Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment
|
|
|
- Arthur McBride
- 5 years ago
- Views:
Transcription
1 Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment BHS Training course Timothy Devos
2 POLYCYTEMIA VERA
 microvascular disturbances: headaches, erythromelalgia hyperviscosity: dizziness, visual disturbances, headaches Landolfi et al.")
3 PV: clinical manifestations thrombosis (art > ven) facial plethora, pruritus (aquagenic) (40%), constitutional Σpt abdominal discomfort (splenomegaly) microvascular disturbances: headaches, erythromelalgia hyperviscosity: dizziness, visual disturbances, headaches Landolfi et al. Leukemia 2008
4 PV: complications thrombosis can be life-threatening risk factors (known): advanced age ( > 60 yr) history of thrombosis smoking and other cardiovascular risk factors risk factors (more recent): leukocytosis (Landolfi et al. Blood 2007) n = 1638 (ECLAP); followed for 2.7 yr; 205 thromboses in 169 patients multivariate analysis: WBC > 15000/µl significantly associated with vascular risk mainly a risk of myocardial infarction lack of correlation between platelet number and thrombosis!
5 PV: complications leukemic transformation (incidence 5-15% over 10 yr) development of PPV myelofibrosis (PPV-MF)
6 PV: complications risk factors (still under debate ): V617F JAK2 allele burden (Passamonti et al. Leukemia 2010) n = 338; prospective study allele burden > 50% significantly related to the risk of developing myelofibrosis (p=0.029) the risk of developing thrombosis or AML NOT significantly related to allele burden!
7 PV: risk stratification Low risk - age below 60 years - no history of trombosis - absence of cardiovascular risk factors (DM, smoking, cholesterol, AHT ao.) High risk - age 60 years or older - history of thrombosis
8 PV: management Low risk - flebotomy - low dose ASA ( mg/d if no contra indication) - manage CV risk factors aggressively High risk - flebotomy - low dose ASA ( mg if no C-I) - cytoreductive therapy (HU of IFNα) - manage CV risk factors aggressively target Hct < 0.45
 female patients on HU: avoid pregancies.")
9 PV: cytoreductive medication HYDROXUREA (HU): antimetabolite, DNA synthesis through inhibition of ribonucleoside reductase starting dose mg/kg/d target hct < 45 % (additional flebotomy if necessary) female patients on HU: avoid pregancies.

10 PV: cytoreductive medication HYDROXUREA (HU): side effects leukopenia en macrocytic anemia drug fever mucocutaneous ulcerations cutaneous leg ulcers hyperpigmentation skin and nails
11 PV: cytoreductive medication INTERFERON α (IFNα) Silver et al dose: 3 x U / week; PEG-IFN: 0.5 µg à 1.0/kg/week overall response: 50% reduction hct < 0,45 77% reduction spleen volume 75% reduction itching contra-indications thyroid or psychological disturbances side effects +++ 1/3 of the patients interrupts treatment indications IFNα selected patient groups young patients (< 40 yr) pregnancy untreatable pruritus hydroxurea intolerance
12 - other therapies - busulfan (> 65 yr) (chlorambucil) ( 32 P radiophosporus) (pipobroman)


13 PV and JAK inhibitors Vannucchi et al. EHA 2014.

14 Vannucchi et al. EHA 2014.
15 ESSENTIAL THROMBOCYTHEMIA
16 ET: clinical symptoms - mostly asymptomatic %: thrombosis (art > ven) - microcirculatory disturbances: headache, dizziness, distal paresthesias, acrocyanosis, erythromelalgia - bleedings (cave: BP > /µl) - itching (15 40 %)
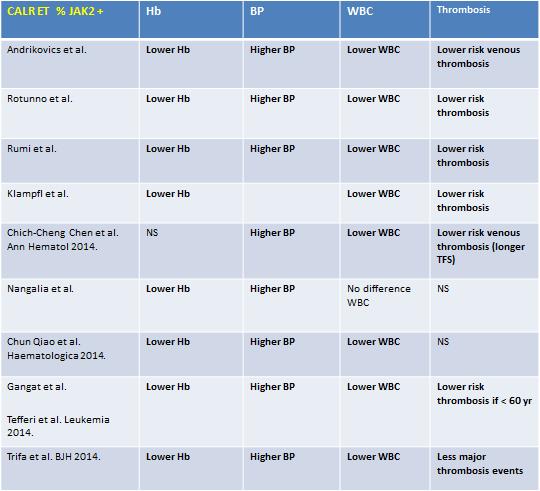
17 ET: risk factors for thrombosis known: age > 60 years history of thrombosis cardiovascular risk factors (important in high risk ET-patients: manage them aggressively!) presence of thrombophilic conditions (but: no reason to screen the patients!) novel markers / risk factors: leukocytosis MPL W515 mutation (rare in ET) no conclusive data JAK2 V617F higher thrombosis risk if JAK2 V617F + CALR lower thrombosis risk if CALR +
18
19 Passamonti et al. Best Practice and Research Clinical Hematology 2014.
20 ET: risk stratification Low risk Intermediate risk - younger < 60 yr - no history of thrombosis - BP < /µl - no clear cut definition (not low, not high) - operational definition : low risk patients with one or more of the following risk factors: CV disease, diabetes, smoking, hypertension, familial thrombophilia, ea. High risk - older > 60 yr - history of thrombo-embolic event(s) - BP > /µl
21 ET: management Low risk low dose ASA (if no contraindication) Intermediate risk low dose ASA treat C-V risk factors aggressively in some patients: BP reduction (decision on individual base) High risk low dose ASA reduce BP to < /µl treat C-V risk factors
22 IPSET thrombosis score Risk group numer risk factors (points) Thrombosis free survival (TFS) Low (41%) % (after 15 yr) Intermediate (47%) 2 first 10 yr as low risk; next 5 yr as high risk High (12%) % (after 7 yr) Risk factors: age > 60 yr: 1 point (< 60 yr: 0 points) CV risk factors: YES 1 point (no 0 points) history thrombo-embolic events : YES 2 points (no: 0 points) JAK2 V617F mutation: present 2 points (absent: 0 points) Barbui et al. Blood 2012
23 ET: cytoreductive medication HYDROXUREA IFN α reserved for young females or contra-indication for anagrelide ANAGRELIDE (Xagrid ) - inhibits cyclic AMP phosphodiesterase III - selective inhibitory effect on the megakaryocytic cell line - effective reduction of BP overall response (76-94%) Harrison et al. NEJM 2005
24 ET: cytoreductive medication ANAGRELIDE : side effects headache (13-35 %) palpitations / tachycardia (9-21 %) increasing cardiac insufficiency ANAGRELIDE : indications HU resistance HU intolerance HU contra-indication Birgegård G. Ann Hematol 2008
25 ET and pregnancy % ET patients succesfull pregnancy pregnancy loss during first trimester % estimation of risk: treatment: high risk: history of major thrombosis or bleeding, history of serious pregnancy complications, BP > /µl, hereditary thrombophilia factors Low risk - low dose ASA ( mg/d) - LMWH 4000 U/d after delivery until 6 weeks postpartum High risk - LMWH during the entire pregnancy (exception: (previous) bleeding complications!) - IFN-α if BP > /µl, previous bleeding complications
26 MYELOFIBROSIS
27 Prognostic score (IPSS PMF) Risk group number of risk factors median survival (years) Low 0 11,3 Intermediate 1 1 7,9 Intermediate High 3 2,3 Risk factors: age > 65 yr Hb < 10 g/dl WBC > 25000/µl peripheral blasts 1 % consitutional Σpt (weight loss > 10 %, night sweats, unexplained fever) Cervantes et al. Blood 2009
 3 additional (D)IPSS independent risk factors o red cell transfusion need o BP < 100000/µl o unfavorable karyotype: complex karyotype, trisomy 8, monosomy 7, 12p-, 11q23")
28 - prognostic scoring - Dynamic IPSS (DIPSS) (Passamonti, Blood 2010) same 5 prognostic variables as IPSS, but anemia = 2 points for use at any time during the disease course (not only at diagnosis) DIPSS-plus (Gangat JCO 2011) 3 additional (D)IPSS independent risk factors o red cell transfusion need o BP < /µl o unfavorable karyotype: complex karyotype, trisomy 8, monosomy 7, 12p-, 11q23 rearrangement, inv(3), -5/5q

29 - myelofibrosis: treatment - natural evolution of PMF: slowly, over several years if blast phase acceleration phase: very bad prognosis AML < PMF median survival 2.6 months (Mesa et al, Cancer 2006) risk-adapted therapy in myelofibrosis!
 T. Devos et al.")
30 Myelofibrosis: risk adjusted treatment 1) Curative treatment: allogeneic stem cell transplantation - intermediate-2 - high risk - blast-phase MF eligibility for Tx also based on: - age - co-morbidities - patient s preference blast-phase MF or fit patients < 45 yrs considered for MAC yr RIC (older patients sibling donor needed) T. Devos et al. Belg J Hematol 2013; 4: 127
 at 5 yr: 35-50% disease free survival (DFS) at 5 yr: 33 % if sibling donor, 27 % if MUD Ballen K, Blood Cancer Journal")
31 allogeneic stem cell transplantation (2) prognosis ~ transplantation risk transplant related mortality (TRM) at 1 yr: % overall survival (OS) at 5 yr: 35-50% disease free survival (DFS) at 5 yr: 33 % if sibling donor, 27 % if MUD Ballen K, Blood Cancer Journal 2012
32 Myelofibrosis: risk adjusted treatment 2) conventional therapies: supportive (not curative, no survival benefit) - hydroxurea non-lasting effect on splenomegaly and constitutional symptoms - transfusions - ESA: if low endogenous EPO levels (symptomatic anemia) - androgens or danazol: response rate 30% - lenalidomide: - first choice for (few) MF patients with isolated 5q - can be combined with prednisone - RR: anemia 22%, thrombocytopenia 50%, splenomegaly 33% - side effect: myelosuppression - thalidomide: - with or without tapering doses of prednisone - side effect: PNP - splenic irradiation non-lasting effect on splenomegaly and constitutional symptoms T. Devos et al. Belg J Hematol 2013; 4: 127

33 Splenectomy indications: drug refractory splenomegaly (> 10 cm below left costal margin) severe discomfort pain (+77%) symptomatic portal hypertension (+ 40%) complications: perioperative mortality 6% morbidity rate 27% short term: bleeding, thrombosis, infections long term: thrombocytosis (HU!), leukocytosis, hepatomegaly (20%) Mesa et al, Cancer 2006 Mesa et al, Blood 2009

34 JAK inhibitors
 15 or 20 mg oral BID n = 146 Best available")
 NEJM 2012 + courtesy")
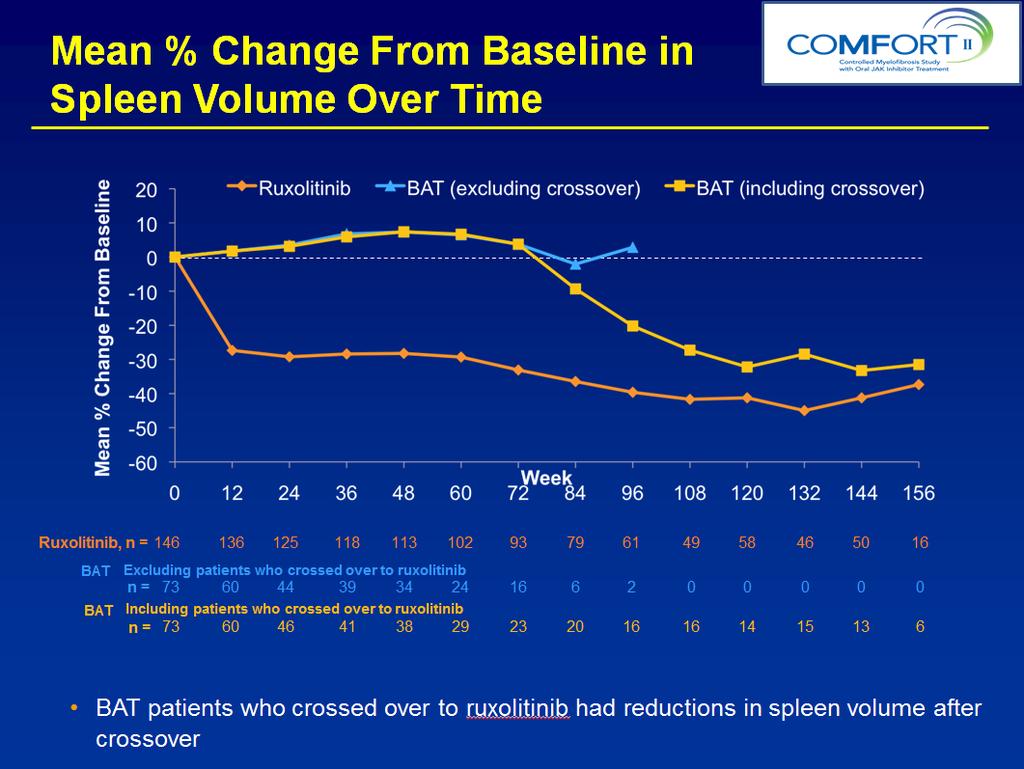
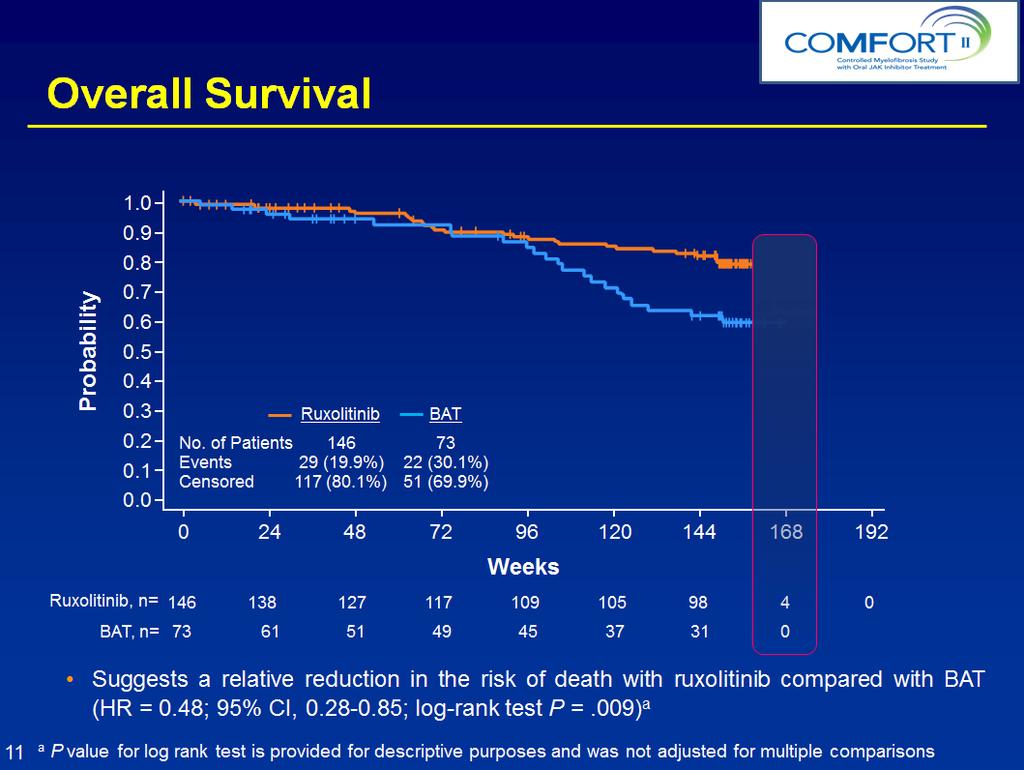
35 COMFORT-II Study Design Randomized, open-label, multicenter phase III trial Patients were stratified based on baseline IPSS risk category Patients with PMF, PPV-MF, or PET-MF with 2 IPSS risk factors 1 N = 219 Randomize 2:1 INC424 (ruxolitinib) 15 or 20 mg oral BID n = 146 Best available therapy (BAT) n = 73 Ruxolitinib Crossover and Extension Phase Progression events that qualified for the crossover and extension phase: Splenectomy Progressive splenomegaly as defined by a 25% increase in spleen volume compared with the on-study nadir (including baseline) NEJM courtesy Harrison C.
 at week 48 as measured by MRI (assessed at weeks 12, 24, 36, and 48) NEJM")
36 COMFORT-II Primary endpoint: Proportion of patients achieving 35% reduction in spleen volume from baseline (BL) at week 48 as measured by MRI (assessed at weeks 12, 24, 36, and 48) NEJM 2012
37 % With 35% spleen volume reduction Comfort II - primary endpoint Ruxolitinib P < % BAT % 0 Ruxolitinib Week 48 BAT Median time to response, weeks NEJM courtesy Harrison C.
38 Better Q of L and reduction of symptoms Worsening Improvement 9.5 Ruxolitinib (n = 69) BAT (n = 28) Mean change from baseline Appetite loss Insomnia Dyspnea Pain Fatigue Meaningful improvements were observed by week 8 and continued through week 48 NEJM courtesy Harrison C.
39
40 Anemia and Thrombocytopenia Worst Lab Value on Study Grade 1 n (%) Grade 2 n (%) Grade 3 n (%) Grade 4 n (%) Hemoglobin Ruxolitinib (n = 146) 24 (16) 55 (38) 50 (34) 12 (8) BAT (n = 70) 16 (23) 28 (40) 15 (21) 7 (10) Platelet count Ruxolitinib (n = 146) 46 (32) 41 (28) 9 (6) 3 (2) BAT (n = 69) 11 (16) 4 (6) 3 (4) 2 (3) The majority of patients (63% ruxolitinib; 67% BAT) had grade 1/2 anemia at baseline In both arms, all patients who entered the study had grade 0-1 thrombocytopenia at baseline manageable with RUX dose reductions or brief interruptions only 1 patient discontinued RUX < thrombopenia, none < anemia
41
42 How can we improve JAK-TKI results? combination trials with different targets: overcome the problem of resistance reduce adverse events of JAK-TKI reduce the clone/s PI3K/mTOR inhibitors HDAC inhibitors Smo inhibitors (LDE225)
43 Myelofibrosis treatment algorithm Odenike O Hematology 2013;2013:
44 THANK YOU FOR YOUR ATTENTION
Molecular aberrations in MPN. and use in the clinic. Timothy Devos MD PhD
 Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later
 Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later Vikas Gupta, MD, FRCP, FRCPath Associate Professor Department of Medicine Leukemia/BMT Programs Princess Margaret Cancer
Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later Vikas Gupta, MD, FRCP, FRCPath Associate Professor Department of Medicine Leukemia/BMT Programs Princess Margaret Cancer
MPNs: JAK2 inhibitors & beyond. Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt
 NCI, Cairo University, Egypt") MPNs: JAK2 inhibitors & beyond Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt Myeloproliferative Neoplasms (MPNs) AGENDA: 1. Molecular biology 2. New WHO diagnostic criteria. 3. Risk stratification
MPNs: JAK2 inhibitors & beyond Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt Myeloproliferative Neoplasms (MPNs) AGENDA: 1. Molecular biology 2. New WHO diagnostic criteria. 3. Risk stratification
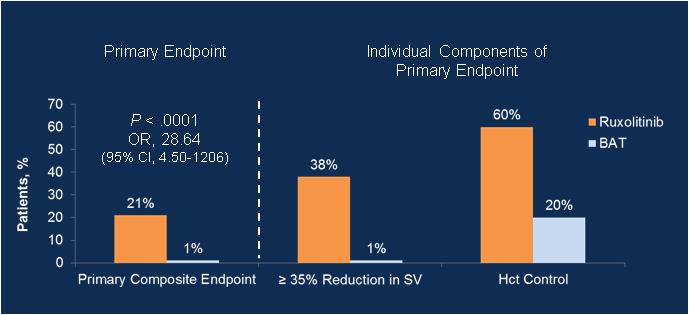
RESPONSE (NCT )
") Changes in Quality of Life and Disease-Related Symptoms in Patients With Polycythemia Vera Receiving Ruxolitinib or Best Available Therapy: RESPONSE Trial Results Abstract #709 Mesa R, Verstovsek S, Kiladjian
Changes in Quality of Life and Disease-Related Symptoms in Patients With Polycythemia Vera Receiving Ruxolitinib or Best Available Therapy: RESPONSE Trial Results Abstract #709 Mesa R, Verstovsek S, Kiladjian
How to monitor MPN patients
 How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis. Francesco Passamonti Università degli Studi dell Insubria, Varese
 Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis Francesco Passamonti Università degli Studi dell Insubria, Varese DIPSS during f-up IPSS at diagnosis Diagnose MF and genotype
Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis Francesco Passamonti Università degli Studi dell Insubria, Varese DIPSS during f-up IPSS at diagnosis Diagnose MF and genotype
Managing ET in Tiziano Barbui MD
 Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Current Prognostication in Primary Myelofibrosis
 Current Prognostication in Primary Myelofibrosis Francisco Cervantes Hematology Department, Hospital Clínic, Barcelona, Spain Florence, April 2011 Survival in PMF No. patients: 1,054 Median Srv (95% CI):
Current Prognostication in Primary Myelofibrosis Francisco Cervantes Hematology Department, Hospital Clínic, Barcelona, Spain Florence, April 2011 Survival in PMF No. patients: 1,054 Median Srv (95% CI):
JAKAFI (ruxolitinib phosphate) oral tablet
 oral tablet") JAKAFI (ruxolitinib phosphate) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
JAKAFI (ruxolitinib phosphate) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Post-ASH 2015 CML - MPN
 Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
MALATTIE MIELOPROLIFERATIVE CRONICHE
 MALATTIE MIELOPROLIFERATIVE CRONICHE Dott. Roberto Latagliata Policlinico Umberto I Università Sapienza, Roma Highlights from EHA 2017: some points to address today WHO 2016 MPN classification: hot topics
MALATTIE MIELOPROLIFERATIVE CRONICHE Dott. Roberto Latagliata Policlinico Umberto I Università Sapienza, Roma Highlights from EHA 2017: some points to address today WHO 2016 MPN classification: hot topics
London Cancer. Myelofibrosis guidelines. August Review August Version v1.0. Page 1 of 12
 London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
Evolving Management of Myelofibrosis
 Evolving Management of Myelofibrosis Srdan (Serge) Verstovsek M.D., Ph.D. Professor of Medicine Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Why do we prognosticate?
Evolving Management of Myelofibrosis Srdan (Serge) Verstovsek M.D., Ph.D. Professor of Medicine Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Why do we prognosticate?
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital
 By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
How I Treat Myelofibrosis. Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom
 How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update
 Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Jeanne Palmer, MD Mayo Clinic, Arizona
 Setting the stage for Transplant in MPN Jeanne Palmer, MD Mayo Clinic, Arizona What will be covered What is a bone marrow transplant? When to start thinking about bone marrow transplant Timing of transplant
Setting the stage for Transplant in MPN Jeanne Palmer, MD Mayo Clinic, Arizona What will be covered What is a bone marrow transplant? When to start thinking about bone marrow transplant Timing of transplant
CLINICAL POLICY DEPARTMENT: Medical Management DOCUMENT NAME: JakafiTM REFERENCE NUMBER: NH.PHAR.98
 PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
What is next: Emerging JAK2 inhibitor combination studies. Alessandro M. Vannucchi. Section of Hematology, University of Florence, Italy
 ymposium JAK2 Inhibition in Myelofibrosis: What Can We Expect in the Clinic? 4 5 May 2012 Lisbon, Portugal What is next: Emerging JAK2 inhibitor combination studies Alessandro M. Vannucchi ection of Hematology,
ymposium JAK2 Inhibition in Myelofibrosis: What Can We Expect in the Clinic? 4 5 May 2012 Lisbon, Portugal What is next: Emerging JAK2 inhibitor combination studies Alessandro M. Vannucchi ection of Hematology,
Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera
 Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera Alessandro M. Vannucchi, MD Laboratorio Congiunto MMPC Department of Experimental and Clinical Medicine University
Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera Alessandro M. Vannucchi, MD Laboratorio Congiunto MMPC Department of Experimental and Clinical Medicine University
Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology
 Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology Angela Fleischman MD PhD UC Irvine March 9, 2019 Disclosures: Angela Fleischman
Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology Angela Fleischman MD PhD UC Irvine March 9, 2019 Disclosures: Angela Fleischman
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Update in Myeloproliferative Neoplasms
 Update in Myeloproliferative Neoplasms 2018 UPDATE IN HEMATOLOGIC MALIGNANCIES January 26, 2018 Daria Babushok, MD PhD Learning Objectives Philadelphia-chromosome negative MPNs 1. To review key changes
Update in Myeloproliferative Neoplasms 2018 UPDATE IN HEMATOLOGIC MALIGNANCIES January 26, 2018 Daria Babushok, MD PhD Learning Objectives Philadelphia-chromosome negative MPNs 1. To review key changes
Ruben A. Mesa, MD & John Camoranio, MD Mayo Clinic
 Arizona, USA Prognosis & MPN Management in 2013 Ruben A. Mesa, MD & John Camoranio, MD Mayo Clinic Arizona, USA Understanding MPN Therapy Options Prognosis and Goals (Mesa & Camoriano) Evolving Rx ET (Vannucchi)
Arizona, USA Prognosis & MPN Management in 2013 Ruben A. Mesa, MD & John Camoranio, MD Mayo Clinic Arizona, USA Understanding MPN Therapy Options Prognosis and Goals (Mesa & Camoriano) Evolving Rx ET (Vannucchi)
JAK2 Inhibitors for Myeloproliferative Diseases
 JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
How I treat high risk myeloproliferative neoplasms. Francesco Passamonti Università dell Insubria Varese - Italy
 How I treat high risk myeloproliferative neoplasms Francesco Passamonti Università dell Insubria Varese - Italy How I treat high risk MF MF Treatment ELN 2018 Guidelines Anemia (Hb < 10 g/dl) Splenomegaly
How I treat high risk myeloproliferative neoplasms Francesco Passamonti Università dell Insubria Varese - Italy How I treat high risk MF MF Treatment ELN 2018 Guidelines Anemia (Hb < 10 g/dl) Splenomegaly
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
New Therapies for MPNs
 Pomalidomide and IMIDS in Myelofibrosis New Therapies for MPNs Fourth International Workshop on CML and MPN Natchez Louisiana Ruben A. Mesa, MD Professor of Medicine Mayo Clinic College of Medicine Director
Pomalidomide and IMIDS in Myelofibrosis New Therapies for MPNs Fourth International Workshop on CML and MPN Natchez Louisiana Ruben A. Mesa, MD Professor of Medicine Mayo Clinic College of Medicine Director
ASBMT MDS/MPN Update Sunil Abhyankar, MD
 ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
June Ruxolitinib for the second-line treatment of myelofibrosis (IPSS intermediate LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Ruxolitinib for the second-line treatment of myelofibrosis (IPSS intermediate risk-1 or above) Ruxolitinib for the second-line treatment of myelofibrosis (IPSS
LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Ruxolitinib for the second-line treatment of myelofibrosis (IPSS intermediate risk-1 or above) Ruxolitinib for the second-line treatment of myelofibrosis (IPSS
Latest updates in Myeloproliferative Neoplasms. Elizabeth Hexner, MD, MSTR
 Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
Chronic Myeloproliferative Disorders
 1 Chronic Myeloproliferative Disorders 15th 9 April2015 Polycythemia vera Essential thrombocythemia Idiopathic primary myelofibrosis 2 Learning objectives To appreciate types of polycythaemia (erythrocytosis)
1 Chronic Myeloproliferative Disorders 15th 9 April2015 Polycythemia vera Essential thrombocythemia Idiopathic primary myelofibrosis 2 Learning objectives To appreciate types of polycythaemia (erythrocytosis)
An Overview of US-Based MPN Guidelines: A First Look
 Northwestern University Feinberg School of Medicine An Overview of US-Based MPN Guidelines: A First Look Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology February
Northwestern University Feinberg School of Medicine An Overview of US-Based MPN Guidelines: A First Look Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology February
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES)
") Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES) Author: Dr N Butt, Consultant Haematologist On behalf of the Haematology CNG Written: July 2010 Reviewed:
Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES) Author: Dr N Butt, Consultant Haematologist On behalf of the Haematology CNG Written: July 2010 Reviewed:
Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]
![Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]](/thumbs/87/95709298.jpg "Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]") Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
OVERALL CLINICAL BENEFIT
 noted that there are case reports of a rebound effect upon discontinuation of ruxolitinib (Tefferi 2012), although this was not observed in either the COMFORT I or COMFORT II studies. Therefore, perc considered
noted that there are case reports of a rebound effect upon discontinuation of ruxolitinib (Tefferi 2012), although this was not observed in either the COMFORT I or COMFORT II studies. Therefore, perc considered
JAK inhibitors in Phmyeloproliferative
 Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Stifel Nicolaus 2013 Healthcare Conference. John Scarlett, M.D. Chief Executive Officer September 11, 2013
 Stifel Nicolaus 2013 Healthcare Conference John Scarlett, M.D. Chief Executive Officer September 11, 2013 1 forward-looking statements Except for the historical information contained herein, this presentation
Stifel Nicolaus 2013 Healthcare Conference John Scarlett, M.D. Chief Executive Officer September 11, 2013 1 forward-looking statements Except for the historical information contained herein, this presentation
Prognostic models in PV and ET
 Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms
 Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Intro alla patologia. Giovanni Barosi. Fondazione IRCCS Policlinico San Matteo Pavia
 Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
Transplants for MPD and MDS
 Transplants for MPD and MDS The question is really who to transplant, with what and when. Focus on myelofibrosis Jeff Szer Royal Melbourne Hospital Myelodysplasia Little needs to be said Despite new therapies
Transplants for MPD and MDS The question is really who to transplant, with what and when. Focus on myelofibrosis Jeff Szer Royal Melbourne Hospital Myelodysplasia Little needs to be said Despite new therapies
Polycythemia Vera: Aligning Real-World Practices With Current Best Practices
 Polycythemia Vera: Aligning Real-World Practices With Current Best Practices Overview Ruben A. Mesa, MD, provides practical insights into treating polycythemia vera. In addition to discussing risk stratification,
Polycythemia Vera: Aligning Real-World Practices With Current Best Practices Overview Ruben A. Mesa, MD, provides practical insights into treating polycythemia vera. In addition to discussing risk stratification,
Presenter Disclosure Information
 Welcome to Master Class for Oncologists Session 3: 2: PM 3:3 PM Pasadena, CA May 1, 21 Myeloproliferative Neoplasms 21 Speaker: Ayalew Tefferi Mayo Clinic, Rochester, MN Presenter Disclosure Information
Welcome to Master Class for Oncologists Session 3: 2: PM 3:3 PM Pasadena, CA May 1, 21 Myeloproliferative Neoplasms 21 Speaker: Ayalew Tefferi Mayo Clinic, Rochester, MN Presenter Disclosure Information
Evolving Guidelines of MPNs Where do new options fit in your treatment plan?
 Evolving Guidelines of MPNs Where do new options fit in your treatment plan? 34 th Chemotherapy Foundation Symposia Innovative Cancer Therapy for Tomorrow Ruben A. Mesa, MD, FACP Professor and Chair, Division
Evolving Guidelines of MPNs Where do new options fit in your treatment plan? 34 th Chemotherapy Foundation Symposia Innovative Cancer Therapy for Tomorrow Ruben A. Mesa, MD, FACP Professor and Chair, Division
Mielofibrosi: inquadramento dei fattori prognostici
 Mielofibrosi: inquadramento dei fattori prognostici Francesco Passamon, Division of Hematology University Hospital, Fondazione Macchi Varese, Italy Reduced survival in PMF and causes of death Median OS
Mielofibrosi: inquadramento dei fattori prognostici Francesco Passamon, Division of Hematology University Hospital, Fondazione Macchi Varese, Italy Reduced survival in PMF and causes of death Median OS
Hematopoietic Cell Transplantation for Myelofibrosis. Outline
 Hematopoietic Cell Transplantation for Myelofibrosis H.Joachim Deeg MD Fred Hutchinson Cancer Research Center & University of Washington, Seattle WA Great Debates, NY, 4/28/2012 Outline Rationale for hematopoietic
Hematopoietic Cell Transplantation for Myelofibrosis H.Joachim Deeg MD Fred Hutchinson Cancer Research Center & University of Washington, Seattle WA Great Debates, NY, 4/28/2012 Outline Rationale for hematopoietic
ASH 2013 Analyst & Investor Event
 ASH 2013 Analyst & Investor Event December 9, 2013 John A. Scarlett, MD President & CEO Forward-Looking Statements Except for the historical information contained herein, this presentation contains forward-looking
ASH 2013 Analyst & Investor Event December 9, 2013 John A. Scarlett, MD President & CEO Forward-Looking Statements Except for the historical information contained herein, this presentation contains forward-looking
Myeloproliferative Neoplasms and Myelofibrosis: Evolving Management
 Myeloproliferative Neoplasms and Myelofibrosis: Evolving Management Ruben A. Mesa, MD Mayo Clinic Cancer Center NCCN.org For Clinicians NCCN.org/patients For Patients Evolving Management of MPNs NCCN MPN
Myeloproliferative Neoplasms and Myelofibrosis: Evolving Management Ruben A. Mesa, MD Mayo Clinic Cancer Center NCCN.org For Clinicians NCCN.org/patients For Patients Evolving Management of MPNs NCCN MPN
OMF. Th. Sliwa 5th Med, Department for Hematology, Ocology an Palliative Care Hietzing Hospital, Vienna Austria
 OMF Th. Sliwa 5th Med, Department for Hematology, Ocology an Palliative Care Hietzing Hospital, Vienna Austria Th. Sliwa 2013 molecular biology Th. Sliwa 2013 Th. Sliwa 2013 Th. Sliwa 2013 Clinical Th.
OMF Th. Sliwa 5th Med, Department for Hematology, Ocology an Palliative Care Hietzing Hospital, Vienna Austria Th. Sliwa 2013 molecular biology Th. Sliwa 2013 Th. Sliwa 2013 Th. Sliwa 2013 Clinical Th.
Transplantation for Myeloproliferative neoplasms in the JAK inh era PARAMESWARAN HARI MEDICAL COLLEGE OF WISCONSIN MILWAUKEE
 Transplantation for Myeloproliferative neoplasms in the JAK inh era PARAMESWARAN HARI MEDICAL COLLEGE OF WISCONSIN MILWAUKEE Abbreviations: HCT, hematopoietic cell transplantation; MF, myelofibrosis; TRM,
Transplantation for Myeloproliferative neoplasms in the JAK inh era PARAMESWARAN HARI MEDICAL COLLEGE OF WISCONSIN MILWAUKEE Abbreviations: HCT, hematopoietic cell transplantation; MF, myelofibrosis; TRM,
HCT for Myelofibrosis
 Allogeneic HSCT for MDS and Myelofibrosis Sunil Abhyankar, MD Professor Medicine, Medical Director, Pheresis and Cell Processing University of Kansas Hospital BMT Program April 27 th, 213 HCT for Myelofibrosis
Allogeneic HSCT for MDS and Myelofibrosis Sunil Abhyankar, MD Professor Medicine, Medical Director, Pheresis and Cell Processing University of Kansas Hospital BMT Program April 27 th, 213 HCT for Myelofibrosis
Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations and Management
 Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms Judit Demeter CML chronic myeloid leukemia Semmelweis University, I st Department of Internal Medicine PV polycythaemia vera ET essential thrombocythaemia MF myelofibrosis
Myeloproliferative Neoplasms Judit Demeter CML chronic myeloid leukemia Semmelweis University, I st Department of Internal Medicine PV polycythaemia vera ET essential thrombocythaemia MF myelofibrosis
Myeloproliferative Neoplasms and Treatment Overview
 Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Leukemia. Roland B. Walter, MD PhD MS. Fred Hutchinson Cancer Research Center University of Washington
 Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Mayo Clinic, Scottsdale, AZ, USA; 14 MD Anderson Cancer Center, Houston, TX, USA.
 RESULTS OF THE PERSIST-2 PHASE 3 STUDY OF PACRITINIB (PAC) VERSUS BEST AVAILABLE THERAPY (BAT), INCLUDING RUXOLITINIB (RUX), IN PATIENTS WITH MYELOFIBROSIS (MF) AND PLATELET COUNTS 100,000/µL John Mascarenhas
RESULTS OF THE PERSIST-2 PHASE 3 STUDY OF PACRITINIB (PAC) VERSUS BEST AVAILABLE THERAPY (BAT), INCLUDING RUXOLITINIB (RUX), IN PATIENTS WITH MYELOFIBROSIS (MF) AND PLATELET COUNTS 100,000/µL John Mascarenhas
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Evidence Review Group Report Ruxolitinib for the treatment of myelofibrosis Erratum
 Amended paragraphs Page 13 Evidence Review Group Report Ruxolitinib for the treatment of myelofibrosis Erratum Whilst the evidence from the two good quality RCTs demonstrates that ruxolitinib is more effective
Amended paragraphs Page 13 Evidence Review Group Report Ruxolitinib for the treatment of myelofibrosis Erratum Whilst the evidence from the two good quality RCTs demonstrates that ruxolitinib is more effective
Disclosures for Angela Fleischman
 Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management
 AJH CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management Author: Ayalew Tefferi If you wish to receive credit for this activity,
AJH CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management Author: Ayalew Tefferi If you wish to receive credit for this activity,
Chi sono i candidati agli inibitori di JAK2
 Chi sono i candidati agli inibitori di JAK2 Francesco Passamon, Hematology, University Hospital Varese, Italy Ruxoli8nib (US approved in MF; EAP study and compassionate use in Italy) SAR302503 (phase 3
Chi sono i candidati agli inibitori di JAK2 Francesco Passamon, Hematology, University Hospital Varese, Italy Ruxoli8nib (US approved in MF; EAP study and compassionate use in Italy) SAR302503 (phase 3
Myeloproliferative Neoplasms (MPNs): Diagnosis, Treatment and Side Effects Management. Transcript. Slide Name & Number
: Diagnosis, Treatment and Side Effects Management. Transcript. Slide Name & Number") Question 1) The major mutation responsible for activating myeloproliferative neoplasms is: a) JAK 2 b) BCR-ABL c) P53 d) BRCA1 2) Risk stratification in myelofibrosis includes: a) Age b) Constitutional
Question 1) The major mutation responsible for activating myeloproliferative neoplasms is: a) JAK 2 b) BCR-ABL c) P53 d) BRCA1 2) Risk stratification in myelofibrosis includes: a) Age b) Constitutional
Opinion 9 January 2013
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 9 January 2013 JAKAVI 5 mg, tablet Bottle of 60 tablets (CIP code : 2246225) JAKAVI 15 mg, tablet Bottle of 60 tablets
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 9 January 2013 JAKAVI 5 mg, tablet Bottle of 60 tablets (CIP code : 2246225) JAKAVI 15 mg, tablet Bottle of 60 tablets
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Single Technology Appraisal (STA) Ruxolitinib for the treatment of myelofibrosis
 Ruxolitinib for the treatment of myelofibrosis") Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Preliminary Results From a Phase I Dose Escalation Trial of Ruxolitinib and the PI3Kδ Inhibitor TGR-1202 in Myelofibrosis
 Preliminary Results From a Phase I Dose Escalation Trial of Ruxolitinib and the PI3Kδ Inhibitor TGR-1202 in Myelofibrosis Tamara K. Moyo, Andrew Sochacki, Gregory D. Ayers, Michael T. Byrne, Stephen A.
Preliminary Results From a Phase I Dose Escalation Trial of Ruxolitinib and the PI3Kδ Inhibitor TGR-1202 in Myelofibrosis Tamara K. Moyo, Andrew Sochacki, Gregory D. Ayers, Michael T. Byrne, Stephen A.
HSCT for Myeloproliferative Disorders. Jane Apperley
 HSCT for Myeloproliferative Disorders Jane Apperley Myeloproliferative disorders CML Polycythemia vera Essential thrombocythemia Primary myelofibrosis bcr-abl + bcr-abl - JAK2 (valine to phenylalanin an
HSCT for Myeloproliferative Disorders Jane Apperley Myeloproliferative disorders CML Polycythemia vera Essential thrombocythemia Primary myelofibrosis bcr-abl + bcr-abl - JAK2 (valine to phenylalanin an
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes A critical reappraisal of anagrelide in the management of ET
 European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Unmet Medical Needs in Myelofibrosis
 Unmet Medical Needs in Myelofibrosis October 17, 2018 Safe Harbor Statement Except for statements of historical fact, any information contained in this presentation may be a forward-looking statement that
Unmet Medical Needs in Myelofibrosis October 17, 2018 Safe Harbor Statement Except for statements of historical fact, any information contained in this presentation may be a forward-looking statement that
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016
 for Polycythemia Vera March 3, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
J Clin Oncol 29: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 29 NUMBER 4 FEBRUARY 1 11 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T DIPSS Plus: A Refined Dynamic International Prognostic Scoring System for Primary Myelofibrosis That Incorporates
VOLUME 29 NUMBER 4 FEBRUARY 1 11 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T DIPSS Plus: A Refined Dynamic International Prognostic Scoring System for Primary Myelofibrosis That Incorporates
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
The Evolving Role of Transplantation for MPN
 The Evolving Role of Transplantation for MPN (PMF, PV, ET) H.Joachim Deeg MD Fred Hutchinson Cancer Research Center, University of Washington, Seattle WA, SCCA jdeeg@fhcrc.org 10 th J. Niblack Conference
The Evolving Role of Transplantation for MPN (PMF, PV, ET) H.Joachim Deeg MD Fred Hutchinson Cancer Research Center, University of Washington, Seattle WA, SCCA jdeeg@fhcrc.org 10 th J. Niblack Conference
Biologia molecolare delle malattie mieloproliferative croniche Ph1-negative tipiche
 41 CONGRESSO NAZIONALE SIE Bologna 14-17 Ottobre 2007 Biologia molecolare delle malattie mieloproliferative croniche Ph1-negative tipiche Alessandro M. Vannucchi Dip.. di Ematologia, Università degli Studi
41 CONGRESSO NAZIONALE SIE Bologna 14-17 Ottobre 2007 Biologia molecolare delle malattie mieloproliferative croniche Ph1-negative tipiche Alessandro M. Vannucchi Dip.. di Ematologia, Università degli Studi
Volume 28, Issue 4 Fall 2018 eissn:
 Volume 28, Issue 4 Fall 2018 eissn: 2368-8076 Myeloproliferative neoplasms (MPNs) Part 1: An overview of the diagnosis and treatment of the classical MPNs by Sabrina Fowlkes, Cindy Murray, Adrienne Fulford,
Volume 28, Issue 4 Fall 2018 eissn: 2368-8076 Myeloproliferative neoplasms (MPNs) Part 1: An overview of the diagnosis and treatment of the classical MPNs by Sabrina Fowlkes, Cindy Murray, Adrienne Fulford,
Inibitori di JAK2 e trapianto nella mielofibrosi
 III SESSIONE: MIELOFIBROSI E COMPLICANZE: Inibitori di JAK2 e trapianto nella mielofibrosi Francesca Patriarca Università di Udine RECOMMENDATIONS FOR ALLO-TRANSPLANT IN MYELOFIBROSIS prognosis of the
III SESSIONE: MIELOFIBROSI E COMPLICANZE: Inibitori di JAK2 e trapianto nella mielofibrosi Francesca Patriarca Università di Udine RECOMMENDATIONS FOR ALLO-TRANSPLANT IN MYELOFIBROSIS prognosis of the
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Should Mutation Status in PMF Guide Therapy? No! Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology
 Should Mutation Status in PMF Guide Therapy? No! Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology Case presentation A 67 yo woman presents to transition care, as her
Should Mutation Status in PMF Guide Therapy? No! Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology Case presentation A 67 yo woman presents to transition care, as her
Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012
 Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012 Outline Case presentation Overview of PV Disease course Mechanisms of thrombosis Case Presentation
Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012 Outline Case presentation Overview of PV Disease course Mechanisms of thrombosis Case Presentation
ASCO 2011: Leukemia. Disclosures
 ASCO 2011: Leukemia E.J. Feldman M.D Weill-Cornell Medical College Disclosures Speaker does not report any affiliations 1 V617F JAK2 mutation in MPDs JAK STAT PATHWAY Signal transducers and activators
ASCO 2011: Leukemia E.J. Feldman M.D Weill-Cornell Medical College Disclosures Speaker does not report any affiliations 1 V617F JAK2 mutation in MPDs JAK STAT PATHWAY Signal transducers and activators
Essential thrombocythemia treatment algorithm 2018
 Tefferi et al. (2018) 8:2 DOI 10.1038/s41408-017-0041-8 CURRENT TREATMENT ALGORITHM Essential thrombocythemia treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open
Tefferi et al. (2018) 8:2 DOI 10.1038/s41408-017-0041-8 CURRENT TREATMENT ALGORITHM Essential thrombocythemia treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open
Emerging diagnostic and risk stratification criteria
 PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
Disease characteristics in Belgian myelofibrosis patients and management guidelines anno 2013
 4 Disease characteristics in Belgian myelofibrosis patients and management guidelines anno 2013 T. Devos, MD, PhD 1, N. Straetmans, MD, PhD 2, C. Schuermans, MD 3, S. Benghiat, MD, PhD 4, V. Robin, MD
4 Disease characteristics in Belgian myelofibrosis patients and management guidelines anno 2013 T. Devos, MD, PhD 1, N. Straetmans, MD, PhD 2, C. Schuermans, MD 3, S. Benghiat, MD, PhD 4, V. Robin, MD
STEM CELL TRANSPLANTATION IN MYELOFIBROSIS
 STEM CELL TRANSPLANTATION IN MYELOFIBROSIS Giovanni Barosi Unit of Clinical Epidemiology/Center for the Study of Myelofibrosis. IRCCS Policlinico S. Matteo Foundation, Pavia, Italy 1 Annual Florence Meeting
STEM CELL TRANSPLANTATION IN MYELOFIBROSIS Giovanni Barosi Unit of Clinical Epidemiology/Center for the Study of Myelofibrosis. IRCCS Policlinico S. Matteo Foundation, Pavia, Italy 1 Annual Florence Meeting
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Efficacy, safety and survival with ruxolitinib in patients with myelofibrosis: results of a median 2-year follow-up of COMFORT-I
 Efficacy, safety and survival with ruxolitinib in patients with myelofibrosis: results of a median 2-year follow-up of COMFORT-I Srdan Verstovsek, University of Texas M.D. Anderson Cancer Center Ruben
Efficacy, safety and survival with ruxolitinib in patients with myelofibrosis: results of a median 2-year follow-up of COMFORT-I Srdan Verstovsek, University of Texas M.D. Anderson Cancer Center Ruben
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Blood Cancers. Blood Cells. Blood Cancers: Progress and Promise. Bone Marrow and Blood. Lymph Nodes and Spleen
 Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Treatment of polycythemia vera with recombinant interferon alpha (rifnα)
") Treatment of polycythemia vera with recombinant interferon alpha (rifnα) Richard T. Silver, MD Professor of Medicine Weill Cornell Medical College New York, New York Outline of Lecture What are interferons?
Treatment of polycythemia vera with recombinant interferon alpha (rifnα) Richard T. Silver, MD Professor of Medicine Weill Cornell Medical College New York, New York Outline of Lecture What are interferons?
Published Ahead of Print on January 31, 2014, as doi: /haematol Copyright 2014 Ferrata Storti Foundation.
 Published Ahead of Print on January 31, 2014, as doi:10.3324/haematol.2013.101733. Copyright 2014 Ferrata Storti Foundation. The International Prognostic Scoring System does not accurately discriminate
Published Ahead of Print on January 31, 2014, as doi:10.3324/haematol.2013.101733. Copyright 2014 Ferrata Storti Foundation. The International Prognostic Scoring System does not accurately discriminate
Sponsor / Company: Sanofi Drug substance(s): SAR302503
: SAR302503") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Allogreffe dans les syndromes myélo-prolifératifs. DU ALLOGREFFE DE CSH 17 avril 2015 Marie Robin, MD, PhD Hôpital Saint-Louis, Paris, France
 Allogreffe dans les syndromes myélo-prolifératifs DU ALLOGREFFE DE CSH 17 avril 2015 Marie Robin, MD, PhD Hôpital Saint-Louis, Paris, France Plan Indication de l allogreffe dans les SMP Risques spécifiques
Allogreffe dans les syndromes myélo-prolifératifs DU ALLOGREFFE DE CSH 17 avril 2015 Marie Robin, MD, PhD Hôpital Saint-Louis, Paris, France Plan Indication de l allogreffe dans les SMP Risques spécifiques