pan-canadian Oncology Drug Review Final Clinical Guidance Report Ipilimumab (Yervoy) for First Line Advanced Melanoma December 22, 2014
|
|
|
- Beverley Owen
- 5 years ago
- Views:
Transcription
1 pan-canadian Oncology Drug Review Final Clinical Guidance Report Ipilimumab (Yervoy) for First Line Advanced Melanoma December 22, 2014
2 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended to help Canadian health systems leaders and policymakers make well-informed decisions and thereby improve the quality of health care services. While patients and others may use this report, they are made available for informational and educational purposes only. This report should not be used as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision making process, or as a substitute for professional medical advice. Liability pcodr does not assume any legal liability or responsibility for the accuracy, completeness or usefulness of any information, drugs, therapies, treatments, products, processes, or services disclosed. The information is provided "as is" and you are urged to verify it for yourself and consult with medical experts before you rely on it. You shall not hold pcodr responsible for how you use any information provided in this report. Reports generated by pcodr are composed of interpretation, analysis, and opinion on the basis of information provided by pharmaceutical manufacturers, tumour groups, and other sources. pcodr is not responsible for the use of such interpretation, analysis, and opinion. Pursuant to the foundational documents of pcodr, any findings provided by pcodr are not binding on any organizations, including funding bodies. pcodr hereby disclaims any and all liability for the use of any reports generated by pcodr (for greater certainty, "use" includes but is not limited to a decision by a funding body or other organization to follow or ignore any interpretation, analysis, or opinion provided in a pcodr report). FUNDING The pan-canadian Oncology Drug Review is funded collectively by the provinces and territories, with the exception of Quebec, which does not participate in pcodr at this time pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW i
3 INQUIRIES Inquiries and correspondence about the pan-canadian Oncology Drug Review (pcodr) should be directed to: pan-canadian Oncology Drug Review 1 University Avenue, suite 300 Toronto, ON M5J 2P1 Telephone: Fax: info@pcodr.ca Website: pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW ii
4 TABLE OF CONTENTS DISCLAIMER AND FUNDING... i INQUIRIES... ii TABLE OF CONTENTS... iii 1 GUIDANCE IN BRIEF Background Key Results and Interpretation Conclusions CLINICAL GUIDANCE Context for the Clinical Guidance Interpretation and Guidance Conclusions BACKGROUND CLINICAL INFORMATION SUMMARY OF PATIENT ADVOCACY GROUP INPUT SUMMARY OF PROVINCIAL ADVISORY GROUP (PAG) INPUT SYSTEMATIC REVIEW Objectives Methods Results Ongoing Trials SUPPLEMENTAL QUESTIONS Comparative Effectiveness of 1 st -Line Ipilimumab 3mg/kg versus 10mg/kg Effectiveness and Safety of 1 st -Line Ipilimumab 3 mg/kg ABOUT THIS DOCUMENT APPENDIX A: LITERATURE SEARCH STRATEGY REFERENCES pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW iii
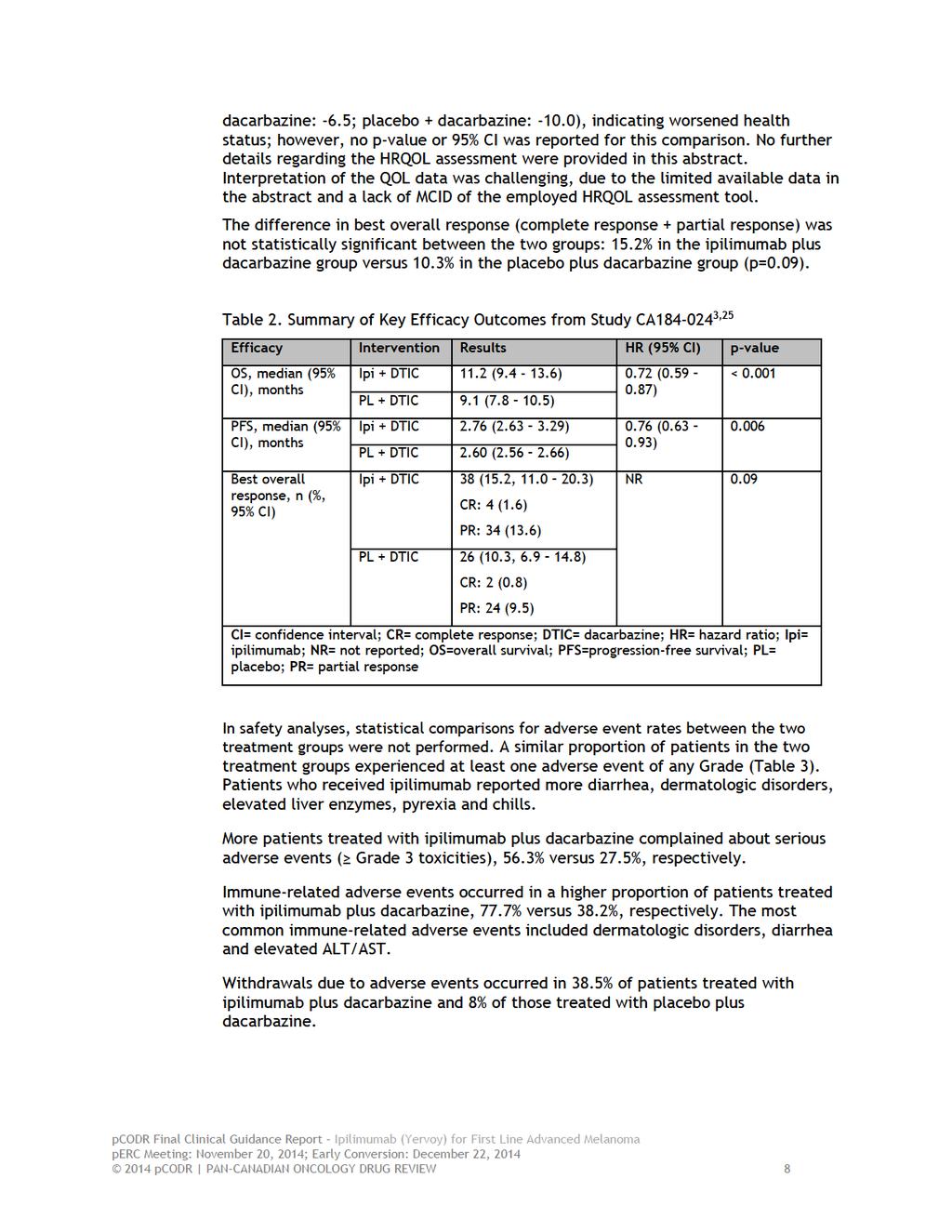
5 1 GUIDANCE IN BRIEF 1.1 Background The purpose of this review was to evaluate the effect of ipilimumab, either alone or in combination, on patient outcomes compared to commonly used therapies, placebo, or best supportive care in the treatment of patients with unresectable melanoma (stage III or stage IV) who had no previous systemic therapy. In 2012, ipilimumab was initially approved by Health Canada for the treatment of unresectable or metastatic melanoma in patients who have failed or do not tolerate other systemic therapy for advanced disease. 1 In September 2014, it was further approved as first line therapy of unresectable or metastatic melanoma. 2 The Health Canadarecommended dose for ipilimumab, in both previously treated and untreated patients, is 3 mg/kg administered intravenously over a 90-minute period every 3 weeks for a total of four doses. 1 The funding indication currently being sought by the manufacturer is for ipilimumab 3 mg/kg in the first line treatment of advanced melanoma. 1.2 Key Results and Interpretation Systematic Review Evidence One multinational, randomized, double-blind trial was identified that compared the use of ipilimumab 10 mg/kg plus dacarbazine versus dacarbazine plus placebo in patients with previously untreated unresectable stage III or stage IV melanoma (Study CA ). 3 The baseline characteristics were balanced between the treatment groups. The mean age of patients was 57.5 years in the ipilimumab-dacarbazine group and 56.4 years in the dacarbazine-placebo group. Approximately 71% of patients in each group had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 (patients were fully active and able to carry on all pre-disease performance without restriction). Patients with CNS metastases, ocular or mucosal melanoma, patients on chronic steroids or immune suppressive agents or with a history or autoimmune disease were excluded from the trial. Efficacy The CA study demonstrated a statistically significant improvement in overall survival, its primary outcome, in favour of ipilimumab-dacarbazine (median 11.2 months) compared to dacarbazine-placebo (median 9.1 months); HR 0.72, 95% confidence interval (CI) 0.59 to A statistically significant difference was also demonstrated for progression-free survival in favour of ipilimumab-dacarbazine. Health-related quality of life (HRQOL) results for this trial were reported in abstract form only. 4 Patients in both groups reported a declined average Global Health Status (GHS) score from baseline (ipilimumab-dacarbazine, -6.5; dacarbazine-placebo, -10.0), indicating worsened health status; however, no p-value or 95% CI was reported for this comparison. Given the limited details of the HRQOL data and the methods used to collect the data, as well as the lack of a validated minimal clinically important difference, interpretation of these data is difficult pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 1
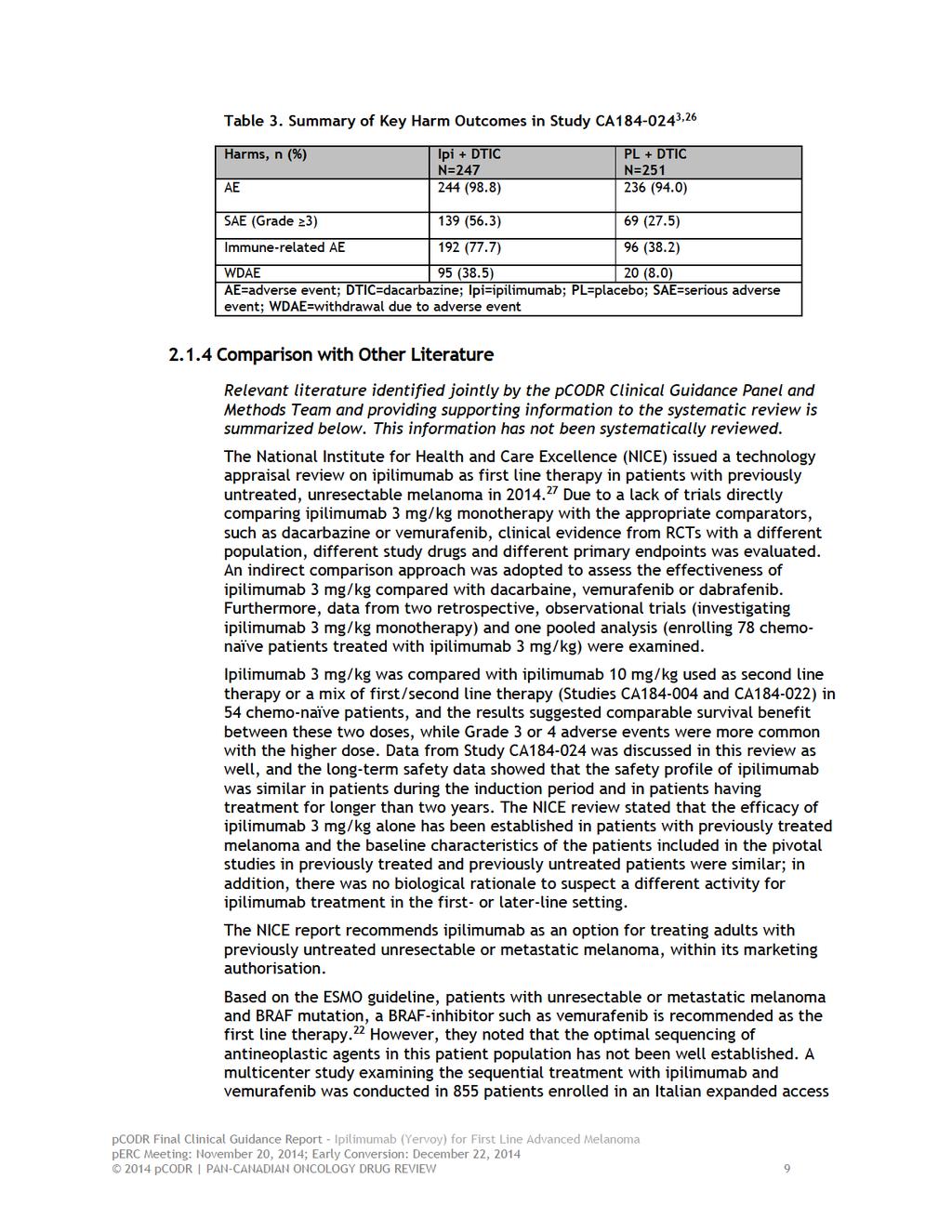
6 Safety No statistical comparisons of the rates of adverse events between the treatment groups were performed. A similar proportion of patients in both treatment groups experienced at least one adverse event of any Grade. Patients who received ipilimumab-dacarbazine experienced more diarrhea, dermatologic disorders, elevated liver enzymes, pyrexia, and chills. Grade 3 or higher adverse events occurred in more patients who received ipilimumabdacarbazine (56.3%) than in patients who received dacarbazine-placebo (27.5%). Immune-related adverse events occurred in a higher proportion of patients treated with ipilimumab-dacarbazine than in those treated with dacarbazine-placebo, 77.7% versus 38.2%, respectively. The most common immune-related adverse events were dermatologic disorders, diarrhea, and elevated ALT/AST. Withdrawals due to adverse events occurred in 38.5% of patients treated with ipilimumabdacarbazine and in 8% of those treated with dacarbazine-placebo Additional Evidence pcodr received input on ipilimumab for the first-line treatment of advanced melanoma from one patient advocacy group, Melanoma Network of Canada (MNC). Provincial Advisory Group input was obtained from all nine provinces participating in pcodr. pcodr previously reviewed the use of ipilimumab 3 mg/kg in patients with unresectable Stage III or Stage IV melanoma who received prior systemic therapy in The pcodr Expert Review Committee (perc) recommended funding ipilimumab, conditional on the cost-effectiveness being improved to an acceptable level, in patients with unresectable Stage III or Stage IV melanoma who have received prior systemic therapy. 5 In addition, two supplemental questions were identified during development of the review protocol as relevant to the pcodr review of ipilimumab and are discussed as supporting information: Comparison of the clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma o No evidence was found in the literature on the comparative efficacy and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma. The clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose used as first line therapy for patients with unresectable or metastatic melanoma. o o One pooled analysis of 78 patients demonstrated median overall survival of months. 6 Many limitations were identified for this pooled analysis. Two ongoing retrospective observational studies (studies CA and CA ) reported median overall survivals of 11.5 months for 90 patients and 14.3 months for 120 patients, respectively. 7,8 The results from the two observational studies should be interpreted with caution due to the high risk of bias associated with their design pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 2
7 1.2.3 Interpretation and Guidance Burden of Illness and Need It is estimated that 6,500 Canadians will be diagnosed with melanoma in 2014, and approximately 1100 patients will die of melanoma in Unresectable stage III or IV melanoma carries a poor prognosis with a median survival of 6.2 months and one-year survival of 25%. 10 Recently, Health Canada has approved the use of ipilimumab 3 mg/kg in the first-line treatment of patients with advanced melanoma. 2 Dacarbazine had been the mainstay of treatment up until 2011 ipilimumab demonstrated an improvement in overall survival in patients with pre-treated unresectable stage III or IV melanoma. 11 There is no evidence that chemotherapy offers any benefit in either quality of life or in overall survival, and as such dacarbazine is felt to be only very modestly effective in inducing responses. 12,13 Effectiveness In patients with previously untreated advanced melanoma, there are no randomized trials comparing ipilimumab at 3 mg/kg for four doses versus dacarbazine or versus ipilimumab at 10 mg/kg. Evidence from one pooled analysis of four RCTs and from two retrospective observational studies was used to understand the effectiveness of ipilimumab at 3 mg/kg in this group of patients. Notwithstanding the limitations of making comparisons across trials, the survival curves in advanced melanoma patients who received ipilimumab at 3 mg/kg in the first-line setting are similar to those who receive it as subsequent therapy. Dacarbazine is only very modestly effective in inducing responses in melanoma and there is no evidence that it improves either quality of life or overall survival, with less than 3% of patients getting long-term survival benefit Most patients only receive one or two cycles of dacarbazine and are then switched to ipilimumab as the median PFS of dacarbazine is only 6 weeks (i.e. 1 st assessment). As there remains some uncertainty about the dose effect of ipilimumab, the US FDA, in their approval of ipilimumab in the first-line setting, mandated that the manufacturer perform a randomized trial comparing the 10 mg/kg dose to the 3 mg/kg dose. This study (BMS 169) has been completed and the results are expected in early Safety In the CA study, 56.3% of patients receiving ipilimumab-dacarbazine experienced a Grade 3 or higher adverse event whereas 27.5% of patients receiving dacarbazine + placebo experienced a Grade 3 or higher adverse event. The most common adverse events are skin related, with the majority being Grade 1 or 2. Although the CA study had a higher rate of withdrawal due to adverse events in the group that received ipilimumab + dacarbazine, most of those were immune-related adverse events which are now better understood and are rapidly reversible with the use of treatment algorithms. The exception to rapid reversibility of immune-related adverse events are the endocrine side effects, which generally require several weeks to months to reverse and about 46% of patients will require long-term steroid replacement. BRAF Mutation-Positive Advanced Melanoma Most patients with BRAF mutated metastatic melanoma are treated with a BRAF inhibitor as first-line therapy. There are no randomized trials comparing upfront treatment with a BRAF inhibitor (vemurafenib or dabrafenib) versus ipilimumab in treatment-naïve patients. Treatment resistance to a BRAF inhibitor is almost always inevitable and the median duration of response to a BRAF inhibitor is less than seven months, whereas approximately 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 3
8 20% of patients who receive ipilimumab experience long-term survival and do not require further treatment. 3 Approximately 30% of patients treated with a BRAF inhibitor will experience an explosive recurrence and many of those will not be candidates to receive ipilimumab, due to a rapid decline in performance status or the development of CNS metastases requiring steroid use. There is uncertainty with respect to sequencing BRAF therapy with ipilimumab; however, some researchers are now moving in the direction of ipilimumab as first-line in patients with good performance status and slower progressing tumours, whereas BRAF inhibitors are reserved for patients with poorer performance status and more rapidly progressing tumours. 1.3 Conclusions The Clinical Guidance Panel concluded that there is an overall net clinical benefit to ipilimumab monotherapy 3 mg/kg in the first-line treatment of patients with unresectable or metastatic (i.e., Stage III-IV) melanoma with ECOG performance status of 0 or 1 and who are not receiving immunosuppressive therapy. This conclusion was based on several factors: One well-conducted randomized controlled trial that demonstrated a clear benefit in overall survival and progression free survival in favour of ipilimumab 10 mg/kg plus dacarbazine compared to dacarbazine plus placebo. A pooled data set from four RCTs, as well as two observational studies that provided supporting evidence of the effectiveness of the 3 mg/kg dose in the firstline setting. The Clinical Guidance Panel also considered that from a clinical perspective: The Health Canada approved dose in the first-line setting is 3 mg/kg for four doses, which is based on the second line study of ipilimumab 3 mg/kg versus gp100 vaccine. The optimal dose in the first line setting is being addressed by the CA study which is comparing the 10 mg/kg dose versus the 3 mg/kg dose in the first-line setting. The results of that study are expected in the first quarter of 2016, and until that time, the CGP agreed that there is no reason or evidence to expect that Ipilimumab 3 mg/kg would be any less effective in the first line than in the second line. Most Canadian patients treated in the first-line setting with dacarbazine receive ipilimumab in the second line, and the majority of those patients are not receiving an overall survival benefit from dacarbazine. Ipilimumab should also be available for the first line treatment of patients with BRAF mutation positive melanoma who have low bulk disease, good performance status and whose disease is not progressing rapidly, as these patients can achieve a long term response from treatment with ipilimumab pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 4
9 2 CLINICAL GUIDANCE This Clinical Guidance Report was prepared to assist the pcodr Expert Review Committee (perc) in making recommendations to guide funding decisions made by the provincial and territorial Ministries of Health and provincial cancer agencies regarding ipilimumab for advanced melanoma. The Clinical Guidance Report is one source of information that is considered in the perc Deliberative Framework. The perc Deliberative Framework is available on the pcodr website, This Clinical Guidance is based on: a systematic review of the literature regarding ipilimumab conducted by the pcodr Clinical Guidance Panel (CGP) and the pcodr Methods Team; input from patient advocacy groups; input from the Provincial Advisory Group; and supplemental issues relevant to the implementation of a funding decision. The systematic review and supplemental issues are fully reported in Sections 6 and 7. Background clinical information provided by the CGP, a summary of submitted Patient Advocacy Group Input on ipilimumab and a summary of submitted Provincial Advisory Group Input on ipilimumab are provided in Sections 3, 4 and 5 respectively. 2.1 Context for the Clinical Guidance Introduction Unresectable stage III or stage IV melanoma is an aggressive skin malignancy with poor prognosis, and treatment options for this patient population are limited. 20,21 The currently accepted standard therapy for patients with advanced melanoma include BRAF inhibitors, MEK inhibitors, immunotherapy (e.g. ipilimumab), and dacarbazine- or paclitaxel-based systemic chemotherapy. 21 Ipilimumab is a monoclonal antibody that binds to and blocks cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), which is located on cytotoxic T lymphocytes, and may play a role in regulating immune response. 2 In 2012, ipilimumab was approved by Health Canada for the treatment of unresectable or metastatic melanoma in patients who have failed or do not tolerate other systemic therapy for advanced disease. 1 In September 2014, it was further approved as first line therapy of unresectable or metastatic melanoma. 2 The Health Canada-recommended dose for ipilimumab in both previously treated and untreated patients is 3 mg/kg administered intravenously over a 90-minute period every 3 weeks for a total of four doses. 1 Ipilimumab, at a dose of 3 mg/kg, has been approved as first-line and second-line therapy of patients with advanced unresectable melanoma by the US Food and Drug Administration (FDA) and European Medicine Agency (EMA) Currently, the manufacturer is requesting funding for ipilimumab 3 mg/kg as first line treatment of advanced melanoma Objectives and Scope of pcodr Review To evaluate the effect of ipilimumab, either alone or in combination, on patient outcomes compared to commonly used therapies, placebo, or best supportive care in the treatment of patients with unresectable melanoma (stage III or stage IV) who had no previous systemic therapy pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 5
10
11
12
13
14 programme. 28 These patients either failed prior systemic therapy or were intolerant to at least one systemic treatment. Among the 855 patients, 173 had positive BRAF status and 93 (53.7%) of them were treated sequentially with both treatments: 48 patients received vemurafenib (doses and treatment duration were not specified) upon disease progression with ipilimumab, while 45 patients received ipilimumab (3 mg/kg intravenously every 3 weeks for 4 doses) upon disease progression with vemurafenib. The median overall survival was 14.5 months (95% CI 11.1 to 17.9) for the first group and 9.7 months (95% CI 4.6 to 14.9) for the second group, p = These preliminary findings suggested that in patients with unresectable or metastatic melanoma and BRAF mutation, to initiate the sequential treatment with ipilimumab may be associated with better survival compared with the reverse sequence. However, the validity of the study results cannot be assessed due to the nature of the study design (small observational study) and the insufficient details presented in this abstract. Furthermore, the effects of the sequential treatment need to be evaluated in patients without prior systemic therapy, preferably in a larger prospective study. On April 18, 2012, the pcodr Expert Review Committee (perc) recommended funding ipilimumab, conditional on the cost-effectiveness being improved to an acceptable level, in patients with unresectable Stage III or Stage IV melanoma who have received prior systemic therapy. 5 perc determined that there is a net clinical benefit associated with ipilimumab, based on clinically meaningful improvements in both relative and absolute measures of overall survival in favour of ipilimumab. The key evidence was a randomized controlled trial comparing ipilimumab 3 mg/kg plus gp100 vaccine versus ipilimumab 3 mg/kg plus placebo versus gp100 plus placebo. Median overall survival was statistically significantly higher in the ipilimumab plus gp100 group (10.0 months) compared with the gp100 plus placebo group (6.4 months), with a hazard ratio of 0.68 (95% CI 0.55 to 0.85; p<0.001). The median overall survival was 10.1 months in the ipilimumab plus placebo arm, which was similar to the ipilimumab plus gp100 arm. In addition, the proportion of patients alive after one year was similar for the ipilimumab plus gp100 group and for the ipilimumab plus placebo group (43.5% and 45.6%, respectively) and higher than the proportion of patients in the placebo plus gp100 group (25.3%). A similar trend was observed in the proportion of patients surviving at two years (21.6% and 23.5% versus 13.7%, respectively). perc noted that there were serious immune-related side effects associated with ipilimumab but that these adverse events are manageable by specialists with the support of other therapies directed at these symptoms and close patient monitoring of adverse events. perc considered that patients receiving ipilimumab should be managed in specialized cancer treatment centres with the medical expertise required to manage these side effects. However, perc also noted that this could impact the feasibility of implementing ipilimumab treatment as there would likely be additional costs associated with patient management and for adverse event monitoring Summary of Supplemental Questions Question 1: Comparison of the clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma. No evidence was found in the literature on the comparative efficacy and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 10
15 See section 7.1 for more information. Question 2: The clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose used as first line therapy for patients with unresectable or metastatic melanoma. A pooled analysis of treatment-naïve or chemotherapy-naïve advanced melanoma patients who were included in four RCTs (MDX010-20, MDX010-08, CA , and CA ) and two ongoing retrospective observational studies (CA , and CA ) investigated the use of 3mg/kg ipilimumab monotherapy in patients with unresectable or metastatic melanoma. The pooled analysis included 78 patients while studies CA and CA included 90 and 120 patients respectively. There were some clinically relevant differences in the baseline characteristics (such as ECOG performance status, presence of brain metastases, disease stage and duration of melanoma) between the three studies. Median overall survival was months in the pooled analysis, while it was 11.5 and 14.3 in studies CA and CA respectively. The one year survival rate was 54.1%, 49.4%, and 59.5% in the pooled analysis, study CA , and study CA , respectively. The two and three year survival rates in the pooled analysis were 31.6% and 23.7%, respectively. The adverse events were reported only in the pooled analysis and study CA Immune-related adverse events of any grade occurred in 84% and 52.5% of patients included in the pooled analysis and study CA , respectively, with Grade 3 or higher immune-related adverse events occurred 8.0% and 13.3% of patients in the pooled analysis and study CA , respectively. Results reported in the pooled analysis might be unreliable due to the many limitations in that analysis. In addition, results from the two observational studies should be interpreted with caution due to the high risk of bias associated with their design. See section 7.2 for more information Other Considerations Patient Advocacy Group Input From a patient perspective, first line access to ipilimumab would be beneficial to patients as response rates for current therapies remain limited. According to a survey, 26% of respondents indicated that they had some regression or stabilization of disease for less than 3 months with current therapies. However, none of the respondents indicated a durable response beyond 6 months before they were switched to another therapy. According to the Melanoma Network of Canada, 94% of respondents who received the full course of treatment with ipilimumab reported durable response, and specifically 83% respondents reported having a durable response over two (2) years. While ipilimumab has been known to cause significant adverse side effects (e.g., rash, potentially deadly colitis, fatigue, headaches), most of the respondents stated they would be willing to take all the necessary steps to manage those side-effects given that other current therapies often have severe and lasting side effects as well, including liver failure. PAG Input Input on the ipilimumab review was obtained from all of the nine provinces (Ministries of Health and/or cancer agencies) participating in pcodr. PAG identified that providing a more effective treatment upfront in the first-line setting eliminates the use of dacarbazine (generally ineffective), as the patients 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 11
16 eventually are treated with ipilimumab in the second line setting. From a PAG perspective, dosing issues with ipilimumab would be of greatest importance. PAG requires clarity on clinical effectiveness of ipilimumab 3 mg/kg for first-line therapy over the 10 mg/kg dose where there is data. Doses of 3 mg/kg versus 10 mg/kg, drug wastage and the number of patients requiring re-inductions could have an impact on the overall cost-effectiveness of ipilimumab and would need to be considered in the economic analysis. Other The final Health Canada product monograph for ipilimumab (Yervoy) provided by the manufacturer (Bristol-Myers Squibb [BMS] Canada) provides the following warnings: 2 Yervoy can cause severe and fatal immune-mediated adverse reactions, including enterocolitis, intestinal perforation, hepatitis, dermatitis, neuropathy, endocrinopathy, as well as toxcities in other organ systems. While most of these reactions occurred during the induction period, onset months after the last dose has been reported. For severe immune-mediated adverse reactions, Yervoy should be permanently discontinued; systemic high-dose corticosteroids with or without additional immunosuppressive therapy may be required for treatment. The monograph provides specific advice on managing the above adverse events. That advice includes when to discontinue ipilimumab and the administration of corticosteroids. The monograph notes that some patients with moderate to severe immune-mediated enterocolitis received infliximab following an inadequate response to corticosteroids. 2.2 Interpretation and Guidance Burden of Illness It is estimated that 6,500 Canadians will be diagnosed with melanoma in 2014, and approximately 1050 patients will die of melanoma in The majority of patients will present with early stage disease and be cured by surgery but those who present with advanced disease or who subsequently relapse, the prognosis remains poor. Although the number of patients developing melanoma is small compared to breast cancer or lung cancer, melanoma remains the number one cause of cancer death in women age 25 to 35, and causes a disproportionate number of years of life lost. Unresectable stage III or stage IV melanoma carries a poor prognosis with a median survival of 6.2 months and only 25.5% of patients surviving to one year, although recently new therapies have improved the prognosis and a small proportion are experiencing long term survival. Effectiveness One multinational, randomized, double-blind trial was identified that investigated the use of ipilimumab plus dacarbazine compared to placebo plus dacarbazine in patients with previously untreated unresectable stage III or stage IV melanoma (the CA study). 3 The trial population excluded patients with CNS metastases, ocular or mucosal melanoma, 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 12
17 patients on chronic steroids or immune suppressive agents or with a history of autoimmune disease. The patient demographics were well balanced between the two arms. Patients were accrued between August 2006 and January At a median follow up of 54 months 82.5% of the patients had died as of the data cutoff in March of Overall survival was statistically significantly higher in the dacarbazine + ipilimumab arm (median 11.2 months) versus the dacarbazine + placebo arm (median 9.1 months; p<0.001). In addition, PFS was also statistically significantly higher in the ipilimumab + dacarbazine group versus the dacarbazine + placebo group (2.76 months. versus 2.6 months, p = 0.006). The one, two, three and four year survivals were 47.5, 28.8, 21.2 and 19 percent in the ipilimumab containing arm respectively versus 36.4, 17.5, 12.1, and 9.6 percent for the dacarbazine + placebo arm respectively. The study met its primary endpoint of improving overall survival. More importantly the survival curve separated early and at 3-years was 20.8% in the ipilimumab plus dacarbazine arm compared with 12.2% in the dacarbazine plus placebo arm. As immuno-oncology has become more mainstream it has become apparent that clinical endpoints have to change and classic chemotherapy response criteria have to be modified. Thus the immune-related response criteria (irrc) and 1, 2 and 3 year survivals have become accepted as more meaningful endpoints in immune checkpoint inhibitor therapy. PFS is not a good surrogate endpoint and thus the primary endpoint of the trial was changed based on emerging evidence during the trial period. Some patients can progress with either pseudo-progression or true progression, and still experience a later response and long term survival. The choice of dose in the CA study was due to the fact that most of the earlier trials of ipilimumab in metastatic melanoma patients had used a dose of 10 mg/kg for four induction doses followed by a maintenance period. Therefore, the first-line registration trial (CA ), which is the primary study in this review, used a dose of 10 mg/kg of ipilimumab, in combination with dacarbazine which was the standard of care in the firstline treatment of metastatic melanoma at that time. The FDA approval mandated that the manufacturer conduct a trial of ipilimumab 10 mg/kg versus 3 mg/kg until disease progression in patients with previously untreated or previously treated advanced melanoma to see if dose had an effect on outcome. This trial has completed accrual and results are expected in early More recently the European Union and subsequently Health Canada approved ipilimumab in untreated metastatic melanoma patients at a dose of 3 mg/kg for four doses. There are no randomized studies comparing ipilimumab at a dose of 3 mg/kg for four doses versus dacarbazine in untreated metastatic melanoma patients or versus ipilimumab at 10 mg/kg. Evidence from one pooled analysis of four RCTs and from two retrospective observational studies was used to understand the effectiveness of ipilimumab at 3 mg/kg in this group of patients. 6-8 Notwithstanding the limitations of making comparisons across studies, the survival curves in untreated melanoma patients for patients who received ipilimumab at 3 mg/kg in the 1 st -line setting are similar to those who receive it as subsequent therapy. Dacarbazine is largely felt to be only very modestly effective in inducing responses in melanoma, as response rates have ranged from 7 to 10% in randomized studies There is no evidence that it improves either quality of life or overall survival, and less than 3% of patients getting long-term survival benefit Most patients only receive one or two cycles of dacarbazine and are then switched to ipilimumab as the median PFS of Dacarbazine is only 6 weeks (i.e. 1 st assessment). In fact, many melanoma oncologists consider dacarbazine an ineffective treatment with respect to overall survival pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 13
18 Safety Ipilimumab is associated with well-defined immune related adverse events. In the CA study, ipilimumab + dacarbazine was associated with a higher rate of adverse events that led to withdrawal than dacarbazine + placebo (38.5% versus 8.0%, respectively), with most being immune-related. Colitis is the most frequent grade III/IV immune-related AE, ranging from 5 to 7% at a dose of 3 mg/kg. Rarely, colitis/diarrhea will be refractory to high dose steroids and will require infliximab at a dose of 5 mg/kg. Usually one dose suffices. Rare patients will require a colectomy (<1%). In the CA study when dacarbazine was combined with ipilimumab there was a 20% incidence of hepatotoxity as opposed to the previously reported rate of 2% when ipilimumab was given as a single agent at a dose of 3 mg kg. There were no patient deaths from hepatotoxicity and all cases reversed with either cessation of therapy or with the use of immunosuppressive therapy such as high dose glucocorticoids. 77.7% of patients on the CA study reported an immune-related adverse event on the ipilimumab + DTIC arm with 41.7% reporting an immune-related adverse event of grade III or greater versus an immune-related adverse event rate of 38.2% in the DTIC + placebo arm (6% with an immune-related adverse event of grade III or greater). The most common adverse event is skin with the majority being Grade I/II. Although the CA study had a higher rate of withdrawal due to adverse events in the group that received ipilimumab +dacarbazine, most of those were immunerelated adverse events which are now better understood and are rapidly reversible with the use of treatment algorithms. The exception to rapid reversibility of immune-related adverse events are the endocrine side effects, which generally require several weeks to months to reverse and about 46% of patients will require long term steroid replacement. Dacarbazine has a higher incidence of nausea, vomiting and myelosuppression than ipilimumab. Need The survival of metastatic melanoma patients had not changed for several decades, and prior to 2010 there was no evidence that any systemic treatment had any impact on overall survival. Dacarbazine remained the mainstay of treatment up until 2011, with select centres offering high dose IL-2. The first drug trial to report an improvement in overall survival was the MDX-020 trial of ipilimumab +/- gp100 versus gp100 alone in pre-treated unresectable stage III/IV melanoma patients. This led to the approval of ipilimumab in either the 1 st line or subsequent line of therapy by the FDA in metastatic melanoma patients, at a dose of 3 mg/kg every 3 weeks for four doses. Both Health Canada and the European Medicines Agency (EMA) subsequently approved Ipilimumab 3 mg/kg in patients who had failed a prior treatment regimen in metastatic melanoma. perc recommended the funding of ipilimumab at 3 mg/kg in the 2 nd -line setting, conditional on the costeffectiveness being improved to an acceptable level. 5 There is no randomized evidence that chemotherapy offers any benefits in either quality of life or in overall survival, with more modern response rates ranging from 7 to 10%, and less than 2% five year survival. 12,14-18 Dacarbazine is felt to be only very modestly effective in inducing responses. BRAF Mutation-Positive Advanced Melanoma Most patients with BRAF mutated metastatic melanoma are now being treated with a BRAF inhibitor as 1 st line therapy. There are no randomized studies comparing upfront treatment of a BRAF inhibitor such as vemurafenib or dabrafenib versus ipilimumab in treatment naïve patients. Treatment resistance to a BRAF inhibitor is almost always inevitable and 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 14
19 the median duration of response to a BRAF inhibitor is less than 7 months. BRAF inhibitor therapy is given as an oral medication twice a day and is associated with significant toxicities including but not limited to pyrexia, arthralgias, skin rash, photosensitivity, fatigue and nausea. Currently the recommended treatment using a BRAF inhibitor is to treat until disease progression or until unacceptable toxicity. Ipilimumab is given as four 90 minute infusions over a period of 12 weeks and approximately 20% of patients experience long term survival and do not require further treatment. 38% of patients versus 8% of patients withdrew from the CA study due to adverse events, but adverse events are almost always reversible (most reversing fully within 4 to 8 weeks). Approximately 30 per cent of patients treated with a BRAF inhibitor will experience an explosive recurrence and many will not be candidates to receive ipilimumab, due to a rapid decline in performance status or the development of CNS metastases requiring steroid use. There is much debate on how to sequence BRAF therapy with ipilimumab and many researchers are now moving in the direction of ipilimumab in patients with good performance status and slower progressing tumors, while BRAF inhibitors are reserved for those patients with a poorer performance status and more rapidly progressing tumors. A retrospective review in 855 patients treated on the EAP program in Italy suggested improved survival in patients who received ipilimumab prior to a BRAF inhibitor as opposed to ipilimumab after a BRAF inhibitor (45 patients versus 48 patients). 28 Again this was a retrospective review and numbers were small. There are ongoing studies examining the appropriate sequencing of therapy for patients with advanced melanoma who have a BRAF mutation. Results are not expected for two years. 2.3 Conclusions The Clinical Guidance Panel concluded that there is an overall net clinical benefit to ipilimumab monotherapy 3 mg/kg in the first-line treatment of patients with unresectable or metastatic (i.e., Stage III-IV) melanoma with ECOG performance status of 0 or 1 and who are not receiving immunosuppressive therapy. This conclusion was based on several factors: One well-conducted randomized controlled trial that demonstrated a clear benefit in overall survival and progression free survival in favour of ipilimumab 10 mg/kg plus dacarbazine compared to dacarbazine plus placebo. A pooled data set from four RCTs, as well as two observational studies that provided supporting evidence of the effectiveness of the 3 mg/kg dose in the firstline setting. The Clinical Guidance Panel also considered that from a clinical perspective: The Health Canada approved dose in the first-line setting is 3 mg/kg for four doses, which is based on the second line study of ipilimumab 3 mg/kg versus gp100 vaccine. The optimal dose in the first line setting is being addressed by the CA study which is comparing the 10 mg/kg dose versus the 3 mg/kg dose in the first-line setting. The results of that study are expected in the first quarter of 2016, and until that time, the CGP agreed that there is no reason or evidence to expect that Ipilimumab 3 mg/kg would be any less effective in the first line than in the second line pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 15
20 Most Canadian patients treated in the first-line setting with dacarbazine receive ipilimumab in the second line, and the majority of those patients are not receiving an overall survival benefit from dacarbazine. Ipilimumab should also be available for the first line treatment of patients with BRAF mutation positive melanoma who have low bulk disease, good performance status and whose disease is not progressing rapidly, as these patients can achieve a long term response from treatment with ipilimumab pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 16
21 3 BACKGROUND CLINICAL INFORMATION This section was prepared by the pcodr Melanoma Clinical Guidance Panel. It is not based on a systematic review of the relevant literature. 1.1 Description of the Condition Melanoma is a malignancy of melanocytes which are distributed throughout the body. Although primary melanoma can occur in a variety of sites, skin is the most common, comprising 95% of cases. In Canada 6500 new cases of primary melanoma were diagnosed in 2014 and approximately 1100 individuals will die from melanoma each year. 9 The incidence of melanoma has been steadily increasing over the past 60 years. Currently the lifetime probability of developing melanoma for women is 1 in 85 and for men is 1 in Staging of melanoma is based on the current American Joint Committee on Cancer (AJCC) 7th edition classification. 30 The tumour characteristics principally involve the Breslow height, presence or absence of ulceration, and mitotic rate. The detection of microscopic and macroscopic lymph node involvement, lactate dehydrogenase (LDH) and sites of metastatic disease are also incorporated in the staging classification. All of these prognostic factors have important impact upon patient outcomes and also serve to guide management decisions. 1.2 Accepted Clinical Practice In early stage melanoma, cures are commonly achieved with surgery alone. The primary site is excised with appropriate surgical margins. Depending upon the T stage and location of the primary, a sentinel node biopsy (SNB) may be performed to assess regional nodal status. If the sentinel node contains metastatic disease, then a completion lymph node dissection of the regional basin is often performed. This additional procedure has been shown to reduce the risk of regional occurrence. 31 Although only 5% of patients present with metastatic disease, the majority of patients who ultimately die from melanoma will have developed recurrent and/or distant disease. About 1/3 of patients with early stage melanoma will develop metastasis; however, 1/2 of the patients with nodal disease will recur and likely die from metastatic disease. 32 Brain metastases are common and occur in up to 75% of patients with overt metastatic disease. In highly selected patients with metastatic disease, clinical benefit may occur from surgical resection of known sites of disease and may result in long term survival. Unfortunately, most metastatic patients are not candidates for surgical resection and systemic treatment is the only alternative. The prognosis for these patients remains poor. The median survival has been 6-9 months with 5 year survival of approximately 6%. 10 With the more recent introduction of new and effective treatments, a significant improvement in survival is being realized. Over the past 30 years, standard first-line systemic treatment has been dacarbazine. 31,33 Although this alkylating agent is generally well tolerated, response rates are low and complete responses are rare. 34 In comparative studies the use of dacarbazine has not been shown to improve survival in metastatic melanoma Temozolomide, an oral imidazole 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 17
22 tetrazene derivative of dacarbazine, is activated to the active metabolite of dacarbazine, and has also been commonly used. In phase III trials comparing temozolomide directly to dacarbazine, similar progression free and overall survival rates were observed In the early 1990s the FDA approved the use of high dose Interleukin-2 based on phase II data showing a response rate of 16% and a durable complete response of 5%. 38,39 Unfortunately, high dose Interleukin-2 is associated with severe toxicity and requires intense cardiac monitoring and hemodynamic support. Interleukin-2 is largely unavailable in Canada. A wide spectrum of chemotherapeutic and immunological treatments has been explored in patients with metastatic melanoma. Until recently limited to no success has been achieved. It has become increasingly apparent that melanoma represents a heterogeneous group of diseases. A variety of genetic abnormalities exists within primary melanomas and their respective metastases and influence both cellular proliferation and ultimately response to therapy The MAP kinase signaling pathway appears to be a key regulatory mechanism for cell growth and differentiation in melanoma. 43 Mutations in the BRAF protein within this pathway can result in uncontrolled cellular proliferation and increased potential for metastatic spread. 44 Approximately 50% of human melanomas appear to have an activated mutation in BRAF which has become a key target for inhibition and potential therapeutic site. 45 Vemurafenib is a BRAF inhibitor that selectively targets the V600E mutation approved by Health Canada in February In a randomized phase III study, vemurafenib use led to a relative reduction of 63% in risk of death and 74% reduction in the risk of tumor progression. The overall response rate was 48%. 12 Vemurafenib has become the first-line treatment of advanced unresectable melanoma in patients harboring the V600 BRAF mutation. Dabrafenib is a similar targeted oral BRAF inhibitor which has a slightly different toxicity profile and which is similarly efficacious in the therapy of patients with BRAF mutant metastatic melanoma Unfortunately, for those patients who are BRAF positive, resistance to the BRAF inhibitors ultimately develops and they experience rapid and often unrelenting disease progression. In the remaining 50% of the patients who do not have BRAF mutation, the BRAF inhibitors are uniformly ineffective and additional therapies are needed. 1.3 Evidence-Based Considerations for a Funding Population Ipilimumab is a monoclonal antibody that binds to and blocks the cytotoxic T-lymphocyte associated antigen 4 (CTLA4) located on cytotoxic T-lymphocytes. CTLA4 appears to play an important role in the regulation of the immune response. 53,54 In 2012, Ipilimumab received a Health Canada indication for treatment of unresectable or metastatic melanoma in patients who have failed or did not tolerate other systemic therapy for advanced disease. Since that time it has been widely used across Canada as second line therapy given at a dose of 3 mg per kg given every 3 weeks for a total of 4 doses. Provision for re-induction has been provided in patients who progress following a response to ipilimumab treatment. The initial approval was principally based upon the findings of a multi-center, double blind placebo controlled trial consisting of three treatment arms randomly assigned 3:1:1: ipilimumab 3 mg/kg + cancer vaccine GP100, ipilimumab alone, GP100 alone. 11 The study 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 18
23 demonstrated an improvement on overall survival (HR 0.66) in the two ipilimumab containing arms compared to GP100 alone. Median overall survival for ipilimumab arms was 10 months compared to 6.4 months in GP100 alone arm. Adverse events were primarily immune related which included diarrhea/colitis, and endocrine problems. Fatigue, rash and anorexia were common but were seldom grade 3 or greater. The study represents the first randomized controlled trial which demonstrated an improvement in survival in patients with metastatic disease. In 2011, Robert and colleagues reported on a randomized controlled trial comparing Ipilimumab 10 mg/kg + dacarbazine 850 mg/m2 versus dacarbazine alone in patients who were previously untreated. 3 Overall survival was improved in the Ipilimumab containing arm (HR 0.72) and appeared to extend out to 3 years. The median survival was 11.2 months in the Ipilimumab arm compared to 9.1 months in the dacarbazine arm. Immune related events were observed in the Ipilimumab arm and grade 3 or 4 adverse events were more common (56.3% vs 27.5%). Rates of elevated liver enzymes appeared to be higher than observed in other studies in which Ipilimumab was used alone. Although the progression free survival and overall survival were similar in these trials, the relative impact of the 3 and 10 mg doses of ipilimumab which were used cannot be directly assessed. Furthermore the positive or negative effect on outcomes and toxicity which the GP100 or dacarbazine had within the combination arms of each trial also remains uncertain. 1.4 Other Patient Populations in Whom the Drug May Be Used A multi-centre randomized trial study which compares ipilimumab at 3 mg/kg versus 10 mg/kg in patients with unresectable/metastatic disease has completed accrual and the results have not yet been reported. There are also on-going studies specifically addressing the impact on patients with brain metastases and include combination with radiotherapy. Ipilimumab is currently being evaluated in patients who are at high risk for recurrence and is being compared to alpha-interferon, as well as in combination with other immunotherapies. Potential indications for ipilimumab are also being explored in other malignancies such as lung, head and neck, prostate, colon and pancreas pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 19
24 4 SUMMARY OF PATIENT ADVOCACY GROUP INPUT One patient advocacy group, Melanoma Network of Canada (MNC), provided input on ipilimumab (Yervoy) for the first-line treatment of adult patients with advanced (unresectable or metastatic) melanoma, and their input is summarized below. MNC conducted an online survey of patients from across Canada through a confidential online survey. Patients were recruited through a generic eblast requesting input from those patients that had been specifically treated with ipilimumab. The survey had a combination of multiple choice, rating and comment open ended questions. MNC reported a total of 18 patients who responded to the survey from 7 different provinces. From a patient perspective, first line access to ipilimumab would be beneficial to patients as response rates for current therapies remain limited. According to the survey, 26% of respondents indicated that they had some regression or stabilization of disease for less than 3 months with current therapies. However, none of the respondents indicated a durable response beyond 6 months, before they were switched to another therapy. According to MNC, 94% of respondents who received the full course of treatment with ipilimumab reported durable response, and specifically 83% respondents reported having a durable response over two (2) years. While ipilimumab has been known to cause significant adverse side effects (e.g., rash, potentially deadly colitis, fatigue, headaches), most of the respondents stated they would be willing to take all the necessary steps to manage those side-effects given that other current therapies often have severe and lasting side effects as well, including liver failure. Please see below for a summary of specific input received from the patient advocacy group. Quotes are reproduced as they appeared in the survey, with no modifications made for spelling, punctuation or grammar. The statistical data that was reported have also been reproduced as is according to the submission and have not been corrected. 4.1 Condition and Current Therapy Information Experiences Patients have with Advanced Melanoma According to MNC, 100% of survey respondents experienced pain and fatigue; 94% experienced loss of appetite, with 83% indicating some depression and loss of regular sleep. Based on prior surveys that were submitted to pcodr in the past, MNC found that key experiences for patients with melanoma included detrimental impact on their quality of life, loss of employment income, as well as negative impacts on caregiver and family related stresses. Below is a summary table of the key adverse physical effect or symptoms that respondents reported in the online survey. Adverse physical effect or symptom related to melanoma % of Respondents indicating symptom pain nausea loss of appetite headaches loss of mobility or immobility 50 9 neuropathy fatigue depression, anxiety or post-traumatic stress N (# of Respondents who responded) 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 20
25 Adverse physical effect or symptom related to melanoma % of Respondents indicating symptom sleep deprivation cognitive impairment 39 7 general weakness N (# of Respondents who responded) Patients Experiences with Current Therapy for Advanced Melanoma MNC reported that there have been several drug therapies approved in the last two years for metastatic melanoma. According to the online survey, 100% of respondents had been treated with some other form of therapy, prior to receiving ipilimumab. Of the 18 respondents, 78% of respondents had been treated with dacarbazine; 67% with interferon. When asked if they had had a positive response to the therapy, in terms of regression of disease or stabilization, it was reported that 26% of respondents indicated that they had some regression or stabilization of disease for less than 3 months. However, none of the respondents indicated a durable response beyond 6 months, before they were switched to another therapy. Below is a summary table that sets out the current therapy that the respondents reported receiving. # of respondents % of respondents indicating treatment Therapy Name: (total=18) Dacarbazine Interferon Zelboraf 2 11 Mekinist 0 0 Tafinlar 1 5 Docetaxel 1 5 According to MNC, 78% of the respondents indicated that the therapies listed above had done little to alleviate adverse symptoms and in the case of chemotherapy, had created more adverse side effects of fatigue, nausea, cognitive impairment, and hair loss. In particular, respondents who received Zelboraf and Tafinlar indicated almost immediate regression of disease, but also experienced rash, fatigue, sun sensitivity and intolerance or progression of disease that required them to stop that therapy. MNC asserted that oncologists are required to use a first line therapy that has been proven to be highly ineffective for most melanoma patients. As an example, MNC found that response rates for current therapies such as dacarbazine have generally been under 15%. While treatment options for some melanoma patients are improving, MNC believes that they remain limited, and for some types of melanoma, almost non-existent Impact of Advanced Melanoma and Current Therapy on Caregivers MNC reported that they did not include caregivers in this survey. MNC noted that they specifically focussed on the experiences of the patient after receiving treatment with ipilimumab as an approved second-line therapy, versus the patient experience with the approved first-line therapy. MNC believes that previous submission to pcodr have included sufficient information from caregivers on the benefits and disadvantages of ipilimumab as treatment for melanoma, and the experiences and side effects with other therapies to demonstrate the impact of advanced melanoma on caregivers pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 21
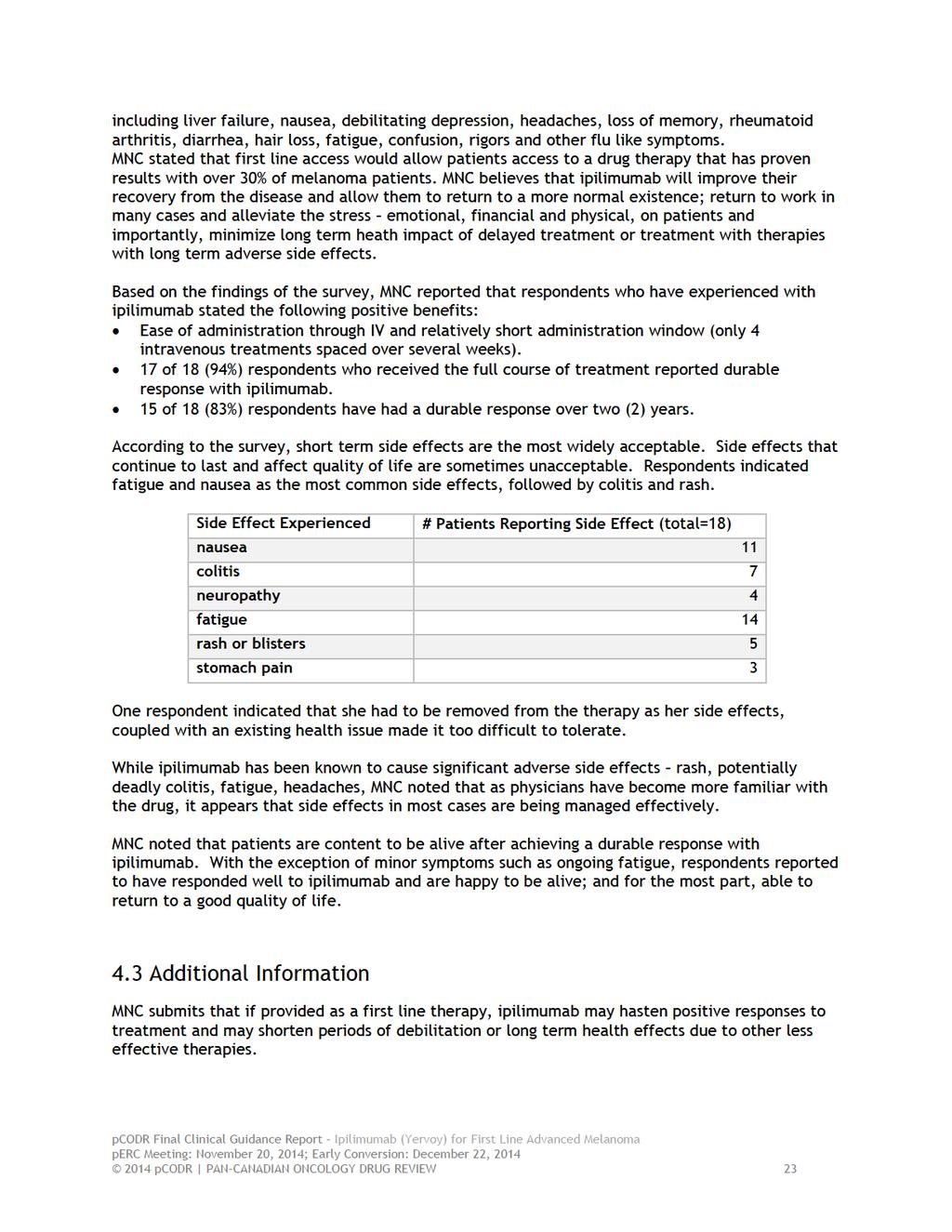
26 4.2 Information about the Drug Being Reviewed Patient Expectations for and Experiences To Date with Ipilimumab As part of the survey questions on patients expectation with using ipilimumab as a treatment, MNC asked respondents if they felt that having ipilimumab available as a first line therapy would be of benefit for patients and to describe what they felt are the key benefits or disadvantages with this therapy. 94% of respondents reported that access to ipilimumab as a first line therapy would benefit patients. 1 respondent did not know. None of the respondents indicated a disadvantage. Below are some of the comments that were received: I ended up on Yervoy twice. The first time I made it through ok, but it took a few months to see any improvement. I was worried that I was out of options. It worked and most of my tumours were gone. There were only a few small ones that were showing on scans. After about 8 months, those ones started to grow again. I went through a second round of treatment with Yervoy and have been basically cancer free for the last two years. I think it would benefit us to go directly to these new therapies instead of wasting time on old ones that don t work. I got sicker and sicker on my chemo, and just watched as my tumours burst through my skin, in my lungs and ruin my spine and liver. My wife was panicked, I was panicked and I thought I was going to die. Clearly we need more effective treatments sooner. Why do they put us through that, if they have something better? That to me is torture. Yervoy wasn t easy. I don t know if I could do it again if I had to. Steroids helped. I had a lot of headaches and diarrhea. I had a big rash too. But maybe having it right up front would have given me a shorter treatment time getting me back to work earlier. I missed a lot of time with having to go through chemo and then this, and it almost cost me my job and my house. I am lucky to be alive though and thankful for that. The big benefit I found is life I am here! What better benefit is that? Yervoy should be made available for doctors for first line therapy. Why sit there and try other drugs that don t work? I would guess that the government wouldn t sit back and do that if it was their own lives on the line. Why do the doctors have to jump through hoops when we have effective therapies? It is criminal in my mind. Yes to this as a front line therapy. There is no debating that. I have just been through treatment and am seeing good results. I am really tired and I am hoping that I start to feel better soon. The results make me feel hopeful, but I have been there before. I don t know if this will be a cure for me, but at least it may get me enough time to try something else. I am really glad that I don t have to continue to take more drugs for the moment. I think it should be available for all patients if their doctors feel it is right for them. According to MNC, while most patients surveyed have direct experience with the adverse side effects of therapies currently available, the survey results indicate that 100% of the respondents are still willing to accept side effects and the serious risks associated with ipilimumab if they know those side-effects can be effectively managed. Most notably, 88% of respondents stated they would be willing to take all the necessary steps to manage those side-effects. MNC noted that other therapies like dacarbazine and interferon have often very severe and lasting side effects 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 22
27
28 5 SUMMARY OF PROVINCIAL ADVISORY GROUP (PAG) INPUT The following issues were identified by the Provincial Advisory Group (PAG) as factors that could affect the feasibility of implementing a funding recommendation for ipilimumab (Yervoy) for the treatment of advanced melanoma. The Provincial Advisory Group includes representatives from provincial cancer agencies and provincial and territorial Ministries of Health participating in pcodr. The complete list of PAG members is available on the pcodr website ( Overall Summary Input on the ipilimumab (Yervoy) review was obtained from all of the nine provinces (Ministries of Health and/or cancer agencies) participating in pcodr. From a PAG perspective, key enablers to implementation include the familiarity with the use of ipilimumab and not requiring BRAF testing. PAG indicated that providing a more effective treatment upfront in the first-line setting eliminates the use of dacarbazine, a generally ineffective treatment, as these patients eventually are treated with ipilimumab in the second line setting. PAG identified that the uncertainty in the data for the 3mg/kg dose in the first line setting and in the use of ipilimumab over vemurafenib for BRAF mutation positive patients are potential barriers. Other key barriers PAG noted are the drug wastage and the high cost of ipilimumab. Please see below for more detailed PAG input on individual parameters. 5.1 Factors Related to Comparators PAG identified that the current standard of practice in the first-line treatment of patients with metastatic melanoma is vemuarfenib for patients with BRAF mutation positive metastatic melanoma and dacarbazine for BRAF negative patients. PAG noted that dacarbazine is not very effective and not well tolerated, thus, the majority of patients generally receive ipilimumab second-line. PAG noted that there may be no randomized controlled trial data available for ipilimumab in the first-line treatment at the 3mg/kg dose and would like clarity on clinical effectiveness of this dose for first-line treatment over the 10mg/kg dose where there is data. 5.2 Factors Related to Patient Population The number of patients with metastatic melanoma is relatively small. PAG noted that using ipilimumab in first-line instead of second-line would provide an option to dacarbazine, particulary for patients who are not BRAF mutation positive. As dacarbazine is considered to be ineffective and has significant toxicities, PAG noted that ipilimumab would replace dacarbazine and dacarbazine would no longer be considered for first-line treatment. Since patients eventually receive ipilimumab second-line and ipilimumab is currently funded in all provinces only for secondline, using ipilimumab in the first-line setting would eliminate the need to treat with dacarbazine first and provide access to a more effective treatment for patients upfront. This is an enabler to implementation as clinicians and patients are requesting use of ipilimumab in first-line pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 24
29 5.3 Factors Related to Accessibility Ipilimumab, being an intravenous drug, would be administered in an outpatient chemotherapy center for appropriate administration and monitoring of toxicities. Intravenous chemotherapy drugs would be fully funded (i.e. no co-payments for patients) in all jurisdictions for eligible patients, which is an enabler for patients. As ipilimumab is a high cost drug and requires monitoring of immune-mediated reactions post-infusion, PAG noted that smaller outpatient cancer centres may not have the resources to administer ipilimumab. This is a barrier as some patients will need to travel to larger cancer centres that have the resources and expertise to administer ipilimumab. 5.4 Factors Related to Dosing In the funding request and the Health Canada submission, the proposed dosing is 3mg/kg given every three weeks for first-line, which is the same as for second-line treatment. This is considered an enabler as there would be no confusion with dosing in the first-line versus second-line setting. However, PAG noted that there is a trial using 10mg/kg in firstline and has concerns regarding dose-creep and the costs of the higher dose, which are barriers. PAG would like perc to address the optimal dose in the first-line setting to achieve clinical benefits. PAG has concerns for incremental costs due to drug wastage, specifically in centers where vial sharing would be difficult because there would be only one patient in the day. As dose is based on weight and there are two vial sizes (50mg and 200mg), a dose of 210mg (3mg/kg x 70kg) would result in significant wastage given that any unused portion would be discarded. PAG noted that only four doses for induction are required and the defined number of doses is an enabler. However, PAG also noted that in the real-world experience, a higher percentage of patients require re-induction than indicated in trial data for second-line treatment. Doses of 10mg/kg, drug wastage and the number of patients requiring re-inductions are barriers to implementation and PAG would like these factors incorporated into the economic analysis. 5.5 Factors Related to Implementation Costs As dacarbazine is considered to be ineffective and not well tolerated, PAG noted that ipilimumab would replace dacarbazine for first-line treatment and the resources needed to treat with dacarbazine and its toxicities would be eliminated. Ipilimumab for first-line treatment would provide access to a more effective treatment upfront, particularly for patients who are not BRAF mutation positive. PAG indicated that the number of patients receiving ipilimumab would not be significantly more in first-line than in second-line and the costs of ipilimumab would just be shifted. This is an enabler to implementation as patients would not need to use dacarbazine first. PAG estimates that each treatment session would require up to 3 hours (90 minutes for the infusion and 1 hour for monitoring time for immune-related reactions post infusion) of chair time, which is a barrier. Since ipilimumab is already being used in the second-line 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 25
30 setting, PAG noted that health care professionals are already familiar with the preparation, administration and monitoring of ipilimumab, which is an enabler. BRAF testing is not required for the use of ipilimumab and this is an enabler. PAG is requesting advice around the use of ipilimumab versus vemurafenib for patients with BRAF mutation positive melanoma in the first-line setting. PAG noted that ipilimumab would provide an option and is seeking information on the use of ipilimumab instead of vemurafenib for BRAF mutation positive patients. However, vemuarfenib is currently only funded for first-line treatment and not funded for second-line treatment. For patients who have used vemurafenib in the first-line setting, ipilimumab is currently funded in the second line setting. PAG is also requesting for information around using vemurafenib after ipilimumab to guide treatment sequence should ipilimumab be used in patients with BRAF mutation positive patients in the first-line treatment over vemurafenib. 5.6 Other Factors None identified pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 26
31 6 SYSTEMATIC REVIEW 6.1 Objectives To evaluate the effect of ipilimumab as first line therapy on patient outcomes compared to standard therapies, placebo, or best supportive care in the treatment of patients with unresectable or metastatic melanoma (stage III or IV) (see Table 4 in Section for outcomes of interest and comparators). Note: Two supplemental questions relevant to the pcodr review and to the Provincial Advisory Group were identified while developing the review protocol and are outlined in Section 7. Comparison of the clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma The clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose used as first line therapy for patients with unresectable or metastatic melanoma 6.2 Methods Review Protocol and Study Selection Criteria The systematic review protocol was developed jointly by the Clinical Guidance Panel and the pcodr Methods Team. Studies were chosen for inclusion in the review based on the criteria in the table below. Outcomes considered most relevant to patients, based on input from patient advocacy groups are those in bold. Table 4. Selection Criteria Clinical Trial Design Patient Population Intervention Published or unpublished RCTs Patients with unresectable or metastatic melanoma Subgroups: Patients with or without brain metastases BRAF mutation status Ipilimumab as 1 st line therapy, alone or in combination with chemotherapy Appropriate Comparators* BRAF inhibitor (e.g. vemurafenib, dabrafenib) MEK inhibitor (e.g. trametinib, alone or combined with dabrafenib) Immunotherapy (e.g. interleukin-2) Chemotherapy (e.g. dacarbazine, paclitaxel) Best supportive care Outcomes OS PFS HRQOL Response rate (CR, PR) % of patients required ipilimumab re-induction AE SAE WDAE Immunerelated SAE Placebo AE=adverse events; CR=complete response; HRQOL=health-related quality of life; OS=overall survival; PFS=progression-free survival; PR=partial response; RCT=randomized controlled trial; SAE=serious adverse event; WDAE=withdrawals due to adverse event * Standard and/or relevant therapies available in Canada (may include drug and non-drug interventions) 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 27
32 6.2.2 Literature Search Methods The literature search was performed by the pcodr Methods Team using the search strategy provided in Appendix A. Published literature was identified by searching the following bibliographic databases: MEDLINE (1946- ) with in-process records & daily updates via Ovid; Embase (1974- ) via Ovid; The Cochrane Central Register of Controlled Trials (July 2014) via Ovid; and PubMed. The search strategy was comprised of both controlled vocabulary, such as the National Library of Medicine s MeSH (Medical Subject Headings), and keywords. The main search concepts were ipilimumab and Yervoy. Methodological filters were applied to limit retrieval to randomized controlled trials or controlled clinical trials. Where possible, retrieval was limited to the human population. The search was also limited to English language documents, but not limited by publication year. The search is considered up to date as of November 5, Grey literature (literature that is not commercially published) was identified by searching the websites of regulatory agencies (Food and Drug Administration and European Medicines Agency), clinical trial registries (U.S. National Institutes of Health clinicaltrials.gov and Canadian Partnership Against Cancer Canadian Cancer Trials) and relevant conference abstracts. Searches of conference abstracts of the American Society of Clinical Oncology (ASCO) were limited to the last five years. Searches were supplemented by reviewing the bibliographies of key papers and through contacts with the Clinical Guidance Panel. In addition, the manufacturer of the drug was contacted for additional information as required by the pcodr Review Team Study Selection One member of the pcodr Methods Team selected studies for inclusion in the review according to the predetermined protocol. All articles considered potentially relevant were acquired from library sources. Two members of the pcodr Methods Team independently made the final selection of studies to be included in the review and differences were resolved through discussion. Included and excluded studies (with reasons for exclusion) are identified in section Quality Assessment Data Analysis Assessment of study bias was performed by one member of the pcodr Methods Team with input provided by the Clinical Guidance Panel and other members of the pcodr Review Team. SIGN-50 Checklists were applied as a minimum standard. Additional limitations and sources of bias were identified by the pcodr Review Team. No additional data analyses were conducted as part of the pcodr review Writing of the Review Report This report was written by the Methods Team, the Clinical Guidance Panel and the pcodr Secretariat: The Methods Team wrote a systematic review of the evidence and summaries of evidence for supplemental questions pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 28
33 The pcodr Clinical Guidance Panel wrote a summary of background clinical information and the interpretation of the systematic review. The Panel provided guidance and developed conclusions on the net overall clinical benefit of the drug. The pcodr Secretariat wrote summaries of the input provided by patient advocacy groups and by the Provincial Advisory Group (PAG) pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 29
34
35 6.3.2 Summary of Included Studies One double-blind RCT (Study CA ) was identified that met the eligibility criteria. The study compared ipilimumab plus dacarbazine versus placebo plus dacarbazine in patients with previously untreated unresectable or metastatic melanoma Detailed Trial Characteristics a) Trials One double-blind randomized controlled trial (CA ) was included in this review (Table 1). 3 The study was conducted in different countries in North America (including Canada) and Europe. It was sponsored by the manufacturer, and the manufacturer was involved in the study design, data collection, data analysis and report writing. A total of 502 patients were randomized in a 1:1 ratio to ipilimumab plus dacarbazine or placebo plus dacarbazine. Randomization was stratified by baseline metastasis stage (M0, M1a, M1b or M1c), study site and ECOG performance status. A centralized randomization scheme was used to assign patients to one of the two treatment groups. The sponsor, patients, investigator and site staff were blinded with respect to the patient s treatment assignment (ipilimumab or placebo). Local pharmacists and the CRO pharmacy monitors were unblinded. An Independent Data Monitoring Committee had the possibility to access unblinded data in order to enable review of emerging safety data. The dacarbazine dose was open-label. 62 The original primary outcome was progression-free survival (PFS). Because the emerging data from other ipilimumab trials suggested that conventional definitions of disease progression and response incompletely reflect overall survival among patients who appear to have a long-term benefit, the primary outcome was changed to overall survival (OS, defined as the time from randomization until death from any cause), and this was approved by the FDA in October A total of 500 patients were required in the initial study design, and there was no change in the size of the study population. In the protocol of this study, the authors estimated that 416 deaths among a total of 500 patients (250 patients in each treatment arm) would have 90% power to detect a 38% improvement in median OS to 11 months with ipilimumab plus dacarbazine versus 8 months with placebo plus dacarbazine, with a corresponding hazard ratio (HR) for death of at a two-sided alpha of The secondary outcomes included PFS, the rate of best overall response, the rate of disease control (defined as a complete response, a partial response or stable disease), time to response, the duration of the response, HRQOL and safety, in particular, immune-mediated adverse events. The efficacy outcomes in CA were assessed by local investigators as well as an Independent Review Committee (IRC), whose members were not aware of the treatment assignments. Because the primary outcome was overall survival, the IRC assessments are considered to be consistent with the investigator assessment. The IRC-reviewed outcomes are presented in this report. Intention-to-treat (ITT) approach was adopted in analyses of baseline characteristics and efficacy endpoints. All randomized patients were taken into account. The safety population was defined as all treated patients who received at least one dose of ipilimumab or placebo and/or dacarbazine. 25 A log-rank test was performed for the analysis of OS. A stratified Cox proportional-hazards model was 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 31
36 used to calculate hazard ratios for OS and PFS. The Kaplan-Meier method was used to analyze the survival outcomes between the two treatment groups. b) Populations The baseline demographic and disease characteristics were balanced between the two treatment arms. The mean age (range) was 57.5 years in the ipilimumab plus dacarbazine group and 56.4 years in the placebo plus dacarbazine group. There were more males (approximately 60%) in the trial than females (40%). More patients had an ECOG performance status of 0 (approximately 71%) than 1 (29%). Patients who received any prior treatment for metastatic disease or concomitant therapy with immunosuppressive agents (including long-term corticosteroids), or those with brain metastasis, primary ocular or mucosal melanoma or autoimmune disease were excluded from the study. In both treatment groups, 26% of patients received prior adjuvant therapy. c) Interventions This phase III study evaluated the efficacy and safety of ipilimumab combined with dacarbazine versus placebo plus dacarbazine. Ipilimumab was administered at 10 mg/kg/dose via a 90-minute intravenous infusion, while dacarbazine was administered at a dose of 850 mg/m 2. The study consisted of two phases: 1) Induction phase: patients were randomly assigned to treatment with ipilimumab plus dacarbazine or placebo plus dacarbazine at weeks 1, 4, 7 and 10, followed by dacarbazine alone every 3 weeks through week 22; treatment in this phase would be terminated if toxic effects associated with the drug or progressive disease was noted. 2) Maintenance phase: starting at week 24, patients with stable disease or an objective response during the induction phase who did not have a dose-limiting adverse event received placebo or ipilimumab every 12 weeks until disease progression, unacceptable toxic effects, withdrawal of consent, or the end of the study. 3 A total of 92 patients (36.8%) in the ipilimumab + dacarbazine group and 165 (65.5%) in the dacarbazine + placebo group received all four doses of ipilimumab or placebo. d) Patient Disposition A total of 502 patients started on the study and 95.8% of the participants discontinued the study prematurely. Higher risks of disease progression were observed in the placebo plus dacarbazine group, while more study drug-related adverse events were reported in the ipilimumab plus dacarbazine group. The follow-up time between the start of the study (the first visit of the first enrolled patient) and the end of the study (the last visit of the last enrolled patient) was 54 months, and the follow-up time between the time the last patient underwent randomization and the end of the study was 36.6 months. Details of patient disposition are presented in Table pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 32

37
38 performance status of 0 and 1 were included limiting the generalizability of the study findings. CA was sponsored by the manufacturer, and the manufacturer was involved in study design, data collection, data analysis and report writing Detailed Outcome Data and Summary of Outcomes Efficacy Outcomes Overall survival The primary endpoint of Study CA was OS between ipilimumab plus dacarbazine and placebo plus dacarbazine. It was defined as the time from randomization to death from any cause and was analyzed using the ITT population. The median OS was statistically significantly longer in patients treated with ipilimumab plus dacarbazine (11.2 months [95% CI: 9.4, 13.6]) compared with those treated with placebo plus dacarbazine (9.1 months [95% CI: 7.8, 10.5]) (Figure 2). The survival curves were similar through the first three months of treatment, after which the ipilimumab curve separated from the placebo curve, and the separation was sustained over time. The hazard ratio (HR) for the between-group comparison of OS was 0.72 (95% CI 0.59 to 0.87, p < 0.001), indicating a 28% risk reduction in OS for ipilimumab plus dacarbazine compared with placebo plus dacarbazine. Subgroup analyses of OS were conducted. A trend in improved OS was observed for the ipilimumab plus dacarbazine group compared with the placebo plus dacarbazine group across various patient subgroups; however, statistical significance was not always achieved (Figure 3). Figure 2. Kaplan-Meier survival curves in CA (data source: Robert ) 2014 pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 34
39
40 Progression-free survival This was a secondary endpoint in the current study. The analysis of PFS was conducted on a database that was locked after 416 events had been documented (March 2011). The survival curves were similar through the first three months of treatment, after which the ipilimumab curve separated from the placebo curve. A statistically significant difference in median PFS was reported in favour of ipilimumab plus dacarbazine (2.76 months [2.63, 3.29]) compared to placebo plus dacarbazine (2.60 months [2.56, 2.66]), although the results were numerically similar between the two groups. The HR for disease progression or death in the ipilimumab plus dacarbazine group as compared with the dacarbazine monotherapy group was 0.76 (95% CI , p = 0.006), indicating a 24% reduction in the risk of progression or death in the former (Table 2). Health-related quality of life In Study CA , patient s HRQOL was examined using the Global Health Status (GHS) scale and the symptom scales of the EORTC-QLQ-C30. The raw scale scores are transformed to scores ranging from 0 to 100. A higher GHS score indicates a better health status, while a higher symptom score indicates more severe symptoms. 66 An MCID for this instrument has not been established yet. The scores were assessed at baseline, week 4, 7, 12 and then every 12 weeks until disease progression. Changes in scores were categorized as no change (0 to 5), a little (5 to 10 points), moderate (10 to 20 points) and very much (> 20). The results of HRQOL assessment were reported in an abstract only. 4 At the end of the double-blind period of this study (week 12), unadjusted mean changes from baseline in both groups were no change to moderate for all HRQOL domains in this scale including symptom scores. Patients in both groups reported declined average GHS scores (ipilimumab + dacarbazine: -6.5; placebo + dacarbazine: ), indicating worsened health status. The 95% CIs or p-value was not reported for this comparison. The authors concluded that during the first 12 weeks of treatment, most scales and symptom scores were similar to baseline. No further details regarding the HRQOL assessment were provided in this abstract. Response rate The rate of best overall response was defined as the proportion of all randomly assigned patients who had a complete (CR) or partial response (PR). This was a secondary endpoint in CA Patients in the ipilimumab plus dacarbazine group were more likely to respond to the treatment compared with the placebo plus dacarbazine group. CR or PR were achieved in 38 patients (15.2%) and 26 patients (10.3%) in the respective groups. However, the between-group difference in the best overall response rate was not statistically significant, p > 0.05 (Table 2). Proportion of patients requiring ipilimumab re-induction Re-induction with ipilimumab following Maintenance was not permitted within Study CA pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 36
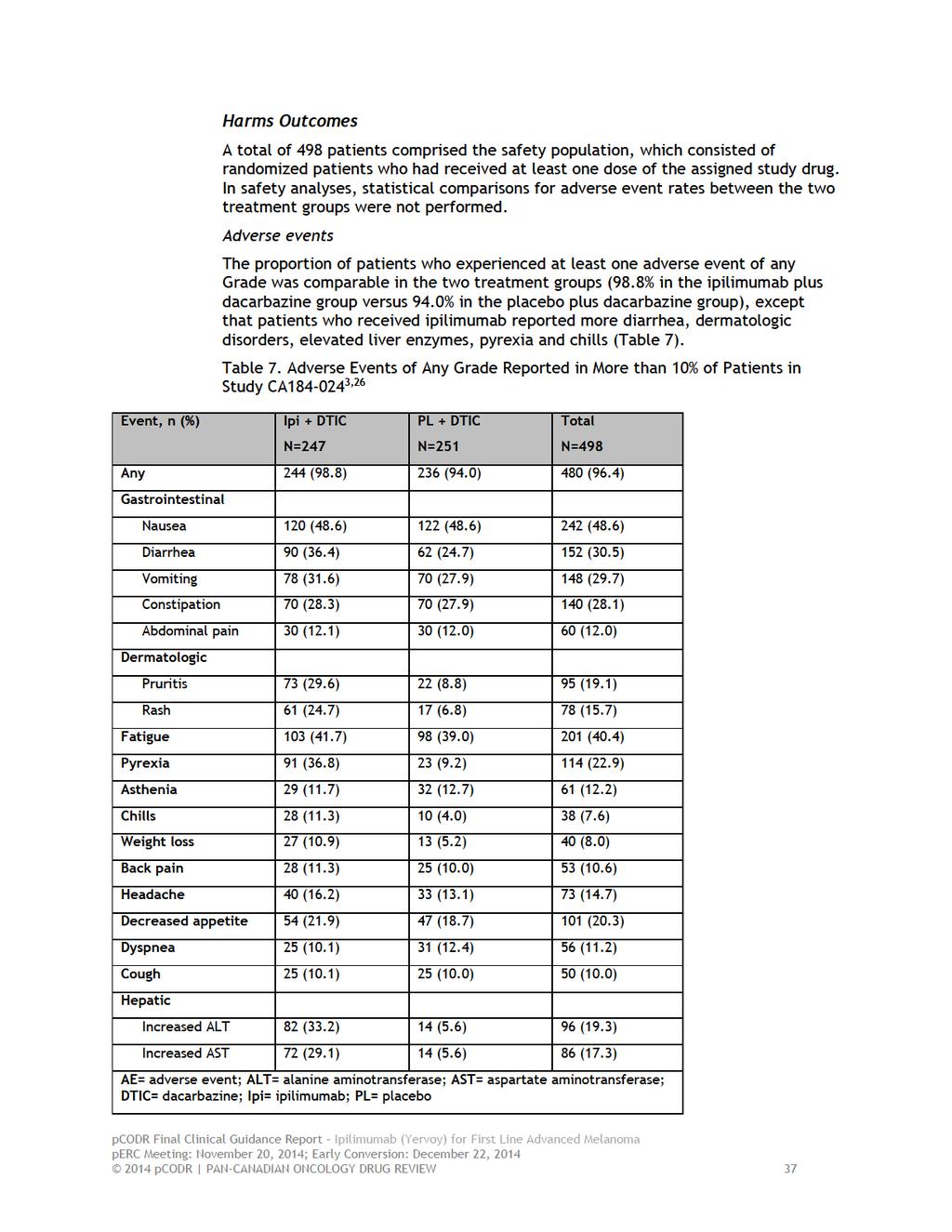
41
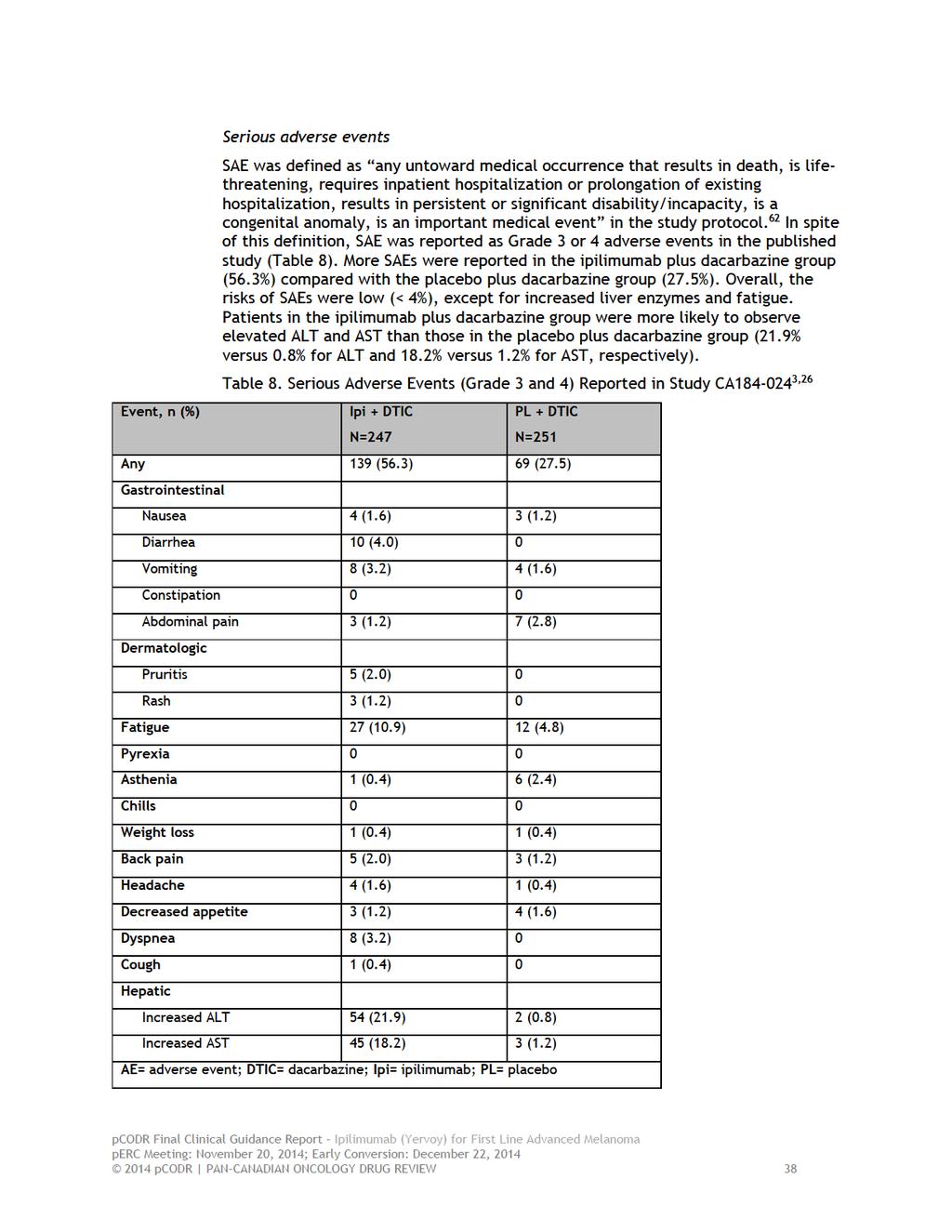
42
43 Withdrawal due to adverse events Of a total of 498 patients in the safety population, 95 of 247 patients (38.5%) with ipilimumab plus dacarbazine withdrew from the study due to adverse events compared to 20 of 251 patients (8.0%) with placebo plus dacarbazine. The common adverse events leading to early study discontinuation were not reported in the published article. During the induction phase, there were 85 patients and 10 patients who discontinued the study in the two groups, respectively, due to an adverse event. 3 According to the additional information provided by the submitter in the checkpoint meeting, in the ipilimumab plus dacarbacine group, the most common adverse events leading to discontinuation was elevated AST/ALT followed by gastrointestinal disorders and hepatobiliary disorders; in the placebo plus dacarbazine group, the most common adverse event leading to discontinuation was neutropenia. 67 Immune-related serious adverse events Table 9 presents data on the immune-related adverse events reported in Study CA Grade 3 or 4 immune-related adverse events occurred in a higher proportion of patients in the ipilimumab plus dacarbazine group (41.7% of 247 patients) as compared to the placebo plus dacarbazine group (6.0% of 251 patients). The most common immune-related adverse events included dermatologic disorders, diarrhea and elevated ALT/AST pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 39
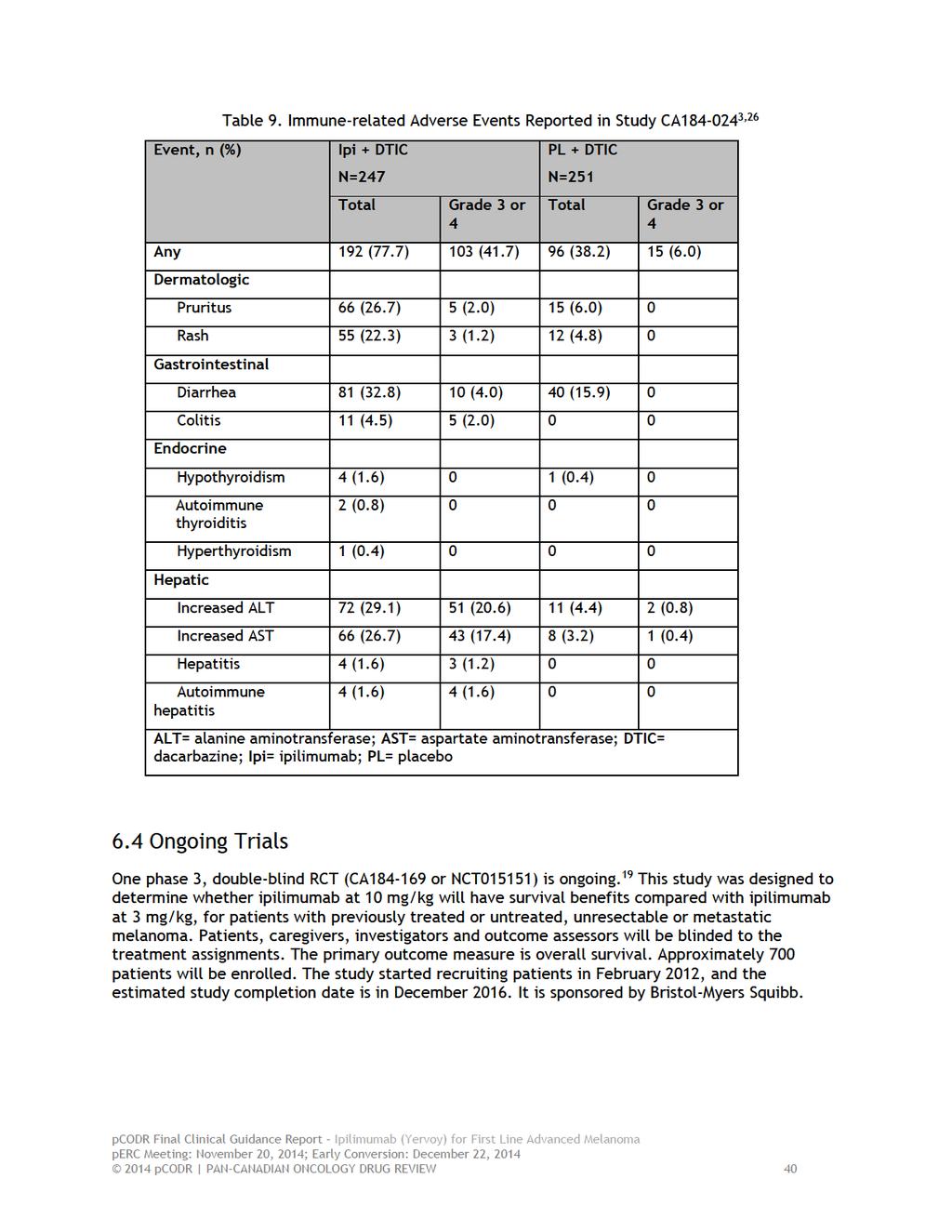
44
45 7 SUPPLEMENTAL QUESTIONS The following supplemental questions were identified during development of the review protocol as relevant to the pcodr review of ipilimumab in patients with unresectable stage III or IV melanoma who had no previous systemic therapy: Comparison of the clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma The clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose used as first line therapy for patients with unresectable or metastatic melanoma Topics considered in this section are provided as supporting information. The information has not been systematically reviewed. 7.1 Comparison of the clinical effectiveness and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma Objective The objective is to report on the efficacy and harms of ipilimumab at 3 mg/kg dose when compared with ipilimumab at 10 mg/kg in first line therapy for patients with unresectable or metastatic melanoma Findings A literature search was conducted to identify RCTs and non RCTs that compared ipilimumab 3mg/kg dose with 10mg/kg dose in the first-line therapy of unresectable stage III or IV melanoma. The Methods Team identified one study which was randomized, double-blind, phase II biomarker study. Patients included were pretreated or treatment-naïve with unresectable stage III/IV melanoma and were randomized to receive either 3 or 10 mg/kg ipilimumab every 3 weeks for 4 doses, Study CA Only twenty patients who were treatment naïve were included in this study, however it is not reported how many of those received 3 mg/kg or 10 mg/kg. Also results were not reported for the treatment naïve patient group. Finally, chemotherapy naïve patients who were included in Study CA were also included in the pooled analyses summarized in the supplemental issue below Summary No evidence was found in the literature on the comparative efficacy and safety of ipilimumab at 3 mg/kg/dose versus 10 mg/kg/dose as first line therapy for patients with unresectable or metastatic melanoma pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 41
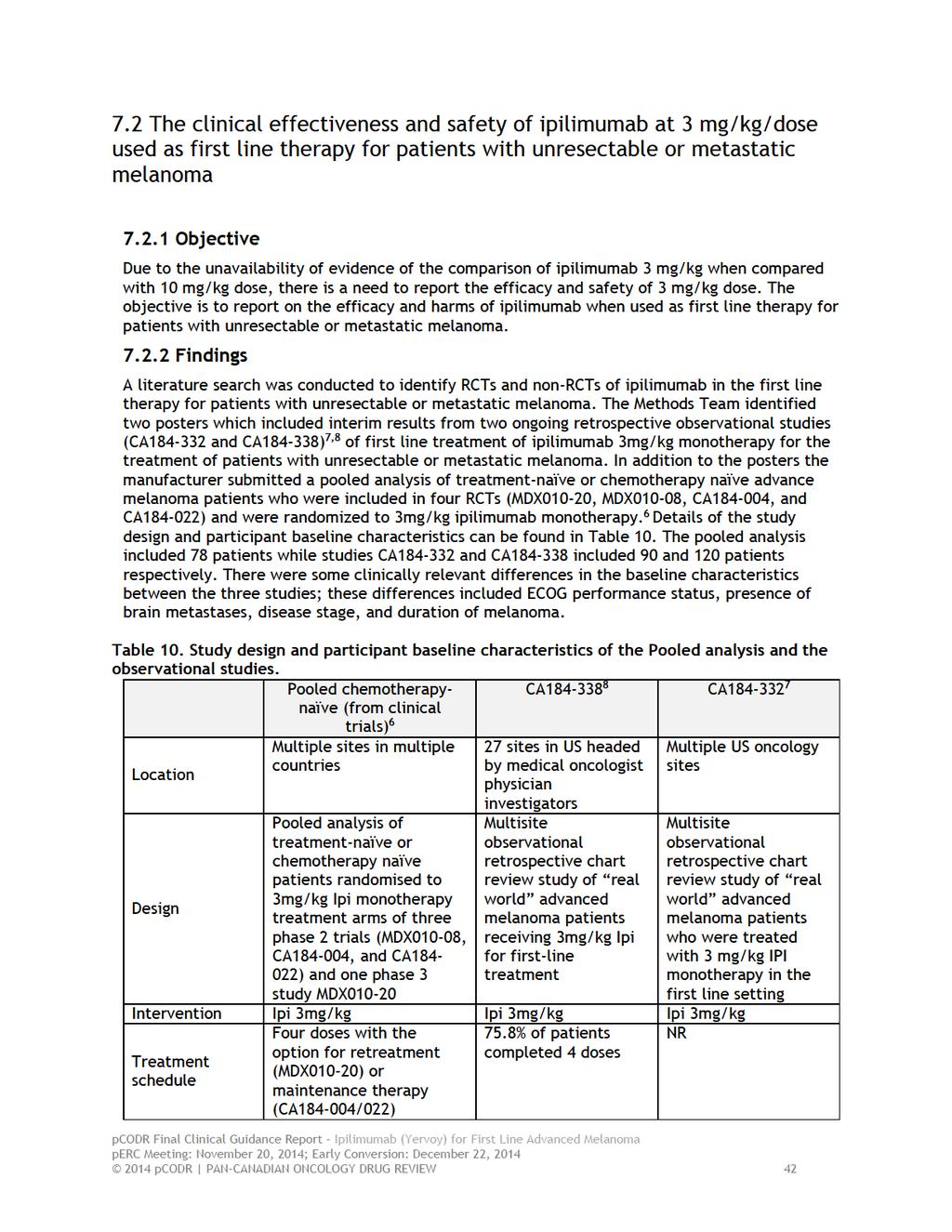
46
47
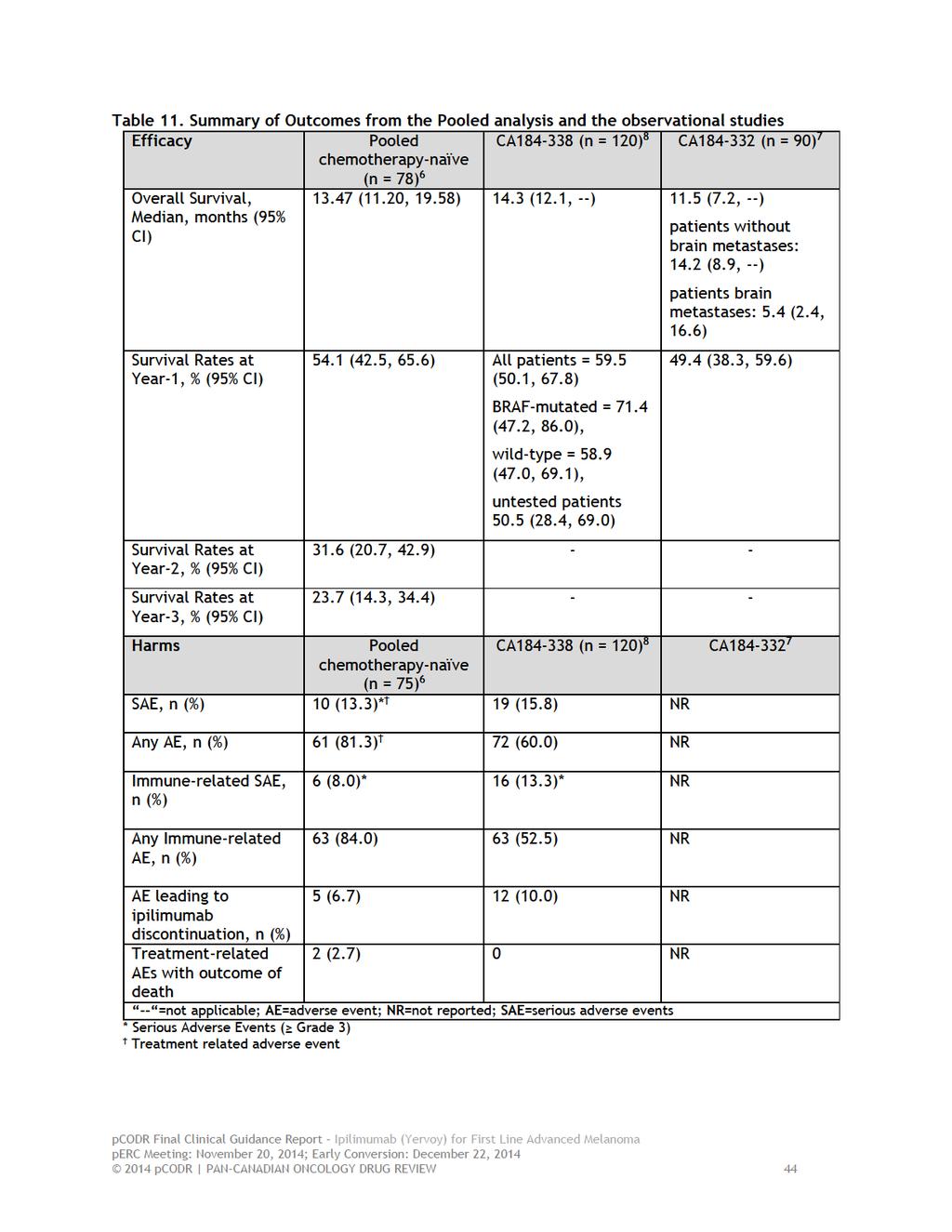
48
49 Efficacy Outcomes Overall Survival In all 3 studies Kaplan-Meier estimates were used to analyze overall survival. Median overall survival was months in the pooled analysis, while it was 11.5 and 14.3 in studies CA and CA respectively. One year survival rate was 54.1%, 49.4% and 59.5% in the pooled analysis, study CA , and study CA , respectively (Table 11) In study CA there were no differences in survival function among BRAF-mutated, wildtype, and untested groups of patients. Harms Outcomes Only the pooled analysis and study CA reported harms outcomes. Major harms outcomes are summarized in Immune-related adverse events of any grade occurred in 84% and 52.5% of patients included in the pooled analysis and study CA , respectively, with Grade 3 or higher immune-related adverse events occurring in 8.0% and 13.3% of patients in the pooled analysis and study CA , respectively. Immune-related adverse events that occurred in the pooled analysis included gastrointestinal and skin, while those occurred in study CA included gastrointestinal, skin (cutaneous), and liver. Grade 3 or higher immune-related adverse events that occurred in the pooled analysis were gastrointestinal and skin, while those occurred in study CA were gastrointestinal, skin, liver, and Endocrine. Limitations Studies included in the pooled analysis had different design and different objectives (one was dose ranging, one was biomarker study, one was phase II and one phase III), these differences in study design would make heterogeneity arise. Overall survival was the primary outcome in only one of the studies (MDX010-20) of which only 13 patients were included in the pooled analysis. In the methods section it was mentioned that only patients who had received ipilimumab alone were included in the analysis; at the checkpoint meeting with the manufacturer it was indicated that 40 patients from study MDX were included in the pooled analysis, however Hersh et al. 69 indicated that out of the 40 patients randomized to receive 3 mg/kg ipilimumab only 37 patients received ipilimumab monotherapy treatment. These differences in numbers between what is used and what should have been used make the reviewer suspect the quality of the pooled analysis overall and how it was undertaken especially as it is not possible to validate what was done. Patients were included in the analysis if they met certain inclusion criteria, and out of 1,051 patients included in these studies only 78 (7.4%) were included in the pooled analysis. This method of selecting patients for inclusion would introduce bias due to breaking randomization and being selective, also this method is similar to pooling results from case reports which is unreliable. The follow-up period in the pooled analysis ranged from 0.03 to 69.7 months indicating huge variation in the length of follow-up between the studies included in the pooled analysis. Given the limitations mentioned above, there is high risk of bias associated with the pooled analysis. Finally of the 78 chemotherapy naïve patients included in the pooled analysis, 41 received prior immunotherapy treatment, hence ipilimumab would be considered as first line treatment for only 37 patients. There are many limitations related to the analysis of the 37 patients who received ipilimumab as first line treatment, due to the small sample. Given all of the limitations in the pooled analysis mentioned above, conclusions from the pooled analysis should be drawn with extreme caution pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 45
50 Studies CA and CA were generally adequate; however there is high risk of bias associated with their study design. Potential loss to follow-up, missing data, potential for selection bias, and underreported or incomplete data collection based upon available data in patient medical charts are limitations in retrospective observational studies. Also it was unclear whether the same patients were included in the two studies, because both of them enrolled patients treated in the US between April 2011 and September The dosing schedule of ipilimumab was not reported. None of them reported if prior immunotherapy was used. In the methods sections of both observational studies, it was mentioned that patients for whom at least 12 months have elapsed since initiation of 3 mg/kg ipilimumab were included in the interim analysis, however the range of follow-up was 2.8 to 14.4 month in study CA and 0.5 to 21.7 month in study CA which means patients with less than 12 months since the initiation of treatment were included in the analysis, which contradicts what was mentioned in the methods section. This would lead us to suspect the accuracy of the presented results Summary A pooled analysis of treatment-naïve or chemotherapy-naïve advanced melanoma patients who were included in four RCTs (MDX010-20, MDX010-08, CA , and CA ) and two ongoing retrospective observational studies (CA , and CA ) investigated the use of 3mg/kg ipilimumab monotherapy in patients with unresectable or metastatic melanoma. The pooled analysis included 78 patients while studies CA and CA included 90 and 120 patients respectively. There were some clinically relevant differences in the baseline characteristics (such as ECOG performance status, presence of brain metastases, disease stage and duration of melanoma) between the three studies. Median overall survival was months in the pooled analysis, while it was 11.5 and 14.3 in studies CA and CA respectively. The one year survival rate was 54.1%, 49.4%, and 59.5% in the pooled analysis, study CA , and study CA , respectively. The two and three year survival rates in the pooled analysis were 31.6% and 23.7%, respectively. The adverse events were reported only in the pooled analysis and study CA Immune-related adverse events of any grade occurred in 84% and 52.5% of patients included in the pooled analysis and study CA , respectively, with Grade 3 or higher immune-related adverse events occurred 8.0% and 13.3% of patients in the pooled analysis and study CA , respectively. Results reported in the pooled analysis might be unreliable due to the many limitations in that analysis. In addition, results from the two observational studies should be interpreted with caution due to the high risk of bias associated with their design pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 46
51 8 ABOUT THIS DOCUMENT This Final Clinical Guidance Report was prepared by the pcodr Melanoma Clinical Guidance Panel and supported by the pcodr Methods Team. This document is intended to advise the pcodr Expert Review Committee (perc) regarding the clinical evidence available on ipilimumab (Yervoy) as first line therapy for advanced melanoma. Issues regarding resource implications are beyond the scope of this report and are addressed by the relevant pcodr Economic Guidance Report. Details of the pcodr review process can be found on the pcodr website ( pcodr considers it essential that perc recommendations be based on information that can be publicly disclosed. Information included in the Clinical Guidance Report was handled in accordance with the pcodr Disclosure of Information Guidelines. There was no non-disclosable information in the Clinical Guidance Report provided to perc for their deliberations. This Final Clinical Guidance Report is publicly posted at the same time that a perc Final Recommendation is issued. The Final Clinical Guidance Report supersedes the Initial Clinical Guidance Report. Note that no revision was made in between posting of the Initial and Final Clinical Guidance Reports. The pcodr Melanoma Clinical Guidance Panel is comprised of three clinical oncologists. The panel members were selected by the pcodr secretariat, as outlined in the pcodr Nomination/Application Information Package, which is available on the pcodr website ( Final selection of the Clinical Guidance Panels was made by the perc Chair in consultation with the pcodr Executive Director. The Panel and the pcodr Methods Team are editorially independent of the provincial and territorial Ministries of Health and the provincial cancer agencies pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 47

52
pan-canadian Oncology Drug Review Final Clinical Guidance Report Trametinib (Mekinist) for Metastatic Melanoma October 22, 2013
 for Metastatic Melanoma October 22, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Trametinib (Mekinist) for Metastatic Melanoma October 22, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Trametinib (Mekinist) for Metastatic Melanoma October 22, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Vemurafenib (Zelboraf) for Advanced Melanoma October 1, 2012
 for Advanced Melanoma October 1, 2012") pan-canadian Oncology Drug Review Final Clinical Guidance Report Vemurafenib (Zelboraf) for Advanced Melanoma October 1, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Vemurafenib (Zelboraf) for Advanced Melanoma October 1, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
 for patients with ECOG PS 0-1 as indicated in the CheckMate-067 trial. Upon reconsideration of the Initial Recommendation, perc noted PAG s feedback requesting guidance on extrapolating eligibility to
for patients with ECOG PS 0-1 as indicated in the CheckMate-067 trial. Upon reconsideration of the Initial Recommendation, perc noted PAG s feedback requesting guidance on extrapolating eligibility to
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 large impact on cost-effectiveness. perc discussed that one of the main factors affecting the costeffectiveness estimates was the survival estimates used in the economic model. In reviewing the clinical
large impact on cost-effectiveness. perc discussed that one of the main factors affecting the costeffectiveness estimates was the survival estimates used in the economic model. In reviewing the clinical
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 brentuximab. Given that the median survival of Hodgkin lymphoma patients who relapse after ASCT is approximately two years, perc considered that the manufacturer had substantially overestimated the incremental
brentuximab. Given that the median survival of Hodgkin lymphoma patients who relapse after ASCT is approximately two years, perc considered that the manufacturer had substantially overestimated the incremental
pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION
 INITIAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION The CADTH pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial M inistries of Health (with the exception
pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION The CADTH pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial M inistries of Health (with the exception
OVERALL CLINICAL BENEFIT
 pcodr systematic review but were excluded from the review because they were retrospective case series. perc confirmed that the inclusion and exclusion criteria of the systematic review were appropriate
pcodr systematic review but were excluded from the review because they were retrospective case series. perc confirmed that the inclusion and exclusion criteria of the systematic review were appropriate
OVERALL CLINICAL BENEFIT
 cetuximab plus FOLFIRI to convert unresectable liver metastatses to resectable, perc confirmed that neither the FIRE-3 study nor the CRYSTAL study were designed to assess resectability and, in the absence
cetuximab plus FOLFIRI to convert unresectable liver metastatses to resectable, perc confirmed that neither the FIRE-3 study nor the CRYSTAL study were designed to assess resectability and, in the absence
The pcodr review also provided contextual information on ALK mutation testing.
 only approximately 4% of NSCLC patients are expected to have the ALK mutation. perc further discussed these estimates in the context of the feasibility of implementing a funding recommendation for crizotinib.
only approximately 4% of NSCLC patients are expected to have the ALK mutation. perc further discussed these estimates in the context of the feasibility of implementing a funding recommendation for crizotinib.
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 ipilimumab aligned with patient values. Although few patients had direct experience using this combination agent, patients indicated that side effects associated with nivolumab plus ipilimumab were few
ipilimumab aligned with patient values. Although few patients had direct experience using this combination agent, patients indicated that side effects associated with nivolumab plus ipilimumab were few
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 perc discussed the feasibility of adoption of intralesional therapy with aldesleukin and noted that aldesleukin had been in use in this way for this patient population for a number of years as it was previously
perc discussed the feasibility of adoption of intralesional therapy with aldesleukin and noted that aldesleukin had been in use in this way for this patient population for a number of years as it was previously
pan-canadian Oncology Drug Review Final Economic Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer July 16, 2015
 Neoadjuvant Breast Cancer July 16, 2015") pan-canadian Oncology Drug Review Final Economic Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer July 16, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer July 16, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 into consideration the concerns of the patient. Upon reconsideration of the perc Initial Recommendation,the Committee discussed feedback from the patient advocacy group reporting concerns that the definition
into consideration the concerns of the patient. Upon reconsideration of the perc Initial Recommendation,the Committee discussed feedback from the patient advocacy group reporting concerns that the definition
pan-canadian Oncology Drug Review Initial Economic Guidance Report Osimertinib (Tagrisso) for Advanced or Metastatic Non-Small Cell Lung Cancer
 for Advanced or Metastatic Non-Small Cell Lung Cancer") pan-canadian Oncology Drug Review Initial Economic Guidance Report Osimertinib (Tagrisso) for Advanced or Metastatic Non-Small Cell Lung Cancer November 1, 2018 DISCLAIMER Not a Substitute for Professional
pan-canadian Oncology Drug Review Initial Economic Guidance Report Osimertinib (Tagrisso) for Advanced or Metastatic Non-Small Cell Lung Cancer November 1, 2018 DISCLAIMER Not a Substitute for Professional
risks. Therefore, perc agreed that the reimbursement criteria should match the eligibility criteria of the SELECT trial.
 risks. Therefore, perc agreed that the reimbursement criteria should match the eligibility criteria of the SELECT trial. perc considered input from one patient advocacy group indicating that patients value
risks. Therefore, perc agreed that the reimbursement criteria should match the eligibility criteria of the SELECT trial. perc considered input from one patient advocacy group indicating that patients value
Initial Recommendation for Ibrutinib (Imbruvica) for Mantle Cell Lymphoma perc Meeting: June 16, pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 4
 for Mantle Cell Lymphoma perc Meeting: June 16, pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 4") although ibrutinib was associated with significant improvements in PFS and QoL, adverse events such as fatigue and bleeding were still observed in patients who received ibrutinib. perc concluded that overall,
although ibrutinib was associated with significant improvements in PFS and QoL, adverse events such as fatigue and bleeding were still observed in patients who received ibrutinib. perc concluded that overall,
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 well structured and organized, provided perc with a much deeper understanding of patients experiences with relapse or refractory CLL/SLL and its treatment. perc deliberated upon the cost effectiveness
well structured and organized, provided perc with a much deeper understanding of patients experiences with relapse or refractory CLL/SLL and its treatment. perc deliberated upon the cost effectiveness
CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab.
 CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab. perc noted that patients with brain metastases were excluded from the CheckMate
CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab. perc noted that patients with brain metastases were excluded from the CheckMate
pan-canadian Oncology Drug Review Initial Economic Guidance Report Obinutuzumab (Gazyva) for Follicular Lymphoma August 30, 2018
 for Follicular Lymphoma August 30, 2018") pan-canadian Oncology Drug Review Initial Economic Guidance Report Obinutuzumab (Gazyva) for Follicular Lymphoma August 30, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Initial Economic Guidance Report Obinutuzumab (Gazyva) for Follicular Lymphoma August 30, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
 Clinician input indicated that avelumab in second-line treatment would be used following chemotherapy and should be strongly considered as first-line. However, perc noted that avelumab in the first-line
Clinician input indicated that avelumab in second-line treatment would be used following chemotherapy and should be strongly considered as first-line. However, perc noted that avelumab in the first-line
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 differ and that they each has a unique mechanism of action. As such perc considered that it would be important for clinicians and patients to be able to choose either drug as a first-line treatment option.
differ and that they each has a unique mechanism of action. As such perc considered that it would be important for clinicians and patients to be able to choose either drug as a first-line treatment option.
OVERALL CLINICAL BENEFIT
 noted that there are case reports of a rebound effect upon discontinuation of ruxolitinib (Tefferi 2012), although this was not observed in either the COMFORT I or COMFORT II studies. Therefore, perc considered
noted that there are case reports of a rebound effect upon discontinuation of ruxolitinib (Tefferi 2012), although this was not observed in either the COMFORT I or COMFORT II studies. Therefore, perc considered
pan-canadian Oncology Drug Review Final Economic Guidance Report Osimertinib (Tagrisso) for Non-Small Cell Lung Cancer January 4, 2019
 for Non-Small Cell Lung Cancer January 4, 2019") pan-canadian Oncology Drug Review Final Economic Guidance Report Osimertinib (Tagrisso) for Non-Small Cell Lung Cancer January 4, 2019 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Economic Guidance Report Osimertinib (Tagrisso) for Non-Small Cell Lung Cancer January 4, 2019 DISCLAIMER Not a Substitute for Professional Advice This report is
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 Overall, perc considered that everolimus aligned with patient values. Patient advocacy group input on everolimus indicated that patients with pnets value the outcome of progression-free survival as a measure
Overall, perc considered that everolimus aligned with patient values. Patient advocacy group input on everolimus indicated that patients with pnets value the outcome of progression-free survival as a measure
pan-canadian Oncology Drug Review Final Economic Guidance Report Venetoclax (Venclexta) for Chronic Lymphocytic Leukemia March 2, 2018
 for Chronic Lymphocytic Leukemia March 2, 2018") pan-canadian Oncology Drug Review Final Economic Guidance Report Venetoclax (Venclexta) for Chronic Lymphocytic Leukemia March 2, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Economic Guidance Report Venetoclax (Venclexta) for Chronic Lymphocytic Leukemia March 2, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 information aligned with the expected toxicity profile of panitumumab, which is well-known as panitumumab is already used as a third-line therapy for patients with mcrc. perc also noted QoL did not deteriorate
information aligned with the expected toxicity profile of panitumumab, which is well-known as panitumumab is already used as a third-line therapy for patients with mcrc. perc also noted QoL did not deteriorate
pan-canadian Oncology Drug Review Final Economic Guidance Report Crizotinib (Xalkori) Resubmission for Advanced Non-Small Cell Lung Cancer
 Resubmission for Advanced Non-Small Cell Lung Cancer") pan-canadian Oncology Drug Review Final Economic Guidance Report Crizotinib (Xalkori) Resubmission for Advanced Non-Small Cell Lung Cancer May 2, 2013 DISCLAIMER Not a Substitute for Professional Advice
pan-canadian Oncology Drug Review Final Economic Guidance Report Crizotinib (Xalkori) Resubmission for Advanced Non-Small Cell Lung Cancer May 2, 2013 DISCLAIMER Not a Substitute for Professional Advice
pan-canadian Oncology Drug Review Final Economic Guidance Report Palbociclib (Ibrance) for Advanced Breast Cancer Resubmission November 21, 2016
 for Advanced Breast Cancer Resubmission November 21, 2016") pan-canadian Oncology Drug Review Final Economic Guidance Report Palbociclib (Ibrance) for Advanced Breast Cancer Resubmission November 21, 2016 DISCLAIMER Not a Substitute for Professional Advice This
pan-canadian Oncology Drug Review Final Economic Guidance Report Palbociclib (Ibrance) for Advanced Breast Cancer Resubmission November 21, 2016 DISCLAIMER Not a Substitute for Professional Advice This
perc deliberated upon: a pcodr systematic review other literature in the Clinical Guidance Report providing clinical context
 require close monitoring. perc noted that induction therapy is generally administered in-hospital while consolidation therapy is administered on an out-patient basis. Because of the potential for serious
require close monitoring. perc noted that induction therapy is generally administered in-hospital while consolidation therapy is administered on an out-patient basis. Because of the potential for serious
that the best available evidence has not demonstrated that pcr can predict long-term outcomes in the neoadjuvant setting.
 pcr in one arm of a randomized clinical trial comparing two neoadjuvant chemotherapies predicts for improved event-free or overall survival in that arm of the clinical trial. perc noted that the NeoALTTO
pcr in one arm of a randomized clinical trial comparing two neoadjuvant chemotherapies predicts for improved event-free or overall survival in that arm of the clinical trial. perc noted that the NeoALTTO
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 perc deliberated upon the cost-effectiveness of lapatinib plus letrozole and discussed the challenges of using letrozole alone as a comparator and/or using trastuzumab plus anastrozole as a comparator.
perc deliberated upon the cost-effectiveness of lapatinib plus letrozole and discussed the challenges of using letrozole alone as a comparator and/or using trastuzumab plus anastrozole as a comparator.
pan-canadian Oncology Drug Review Initial Economic Guidance Report Palbociclib (Ibrance) for Advanced Breast Cancer May 5, 2016
 for Advanced Breast Cancer May 5, 2016") pan-canadian Oncology Drug Review Initial Economic Guidance Report Palbociclib (Ibrance) for Advanced Breast Cancer May 5, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Initial Economic Guidance Report Palbociclib (Ibrance) for Advanced Breast Cancer May 5, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Ibrutinib (Imbruvica) for Mantle Cell Lymphoma July 19, 2016
 for Mantle Cell Lymphoma July 19, 2016") pan-canadian Oncology Drug Review Final Economic Guidance Report Ibrutinib (Imbruvica) for Mantle Cell Lymphoma July 19, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Ibrutinib (Imbruvica) for Mantle Cell Lymphoma July 19, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013
 for metastatic Renal Cell Carcinoma March 7, 2013") pan-canadian Oncology Drug Review Final Economic Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Irinotecan liposome (Onivyde) for Metastatic Pancreatic Cancer January 5, 2018
 for Metastatic Pancreatic Cancer January 5, 2018") pan-canadian Oncology Drug Review Final Economic Guidance Report Irinotecan liposome (Onivyde) for Metastatic Pancreatic Cancer January 5, 2018 DISCLAIMER Not a Substitute for Professional Advice This
pan-canadian Oncology Drug Review Final Economic Guidance Report Irinotecan liposome (Onivyde) for Metastatic Pancreatic Cancer January 5, 2018 DISCLAIMER Not a Substitute for Professional Advice This
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer June 3, 2016
 for Non-Small Cell Lung Cancer June 3, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer June 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer June 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016
 for Metastatic Renal Cell Carcinoma September 1, 2016") pan-canadian Oncology Drug Review Final Economic Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Economic Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
Technology appraisal guidance Published: 23 July 2014 nice.org.uk/guidance/ta319
 Ipilimumab for previously untreated advanced (unresectable or metastatic) melanoma Technology appraisal guidance Published: 23 July 2014 nice.org.uk/guidance/ta319 NICE 2018. All rights reserved. Subject
Ipilimumab for previously untreated advanced (unresectable or metastatic) melanoma Technology appraisal guidance Published: 23 July 2014 nice.org.uk/guidance/ta319 NICE 2018. All rights reserved. Subject
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
untreated chronic lymphocytic leukemia (CLL), for whom fludarabine treatment is considered inappropriate.
, for whom fludarabine treatment is considered inappropriate.") perc deliberated on the potential cost-effectiveness of obinutuzumab plus chlorambucil in comparison with chlorambucil alone and determined that it was cost-effective. perc agreed with the Economic Guidance
perc deliberated on the potential cost-effectiveness of obinutuzumab plus chlorambucil in comparison with chlorambucil alone and determined that it was cost-effective. perc agreed with the Economic Guidance
pan-canadian Oncology Drug Review Initial Economic Guidance Report Fulvestrant (Faslodex) for Metastatic Breast Cancer November 30, 2017
 for Metastatic Breast Cancer November 30, 2017") pan-canadian Oncology Drug Review Initial Economic Guidance Report Fulvestrant (Faslodex) for Metastatic Breast Cancer November 30, 2017 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Initial Economic Guidance Report Fulvestrant (Faslodex) for Metastatic Breast Cancer November 30, 2017 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Economic Guidance Report Fulvestrant (Faslodex) for Metastatic Breast Cancer February 1, 2018
 for Metastatic Breast Cancer February 1, 2018") pan-canadian Oncology Drug Review Final Economic Guidance Report Fulvestrant (Faslodex) for Metastatic Breast Cancer February 1, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Economic Guidance Report Fulvestrant (Faslodex) for Metastatic Breast Cancer February 1, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013
 for Advanced Breast Cancer March 25, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Nivolumab (Opdivo) for Metastatic Melanoma April 1, 2016
 for Metastatic Melanoma April 1, 2016") pan-canadian Oncology Drug Review Final Economic Guidance Report Nivolumab (Opdivo) for Metastatic Melanoma April 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Economic Guidance Report Nivolumab (Opdivo) for Metastatic Melanoma April 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer April 1, 2016
 for Non-Small Cell Lung Cancer April 1, 2016") pan-canadian Oncology Drug Review Initial Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer April 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer April 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
one patient advocacy group (Myeloma Canada) the submitter (Cancer Care Ontario Hematology Disease Site Group) the manufacturer (Janssen Inc.
 the submitter (Cancer Care Ontario Hematology Disease Site Group) the manufacturer (Janssen Inc.") perc noted that the pcodr Economic Guidance Panel s estimates of the use of bortezomib in both pre- ASCT and post-asct settings when compared with standard induction therapy and observation-only maintenance
perc noted that the pcodr Economic Guidance Panel s estimates of the use of bortezomib in both pre- ASCT and post-asct settings when compared with standard induction therapy and observation-only maintenance
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION
 FINAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
midostaurin should be extended to patients who are deemed fit to receive intensive induction and consolidation, regardless of age.
 midostaurin should be extended to patients who are deemed fit to receive intensive induction and consolidation, regardless of age. perc deliberated on the toxicity profile of midostaurin and noted that
midostaurin should be extended to patients who are deemed fit to receive intensive induction and consolidation, regardless of age. perc deliberated on the toxicity profile of midostaurin and noted that
pan-canadian Oncology Drug Review Final Clinical Guidance Report Eribulin (Halaven) for Metastatic Breast Cancer August 2, 2012
 for Metastatic Breast Cancer August 2, 2012") pan-canadian Oncology Drug Review Final Clinical Guidance Report Eribulin (Halaven) for Metastatic Breast Cancer August 2, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Eribulin (Halaven) for Metastatic Breast Cancer August 2, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Enzalutamide (Xtandi) for Metastatic Castration-Resistant Prostate Cancer
 for Metastatic Castration-Resistant Prostate Cancer") pan-canadian Oncology Drug Review Final Economic Guidance Report Enzalutamide (Xtandi) for Metastatic Castration-Resistant Prostate Cancer July 23, 2013 DISCLAIMER Not a Substitute for Professional Advice
pan-canadian Oncology Drug Review Final Economic Guidance Report Enzalutamide (Xtandi) for Metastatic Castration-Resistant Prostate Cancer July 23, 2013 DISCLAIMER Not a Substitute for Professional Advice
 status should be eligible for treatment with atezolizumab. perc acknowledged the small number of patients with an EGFR or ALK mutation positive disease recruited on the trials but agreed that the overall
status should be eligible for treatment with atezolizumab. perc acknowledged the small number of patients with an EGFR or ALK mutation positive disease recruited on the trials but agreed that the overall
SUMMARY OF perc DELIBERATIONS ON REQUEST FOR ADVICE
 SUMMARY OF perc DELIBERATIONS ON REQUEST FOR ADVICE On March 7, 2013, perc issued a reimbursement recommendation for axitinib (Inlyta) for metastatic RCC. On April 18, 2017, the pcodr PAG submitted a Request
SUMMARY OF perc DELIBERATIONS ON REQUEST FOR ADVICE On March 7, 2013, perc issued a reimbursement recommendation for axitinib (Inlyta) for metastatic RCC. On April 18, 2017, the pcodr PAG submitted a Request
Initial Recommendation for Olaparib (Lynparza) for Ovarian Cancer perc Meeting: July 21, pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 4
 for Ovarian Cancer perc Meeting: July 21, pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 4") Overall, perc concluded that there may be a net clinical benefit with olaparib compared with placebo but the results are uncertain due to the limitations in the evidence from Study 19. perc discussed one
Overall, perc concluded that there may be a net clinical benefit with olaparib compared with placebo but the results are uncertain due to the limitations in the evidence from Study 19. perc discussed one
pan-canadian Oncology Drug Review Final Economic Guidance Report Olaparib (Lynparza) for Ovarian Cancer September 29, 2016
 for Ovarian Cancer September 29, 2016") pan-canadian Oncology Drug Review Final Economic Guidance Report Olaparib (Lynparza) for Ovarian Cancer September 29, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Economic Guidance Report Olaparib (Lynparza) for Ovarian Cancer September 29, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Economic Guidance Report Brentuximab Vedotin (Adcetris) for Hodgkin Lymphoma August 29, 2013
 for Hodgkin Lymphoma August 29, 2013") pan-canadian Oncology Drug Review Final Economic Guidance Report Brentuximab Vedotin (Adcetris) for Hodgkin Lymphoma August 29, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Brentuximab Vedotin (Adcetris) for Hodgkin Lymphoma August 29, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION
 FINAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
acceptance of PFS as a clinically meaningful endpoint and its agreement with the CGP that PFS is a likely surrogate of OS in MTC.
 acceptance of PFS as a clinically meaningful endpoint and its agreement with the CGP that PFS is a likely surrogate of OS in MTC. perc deliberated upon the cost-effectiveness of vandetanib and concluded
acceptance of PFS as a clinically meaningful endpoint and its agreement with the CGP that PFS is a likely surrogate of OS in MTC. perc deliberated upon the cost-effectiveness of vandetanib and concluded
 limitations of the indirect evidence submitted to pcodr, perc concluded that there is considerable uncertainty on how alectinib compares with ceritinib with regard to outcomes important to decision making
limitations of the indirect evidence submitted to pcodr, perc concluded that there is considerable uncertainty on how alectinib compares with ceritinib with regard to outcomes important to decision making
pan-canadian Oncology Drug Review Final Economic Guidance Report Vandetanib (Caprelsa) for Medullary Thyroid Cancer March 30, 2017
 for Medullary Thyroid Cancer March 30, 2017") pan-canadian Oncology Drug Review Final Economic Guidance Report Vandetanib (Caprelsa) for Medullary Thyroid Cancer March 30, 2017 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Vandetanib (Caprelsa) for Medullary Thyroid Cancer March 30, 2017 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION
 INITIAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception
pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception
pan-canadian Oncology Drug Review Final Clinical Guidance Report Regorafenib (Stivarga) for Metastatic Colorectal Cancer November 15, 2013
 for Metastatic Colorectal Cancer November 15, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Regorafenib (Stivarga) for Metastatic Colorectal Cancer November 15, 2013 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Regorafenib (Stivarga) for Metastatic Colorectal Cancer November 15, 2013 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Economic Guidance Report Ofatumumab (Arzerra) for Chronic Lymphocytic Leukemia January 29, 2015
 for Chronic Lymphocytic Leukemia January 29, 2015") pan-canadian Oncology Drug Review Final Economic Guidance Report Ofatumumab (Arzerra) for Chronic Lymphocytic Leukemia January 29, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Economic Guidance Report Ofatumumab (Arzerra) for Chronic Lymphocytic Leukemia January 29, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION
 FINAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic
 Dabrafenib for treating unresectable, advanced or metastatic") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
pan-canadian Oncology Drug Review Final Economic Guidance Report Pembrolizumab (Keytruda) for Metastatic Melanoma November 16, 2015
 for Metastatic Melanoma November 16, 2015") pan-canadian Oncology Drug Review Final Economic Guidance Report Pembrolizumab (Keytruda) for Metastatic Melanoma November 16, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Pembrolizumab (Keytruda) for Metastatic Melanoma November 16, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Lapatinib (Tykerb) with Letrozole for Metastatic Breast Cancer July 5, 2013
 with Letrozole for Metastatic Breast Cancer July 5, 2013") pan-canadian Oncology Drug Review Final Economic Guidance Report Lapatinib (Tykerb) with Letrozole for Metastatic Breast Cancer July 5, 2013 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Economic Guidance Report Lapatinib (Tykerb) with Letrozole for Metastatic Breast Cancer July 5, 2013 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Pomalidomide (Pomalyst) for Multiple Myeloma July 31, 2014
 for Multiple Myeloma July 31, 2014") pan-canadian Oncology Drug Review Final Clinical Guidance Report Pomalidomide (Pomalyst) for Multiple Myeloma July 31, 2014 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Pomalidomide (Pomalyst) for Multiple Myeloma July 31, 2014 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 metastases were similar to the overall trial results, leading perc to conclude that osimertinib should be made available to patients with stable CNS metastases. Furthermore, perc noted that patients with
metastases were similar to the overall trial results, leading perc to conclude that osimertinib should be made available to patients with stable CNS metastases. Furthermore, perc noted that patients with
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016
 for Metastatic Renal Cell Carcinoma September 1, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Name of Policy: Yervoy (Ipilimumab)
") Name of Policy: Yervoy (Ipilimumab) Policy #: 335 Latest Review Date: October 2013 Category: Pharmacology Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Yervoy (Ipilimumab) Policy #: 335 Latest Review Date: October 2013 Category: Pharmacology Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
pan-canadian Oncology Drug Review Final Economic Guidance Report Obinutuzumab (Gazyva) for Follicular Lymphoma November 1, 2018
 for Follicular Lymphoma November 1, 2018") pan-canadian Oncology Drug Review Final Economic Guidance Report Obinutuzumab (Gazyva) for Follicular Lymphoma November 1, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Economic Guidance Report Obinutuzumab (Gazyva) for Follicular Lymphoma November 1, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
National Horizon Scanning Centre. Ipilimumab (MDX-010) for unresectable stage III or IV metastatic melanoma - first or second line treatment
 for unresectable stage III or IV metastatic melanoma - first or second line treatment") Ipilimumab (MDX-010) for unresectable stage III or IV metastatic melanoma - first or second line treatment April 2008 This technology summary is based on information available at the time of research and
Ipilimumab (MDX-010) for unresectable stage III or IV metastatic melanoma - first or second line treatment April 2008 This technology summary is based on information available at the time of research and
pan-canadian Oncology Drug Review Final Clinical Guidance Report Dabrafenib (Tafinlar) and Trametinib (Mekinist) for Non-Small Cell Lung Cancer
 and Trametinib (Mekinist) for Non-Small Cell Lung Cancer") pan-canadian Oncology Drug Review Final Clinical Guidance Report Dabrafenib (Tafinlar) and Trametinib (Mekinist) for Non-Small Cell Lung Cancer November 2, 2017 DISCLAIMER Not a Substitute for Professional
pan-canadian Oncology Drug Review Final Clinical Guidance Report Dabrafenib (Tafinlar) and Trametinib (Mekinist) for Non-Small Cell Lung Cancer November 2, 2017 DISCLAIMER Not a Substitute for Professional
pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION
 INITIAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception
pcodr EXPERT REVIEW COMMITTEE (perc) INITIAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 to be meaningful. Considering the impact of cough on patients QoL, perc noted that improvement in cough within the FLAURA trial was meaningful to patients. perc, however, noted that fatigue was the most
to be meaningful. Considering the impact of cough on patients QoL, perc noted that improvement in cough within the FLAURA trial was meaningful to patients. perc, however, noted that fatigue was the most
pan-canadian Oncology Drug Review Final Clinical Guidance Report Brentuximab Vedotin (Adcetris) for Hodgkin Lymphoma August 29, 2013
 for Hodgkin Lymphoma August 29, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Brentuximab Vedotin (Adcetris) for Hodgkin Lymphoma August 29, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Brentuximab Vedotin (Adcetris) for Hodgkin Lymphoma August 29, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
 perc noted that it was challenging to interpret the data and that limited conclusions could be drawn from these non-comparative trials. The Committee discussed the likelihood of conducting a higher-quality
perc noted that it was challenging to interpret the data and that limited conclusions could be drawn from these non-comparative trials. The Committee discussed the likelihood of conducting a higher-quality
 QoL compared with ADT plus placebo. perc considered this to be reasonable in the nmcrpc setting, where patients QoL is expected to be relatively high and stable. perc discussed that there is a net clinical
QoL compared with ADT plus placebo. perc considered this to be reasonable in the nmcrpc setting, where patients QoL is expected to be relatively high and stable. perc discussed that there is a net clinical
patients who have received multiple lines of prior chemotherapy including a platinum-containing regimen patients without formal measurable disease
 patients who have received multiple lines of prior chemotherapy including a platinum-containing regimen patients without formal measurable disease First, perc agreed with CGP that the diagnosis of urothelial
patients who have received multiple lines of prior chemotherapy including a platinum-containing regimen patients without formal measurable disease First, perc agreed with CGP that the diagnosis of urothelial
pan-canadian Oncology Drug Review Submitter or Manufacturer Feedback on a pcodr Expert Review Committee Initial Recommendation
 pan-canadian Oncology Drug Review Submitter or Manufacturer Feedback on a pcodr Expert Review Committee Initial Recommendation Vemurafenib (Zelboraf) for Advanced Melanoma June 1, 2012 3 Feedback on perc
pan-canadian Oncology Drug Review Submitter or Manufacturer Feedback on a pcodr Expert Review Committee Initial Recommendation Vemurafenib (Zelboraf) for Advanced Melanoma June 1, 2012 3 Feedback on perc
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer October 29, 2015
 for Gastric Cancer October 29, 2015") pan-canadian Oncology Drug Review Final Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer October 29, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer October 29, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pembrolizumab (Keytruda) for Nonsquamous Non-small Cell Lung Cancer April 4, 2019
 for Nonsquamous Non-small Cell Lung Cancer April 4, 2019") pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pembrolizumab (Keytruda) for Nonsquamous Non-small Cell Lung Cancer April 4, 2019 DISCLAIMER Not a Substitute for Professional Advice
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pembrolizumab (Keytruda) for Nonsquamous Non-small Cell Lung Cancer April 4, 2019 DISCLAIMER Not a Substitute for Professional Advice
vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd.
 SMC No. (792/12) Roche Products Ltd.") Resubmission vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd. 08 November 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Resubmission vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd. 08 November 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
 at least one dose interruption. perc noted the manufacturer of ponatinib issued a dose reduction recommendation in the PACE study; however, there are currently no data on the optimal starting dose for
at least one dose interruption. perc noted the manufacturer of ponatinib issued a dose reduction recommendation in the PACE study; however, there are currently no data on the optimal starting dose for
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenalidomide (Revlimid) for Multiple Myeloma October 22, 2013
 for Multiple Myeloma October 22, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenalidomide (Revlimid) for Multiple Myeloma October 22, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenalidomide (Revlimid) for Multiple Myeloma October 22, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 where cytotoxic chemotherapy has been administered, perc agreed that it would be reasonable to treat patients with nivolumab, provided they meet all other criteria within this Recommendation. perc also
where cytotoxic chemotherapy has been administered, perc agreed that it would be reasonable to treat patients with nivolumab, provided they meet all other criteria within this Recommendation. perc also
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Ipilimumab (Yervoy) Reference Number: CP.PHAR.319 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Coding Implications Revision Log See Important
Clinical Policy: Ipilimumab (Yervoy) Reference Number: CP.PHAR.319 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Coding Implications Revision Log See Important
 combination with everolimus with other relevant treatment options, perc considered the results of a submitted indirect treatment comparison (ITC) that included comparisons of lenvatinib in combination
combination with everolimus with other relevant treatment options, perc considered the results of a submitted indirect treatment comparison (ITC) that included comparisons of lenvatinib in combination
pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013
 for metastatic Renal Cell Carcinoma March 7, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Regorafenib (Stivarga) for Gastrointestinal Stromal Tumors
 for Gastrointestinal Stromal Tumors") pan-canadian Oncology Drug Review Final Clinical Guidance Report Regorafenib (Stivarga) for Gastrointestinal Stromal Tumors May 2, 2014 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Clinical Guidance Report Regorafenib (Stivarga) for Gastrointestinal Stromal Tumors May 2, 2014 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Differentiated Thyroid Cancer September 20, 2016
 for Differentiated Thyroid Cancer September 20, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Differentiated Thyroid Cancer September 20, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Differentiated Thyroid Cancer September 20, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
Cost-effectiveness of nivolumab with ipilimumab (Opdivo with Yervoy ) for the treatment of advanced (unresectable or metastatic) melanoma.
 for the treatment of advanced (unresectable or metastatic) melanoma.") Cost-effectiveness of nivolumab with ipilimumab (Opdivo with Yervoy ) for the treatment of advanced (unresectable or metastatic) melanoma. The National Centre for Pharmacoeconomics (NCPE) has issued a
Cost-effectiveness of nivolumab with ipilimumab (Opdivo with Yervoy ) for the treatment of advanced (unresectable or metastatic) melanoma. The National Centre for Pharmacoeconomics (NCPE) has issued a
CONTEXT OF THE RESUBMISSION EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 treatment option, there is a notable pill burden at five tablets per day. perc also noted that patients valued additional treatment options relevant to their genotype. perc, however, noted that the increased
treatment option, there is a notable pill burden at five tablets per day. perc also noted that patients valued additional treatment options relevant to their genotype. perc, however, noted that the increased
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION
 FINAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
Yervoy. Yervoy (ipilimumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.13 Subject: Yervoy Page: 1 of 5 Last Review Date: September 15, 2017 Yervoy Description Yervoy (ipilimumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.13 Subject: Yervoy Page: 1 of 5 Last Review Date: September 15, 2017 Yervoy Description Yervoy (ipilimumab)
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Renal Cell Carcinoma
 for Renal Cell Carcinoma") pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Renal Cell Carcinoma January 4, 2019 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Lenvatinib (Lenvima) for Renal Cell Carcinoma January 4, 2019 DISCLAIMER Not a Substitute for Professional Advice This report is primarily