CURRENT STANDARD OF CARE OF LUNG CANCER. Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff
|
|
|
- Christian Stevenson
- 5 years ago
- Views:
Transcription
1 CURRENT STANDARD OF CARE OF LUNG CANCER Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff
2
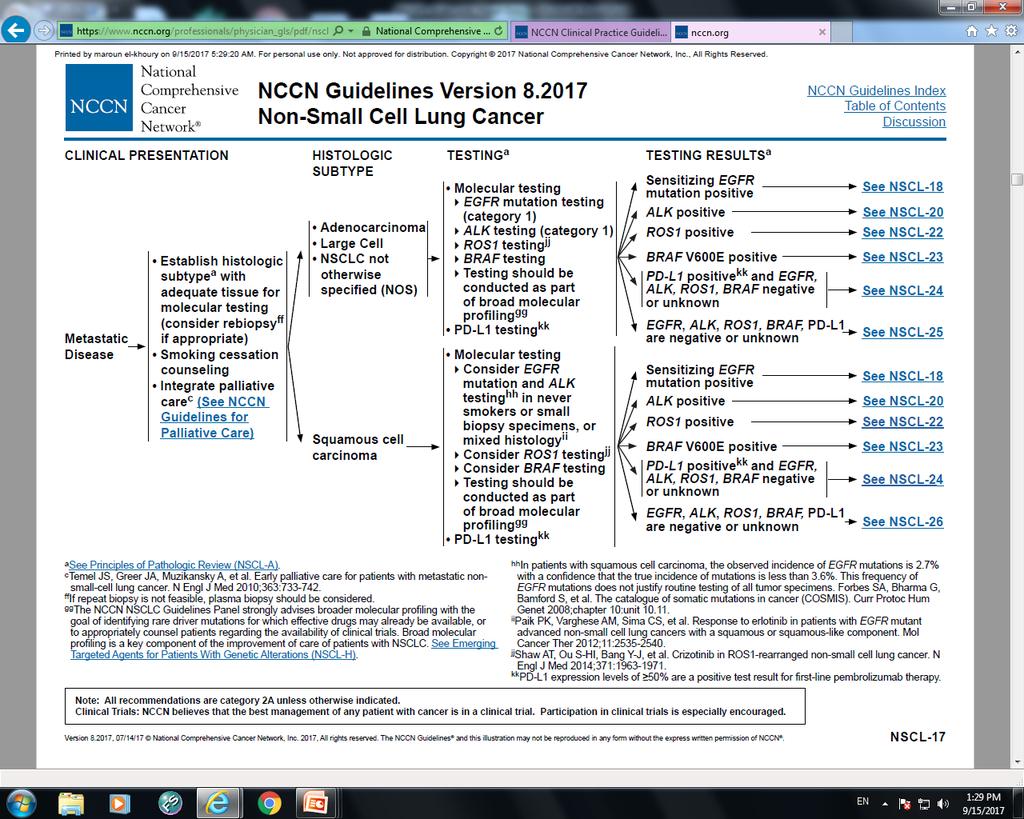
3 Biopsy: Establish Diagnosis, Determine Histologic Subtype, Molecular Testing Adequate tissue for histologic subtyping, molecular analysis critical Choice of site to biopsy (avoid bone if possible) Determination of EGFR mutation, ALK, and ROS1 translocations indicated in all nonsquamous cancers Determination of PD-L1 expression indicated in all NSCLC Rebiopsy at time of progression from targeted therapy Helps in determining resistance in EGFR-mutated and ALKpositive cases Liquid biopsy Masters GA, et al. J Clin Oncol. 2015;33: Novello S, et al. Ann Oncol. 2016;27:v1-v27.
4 Liquid Biopsy Potential Clinical Applications Alix-Panabieres C, Pantel K. Cancer Discov Screening and early detection of cancer EGFR mutations in ctdna CTC counts Stratification and therapeutic intervention Real time monitoring of therapy Therapeutic targets and resistance mechanisms Risk for metastatic relapse (prognosis)
5

6 Chemotherapy Targeted TKI Therapy Checkpoint Inhibitors Histologic subtype EGFR ALK ROS1 BRAF V600E Anti PD-1 Anti PD-L1 1970s - today 2000s - today today How do we optimize therapy in individual pts (ie, first line, second line, third line)?
7 EGFR Mutations: Context Found in 10% to 30% of NSCLC pts [1] More common in never-smokers, adenocarcinomas, females, Asians [1,2] Predominantly located in EGFR exons [2] ~ 85% of EGFR mutations are either deletions in exon 19 or a single-point mutation in exon 21 (L858R) [3] Specific EGFR mutation identified is important There are sensitive mutations, primary resistance mutations (often exon 20), and acquired resistance mutations (T790M) [3] 1. Pao W, et al. J Clin Oncol. 2005;23: Wu YL, et al. J Thorac Oncol. 2007;2: Gazdar AF. Oncogene. 2009;28:S24-S31.
8 Summary of EGFR Mutation Driven NSCLC EGFR sensitizing mutations predict higher response rate, PFS, and QoL if treated with EGFR TKI first line Several approved EGFR TKIs Specific EGFR mutation is important to know since some predict resistance to EGFR TKIs (eg. exon 20 insertions) Choice of specific EGFR TKI dependent on physician and patient preferences Upon progression, postprogression biopsy is important to establish the mechanism of resistance Liquid biopsy is an option Osimertinib approved for pts with EGFR T790M-positive disease (preferred treatment choice)
![Study Treatment N Median PFS, Mos ORR, % Median OS, Mos Maemondo [1] Mitsudomi [2,3 ] OPTIMAL [4,5] EURTAC [6] Gefitinib vs carboplatin/ paclitaxel Gefitinib vs cisplatin/docetaxel Erlotinib vs](/docs-images/83/88173754/images/9-1.jpg "carboplatin/gemcitabine Erlotinib vs platinum-based chemotherapy LUX-Lung Afatanib vs 3 [7,8] cisplatin/pemetrexed LUX-Lung Afatinib vs 6 [8,9] cisplatin/gemcitabine 230 172 165 173 345 364 10.8 vs 5.")
9 Study Treatment N Median PFS, Mos ORR, % Median OS, Mos Maemondo [1] Mitsudomi [2,3 ] OPTIMAL [4,5] EURTAC [6] Gefitinib vs carboplatin/ paclitaxel Gefitinib vs cisplatin/docetaxel Erlotinib vs carboplatin/gemcitabine Erlotinib vs platinum-based chemotherapy LUX-Lung Afatanib vs 3 [7,8] cisplatin/pemetrexed LUX-Lung Afatinib vs 6 [8,9] cisplatin/gemcitabine vs 5.4 (P <.001) 9.2 vs 6.3 (P <.0001) 13.1 vs 4.6 (P <.0001) 9.7 vs 5.2 (P <.0001) 11.1 vs 6.9 (P =.001) 11.0 vs 5.6 (P <.0001) 74 vs vs vs vs vs vs vs 23.6 (P =.31) 34.8 vs 37.3 (HR: 1.25) 22.8 vs 27.2 (HR: 1.19) 19.3 vs 19.5 (P =.87) 28.2 vs 28.2 (P =.39) 23.1 vs 23.5 (P =.61) 1. Maemondo M, et al. N Engl J Med. 2010;362: Mitsudomi T, et al. Lancet Oncol. 2010;11: Yoshioka H, et al. ASCO Abstract Zhou C, et al. Lancet Oncol. 2011;12: Zhou C, et al. Ann Oncol. 2015;26: Rosell R, et al. Lancet Oncol. 2012;13: Sequist LV, et al. J Clin Oncol. 2013;31: Yang JC, et al. Lancet Oncol. 2015;16: Wu YL, et al. Lancet Oncol. 2014;15:
10 Meta-analysis of Randomized First-line EGFR TKI Studies: Improved PFS Study EGFRmut (first-line therapy) EURTAC First-SIGNAL GTOWG INTACT1-2 IPASS LUX LUNG3 NEJ002 OPTIMAL TALENT TOPICAL TRIBUTE WJTOG3405 Subtotal HR (95% CI) 0.37 ( ) 0.54 ( ) 1.08 ( ) 0.55 ( ) 0.48 ( ) 0.58 ( ) 0.32 ( ) 0.16 ( ) 0.59 ( ) 0.90 ( ) 0.49 ( ) 0.52 ( ) 0.43 ( ) HR (95% CI) Favors EGFR TKI Favors Chemo Lee CK, et al. J Natl Cancer Inst. 2013;105:
11 Estimated OS Probability Estimated OS Probability LUX-Lung 3+6: OS by del(19) and L858R Mutation Status for Afatinib vs Chemo del(19) Afatinib (n = 236) Chemo (n = 119) L858R Afatinib (n = 183) Chemo (n = 93) 1.0 Median, mos HR (95% CI) 0.59 ( ) P = Median, mos HR (95% CI) 1.25 ( ) P = Mos Mos Yang JC, et al. Lancet Oncol. 2015;16:
12 Pts (%) LUX-Lung 7: PFS With First-line Afatinib vs Gefitinib in EGFR-Mutated NSCLC PFS significantly longer with afatinib vs gefitinib Afatinib (n = 160) Gefitinib (n = 159) Median PFS, Mos (95% CI) 11.0 ( ) 10.9 ( ) 12-Mo PFS *, % (95% CI) 47.4 ( ) 41.3 ( ) 24-Mo PFS *, % (95% CI) 17.6 ( ) 7.6 ( ) HR: 0.73 (95% CI: ; P =.017) *Estimated using exploratory Kaplan-Meier analyses Mos Park K, et al. Lancet Oncol. 2016;17:










13 Study or Subgroup T790M Total Percent Chen HJ, et al., % Kosaka T, et al., % Onitsuka T, et al., % Lung CA Oxnard, et al., % Total % Small Cell CA NSCL CA Squamous Cell Lung CA Non Squamous Cell Lung CA (Adeno, large cell) Wild PDL1 50% ALK Rearrangement ROS 1 EGFR mutation Other mutation T790m 50%
14 Phase I AURA Design AURA Ph I/II Patients with T790M-positive ansclc whose disease has progressed following either one prior therapy with an EGFR-TKI or following treatment with both EGFR-TKI and other anticancer therapy Rolling six design AURA2 Ph II Patients with confirmed EGFRm locally advanced or metastatic NSCLC who have progressed following prior therapy with an approved EGFR-TKI Escalation Cohort 1 20 mg Cohort 2 40 mg Negative Cohort 3 80 mg n=63 Negative Cohort mg Cohort mg Positive Positive Positive Positive Positive Negative Central T790M mutation testing* of biopsy sample collected following confirmed disease progression Expansion First-line Biopsy Tablet Cytology First-line Biopsy T790M positive T790M negative AURA Phase II Extension (n=201) Osimertinib 80 mg QD Pooled Phase II AURA2 (n=210) Osimertinib 80 mg QD Not eligible for enrollment AURA Ph I data cut-off 4 January, 2016; AURA pooled Ph II data cut-off 1 November, *The EGFR T790M mutation status of the patient s tumour was prospectively determined by the designated central laboratory using the cobas EGFR Mutation Test (Roche Molecular Systems) by biopsy taken after confirmation of disease progression on the most recent treatment regimen. Paired biopsy cohort patients with T790M positive tumours; safety and efficacy data only reported here. Data from cohorts in grayed out boxes are not included in the analyses reported here. Yang, ELCC 2016
15 Response Rates of EGFR T790M Positive Cohorts to Osimertinib D D*D* D DDD D D DD D DD 20 mg 40 mg 80 mg 160 mg 240 mg D DD D Best % Change From Baseline in Target Lesion D D DD DD DD D D D DD D D D DD DDD D D D D D DD D D DD D D D D D D D D *Imputed values for pts who died within 14 wks (98 days) of start of treatment and had no evaluable target lesion assessments. D Study discontinuation. T790M mutation determined by central test. n = mg 40 mg 80 mg 160 mg 240 mg Total n ORR, % (95% CI) 50 (19-81) DCR (CR, PR, or SD): 90% (95% CI: 84-94); activity in LM Jänne PA, et al. New Engl J Med. 2015;372: Jänne PA, et al. ELCC 2015; Abstract LBA3. Yang, J C-H, et al. ASCO Abstract (41-76) 66 (52-77) 51 (35-67) 54 (25-81) 59 (51-66)

16 Osimertinib in EGFR inhibitor resistant NSCLC RR 61% RR 21% Jänne, NEJM 2015
17 ALK-Driven Disease All nonsquamous NSCLC should be tested for ALK rearrangements Pts tend to develop brain metastases ALK rearrangements predict higher ORR and PFS if treated with ALK TKI first line Crizotinib and ceritinib are approved Alectinib demonstrated improved PFS and CNS activity over crizotinib as first-line therapy (ALEX) Alectinib, brigatinib, and ceritinib are approved for secondary refractory disease or intolerance to crizotinib Next-generation ALK inhibitors active in CNS disease Many ALK-positive pts may derive benefit from multiple sequential ALK inhibitors
18 PFS (%) PROFILE 1014: First-line Crizotinib vs Pemetrexed/Platinum* in Advanced NSCLC Phase III trial (N = 343) ALK-positive pts with nonsquamous NSCLC and no prior systemic treatment for advanced disease Crizotinib Crizotinib (n = 172) Chemotherapy (n = 171) Median PFS, mos HR (95% CI) 0.45 ( ) P value <.001 ORR, % P value < Pts at Risk, n Crizotinib CT Mos Chemotherapy *Carboplatin or cisplatin. Solomon BJ, et al. N Engl J Med. 2014;371:
19 Acquired Resistance in ALK+ NSCLC ALK+ NSCLC is sensitive to crizotinib [1-3 ] ORR: 60% Median PFS: 8-10 mos Most patients with develop resistance to crizotinib [4,5] Usually within 1-2 yrs CNS relapses are common [6] Mechanisms of resistance are diverse [4,5] ALK resistance mutations Alternative signaling pathways Unknown ALK amp ALK+ No ALK amp or mut Bypass tracks EGFR MT KRAS MT ALK mut 1. Camidge DR, et al. Lancet Oncol. 2012;13: Kim DW, et al. ESMO Abstract 1230PD. 3. Show AT, et al. ESMO Abstract LBA1_PR. 3. Katayama R, et al. Sci Trans Med. 2012;4:120ra Doebele RC, et al. Clin Cancer Res. 2012;18: Takeda M, et al. J Thorac Oncol. 2013; 8: Used with permission.
20 TKI Therapy In Pts With ALK+ NSCLC Inhibitors of ALK tyrosine kinase are active in pts with ALK+ NSCLC [1] ALK inhibitor crizotinib preferred therapy for advanced ALK+ NSCLC Phase III PROFILE 1014 study found crizotinib superior to standard first-line pemetrexed + platinum chemotherapy in this setting [2] Crizotinib arm, median PFS: 10.9 mos; ORR: 74% CNS is common initial progression site in ALK+ pts receiving crizotinib [3] Alectinib has demonstrated activity in crizotinib-refractory ALK+ NSCLC [4-6] Current phase III global study designed to compare alectinib vs crizotinib as first-line therapy for advanced ALK+ NSCLC [7] 1. Kwak EL, et al. N Engl J Med. 2010;363: Solomon BJ, et al. N Engl J Med. 2014;371: Yoshida T, et al. Lung Cancer. 2016;97: Ou SH, et al. J Clin Oncol. 2016;34: Shaw AT, et al. Lancet Oncol. 2016;17: Gadgeel SM, et al. J Clin Oncol. 2016;34: Peters S, et al. N Engl J Med. 2017;[Epub ahead of print].
21 Second-Generation ALK Inhibitors N Phase Prior Cri? ORR % Median PFS Ceritinib ASCEND-1 [1] ASCEND-2 [2] ASCEND-3 [3] Alectinib Shaw [4] Ou [5] I I II II II II Yes No Yes No Yes Yes Brigatinib [6] 222 II Yes Lorlatinib [7] 54 I/II Yes (40/41 pts) (90 mg QD) 54 (180 mg QD) (90 mg QD) NR (180 mg QD) Kim DW, et al. Lancet Oncol. 2016;17: Mok T, et al. ASCO Abstract Felip E, et al. ASCO Abstract Shaw AT, et al. Lancet Oncol. 2016;17: Ou SH, et al. J Clin Oncol. 2016;34: Kim DW, et al. ASCO Abstract Solomon BJ, et al. ASCO Abstract 9009.
22 Pts with advanced or metastatic ALK+ NSCLC, no previous systemic therapy for advanced disease, ECOG PS 0-2 (N = 303) Alectinib 600 mg BID PO (n = 152) Crizotinib 250 mg BID PO (n = 151) No crossover allowed Primary endpoint: PFS by investigator review Secondary endpoints: PFS by IRC, time to CNS progression, ORR, DoR, OS, safety Median duration of follow-up at time of analysis, alectinib: 18.6 mos (range: mos); crizotinib: 17.6 mos (range: mos) Peters S, et al. N Engl J Med. 2017;[Epub ahead of print].
23 PFS (%) n Crizotinib Alectinib 151 Investigator-Assessed PFS mos Mos Alectinib Median PFS Investigat orassessed, mos (95% CI) IRCassessed, mos (95% CI) Alectin ib (n = 152) NR (17.7- NR) 25.7 (19.9- NR) Shaw A, et al. ASCO Abstract LBA9008. Peters S, et al. N Engl J Med. 2017;[Epub ahead of print] NR Crizotinib Crizoti nib (n = 151) 11.1 ( ) 10.4 ( ) HR (95% CI) 0.47 ( ) 0.50 ( ) P Valu e <.001 <.001 Slide credit: clinicaloptions
24 J-ALEX: Efficacy Outcome Alectinib (n = 103) Crizotinib (n = 104) HR ( % CI); P Value ORR by Investigator (ITT population) ORR, % (95% CI) CR or PR, n 85.4 ( ) ( ) ORR a by IRF ORR, % (95% CI) CR or PR, n (n = 83) 91.6 ( ) 76 (n = 90) 78.9 ( ) a In pts with measurable disease at baseline by IRF. Alectinib showed consistent favorable treatment effect vs crizotinib for multiple prognostic factors Brain metastases: HR: 0.08 (95% CI: ) Nokihara H, et al. ASCO Abstract 9008.
25 Conclusions In pts with advanced or metastatic ALK+ NSCLC, first-line treatment with alectinib provided greater clinical benefit vs crizotinib Prolonged median PFS: HR 0.47 (95% CI: ; P <.0001) Delayed time to CNS progression Favorable toxicity Investigators conclude alectinib is the new first-line standard of care for pts with advanced ALK+ NSCLC Initial alectinib potentially superior to sequential crizotinib and alectinib based on large median PFS benefit Shaw A, et al. ASCO Abstract LBA9008.
26 ROS1 Fusion in Advanced NSCLC Most common in younger pts, never-smokers, adenocarcinoma, high-grade histology [1] Frequency: 1.2% to 1.7% overall [2] Several variants identified with different activation mechanisms; clinical significance unknown [3] FIG-, CD74-, SCL34A2-, TPM3-, SDC4-, EZR-, LRIG3, KDELR2-, and CCDC6- Testing: Vysis break apart FISH (> 15% cells with split signal in 50 nuclei scored) [4-6] ROS PCR, IHC Crizotinib active; FDA approved in March 2016 for ROS1-positive NSCLC [7] 1. Bergethon K, et al. J Clin Oncol. 2012;30: Davies KD, et al. Clin Cancer Res. 2012;18: Takeuchi K, et al. Nat Med. 2012;18: Gu TL, et al. PLoS One. 2011;6:e Birch AH, et al. PLoS One. 2011;6:e Lee J, et al. Cancer. 2013;119: Shaw AT, et al. ASCO Abstract 7508.
27 BRAF V600E Mutation in Advanced NSCLC Occurs predominantly in pts with adenocarcinoma, [1] both those with a history of smoking and neversmokers [2,3] Frequency: 1% to 2% overall [3] Testing: NGS (1 assay approved by FDA) Dabrafenib plus trametinib active; approved for BRAF V600E-positive metastatic (FDA [4] ) or advanced (EU [5] ) NSCLC 1. Chen D, et al. PLoS One. 2014;9:e Paik PK, et al. J Clin Oncol. 2011;29: Planchard D, et al. Lancet Oncol. 2016;17: Dabrafenib [package insert] EMA. Tafinlar product information
28
29 Advanced NSCLC (Molecular Biomarker Positive) EGFR mutation positive ALK positive ROS1 positive BRAF V600E positive PD-L1 positive First line Erlotinib, afatinib, or gefitinib Alectinib, ceritinib, or crizotinib Crizotinib Dabrafenib/ trametinib Pembrolizumab Progression EGFR T790M mutation positive Osimertinib EGFR T790M mutation negative Alectinib, brigatinib, or ceritinib dependent on previous therapy Second line and beyond Follow treatment options for adenocarcinoma or squamous cell carcinoma without actionable biomarker
30 Immune Checkpoint Inhibitors in Pretreated Advanced NSCLC: Randomized Late-StageTrials CheckMate 017 CheckMate 057 Squamous Stage IIIB/IV (N = 272) Nivolumab Docetaxel Nonsquamous Stage IIIB/IV (N = 582) Nivolumab Docetaxel Advanced NSCLC with 1% PD-L1+ tumor cells (N = 1034) KEYNOTE-010 Pembrolizumab (2 mg/kg) Pembrolizumab (10 mg/kg) Docetaxel Advanced NSCLC (2L/3L) (N = 1225) OAK Atezolizumab Docetaxel
31 OS (%) OS (%) CheckMate 017 and 057: Kaplan-Meier Estimates of OS CheckMate 017 (SQ NSCLC) CheckMate 057 (non-sq NSCLC) 100 Nivolumab (n=135) Docetaxel (n=137) Events, n (%) 110 (81) 128 (93) 100 Nivolumab (n=292) Docetaxel (n=290) Events, n (%) 228 (78) 247 (85) 80 Median OS, mo (95% CI) 9.2 (7.3, 12.6) 6.0 (5.1, 7.3) 80 Median OS, mo (95% CI) 12.2 (9.7, 15.1) 9.5 (8.1, 10.7) HR (95% CI) 0.62 (0.47, 0.80) HR (95% CI) 0.75 (0.63, 0.91) 60 Nivolumab 60 Nivolumab Δ18% 1-yr OS=24% 1-yr OS=42% Δ15% Docetaxel 2-yr OS=23% Δ12% 1-yr OS=39% Δ13% 1-yr OS=51% 2-yr OS=16% Docetaxel 2-yr OS=29% 2-yr OS=8% Time (Months) Time (Months) Based on February 2016 DBL. Symbols refer to censored observations. Minimum follow-up for survival: 24.2 months.borghaei H et al. Poster presentation at ASCO
32 OS (%) OS (%) KEYNOTE-010: Overall Survival at TPS 1% and TPS 50% 1% PD-L1 Expression vs 10 mg/kg: HR 1.17, 95% CI 0.94, Pembro 2 mg/kg 20 Pembro 10 mg/kg 10 Docetaxel Time (mos) 50% PD-L1 Expression vs 10 mg/kg: 80 HR 1.12, 95% CI 0.77, Pembro 2 mg/kg 20 Pembro 10 mg/kg 10 Docetaxel Time (mos) Treatment Arm Median (95% CI), mo Rate at 1 yr Pembro 2 mg/kg 10.4 (9.4, 11.9) 43.2% Pembro 10 mg/kg 12.7 (10.0, 17.3) 52.3% HR* (95% CI) P value 0.71 (0.58, 0.88) 0.61 (0.49, 0.75) < Docetaxel 8.5 ( ) 34.6% Treatment Arm Pembro 2 mg/kg Pembro 10 mg/kg Median (95% CI), mo 14.9 (10.4, NR) 17.3 (11.8, NR) HR* (95% CI) P value 0.54 (0.38, 0.77) 0.50 (0.36, 0.70) < Docetaxel 8.2 (6.4, 10.7) * Comparison of pembrolizumab vs docetaxel. Analysis cut-off date: September 30, Herbst RS et al. Oral presentation at ESMO Asia
 Median 13.8 mo (95% CI, 11.8, 15.")
33 Overall Survival (%) Overall survival, ITT (n = 850) HR, 0.73 a (95% CI, 0.62, 0.87) P = Minimum follow up = 19 months Atezolizum Docetaxel Median 9.6 mo (95% CI, 8.6, 11.2) Median 13.8 mo (95% CI, 11.8, 15.7) Months Barlesi et al, Atezolizumab Phase III OAK Study.
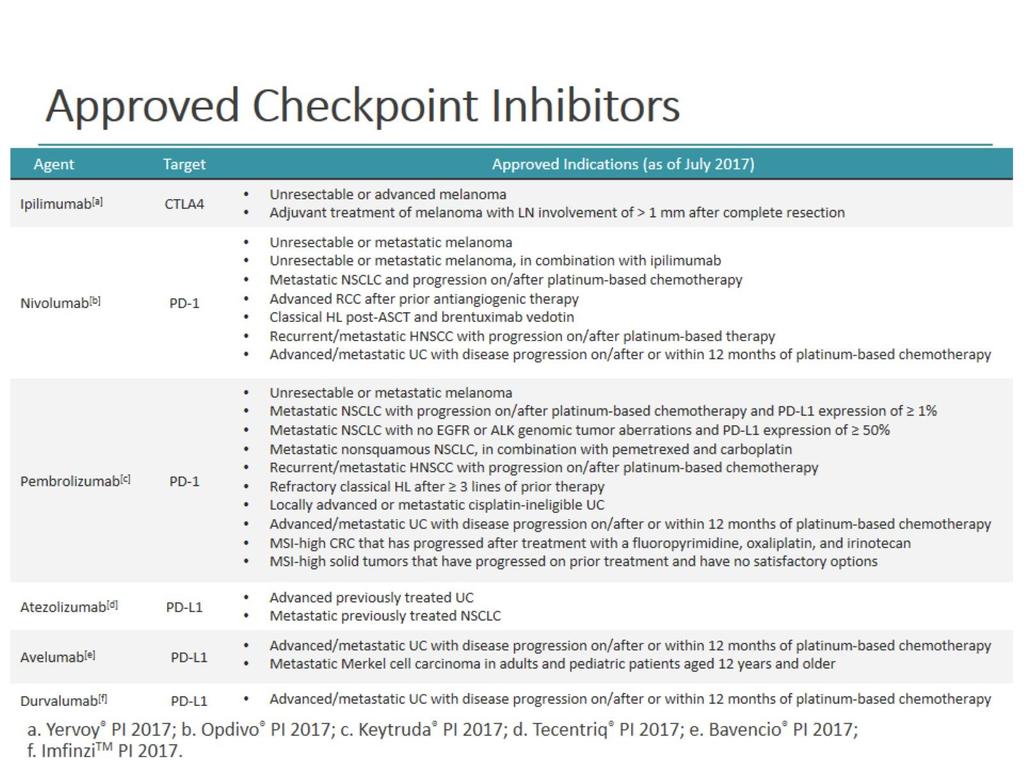
34 PD-L1 testing requirements with approved agents in 2l+ nsclc OPDIVO (Nivolumab) 1 KEYTRUDA (Pembrolizumab) 2 TECENTRIQ (Atezolizumab) US PI Metastatic non-small cell lung cancer and progression on or after platinum-based chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDAapproved therapy for these aberrations prior to receiving OPDIVO patients with metastatic NSCLC whose tumors express PD-L1 (TPS 1%) as determined by an FDA-approved test, with disease progression on or after platinum-containing chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving KEYTRUDA. Metastatic non-small cell lung cancer who have disease progression during or following platinum-containing chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA approved therapy for these aberrations prior to receiving TECENTRIQ Companion Diagnostic Not Required Required as per FDA approval. PD-L1 IHC 22C3 pharmdx diagnostic test by Dako Essential for safe and effective use of a drug Not Required 1. US Prescribing Information, Opdivo. October US Prescribing Information, Keytruda. October US Prescribing Information Tecentriq October
35
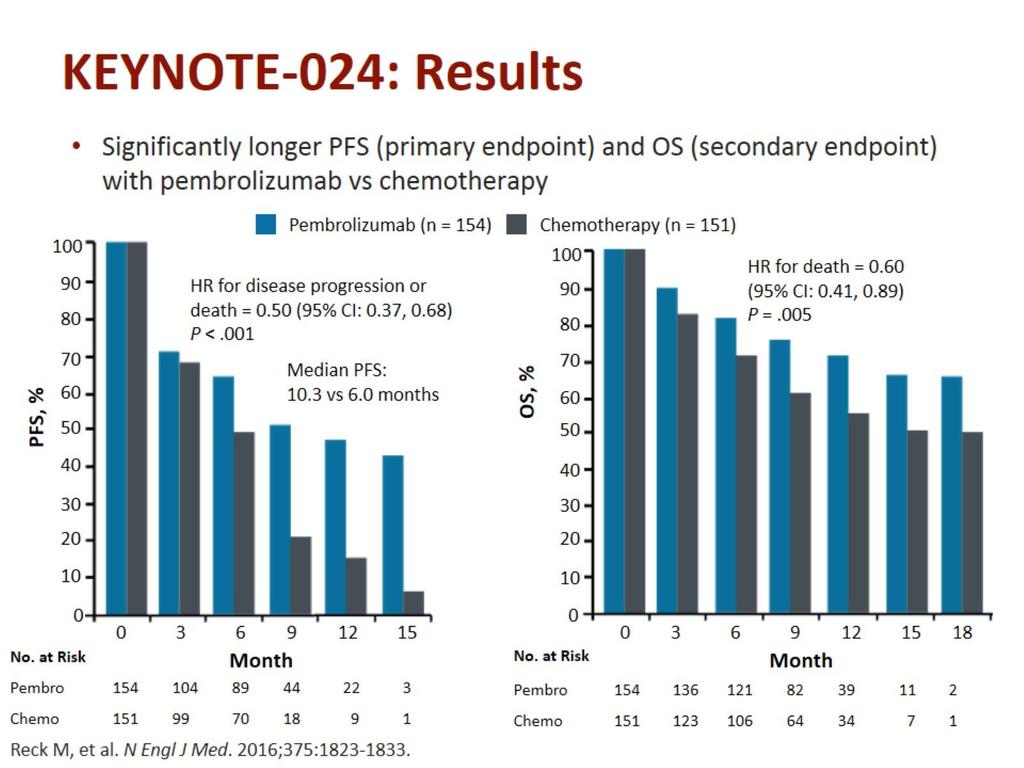
36 KEYNOTE-024: Study design A phase III, randomized, open-label study of pembrolizumab vs platinum-doublet chemotherapy as first-line therapy in patients with advanced or metastatic NSCLC that expresses PD-L1 in 50% of tumor cells N=305 Key Inclusion Criteria Advanced or metastatic, previously untreated NSCLC PD-L1+ tumor expression 50% No EGFR sensitizing mutation or ALK translocation ECOG PS 1 Primary endpoint: PFS Secondary endpoints: ORR, OS, safety, and tolerability R Pembrolizumab 200 mg Q3W Given until disease progression, intolerable toxicity, investigator decision, or completion of 35 cycles Optional crossover after disease progression Investigator choice of platinum-based chemotherapy For 4 6 cycles Pembrolizumab is currently not approved for 1L advanced/metastatic NSCLC. Investigator choice of chemotherapy included carboplatin AUC 5/6 IV Q3W or cisplatin 75 mg/m 2 IV Q3W plus pemetrexed 500 mg/m 2 IV Q3W or gemcitabine 1250 mg/m 2 IV Q3W or carboplatin AUC5/6 IV Q3W plus paclitaxel 200 mg/m 2 IV Q3W. Clinicaltrials.gov. NCT Accessed September 08, 2016.
37 Progression-Free Survival 50% PD-L1+ PFS, % % 50% Assessed per RECIST v1.1 by blinded, independent central review. Data cut-off: May 9, Events, n Median, mo HR P Pembro Chemo ( ) Time, months 48% 15% <0.001
38
39
40
41

42 Proposed treatment algorithm (no actionable biomarker) Good PS Clinical (PS) Poor PS Progressi on * Bevacizumab eligible Plt/pemetrexed (or other*) ± bevacizumab, carboplatin/pemetrexed + pembrolizumab Bevacizumab, pemetrexed, bevacizumab + pemetrexed, gemcitabine, pembrolizumab Histologic Nonsquamous Squamous Single-agent or combination chemotherapy Clinical Bevacizumab ineligible Platinum/pemetrexed (or other*), carboplatin/pemetrexed + pembrolizumab Pemetrexed, gemcitabine, or pembrolizumab Based on prior therapy: atezolizumab, nivolumab, pembrolizumab (if PD-L1+), or other systemic agents including docetaxel ± ramucirumab, pemetrexed, gemcitabine Platinum doublet* or cisplatin/gemcitabine/ necitumumab Docetaxel or gemcitabine Based on prior therapy Based on prior therapy: atezolizumab, nivolumab, pembrolizumab (if PD-L1+), or other systemic agents including docetaxel ± ramucirumab, gemcitabine, or possibly afatinib First line Maintenance Second line and beyond
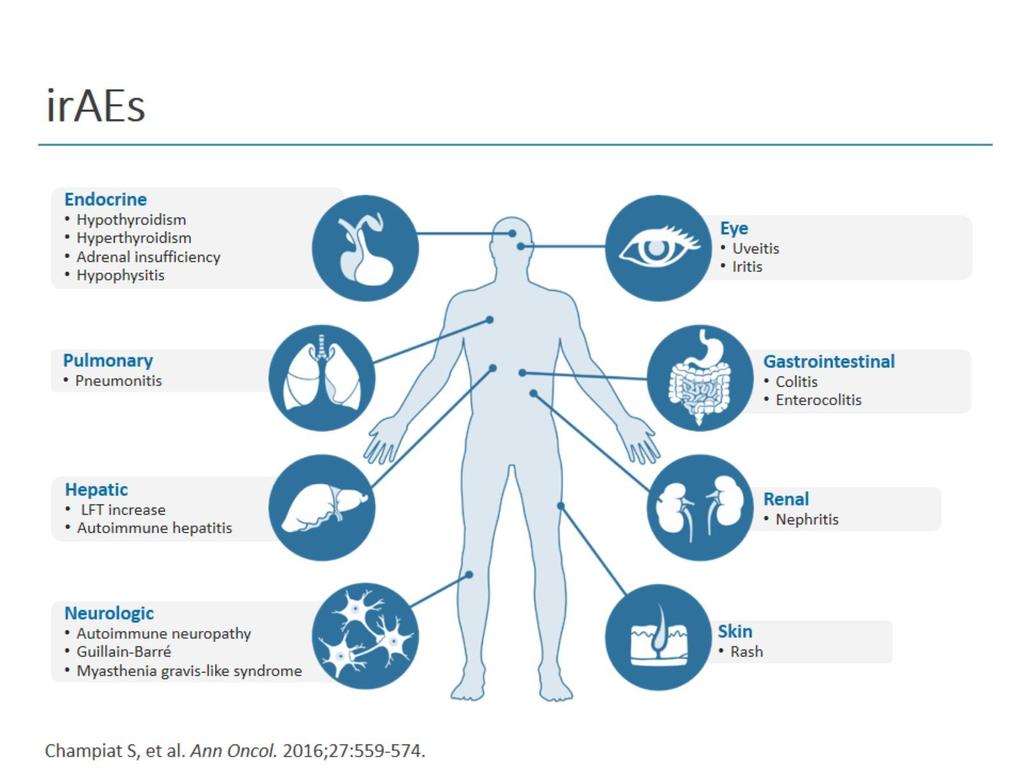
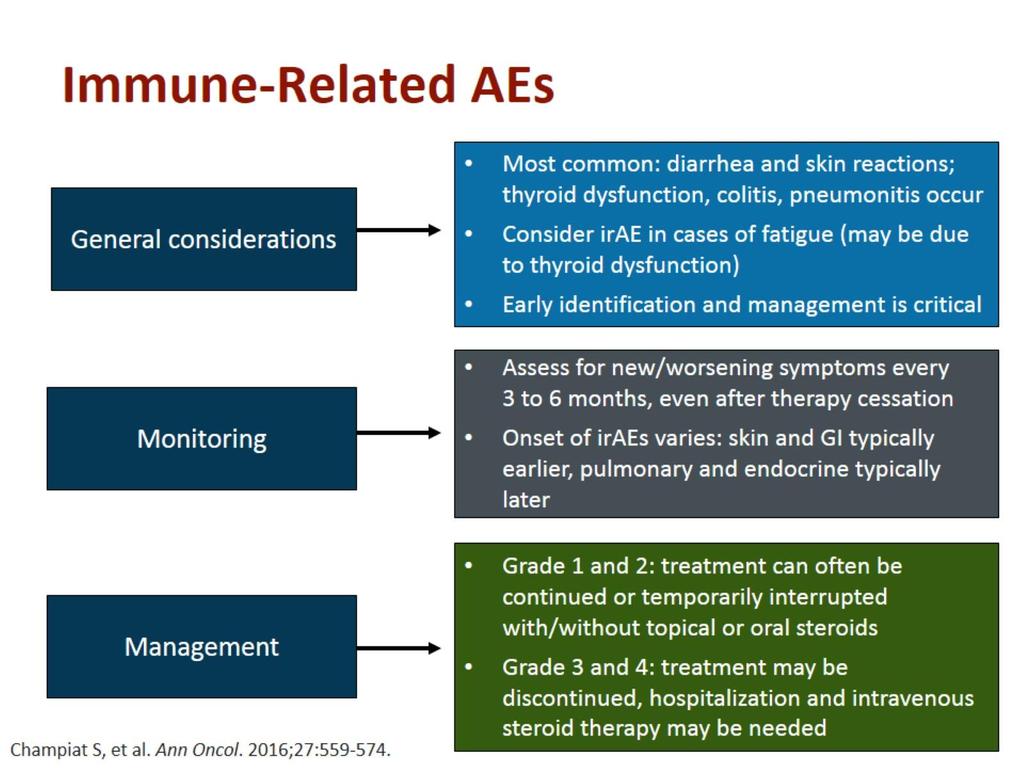
43 Conclusions Testing for actionable molecular mutations and PD-L1 expression is critical for all patients with newly-diagnosed advanced NSCLC Approved targeted therapies are available for EGFR mutations, ALK rearrangements, ROS1 rearrangements, and the BRAF V600E mutation PD-1/PD-L1 inhibitors have revolutionized advanced NSCLC care First-line: pembrolizumab is approved for high PD-L1 tumor expression ( 50%) and, for nonsquamous histology, in combination with carboplatin/pemetrexed Progressive disease: atezolizumab, nivolumab, and pembrolizumab ( 1% PD-L1) are approved Vigilance for immune-related AEs along with rapid intervention is key to optimal management


44 Survival Survival Where We Are Now Where We Want to Be? Time Time Control Targeted therapies Modified from Ribas A, et al. Clin Cancer Res. 2012;18: Immune checkpoint blockade Combinations/sequencing
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
INNOVATION IN LUNG CANCER MANAGEMENT. Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy
 INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
Molecular Targets in Lung Cancer
 Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Recent Advances in Lung Cancer: Updates from ASCO 2017
 Recent Advances in Lung Cancer: Updates from ASCO 2017 Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University of Pennsylvania 6/15/2017
Recent Advances in Lung Cancer: Updates from ASCO 2017 Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University of Pennsylvania 6/15/2017
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Targeted Therapy for NSCLC: EGFR and ALK Fadlo R. Khuri, MD
 EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC
EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
NSCLC: Terapia medica nella fase avanzata. Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza
 NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors
 Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors Conor E. Steuer, MD Assistant Professor The Winship Cancer Institute of Emory University July 27, 2017 1 Lung Cancer One
Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors Conor E. Steuer, MD Assistant Professor The Winship Cancer Institute of Emory University July 27, 2017 1 Lung Cancer One
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Sequencing in EGFR-Mutated NSCLC: Does Order Matter?
 Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont. Masterclass 27 september 2018
 Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont Masterclass 27 september 2018 Outline Introduction EGFR TKI ALK TKI TKI for uncommon driver mutations Take home messages The promise of
Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont Masterclass 27 september 2018 Outline Introduction EGFR TKI ALK TKI TKI for uncommon driver mutations Take home messages The promise of
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD
 State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
Targeted therapies for advanced non-small cell lung cancer. Tom Stinchcombe Duke Cancer Insitute
 Targeted therapies for advanced non-small cell lung cancer Tom Stinchcombe Duke Cancer Insitute Topics ALK rearranged NSCLC ROS1 rearranged NSCLC EGFR mutation: exon 19/exon 21 L858R and uncommon mutations
Targeted therapies for advanced non-small cell lung cancer Tom Stinchcombe Duke Cancer Insitute Topics ALK rearranged NSCLC ROS1 rearranged NSCLC EGFR mutation: exon 19/exon 21 L858R and uncommon mutations
Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS
 Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS Driver Mutations to Classify Lung Cancer Unknown 36% KRAS 25% EGFR 15% ALK 4% HER2 2% Double Mut 2% BRAF 2% PIK3CA
Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS Driver Mutations to Classify Lung Cancer Unknown 36% KRAS 25% EGFR 15% ALK 4% HER2 2% Double Mut 2% BRAF 2% PIK3CA
Targeted Therapies for Advanced NSCLC
 Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC. Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy
 PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016
 Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
EGFR Mutation-Positive Acquired Resistance: Dominance of T790M
 Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Personalized Treatment Approaches for Lung Cancer
 Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
OTRAS TERAPIAS BIOLÓGICAS EN CPNM: Selección y Secuencia Óptima del Tratamiento
 OTRAS TERAPIAS BIOLÓGICAS EN CPNM: Selección y Secuencia Óptima del Tratamiento Dolores Isla Servicio de Oncología Médica HCU Lozano Besa de Zaragoza 2008 Selection Factors in Advanced NSCLC ( 8y ago)
OTRAS TERAPIAS BIOLÓGICAS EN CPNM: Selección y Secuencia Óptima del Tratamiento Dolores Isla Servicio de Oncología Médica HCU Lozano Besa de Zaragoza 2008 Selection Factors in Advanced NSCLC ( 8y ago)
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Quale sequenza terapeutica nella malattia EGFR+
 Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Medical Treatment of Advanced Lung Cancer
 Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Joachim Aerts Erasmus MC Rotterdam, Netherlands. Drawing the map: molecular characterization of NSCLC
 Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Opzioni terapeutiche nel paziente ALK-traslocato
 Opzioni terapeutiche nel paziente ALK-traslocato Giulio Metro S.C. Oncologia Medica Ospedale Santa Maria della Misericordia, Azienda Ospedaliera di Perugia Carcinoma del polmone non microcitoma: quali
Opzioni terapeutiche nel paziente ALK-traslocato Giulio Metro S.C. Oncologia Medica Ospedale Santa Maria della Misericordia, Azienda Ospedaliera di Perugia Carcinoma del polmone non microcitoma: quali
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement. Reference Slides Introduction
 Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Improving outcomes for NSCLC patients with brain metastases
 Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Second-line treatment for advanced NSCLC
 UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Slide 1. Slide 2 Maintenance Therapy Options. Slide 3. Maintenance Therapy in the Management of Non-Small Cell Lung Cancer. Maintenance Chemotherapy
 Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Lung Cancer Update 2016 BAONS Oncology Care Update
 Lung Cancer Update 2016 BAONS Oncology Care Update Matthew Gubens, MD, MS Assistant Professor Chair, Thoracic Oncology Site Committee UCSF Helen Diller Family Comprehensive Cancer Center Disclosures Consulting
Lung Cancer Update 2016 BAONS Oncology Care Update Matthew Gubens, MD, MS Assistant Professor Chair, Thoracic Oncology Site Committee UCSF Helen Diller Family Comprehensive Cancer Center Disclosures Consulting
Optimum Sequencing of EGFR targeted therapy in NSCLC. Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey
 Optimum Sequencing of EGFR targeted therapy in NSCLC Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey Lung cancer NSCLC SCLC adeno squamous EGFR ALK ROS1 BRAF HER2 KRAS EGFR Transl Lung Cancer
Optimum Sequencing of EGFR targeted therapy in NSCLC Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey Lung cancer NSCLC SCLC adeno squamous EGFR ALK ROS1 BRAF HER2 KRAS EGFR Transl Lung Cancer
ALK positive Lung Cancer. Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan
 ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
Emerging Algorithm for Optimal Sequencing of EGFR TKIs in EGFR Mutation Positive NSCLC
 Emerging Algorithm for Optimal Sequencing of EGFR TKIs in EGFR Mutation Positive NSCLC Keunchil Park, MD, PhD Samsung Medical Center, Sungkyunkwan University School of Medicine Faculty Disclosure Consulting
Emerging Algorithm for Optimal Sequencing of EGFR TKIs in EGFR Mutation Positive NSCLC Keunchil Park, MD, PhD Samsung Medical Center, Sungkyunkwan University School of Medicine Faculty Disclosure Consulting
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
The Rapidly Changing World of EGFR Mutation-Positive Acquired Resistance
 The Rapidly Changing World of EGFR Mutation-Positive Acquired Resistance H. Jack West, MD Swedish Cancer Institute Seattle, WA GRACE Targeted Therapies Forum September 16, 2017 Cleveland, OH EGFR Mutation-Positive
The Rapidly Changing World of EGFR Mutation-Positive Acquired Resistance H. Jack West, MD Swedish Cancer Institute Seattle, WA GRACE Targeted Therapies Forum September 16, 2017 Cleveland, OH EGFR Mutation-Positive
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung
 Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
EGFR TKI sequencing: does order matter?
 EGFR TKI sequencing: does order matter? Nicolas Girard Thorax Institut Curie-Montsouris, Paris, France In Switzerland, afatinib is approved as monotherapy for patients with non-small cell lung cancer (Stage
EGFR TKI sequencing: does order matter? Nicolas Girard Thorax Institut Curie-Montsouris, Paris, France In Switzerland, afatinib is approved as monotherapy for patients with non-small cell lung cancer (Stage
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
NSCLC with squamous histology: Current treatment and new options on horizon
 NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
Cáncer de pulmón no microcítico
 DEFINIENDO LA SECUENCIA O PTIMA DE TRATAMIENTO EN CA NCER AVANZADO Cáncer de pulmón no microcítico Enriqueta Felip Hospital Vall d Hebron, Barcelona Molecular events in NSCLC Adenocarcinoma EGFR-resistance
DEFINIENDO LA SECUENCIA O PTIMA DE TRATAMIENTO EN CA NCER AVANZADO Cáncer de pulmón no microcítico Enriqueta Felip Hospital Vall d Hebron, Barcelona Molecular events in NSCLC Adenocarcinoma EGFR-resistance
Non-Small Cell Lung Cancer:
 Non-Small Cell Lung Cancer: Where We Are Today Sila Shalhoub, PharmD PGY2 Oncology Pharmacy Resident Shalhoub.Sila@mayo.edu Pharmacy Grand Rounds September 26, 2017 2017 MFMER slide-1 Objectives Identify
Non-Small Cell Lung Cancer: Where We Are Today Sila Shalhoub, PharmD PGY2 Oncology Pharmacy Resident Shalhoub.Sila@mayo.edu Pharmacy Grand Rounds September 26, 2017 2017 MFMER slide-1 Objectives Identify
Optimizing Outcomes in Advanced Non-Small Cell Lung Cancer: Integrating Novel Personalized Therapy into the Treatment Paradigm. Joel W.
 Optimizing Outcomes in Advanced Non-Small Cell Lung Cancer: Integrating Novel Personalized Therapy into the Treatment Paradigm Joel W. Neal, MD, PhD Assistant Professor of Medicine/Oncology Stanford University/Stanford
Optimizing Outcomes in Advanced Non-Small Cell Lung Cancer: Integrating Novel Personalized Therapy into the Treatment Paradigm Joel W. Neal, MD, PhD Assistant Professor of Medicine/Oncology Stanford University/Stanford
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER
 PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
Target therapy nel NSCLC con EGFR M+ Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy)
") Target therapy nel NSCLC con EGFR M+ Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy) cgridelli@libero.it First-Line Treatment of Advanced NSCLC EGFR-mutation analysis
Target therapy nel NSCLC con EGFR M+ Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy) cgridelli@libero.it First-Line Treatment of Advanced NSCLC EGFR-mutation analysis
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Cancer de Pulmón ALK+: Nueva generación de inhibidores. Incremento de supervivencia
 Cancer de Pulmón ALK+: Nueva generación de inhibidores. Incremento de supervivencia Carlos Camps Jefe Servicio Oncología Médica Hospital General Universitario Valencia Profesor Titular Medicina Lab Oncologia
Cancer de Pulmón ALK+: Nueva generación de inhibidores. Incremento de supervivencia Carlos Camps Jefe Servicio Oncología Médica Hospital General Universitario Valencia Profesor Titular Medicina Lab Oncologia
Next Generation EGFR Inhibitors
 Next Generation EGFR Inhibitors Tony Mok MD Li Shu Fan Medical Foundation Professor of Clinical Oncology Dept. of Clinical Oncology The Chinese University of Hong Kong EGFR TKIs First Generation -Gefitinib
Next Generation EGFR Inhibitors Tony Mok MD Li Shu Fan Medical Foundation Professor of Clinical Oncology Dept. of Clinical Oncology The Chinese University of Hong Kong EGFR TKIs First Generation -Gefitinib
PROGRESSION AFTER THIRD GENERATION TKI
 PROGRESSION AFTER THIRD GENERATION TKI What next? National Cancer Center Hospital Yuichiro Ohe, MD Name of lead presenter Yuichiro Ohe employee of company and/or profit-making organization adviser of company
PROGRESSION AFTER THIRD GENERATION TKI What next? National Cancer Center Hospital Yuichiro Ohe, MD Name of lead presenter Yuichiro Ohe employee of company and/or profit-making organization adviser of company
Making the first decision: EGFR mutation-positive NSCLC in the advanced setting
 ELCC May 217, Switzerland Making the first decision: EGFR mutation-positive NSCLC in the advanced setting Noemí Reguart, MD, PhD Hospital Clínic de Barcelona, Spain Disclosures Consultant or Advisory Role
ELCC May 217, Switzerland Making the first decision: EGFR mutation-positive NSCLC in the advanced setting Noemí Reguart, MD, PhD Hospital Clínic de Barcelona, Spain Disclosures Consultant or Advisory Role
1st line chemotherapy and contribution of targeted agents
 ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
Molecular Testing in Lung Cancer
 Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Hacia una mayor individualización clínica en el CPNM. J.M. Sánchez Torres H.U. Princesa, Madrid
 Hacia una mayor individualización clínica en el CPNM J.M. Sánchez Torres H.U. Princesa, Madrid Lung cancer histologic subtypes NSCLC (80-85%) SCLC (15-20%) Squamous carcinoma (25 30%) Non-squamous carcinoma
Hacia una mayor individualización clínica en el CPNM J.M. Sánchez Torres H.U. Princesa, Madrid Lung cancer histologic subtypes NSCLC (80-85%) SCLC (15-20%) Squamous carcinoma (25 30%) Non-squamous carcinoma
Beyond ALK and EGFR: Novel molecularly driven targeted therapies in NSCLC Federico Cappuzzo AUSL della Romagna, Ravenna, Italy
 Beyond ALK and EGFR: Novel molecularly driven targeted therapies in NSCLC Federico Cappuzzo AUSL della Romagna, Ravenna, Italy Oncogenic drivers in NSCLC Certain tumours arise as a result of aberrant activation
Beyond ALK and EGFR: Novel molecularly driven targeted therapies in NSCLC Federico Cappuzzo AUSL della Romagna, Ravenna, Italy Oncogenic drivers in NSCLC Certain tumours arise as a result of aberrant activation
Recent Advances in Lung Cancer: Updates from ASCO 2016
 Recent Advances in Lung Cancer: Updates from ASCO 2016 Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University of Pennsylvania 6/23/2016
Recent Advances in Lung Cancer: Updates from ASCO 2016 Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University of Pennsylvania 6/23/2016
Ludger Sellmann 1, Klaus Fenchel 2, Wolfram C. M. Dempke 3,4. Editorial
 Editorial Improved overall survival following tyrosine kinase inhibitor treatment in advanced or metastatic non-small-cell lung cancer the Holy Grail in cancer treatment? Ludger Sellmann 1, Klaus Fenchel
Editorial Improved overall survival following tyrosine kinase inhibitor treatment in advanced or metastatic non-small-cell lung cancer the Holy Grail in cancer treatment? Ludger Sellmann 1, Klaus Fenchel
Understanding Options: When Should TKIs be Considered?
 Advanced Stage Squamous NSCLC: Evolution and Increasing Complexity of the Therapeutic Landscape Understanding Options: When Should TKIs be Considered? David R. Gandara, MD University of California Davis
Advanced Stage Squamous NSCLC: Evolution and Increasing Complexity of the Therapeutic Landscape Understanding Options: When Should TKIs be Considered? David R. Gandara, MD University of California Davis
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007
 Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC
 1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
Is advanced lung cancer becoming a chronic disease?
 Is advanced lung cancer becoming a chronic disease? James Chung-Man HO ( 何重文 ) M.D. FRCP Associate Professor, The University of Hong Kong Honorary Consultant, Department of Medicine Specialist in Respiratory
Is advanced lung cancer becoming a chronic disease? James Chung-Man HO ( 何重文 ) M.D. FRCP Associate Professor, The University of Hong Kong Honorary Consultant, Department of Medicine Specialist in Respiratory
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Agenda. 6:30pm 7:00pm. Dinner. 7:00pm 7:15pm. NSCLC Treatment in 2014: Focus on Use of 2nd Generation TKIs in Clinical Practice.
 Agenda 6:30pm 7:00pm Dinner 7:00pm 7:15pm Welcome and Introductions Natasha Leighl, MD 7:15pm 7:50pm 7:50pm 8:00pm NSCLC Treatment in 2014: Focus on Use of 2nd Generation TKIs in Clinical Practice Questions
Agenda 6:30pm 7:00pm Dinner 7:00pm 7:15pm Welcome and Introductions Natasha Leighl, MD 7:15pm 7:50pm 7:50pm 8:00pm NSCLC Treatment in 2014: Focus on Use of 2nd Generation TKIs in Clinical Practice Questions
EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS
 EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS Federico Cappuzzo Istituto Clinico Humanitas IRCCS Rozzano-Italy The EGFR/HER Family Ligand binding domain
EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS Federico Cappuzzo Istituto Clinico Humanitas IRCCS Rozzano-Italy The EGFR/HER Family Ligand binding domain
Osimertinib as first-line treatment of EGFR mutant advanced nonsmall-cell
 Editorial Osimertinib as first-line treatment of EGFR mutant advanced nonsmall-cell lung cancer Chong-Kin Liam Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Editorial Osimertinib as first-line treatment of EGFR mutant advanced nonsmall-cell lung cancer Chong-Kin Liam Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Molecular Analysis for Targeted Therapy of Non-Small-Cell Lung Cancer Page 1 of 52 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Molecular Analysis for Targeted
Molecular Analysis for Targeted Therapy of Non-Small-Cell Lung Cancer Page 1 of 52 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Molecular Analysis for Targeted
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
14,30 18,20. II Sessione. Moderatori: Giovanni Apolone, Roberto Labianca
 14,30 18,20 II Sessione Moderatori: Giovanni Apolone, Roberto Labianca 15,10 15,30 Ca polmonare (never smokers): attualità e prospettive di ricerca Giulio Metro Ca polmonare (never smokers): attualità
14,30 18,20 II Sessione Moderatori: Giovanni Apolone, Roberto Labianca 15,10 15,30 Ca polmonare (never smokers): attualità e prospettive di ricerca Giulio Metro Ca polmonare (never smokers): attualità
ASCO Highlights and Controversies in advanced Lung Cancer. Torino, 11 giugno 2015
 ASCO 2015 Highlights and Controversies in advanced Lung Cancer Torino, 11 giugno 2015 Paolo Bironzo AOU S Luigi Gonzaga - Orbassano Scuola di Specializzazione in Oncologia Medica Università di Torino What
ASCO 2015 Highlights and Controversies in advanced Lung Cancer Torino, 11 giugno 2015 Paolo Bironzo AOU S Luigi Gonzaga - Orbassano Scuola di Specializzazione in Oncologia Medica Università di Torino What
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
ESMO 2017 CONGRESS September 2017 Madrid, Spain. Developed in association with the European Thoracic Oncology Platform
 Developed in association with the European Thoracic Oncology Platform ESMO 2017 CONGRESS Congress 8 12 September 2017 Madrid, Spain Supported by Eli Lilly and Company. Eli Lilly and Company has not influenced
Developed in association with the European Thoracic Oncology Platform ESMO 2017 CONGRESS Congress 8 12 September 2017 Madrid, Spain Supported by Eli Lilly and Company. Eli Lilly and Company has not influenced
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Lung Cancer. Karen Reckamp, MD Medical Director, Clinical Research. Click to edit Master Presentation Date
 Advances in Targeted Therapy for Lung Cancer Karen Reckamp, MD Medical Director, Clinical Research City of Hope Comprehensive Cancer Center Click to edit Master Presentation Date Disclosures Consultant
Advances in Targeted Therapy for Lung Cancer Karen Reckamp, MD Medical Director, Clinical Research City of Hope Comprehensive Cancer Center Click to edit Master Presentation Date Disclosures Consultant
Personalized Medicine for Advanced NSCLC in East Asia
 Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proteomic Testing for Systemic Therapy in Non-Small-Cell Lung Cancer Page 1 of 41 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proteomic Testing for Systemic
Proteomic Testing for Systemic Therapy in Non-Small-Cell Lung Cancer Page 1 of 41 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proteomic Testing for Systemic
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proteomic Testing for Systemic Therapy in Non-Small-Cell Lung Cancer Page 1 of 43 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proteomic Testing for Systemic
Proteomic Testing for Systemic Therapy in Non-Small-Cell Lung Cancer Page 1 of 43 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proteomic Testing for Systemic
Best of ASCO 2014: Highlights in Metastatic Non-Small Cell Lung Cancer
 Best of ASCO 2014: Highlights in Metastatic Non-Small Cell Lung Cancer Howard (Jack) West, M JackWestM@gmail.com @JackWestM Swedish Cancer Institute Seattle, WA Best of ASCO 2014 Seattle, WA Learning Objectives
Best of ASCO 2014: Highlights in Metastatic Non-Small Cell Lung Cancer Howard (Jack) West, M JackWestM@gmail.com @JackWestM Swedish Cancer Institute Seattle, WA Best of ASCO 2014 Seattle, WA Learning Objectives
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer
 Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Medical Policy. MP Proteomic Testing for Targeted Systemic in Non-Small-Cell Lung Cancer
 Medical Policy MP 2.04.125 Proteomic Testing for Targeted Systemic in Non-Small-Cell Lung Cancer BCBSA Ref. Policy: 2.04.125 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related
Medical Policy MP 2.04.125 Proteomic Testing for Targeted Systemic in Non-Small-Cell Lung Cancer BCBSA Ref. Policy: 2.04.125 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care
 Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
IMPORTANT PATHWAYS TO TARGET IN (ADVANCED) NSCLC:
 NSCLC:") IMPORTANT PATHWAYS TO TARGET IN (ADVANCED) NSCLC: A focus on EGFR-inhibition and implications for clinical practice Floriana Morgillo, MD PhD and Morena Fasano, MD PhD Faculty of Medicine, Università degli
IMPORTANT PATHWAYS TO TARGET IN (ADVANCED) NSCLC: A focus on EGFR-inhibition and implications for clinical practice Floriana Morgillo, MD PhD and Morena Fasano, MD PhD Faculty of Medicine, Università degli
Medical Policy. MP Molecular Analysis for Targeted Therapy of Non-Small-Cell Lung Cancer
 Medical Policy MP 2.04.45 BCBSA Ref. Policy: 2.04.45 Last Review: 10/30/2017 Effective Date: 10/30/2017 Section: Medicine Related Policies 2.04.115 Molecular Panel Testing of Cancers to Identify Targeted
Medical Policy MP 2.04.45 BCBSA Ref. Policy: 2.04.45 Last Review: 10/30/2017 Effective Date: 10/30/2017 Section: Medicine Related Policies 2.04.115 Molecular Panel Testing of Cancers to Identify Targeted