Active Surveillance Current status and future directions. Laurence Klotz Professor of Surgery Sunnybrook Health Sciences Centre University of Toronto
|
|
|
- Felix Nelson
- 5 years ago
- Views:
Transcription
1 Active Surveillance Current status and future directions. Laurence Klotz Professor of Surgery Sunnybrook Health Sciences Centre University of Toronto
2 Case 1 60 year old healthy male, PSA 6, no family history, DRE 40 cc benign feeling prostate PSA increased to 8 over 2 years Biopsy: Gleason 3+3=6 in 4/12 cores (bilateral), 10-30% core involvement I am most likely to offer him 1. Radical prostatectomy 2. Brachytherapy 3. IMRT 4. Active surveillance 5. Other (Focal/cryo/HIFU)
3 Our world has changed over last decade Benefits of PSA unquestioned by urological community Enthusiasm for 5 ARI for chemoprevention (Thompson 2003) Optimism about Vit E and Selenium (SELECT) Benefit of RP on Pca mortality confirmed (SPCG-4, NEJM 2002) Menon RALP lecture SUO % of low grade Pca treated radically USPSTF Grade D recommendation on PSA screening (Chou et al Ann Int Med 2011) Chemoprevention dead FDA denies 5 ARI approval SELECT trial negative, increased Pca Vit E arm No impact of RP on all cause mortality and Pca mortality in PIVOT (Wilt, NEJM 2012) In US: Open RP on life support, >80% RALP Active Surveillance
4 Active Surveillance for low risk PCa What has changed (Klotz, Choo J Urol Urol, 167: 1664, 2002) g (,,, ) Greater recognition of overtreatment problem, wider acceptance of surveillance Molecular characterization of Gleason pattern 3 vs 4 Better understanding of nature of occult high grade disease New definition of clinically insignificant disease Better understanding of flaws of PSA kinetics Increasing data on multiparametric MRI New modelling studies Longer follow up of surveillance cohorts Randomized data on role of 5 ARIs
5 If the past quarter century has brought minimally invasive procedures, the next may bring the elimination of invasion. N Engl J Med 2012;366:
6 .strong consideration should be given to modifying the anxietyprovoking term cancer for this condition
7 US Preventive Services Task Force summary on PSA screening 10/2011: small to no reduction in 10 year prostate cancer-specific mortality; harms related to false-positive test results, subsequent evaluation, and therapy, including overdiagnosis and overtreatment. optimal screening intervals and PSA thresholds remain uncertain. The Task Force recommends against PSA- based screening a Grade D recommendation.
8 Laurence Klotz, Professor of Surgery (Urology) April 1, 2013 The US Preventive Services Task Force recommendation was a wake up call to the urological and radiation oncology communities that something had to change. Trends in Urology blog, submitted at request of R. Kirby Mr Sandy Tyndale-Biscoe April 2, 2013 Wake up call, eh? Apity it is at the expense of the thousands of men who ll die unnecessarily because their primary care physicians, not being specialists, and not understanding the complex issues, advise their patients not to know their PSA. I m not sure that wake up call is quite the term I d use; what about culpable homicide? There is an encouraging trend towards litigation by patients who are diagnosed with metastatic PCa having been earlier denied a PSA test by their doctors. My organisation has helped some of them. It s the only recourse in the face of the arrogance of those who argue that t a man is better off not knowing his PSA.
9 2 reactions to USPSTF Head in sand, or reduce overdx/overtreatment t t






10 NYT Oct from
11 Causes of overdiagnosis Redefinition of disease Imaging studies Screening tests
12 Effect of lower diagnostic thresholds on the number of sick Americans Disease Change in Old Disease New Thresholdh Prevalence Disease Prevalence New Cases Diabetes Fasting 11,700,000 13,380,000 1,620,000 14% Glucose Increase Hypertension Systolic 38,700, ,180,, ,480, % Diast Hyperlipidemia Osteoporosis in women Androgen deficiency Total Chol T score Total Testost < 11 nm (320 ng/dl) 49,480,000 92,127,000 42,647,000 86% 8,010,000 14,800,000 6,790,000 85% 20% of men > 70, 30% > 80 10,000,000
13 Problems of overdiagnosis Asthma Canadian study: 30% with diagnosis may not have asthma, 66% may not require medications Attention deficit hyperactivity disorder Widened definitions & overdiagnosis Boys born at end of the school year have 30% higher chance of diagnosis and 40% higher chance of medication than those born at beginning of year Breast cancer one third of screening detected cancers may be overdiagnosed Chronic kidney disease egfr definition classifies 1 in 10 as having disease concerns about overdiagnosis of many elderly people Gestational ti diabetes Expanded definition classifies 1 in 5 pregnant women High blood pressure Systematic review suggests substantial overdiagnosis High cholesterol up l to 80% with mild elevation cholesterol l overdiagnosed d Lung cancer 25% of screening detected lung cancers overdiagnosed Osteoporosis Expanded E d d definitions--many iti treated t low risk women have net harm from treatment Pulmonary embolism Increased diagnostic sensitivity detection of small emboli. Many may not require anticoagulant treatment Thyroid cancer Much of the observed increase in incidence overdiagnosis
14 Factors promoting overdiagnosis of cancer Welch H G, Black W C JNCI J Natl Cancer Inst 2010;102: Existence of a silent disease reservoir Activities leading to its detection, ie screening Long natural history hence modest cancer specific mortality
15 Two distinct patterns of rapid rises in the rate of diagnosis Welch H G, Black W C JNCI J Natl Cancer Inst 2010;102:
16 Rate of new diagnoses and death SEER 1975 to Epidemic or Epidemic or overdiagnosis?






17 Rates of new diagnosis and death for five types of cancer in the US, Epidemic or overdiagnosis? Moynihan R et al. BMJ 2012;344:bmj.e3502
18 Natural history of breast cancers detected in the Swedish mammography screening programme Zahl P et al Lancet Oncology 12 (12), , Nov , women screened x 6 yrs vs 320, controls screened at study end Screened group: Higher 6-year incidence of invasive cancer 1443 per vs 1269 per ; RR 1 14 Expected Observed Disappeare d cancers
19 10% of impalpable 2 cm breast cancers, 50% of 1 cm cancers, and 99% of 1 mm cancers disappear S. Narod, Professor of Epidemiology, Dalla Lana School of Public Health, University of Toronto
20 Extended lung cancer incidence follow-up in the Mayo Lung Project and overdiagnosis. Marcus PM et al, JNCI Jun 7;98(11): Randomized trial of CXR and sputum cytology screening End point lung cancers detected at 6 years, 46 extra cancers in screened group.
21 Drivers of overdiagnosis Technological l changes detecting ti ever smaller abnormalities Sincere interest in finding/preventing life threatening disease Commercial and professional vested interests Conflicted panels producing expanded disease definitions and writing guidelines Legal incentives that punish underdiagnosis but not overdiagnosis Health system incentives favouring more tests t and treatments Cultural beliefs that more is better; faith in early detection unmodified by its risks
22 Prevalence of invasive prostate cancer in men dying of trauma. Sakr W, Eur Urol 30:138, /1/2014
23 Prevalence of Autopsy Prostate Canceron Unscreened Caucasian and Asian Men Zlotta A, Klotz L, Egawa S, Pushkar D JNCI J Natl Cancer Inst Jul 17;105(14): Asian and 226 Russian men dying of other causes Unscreened PCaPrevalence 35 and 37% Age % with Gleason 7 Asian N % Russian N % /1 0 4/ /8 25 4/ / /34 29

24 Hallmarks of Cancer Hannahan and Weinberg, Cell 2011
25 Molecular pathways mediating the hallmarks of cancer Adapted from Hanahan and Weinberg, Cell 2011 Dysregulated cellular energetics Avoiding Immune destruction
26 Emerging hallmarks and enabling characteristics Hanahan and Weinberg, Cell 2011
27 Gleason 3 lacks hallmarks of cancer Characteristic/Pathway Gleason 3 Gleason4 Expression of pro-proliferation embryonic, neuronal, hematopoietic stem cell genes, EGF, EGFR No Overexpressed AKT pathway: MAP2K4, RALA, PHLPP, PML No Aberrant HER2/neu No Amplified Insensitivity to Antigrowth signals (Cyclin D2 methylation, CKDN1β) Expressed Absent Resisting apoptosis: DAD1 Negative Strong Exp BCL2 Mostly Neg. Upregulated Absence of senescence: TMPRSS2-ERG ERG normal Increased Sustained angiogenesis: VEGF Expression of other pro-angiogenic factors, microvessel density Expression low Normal Increased Increased Tissue invasion/metastasis markers (CXCR4, others) Normal Overexpressed Clinical evidence of metastasis/mortality Absent Present
28 20 Year Prostate Cancer Specific Mortality After Radical Prostatectomy. Eggener S, Scardino P, Walsh P et al N=23,910 12,000 Gleason 2-6 Risk of Pca death after RP in men age 60-69: 02%at20 0.2% 20 years (although significant PSA failure rate) J Urol 185 (3), March 2011
29 Does Gleason Score <=6 Metastasize to Lymph Nodes? Ross HM et al American Journal of Surgical Pathology 36(9), September 2012, p ,123 cases of path. confirmed Gleason 6 22 cases with positive LN. 100% of these had higher grade than originally reported NOT A SINGLE CASE of confirmed Gleason 6 tumor with LN mets
30 PIVOT Prostate cancer survival Wilt T et al, NEJM 367;3, July 2012:
31 But biology is rarely so black and white
32 The clonal origin of lethal prostate cancer Haffner M, Yegasubramanian et al, JCI, epub Oct year old male, RP 1995: Gleason 4+3 pt3a N1 Died of CRPC 2012; Warm autopsy acquisition of 7 metastatic sites Whole-genome sequencing & molecular profiling Whole-genome sequencing & molecular profiling Small Gleason 3+3 focus source of original metastasis (lung)




33 The clonal origin of lethal prostate cancer Haffner M, Yegasubramanian et al, JCI, epub Oct
34 Linear vs bifurcated models of Pca development (Droller M et al 2012) Haffner
35 Rate of upgrading from time of diagnostic biopsy Slope = 1.0%/year
36 Analysis of the Tumor Volume Threshold for Clinically Insignificant PCa from ERSPC. Wolters T, Roobol M, Schröder F, van der Kwast T. J Urol 185, , Stamey 1982 Wolter et al, ERSPC 8% incidence of clinical Pca Diagnosis rate in 8% of cysto-prostatectomy unscreened arm 50% of specimens had > 0.5 cc Gleason that t in screened arm 3 or some 4 Volume of 325 RP Cancers 4/3πr 3 =1.0cc diameter sphere Threshold volume = 1.3 cc (1.4 cc diameter sphere) for Gleason 6 4/1/ cm
37 For Which Older Men is Surveillance a Safe Management Option? Low risk (D Amico) Stage T1c/T2a PSA <10ng/ml Gleason score <6 Very low risk (Epstein) Stage T1c PSAD <0.15 Gleason score <6 <3 cores with cancer <50% core involvement Favorable Risk
38 National Comprehensive Cancer Network Practice Guidelines RECURRENCE EXPECTED INITIAL RISK SURVIVAL THERAPY Very Low (Epstein Criteria) <20 yr Active Surveillance Preferred Low Risk >20 yr 1) Active Surveillance (D Amico Criteria) >10yr 2) Radiotherapy 3) Radical Prostatectomy Mohler et al, J Natl Compr Canc Netw. 2010
39 Predictive factors for upgrading: Volume counts. Toronto cohort. Higher volume Gleason 6 predicts for increased risk of higher grade cancer Multivariate Model Variable OR 95% CI p-value Clinical T-stage (T2 vs T1) Higher PSA at baseline % cores involved <.0001 at diagnostic biopsy
40 Predictive factors for Gleason upgrading in candidates for active surveillance: Tosoian J, Epstein J, Carter HB et al, J Urol 2013 N=7,486 RPs since 1975 with LR or VLR disease LR Low risk VLR Very low risk
41 Factors predicting upgrading in a Swedish RP cohort Bratt O, Klotz L et al JCO N=1286 low risk patients OR 95% CI p-value Clinical i l stage T1c 1.00 ( Reference ) T ( ) No. of positive biopsies ( Reference ) ( ) ( ) < ( ) 0.02 Cancer extent < 4mm 1.00 ( Reference ) 4 8mm 1.21 ( ) mm 1.69 ( ) < mm 1.88 ( ) <0.001
42 Factors predicting upgrading in a Swedish RP cohort Bratt O, Klotz L et al JCO Cancer extent and pos cores
43 Medium-term Outcomes of Active Surveillance for Localised Prostate Cancer: Selvadurai E, Parker C et al European Urol Feb N=471 Median f/u 5.7 yr 27 deaths 2 from Pca Both had early upgrading Adverse histology=gleason 4+3 or PPC > 50%%.
44 Predicting adverse pathology in 4,500 low risk men from NPCR who underwent RP: Vellekoop A, Stattin P et al, The Journal of Urology, Volume 191, Issue 2, 2014,
45 How?
46 Selection criteria for active surveillance Author Dall Era Gleason Positive %core score cores involvement 6 (no 4 or 5 pattern) % positive PSA PSA density cores <33 <10 2a Ercole 6 2 <50 <10 2a Klotz 6 10* 2b Soloway Tosoian 6 2 <50 <0.15 1c Ischia 6 <10 2a Bul Godtman 6 <10 2a Thomsen 6 3 < a Selvadurai 6 50 <15 2 ct stage


47 Follow-up Toronto and PRIAS (Rotterdam) DRE/PSA every 3 months for 2yrs, then every 6 months Biopsy 6-12 months after enrollment, then every 3-5 yrs Johns Hopkins DRE/PSA at 6 month intervals Biopsy annually until age 75yrs
48 Progression criteria used in active surveillance Publication Gleason Positive % of core % pos PSAdt score* cores involved cores (years) PSAv (ng/ml/ye ar) ct stage Dall Era Increase >0.75 Ercole Progression Increase Increase Change Klotz 4+3 <3 Increase Soloway (grade) >3 >2 Tosoian >6 >2 >50 Ischia Upgrade * Upstage Bul Godtman Upgrade * Upstage Thomsen 3+4 >3 <3/5* Increase Selvadurai >50 >1 *Patients with PSAdt<3 years were recommended curative treatment while treatment options were discussed with patients with a PSAdt 3-5 years
49 Comparing PSA Triggers for Intervention in Men With Stable Prostate Cancer on Active Surveillance Loblaw A, Klotz L J Urol 184(5) 1942 (2010) 305/453 men whose disease was stable by all criteria No metastasis, t no radical intervention, ti no upgrading to > 3+4 PSA trigger Percent triggered ( Median # of times triggered PSA DT < 3 yrs by linear regression 50% 3 PSA velocity > 2 ng/ml/yr 42% 3 1 year PSA Vel > 2 51% 2 PSA > 10 38% 3 PSA > 20 13% 1
50 Systematic Review of Pretreatment PSA Velocity and Doubling Time As PCA Predictors. Vickers A J Clin Oncol 27: Studies with > 200 patients Author Study Performance of PSA velocity vs PSA Eggener 995 neg initial bx PPV Velocity 3% higher Djavan 559 Bx result Worse AUC Sun Ca screen Worse AUC (Verification bias) Moul Ca screen Worse AUC Carter 980 Ca death long term Velocity AUC 0.75 vs PSA 0.74 Berger 4800 Ca screen Velocity 0.87 vs PSA 0.65 (VB) Whittemore 320 Ca death long term Worse AUC Loeb 6844 Ca screen AUC 0.83 vs 0.81 (VB) Thompson 5519 Bx in PCPT No difference Verification bias (VB): Men not having a biopsy assumed to be cancer free Little evidence that pretreatment PSA velocity or doubling time are of value for early-stage prostate cancer.
51 Toronto cohort: Intervention free survival N=840
52 Toronto Cohort overall survival 2014 N=840
53 Proportion discontinuing surveillance at 3, 5, and 10 years Publication, year Study design No patients Median Median T follow-up from Dx (years) to Rx 5 years (%) 10 years (%) Pca mortality Dall Era P Na 0 Ercole R Na 0 Klotz P NR Soloway R Na 0 Tosoian P Ischia R (mean) Bul RP /40 50/70 0 Godtman RP NR Thomsen P NR 40 Na 0 Selvadura i 3% 10 yr P Na 2% 8 yr Ttl 4453
54 PRIAS results: Active therapy free survival over time Bul et al, European Urology 63 (4) April 2013:
55 Prostate cancer survival with active surveillance Age > or < 70
56 Time to PSA failure as a proportion of all patients 6.3% of cohort had PSA failure after surgery or radiation
57 22/993 men developed metastasis Overall Survival in this group Median: 7.3yr
58 Cox Regression Analysis p-value Odds ratio 95%CI Age Age 70 vs 70< PSA PSA 10 vs 10< Clinical Stage T1 vs T Treatment PSADT 3y vs 3y< PSADT 2y vs 2y< Primary Biopsy GS 6 vs Positive core 2 vs 2< Positive Core rate 50 vs 50< Confirmatory biopsy N/A vs Available GS 6 vs 7 vs Positive core 2 vs 2< Positive Core rate 50 vs 50<
59 Time from diagnosis to post-treatment PSA failure
60 RP Pathology Is Favorable in Men Following Initial Active Surveillance Hong SK, Toujier K, Eastham J et al Euro Urol Epub Aug 2013
61 Cumulative hazard ratio for prostate cancer and other cause mortality Overall Stratified by age or > 70
62 Prospective active surveillance studies Median Freedom from bned after deferred Prostate cancer Mortality from other Study n follow up yr treatment treatment mortality % causes UCSF % at 5 yr 1 recurrence at 3 yr 0 0 University of 10 yr OS: Toronto % at 5 yr 5 yr bned: 47% 3% at 15 yr 68% Multicentre PRIAS % at 2 yr No data 0 4 yr OS: 87% University of Miami % at 5 yr No recurrences 0 No data Johns 90.6% recurrence free 1.8% of Hopkins % at 5 yr at 2 yr 0 cohort Royal Marsden % at 5 yr 85% PSA failure free at 5 yr 2% at 8 yr 9% at 8 yr
63 Comparison of mortality outcome: Surveillance vs radical treatment with propensity score analysis. Stephenson A, Klotz L et al ,881 men treated between AS, 6485 RP, 2264 XRT, 1680 Brachy AS: 71% low risk, 16% intermediate, 5% high Radical Rx: 57% low, 31% int, 12% high Increased all cause mortality in treated group HR1.5 (XRT and brachy, not RP) No difference in prostate cancer mortality
64 Multivariable competing risk regression analysis Cancer specific mortality Other cause mortality HR CI P Value HR CI P Value Radical Therapy vs. Active Surveillance Year of Diagnosis < Age at Diagnosis PSA at Diagnosis Clinical Stage Biopsy Gleason Score Comorbidity < T2b vs T1ab T2c vs T1ab T3 vs T1ab vs < vs < Mild vs. None < Moderate vs. None < Severe vs. None < 0.001
65 Threshold Analysis of Utility of Active Surveillance and Probability of Prostate Cancer Specific Death (PCSD) x Hayes, J. H. et al. JAMA 2010;304: Copyright restrictions may apply.
66 PRIAS results: Bul et al, European Urology 63 (4) April 2013: Reason for deferred therapy in 527 treated patients Treatment type No. (%) Radical prostatectomy 253 (48.0) Radiotherapy 238 (45.2) Hormonal therapy 8 (1.5) Other* or unknown therapy 28 (5.3) Reason for treatment t t Protocol based 387 (73.4) Gleason score >6** 61 (15.8) More than two positive cores 146 (37.7) Gleason score >6 and more than two positive cores 99 (25.6) PSA DT <3 yr 81 (20.9) Anxiety 47 (8.9) Other*** 93 (17.6)
67 Outcome of repeat biopsies (N=592) Toronto Cohort
68 RP vs WW in Early PCa Bill-Axelson A, Holmberg L NEJM 364;18, May NNT 15; 7 for men < 65 yrs
69 Mortality in low risk disease Scandinavian trial vs Sunnybrook active surveillance. Klotz L, Thompson I NEJM 265(6): Low Risk Disease Active surveillance
70 Long term quality-of-life outcomes after radical prostatectomy or watchful waiting: SPCG-4 randomised trial Johansson E, Gunnar Steineck. Lancet Oncol 12(9), 891, 2011 No difference in any measure of psychological functioning Between RP and WW group at 12 years
71 Dutasteride in surveillance: time to pathological progression 302 patients t randomized d between dutasteride t and placebo Biopsy Biopsy Relative Risk Reduction 44.3% 57.4%% P = P = REDEEM: DS Figure 7.1, Table 7.4
72 5 ARIs in surveillance. Chiang A, Klotz L et al, CUAJ 2013, 7(11-12), 12) men on AS placed on 5 ARI, 3 PSAs pre and post treatment. Median F/U 6 years Median PSA DT pre treatment 56 months, post treatment 25 months Percent change in pre 5 ARI vs post-nadir PSA DT
73 How we can do surveillance better 1. Broader inclusion (Gleason 3 + small amount of 4)
74 Challenges in active surveillance Classification To risk stratify accurately Responsiveness To detect change when it occurs Harm reduction To reduce the burden of the biopsy
75 Limitations of current approach Systematic biopsy: Doesn t exclude significant cancer May overdiagnose some clinically insignificant disease Urosepsis rate after biopsy 4% Many men elect treatment without objective change in disease Men don t like it PSA limitations Labile analyte Unreliable DRE: normal in most men on surveillance
76 Case 2 60 year old healthy male, PSA 8, no family history, DRE 40 cc benign feeling prostate Biopsy: Gleason 3+4=7 in 2/12 cores, 10-15% core involvement, 10% pattern 4 I am most likely to offer him 1. Radical prostatectomy 2. Brachytherapy 3. IMRT 4. Active surveillance 5. Other (focal/cryo/hifu)
77 Difference between original and modified (2005) Gleason scoring system
78 Effect of tangential cutting on Gleason grade 25% of surveillance candidates Condordance between GU pathologists for these lesions 27% McKenney ey J, Carroll P J Urol (2), pg
79 Modified Gleason scoring 2005: Grade inflation Reference Traditional Gleason Modified d Gleason Helpap Gleason 6 48% 22% Gleason 7 26% 68% Billis Gleason 6 68% 49% Gleason 7 26% 39% Helpap B Virchows Arch 2006 Dec;449(6):622-7 pp ; ( ) Billis A J Urol Aug;180(2):548-52
80 1 Gleason score not predictive of progression in surveillance cohort: Choo R, Klotz L J Urol 167(4):1664-9
81 Slide 80 1 Laurence Klotz; 17/02/2012
82 Time to progression for patients with low- and intermediate-risk risk prostate cancer on surveillance. 90 men with intermediate risk disease 1/3 had Gleason 7, 2/3 PSA > 10 No difference in any outcome compared to low risk Cooperberg M R et al. JCO 2011;29: by American Society of Clinical Oncology
83 How we can do surveillance better 2. Earlier identification of high risk patients
84 Pathology at RP by Race in men managed with surveillance followed by RP Sundi D, Epstein J et al. J Urol 191 (1) 2014: Dominant nodules Very low risk Very low risk upgraded
85 The role of multiparametric MRI in managing early prostate cancer 1. Not readily available; I don t use it. 2. Would use it more, but cost prohibitive 3. Unsure of its role; use selectively for staging g 4. Use routinely in men considering surveillance 5. I obtain it in all newly diagnosed patients





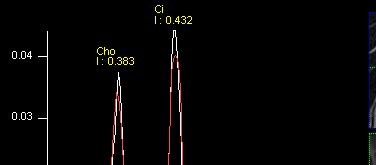



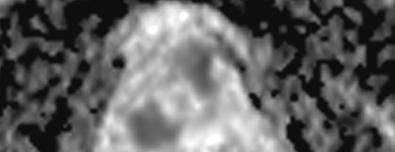



86 Multiparametric Prostate MRI = Comprehensive Morphologic/Biologic l i Imaging T2w-MRI DCE-MRI 3D- 1 H-MRSI DW-MRI (ADC) Morphology Perfusion Metabolism Cell Density/Grade
87 Diffusion weighted image and grade. Hambrock et al, May 2011 Radiology, 259,
88 Potential for MRI in active surveillance










89 Biopsy Missed Tumors (Anterior/Base/Apex) 30% 70% Copyright Radiological Society of North America, 2007 Choi, Y. J. et al. Radiographics 2007;27:63-75
90 Central Gland Tumors 30% of tumors involve the central gland central zone + transition zone + periurethral glands






91 T2 ADC DCE MRI k ep map
92 Can we target a prostate cancer tumour on MRI TARGET: 2/5 cores positive: 1 and 4mm CCLmax Gleason (20%) NON-TARGET 28 cores negative
93 64-year-old PSA 3.7 ng/ml, one positive biopsy core Gleason 6. All MR images negative. RP: Gleason 6 pt2 T2WI DWI DCEI
94 66-year-old, PSA 4.81 ng/ml, one positive biopsy core Gleason T MRI: decreased T2, DWI, and abnormal DCE left PZ. RP: Gleason 7 (3+4), pt2
95 388 men low D Amico risk score MRI and confirmatory biopsy within 6 months of initial biopsy MRI 1-2/5 0-4% upgrade (NPV 97%) MRI score 5/ % upgrade 94
96 60 men with biopsy suitable for AS Negative MRI: 38% Concordant MRI: 40% Discordant MRI: 22% (13/60) of which 10/13 (77%) showed upgrade on confirmatory biopsy
97
98 Template vs MRI targeted biopsy Characteristic MRI-Targeted Template Prostate Biopsy Biopsy Total number of cores, n Number of cores per patient, median (IQR) Median sampling density, number of biopsies/ml of prostate t (IQR) Number of cores positive for any cancer, n (proportion of total cores) 5 (4-6) 30 (22-53) 0.11 ( ) 0.88 ( ) 356 (38.2%) 971 (13.5%)
99 Cancer Detection Rates: Clinic cally Signif ficant Clinically Significant Template Biopsy Clinically Insignificant All Cancer: 78% Clinically Significant Cancer: 64% Clin nically Insig gnificant MRI- -Targe eted Biops sy No cance er No cancer Totals Totals



 Accounting for probe-induced")

100 Commercial systems Eigen Artemis: 3D TRUS-guided biopsy Compatible with wide range of TRUS probes Non-rigid, surface-based registration ti MR-TRUS TRE ~3.1 +/- 1.4mm (Narayanan et al., 2009) 4-5mm (Cool et al. 2011) Accounting for probe-induced prostate deformation after repositioning the probe for each biopsy sample can lead to a time- consuming procedure




101 MedCom/Pi Medical BiopSee 3D-image-guided transperineal biopsy and therapy Integrated solution Rigid registration Commercial systems Accuracy not fully quantified (Zagel et al. 2011)
102 Tumour targeting using the SmartTarget TM system
103 Systematic versus image-guided guided biopsies Systematic TRUS biopsy Gleason 3 plus 4 1 of 12 cores +ve CCLmax 3mm
104 Systematic versus image-guided guided biopsies Image-guided biopsy Gleason 4 plus 4 100% positive CCLmax=8mm
105 Risk shift using targeted biopsies Robertson NL et al. Eur Urol. 2013
106 Active Surveillance Magnetic Resonance Imaging Study (ASIST TRIAL) Laurence Klotz (study chair) 1 Andrew Loblaw (co-chair) 2 Masoom Haider (co-chair) 3,4 Aaron Fenster 6 Linda Sugar 7 Theo Van der Kwast 8 Robert Bristow 9 Danny Vesprini 2 This study was funded by an Ontario Instit of Cancer Research gr
107 ASIST Trial Summary Randomize (within 6-12 months of initial diagnostic biopsy) ARM 1 Active surveillance with core biopsy at 9 months (6-13 months) after initial biopsy, and serial PSA determinations ARM 2 Active surveillance with MR imaging and guided biopsy at 9 months (6-13 months) after initial biopsy, and serial PSA determinations Pathologic Upgrading N of pts having treatment Clinical i l stage Number, size, location of radiographic lesions PSA failure post treatment Clinical progression 275 bj t ill b d f th ti i ti C di U l R h 275 subjects will be accrued from three participating Canadian Urology Research Consortium (CURC) sites in an estimated time of 2 years. Primary analysis is planned one year after study recruitment is
108 Modern challenges in active surveillance Classification To risk stratify with precision Responsiveness To be able to detect change when it occurs Prediction To reduce the burden AS
109 Stable on surveillance Gleason Targeted 3/4 cores positive CCLmax 5mm
110 2009 Progression on surveillance year old man <5% cancer on TURP. MRI 2009, PSA 0.9. PSA rose to 2.6 in Increase in size of right PZ lesion, particularly marked on diffusion
111 PCA3 score association with pathological findings References No. Men Insignificant PCa p Value <.05 Tumor Vol Less Than 05cm p Value <.05 Gleason Score 7 p Value <.05 Auprich 160 No Yes Yes No Whitman 72 No Yes No Yes Nakanishi 83 No Yes Yes No Liss 100 Yes N/A No No Hessels 70 Yes No No N/A van Gils 62 Yes Yes No No Extracapsular Extension p Value
112 Genetic markers for assessment of risk of developing prostate cancer, and for screening, prognosis, and prediction of response to therapy
113 PSA, TMPRSS2:ERG, and PCA3, alone and in combination, for prediction of high Gleason grade ( 7) Lin D W et al. Clin Cancer Res 2013;19: by American Association for Cancer Research
114 If you tell someone they are on fire, they run for a fire extinguisher. We need to communicate a difference message. 4/1/2014
115 Likelihood of a low risk Pca patient being managed by surveillance, by urologist. Hoffman K et al JCO % of patients offered surveillance were managed by care of 3.5% of urologists.
116 Multidisciplinary care and choice of active surveillance Aizer A, D Amico A, JCO 2012 Multidisciplinary clinic doubled the number choosing surveillance


117 Favorable risk disease is heterogeneous Pseudo-disease Evasive anterior cancer Carey map cm 4/1/2014 Favorable but significant
118 Surveillance vs focal vs radical Surveillance Gleason 6 and microfocal or older patients Radical Treatment Most Gleason 7 (4+3 unifocal or 3+4 multifocal) Focal Therapy Gleason 6 with large volume, or Gl 7, unilateral 4/1/2014
119





120 Focal Therapy: Concept Novel imaging and precision biopsy can identify those lesions that are likely to progress Selective therapy to Clinically significant lesions alone will be as effective as whole-gland treatment with less harm
121 Trifecta rate after focal HIFU. Ahmed H, Emberton M et al Lancet Oncology (June 2012), 13 (6), pg Hashim U Ahmed
122 MRI and surveillance: Challenging questions Should men with Gleason 6 and MR visible disease > ~1 cm remain on surveillance? Should MRI be used as a trigger for biopsy or for treatment in men on surveillance? Is biopsy still required if MRI negative? How often should MRI be performed? Role of biomarkers?
123 AS: Current approach Offered to Gleason 6, PSA 10 (accepted by most) Increased volume of Gleason 6 a marker for higher h grade disease, not necessarily intervention PSA kinetics a guide only Confirmatory biopsy within 1 year, targeting g anterior/anterolateral horn Repeat biopsy q 3-5 years (age, risk tolerance, PSA) to 80 MP-MRI for PSA DT < 3 years or volume increase or 3+minor element 4 Consider treating if significant Gleason 4 or PiRADS 5 lesion > 1.3 cc on MRI
124 The future of active surveillance Screening will be image/risk factor based, hence many fewer biopsies and fewer clinically insignificant cancers. Avoid cancer diagnosis in low risk patients In favorable risk disease: Imaging/biomarker to identify aggressive disease at diagnosis Must be affordable, widely available, reproducible In intermediate risk disease: indolent variant identifiable at diagnosis i Goal: NNT = 1.0


125 University of Toronto UroOncology Fellowship Clinical and research training program Experienced UroOncologist faculty Dr. Anthony Finelli Dr. Neil Fleshner Dr. Rob Hamilton Dr. Michael Jewett Dr. Girish Kulkarni Dr. Laurence Klotz Dr. Rob Nam Dr. John Trachtenberg Dr. Alex Zlotta Rotations in Medical and Radiation Oncology Laparoscopic /Robotic training SUO Accredited d One clinical year and up to two research years with graduate degree opportunity Remuneration includes: Salary, travel expenses, tuition if necessary Contact Laurence.klotz@sunnybrook.ca University of Toronto
Sommerakademie Munich, June
 Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
Active surveillance: Shrinking the grey zone. Sommerakademi e Munich, June rd FOIUS Tel Aviv, July 2016
 Active surveillance: Shrinking the grey zone Active surveillance: 3 rd FOIUS Tel Aviv, July 2016 Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Active Surveillance for low risk PCa What has
Active surveillance: Shrinking the grey zone Active surveillance: 3 rd FOIUS Tel Aviv, July 2016 Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Active Surveillance for low risk PCa What has
Conceptual basis for active surveillance
 Conceptual basis for active surveillance 1. Screening results in overdiagnosis 2. Clinically insignificant disease can be identified 3. All treatments have significant side effects and cost. 4. Delayed
Conceptual basis for active surveillance 1. Screening results in overdiagnosis 2. Clinically insignificant disease can be identified 3. All treatments have significant side effects and cost. 4. Delayed
Pre-test. Prostate Cancer The Good News: Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest
 Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
Detection & Risk Stratification for Early Stage Prostate Cancer
 Detection & Risk Stratification for Early Stage Prostate Cancer Andrew J. Stephenson, MD, FRCSC, FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Risk Stratification:
Detection & Risk Stratification for Early Stage Prostate Cancer Andrew J. Stephenson, MD, FRCSC, FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Risk Stratification:
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
ACTIVE SURVEILLANCE FOR PROSTATE CANCER
 ACTIVE SURVEILLANCE FOR PROSTATE CANCER Dr. Michael J Metcalfe PGY-2 Department of Urological Sciences April 25, 2012 CASE RM 65 year old active Caucasian male, married. PSA= 7.0 T2a Gleason 3+3=6 2/6
ACTIVE SURVEILLANCE FOR PROSTATE CANCER Dr. Michael J Metcalfe PGY-2 Department of Urological Sciences April 25, 2012 CASE RM 65 year old active Caucasian male, married. PSA= 7.0 T2a Gleason 3+3=6 2/6
ACTIVE SURVEILLANCE OR WATCHFUL WAITING
 Prostate Cancer ACTIVE SURVEILLANCE OR WATCHFUL WAITING María Teresa Bourlon, MD MS Head, Urologic Oncology Clinic Hemato-Oncology Department Instituto Nacional de Ciencias Médicas y Nutrición Salvador
Prostate Cancer ACTIVE SURVEILLANCE OR WATCHFUL WAITING María Teresa Bourlon, MD MS Head, Urologic Oncology Clinic Hemato-Oncology Department Instituto Nacional de Ciencias Médicas y Nutrición Salvador
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Sorveglianza Attiva update
 Sorveglianza Attiva update Dr. Sergio Villa Dr. Riccardo Valdagni www.thelancet.com Published online August 7, 2014 http://dx.doi.org/10.1016/s0140-6736(14)60525-0 the main weakness of screening is a high
Sorveglianza Attiva update Dr. Sergio Villa Dr. Riccardo Valdagni www.thelancet.com Published online August 7, 2014 http://dx.doi.org/10.1016/s0140-6736(14)60525-0 the main weakness of screening is a high
Prostate Cancer Screening: Risks and Benefits across the Ages
 Prostate Cancer Screening: Risks and Benefits across the Ages 7 th Annual Symposium on Men s Health Continuing Progress: New Gains, New Challenges June 10, 2009 Michael J. Barry, MD General Medicine Unit
Prostate Cancer Screening: Risks and Benefits across the Ages 7 th Annual Symposium on Men s Health Continuing Progress: New Gains, New Challenges June 10, 2009 Michael J. Barry, MD General Medicine Unit
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
J Clin Oncol 28: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
Where are we with PSA screening?
 Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
Controversies in Prostate Cancer Screening
 Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Prostate Cancer Screening: Con. Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto
 Prostate Cancer Screening: Con Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto / Why not PSA screening? Overdiagnosis Overtreatment Risk benefit ratio unfavorable Flaws of PSA
Prostate Cancer Screening: Con Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto / Why not PSA screening? Overdiagnosis Overtreatment Risk benefit ratio unfavorable Flaws of PSA
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality
 Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Active surveillance: Shrinking the grey zone. Sommerakademi e Munich, June Who is the Right Patient and what is the right Protocol?
 Active surveillance: Who is the Right Patient and what is the right Protocol? Active surveillance: Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Or: Shrinking the Gray Zone IPCU 2017 Active
Active surveillance: Who is the Right Patient and what is the right Protocol? Active surveillance: Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Or: Shrinking the Gray Zone IPCU 2017 Active
Active surveillance: From Biology to Bedside. Who is Going to Fail? Active surveillance: Shrinking the grey zone. Sommerakademi e Munich, June
 Active surveillance: From Biology to Bedside Who is Going to Fail? Active surveillance: Shrinking the grey zone Sommerakademi e Munich, June 30 2016 What is the main reason low risk patients fail? 1. GG1/Gleason
Active surveillance: From Biology to Bedside Who is Going to Fail? Active surveillance: Shrinking the grey zone Sommerakademi e Munich, June 30 2016 What is the main reason low risk patients fail? 1. GG1/Gleason
Risk Migration ( ct2c=high)
") Risk Migration ( ctc=high) Prostate Cancer Over- Detection, but Selective Treatment Active Surveillance Peter R. Carroll, MD, MPH Department of Urology University of California, San Francisco February,
Risk Migration ( ctc=high) Prostate Cancer Over- Detection, but Selective Treatment Active Surveillance Peter R. Carroll, MD, MPH Department of Urology University of California, San Francisco February,
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Expanded criteria for active surveillance in prostate cancer: a review of the current data
 Review Article Expanded criteria for active surveillance in prostate cancer: a review of the current data Cameron Jones 1, Mina M. Fam 2, Benjamin J. Davies 2 1 University of Pittsburgh School of Medicine,
Review Article Expanded criteria for active surveillance in prostate cancer: a review of the current data Cameron Jones 1, Mina M. Fam 2, Benjamin J. Davies 2 1 University of Pittsburgh School of Medicine,
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
PROSTATE CANCER Amit Gupta MD MPH
 PROSTATE CANCER Amit Gupta MD MPH Depts. of Urology and Epidemiology Amit-Gupta-1@uiowa.edu dramitgupta@gmail.com Tel: 319-384-5251 OUTLINE PSA screening controversy How to use PSA more effectively Treatment
PROSTATE CANCER Amit Gupta MD MPH Depts. of Urology and Epidemiology Amit-Gupta-1@uiowa.edu dramitgupta@gmail.com Tel: 319-384-5251 OUTLINE PSA screening controversy How to use PSA more effectively Treatment
PCa Commentary. Executive Summary: The "PCa risk increased directly with increasing phi values."
 1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 77 September October 2012 CONTENT Page The Prostate 1 Health Index Active Surveillance 2 A
1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 77 September October 2012 CONTENT Page The Prostate 1 Health Index Active Surveillance 2 A
Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144
 Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144 Objectives: Detection of prostate cancer the need for better imaging What
Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144 Objectives: Detection of prostate cancer the need for better imaging What
Active Surveillance for Intermediate Risk Prostate Cancer
 Active Surveillance for Intermediate Risk Prostate Cancer Eric Wallen, M.D., FACS Professor Department of Urology The University of North Carolina at Chapel Hill Disclosures: None Objectives Understand
Active Surveillance for Intermediate Risk Prostate Cancer Eric Wallen, M.D., FACS Professor Department of Urology The University of North Carolina at Chapel Hill Disclosures: None Objectives Understand
PSA and the Future. Axel Heidenreich, Department of Urology
 PSA and the Future Axel Heidenreich, Department of Urology PSA and Prostate Cancer EAU Guideline 2011 PSA is a continuous variable PSA value (ng/ml) risk of PCa, % 0 0.5 6.6 0.6 1 10.1 1.1 2 17.0 2.1 3
PSA and the Future Axel Heidenreich, Department of Urology PSA and Prostate Cancer EAU Guideline 2011 PSA is a continuous variable PSA value (ng/ml) risk of PCa, % 0 0.5 6.6 0.6 1 10.1 1.1 2 17.0 2.1 3
To be covered. Screening, early diagnosis, and treatment including Active Surveillance for prostate cancer: where is Europe heading for?
 To be covered Screening, early diagnosis, and treatment including Active Surveillance for prostate cancer: where is Europe heading for? Europa Uomo meeting Stockholm 29 Chris H.Bangma Rotterdam, The Netherlands
To be covered Screening, early diagnosis, and treatment including Active Surveillance for prostate cancer: where is Europe heading for? Europa Uomo meeting Stockholm 29 Chris H.Bangma Rotterdam, The Netherlands
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
MR-US Fusion Guided Biopsy: Is it fulfilling expectations?
 MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
Published Ahead of Print on April 4, 2011 as /JCO J Clin Oncol by American Society of Clinical Oncology INTRODUCTION
 Published Ahead of Print on April 4, 2011 as 10.1200/JCO.2010.32.8112 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.32.8112 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Published Ahead of Print on April 4, 2011 as 10.1200/JCO.2010.32.8112 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.32.8112 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Long-Term Follow-Up of a Large Active Surveillance Cohort of Patients With Prostate Cancer
 Published Ahead of Print on December 15, 1 as 1.1/JCO.1.55.119 The latest version is at http://jco.ascopubs.org/cgi/doi/1.1/jco.1.55.119 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Long-Term
Published Ahead of Print on December 15, 1 as 1.1/JCO.1.55.119 The latest version is at http://jco.ascopubs.org/cgi/doi/1.1/jco.1.55.119 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Long-Term
Elevated PSA. Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017
 Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Prostate Biopsy. Prostate Biopsy. We canʼt go backwards: Screening has helped!
 We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
Focal Therapy is a Fool s Paradise : The whole prostate must be treated!
 Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know
 MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
PSA Screening and Prostate Cancer. Rishi Modh, MD
 PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
Urological Society of Australia and New Zealand PSA Testing Policy 2009
 Executive summary Urological Society of Australia and New Zealand PSA Testing Policy 2009 1. Prostate cancer is a major health problem and is the second leading cause of male cancer deaths in Australia
Executive summary Urological Society of Australia and New Zealand PSA Testing Policy 2009 1. Prostate cancer is a major health problem and is the second leading cause of male cancer deaths in Australia
Problems: TRUS Bx. Clinical questions in PCa. Objectives. Jelle Barentsz. Prostate MR Center of Excellence.
 Multi-parametric MR imaging in Problems: TRUS Bx Low Risk Prostate Cancer Important cancers are missed Jelle Barentsz Clinically insignificant cancers are identified by Prostate MR Center of Excellence
Multi-parametric MR imaging in Problems: TRUS Bx Low Risk Prostate Cancer Important cancers are missed Jelle Barentsz Clinically insignificant cancers are identified by Prostate MR Center of Excellence
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC
 PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
NIH Public Access Author Manuscript World J Urol. Author manuscript; available in PMC 2012 February 1.
 NIH Public Access Author Manuscript Published in final edited form as: World J Urol. 2011 February ; 29(1): 11 14. doi:10.1007/s00345-010-0625-4. Significance of preoperative PSA velocity in men with low
NIH Public Access Author Manuscript Published in final edited form as: World J Urol. 2011 February ; 29(1): 11 14. doi:10.1007/s00345-010-0625-4. Significance of preoperative PSA velocity in men with low
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Active Surveillance for Prostate Cancer: How to Do It Right
 Review Article [1] May 15, 2017 Oncology Journal [2], Prostate Cancer [3] By Juan D. Garisto, MD [4] and Laurence Klotz, MD, FRCSC, CM [5] In this review of active surveillance for favorable-risk prostate
Review Article [1] May 15, 2017 Oncology Journal [2], Prostate Cancer [3] By Juan D. Garisto, MD [4] and Laurence Klotz, MD, FRCSC, CM [5] In this review of active surveillance for favorable-risk prostate
Prostate Biopsy in 2017
 Prostate Biopsy in 2017 Bob Djavan, MD, PhD Professor and Chairman, Department of Urology, Rudolfinerhaus Foundation Hospital,Vienna, Austria Director Vienna Urology foundation Board member Scientific
Prostate Biopsy in 2017 Bob Djavan, MD, PhD Professor and Chairman, Department of Urology, Rudolfinerhaus Foundation Hospital,Vienna, Austria Director Vienna Urology foundation Board member Scientific
Contemporary Approaches to Screening for Prostate Cancer
 Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
Essential Initial Activities and Clinical Outcomes
 Essential Initial Activities and Clinical Outcomes Crystal Farrell 1,2 & Sabrina L. Noyes 2, Joe Joslin 2, Manish Varma 2,3, Andrew Moriarity 2,3, Christopher Buchach 2,3, Leena Mammen 2,3, Brian R. Lane
Essential Initial Activities and Clinical Outcomes Crystal Farrell 1,2 & Sabrina L. Noyes 2, Joe Joslin 2, Manish Varma 2,3, Andrew Moriarity 2,3, Christopher Buchach 2,3, Leena Mammen 2,3, Brian R. Lane
Untreated Gleason Grade Progression on Serial Biopsies during Prostate Cancer Active Surveillance: Clinical Course and Pathological Outcomes
 Untreated Gleason Grade Progression on Serial Biopsies during Prostate Cancer Active Surveillance: Clinical Course and Pathological Outcomes A. A. Hussein,* C. J. Welty,* N. Ameli,* J. E. Cowan, M. Leapman,*
Untreated Gleason Grade Progression on Serial Biopsies during Prostate Cancer Active Surveillance: Clinical Course and Pathological Outcomes A. A. Hussein,* C. J. Welty,* N. Ameli,* J. E. Cowan, M. Leapman,*
Early outcomes of active surveillance for localized prostate cancer
 Original Article ACTIVE SURVEILLANCE FOR LOCALIZED PROSTATE CANCER HARDIE et al. Early outcomes of active surveillance for localized prostate cancer CLAIRE HARDIE, CHRIS PARKER, ANDREW NORMAN*, ROS EELES,
Original Article ACTIVE SURVEILLANCE FOR LOCALIZED PROSTATE CANCER HARDIE et al. Early outcomes of active surveillance for localized prostate cancer CLAIRE HARDIE, CHRIS PARKER, ANDREW NORMAN*, ROS EELES,
Diagnosis and management of prostate cancer in the
 Diagnosis and management of prostate cancer in the Jeremy Teoh ( 張源津 ) Assistant Professor, Department of Surgery, The Chinese University of Hong Kong. Email: jeremyteoh@surgery.cuhk.edu.hk Estimated age-standardised
Diagnosis and management of prostate cancer in the Jeremy Teoh ( 張源津 ) Assistant Professor, Department of Surgery, The Chinese University of Hong Kong. Email: jeremyteoh@surgery.cuhk.edu.hk Estimated age-standardised
Overdiagnosis. Making people sick in the pursuit of health Drs Gilbert Welch, Lisa Schwartz, Steven Woloshin
 Overdiagnosis Making people sick in the pursuit of health Drs Gilbert Welch, Lisa Schwartz, Steven Woloshin Screening for prostate cancer «Screening for prostate cancer has become the poster child of overdiagnosis
Overdiagnosis Making people sick in the pursuit of health Drs Gilbert Welch, Lisa Schwartz, Steven Woloshin Screening for prostate cancer «Screening for prostate cancer has become the poster child of overdiagnosis
Adam Raben M.D. Helen F Graham Cancer Center
 Adam Raben M.D. Helen F Graham Cancer Center Is the biopsy sample representative of the extent of the disease in your patient with clinically low-risk prostate cancer? BIOPSY RP registry (n=8095) 3+3=6
Adam Raben M.D. Helen F Graham Cancer Center Is the biopsy sample representative of the extent of the disease in your patient with clinically low-risk prostate cancer? BIOPSY RP registry (n=8095) 3+3=6
Prostate MRI: Who needs it?
 Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
Providing Treatment Information for Prostate Cancer Patients
 Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
PROSTATE CANCER: HOW CAN SUCH A COMMON DISEASE BE SO CONTROVERSIAL
 PROSTATE CANCER: HOW CAN SUCH A COMMON DISEASE BE SO CONTROVERSIAL Shahrokh F. Shariat, MD Professor of Urology, Medical University of Vienna, Vienna, AUT Adjunct Professor of Urology and Medical Oncology,
PROSTATE CANCER: HOW CAN SUCH A COMMON DISEASE BE SO CONTROVERSIAL Shahrokh F. Shariat, MD Professor of Urology, Medical University of Vienna, Vienna, AUT Adjunct Professor of Urology and Medical Oncology,
Prostate cancer smart screening, precision diagnosis, personalised treatment'
 Prostate cancer smart screening, precision diagnosis, personalised treatment' Prof. Hashim Ahmed PhD, FRCS(Urol), BM, BCh (Oxon), BA(Hons) Consultant Urological Surgeon Bupa Cromwell Hospital Clinics:
Prostate cancer smart screening, precision diagnosis, personalised treatment' Prof. Hashim Ahmed PhD, FRCS(Urol), BM, BCh (Oxon), BA(Hons) Consultant Urological Surgeon Bupa Cromwell Hospital Clinics:
Predictive Models. Michael W. Kattan, Ph.D. Department of Quantitative Health Sciences and Glickman Urologic and Kidney Institute
 Predictive Models Michael W. Kattan, Ph.D. Department of Quantitative Health Sciences and Glickman Urologic and Kidney Institute Treatment for clinically localized prostate cancer Trade off: Substantial
Predictive Models Michael W. Kattan, Ph.D. Department of Quantitative Health Sciences and Glickman Urologic and Kidney Institute Treatment for clinically localized prostate cancer Trade off: Substantial
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA
 Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
Prostate Cancer. Axiom. Overdetection Is A Small Issue. Reducing Morbidity and Mortality
 Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
Anatomic Imaging of Prostate Cancer
 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute of Cancer Research Senior Scientist, Sunnybrook Research Institute Chief, Dept of Medical
Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute of Cancer Research Senior Scientist, Sunnybrook Research Institute Chief, Dept of Medical
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Prostate Cancer Active Surveillance: Rationale, Outcomes and Future Directions
 Prostate Cancer Active Surveillance: Rationale, Outcomes and Future Directions Daniel W. Lin, MD Professor and Chief of Urologic Oncology Bridges Endowed Professorship of Prostate Cancer Research Department
Prostate Cancer Active Surveillance: Rationale, Outcomes and Future Directions Daniel W. Lin, MD Professor and Chief of Urologic Oncology Bridges Endowed Professorship of Prostate Cancer Research Department
Prostate Cancer MRI. Accurate Diagnosis and Treatment. PSA to Prostate MRI. for patients and curious doctors
 6 Prostate Cancer MRI Accurate Diagnosis and Treatment PSA to Prostate MRI for patients and curious doctors Samuel Aronson, M.D. Vincent Pelsser, M.D. Franck Bladou, M.D. Armen Aprikian, M.D. & Marc Emberton,
6 Prostate Cancer MRI Accurate Diagnosis and Treatment PSA to Prostate MRI for patients and curious doctors Samuel Aronson, M.D. Vincent Pelsser, M.D. Franck Bladou, M.D. Armen Aprikian, M.D. & Marc Emberton,
MR-TRUS Fusion Biopsy
 MR-TRUS Fusion Biopsy Silvan Boxler Department of Urology Prostate cancer mortality according to risk groups Prevention of overdiagnosis and overtreatment Rider J, Eur Urol 2013 MR-TRUS Fusion Biopsy /
MR-TRUS Fusion Biopsy Silvan Boxler Department of Urology Prostate cancer mortality according to risk groups Prevention of overdiagnosis and overtreatment Rider J, Eur Urol 2013 MR-TRUS Fusion Biopsy /
PROSTATE CANCER SCREENING: AN UPDATE
 PROSTATE CANCER SCREENING: AN UPDATE William G. Nelson, M.D., Ph.D. Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins American Association for Cancer Research William G. Nelson, M.D., Ph.D. Disclosures
PROSTATE CANCER SCREENING: AN UPDATE William G. Nelson, M.D., Ph.D. Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins American Association for Cancer Research William G. Nelson, M.D., Ph.D. Disclosures
Active surveillance for prostate cancer: patient selection and management
 UROLOGIC ONCOLOGY Active surveillance for prostate cancer: patient selection and management L. Klotz md ABSTRACT Screening for prostate cancer using prostate-specific antigen (psa) has been appealing.
UROLOGIC ONCOLOGY Active surveillance for prostate cancer: patient selection and management L. Klotz md ABSTRACT Screening for prostate cancer using prostate-specific antigen (psa) has been appealing.
Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study
 Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study Luke Witherspoon MD MSc, Johnathan L. Lau BSc, Rodney H. Breau MD MSc, Christopher
Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study Luke Witherspoon MD MSc, Johnathan L. Lau BSc, Rodney H. Breau MD MSc, Christopher
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation. Roberto Alonzi Mount Vernon Cancer Centre
 The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
How to detect and investigate Prostate Cancer before TRT
 How to detect and investigate Prostate Cancer before TRT Frans M.J. Debruyne Professor of Urology Andros Men s Health Institutes, The Netherlands Bruges, 25-26 September 2014 PRISM Recommendations for
How to detect and investigate Prostate Cancer before TRT Frans M.J. Debruyne Professor of Urology Andros Men s Health Institutes, The Netherlands Bruges, 25-26 September 2014 PRISM Recommendations for
Introduction. American Society of Clinical Oncology All rights reserved.
 Active Surveillance for the Management of Localized Prostate Cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement This is an endorsement
Active Surveillance for the Management of Localized Prostate Cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement This is an endorsement
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
The role of PSA in detection and management of prostate cancer
 The role of PSA in detection and management of prostate cancer Kirby R. The role of PSA in detection and management of prostate cancer. Practitioner 2016; 260(1792):17-21 Professor Roger Kirby MA MD FRCS
The role of PSA in detection and management of prostate cancer Kirby R. The role of PSA in detection and management of prostate cancer. Practitioner 2016; 260(1792):17-21 Professor Roger Kirby MA MD FRCS
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017
 Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
AUA Update Series. Lesson 33 Volume Active Surveillance for Prostate Cancer: Patient Selection and Management
 AUA Update Series Lesson 33 Volume 27 2008 Active Surveillance for Prostate Cancer: Patient Selection and Management Learning Objective: At the conclusion of this continuing medical education activity,
AUA Update Series Lesson 33 Volume 27 2008 Active Surveillance for Prostate Cancer: Patient Selection and Management Learning Objective: At the conclusion of this continuing medical education activity,
Prostate Cancer Who needs active surveillance?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller Prostate Cancer Who needs active surveillance? Klinische und molekulare Charakterisierung des Hoch-Risiko-Prostatakarzinoms.
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller Prostate Cancer Who needs active surveillance? Klinische und molekulare Charakterisierung des Hoch-Risiko-Prostatakarzinoms.
Prostate Cancer Innovations in Surgical Strategies Update 2007!
 Prostate Cancer Innovations in Surgical Strategies Update 2007! Curtis A. Pettaway, M.D. Professor Department of Urology The University of Texas M. D. Anderson Cancer Center Radical Prostatectomy Pathologic
Prostate Cancer Innovations in Surgical Strategies Update 2007! Curtis A. Pettaway, M.D. Professor Department of Urology The University of Texas M. D. Anderson Cancer Center Radical Prostatectomy Pathologic
Cancer. Description. Section: Surgery Effective Date: October 15, 2016 Subsection: Original Policy Date: September 9, 2011 Subject:
 Subject: Saturation Biopsy for Diagnosis, Last Review Status/Date: September 2016 Page: 1 of 9 Saturation Biopsy for Diagnosis, Description Saturation biopsy of the prostate, in which more cores are obtained
Subject: Saturation Biopsy for Diagnosis, Last Review Status/Date: September 2016 Page: 1 of 9 Saturation Biopsy for Diagnosis, Description Saturation biopsy of the prostate, in which more cores are obtained
Utility of Prostate MRI. John R. Leyendecker, MD
 Utility of Prostate MRI John R. Leyendecker, MD Professor of Radiology and Urology Executive Vice Chair of Clinical Operations Section Head, Abdominal Imaging Wake Forest University School of Medicine;
Utility of Prostate MRI John R. Leyendecker, MD Professor of Radiology and Urology Executive Vice Chair of Clinical Operations Section Head, Abdominal Imaging Wake Forest University School of Medicine;
Mr Declan Cahill Consultant Urological Surgeon The Royal Marsden
 Diagnosing prostate cancer Mr Declan Cahill Consultant Urological Surgeon 2 Marsden GP Education Day 22 February 2016 Should I have a PSA test? Can I have a PSA test? prostatecanceruk.org 4 83% raised
Diagnosing prostate cancer Mr Declan Cahill Consultant Urological Surgeon 2 Marsden GP Education Day 22 February 2016 Should I have a PSA test? Can I have a PSA test? prostatecanceruk.org 4 83% raised
Dong Hoon Lee, Ha Bum Jung, Seung Hwan Lee, Koon Ho Rha, Young Deuk Choi, Sung Jun Hong, Seung Choul Yang and Byung Ha Chung *
 Jpn J Clin Oncol 2012;42(11)1079 1085 doi:10.1093/jjco/hys147 Advance Access Publication 17 September 2012 Comparison of Pathological Outcomes of Active Surveillance Candidates Who Underwent Radical Prostatectomy
Jpn J Clin Oncol 2012;42(11)1079 1085 doi:10.1093/jjco/hys147 Advance Access Publication 17 September 2012 Comparison of Pathological Outcomes of Active Surveillance Candidates Who Underwent Radical Prostatectomy
Disclosures. Prostate and Bladder Cancer: Jonathan E. Rosenberg, M.D. U.S. Cancer Statistics: Prostate Cancer Known Risk Factors
 Prostate and Bladder Cancer: 2012 Jonathan E. Rosenberg, M.D. Associate Attending Section Head, Non-Prostate Genitourinary Oncology Service Memorial Sloan-Kettering Cancer Center Disclosures Consulting
Prostate and Bladder Cancer: 2012 Jonathan E. Rosenberg, M.D. Associate Attending Section Head, Non-Prostate Genitourinary Oncology Service Memorial Sloan-Kettering Cancer Center Disclosures Consulting
PSA screening. To screen or not to screen, that s the question Walid Shahrour FRCSC, MDCM, BSc Assistant professor Northern Ontario School of Medicine
 PSA screening To screen or not to screen, that s the question Walid Shahrour FRCSC, MDCM, BSc Assistant professor Northern Ontario School of Medicine Conflict of Interest Declaration: Nothing to Disclose
PSA screening To screen or not to screen, that s the question Walid Shahrour FRCSC, MDCM, BSc Assistant professor Northern Ontario School of Medicine Conflict of Interest Declaration: Nothing to Disclose
Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement
 Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Objectives. Prostate Cancer Screening and Surgical Management
 Prostate Cancer Screening and Surgical Management Dr. Ken Jacobsohn Director, Minimally Invasive Urologic Surgery Assistant Professor, Department of Urology Medical College of Wisconsin Objectives Update
Prostate Cancer Screening and Surgical Management Dr. Ken Jacobsohn Director, Minimally Invasive Urologic Surgery Assistant Professor, Department of Urology Medical College of Wisconsin Objectives Update
Low risk. Objectives. Case-based question 1. Evidence-based utilization of imaging in prostate cancer
 Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
BPH with persistently elevated PSA 아주대학교김선일
 BPH with persistently elevated PSA 아주대학교김선일 PSA in BPH: present status AUA & EAU BPH guideline: PSA: recommended test AUA practice guideline committee. J Urol 2003;170:530 Madersbacher. Eur Urol 2004;46:547
BPH with persistently elevated PSA 아주대학교김선일 PSA in BPH: present status AUA & EAU BPH guideline: PSA: recommended test AUA practice guideline committee. J Urol 2003;170:530 Madersbacher. Eur Urol 2004;46:547
The Evolving Role of PSA for Prostate Cancer. The Evolving Role of PSA for Prostate Cancer: 10/30/2017
 The Evolving Role of PSA for Prostate Cancer Adele Marie Caruso, DNP, CRNP Adult Nurse Practitioner Perelman School of Medicine at the University of Pennsylvania November 4, 2017 The Evolving Role of PSA
The Evolving Role of PSA for Prostate Cancer Adele Marie Caruso, DNP, CRNP Adult Nurse Practitioner Perelman School of Medicine at the University of Pennsylvania November 4, 2017 The Evolving Role of PSA
Mr Jeremy Grummet, Urological Surgeon MBBS, MS, FRACS Foundation 49 Men s Health Symposium August 2015
 www.drjeremygrummet.com.au www.aua.com.au Mr Jeremy Grummet, Urological Surgeon MBBS, MS, FRACS Foundation 49 Men s Health Symposium August 2015 The dilemma Most men die with prostate cancer rather than
www.drjeremygrummet.com.au www.aua.com.au Mr Jeremy Grummet, Urological Surgeon MBBS, MS, FRACS Foundation 49 Men s Health Symposium August 2015 The dilemma Most men die with prostate cancer rather than
Yiannis Philippou 1, Hary Raja 2 and Vincent J. Gnanapragasam 2*
 Philippou et al. BMC Urology (2015) 15:52 DOI 10.1186/s12894-015-0049-y RESEARCH ARTICLE Open Access Active surveillance of prostate cancer: a questionnaire survey of urologists, clinical oncologists and
Philippou et al. BMC Urology (2015) 15:52 DOI 10.1186/s12894-015-0049-y RESEARCH ARTICLE Open Access Active surveillance of prostate cancer: a questionnaire survey of urologists, clinical oncologists and
Predictive role of free prostate specific antigen in a prospective active surveillance program (PRIAS)
") World J Urol (2015) 33:1735 1740 DOI 10.1007/s00345-015-1542-3 ORIGINAL ARTICLE Predictive role of free prostate specific antigen in a prospective active surveillance program (PRIAS) Hanna Vasarainen 1
World J Urol (2015) 33:1735 1740 DOI 10.1007/s00345-015-1542-3 ORIGINAL ARTICLE Predictive role of free prostate specific antigen in a prospective active surveillance program (PRIAS) Hanna Vasarainen 1
Prostate Cancer Screening. Eric Shreve, MD Bend Urology Associates
 Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
Estimating and comparing cancer progression risks under varying surveillance protocols: moving beyond the Tower of Babel
 Estimating and comparing cancer progression risks under varying surveillance protocols: moving beyond the Tower of Babel Jane Lange March 22, 2017 1 Acknowledgements Many thanks to the multiple project
Estimating and comparing cancer progression risks under varying surveillance protocols: moving beyond the Tower of Babel Jane Lange March 22, 2017 1 Acknowledgements Many thanks to the multiple project
Newer Aspects of Prostate Cancer Underwriting
 Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
Pathologists Perspective on Focal Therapy: The Role of Mapping Biopsies and Markers
 Pathologists Perspective on Focal Therapy: The Role of Mapping Biopsies and Markers M. Scott Lucia, MD Professor and Vice Chair of Anatomic Pathology Chief of Genitourinary and Renal Pathology Dept. of
Pathologists Perspective on Focal Therapy: The Role of Mapping Biopsies and Markers M. Scott Lucia, MD Professor and Vice Chair of Anatomic Pathology Chief of Genitourinary and Renal Pathology Dept. of