censored Months Nonblastoid (n = 326) Blastoid (n = 44) Months CI, confidence interval. *Statistically significant. 12
13 Median 3.5-Year follow-up of ibrutinib treatment in patients with relapsed/refractory MCL: a pooled analysis " In this pooled analysis of 370 patients: Approximately one-third (n = 115, 31.1%) were treated with ibrutinib for 2 years 54 remained on ibrutinib at time of analysis, with a median exposure of 46.3 months (range ) Maximum treatment exposure was 72 months Ibru1nib Exposure in Pa1ents With 2 Years of Exposure (N = 115) 4 yrs 40 (34.8%) 2 to < 3 yrs 32 (27.8%) 3 to < 4 yrs 43 (37.4%) Rule et al., ASH 2017 (abstract 151, oral presentation)
14 Ibrutinib in MCL: Overall response and PFS/OS by best response 100% 80% 60% 40% 20% 0% ORR: 69.7% (n = 258) 26,5% 36,4% 22,9% 43,2% 41,4% 43,9% ITT N = 370 ORR ORR: 77.8% (n = 77) 1 prior line > 1 prior line N = 99 CR PR ORR: 66.8% (n = 181) N = 271 Median, Months (95% CI) PFS OS Kaplan-Meier estimate of median. Best Response CR (n = 98) 46.2 (42.1-NE) NE (59.9-NE) PR (n = 160) 14.3 ( ) 26.2 ( ) CR rate was 36% in patients with 1 prior line of therapy Median PFS was nearly 4 years in patients who achieved a CR ITT, intent-to treat; ORR, overall response rate; PR, partial response. Rule et al., ASH 2017 (abstract 151, oral presentation)
15 Ibrutinib in MCL: DOR by best response and line of therapy Median DOR, Months (Range) Overall (n = 258) CR (n = 98) PR (n = 160) Overall (n = 258) 22.2 ( ) 55.7 (55.7-NE) 10.4 ( ) Prior Lines of Therapy 1 (n = 77) 34.4 (23.1-NE) 55.7 (33.1-NE) 22.1 ( ) > 1 (n = 181) 16.0 ( ) NE (40.7-NE) 8.5 ( ) Median DOR was 4.5 years in patients achieving a CR Patients with 1 prior line had 2 longer DOR than patients with > 1 prior line DOR, duration of response. Rule et al., ASH 2017 (abstract 151, oral presentation)
16 Ibrutinib in MCL: Grade 3 treatment-emergent AEs over time and by line of therapy 100% 80% 60% 40% 20% 0% N = 79,7% ,8% 25 1 ITT 1 Prior Line > 1 Prior Line 47,8% 34,8% 36,1% ,0% 8 68,7% 68 55,6% 55 34,4% 29,8% 29,4% ,1% 83,8% 72,3% 54,6% 38,2% 40,8% 26,9% 1 Overall Yr 1 Yr 2 Yr 3 Yr 4 Yr > 4 Overall Yr 1 Yr 2 Yr 3 Yr 4 Yr > 4 Overall Yr 1 Yr 2 Yr 3 Yr 4 Yr > ! New onset grade 3 TEAEs generally decreased after the first year of treatment Similar trend was seen for atrial fibrillation (AF) and bleeding! New onset grade 3 TEAEs were generally lower in patients with 1 vs > 1 prior line Number of patients with event shown on bars. Rule et al., ASH 2017 (abstract 151, oral presentation)
17 Ibrutinib in MCL: Cardiac risk factors and atrial fibrillation Studies enrolled patients with significant cardiac risk factors, including 53 patients with a history of (or ongoing controlled) AF/arrhythmia Patient History: Factors that May Increase Cardiac Risk, n (%) Total (N = 370) Hypertension 176 (47.6) Hyperlipidemia 60 (16.2) Atrial fibrillation/abnormal heart rhythm 53 (14.3) Diabetes 48 (13.0) Coronary artery disease 31 (8.4) The majority (70%; 37 of 53) of patients who entered the study with a history of AF or arrhythmia did not have a recurrence Exclusion criterion: Clinically significant cardiovascular disease such as uncontrolled or symptomatic arrhythmias, congestive heart failure, or myocardial infarction within 6 months of screening, or any class 3 (moderate) or 4 (severe) cardiac disease as defined by the New York Heart Association Functional Classification. Rule et al., ASH 2017 (abstract 151, oral presentation)
18 Ibrutinib in MCL: Management of ibrutinib in patients with bleeding or atrial fibrillation Safety Population Ibrutinib (N = 370) Grade 3 bleeding 21 (5.7%) Dose reduction 1 (0.3%) Discontinuation* 3 (0.8%) Grade 3 atrial fibrillation 22 (5.9%) Dose reduction 2 (0.5%) Discontinuation* 0 *Treatment discontinuation! < 2% of 370 patients treated with ibrutinib discontinued or had a dose reduction due to grade 3 bleeding or AF! No patients discontinued ibrutinib due to grade 3 AF Rule et al., ASH 2017 (abstract 151, oral presentation)
19 Next generation BTKi s BGB 3111 ONO 4059 ACP 196 M 7583


20 Next generation BTKi s Zanubrutinib Tirabrutinib Acalabrutinib M 7583

21

22 Acalabrutinib (ACP-196) Acalabrutinib is more selective for BTK with less offtarget kinase inhibition compared with ibrutinib in vitro Kinase Inhibition Average IC 50 (nm) Kinase Selectivity Profiling at 1 µm Acalabrutinib Ibrutinib Larger red circles represent stronger inhibition Kinase Acalabrutinib Ibrutinib BTK TEC ITK > BMX TXK EGFR > ERBB2 ~ ERBB BLK > JAK3 > BLK = B lymphocyte kinase; BMX = bone marrow tyrosine kinase gene in chromosome X; BTK = Bruton tyrosine kinase; EGFR = epidermal growth factor receptor; ERBB2 = erb-b2 receptor tyrosine kinase; ERBB4 = erb-b4 receptor tyrosine kinase; IC50 = inhibitory concentration of 50%; ITK = interleukin-2-inducible T-cell kinase; JAK3 = Janus kinase 3; TEC = tyrosine kinase expressed in hepatocellular carcinoma; TXK = T and X cell expressed kinase. Barf T, et al. J Pharmacol Exp Ther. 2017;363(2): Byrd et al., ASH 2017 (abstract 498, oral presentation)

23 ACE-LY-004: Acalabrutinib monotherapy in R/R MCL Enrollment: March 12th, 2015, through January 5th, 2016, at 40 sites across 9 countries 124 Patients with R/R MCL 1-5 prior therapies Acalabrutinib 100 mg BID PO in 28-day cycles until disease progression Primary endpoint: ORR by investigator assessment based on the Lugano Classification 1 Secondary endpoints: ORR by Independent Review Committee (IRC) assessment DOR, PFS, OS Safety Pharmacokinetics and pharmacodynamics Exploratory endpoints: Time to response IRC-assessed ORR per the 2007 International Harmonization Project criteria 2 Data cutoff: February 28, 2017 BID = twice daily; DOR = duration of response; MCL = mantle cell lymphoma; ORR = overall response rate; PFS = progression-free survival; PO = orally; R/R = relapsed/refractory. 1. Cheson BD, et al. J Clin Oncol. 2014;32: Cheson BD, et al. J Clin Oncol. 2007;25: Wang et al., ASH 2017 (abstract 155, oral presentation)
24 ACE-LY-004: Baseline patient characteristics Characteristic N=124 Median age, years (range) 68 (42-90) Male sex, n (%) 99 (80) ECOG PS 1, n (%) 115 (93) Simplified MIPI score, n (%) a Low risk (0-3) 48 (39) Intermediate risk (4-5) 54 (44) High risk (6-11) 21 (17) Ann Arbor Stage IV disease, n (%) 93 (75) Tumor bulk, n (%) 5 cm 46 (37) 10 cm 10 (8) Extranodal disease, n (%) 90 (73) Bone marrow 63 (51) Gastrointestinal 13 (10) Lung 12 (10) a Missing data, n=1 patient. ECOG PS = Eastern Cooperative Oncology Group performance status; MIPI = Mantle Cell Lymphoma International Prognostic Index. Wang et al., ASH 2017 (abstract 155, oral presentation)
25 Response to acalabrutinib The primary endpoint was investigator-assessed ORR according to the 2014 Lugano Classification 1 High concordance was observed between investigator- and IRCassessed ORR and CR (91% and 94%, respectively) IRC-assessed ORR by 2007 IHP criteria (exploratory endpoint) was 75% with a CR rate of 30% 2 ORR using the 2014 Lugano Classification N=124 Investigator assessed IRC assessed n (%) n (%) ORR (CR + PR) 100 (81) 99 (80) Best response CR 49 (40) 49 (40) PR 51 (41) 50 (40) SD 11 (9) 9 (7) PD 10 (8) 11 (9) Not evaluable 3 (2) 5 (4) CR = complete response; IHP = International Harmonization Project; IRC = Independent Review Committee; ORR = overall response rate; PD = progressive disease; PR = partial response; SD = stable disease. 1. Cheson BD, et al. J Clin Oncol. 2014;32: Cheson BD, et al. J Clin Oncol. 2007;25: Wang et al., ASH 2017 (abstract 155, oral presentation)




26 ACE-LY-004: Results At a median follow-up of 15.2 months, 56% of patients remain on treatment AEs occurring in 15% of all patients Headac Diarrhea Fatigue Myalgia Cough Nausea Pyrexia Grade 3 AEs occurring in 5% of all patients Anemia Neutrop Pneumo Grade 1 Grade 2 Grade 3 Grade Wang et al., ASH 2017 (abstract 155, oral presentation)
27 ACE-LY-004: Duration of response Median time to response was 1.9 months (range ) 92% of responders had initial response by end of cycle 2 Median DOR has not been reached; the 12-month DOR rate was 72% (95% CI: 62%, 80%) CR = complete response; DOR = duration of response; PR = partial response. Wang et al., ASH 2017 (abstract 155, oral presentation)
28 ACE-LY-004: PFS and OS Median PFS and median OS have not been reached PFS OS 12-month PFS rate: 67% (95% CI: 58%, 75%) 12-month OS rate: 87% (95% CI: 79%, 92%) Wang et al., ASH 2017 (abstract 155, oral presentation) OS = overall survival; PFS = progression-free survival.
29 Safety and Activity of BTK Inhibitor BGB-3111 in patients with DLBCL, MCL, FL and MZL Dose Dose escalation Enrolled (indolent, aggressive) 40 mg QD 4 (0,1) 80 mg QD 5 (0,1) 160 mg QD 6 (0,2) 320 mg QD 6 (0,1) 160 mg BID 4 (0,2) Recommended Phase 2 dose (RP2D) 320 mg QD or 160 mg BID Dose expansion Population RP2D Disease Planned R/R BID, QD MCL, MZL, FL, GCB DLBCL R/R BID Non-GCB DLBCL R/R BID, QD MCL 20 TN BID, QD MCL 20 R/R BID inhl 40 Eligibility WHO-defined B-cell malignancy No available higher priority treatment ECOG 0-2 ANC > 1000µ L, platelets > 100,000/µL Adequate renal and hepatic function No significant cardiac disease Primary endpoints Safety including AEs and SAEs Recommended phase 2 dose Select secondary endpoints Pharmacokinetics Efficacy Tam et al., ASH 2017 (abstract 152, oral presentation)
30 BGB-3111 in patients with DLBCL/MCL (n=65): most frequent and selected AEs Adverse event All grades, n(%) Grade 3-5, n(%) Petechiae/purpura/contusion 16 (25) 0 Diarrhea 15 (23) 1 (2) Constipation 14 (22) 0 Fatigue 12 (18) 0 Upper respiratory tract infection 12 (18) 1 (2) Anemia 11 (17) 7 (11) Cough 10 (15) 0 Pyrexia 10 (15) 2 (3) Thrombocytopenia 10 (15) 6 (9) Neutropenia 8 (12) 6 (9) Pneumonia 6 (9) 4 (6)* Event, n(%) DLBCL/MCL (n=65) Patients with 1 AE grade 3 39 (60) Patients with 1 serious AE 26 (40) Event leading to treatment discontinuation 8 (12) Fatal AE 6 (9) AE of special interest Petechiae/purpura/contusion 16 (25) Diarrhea 15 (23) Hypertension 5 (8) Severe haemorrhage 2 (3) Atrial fibrillation 2 (3) *1 Grade 5 event in the setting of progressive disease Tam et al., ASH 2017 (abstract 152, oral presentation)
31 BGB-3111 in patients with MCL: response Response (based on CT for majority of patients) Median efficacy followup, months (range) Best response, n(%) MCL* (n=32) 9.5 ( ) ORR 28 (88) CR 8 (25) PR 20 (63) SD 1 (3) PD 1 (3) NE 2** (6) *In MCL patients treated with minimum of 320 mg/ d ORR is 93% and CR is 28% ** Off study for AE before response assessment PFS Tam et al., ASH 2017 (abstract 152, oral presentation)
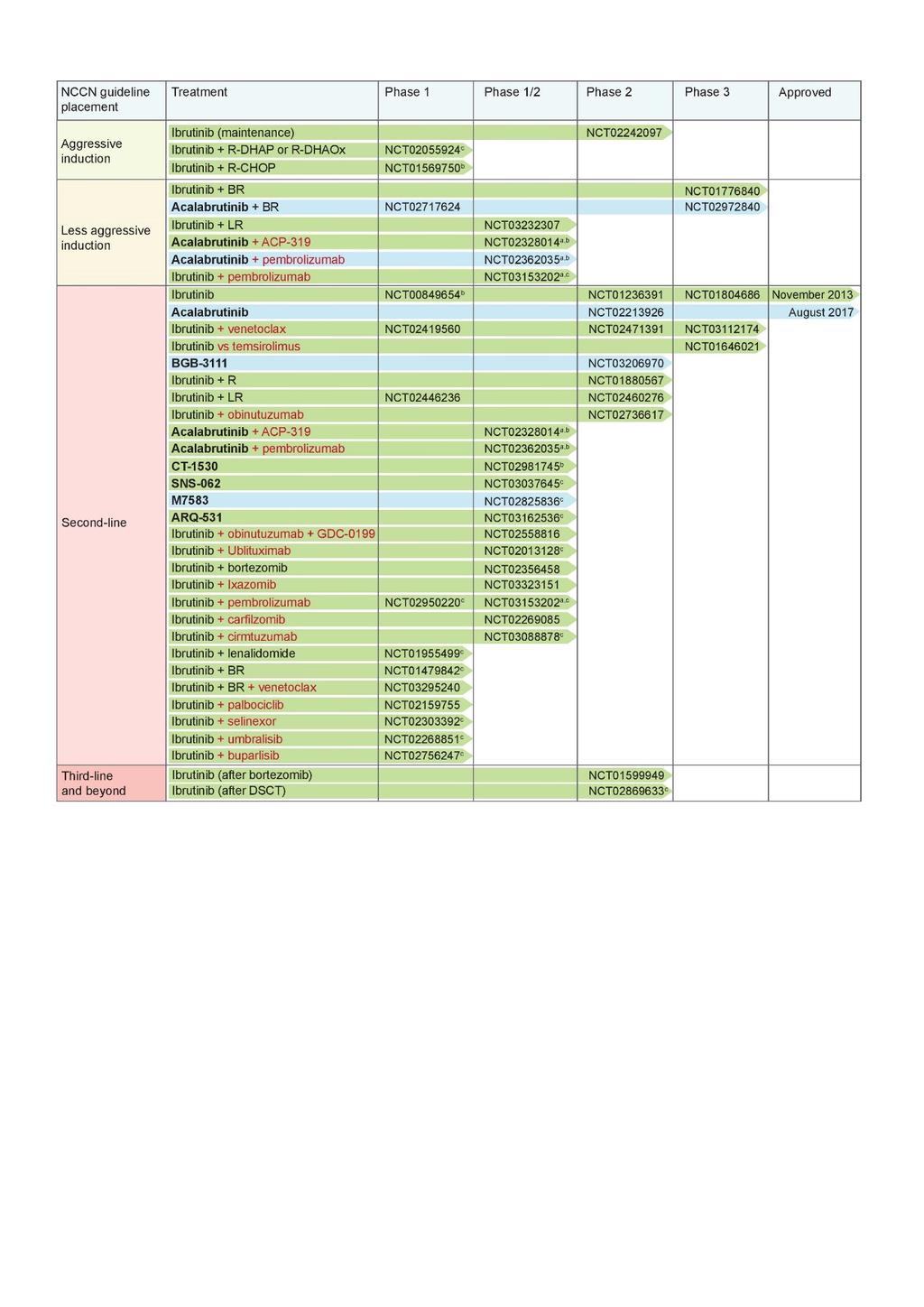
32 BTKI TRIALS IN MCL (2017)
33 Trials with BTKi in MCL Study ID Intervention Condition Phase Primary endpoint(s) N Completio NCT NCT NCT NCT NCT NCT NCT NCT NCT NCT n a Approvals Acalabrutinib R/R MCL 2 ORR (at least 1 year) 124 Feb 2017 FDA (Aug 2017) Acalabrutinib + NHL, MM and B- 1/2 AEs (up to 1 year) 126 c Aug 2017 None ACP-319 ALL b CT-1530 R/R BCNHL, CLL, 1/2 DLTs (28 days) 200 c Sep 2018 None MCL, WM, MZL, DFCL and DLBCL MTD and/or RP2D SNS-062 R/R CLL, LL, MCL, 1/2 MTD and/or RP2D (up to c Sep 2018 None SLL and WM months) ORR (up to 24 months) BGB-3111 R/R MCL 2 ORR (up to 3 years) 80 c Nov 2018 None ARQ-531 M7583 Acalabrutinib + BR Acalabrutinib + Pembrolizumab Acalabrutinib + BR vs placebo + BR R/R BCL, DLBCL, SLL, CLL, MCL, WM R/R BCM, MCL and DLBCL Untreated and R/R MCL NHL, MM, HL, CLL, RS, WM b 1 AEs (up to 28 weeks) RP2D (up to 24 weeks) 1/2 DLTs (up to 28 days) 120 c Dec 2018 None 60 c Oct 2019 None BOR (up to 6 months) 1b TEAEs (timeframe unclear) 48 c Feb 2021 None 1b/2 TEAEs (2 years) 159 Apr 2021 None Untreated MCL 3 PFS (48 months) 546 c Oct 2022 None
34
35 Study Therapy PART I: Chemo-free Ibrutinib + Rituximab Oral ibrutinib at 560 mg daily, each cycle is 28 days 4 weekly loading doses IV rituximab at 375 mg/m² in Cycle 1, then 1 dose/cycle in Cycles 3-12 Restage every 2 cycles Any time CR in PART I, will enter PART II Up to 12 months to reach best response. =CR Part 2 R-I 2 cycles =PR /SD# 2 cycles =CR =PR Part 2 2 cycles =CR =PR Part 2 2 cycles Cycles continue up to 12 cycles until no more PR or best response (As long as patient has PR from last restaging. R-I continues =PD Part 2 =SD# /PD Part 2 =SD# /PD Part 2 Oral Presentation ASH 2016 Wang

 Part II")
36 Window I/II Study: the Best Response Rate ORR 100% ORR 100% % of patients C R P R 20 0 Part I (N = 50) Part II (N = 47)

37 37


38 ENRICH NCRI MULTICENTRE RANDOMISED OPEN LABEL PHASE II/III TRIAL OF RITUXIMAB & IBRUTINIB VS RITUXIMAB & CHEMOTHERAPY IN ELDERLY MANTLE CELL LYMPHOMA



 for")
 for 2 years")

")

39 ENRICH NCRI multicentre Randomised open label phase III trial of Rituximab & Ibrutinib vs Rituximab & CHemotherapy in Elderly mantle cell lymphoma R-CHEMO/R Standard care R-CHEMO (every 21 days) for 6-8 cycles Rituximab (every 56 days) for 2 years Follow-up until disease progression R IR/R Intervention Ibrutinib daily + Rituximab (every 21 days) for 8 cycles Ibrutinib daily + Rituximab (every 56 days) for 2 years Ibrutinib to continue until disease progression CI S Rule
40 Summary Ibrutinib Early use translates into better outcomes No evolving toxicity Combination trials on-going Second generation BTKi Efficacy is broadly the same Appear to have fewer cardiac events Acalabrutinib licensed in the USA for MCL
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia
 Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111)
 and Zanubrutinib (BGB-3111)") Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111) Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia
Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111) Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia
ACALABRUTINIB IN MCL
 ACALABRUTINIB IN MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK BRUTON S TYROSINE KINASE (BTK): A CRITICAL KINASE
ACALABRUTINIB IN MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK BRUTON S TYROSINE KINASE (BTK): A CRITICAL KINASE
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth
 Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth") VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia
, a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia") Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
POST ICML Indolent lymphomas relapse treatment
 POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
BTK Inhibitors and BCL2 Antagonists
 BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Chronic Lymphocytic Leukemia: State of the Art
 14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
Disclosures. I receive honoraria and research funding from Beigene, Janssen and AbbVie.
 Improved depth of response with increased follow-up in phase 1 trial of patients with Waldenström macroglobulinemia (WM) treated with oral Bruton tyrosine kinase (BTK) inhibitor zanubrutinib (BGB-3111)
Improved depth of response with increased follow-up in phase 1 trial of patients with Waldenström macroglobulinemia (WM) treated with oral Bruton tyrosine kinase (BTK) inhibitor zanubrutinib (BGB-3111)
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
MANTLE CELL LYMPHOMA MTOR-INHIBITION
 MANTLE CELL LYMPHOMA MTOR-INHIBITION Rome, 23. March 2017 Prof. Dr. med. Georg Heß III. Med. Klinik Universitäres Centrum für Tumorerkrankungen Universitätsmedizin der Johannes Gutenberg-Universität Mainz
MANTLE CELL LYMPHOMA MTOR-INHIBITION Rome, 23. March 2017 Prof. Dr. med. Georg Heß III. Med. Klinik Universitäres Centrum für Tumorerkrankungen Universitätsmedizin der Johannes Gutenberg-Universität Mainz
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced CLL and NHL
, ublituximab, and ibrutinib in patients with advanced CLL and NHL") Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Background. Approved by FDA and EMEA for CLL and allows for treatment without chemotherapy in all lines of therapy
 Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
Media Inquiries: Satu Glawe Phone: Bernadette King Phone:
 Media Inquiries: Satu Glawe Phone: +49-172-294-6264 Bernadette King Phone: 1-215-778-3027 Investor Relations: Christopher DelOrefice Phone: 1-732-524-2955 Lesley Fishman Phone: 1-732-524-3922 U.S. Medical
Media Inquiries: Satu Glawe Phone: +49-172-294-6264 Bernadette King Phone: 1-215-778-3027 Investor Relations: Christopher DelOrefice Phone: 1-732-524-2955 Lesley Fishman Phone: 1-732-524-3922 U.S. Medical
PCI-32765DBL1002. Janssen Research & Development, Raritan, NJ, USA; 9 Janssen Research & Development, Belgrade, Serbia; 10
 Phase 1b Study Combining Ibrutinib With Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP) in Patients With CD20-Positive B-Cell Non-Hodgkin Lymphoma (NHL) Anas Younes, 1 Ian
Phase 1b Study Combining Ibrutinib With Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP) in Patients With CD20-Positive B-Cell Non-Hodgkin Lymphoma (NHL) Anas Younes, 1 Ian
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
*Jagiellonian University, Kraków, Poland
 Single-Agent MOR208 in Relapsed or Refractory (R-R) Non-Hodgkin s Lymphoma (NHL): Results from Diffuse Large B-Cell Lymphoma (DLBCL) and Indolent NHL Subgroups of a Phase IIa Study Wojciech Jurczak, *
Single-Agent MOR208 in Relapsed or Refractory (R-R) Non-Hodgkin s Lymphoma (NHL): Results from Diffuse Large B-Cell Lymphoma (DLBCL) and Indolent NHL Subgroups of a Phase IIa Study Wojciech Jurczak, *
M Trneny 5. C Joao 8 M Witzens-Harig 9. M Jerkeman 3. D Caballero 7. SRule 1. C Rusconi 4. W Jurczak 2. F Offner 6. I Bence-Bruckler 11.
 Leukemia https://doi.org/10.1038/s41375-018-0023-2 BRIEF COMMUNICATION Ibrutinib versus temsirolimus: 3-year follow-up of patients with previously treated mantle cell lymphoma from the phase 3, international,
Leukemia https://doi.org/10.1038/s41375-018-0023-2 BRIEF COMMUNICATION Ibrutinib versus temsirolimus: 3-year follow-up of patients with previously treated mantle cell lymphoma from the phase 3, international,
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
BR is an established treatment regimen for CLL in the front-line and R/R settings
 Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
State of the Art Treatment for Relapsed Mantle Cell Lymphoma
 Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Dr Claire Burney, Lymphoma Clinical Fellow, Bristol Haematology and Oncology Centre, UK
 EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
Management of CLL in the Targeted Therapy Era
 Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents
 Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Department of Medicine, Division of Hematology-Oncology, Weill Cornell Medical College, New York, NY 3
 The Bruton s Tyrosine Kinase (BTK) Inhibitor Ibrutinib (PCI-32765) is Highly Active and Tolerable in Treatment Naïve (TN) Chronic Lymphocytic Leukemia (CLL) Patients: Interim Results of a Phase Ib/II Study
The Bruton s Tyrosine Kinase (BTK) Inhibitor Ibrutinib (PCI-32765) is Highly Active and Tolerable in Treatment Naïve (TN) Chronic Lymphocytic Leukemia (CLL) Patients: Interim Results of a Phase Ib/II Study
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia
 Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
Highlights in chronic lymphocytic leukemia
 Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Bcl-2 inhibition in NHL. Jonathan W. Friedberg M.D., M.M.Sc.
 Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
NASDAQ: TGTX Jefferies Healthcare Conference June 2015
 NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
Chronic Lymphocytic Leukemia Update. Learning Objectives
 Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
What from the basket of BTK and PI3K inhibitors?
 What from the basket of BTK and PI3K inhibitors? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Associate Professor of Medicine Weill Cornell Medical
What from the basket of BTK and PI3K inhibitors? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Associate Professor of Medicine Weill Cornell Medical
How to Integrate the New Drugs into the Management of Multiple Myeloma
 How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
Venetoclax in MCL. Prof. Le Gouill Nantes Medical University, France
 Venetoclax in MCL Prof. Le Gouill Nantes Medical University, France Evasion of Apoptosis, or Cell Death, is 1. Resisting Cell Death 2. Sustained angiogenesis for growth and survival (primarily solid tumors)
Venetoclax in MCL Prof. Le Gouill Nantes Medical University, France Evasion of Apoptosis, or Cell Death, is 1. Resisting Cell Death 2. Sustained angiogenesis for growth and survival (primarily solid tumors)
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
Targeting Bruton s Tyrosine Kinase (BTK)
") Targeting Bruton s Tyrosine Kinase (BTK) Lapo Alinari, MD, PhD 4 th International Conference, Translational Research in Oncology Forli, November 9-11/2016 The Ohio State University Comprehensive Cancer
Targeting Bruton s Tyrosine Kinase (BTK) Lapo Alinari, MD, PhD 4 th International Conference, Translational Research in Oncology Forli, November 9-11/2016 The Ohio State University Comprehensive Cancer
Managing patients with relapsed follicular lymphoma. Case
 Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Pharmacyclics Reports Updated Clinical Results from its Phase IA Trial of its First in Human BTK- Inhibitor PCI-32765
 Contact: Ramses Erdtmann Vice President of Finance Phone: 408-215-3325 Pharmacyclics Reports Updated Clinical Results from its Phase IA Trial of its First in Human BTK- Inhibitor PCI-32765 Company to Host
Contact: Ramses Erdtmann Vice President of Finance Phone: 408-215-3325 Pharmacyclics Reports Updated Clinical Results from its Phase IA Trial of its First in Human BTK- Inhibitor PCI-32765 Company to Host
Imbruvica. Imbruvica (ibrutinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.41 Subject: Imbruvica Page: 1 of 5 Last Review Date: June 22, 2017 Imbruvica Description Imbruvica
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.41 Subject: Imbruvica Page: 1 of 5 Last Review Date: June 22, 2017 Imbruvica Description Imbruvica
Firenze, settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo
 Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
TRANSPARENCY COMMITTEE OPINION. 27 January 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 27 January 2010 TORISEL 25 mg/ml, concentrate for solution and diluent for solution for infusion Box containing 1
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 27 January 2010 TORISEL 25 mg/ml, concentrate for solution and diluent for solution for infusion Box containing 1
ANCO: ASCO Highlights 2018 Hematologic Malignancies
 ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
MANTLE CELL LYMPHOMA
 MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia
 Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia Edward Libby M.D. Associate Professor, University of Washington Department of Medicine, Division of Medical Oncology Fred Hutchinson
Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia Edward Libby M.D. Associate Professor, University of Washington Department of Medicine, Division of Medical Oncology Fred Hutchinson
Disclosures for Dr. Peter Borchmann 48 th ASH Annual meeting, Orlando, Florida
 Phase II Study of Pixantrone in Combination with Cyclophosphamide, Vincristine, and Prednisone (CPOP) in Patients with Relapsed Aggressive Non-Hodgkin s Lymphoma P Borchmann Universitaet de Koeln, Koeln,
Phase II Study of Pixantrone in Combination with Cyclophosphamide, Vincristine, and Prednisone (CPOP) in Patients with Relapsed Aggressive Non-Hodgkin s Lymphoma P Borchmann Universitaet de Koeln, Koeln,
US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA
 FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA") US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA Accelerated approval of Bruton tyrosine kinase (BTK) inhibitor in MCL marks AstraZeneca
US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA Accelerated approval of Bruton tyrosine kinase (BTK) inhibitor in MCL marks AstraZeneca
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
ASH POSTER: LYMRIT UPDATE
 ASH POSTER: LYMRIT 37-01 UPDATE DECEMBER 2018 EDUARDO BRAVO, CEO LISA ROJKJAER, MD, CMO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com IR contact: ir@nordicnanovector.com
ASH POSTER: LYMRIT 37-01 UPDATE DECEMBER 2018 EDUARDO BRAVO, CEO LISA ROJKJAER, MD, CMO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com IR contact: ir@nordicnanovector.com
BENDAMUSTINE + RITUXIMAB IN CLL
 BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
OSCO/OU ASH-SABC Review. Lymphoma Update. Mohamad Cherry, MD
 OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
Options in Mantle Cell Lymphoma Therapy
 Options in Mantle Cell Lymphoma Therapy Carlo Visco, MD Dept of Cell Therapy and Hematology San Bortolo Hospital, Vicenza, taly My Disclosures: ADVSOR OR ADVSORY BOARDS: Lundbeck Canada nc, Celgene Europe,
Options in Mantle Cell Lymphoma Therapy Carlo Visco, MD Dept of Cell Therapy and Hematology San Bortolo Hospital, Vicenza, taly My Disclosures: ADVSOR OR ADVSORY BOARDS: Lundbeck Canada nc, Celgene Europe,
Disclosures WOJCIECH JURCZAK
 Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
Smoldering Myeloma: Leave them alone!
 Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia
 Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia Pollyea DA 1, Tallman MS 2,3, de Botton S 4,5, DiNardo CD 6, Kantarjian HM
Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia Pollyea DA 1, Tallman MS 2,3, de Botton S 4,5, DiNardo CD 6, Kantarjian HM
Long-term safety and efficacy of vismodegib in patients with advanced basal cell carcinoma (BCC): 24-month update of the pivotal ERIVANCE BCC study
: 24-month update of the pivotal ERIVANCE BCC study") Long-term safety and efficacy of vismodegib in patients with advanced basal cell carcinoma (BCC): 24-month update of the pivotal ERIVANCE BCC study A Sekulic, 1 MR Migden, 2 AE Oro, 3 L Dirix, 4 K Lewis,
Long-term safety and efficacy of vismodegib in patients with advanced basal cell carcinoma (BCC): 24-month update of the pivotal ERIVANCE BCC study A Sekulic, 1 MR Migden, 2 AE Oro, 3 L Dirix, 4 K Lewis,
Study No Title : Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2018 KSMO Immune Oncology Forum. Immune checkpoint inhibitors in hematologic. malignancies: evidences and perspectives 서울아산병원종양내과 홍정용
 2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
Aggressive lymphomas ASH Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV
 Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Dana-Farber Cancer Institute, Boston, MA, USA; 2. H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, USA; 3
 The investigational agent MLN9708, an oral proteasome inhibitor, in patients with relapsed and/or refractory multiple myeloma (MM): results from the expansion cohorts of a phase 1 dose-escalation study
The investigational agent MLN9708, an oral proteasome inhibitor, in patients with relapsed and/or refractory multiple myeloma (MM): results from the expansion cohorts of a phase 1 dose-escalation study
Imbruvica. Imbruvica (ibrutinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.41 Subject: Imbruvica Page: 1 of 5 Last Review Date: September 15, 2017 Imbruvica Description Imbruvica
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.41 Subject: Imbruvica Page: 1 of 5 Last Review Date: September 15, 2017 Imbruvica Description Imbruvica
ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan. June 16, 2017
 ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan June 16, 2017 Forward Looking Statements Certain statements contained in this presentation, other than statements of fact that are
ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan June 16, 2017 Forward Looking Statements Certain statements contained in this presentation, other than statements of fact that are
Sponsor / Company: Sanofi Drug substance(s): Docetaxel (Taxotere )
: Docetaxel (Taxotere )") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Bendamustine: A Transversal * Chemotherapy Agent
 Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
La lenalidomide: meccanismo d azione e risultati terapeutici. F. Ferrara
 La lenalidomide: meccanismo d azione e risultati terapeutici F. Ferrara MDS: new treatment goals Emerging treatment options expected to facilitate shift from supportive care to active therapy in MDS New
La lenalidomide: meccanismo d azione e risultati terapeutici F. Ferrara MDS: new treatment goals Emerging treatment options expected to facilitate shift from supportive care to active therapy in MDS New
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
Product: Blinatumomab (AMG 103) Clinical Study Report: MT Date: 19 April 2013 Page 2 of 9510
 Clinical Study Report: MT Date: 19 April 2013 Page 2 of 9510") Date: 19 April 2013 Page 2 of 9510 2. SYNOPSIS Name of Sponsor: Amgen Research (Munich), formerly Micromet AG/Micromet GmbH, Staffelseestrasse 2, 81477 Munich, Germany Name of Finished Product: Blinatumomab
Date: 19 April 2013 Page 2 of 9510 2. SYNOPSIS Name of Sponsor: Amgen Research (Munich), formerly Micromet AG/Micromet GmbH, Staffelseestrasse 2, 81477 Munich, Germany Name of Finished Product: Blinatumomab
Richter s Syndrome: Risk, Predictors and Treatment
 Richter s Syndrome: Risk, Predictors and Treatment 10/23/2015 John N. Allan MD Assistant Professor of Medicine Division of Hematology and Medical Oncology CLL Research Center Weill Cornell Medicine Agenda
Richter s Syndrome: Risk, Predictors and Treatment 10/23/2015 John N. Allan MD Assistant Professor of Medicine Division of Hematology and Medical Oncology CLL Research Center Weill Cornell Medicine Agenda
Dana-Farber Cancer Institute, Boston, MA, USA; 2 Fred Hutchinson Cancer Research Center, Seattle, WA, USA; 3
 Ibrutinib in Combination With Low-Dose Dexamethasone in Patients With Relapsed or Relapsed and Refractory Multiple Myeloma: Results From a Multicenter Phase 2 Trial Paul G. Richardson, MD 1 *, William
Ibrutinib in Combination With Low-Dose Dexamethasone in Patients With Relapsed or Relapsed and Refractory Multiple Myeloma: Results From a Multicenter Phase 2 Trial Paul G. Richardson, MD 1 *, William
Phase I Study of Carfilzomib and Panobinostat for Patients with Relapsed and Refractory Myeloma: A Multicenter MMRC Clinical Trial
 Phase I Study of Carfilzomib and Panobinostat for Patients with Relapsed and Refractory Myeloma: A Multicenter MMRC Clinical Trial Jonathan L. Kaufman, Todd Zimmerman, Cara A. Rosenbaum, Anuj Mahindra,
Phase I Study of Carfilzomib and Panobinostat for Patients with Relapsed and Refractory Myeloma: A Multicenter MMRC Clinical Trial Jonathan L. Kaufman, Todd Zimmerman, Cara A. Rosenbaum, Anuj Mahindra,
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia
 Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia Abstract 102 Wei AH, Strickland SA, Roboz GJ, Hou J-Z, Fiedler W, Lin TL,
Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia Abstract 102 Wei AH, Strickland SA, Roboz GJ, Hou J-Z, Fiedler W, Lin TL,
CLL: Future Therapies. Dr. Anca Prica
 CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
NASDAQ: TGTX. 33 rd Annual JP Morgan Healthcare Conference
 NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Mantle Cell Lymphoma: Update in Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency
 Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial
 Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial 2014-309-00CH1 Presenter: Jifang Gong, Beijing Cancer Hospital Lin Shen 1, Li Zhang 2, Hongyun Zhao 2, Wenfeng Fang 2,
Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial 2014-309-00CH1 Presenter: Jifang Gong, Beijing Cancer Hospital Lin Shen 1, Li Zhang 2, Hongyun Zhao 2, Wenfeng Fang 2,
Clinical Commissioning Policy Proposition: Bortezomib for relapsed/refractory mantle cell lymphoma
 Clinical Commissioning Policy Proposition: Bortezomib for relapsed/refractory mantle cell lymphoma Reference: NHS England xxxxx 1 First published: TBC Prepared by NHS England Specialised Services Clinical
Clinical Commissioning Policy Proposition: Bortezomib for relapsed/refractory mantle cell lymphoma Reference: NHS England xxxxx 1 First published: TBC Prepared by NHS England Specialised Services Clinical
Follicular Lymphoma New Agents. Idelalisib
 Indolent Lymphoma Workshop Bologna 2017 Follicular Lymphoma New Agents Idelalisib Sven de Vos, MD, PhD Director, UCLA Lymphoma Program Los Angeles, CA Disclosures of Sven de Vos Company name Research support
Indolent Lymphoma Workshop Bologna 2017 Follicular Lymphoma New Agents Idelalisib Sven de Vos, MD, PhD Director, UCLA Lymphoma Program Los Angeles, CA Disclosures of Sven de Vos Company name Research support
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
IMBRUVICA. ibrutinib NEW ZEALAND DATA SHEET
 1. PRODUCT NAME IMBRUVICA 140 mg capsules IMBRUVICA ibrutinib NEW ZEALAND DATA SHEET 2. QUALITATIVE AND QUANTITATIVE COMPOSITION IMBRUVICA is supplied as white opaque capsules that contain 140 mg ibrutinib
1. PRODUCT NAME IMBRUVICA 140 mg capsules IMBRUVICA ibrutinib NEW ZEALAND DATA SHEET 2. QUALITATIVE AND QUANTITATIVE COMPOSITION IMBRUVICA is supplied as white opaque capsules that contain 140 mg ibrutinib
SEQUENCING FOLLICULAR LYMPHOMA
 SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies
 December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
Daratumumab: Mechanism of Action
 Phase 3 Randomized Controlled Study of Daratumumab, Bortezomib and Dexamethasone (D) vs Bortezomib and Dexamethasone () in Patients with Relapsed or Refractory Multiple Myeloma (RRMM): CASTOR* Antonio
Phase 3 Randomized Controlled Study of Daratumumab, Bortezomib and Dexamethasone (D) vs Bortezomib and Dexamethasone () in Patients with Relapsed or Refractory Multiple Myeloma (RRMM): CASTOR* Antonio
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014
![[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014](/thumbs/73/68853651.jpg "[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014") [ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
Clinical Commissioning Policy: Bortezomib for relapsed/refractory mantle cell lymphoma (all ages) NHS England Reference: P
 NHS England Reference: P") Clinical Commissioning Policy: Bortezomib for relapsed/refractory mantle cell lymphoma (all ages) NHS England Reference: 1735P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Clinical Commissioning Policy: Bortezomib for relapsed/refractory mantle cell lymphoma (all ages) NHS England Reference: 1735P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents