MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
|
|
|
- Antonia Elizabeth Rodgers
- 5 years ago
- Views:
Transcription
1 MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
2 These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia, and myelofibrosis are the non-leukaemic myeloproliferative neoplasms. Some have overlapping features and there is progression from one to another. A mutation in the gene on chromosome 9 signal transduction molecule JAK-2 which has been found in more than 95% of PRV cases and 50% of those with essential thrombocyathaemia and 50% in myelofibrosis.
3 Myeloproliferative Neoplasm AML Acute Myeloid Leukaemia Haematopoietic Stem Cell
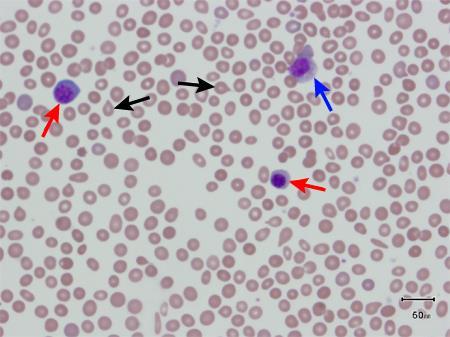
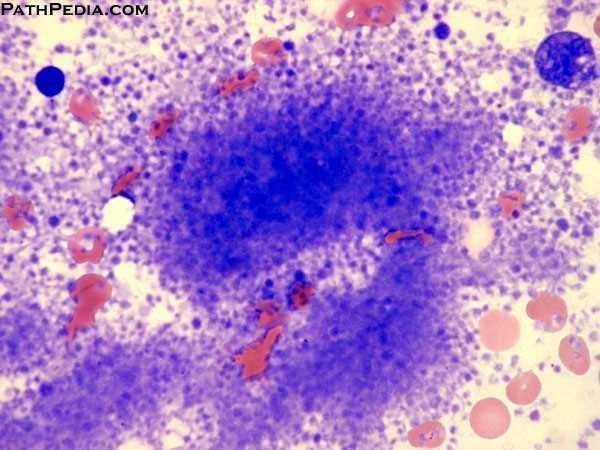
4 Myelofibrosis The marrow is initially hypercellular, with an excess of abnormal megakaryocytes, producing platelet-derived growth factor to the marrow microenvironment, resulting in a reactive proliferation of fibroblasts, leading finally to fibrosis. Clinically: age over 50 yrs., and complain of lassitude, weight loss and night sweats. Spleen can be massively enlarged due to extramedullary haematopoiesis and painful due to splenic infarct. Blood picture-leucoerythroblastic anaemia, with reticulocytes, nucleated RBC and myelocytes. RBC show teardrop poikilocytes, and giant platelets might be seen in the blood. WBC vary from low to moderately high, as well as platelets might be high normal or low. Urates level may be high due to increased cell breakdown. Folate deficiency is common. Bone marrow is difficult to aspirate(dry tap), megakaryocytes increase in number, as well as reticulin and fibrous tissue. Jak2 mutation support the diagnosis.
5
6 Treatment RBC transfusions for anaemia, folic acid, Hydroxycarbamide, may help control spleen size, WBC count and systemic symptoms. Splenectomy for grossly enlarged one, or symptomatic pancytopaenia due to hypersplenism and splenic pooling. HSCT for young patients. Ruxolitinib, an inhibitor of JAK-2 is effective for reducing systemic manifestations and splenomegaly.
7
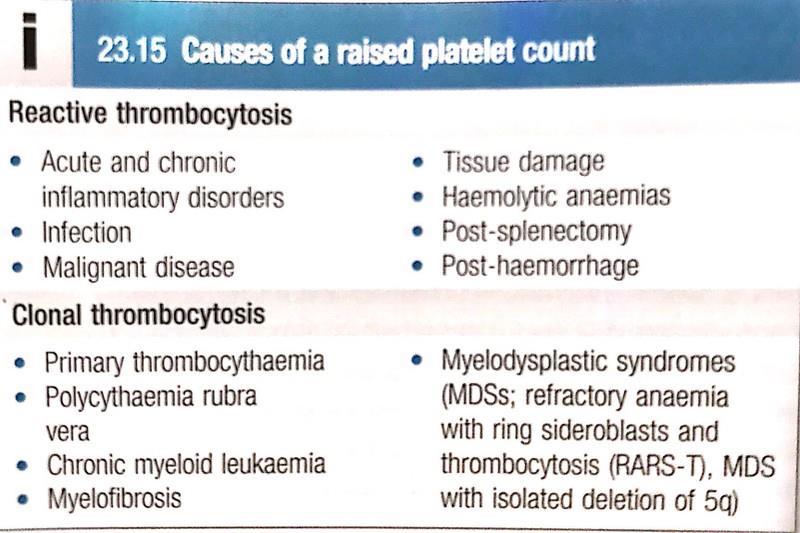
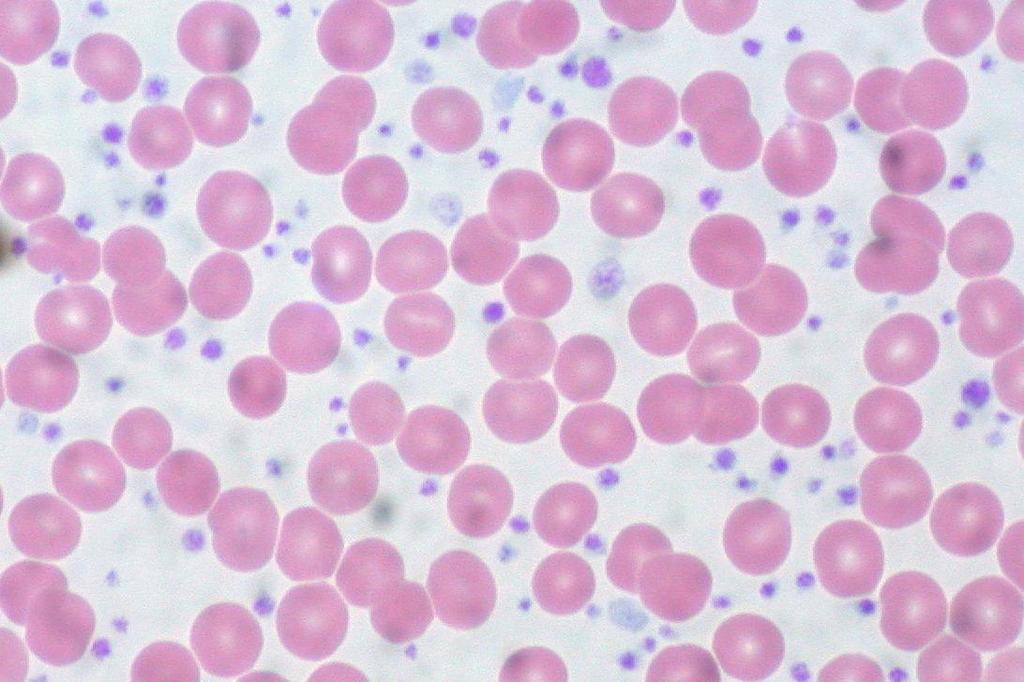
8 Essential Thrombocythaemia Uncontrolled proliferation of megakaryocytes results in raised circulating levels of platelets that are often dysfunctional, reactive causes must be excluded. JAK2, CALR or rarely MPL mutations support the diagnosis but not universal. Presentations; age 60 yrs., vascular occlusion, bleeding or with an asymptomatic isolated platelets count. 5% transform to acute leukaemia and others to myelofibrosis, most patients benefit from low dose aspirin to reduce the risk of occlusive vascular events. Low risk patients(age less than 40yrs and platelet count less than 1.5 millions and no bleeding or thrombosis) may not need treatment to reduce platelet count. If above 1.5 millions with symptoms or other risk factors for thrombosis in e.g. hypertension or DM, treatment should be given, Hydroxycarbamide or anagrelide, an inhibitor of platelet maturation and intravenous radioactive phosphorous in old age.
9
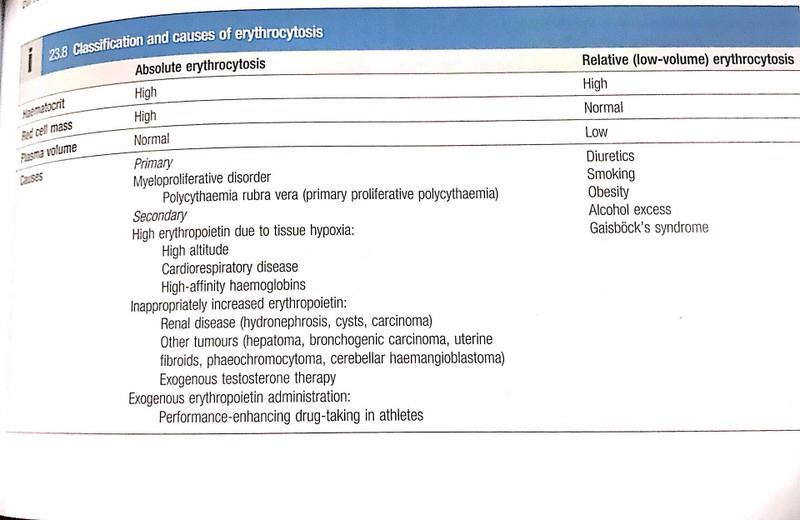
10 High Haemoglobin-Polycythaemia Patients with persistently raised haematocrit, (Hct above 0.52 males or 0.48 females)for more than 2 months should be investigated. True polycythaemia indicate an excess of RBC, while relative or low volume polycythaemia is due to a decreased plasma volume. These include increase erythropoiesis in the bone marrow, either due to primary increase of in marrow activity, or in response to increased erythropoietin(epo levels) in secondary type(in hypoxia), or due to inappropriate secretion of Epo. Athletes who seek to increase oxygen carrying capacity have been known to use Epo. To achieve this. Low volume is polycythaemia associated with hypertension, diuretic use, smoking, and alcohol. Males and females with Hct values of over0.6 and 0.56 respectively, can be assumed to have erythrocytosis. PRV is a high risk for arterial thrombosis (stroke) and VTE, they may have aquagenic pruritus, hepatosplenomegaly and gout(due to high RBC turnover.

11
12
13 Polycyathaemia rubra vera Age over 40 yrs., present as an incidental finding or with symptoms of hyperviscosity, such as lassitude, lack of concentration, headache, dizziness, blackouts, pruritus and epistaxis. Peripheral arterial or cerebrovascular disease, VTE, peptic ulcer disease sometimes complicated with bleeding. Patients are often plethoric and may have a palpable spleen at diagnosis. Investigations; high haematocrit, presence of JAK-2 V617F mutation (positive in 95% of patients). In absence of mutation raised RBC mass and absence of causes of secondary erythrocytosis must be established. Splenomegaly, neutrophil and platelet count are frequently raised. Treatment; venesection, Hydroxycarbamide, interferon alpha to suppress platelet count, which may reduce the risk of vascular occlusion, control spleen size and reduce myelofibrosis transformation. In old age radioactive phosphosphorus which carry 6-10 times increased risk in acute leukaemia. May convert to any myeloproliferative disorder, and 15% progress to acute leukaemia. CVA or coronary artery disease develop in 60% of patients.
14
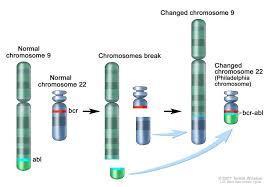
15 Chronic Myeloid Leukaemia CML CML is a shortened chromosome 22 (Philadelphia) resulting from reciprocal translocation material with chromosome 9, (Break Point Cluster Region, BCR, ABL oncogene). It is a myeloproliferative stem cell disorder resulting in haematopoietic lineage but manifesting predominantly in the granulocytic series. Maturation of cells proceed normally. Age 55 yrs., incidence 1.8/100000, accounts for 20% of all leukaemias. A chronic phase; disease is responsive to treatment and is easy to control, which lasts 2-3 yrs., with imatinib therapy life expectancy is normal in many patients. Accelerated phase; in which disease control become more difficult. Blast crises; in which disease turn to either(70% )myeloblastic or (30%) lymphoblastic leukaemia, which is refractory to treatment. This is the cause of death in the majority of cases.
16
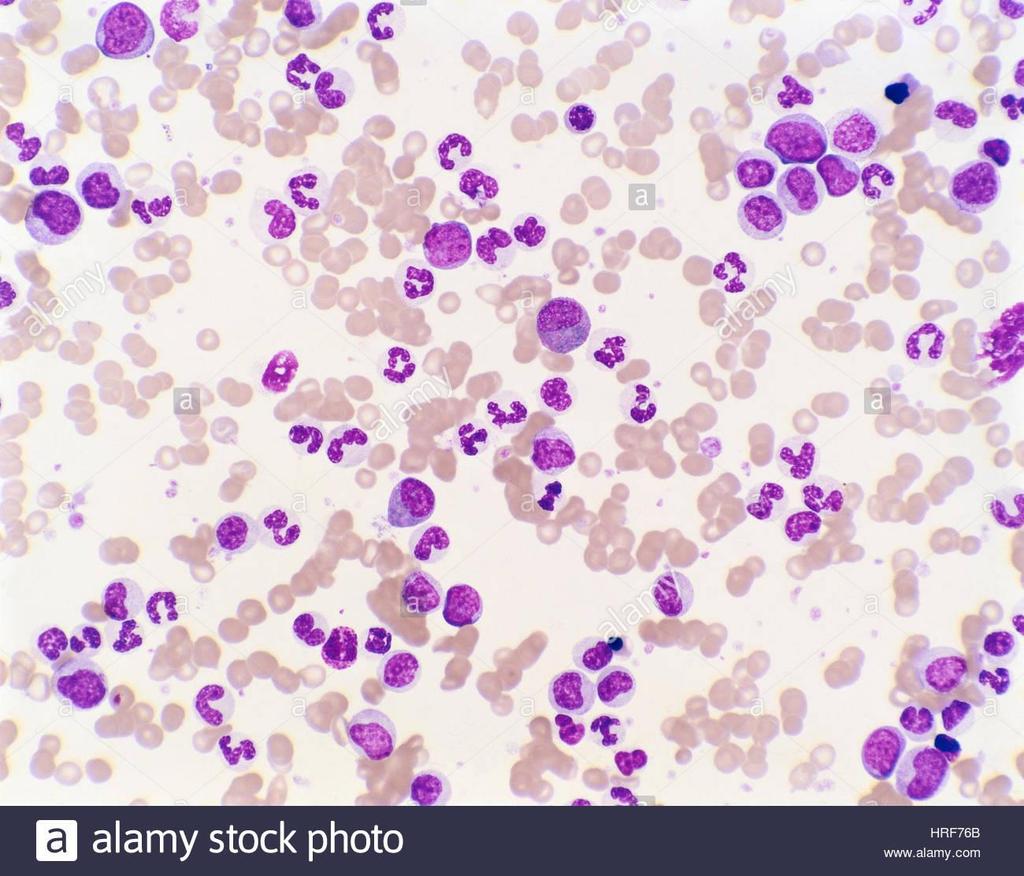
17 Clinical features Lethargy, weight loss. Abdominal pain, gout and sweating, but about 25% are a symptomatic at diagnosis. Signs; splenomegaly in 90% of cases. A friction rub might be heard in splenic infarcts. Hepatomegaly in 50%, but lymph adenopathy is unusual. Investigations; normocytic normochromic anaemia, WBC , and the full range of granulocytes precursors, from myeloblasts to mature neutrophils are seen in the blood film. Myeloblasts are less than 10%.There is increased eosinophils, basophils and nucleated RBC. In one third of patients platelets are high and can be LDH and uric acid are high. Bone marrow should be obtained to confirm diagnosis and phase by morphology. Management; Tyrosine Kinase Inhibitors, imanitib, nilotinib and dasanitib are first line treatment. HSCT
18 MYELODYSPLASIA MDSs constitute a group of clonal haematopoietic disorders with the common features off ineffective blood cell production and a tendency to progress to AML, as such they are pre-leukaemic. MDS presents with consequences of bone marrow failure, (anaemia, recurrent infection or bleeding)usually in older people(median age of diagnosis is 73 yrs.) Incidence 30/ in people over 70yrs. Blood film characterised by cytopaenia and abnormal looking (dysplastic) blood cells including macrocytic RBC (high MCV), hypogranular neutrophils with hypo- or hypersegmentation. The bone marrow is hypercellular, with dysplastic changes in at least 10% of cells of one or more cell lines. The blast cells might be increased but don t reach the 20% level that indicates acute leukaemia. Chromosomes frequently reveals abnormalities, particularly chromosome 5 or7. Prognosis; natural history of MDS is progressive, and worsening of dysplasia leading to bone marrow failure or AML in 30% of cases. The time of progression varies from months to years. Management; for the vast majority patients who are elderly, the disease is incurable, and supportive care with packed RBCs and platelets transfusions is the main stay of treatment. Allogenic bone marrow transplant. Azacytidine has improved survival for 9 months in high-risk patients who are not eligible for transplant.
19
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital
 By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Chronic Myeloproliferative Disorders
 1 Chronic Myeloproliferative Disorders 15th 9 April2015 Polycythemia vera Essential thrombocythemia Idiopathic primary myelofibrosis 2 Learning objectives To appreciate types of polycythaemia (erythrocytosis)
1 Chronic Myeloproliferative Disorders 15th 9 April2015 Polycythemia vera Essential thrombocythemia Idiopathic primary myelofibrosis 2 Learning objectives To appreciate types of polycythaemia (erythrocytosis)
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms Judit Demeter CML chronic myeloid leukemia Semmelweis University, I st Department of Internal Medicine PV polycythaemia vera ET essential thrombocythaemia MF myelofibrosis
Myeloproliferative Neoplasms Judit Demeter CML chronic myeloid leukemia Semmelweis University, I st Department of Internal Medicine PV polycythaemia vera ET essential thrombocythaemia MF myelofibrosis
MYELOPROLIFERATIVE DISEASE. Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG
, MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG") MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
London Cancer. Myelofibrosis guidelines. August Review August Version v1.0. Page 1 of 12
 London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES)
") Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES) Author: Dr N Butt, Consultant Haematologist On behalf of the Haematology CNG Written: July 2010 Reviewed:
Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES) Author: Dr N Butt, Consultant Haematologist On behalf of the Haematology CNG Written: July 2010 Reviewed:
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Myeloproliferative Neoplasms and Treatment Overview
 Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
Greater Manchester and Cheshire Cancer Network
 Greater Manchester and Cheshire Cancer Network Guidelines for the diagnosis and treatment of primary myelofibrosis, post-essential thrombocythaemia myelofibrosis and post-polycythaemia myelofibrosis Tim
Greater Manchester and Cheshire Cancer Network Guidelines for the diagnosis and treatment of primary myelofibrosis, post-essential thrombocythaemia myelofibrosis and post-polycythaemia myelofibrosis Tim
Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms
 Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1
Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1
2013 Pathology Student
 About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA
 BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA Abstract Pages with reference to book, From 151 To 153 Khalid Hassan ( Department of Pathology (Haematology)
BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA Abstract Pages with reference to book, From 151 To 153 Khalid Hassan ( Department of Pathology (Haematology)
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease
 The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms
 Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Managing ET in Tiziano Barbui MD
 Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Department of Clinical Haematology
 Diagnosis in Primary Care and referral pathway for patients with a raised haematocrit Why implement this pathway? A raised haemoglobin or haematocrit is a common finding and can be a reason for referral.
Diagnosis in Primary Care and referral pathway for patients with a raised haematocrit Why implement this pathway? A raised haemoglobin or haematocrit is a common finding and can be a reason for referral.
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
June Ruxolitinib for the second-line treatment of myelofibrosis (IPSS intermediate LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Ruxolitinib for the second-line treatment of myelofibrosis (IPSS intermediate risk-1 or above) Ruxolitinib for the second-line treatment of myelofibrosis (IPSS
LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Ruxolitinib for the second-line treatment of myelofibrosis (IPSS intermediate risk-1 or above) Ruxolitinib for the second-line treatment of myelofibrosis (IPSS
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Diseases Of The Blood
 Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
MPDs. Myeloproliferative Disorders OBJECTIVES MYELOPROLIFERATIVE NEOPLASMS
 MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
MPDs. Myeloproliferative Disorders OBJECTIVES MYELOPROLIFERATIVE NEOPLASMS
 MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
Introduction to Haematology. Prof Roger Pool Department of Haematology University of Pretoria
 Introduction to Haematology Prof Roger Pool Department of Haematology University of Pretoria Suggested reading Haematology at a Glance Atul Mehta & Victor Hoffbrand Second Edition Published by Blackwell
Introduction to Haematology Prof Roger Pool Department of Haematology University of Pretoria Suggested reading Haematology at a Glance Atul Mehta & Victor Hoffbrand Second Edition Published by Blackwell
Glossary of Blood, MPN, and Mutation Terms
 Glossary of Blood, MPN, and Mutation Terms Acute Lymphocytic Leukemia ALL Excess of lymphoblasts. Most common type of cancer in children with cure rate up to 80%. Cure rate for adults is up to 60%. Acute
Glossary of Blood, MPN, and Mutation Terms Acute Lymphocytic Leukemia ALL Excess of lymphoblasts. Most common type of cancer in children with cure rate up to 80%. Cure rate for adults is up to 60%. Acute
How to monitor MPN patients
 How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
HEFT Pathology Guideline. GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia
 HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination
 Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Chronic Neutrophilic Leukaemia (CNL)
") Chronic Neutrophilic Leukaemia (CNL) A Guide for Patients Introduction Being diagnosed with chronic neutrophilic leukaemia (CNL) can be a shock, particularly when you may never have heard of it. If you
Chronic Neutrophilic Leukaemia (CNL) A Guide for Patients Introduction Being diagnosed with chronic neutrophilic leukaemia (CNL) can be a shock, particularly when you may never have heard of it. If you
Myeloproliferative disorders
 should identify drugs that may have to be stopped. Some individuals are particularly sensitive to the usually mild anticoagulant effect of aspirin. A single episode of abnormal surgical bleeding may not
should identify drugs that may have to be stopped. Some individuals are particularly sensitive to the usually mild anticoagulant effect of aspirin. A single episode of abnormal surgical bleeding may not
Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]
![Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]](/thumbs/87/95709298.jpg "Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]") Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Transplants for MPD and MDS
 Transplants for MPD and MDS The question is really who to transplant, with what and when. Focus on myelofibrosis Jeff Szer Royal Melbourne Hospital Myelodysplasia Little needs to be said Despite new therapies
Transplants for MPD and MDS The question is really who to transplant, with what and when. Focus on myelofibrosis Jeff Szer Royal Melbourne Hospital Myelodysplasia Little needs to be said Despite new therapies
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
CLINICAL CASE PRESENTATION
 European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY
 Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
r). SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES
. SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES") r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
Post-ASH 2015 CML - MPN
 Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
MYELODYSPLASTIC AND MYELOPROLIFERATIVE
 MYELODYSPLASTIC AND MYELOPROLIFERATIVE DISORDERS Pediatric Hemato-Oncology Division Medical Faculty University of Sumatera Utara 1 MYELODYSPLASIA SYNDROME A group of disorder defect in hematopoetic cell
MYELODYSPLASTIC AND MYELOPROLIFERATIVE DISORDERS Pediatric Hemato-Oncology Division Medical Faculty University of Sumatera Utara 1 MYELODYSPLASIA SYNDROME A group of disorder defect in hematopoetic cell
Contents SECTION 1: PHYSIOLOGY OF BLOOD
 Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Disorders of Blood Cells & Blood Coagulation
 Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Molecular aberrations in MPN. and use in the clinic. Timothy Devos MD PhD
 Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
CLINICAL POLICY DEPARTMENT: Medical Management DOCUMENT NAME: JakafiTM REFERENCE NUMBER: NH.PHAR.98
 PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
CHRONIC MYELOID LEUKEMIA. Dr.M SAI SRAVANTHI POST GRADUATE DEPT OF GENERAL MEDICINE KAMINENI INSTITUTE OF MEDICAL SCIENCES
 CHRONIC MYELOID LEUKEMIA Dr.M SAI SRAVANTHI POST GRADUATE DEPT OF GENERAL MEDICINE KAMINENI INSTITUTE OF MEDICAL SCIENCES CHRONIC MYELOID LEUKEMIA INCIDENCE The incidence of CML is 1.5 per 100,000 people
CHRONIC MYELOID LEUKEMIA Dr.M SAI SRAVANTHI POST GRADUATE DEPT OF GENERAL MEDICINE KAMINENI INSTITUTE OF MEDICAL SCIENCES CHRONIC MYELOID LEUKEMIA INCIDENCE The incidence of CML is 1.5 per 100,000 people
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
BIOS222 Pathology and Clinical Science 2 & 3
 BIOS222 Pathology and Clinical Science 2 & 3 Session 6 Lymphatic and Haematological Disorders 4 Bioscience Department www.endeavour.edu.au Session Learning Outcomes At the end of the session, student should
BIOS222 Pathology and Clinical Science 2 & 3 Session 6 Lymphatic and Haematological Disorders 4 Bioscience Department www.endeavour.edu.au Session Learning Outcomes At the end of the session, student should
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment
 Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment BHS Training course 2013-2015 Timothy Devos POLYCYTEMIA VERA PV: clinical manifestations thrombosis (art > ven) facial
Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment BHS Training course 2013-2015 Timothy Devos POLYCYTEMIA VERA PV: clinical manifestations thrombosis (art > ven) facial
Disclosure: Objectives/Outline. Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations. Nothing to disclose.
 RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
Agnogenic myeloid metaplasia: role of splenectomy
 Postgrad. med. J. (April 1969) 45, 261-265. Agnogenic myeloid metaplasia: role of splenectomy CHARLES MARKS M.D., M.S., M.R.C.P., F.R.C.S. Director, Division of Surgery, The Mount Sinai Hospital of Cleveland;
Postgrad. med. J. (April 1969) 45, 261-265. Agnogenic myeloid metaplasia: role of splenectomy CHARLES MARKS M.D., M.S., M.R.C.P., F.R.C.S. Director, Division of Surgery, The Mount Sinai Hospital of Cleveland;
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
[COMPREHENSIVE GENETIC ASSAY PANEL ON
 2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
SH A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL
 SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
Bone marrow histopathology in Ph - CMPDs. - the new WHO classification - Juergen Thiele Cologne, Germany
 Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
The BCR-ABL1 fusion. Epidemiology. At the center of advances in hematology and molecular medicine
 At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
HAEMATOLOGY CLINICAL GUIDELINES (LANCASHIRE & SOUTH CUMBRIA) May Review date: March 2016 (or earlier if new guidance published)
 May Review date: March 2016 (or earlier if new guidance published)") HAEMATOLOGY CLINICAL GUIDELINES (LANCASHIRE & SOUTH CUMBRIA) May 2015 Review date: March 2016 (or earlier if new guidance published) 1 Index: Page No Chronic Lymphocytic Leukaemia 3 Precursor Acute Lymphoblastic
HAEMATOLOGY CLINICAL GUIDELINES (LANCASHIRE & SOUTH CUMBRIA) May 2015 Review date: March 2016 (or earlier if new guidance published) 1 Index: Page No Chronic Lymphocytic Leukaemia 3 Precursor Acute Lymphoblastic
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Polycythemia Vera and Essential Thombocythemia A Single Institution Experience
 INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Neoplastic proliferation arising from white blood cells. Introductory remarks. Classification
 Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations and Management
 Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
رناد زكريا Dr. ahmad Dr. ahmad. P a g e 1
 5 رناد زكريا Dr. ahmad Dr. ahmad P a g e 1 Before we start. -This sheet was written according to section 2 s record and reviewed according to section 1 s record by Ruba Hussien with all thanks and I referred
5 رناد زكريا Dr. ahmad Dr. ahmad P a g e 1 Before we start. -This sheet was written according to section 2 s record and reviewed according to section 1 s record by Ruba Hussien with all thanks and I referred
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Chronic Myelogenous Leukemia in a 66-Year-Old Male with Concurrent Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma
 Chronic Myelogenous Leukemia in a 66-Year-Old Male with Concurrent Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Linda J. Szymanski, DO, 1 Hashem Ayyad, MD, 1 Kedar Inamdar, MD, PhD 1* CLINICAL
Chronic Myelogenous Leukemia in a 66-Year-Old Male with Concurrent Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Linda J. Szymanski, DO, 1 Hashem Ayyad, MD, 1 Kedar Inamdar, MD, PhD 1* CLINICAL
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Imaging features of myeloproliferative neoplasms.
 Imaging features of myeloproliferative neoplasms. Poster No.: C-0410 Congress: ECR 2016 Type: Educational Exhibit Authors: I. Murphy, E. Mitchell, A. Godfrey, E. M. Godfrey ; Cambridge, 1 2 2 2 1 2 Cambridgeshire/UK,
Imaging features of myeloproliferative neoplasms. Poster No.: C-0410 Congress: ECR 2016 Type: Educational Exhibit Authors: I. Murphy, E. Mitchell, A. Godfrey, E. M. Godfrey ; Cambridge, 1 2 2 2 1 2 Cambridgeshire/UK,
How I Treat Myelofibrosis. Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom
 How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
Extensive bone marrow infarction followed by myelofibrosis in a patient with Ph' positive chronic granulocytic leukaemia
 J Clin Pathol 1980; 33: 449-453 Extensive bone marrow infarction followed by myelofibrosis in a patient with Ph' positive chronic granulocytic leukaemia BARBARA BAIN From the Department of Haematology,
J Clin Pathol 1980; 33: 449-453 Extensive bone marrow infarction followed by myelofibrosis in a patient with Ph' positive chronic granulocytic leukaemia BARBARA BAIN From the Department of Haematology,