Case Report Rapid Progression of Pulmonary Blastomycosis in an Untreated Patient of Chronic Lymphocytic Leukemia
|
|
|
- Helena Harper
- 5 years ago
- Views:
Transcription
1 Case Reports in Medicine, Article ID , 5 pages Case Report Rapid Progression of Pulmonary Blastomycosis in an Untreated Patient of Chronic Lymphocytic Leukemia Pralay K. Sarkar, 1,2,3 Paras Malhotra, 1 and P. S. Sriram 1 1 Divisions of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, University of Florida, Gainesville, FL 32608, USA 2 Pulmonary and Critical Care Medicine, Baylor College of Medicine, One Baylor Plaza, Houston, TX 77030, USA 3 Ben Taub General Hospital, 1504 Taub Loop, BTGH-6PF80002, Houston, TX 77030, USA Correspondence should be addressed to Pralay K. Sarkar; pralay.sarkar@gmail.com Received 21 January 2014; Revised 1 March 2014; Accepted 17 March 2014; Published 13 April 2014 Academic Editor: Masahiro Kohzuki Copyright 2014 Pralay K. Sarkar et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Chroniclymphocytic leukemia (CLL) is associated with a state of immunosuppression characterized by hypogammaglobulinemia as well as B and T lymphocyte dysfunction. Though opportunistic infections are common in CLL patients, particularly after treatment, reports of infections by endemic dimorphic fungi are very few. Here we report a case of pulmonary blastomycosis in a CLL patient who initially presented with an indolent pulmonary mass lesion. The pulmonary lesions progressed rapidly over a two-week period. The diagnosis was established by transbronchial lung biopsy. He was treated with Amphotericin B lipid complex followed by oral itraconazole and recovered uneventfully. This case illustrates the importance of a timely diagnosis and treatment. The presentation of blastomycosis in immunocompromised patients, diagnosis, and treatment are discussed. 1. Introduction Blastomycosis refers to an endemic mycosis caused by the dimorphic fungus Blastomyces dermatitidis. It is endemic in midwestern, south-eastern, and south central United States. In immunocompromised patients, disseminated infection has been reported. Here we described a case of rapidly progressive pulmonary blastomycosis in a patient with CLL. 2. Case Report A 50-year-old nonsmoker man was referred to the pulmonary clinic with 4-week history of nonproductive cough, right sided pleuritic chest pain, night sweats, and unquantified weight loss. He did not have any hemoptysis, dyspnea, or wheezing. He was diagnosed to have B-cell chronic lymphocytic leukemia (B-CLL) 4 years prior to this presentation. However, as he was asymptomatic, no treatment was required for CLL till this presentation. His other medical history included a diagnosis of type 2 diabetes mellitus. His vital signs at the time of our initial evaluation were as follows: temperature 37 C, heart rate 75 beats/min, blood pressure 105/63 mm Hg, respiratory rate 18/min, and oxygen saturation 98% on room air. On physical examination, he had no evident respiratory distress. He had generalized lymphadenopathy, consistent with his known diagnosis of CLL. Examination of the respiratory system revealed bilateral vesicular breath sounds without any adventitious sounds. Examination of cardiovascular system, abdomen, and central nervous system was unremarkable. Laboratory examination revealed a white blood cell count of 117,000/mm 3 (1% neutrophils, 96% lymphocytes, and 2% monocytes), 1.4% hemoglobin 8.9 g/dl, hematocrit 28.1%, and platelet count 243,000/mm 3. Serum electrolytes, renal function, and liver function tests were normal. Chest X-ray (CXR) revealed a right lower lobe mass (Figure1). CT scan chest revealed right lower lobe mass with mediastinal invasion and small right pleural effusion (Figure 2). A possible diagnosis of primary bronchogenic carcinoma was entertained and the patient underwent an outpatient fiberoptic bronchoscopy.


. The patient did not report any worsening of his respiratory symptoms or any extrapulmonary symptoms.")
2 2 Case Reports in Medicine Figure 1: CXR showing right lower lobe mass lesion at the time of presentation. Figure 2: CT scan chest at presentation showing areas of consolidation in the right lower lobe. Also note the small right pleural effusion. Bronchoscopy did not reveal any endobronchial lesion. Bronchoalveolar lavage (BAL) and a transbronchial lung biopsy were obtained from right lower lobe segments. Cytological analysisofbalshowedamixedinflammatoryinfiltratewith predominant lymphocytes. One week after the bronchoscopy, before the biopsy report was available, he was admitted in view of marked fatigue and weakness. CXR showed progression of the radiological changes, in the intervening two weeks from the initial imaging, with a new development of a miliary pattern (Figure 3). CT scan obtained at this time confirmed the miliary dissemination (Figure 4). The patient did not report any worsening of his respiratory symptoms or any extrapulmonary symptoms. The transbronchial lung biopsy results from the right lower lobe returned and showed numerous lymphocytes, histiocytes, and many multinucleated giant cells, forming ill-defined granulomas (Figure 5(a)). The biopsy also revealed presence of thick-walled singleyeast forms of approximately 8 15 μm size (Figure 5(b)). The organisms stained positively with Gömöri methenamine silver (GMS) stain and did not stain with mucicarmine (Figures 5(c) and 5(d)). Some of these yeast forms showed eccentric broad based budding (Figure 5(c)), overall morphologyconsistentwithblastomycosis.bronchialbiopsyand BAL cultures did not show any growth of fungus in 4 weeks. CT scan of abdomen and pelvis did not show any lesion in liver, spleen, or kidneys. Magnetic resonance imaging of the brain did not show any lesion. Cerebrospinal fluid analysis was normal. The patient received eight days of treatment with Amphotericin B lipid complex at a dose of 5 mg/kg body weight. Treatment was subsequently continued with itraconazole 400 mg/day for 12 months. Follow-up imaging of the lungs showed satisfactory resolution of the pulmonary lesions. The patient was continued indefinitely on itraconazole 200 mg/day as he subsequently required chemotherapy for management of CLL. 3. Discussion In this report, we have a described a case of rapid progression of pulmonary blastomycosis, from a single mass lesion to miliary dissemination over 2 weeks, in a patient with untreated Figure 3: CXR showing progression of right lower lobe lesion and development of bilateral miliary nodules. There was 2-week time interval between thiscxrand CXRshowninFigure 1. CLL. This case highlights the importance of prompt diagnosis and institution of treatment in immunocompromised patients. Though our patient did not develop respiratory failure in spite of miliary involvement of the lungs, blastomycosis isknowntocauseacuterespiratorydistresssyndromewitha high mortality [1] and therefore an early diagnosis leads to a favorable outcome. Blastomycosis has been reported in association with different immunosuppressive states, including a treatedcaseofcllwithresultantabsoluteneutropenia[2]; our patient had rapid progression to disseminated disease in absence of neutropenia or recent chemotherapy. Our patient did not have any history of living in or traveling to a zone knowntobeendemicforblastomycosis.thiscasehighlights the difficulty of diagnosing a sporadic case of blastomycosis in nonendemic areas. CLL is characterized by a state of immunodeficiency and infection is a common cause of death [3]. Along with the well-known abnormality of hypogammaglobulinemia, there is also evidence of defects in cell mediated immunity, relevant in causing predisposition to intracellular pathogens like Blastomyces spp. In most patients with CLL, there is an increase in both CD8+ and CD4+ T-cell numbers and reversal of CD4/CD8 ratio; however, it has been suggested that

3 Case Reports in Medicine 3 Figure 4: CT scan obtained 2 weeks following the initial evaluation confirmed the miliary dissemination, progression of the index mass lesion, and several new satellite lesions. the T cell in B-CLL may be unable to start, maintain, and complete an immune response to the malignant B cell and other antigens, the result being susceptibility to infections and sustenance of the tumor [4]. Defects in phagocytic function and cytotoxic activity of neutrophils, monocytes, and natural killer (NK) cells and defects in complement system are other immunological changes described in CLL [5]. As a defect in cell-mediated immunity will predict, CLL patients are susceptible to a host of opportunistic infections, for example, Listeria spp., Nocardia spp., Candida spp., Aspergillus spp., Pneumocystis jirovecii, Histoplasma capsulatum, Cryptococcus neoformans and atypical mycobacteria; these do not occur commonly in untreated patients. As patients are treated, depending on the type of treatment agent (alkylating agent, purine analogues, or monoclonal antibodies), somewhat different clinical spectrums of opportunistic infections are seen [6]. A wide variety of radiographic changes have been reported in pulmonary blastomycosis; radiological findings have been reported to be largely similar in immunocompromised and immunocompetent patients [7, 8]. Common chest radiological patterns in blastomycosis include alveolar infiltrates, solitary pulmonary nodules, lung mass with or without cavitation, interstitial infiltrates, mediastinal lymphadenopathy, and pleural involvement [8]. Alveolar infiltrates are more common in acute presentation, whereas mass like lesions are more common in chronic presentation. CT chest similarly shows a broad range of findings: mass lesions, consolidation with air bronchogram, intermediate-sized nodules, satellite lesions around mass or consolidation, pleural thickening, small effusions, and cavitation [9]. There is no pathognomonic radiological pattern in blastomycosis [10, 11]; therefore, presentation in a nonendemic area with a mass-like lesionmayraiseobviousdiagnosticdifficulties,ashappened in our index case. Miliary pattern is less commonly seen. We speculate that the rapid progression of the pulmonary lesions in our case, from a solitary lesion to a miliary pattern, resulted from erosion into a pulmonary vessel; however, an earlier autopsy report of a case of miliary blastomycosis did not identify vascular invasion [12]. Systemic dissemination is likely in a case of miliary dissemination; however, our patient did not have any evidence of clinical disease in any extrapulmonary site. Diagnosis can be established by direct visualization of the fungus in clinical specimen or culture of body fluid or tissue. Rapid diagnosis can be established by microscopic examination of sputum or bronchial washing, digested with 10% potassium hydroxide. B. dermatitidis can be identified by its characteristic morphology: the yeast-like cells of the fungus are oval to spherical, 8 15 μm indiameter,andwiththick refractile wall. They are multinucleate and show single broadbased budding: useful diagnostic features. Different stains can be used to demonstrate the organism. Papanicolaou staining of respiratory tract specimens has a high diagnostic yield (93%); the organism appears to be refractile and pale bluegreen with this stain. Other useful special stains are Gömöri methenamine-silver (GMS) or periodic acid-schiff (PAS) stains. Identification of B. dermatitidis in hematoxylin-eosin (H&E)stainedhistopathologicspecimensisoftendifficult. Mucicarmine stain is useful in differentiation from capsule deficient forms of Cryptococcus neoformans, being negative in case of B. dermatitidis. Therespiratorytractspecimenswere sterile in our index case; however, microorganisms have been recovered in a high percentage of cases with documented pulmonary disease [13]. Amphotericin B (AmB) remains the drug of choice in blastomycosis with life threatening disease or with CNS involvement, for patients who are immunocompromised or for whom azole treatment has failed [14, 15]. For moderate to severe pulmonary disease, current guidelines recommend treatment with a lipid formulation of AmB at a dosage of 3 5 mg/kg per day or AmB deoxycholate at a dosage of mg/kg per day for 1-2 weeks or until improvement is noted, followed by oral itraconazole [15]. However, the cost and toxicity are substantial. Among the azole antifungals, ketoconazole was the first one used with success in treatment of blastomycosis. However, in the current guidelines, itraconazole has replaced ketoconazole as the azole of choice for its better antimycotic effect, better tolerability, and higher (up to 95%) rate of cure [15]. Treatment duration is 6 12 months or till resolution of radiological abnormalities. There are no standard guidelines for antimicrobial prophylaxis in CLL patients. Clinical practice therefore varies, andinmostcases,theprophylaxisisdirectedagainstherpes viruses, Pneumocystis jirovecii, and toxoplasmosis (e.g., acyclovir, sulfamethoxazole, and trimethoprim). A good case of antifungalprophylaxisisinselectedclinicalscenarios:treatment with either purine analogue or alemtuzumab, following stem cell allografts, previous systemic fungal infection, severe and prolonged neutropenia, and use of high-dose steroids and several previous rounds of immunosuppressive therapy [3]. 4. Conclusion CLL is characterized by a state of immunosuppression even in untreated patients. Blastomycosis is an endemic fungal infection and, particularly in an immunocompromised patient, can progress rapidly. Timely diagnosis helps in successful
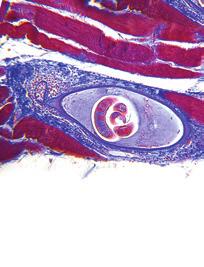
 Intracellular fungal organism within a giant cell (arrowheads) (H & E stain 600). (c) Yeast-like cells of Blastomyces dermatitidis.")

![References [1] L. B. Lemos, M. Baliga, and M. Guo, Acute respiratory distress syndrome and blastomycosis: presentation of nine cases and review of the literature, Annals of Diagnostic Pathology, vol.](/docs-images/85/93034900/images/4-2.jpg "5, no. 1, pp. 1 9, 2001. [2] P.A.Isotalo,J.C.Ford,andJ.P.Veinot, Miliaryblastomycosis developing in an immunocompromised host with chronic lymphocytic leukaemia, Pathology, vol. 34, no. 3, pp.")
![293 295, 2002. [3] A. D. Hamblin and T. J. Hamblin, The immunodeficiency of chronic lymphocytic leukaemia, British Medical Bulletin, vol. 87, no. 1, pp. 49 62, 2008. [4]S.Scrivener,R.V.Goddard,E.R.Kaminski,andA.](/docs-images/85/93034900/images/4-3.jpg "G.Prentice, Abnormal T-cell function in B-cell chronic lymphocytic leukaemia, Leukemia and Lymphoma, vol.44,no.3,pp.383 389, 2003. [5] F. Ravandi and S.")
4 4 Case Reports in Medicine (a) (b) (c) (d) Figure 5: Representative photomicrographs from the transbronchial lung biopsy. (a) Lymphocytic infiltration and multiple giant cells (H & E, 200). (b) Intracellular fungal organism within a giant cell (arrowheads) (H & E stain 600). (c) Yeast-like cells of Blastomyces dermatitidis. Note the characteristic broad based budding (arrowhead) (GMS stain, 400). (d) A representative section with negative mucicarmine stain ( 200). outcome. Amphotericin B and itraconazole are currently recommended treatments. Conflict of Interests The authors declare that there is no conflict of interests regarding the publication of this paper. References [1] L. B. Lemos, M. Baliga, and M. Guo, Acute respiratory distress syndrome and blastomycosis: presentation of nine cases and review of the literature, Annals of Diagnostic Pathology, vol.5, no. 1, pp. 1 9, [2] P.A.Isotalo,J.C.Ford,andJ.P.Veinot, Miliaryblastomycosis developing in an immunocompromised host with chronic lymphocytic leukaemia, Pathology, vol. 34, no. 3, pp , [3] A. D. Hamblin and T. J. Hamblin, The immunodeficiency of chronic lymphocytic leukaemia, British Medical Bulletin, vol. 87, no. 1, pp , [4]S.Scrivener,R.V.Goddard,E.R.Kaminski,andA.G.Prentice, Abnormal T-cell function in B-cell chronic lymphocytic leukaemia, Leukemia and Lymphoma, vol.44,no.3,pp , [5] F. Ravandi and S. O Brien, Immune defects in patients with chronic lymphocytic leukemia, Cancer Immunology, Immunotherapy,vol.55,no.2,pp ,2006. [6] V. A. Morrison, Infectious complications of chronic lymphocytic leukaemia: pathogenesis, spectrum of infection, preventive approaches, Best Practice and Research: Clinical Haematology, vol. 23, no. 1, pp , [7] L.D.Recht,S.F.Davies,M.R.Eckman,andG.A.Sarosi, Blastomycosis in immunosuppressed patients, American Review of Respiratory Disease,vol.125,no.3,pp ,1982. [8] R. G. Patel, B. Patel, M. F. Petrini, R. R. Carter III, and J. Griffith, Clinical presentation, radiographic findings, and diagnostic methods of pulmonary blastomycosis: a review of 100 consecutive cases, Southern Medical Journal, vol. 92, no. 3, pp , [9]H.T.Winer-Muram,D.H.Beals,andF.H.ColeJr., Blastomycosis of the lung: CT features, Radiology,vol.182,no.3,pp , [10] L. R. Brown, S. J. Swensen, R. E. Van Scoy, U. B. S. Prakash, D. T. Coles, and T. V. Colby, Roentgenologic features of pulmonary blastomycosis, Mayo Clinic Proceedings, vol. 66, no. 1, pp , [11] J. R. Sheflin, J. A. Campbell, and G. P. Thompson, Pulmonary blastomycosis: findings on chest radiographs in 63 patients, The AmericanJournalofRoentgenology,vol.154,no.6,pp , 1990.
5 Case Reports in Medicine 5 [12] P. M. Kar, F. A. Montalvo, D. M. Salazar, and S. M. Kar, Blastomycosis: case report investigating a persistent pulmonary lesion in an immunocompromised patient, The the Kentucky Medical Association,vol.107,no.7,pp ,2009. [13] M.A.MartynowiczandU.B.S.Prakash, Pulmonaryblastomycosis: an appraisal of diagnostic techniques, Chest,vol.121,no. 3, pp , [14] S. W. Chapman, J. Bradsher R.W., J. Campbell G.D., P. G. Pappas, and C. A. Kauffman, Practice guidelines for the management of patients with blastomycosis, Clinical Infectious Diseases, vol. 30, no. 4, pp , [15] S. W. Chapman, W. E. Dismukes, L. A. Proia et al., Clinical practice guidelines for the management of blastomycosis: 2008 Update by the infectious diseases society of America, Clinical Infectious Diseases,vol.46,no.12,pp ,2008.










6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Lecture 7: Mycoses Caused by Dimorphic Fungi, Part I
 BIOL 4849 Medical Mycology Summer 2006 Histoplasmosis Lecture 7: Mycoses Caused by Dimorphic Fungi, Part I u Most common endemic mycotic disease in the United States u Two different varieties (actually
BIOL 4849 Medical Mycology Summer 2006 Histoplasmosis Lecture 7: Mycoses Caused by Dimorphic Fungi, Part I u Most common endemic mycotic disease in the United States u Two different varieties (actually
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Practice Guidelines for the Management of Patients with Blastomycosis
 679 Practice Guidelines for the Management of Patients with Blastomycosis Stanley W. Chapman, 1 Robert W. Bradsher, Jr., 2 G. Douglas Campbell, Jr., 3 Peter G. Pappas, 4 and Carol A. Kauffman 5 From the
679 Practice Guidelines for the Management of Patients with Blastomycosis Stanley W. Chapman, 1 Robert W. Bradsher, Jr., 2 G. Douglas Campbell, Jr., 3 Peter G. Pappas, 4 and Carol A. Kauffman 5 From the
2046: Fungal Infection Pre-Infusion Data
 2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
Pneumocystis. Pneumocystis BIOL Summer Introduction. Mycology. Introduction (cont.) Introduction (cont.)
 Introduction (cont.)") Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
Pleural effusion as an initial manifestation in a patient with primary pulmonary monoclonal B-cell lymphocyte proliferative disease
 Du et al. Respiratory Research (2018) 19:247 https://doi.org/10.1186/s12931-018-0941-6 LETTER TO THE EDITOR Pleural effusion as an initial manifestation in a patient with primary pulmonary monoclonal B-cell
Du et al. Respiratory Research (2018) 19:247 https://doi.org/10.1186/s12931-018-0941-6 LETTER TO THE EDITOR Pleural effusion as an initial manifestation in a patient with primary pulmonary monoclonal B-cell
Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD
 Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches
Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches
Fungal Diseases of the Respiratory System
 Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma of Thyroid
 Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Non-resolving Community Acquired Pneumonia (CAP) due to Blastomyces dermatitidis (Pulmonary Blastomycosis): Case Report and Review of Literature
 due to Blastomyces dermatitidis (Pulmonary Blastomycosis): Case Report and Review of Literature") The University of Louisville Journal of Respiratory Infections Volume 2 Issue 1 Article 9 4-6-2018 Non-resolving Community Acquired Pneumonia (CAP) due to Blastomyces dermatitidis (Pulmonary Blastomycosis):
The University of Louisville Journal of Respiratory Infections Volume 2 Issue 1 Article 9 4-6-2018 Non-resolving Community Acquired Pneumonia (CAP) due to Blastomyces dermatitidis (Pulmonary Blastomycosis):
Invasive Pulmonary Aspergillosis in
 Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids
 Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Patient: Chief Complaint: Family history: Social history: History of Present Illness: Physical Examination Results:
 Uncontrolled Pneumonia in a 49-Year-Old White Man Farnoush Taghizadeh, BS, MLS(ASCP),1* Raghuraj S Raghuwanshi M, MD Lab Med Summer 2014;45:e123-e127 DOI: 10.1309/LMeq9ie7aqqpgdgdoy Clinical History Patient:
Uncontrolled Pneumonia in a 49-Year-Old White Man Farnoush Taghizadeh, BS, MLS(ASCP),1* Raghuraj S Raghuwanshi M, MD Lab Med Summer 2014;45:e123-e127 DOI: 10.1309/LMeq9ie7aqqpgdgdoy Clinical History Patient:
Pulmonary Cryptococcosis in an HIV-infected Patient
 Case Report Vol. 28 No. 3 Pulmonary Cryptococcosis:- Wongkulab P, et al. 203 Pulmonary Cryptococcosis in an HIV-infected Patient Panuwat Wongkulab, M.D., Nontakan Nuntachit, M.D., Romanee Chaiwarith, M.D.,
Case Report Vol. 28 No. 3 Pulmonary Cryptococcosis:- Wongkulab P, et al. 203 Pulmonary Cryptococcosis in an HIV-infected Patient Panuwat Wongkulab, M.D., Nontakan Nuntachit, M.D., Romanee Chaiwarith, M.D.,
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Case Report Pulmonary Tuberculosis and Lepromatous Leprosy Coinfection
 Case Reports in Dermatological Medicine Volume 2015, Article ID 898410, 4 pages http://dx.doi.org/10.1155/2015/898410 Case Report Pulmonary Tuberculosis and Lepromatous Leprosy Coinfection F. A. Sendrasoa,
Case Reports in Dermatological Medicine Volume 2015, Article ID 898410, 4 pages http://dx.doi.org/10.1155/2015/898410 Case Report Pulmonary Tuberculosis and Lepromatous Leprosy Coinfection F. A. Sendrasoa,
The Differentiation of Yeast and Yeast-Like Forms in Human Tissues. Introduction. Histochemical Stains Used to Detect Fungi. Histopathologic Diagnoses
 The Differentiation of Yeast and Yeast-Like Forms in Human Tissues Gary W. Procop, MD Chair, Clinical Pathology Staff, Anatomic Pathology Director, Molecular Microbiology, Mycology, and Parasitology Cleveland
The Differentiation of Yeast and Yeast-Like Forms in Human Tissues Gary W. Procop, MD Chair, Clinical Pathology Staff, Anatomic Pathology Director, Molecular Microbiology, Mycology, and Parasitology Cleveland
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Study of systemic fungal infections in renal transplant recipients
 Original Research Article Study of systemic fungal infections in renal transplant recipients N.D. Srinivasaprasad 1*, G. Chandramohan 1, M. Edwin Fernando 2 1 DM (Nephrology), Assistant Professor, 2 DM
Original Research Article Study of systemic fungal infections in renal transplant recipients N.D. Srinivasaprasad 1*, G. Chandramohan 1, M. Edwin Fernando 2 1 DM (Nephrology), Assistant Professor, 2 DM
Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
 Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule
 Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Case Report Pulmonary Embolism Originating from a Hepatic Hydatid Cyst Ruptured into the Inferior Vena Cava: CT and MRI Findings
 Case Reports in Radiology Volume 2016, Article ID 3589812, 4 pages http://dx.doi.org/10.1155/2016/3589812 Case Report Pulmonary Embolism Originating from a Hepatic Hydatid Cyst Ruptured into the Inferior
Case Reports in Radiology Volume 2016, Article ID 3589812, 4 pages http://dx.doi.org/10.1155/2016/3589812 Case Report Pulmonary Embolism Originating from a Hepatic Hydatid Cyst Ruptured into the Inferior
Fungal Infections. Fungal Infections
 Fungal Infection in the Immune Competent Host Steven L. Primack, MD Fungal Infection in the Immune Competent Host Steven L. Primack, MD Department of Radiology Oregon Health & Science University Fungal
Fungal Infection in the Immune Competent Host Steven L. Primack, MD Fungal Infection in the Immune Competent Host Steven L. Primack, MD Department of Radiology Oregon Health & Science University Fungal
HAEMATOLOGY ANTIFUNGAL POLICY
 HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
A Case of Pulmonary Cryptococcosis by Capsule-deficient Cryptococcus neoformans
 The Korean Journal of Internal Medicine: 21:83-87, 2006 A Case of Pulmonary Cryptococcosis by Capsule-deficient Cryptococcus neoformans Won Seok Cheon, M.D., Kwang-Seok Eom, M.D., Byoung Kwan Yoo, M.D.,Seung
The Korean Journal of Internal Medicine: 21:83-87, 2006 A Case of Pulmonary Cryptococcosis by Capsule-deficient Cryptococcus neoformans Won Seok Cheon, M.D., Kwang-Seok Eom, M.D., Byoung Kwan Yoo, M.D.,Seung
PARASITOLOGY CASE HISTORY 10 (HISTOLOGY) (Lynne S. Garcia)
 (Lynne S. Garcia)") PARASITOLOGY CASE HISTORY 10 (HISTOLOGY) (Lynne S. Garcia) A 46-year-old man with AIDS was admitted to the hospital for complaints of a persisting fever and dry cough. A chest radiograph showed bilateral
PARASITOLOGY CASE HISTORY 10 (HISTOLOGY) (Lynne S. Garcia) A 46-year-old man with AIDS was admitted to the hospital for complaints of a persisting fever and dry cough. A chest radiograph showed bilateral
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Fungal Infection Post-Infusion Data
 Fungal Infection Post-Infusion Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: Event date: / / Visit: 100 day 6 months 1 year 2 years >2 years. Specify: CIBMTR Form 2146 revision
Fungal Infection Post-Infusion Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: Event date: / / Visit: 100 day 6 months 1 year 2 years >2 years. Specify: CIBMTR Form 2146 revision
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
The Pulmonary Pathology of Iatrogenic Immunosuppression. Kevin O. Leslie, M.D. Mayo Clinic Scottsdale
 The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host
 Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
CASE REPORT PULMONARY BLASTOMYCOSIS DIAGNOSED IN HAWAI I
 CASE REPORT PULMONARY BLASTOMYCOSIS DIAGNOSED IN HAWAI I Michael V Arnett 1, Susan L Fraser 2 and Vincent X Grbach 1 1 Tripler Army Medical Center, Honolulu, HI; 2 Walter Reed Army Medical Center, Washington
CASE REPORT PULMONARY BLASTOMYCOSIS DIAGNOSED IN HAWAI I Michael V Arnett 1, Susan L Fraser 2 and Vincent X Grbach 1 1 Tripler Army Medical Center, Honolulu, HI; 2 Walter Reed Army Medical Center, Washington
New respiratory symptoms and lung imaging findings in a woman with polymyositis
 Maria Bolaki 1, Konstantinos Karagiannis 1, George Bertsias 2, Ioanna Mitrouska 1, Nikolaos Tzanakis 1, Katerina M. Antoniou 1 kantoniou@uoc.gr 1 Dept of Thoracic Medicine, Heraklion University Hospital,
Maria Bolaki 1, Konstantinos Karagiannis 1, George Bertsias 2, Ioanna Mitrouska 1, Nikolaos Tzanakis 1, Katerina M. Antoniou 1 kantoniou@uoc.gr 1 Dept of Thoracic Medicine, Heraklion University Hospital,
Eosinophils and effusion: a clinical conundrum
 Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Reverse Halo Sign in Pulmonary Mucormyosis
 QJM Advance Access published February 6, 2014 Reverse Halo Sign in Pulmonary Mucormyosis Yu-Hsiang Juan MD 1,2, Sachin S Saboo, MD FRCR 1, Yu-Ching Lin MD 2, James R. Conner MD, Ph.D 3, Francine L. Jacobson
QJM Advance Access published February 6, 2014 Reverse Halo Sign in Pulmonary Mucormyosis Yu-Hsiang Juan MD 1,2, Sachin S Saboo, MD FRCR 1, Yu-Ching Lin MD 2, James R. Conner MD, Ph.D 3, Francine L. Jacobson
Case Report A Unique Case of Left Second Supernumerary and Left Third Bifid Intrathoracic Ribs with Block Vertebrae and Hypoplastic Left Lung
 Volume 2013, Article ID 620120, 4 pages http://dx.doi.org/10.1155/2013/620120 Case Report A Unique Case of Left Second Supernumerary and Left Third Bifid Intrathoracic Ribs with Block Vertebrae and Hypoplastic
Volume 2013, Article ID 620120, 4 pages http://dx.doi.org/10.1155/2013/620120 Case Report A Unique Case of Left Second Supernumerary and Left Third Bifid Intrathoracic Ribs with Block Vertebrae and Hypoplastic
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Fungi More or Less Obligately Associated with Humans. Requirements for Designating a Mycosis*
 P Fungi More or Less Obligately Associated with Humans a. a few dermatophytes (the anthropophilic species ) b. Malassezia furfur c. Candida albicans d. + Lacazia (Loboa) loboi*p e. + Pneumocystis jirovecii*p
P Fungi More or Less Obligately Associated with Humans a. a few dermatophytes (the anthropophilic species ) b. Malassezia furfur c. Candida albicans d. + Lacazia (Loboa) loboi*p e. + Pneumocystis jirovecii*p
Case Studies in Fungal Infections and Antifungal Therapy
 Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
HIV-associated Pulmonary Disease. Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond QUESTION: HIV-associated Pulmonary Diseases
 Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Review Article Correlation between Clinical Characteristics and Chest Computed Tomography Findings of Pulmonary Cryptococcosis
 Pulmonary Medicine Volume 2015, Article ID 703407, 7 pages http://dx.doi.org/10.1155/2015/703407 Review Article Correlation between Clinical Characteristics and Chest Computed Tomography Findings of Pulmonary
Pulmonary Medicine Volume 2015, Article ID 703407, 7 pages http://dx.doi.org/10.1155/2015/703407 Review Article Correlation between Clinical Characteristics and Chest Computed Tomography Findings of Pulmonary
Clinical Practice Guidelines for the Management of Blastomycosis: 2008 Update by the Infectious Diseases Society of America
 IDSA GUIDELINES Clinical Practice Guidelines for the Management of Blastomycosis: 2008 Update by the Infectious Diseases Society of America Stanley W. Chapman, 1 William E. Dismukes, 2 Laurie A. Proia,
IDSA GUIDELINES Clinical Practice Guidelines for the Management of Blastomycosis: 2008 Update by the Infectious Diseases Society of America Stanley W. Chapman, 1 William E. Dismukes, 2 Laurie A. Proia,
Common things are common, but not always the answer
 Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
ESCMID Online Lecture Library. by author. CASE PRESENTATION ECCMID clinical grand round May Anat Stern, MD Rambam medical center Haifa, Israel
 CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
Case Report Chronic Lipoid Pneumonia in a 9-Year-Old Child Revealed by Recurrent Chest Pain
 Case Reports in Pediatrics Volume 2015, Article ID 402926, 4 pages http://dx.doi.org/10.1155/2015/402926 Case Report Chronic Lipoid Pneumonia in a 9-Year-Old Child Revealed by Recurrent Chest Pain A. Hochart,
Case Reports in Pediatrics Volume 2015, Article ID 402926, 4 pages http://dx.doi.org/10.1155/2015/402926 Case Report Chronic Lipoid Pneumonia in a 9-Year-Old Child Revealed by Recurrent Chest Pain A. Hochart,
Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections.
 In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
Fungi. Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy:
 Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy:") MYCOLOGY Mycology I Fungi Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy: Morphology Spore formation FFungi Yeast Mold Yeastlike
MYCOLOGY Mycology I Fungi Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy: Morphology Spore formation FFungi Yeast Mold Yeastlike
Chapter 18. Fungal Diseases of the Lung. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 18 Fungal Diseases of the Lung 1 YLS S M AC Figure 18-1. Fungal disease of the lung. Cross-sectional view of alveoli infected with Histoplasma capsulatum. AC, alveolar consolidation; M, alveolar
Chapter 18 Fungal Diseases of the Lung 1 YLS S M AC Figure 18-1. Fungal disease of the lung. Cross-sectional view of alveoli infected with Histoplasma capsulatum. AC, alveolar consolidation; M, alveolar
Case Report Pulmonary Sarcoidosis following Etanercept Treatment
 Case Reports in Rheumatology Volume 2012, Article ID 724013, 4 pages doi:10.1155/2012/724013 Case Report Pulmonary Sarcoidosis following Etanercept Treatment Kuljeet Bhamra and Richard Stevens Department
Case Reports in Rheumatology Volume 2012, Article ID 724013, 4 pages doi:10.1155/2012/724013 Case Report Pulmonary Sarcoidosis following Etanercept Treatment Kuljeet Bhamra and Richard Stevens Department
Case Report Diagnostic Challenges of Tuberculous Lymphadenitis Using Polymerase Chain Reaction Analysis: A Case Study
 Case Reports in Infectious Diseases Volume 2015, Article ID 723726, 4 pages http://dx.doi.org/10.1155/2015/723726 Case Report Diagnostic Challenges of Tuberculous Lymphadenitis Using Polymerase Chain Reaction
Case Reports in Infectious Diseases Volume 2015, Article ID 723726, 4 pages http://dx.doi.org/10.1155/2015/723726 Case Report Diagnostic Challenges of Tuberculous Lymphadenitis Using Polymerase Chain Reaction
R. F. Falkenstern-Ge, 1 S. Bode-Erdmann, 2 G. Ott, 2 M. Wohlleber, 1 and M. Kohlhäufl Introduction. 2. Histology
 Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication for Repeat Metastasectomy
 Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report of Neoadjuvant Use Enabling Complete Surgical Resection
 Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Nitrofurantoin-Induced Lung Toxicity
 Severe Nitrofurantoin-Induced Lung Toxicity Rami Jambeih, M.D. 1, John Flesher, M.D. 1,3, Joe J. Lin, M.D. 2,4 University of Kansas School of Medicine Wichita 1 Department of Internal Medicine 2 Department
Severe Nitrofurantoin-Induced Lung Toxicity Rami Jambeih, M.D. 1, John Flesher, M.D. 1,3, Joe J. Lin, M.D. 2,4 University of Kansas School of Medicine Wichita 1 Department of Internal Medicine 2 Department
Case Report Pulmonary Hilar Tumor: An Unusual Presentation of Sclerosing Hemangioma
 Volume 2016, Article ID 8919012, 4 pages http://dx.doi.org/10.1155/2016/8919012 Case Report Pulmonary Hilar Tumor: An Unusual Presentation of Sclerosing Hemangioma Jui-Hung Hung, Ching Hsueh, Chiung-Ying
Volume 2016, Article ID 8919012, 4 pages http://dx.doi.org/10.1155/2016/8919012 Case Report Pulmonary Hilar Tumor: An Unusual Presentation of Sclerosing Hemangioma Jui-Hung Hung, Ching Hsueh, Chiung-Ying
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal and Anterior Mediastinal Abscess
 Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis
 Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis Identify the structures neutrophils macrophages x40 Organisms 8 30 micron in size, with variable capsule
Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis Identify the structures neutrophils macrophages x40 Organisms 8 30 micron in size, with variable capsule
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Epidemiology and ecology of fungal diseases
 Epidemiology and ecology of fungal diseases Healthcare Focus on: - individual - diagnosis - treatment Public Health Focus on: - population - prevention The nature of fungi Kingdom Fungi (lat. fungus, -i)
Epidemiology and ecology of fungal diseases Healthcare Focus on: - individual - diagnosis - treatment Public Health Focus on: - population - prevention The nature of fungi Kingdom Fungi (lat. fungus, -i)
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Voriconazole Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 4004 Table of Contents Coverage Policy... 1 General Background...
Cigna Drug and Biologic Coverage Policy Subject Voriconazole Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 4004 Table of Contents Coverage Policy... 1 General Background...
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS
 MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy
 Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
HIV related pulmonary infections. A radiologic pictorial review.
 HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
Mycobacteria and fungal infections of the respiratory tract
 Before you start: You must read the slides! The Dr. did not bother to explain them all Mycobacteria and fungal infections of the respiratory tract - TB is a global problem that the WHO is trying to combat.
Before you start: You must read the slides! The Dr. did not bother to explain them all Mycobacteria and fungal infections of the respiratory tract - TB is a global problem that the WHO is trying to combat.
Clinico-Pathologic Conferences Early Bronchus-Associated Lymphoid Tissue Lymphoma Diagnosed with Immunoglobulin Heavy Chain Molecular Testing
 Canadian Respiratory Journal Volume 2016, Article ID 7056035, 4 pages http://dx.doi.org/10.1155/2016/7056035 Clinico-Pathologic Conferences Early Bronchus-Associated Lymphoid Tissue Lymphoma Diagnosed
Canadian Respiratory Journal Volume 2016, Article ID 7056035, 4 pages http://dx.doi.org/10.1155/2016/7056035 Clinico-Pathologic Conferences Early Bronchus-Associated Lymphoid Tissue Lymphoma Diagnosed
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Multiple bilateral pulmonary nodules masquerading as pulmonary metastasis; a case of nodular sarcoidosis
 Electronic Physician (ISSN: 2008-5842) August 2016, Volume: 8, Issue: 8, Pages: 2802-2806, DOI: http://dx.doi.org/10.19082/2802 Multiple bilateral pulmonary nodules masquerading as pulmonary metastasis;
Electronic Physician (ISSN: 2008-5842) August 2016, Volume: 8, Issue: 8, Pages: 2802-2806, DOI: http://dx.doi.org/10.19082/2802 Multiple bilateral pulmonary nodules masquerading as pulmonary metastasis;
Indre Vengalyte MD¹, Regina Pileckyte MD¹, Laimonas Griskevicius MD PhD 1, 2
 ASPERGILLUS GALACTOMANNAN (GM) ANTIGEN IN THE BRONCHOALVEOLAR LAVAGE (BAL) FLUID FOR THE DIAGNOSIS OF INVASIVE PULMONARY ASPERGILLOSIS (IPA) IN HEMATOLOGICAL PATIENTS Indre Vengalyte MD¹, Regina Pileckyte
ASPERGILLUS GALACTOMANNAN (GM) ANTIGEN IN THE BRONCHOALVEOLAR LAVAGE (BAL) FLUID FOR THE DIAGNOSIS OF INVASIVE PULMONARY ASPERGILLOSIS (IPA) IN HEMATOLOGICAL PATIENTS Indre Vengalyte MD¹, Regina Pileckyte
Common Fungi. Catherine Diamond MD MPH
 Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Diagnosis of Invasive Septate Mold Infections A Correlation of Microbiological Culture and Histologic or Cytologic Examination
 Microbiology and Infectious Disease / DIAGNOSIS OF SEPTATE MOLD INFECTIONS Diagnosis of Invasive Septate Mold Infections A Correlation of Microbiological Culture and Histologic or Cytologic Examination
Microbiology and Infectious Disease / DIAGNOSIS OF SEPTATE MOLD INFECTIONS Diagnosis of Invasive Septate Mold Infections A Correlation of Microbiological Culture and Histologic or Cytologic Examination
generalised lymphadenopathy presenting with shortness of breath and infiltrates on chest
 Abhishek Biswas 1, Herman Gaztambide 1, Dara N. Wakefield 2, Peruvemba S. Sriram 1 abiswas@ufl.edu 1 University of Florida, Division of Pulmonary Critical Care and Sleep Medicine, Gainesville, FL, USA.
Abhishek Biswas 1, Herman Gaztambide 1, Dara N. Wakefield 2, Peruvemba S. Sriram 1 abiswas@ufl.edu 1 University of Florida, Division of Pulmonary Critical Care and Sleep Medicine, Gainesville, FL, USA.
Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus Irinotecan and Radiotherapy
 Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Pneumonia in immunosuppressed patients
 Blackwell Science, LtdOxford, UKRESRespirology1323-77992004 Blackwell Science Asia Pty LtdMarch 20049S1S25S29Original ArticlePneumonia in immunosuppressed patientss Kohno et al. Respirology (2004) 9, S25
Blackwell Science, LtdOxford, UKRESRespirology1323-77992004 Blackwell Science Asia Pty LtdMarch 20049S1S25S29Original ArticlePneumonia in immunosuppressed patientss Kohno et al. Respirology (2004) 9, S25
Eastern Mediterranean Health Journal, Vol. 14, No. 5,
 Eastern Mediterranean Health Journal, Vol. 14, No. 5, 2008 1217 Case report Inappropriate use of steroid and Pneumocystis jiroveci pneumonia: report of two cases P. Tabarsi, 1 M. Mirsaeidi, 1 M. Amiri,
Eastern Mediterranean Health Journal, Vol. 14, No. 5, 2008 1217 Case report Inappropriate use of steroid and Pneumocystis jiroveci pneumonia: report of two cases P. Tabarsi, 1 M. Mirsaeidi, 1 M. Amiri,
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Pulmonary blastomycosis presenting as primary lung cancer
 Hussaini et al. BMC Infectious Diseases (2018) 18:336 https://doi.org/10.1186/s12879-018-3244-0 CASE REPORT Open Access Pulmonary blastomycosis presenting as primary lung cancer Syed Mohammed Qasim Hussaini
Hussaini et al. BMC Infectious Diseases (2018) 18:336 https://doi.org/10.1186/s12879-018-3244-0 CASE REPORT Open Access Pulmonary blastomycosis presenting as primary lung cancer Syed Mohammed Qasim Hussaini
Devendra V. Kulkarni, Rahul G. Hegde, Ankit Balani, and Anagha R. Joshi. 2. Case Report. 1. Introduction
 Case Reports in Radiology, Article ID 614647, 4 pages http://dx.doi.org/10.1155/2014/614647 Case Report A Rare Case of Pulmonary Atresia with Ventricular Septal Defect with a Right Sided Aortic Arch and
Case Reports in Radiology, Article ID 614647, 4 pages http://dx.doi.org/10.1155/2014/614647 Case Report A Rare Case of Pulmonary Atresia with Ventricular Septal Defect with a Right Sided Aortic Arch and
Clinical Manifestations of HIV
 HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
Accurate Diagnosis Of Postoperative Pneumonia Requires Objective Data
 Accurate Diagnosis Of Postoperative Pneumonia Requires Objective Data David Ebler, MD David Skarupa, MD Andrew J. Kerwin, MD, FACS Jhun de Villa, MD Michael S. Nussbaum, MD, FACS J.J. Tepas III, MD, FACS
Accurate Diagnosis Of Postoperative Pneumonia Requires Objective Data David Ebler, MD David Skarupa, MD Andrew J. Kerwin, MD, FACS Jhun de Villa, MD Michael S. Nussbaum, MD, FACS J.J. Tepas III, MD, FACS
Case Presentation. Intern Tutor VS 2007/01/26
 Case Presentation Intern 8931150 Tutor VS 2007/01/26 About The Patient 38 years old worker ID: M120794700 Admission date: 2006/12/28 C.C.: Fever with headache for 2 days Present Illness Smoker, alcoholism
Case Presentation Intern 8931150 Tutor VS 2007/01/26 About The Patient 38 years old worker ID: M120794700 Admission date: 2006/12/28 C.C.: Fever with headache for 2 days Present Illness Smoker, alcoholism
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
 Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old