Lipoprotein (a) Thomas Dayspring MD, FACP
|
|
|
- Hortense Hamilton
- 5 years ago
- Views:
Transcription

1 Lipoprotein(a) / Lp(a) Measurement, Risk & Treatment an evolving story James A. Underberg, MS, MD, FACPM, FACP, FASH, FNLA Clinical Assistant Professor of Medicine NYU School of Medicine NYU Center for Prevention of Cardiovascular Disease Director, Bellevue Hospital Lipid Clinic, New York, NY Treasurer, National Lipid Association Slides Courtesy of Tom Daysping Disclosures Consultant: Aegerion Pharmaceuticals, Amarin, Amgen, AstraZeneca, Eli Lilly & Co., Genzyme, Sanofi, Alexion, Synageva, Recombine Contracted research: Aegerion, Genzyme, Pfizer Advisory board: Amgen, Aegerion, Sanofi, Regeneron, Genzyme,Akcea, Kowa Pharmaceuticals, Speakers bureau: Amgen, Genzyme, Aegerion, Regeneron, AstraZeneca, Merck & Co., Inc., Alexion/Synageva Lipoprotein (a) or Lp(a) Lipoprotein (a) is a lipid trafficking particle with structural similarity to low density lipoprotein (LDL) in that it has a core consisting of hydrophobic cholesteryl esters and triacylgycerols surrounded by a surface of amphipathic phospholipids and unesterified cholesterol Lp(a) like LDL has as its structural apolipoprotein a large peptide called apoprotein B 100 but differs as it also has bound on a 1:1 molar basis via a disulfide bond another protein called apoprotein (a) Scanu AM. N Engl J Med 2003;349;22:
 Phospholipids Surface Free cholesterol Core lipids (cholesteryl ester and triglycerides Adapted from Kostner KM et al.")
 are both composed of chains of kringles Scanu AM.")
2 Lipoprotein (a) or Lp(a) The disulfide bridge links Cys4326 in apob- 100 with the only free Cys4057 in apo(a), located in kringle four (K-IV) type 9 Disulfide bond S S H 2N Apolipoprotein B 100 HO O C Apolipoprotein (a) Phospholipids Surface Free cholesterol Core lipids (cholesteryl ester and triglycerides Adapted from Kostner KM et al. European Heart Journal (2013) 34, Lipoprotein (a) or Lp(a) There is significant heterogeneity (amino acid composition) of apoprotein(a) within and among persons with molecular weights ranging between 300 and 800 kd The amino acids are located in looped peptide chains called kringles Plasminogen and apoprotein (a) are both composed of chains of kringles Scanu AM. N Engl J Med 2003;349;22: Plasminogen Structure The characteristic glycoprotein component of plasminogen has a unique structure consisting of repetitive protein segments called kringles (I-V) III II IV V Active protease domain S S Kringle I Plasminogen S-S S-S Each kringle is stabilized by three internal disulfide bonds that produce the typical triple-loop structural motif referred to as a kringle The Kringle domains interact with plasminogen activators and plasmin binding sites on endothelial surfaces 2
 can have from 17 to > 30 kringles 110 E 1 A E 10 V 90 E 100 C =")
 domain, one copy of kringle V domain, and an inactive protease domain There are")
3 Typical Extended Kringle S R 30 G T T G 20 Y S G T D P 80 T Y S S Q W M R W Y E 70 P Y N L T D P N R 40 P H Y 60 N L H G R 50 Y P N Kringles contain approximately 80 amino acids that are crosslinked by 3 internal disulfide bonds Having three cross links within such a small domain distorts it, creating the kringle shape Apo(a) can have from 17 to > 30 kringles 110 E 1 A E 10 V 90 E 100 C = cysteine O HS OH NH 2 Letters represent various amino acids Gotto & Pownall Manual of Lipid Disorders Lippincott 1999 Apoprotein (a) Apo(a) comprises three distinct structural domains, each of which shares a high degree of sequence identity with plasminogen: multiple copies of the plasminogen-like like kringle IV (4) domain, one copy of kringle V domain, and an inactive protease domain There are 10 different types of kringle IV (4) domains, numbered 1-10, 10, each present in a single copy except for the type 2 repeat Kringle IV subtypes are listed as KIV (n) or KIV-(n) or K4(n) where n = Kringle IV type 2 (KIV-2, KIV 2 or K4-2) varies from 3 to 40 repeats in the apo(a) alleles and is responsible for the intra- and interindividual size heterogeneity of apo(a) and Lp(a) mass Kringles are reported as type 1-5 or I - V Scanu AM. N Engl J Med 2003;349;22: Plasminogen and Apoprotein (a) Structure III II IV V Plasminogen Active protease domain The Kringle domains interact with plasminogen activators and plasmin binding sites on endothelial surfaces I Inactive protease domain IV 1 IV 2 On KIV 9 Disulfide bond links to apob S S V Apoprotein(a) IV 10 IV 3 IV 9 IV4 IV5 IV 6 IV7 IV 8 Variable size of K-IV 2 repeat domain (at least 30 alleles) results in over 500 phenotypically different forms of apo(a) Lysine binding domain on KIV 10 3
4 2010 European Atherosclerosis Society Consensus Panel on Lp(a) Apolipoprotein(a) genotype, which determines both the synthetic rate and size of the apolipoprotein(a) moiety of Lp(a), alone accounts for 90% of plasma concentrations of Lp(a) Hepatic secretion rates are lower for large apolipoprotein(a) isoforms As most individuals are heterozygous for two different isoforms, the smallest isoform typically predominates in plasma Nordesgaard BG et al. Eur Heart J Dec;31(23): Lipoprotein (a) Assembly Upon maturation, intracellular apo(a) reaches the Golgi and is secreted in a mature form as a glycoprotein, most probably without being attached to LDL The genetically determined size of apo(a) reflecting the number of K-IV repeats correlates with the intracellular residence time and thus, small isoforms are secreted much faster when compared with large isoforms explaining the reason for the inverse correlation between apo(a) size and plasma Lp(a) Assembly of Lp(a) from apo(a) and LDL is a two-step process In the first step, specific K-IVs of apo(a), mostly K-IV types 3 6 non-covalently bind to lysine groups of apo B in LDL This binding is still reversible Kostner KM et al. Eur Heart J 2013;34: Oxidized Phospholipids on Lp(a) + NH 3 Lysine O H 3N Oxidized + phospholipid O Lysine binding domains Apolipoprotein(a) Lp(a) Kringle loops Modified Lp(a) lipoprotein, which accumulates in atherosclerotic lesions traffics oxidized phospholipids at its lysine binding domains Berliner JA et al. NEJM 2005;351:9-11 4
5 Lipoprotein (a) or Lp(a) Apolipoprotein (a) K IV 1 2n V P N C The length of apolipoprotein (a) is genetically determined, indicated by the break in the line at K IV-2; its variability (3-40 copies) has an effect on the density of Lp(a) lipoprotein The more the number of KIV-2 repeats, the higher the molecular weight of Lp(a) or conversely the fewer the lower the MW will be Scanu AM. N Engl J Med 2003;349;22: Comparison of Plasminogen and Apo(a) cdnas A signal sequence, is a short (5-30 amino acids long) peptide present at the N-terminus of the majority of newly synthesized proteins Plasminogen Gene MW ~ 90 kda SS T P 3 Complementary DNA (cdna) is doublestranded DNA synthesized from a messenger RNA (mrna) template Apoprotein (a) Gene MW ~ kda 5 SS P 3 % sequence identity SS = signal sequence; T = tail region; 1-5 = kringle 1-5; P = protease domain GawA, Hobbs H. Chapter 6 in Lipoproteins in Health and Disease Arnold & Oxford University Press 1999 Lipoprotein (a) Based on genetic evidence provided by studies conducted over the last two decades, Lp(a), is now considered to be the strongest genetic risk factor for coronary heart disease (CHD) with > a 90% heritability in Europeans and Africans Alleles with a low kringle IV copy number that together have a population frequency of 25 35% are associated with a doubling of the relative risk for outcomes, which is exceptional in the field of complex genetic phenotypes Lp(a) mass concentrations remain relatively stable over an individual's lifetime and are unaffected by age and gender 1000-fold intra-population range (from 0 to >200 mg dl1) and fourfold inter-population range with a skewed distribution in most populations (majority of Europeans have concentrations below 10 mg dl) Kronenburg F et al J Int Med 2013;273(1):6-30 5
6 Apoprotein (a) With codominant inheritance almost everyone and their progeny has the LPA gene but only ~ one third of patients will have an at-risk plasma mass concentration of the protein apo(a) Previous assumption was that more than 90% of the variance of LP(a) mass was under genetic control but newer data suggest ~ one third of the variation is due to heterogeneity of the Lp(a) locus, meaning the KIV-2 makeup of LPA is not the only determinant of Lp(a) mass concentration Single nucleotide polymorphisms (SNPs) are also at play and as has been the case with other lipids it is likely that additional apo(a) modifying genes or even epigenetic factors yet to be discovered have an effect Kronenberg F & Utermann G. J Intern Med 2013;273:6-30 LDL and Lp(a) Peak Density LDL Lp(a) Plasma from 75 subjects, obtained at the time of entry into the study, was subjected to density gradient ultracentrifugation, and the densities of the LDL & Lp(a) peak fractions were measured for each subject Peak density gm/ml Nakjima K et al. ATVB 2001;21: Chromosome 6 Lipoprotein (a) Genetics The specific genetics of Lp(a) are significantly more complex than classic lipid monogenic disorders like autosomal dominant or recessive familial hypercholesterolemia (FH) Codominant Inheritance: two alleles of a gene pair in a heterozygote both have full phenotypic expression: Heterozygotes for Kringle IV Type 2 (KIV-2) repeats have 2 different Lp(a) particles in their plasma (which can be physically separated) Lp(a) mass is largely controlled by a size polymorphism of the LPA gene on chromosome 6q26-q27 q27 and of the apo(a) protein (>30 alleles and isoforms) which control the Copy Number Variation (CNV) of KIV-2 in LPA (apoprotein a) 6q Kronenburg F et al J Int Med 2013;273(1):6-30 6
7 Lipoprotein (a) Genetics Chromosome 6 The incidence of at-risk Lp(a) mass concentration depends on what level is defined as high risk: If 30 mg/dl is used then ~30 % (1 in 3) of Caucasians (100 million in the US) As many as 50% of African Americans (~12 million) have an at-risk Lp(a) concentration > 30 mg/dl Two LPA variants or single nucleotide polymorphisms (SNPs), namely rs , which is a noncoding intronic SNP, and rs which is a missense variant are the SNPs that are most consistently associated with both plasma Lp(a) levels and CHD risk 6q Kronenburg F et al J Int Med 2013;273(1):6-30. Clark R et al. N Engl J Med 2009;361: European Atherosclerosis Society Consensus Panel on Lp(a) Fraction of population Men 30% (levels > 30 mg/dl) 20% (levels > 50 mg/dl) Women 30% (levels > 30 mg/dl) 20% (levels > 50 mg/dl) Green color indicates levels below the 80th percentile, whereas red color indicates levels above the 80th percentile Lp(a) mg/dl Lp(a) mg/dl Typical distributions of lipoprotein(a) levels in the general population. These graphs are based on non-fasting fresh serum samples from 3000 men and 3000 women from the Copenhagen General Population Study collected from 2003 through 2004 adapted from NordesgaardBG et al. Eur Heart J Dec;31(23): Multi-Ethnic thnic Study of Atherosclerosis (MESA) Histograms of Lp(a) Mass Distribution 25 th %ile Mean 75 th %ile Blacks Caucasians Lp(a) (mg/dl) Lp(a) (mg/dl) 50 Histograms mg/dl cut point of identifies Lp(a) distribution CHD risk in frequency 3 of 4 races/ethnicities, and quartile box but the plots lower of 30 mg/dl Lp(a) cut point levels may in be the more Black appropriate and Caucasian for detecting groups CHD risk for black individuals The left and right box edges correspond to 25% and 75% percentiles, and the vertical line within the box indicates the median level Guan W, et al. ATVB 2015;35:
8 Atherosclerosis Risk in Communities (ARIC) Study Lipoprotein (a), Ethnicity & Cardiovascular Risk CVD Caucasian CHD Stroke African American African American Caucasian African American Caucasian Hazard Ratio per standard deviation increase in log-transformed Lp(a) mass values Lp(a) levels in ARIC were significantly higher among the black group than the white group, and in both populations, increasing Lp(a) levels tended to correlate positively with low-density lipoprotein cholesterol and negatively with triglycerides Increasing quintiles of Lp(a) were just as predictive of future cardiovascular disease in the black population as in the white population Paul Ridker Circulation 2012, 125: Relationship Between Apo(a) Isoform Size & Lp(a) Mass in a Caucasian Population Lp(a) mass (mg/dl) Isoform MW: kda Frequency B S1 S2 S3 S % 12% 28% 26% 31% The larger isoforms (S1-4) are associated with lower plasma Lp(a) mass concentrations are most common in Caucasian populations The smaller (F & B) isoforms are associated with higher plasma concentrations of Lp(a) mass MW = molecular weight, B = Smaller isoforms, S = Larger isoforms Utermann Science 1989;246(4932): Lipoprotein (a) Particles Apo(a) Isoforms: Kringle IV-2 Copy Variation Lp(a) mass is the cumulative mass of apo(a), apo(b), other LDL proteins, phospholipids, free cholesterol, cholesteryl ester, triglycerides and other lipid moieties K IV, Type 1 Protease domain Disulfide bond K V K IV, Types 3-10 Apo B 100 K IV, Type 2 K IV, Type 1 12 Kringles K IV, Type 2 35 Kringles K IV, Types 3-10 Apo B 100 Disulfide bond Low MW apo(a) K V Protease domain High MW apo(a) 8
9 Lipoprotein (a) Lipoprotein (a) Heterogeneity Small Dense LDL Buoyant LDL? Highest atherogenic potential Large apo (a) isoform Small apo (a) isoform Both apo(a) and the particles of LDL that are found in Lp(a) lipoprotein also vary in size Scanu AM. N Engl J Med 2003;349;22: K IV, Type 1 Apo B100 K IV, Type 2 B A Understand that apoprotein (a) size has nothing to do with LDL particle size D Disulfide bond K IV, Types 3-10 KV Protease domain C Lp(a) Testing Apo(a) mass Lp(a)-C Variable: High & low molecular weight Variable: particle cholesterol mass Cholesterol Cholesteryl ester Phospholipids Lp(a) mass Lp(a)-P Multiple variables No variables Triglyceride 9
10 Lipoprotein(a)-P versus Lp(a) mass Concentrations Lp(a)-P (nmol/l) MW = HIGH MW = MW = LOW Lp(a) isoform sizes determined by Western blot analysis Lp(a) mass (mg/dl) 250 Comparison of Lipo- IFE Lp(a)-P concentrations with Lp(a) mass for samples of large (blue, n=51), intermediate (green, n=25)) and small (red, n=38) isoforms Because the Lipo- IFE concentration assay is not influenced by isoform size, the difference in slopes observed here indicates that the mass assay is influenced by isoform size Guadagno PA et al Clin Chim Acta 2015;439: Bruneck Study Lp(a) & Risk of Advanced Atherogenesis n = Adjusted OR n = n = 14 n = 189 High Low Lp(a) concentration: Cutoff 32 mg/dl Risk of advanced atherogenesis (incident stenosis >40%) according to 4 categories built by Low and high Lp(a) mass (cutoff, 32 mg/dl) HMW and LMW apo(a) phenotypes (cutoff, 22 K-IV repeats) ORs adjusted for age, ferritin, factor V Leiden, fibrinogen, diabetes, LDL, HTN, smoking & alcohol, antithrombin III Kronenberg F, et al. Circulation. 1999;100; OR of incident stenosis OR of incident stenosis n = Lp(a) mg/dl > 40 Kringle IV Repeats 3.5 ( ) p< ( ) p<0.01 > n = 32 HMW LMW HMW LMW ( ) p<0.01 ( ) p< Bruneck Study Lp(a) & Risk of Advanced Atherogenesis Risk of advanced atherogenesis (incident stenosis > 40%) according to categories of Lp(a) concentrations apo(a) phenotypes Graph demonstrates a binary type of association with a clear cutoff at 32 mg/dl of Lp(a) concentration and 22 K-IV repeats (the low MW isoforms) ORs adjusted for age, ferritin, factor V Leden, fibrinogen, diabetes, LDL, HTN, smoking & alcohol, antithrombin III Kronenberg F, et al. Circulation. 1999;100;
 concentration 7 35-37 5 > 37 Mean Lp(a) concentration in various groups of subjects stratified by the number")
11 Lipoprotein (a) Mass Concentrations Lp(a) mg/dl Low (LMW) Molecular Weight of Apo(a) High (HMW) Number of KIV Repeats There is a clear inverse correlation between the number of KIV repeats and Lp(a) concentration > 37 Mean Lp(a) concentration in various groups of subjects stratified by the number of kringle (K) IV (KIV) repeats; KIV repeats are considered as low molecular weight (LMW) or small isoforms and those with >22 KIV repeats are considered as high molecular weight (HMW) or large apolipoprotein(a) [apo(a)] isoforms Kronenberg F et al. J Int Med 2013 LDL-cholesterol (LDL-C) Direct Calculated LDL-cholesterol LDL-cholesterol is the cholesterol is the cholesterol trafficked within trafficked all of the within low all density of the lipoproteins low and intermediate and Lp(a) in density lipoproteins a deciliter in of a plasma deciliter of plasma IDL apoe LDL Apo(a) Lp(a) apob apob apob IDL-C + LDL-C + Lp(a) (a)-c Calculated Direct LDL-Cholesterol Lipoprotein (a) Metabolism 11
12 In two different cell lines (HEK293 & HeLA) Lp(a) is a ligand for the SR- BI receptor Both cell lines when transfected with SR-BI showed increased association with Lp(a) SR-BI can promote the selective lipid uptake of CEs from Lp(a), as it does from other lipoproteins although SR-BI appears to preferentially promote the uptake of CE, a neutral core lipid Lp(a) and not LDL has also been shown to be the principal carrier of negatively charged oxidized lipids in plasma and enrichment of anionic charged lipids has been shown to enhance the uptake of lipoproteins by SR-BI Thus, negatively charged oxidized lipids could potentially explain the affinity of Lp(a) for SR-BI J Lipid Res 2013;54: Overexpression of the low-density lipoprotein (LDL) receptor (LDLr) in HepG2 cells dramatically increased the internalization of Lp(a) Internalization of Lp(a) was markedly reduced following treatment of HepG2 cells with a function-blocking monoclonal antibody against the LDLr or the use of primary human fibroblasts from an individual with familial hypercholesterolemia; in both cases, Lp(a) internalization was not affected by PCSK9 Lp(a) internalization by hepatic HepG2 cells and primary human fibroblasts was effectively reduced by PCSK9 Optimal Lp(a) internalization in both hepatic and primary human fibroblasts was dependent on the LDL rather than the apolipoprotein(a) component of Lp(a) Romagnuolo R et al. J Biol Chem 2015;290: Adapted from J Biol Chem 2015;290: K IV, Type 1 Apo B 100 K IV, Type 2 Apo B 100 Apo(a) Lp(a) LDL K IV Types 3-10 K V Protease domain Plasminogen receptors LDL receptors Romagluono J Biolog Chem
 <Median Lp(a) > Median Lp(a) <Median Lp(a) > Median 0.25 0.5 1.0 2.0 Primary Endpoint + Total Mortality 0.25 0.5 1.0 2.0 Khera A et al. Circulation.")
13 Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin ( JUPITER) Study: Lp(a) Median overall value = 23, 60 mg/dl (Caucasians, Blacks) Primary Endpoint Lp(a) <Median Lp(a) > Median Lp(a) <Median Lp(a) > Median Primary Endpoint + Total Mortality Khera A et al. Circulation. 2014;129: Efficacy of rosuvastatin according to baseline lipoprotein(a) concentration Hazard ratios and 95% confidence intervals according to intention-to-treat analysis for the primary endpoint (top) and the expanded endpoint (bottom) by baseline lipoprotein(a) mass concentrations For the primary endpoint, hazard ratio with rosuvastatin therapy was 0.47 (95%CI ) for participants with baseline Lp(a) mass concentration below the median and 0.62 (95%CI ) in those above the median (p-interaction = 0.33) Similarly, for the expanded endpoint, hazard ratios were 0.46 (95%CI ) and 0.72 (95%CI ) for those below and above the median respectively (p-interaction = 0.10) Although the median change in Lp(a) mass with rosuvastatin and placebo was zero, rosuvastatin nonetheless resulted in a small but statistically significant positive shift in the overall Lp(a) distribution (P<0.0001) Effect of Statins on LDL-receptor and PCSK9 Statin Lysosomal Degradation oxysterols SREBP-2 LDLr PCSK9 SREBP-2 Sterol regulatory element binding protein - 2 Konrad RJ et al. Lipids Health Dis. 2011;10:38 Atherothrombosis Intervention in Metabolic Syndrome with Low HDL-C/High Triglyceride and Impact on Global Health Outcomes (AIM-HIGH) The principal findings of our study were at 1 year, compared to the placebo group, those randomized to ERN had significantly higher apoa-i levels, a lower apob/apoa-i ratio, and lower levels of Lp(a) Despite these favorable changes with ERN, apoa-1, apob, and Lp(a) variables did not identify any subgroup of participants who benefited from ERN therapy Baseline and on-study Lp(a) predicted CV events in both the control LDL-lowering therapy plus placebo and LDL lowering therapy plus ERN arms, suggesting that Lp(a) still contributes to residual CV risk in patients achieving target LDL-C levels with statin therapy Albers JJ et al. Am Coll Cardiol 2013;62:
 mean (95% confidence interval) dose-related reductions in Lp(a) compared to control: 29.5% (23.3% to 35.7%) and 24.5% (20.4% to 28.")

14 Current therapeutic options to reduce Lp(a) are limited Evolocumab treatment for 12 weeks resulted in significant (p < 0.001) mean (95% confidence interval) dose-related reductions in Lp(a) compared to control: 29.5% (23.3% to 35.7%) and 24.5% (20.4% to 28.7%) with 140 mg and 420 mg, dosed every 2 and 4 weeks, respectively, with no plateau of effect Lp(a) reductions were significantly correlated with percentages of reductions in LDL-C and apolipoprotein B Mean percentage reductions did not differ based on age or sex but the trend was greater in those patients taking statins Raal FJ et al. JACC 2014;63: Evolocumab-induced Lp(a) Percentage Change from Baseline to 12 weeks Lipoprotein (a) mass Percentage Change from Baseline Evolocumab Q 2 wks Evolocumab Q 4 wks 70 mg 105 mg 140 mg 280 mg 350 mg 420 mg -13.8* -18.7* -21.3* -24.5* -25.2* -29.5* Current therapeutic options to Statistically significant mean reductions in Lp(a) mass were observed with all doses of evolocumab compared with those of control. Leastsquares mean differences (95% CI) from ANCOVA model are shown with last observation carried forward (LOCF) imputation Treatment difference within each dose frequency group used control in the same frequency group as the reference *p < Raal FJ et al. JACC 2014;63: Model for receptor-mediated catabolism of apo(a) and Lp(a). Koschinsky ML, Biol Chem 2015;290:

 and OxPL-apoB")

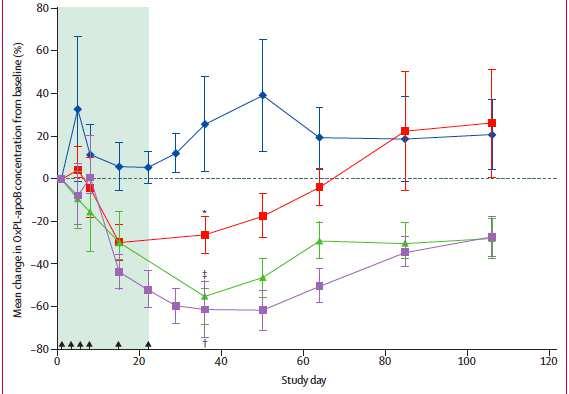
15 Sotirios Tsimikas, Lancet 2015; 386: Mean percent change in Lp(a) and OxPL-apoB with time by treatment group in the multi-dose cohorts Sotirios Tsimikas, Lancet 2015; 386:
 is a risk factor for ASCVD, Aortic Stenosis and Thrombotic disease Family screening is important when index patients identified The")
16 Effect of mipomersen and ISIS on Lp(a) and apo(a) plasma levels. Sotirios Tsimikas, JLR Accessed online Feb Summary Lp(a) is a risk factor for ASCVD, Aortic Stenosis and Thrombotic disease Family screening is important when index patients identified The measurement of Lp(a) is a complex issue Lp(a) levels can be used to guide lipid lowering therapy and ASCVD risk reduction paradigms Investigational agents in development lower Lp(a) and may offer additonal options for treating patients. 16


17 Additional Information / Resources The Lipoprotein (a) Foundation 17
Lipid Metabolism in Familial Hypercholesterolemia
 Lipid Metabolism in Familial Hypercholesterolemia Khalid Al-Rasadi, BSc, MD, FRCPC Head of Biochemistry Department, SQU Head of Lipid and LDL-Apheresis Unit, SQUH President of Oman society of Lipid & Atherosclerosis
Lipid Metabolism in Familial Hypercholesterolemia Khalid Al-Rasadi, BSc, MD, FRCPC Head of Biochemistry Department, SQU Head of Lipid and LDL-Apheresis Unit, SQUH President of Oman society of Lipid & Atherosclerosis
Lipid metabolism in familial hypercholesterolemia
 Lipid metabolism in familial hypercholesterolemia Khalid Al-Rasadi, BSc, MD, FRCPC Head of Biochemistry Department, SQU Head of Lipid and LDL-Apheresis Unit, SQUH President of Oman society of Lipid & Atherosclerosis
Lipid metabolism in familial hypercholesterolemia Khalid Al-Rasadi, BSc, MD, FRCPC Head of Biochemistry Department, SQU Head of Lipid and LDL-Apheresis Unit, SQUH President of Oman society of Lipid & Atherosclerosis
Cholesterol; what are the future lipid targets?
 Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Lipoprotein (a) Disclosures 2/20/2013. Lipoprotein (a): Should We Measure? Should We Treat? Health Diagnostic Laboratory, Inc. No other disclosures
 Disclosures 2/20/2013. Lipoprotein (a): Should We Measure? Should We Treat? Health Diagnostic Laboratory, Inc. No other disclosures") Lipoprotein (a): Should We Measure? Should We Treat? Joseph P. McConnell, Ph.D. DABCC Health Diagnostic Laboratory Inc. Baptist Health South Florida Eleventh Annual Cardiovascular Disease Prevention International
Lipoprotein (a): Should We Measure? Should We Treat? Joseph P. McConnell, Ph.D. DABCC Health Diagnostic Laboratory Inc. Baptist Health South Florida Eleventh Annual Cardiovascular Disease Prevention International
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Metabolism and Atherogenic Properties of LDL
 Metabolism and Atherogenic Properties of LDL Manfredi Rizzo, MD, PhD Associate Professor of Internal Medicine Faculty of Medicine, University of Palermo, Italy & Affiliate Associate Professor of Internal
Metabolism and Atherogenic Properties of LDL Manfredi Rizzo, MD, PhD Associate Professor of Internal Medicine Faculty of Medicine, University of Palermo, Italy & Affiliate Associate Professor of Internal
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Pathophysiology of Lipid Disorders
 Pathophysiology of Lipid Disorders Henry Ginsberg, M.D. Division of Preventive Medicine and Nutrition CHD in the United States CHD is the single largest killer of men and women 12 million have history
Pathophysiology of Lipid Disorders Henry Ginsberg, M.D. Division of Preventive Medicine and Nutrition CHD in the United States CHD is the single largest killer of men and women 12 million have history
Behind LDL: The Metabolism of ApoB, the Essential Apolipoprotein in LDL and VLDL
 Behind LDL: The Metabolism of ApoB, the Essential Apolipoprotein in LDL and VLDL Sung-Joon Lee, PhD Division of Food Science Institute of Biomedical Science and Safety Korea University Composition of Lipoproteins:
Behind LDL: The Metabolism of ApoB, the Essential Apolipoprotein in LDL and VLDL Sung-Joon Lee, PhD Division of Food Science Institute of Biomedical Science and Safety Korea University Composition of Lipoproteins:
Disclosures. Background 1 What is Known MENOPAUSE, ESTROGENS, AND LIPOPROTEIN PARTICLES. Background 2 What is Not Known 10/2/2017
 Disclosures MENOPAUSE, ESTROGENS, AND LIPOPROTEIN PARTICLES Grants: NIH, Quest Diagnostics Consultant: Quest Diagnostics Merck Global Atherosclerosis Advisory Board Ronald M. Krauss, Children s Hospital
Disclosures MENOPAUSE, ESTROGENS, AND LIPOPROTEIN PARTICLES Grants: NIH, Quest Diagnostics Consultant: Quest Diagnostics Merck Global Atherosclerosis Advisory Board Ronald M. Krauss, Children s Hospital
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Chapter VIII: Dr. Sameh Sarray Hlaoui
 Chapter VIII: Dr. Sameh Sarray Hlaoui Lipoproteins a Lipids are insoluble in plasma. In order to be transported they are combined with specific proteins to form lipoproteins: Clusters of proteins and lipids.
Chapter VIII: Dr. Sameh Sarray Hlaoui Lipoproteins a Lipids are insoluble in plasma. In order to be transported they are combined with specific proteins to form lipoproteins: Clusters of proteins and lipids.
Tina-quant Lipoprotein (a) Gen. 2 For accurate and reliable assessment of cardiovascular risk
 Gen. 2 For accurate and reliable assessment of cardiovascular risk") Tina-quant Lipoprotein (a) Gen. 2 For accurate and reliable assessment of cardiovascular risk cobas modular platform Flexible configurations for tailormade solutions With the cobas modular platform (cobas
Tina-quant Lipoprotein (a) Gen. 2 For accurate and reliable assessment of cardiovascular risk cobas modular platform Flexible configurations for tailormade solutions With the cobas modular platform (cobas
Management of LDL as a Risk Factor. Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil
 Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
PCSK9 Inhibition: From Genetics to Patients
 PCSK9 Inhibition: From Genetics to Patients John Chapman BSc, Ph.D., D.Sc., FESC Research Professor, University of Pierre and Marie Curie Director Emeritus, INSERM Dyslipidemia and Atherosclerosis Research
PCSK9 Inhibition: From Genetics to Patients John Chapman BSc, Ph.D., D.Sc., FESC Research Professor, University of Pierre and Marie Curie Director Emeritus, INSERM Dyslipidemia and Atherosclerosis Research
Regence. Medical Policy Manual. Date of Origin: May Topic: Genetic Testing for Lipoprotein(a) Variant(s) as a Decision Aid for Aspirin Treatment
 Variant(s) as a Decision Aid for Aspirin Treatment") Regence Medical Policy Manual Topic: Genetic Testing for Lipoprotein(a) Variant(s) as a Decision Aid for Aspirin Treatment Date of Origin: May 2013 Section: Genetic Testing Last Reviewed Date: June 2013
Regence Medical Policy Manual Topic: Genetic Testing for Lipoprotein(a) Variant(s) as a Decision Aid for Aspirin Treatment Date of Origin: May 2013 Section: Genetic Testing Last Reviewed Date: June 2013
CETP inhibition: pros and cons. Philip Barter The Heart Research Institute Sydney, Australia
 CETP inhibition: pros and cons Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies or membership of advisory boards from:
CETP inhibition: pros and cons Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies or membership of advisory boards from:
The New Gold Standard for Lipoprotein Analysis. Advanced Testing for Cardiovascular Risk
 The New Gold Standard for Lipoprotein Analysis Advanced Testing for Cardiovascular Risk Evolution of Lipoprotein Testing The Lipid Panel Total Cholesterol = VLDL + LDL + HDL Evolution of Lipoprotein Testing
The New Gold Standard for Lipoprotein Analysis Advanced Testing for Cardiovascular Risk Evolution of Lipoprotein Testing The Lipid Panel Total Cholesterol = VLDL + LDL + HDL Evolution of Lipoprotein Testing
Lipid/Lipoprotein Structure and Metabolism (Overview)
") Lipid/Lipoprotein Structure and Metabolism (Overview) Philip Barter President, International Atherosclerosis Society Centre for Vascular Research University of New South Wales Sydney, Australia Disclosures
Lipid/Lipoprotein Structure and Metabolism (Overview) Philip Barter President, International Atherosclerosis Society Centre for Vascular Research University of New South Wales Sydney, Australia Disclosures
Inhibition of PCSK9: The Birth of a New Therapy
 Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Lp(a) Ready for prime time? E Stroes AMC
 Ready for prime time? E Stroes AMC") Lp(a) Ready for prime time? E Stroes AMC Case Male, 45 years old Hypertension: DM: Smoking: Dyslipidemia: Fam history: brother MI (55yr) Lipoprotein(a): 1240 mg/l!!! Lipoprotein(a) = LDL + apo(a) tail
Lp(a) Ready for prime time? E Stroes AMC Case Male, 45 years old Hypertension: DM: Smoking: Dyslipidemia: Fam history: brother MI (55yr) Lipoprotein(a): 1240 mg/l!!! Lipoprotein(a) = LDL + apo(a) tail
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Northwest Lipid Metabolism and Diabetes Research Laboratories, Division of Metabolism,
 Lp(a) Measurements for Clinical Application Santica M Marcovina and John J Albers Northwest Lipid Metabolism and Diabetes Research Laboratories, Division of Metabolism, Endocrinology, and Nutrition, Department
Lp(a) Measurements for Clinical Application Santica M Marcovina and John J Albers Northwest Lipid Metabolism and Diabetes Research Laboratories, Division of Metabolism, Endocrinology, and Nutrition, Department
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
*Carbohydrate & Lipid Metabolism Research Unit, Faculty of Health Sciences, University of Witwatersrand, Johannesburg, South Africa
 Tuesday, May 26, 2015 Clinical Breakthroughs: Modifying LDL Cholesterol to Prevent CV Events International Society of Atherosclerosis, Amsterdam, Netherlands Long-term Treatment With Evolocumab in Patients
Tuesday, May 26, 2015 Clinical Breakthroughs: Modifying LDL Cholesterol to Prevent CV Events International Society of Atherosclerosis, Amsterdam, Netherlands Long-term Treatment With Evolocumab in Patients
High density lipoprotein metabolism
 High density lipoprotein metabolism Lipoprotein classes and atherosclerosis Chylomicrons, VLDL, and their catabolic remnants Pro-atherogenic LDL HDL Anti-atherogenic Plasma lipid transport Liver VLDL FC
High density lipoprotein metabolism Lipoprotein classes and atherosclerosis Chylomicrons, VLDL, and their catabolic remnants Pro-atherogenic LDL HDL Anti-atherogenic Plasma lipid transport Liver VLDL FC
PCSK9 and its Role in LDL Receptor Regulation Muscat, Oman - 9 February 2019
 PCSK9 and its Role in LDL Receptor Regulation Muscat, Oman - 9 February 2019 Professor Gilles Lambert, PhD LaboratoireInserm U1188 Universitéde la Réunion Faculté de Médecine Saint Denis de la Réunion,
PCSK9 and its Role in LDL Receptor Regulation Muscat, Oman - 9 February 2019 Professor Gilles Lambert, PhD LaboratoireInserm U1188 Universitéde la Réunion Faculté de Médecine Saint Denis de la Réunion,
LP(A) AND TRIGLYCERIDE RICH LIPOPROTEINS
 AND TRIGLYCERIDE RICH LIPOPROTEINS") LP(A) AND TRIGLYCERIDE RICH LIPOPROTEINS Alan S Brown, MD FACC FNLA President, National Lipid Association Director, Division of Cardiology Advocate Lutheran General Hospital Park Ridge, Illinois Clinical
LP(A) AND TRIGLYCERIDE RICH LIPOPROTEINS Alan S Brown, MD FACC FNLA President, National Lipid Association Director, Division of Cardiology Advocate Lutheran General Hospital Park Ridge, Illinois Clinical
PCSK9 inhibition in homozygous familial hypercholesterolaemia
 PCSK9 inhibition in homozygous familial hypercholesterolaemia Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis Research Center
PCSK9 inhibition in homozygous familial hypercholesterolaemia Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis Research Center
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies
 Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS
 THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
From Biology to Therapy The biology of PCSK9 in humans Just LDL-cholesterol or more? May 24th. Dr. Gilles Lambert
 Dr. Gilles Lambert Associate Professor in Cell Biology University of Nantes Medical School Group Leader, Laboratory of Nutrition and Metabolism, University Hospital of Nantes From Biology to Therapy The
Dr. Gilles Lambert Associate Professor in Cell Biology University of Nantes Medical School Group Leader, Laboratory of Nutrition and Metabolism, University Hospital of Nantes From Biology to Therapy The
Central role of apociii
 University of Copenhagen & Copenhagen University Hospital Central role of apociii Anne Tybjærg-Hansen MD DMSc Copenhagen University Hospital and Faculty of Health and Medical Sciences, University of Copenhagen,
University of Copenhagen & Copenhagen University Hospital Central role of apociii Anne Tybjærg-Hansen MD DMSc Copenhagen University Hospital and Faculty of Health and Medical Sciences, University of Copenhagen,
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
The Addition of Ezetimibe to Statin therapy in. Patients with Homozygous Familial. Hypercholesterolaemia
 The Addition of Ezetimibe to Statin therapy in Patients with Homozygous Familial Hypercholesterolaemia Submitted in fulfilment with the requirements for the degree Master in Medicine (MMed) Dr Adriano
The Addition of Ezetimibe to Statin therapy in Patients with Homozygous Familial Hypercholesterolaemia Submitted in fulfilment with the requirements for the degree Master in Medicine (MMed) Dr Adriano
Lipids, Lipoproteins and Cardiovascular Risk: Getting the Most out of New and Old Biomarkers. New and Old Biomarkers. Disclosures
 Lipids, Lipoproteins and Cardiovascular Risk: Getting the Most out of New and Old Biomarkers William Cromwell, MD, FAHA, FNLA Diplomate, American Board of Clinical Lipidology Chief Lipoprotein and Metabolic
Lipids, Lipoproteins and Cardiovascular Risk: Getting the Most out of New and Old Biomarkers William Cromwell, MD, FAHA, FNLA Diplomate, American Board of Clinical Lipidology Chief Lipoprotein and Metabolic
Lipoproteins Metabolism
 Lipoproteins Metabolism LEARNING OBJECTIVES By the end of this Lecture, the student should be able to describe: What are Lipoproteins? Describe Lipoprotein Particles. Composition of Lipoproteins. The chemical
Lipoproteins Metabolism LEARNING OBJECTIVES By the end of this Lecture, the student should be able to describe: What are Lipoproteins? Describe Lipoprotein Particles. Composition of Lipoproteins. The chemical
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials?
 PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
Robert A. Vogel, MD Clinical Professor of Medicine University of Colorado Denver
 Robert A. Vogel, MD Clinical Professor of Medicine University of Colorado Denver Disclosures: National Coordinator: ODYSSEY Outcomes Study (Phase III Sanofi) Speakers Bureau: Sanofi, Regeneron Case Report
Robert A. Vogel, MD Clinical Professor of Medicine University of Colorado Denver Disclosures: National Coordinator: ODYSSEY Outcomes Study (Phase III Sanofi) Speakers Bureau: Sanofi, Regeneron Case Report
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Unit IV Problem 3 Biochemistry: Cholesterol Metabolism and Lipoproteins
 Unit IV Problem 3 Biochemistry: Cholesterol Metabolism and Lipoproteins - Cholesterol: It is a sterol which is found in all eukaryotic cells and contains an oxygen (as a hydroxyl group OH) on Carbon number
Unit IV Problem 3 Biochemistry: Cholesterol Metabolism and Lipoproteins - Cholesterol: It is a sterol which is found in all eukaryotic cells and contains an oxygen (as a hydroxyl group OH) on Carbon number
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
thematic review series
 thematic review series Thematic Review Series: Lipoprotein (a): Coming of Age at Last Lipoprotein (a) as a cause of cardiovascular disease: insights from epidemiology, genetics, and biology Børge G. Nordestgaard
thematic review series Thematic Review Series: Lipoprotein (a): Coming of Age at Last Lipoprotein (a) as a cause of cardiovascular disease: insights from epidemiology, genetics, and biology Børge G. Nordestgaard
Familial Hypercholesterolemia New treatments
 Familial Hypercholesterolemia New treatments Prof. Shlomo Keidar Head Internal Medicine A Rambam Health Care Campus IAS, Haifa May 2013 Effect of treatment on CV survival in Familial Hypercholesterolemia
Familial Hypercholesterolemia New treatments Prof. Shlomo Keidar Head Internal Medicine A Rambam Health Care Campus IAS, Haifa May 2013 Effect of treatment on CV survival in Familial Hypercholesterolemia
Plasma lipoproteins & atherosclerosis by. Prof.Dr. Maha M. Sallam
 Biochemistry Department Plasma lipoproteins & atherosclerosis by Prof.Dr. Maha M. Sallam 1 1. Recognize structures,types and role of lipoproteins in blood (Chylomicrons, VLDL, LDL and HDL). 2. Explain
Biochemistry Department Plasma lipoproteins & atherosclerosis by Prof.Dr. Maha M. Sallam 1 1. Recognize structures,types and role of lipoproteins in blood (Chylomicrons, VLDL, LDL and HDL). 2. Explain
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Contributions in Medicine: Will CETP Inhibition Contribute Toward Reduction of Cardiovascular Risk?
 Contributions in Medicine: Will TP Inhibition Contribute Toward Reduction of Cardiovascular Risk? Activity presentations are considered intellectual property. These slides may not be published or posted
Contributions in Medicine: Will TP Inhibition Contribute Toward Reduction of Cardiovascular Risk? Activity presentations are considered intellectual property. These slides may not be published or posted
Genetics of Arterial and Venous Thrombosis: Clinical Aspects and a Look to the Future
 Genetics of Arterial and Venous Thrombosis: Clinical Aspects and a Look to the Future Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Genetics of Arterial and Venous Thrombosis: Clinical Aspects and a Look to the Future Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Summary and concluding remarks
 Summary and concluding remarks This thesis is focused on the role and interaction of different cholesterol and phospholipid transporters. Cholesterol homeostasis is accomplished via a tightly regulated
Summary and concluding remarks This thesis is focused on the role and interaction of different cholesterol and phospholipid transporters. Cholesterol homeostasis is accomplished via a tightly regulated
Cholesteryl ester transfer protein inhibitors - what have we learnt? Philip Barter The Heart Research Institute Sydney, Australia
 Cholesteryl ester transfer protein inhibitors - what have we learnt? Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies
Cholesteryl ester transfer protein inhibitors - what have we learnt? Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
The inhibition of CETP: From simply raising HDL-c to promoting cholesterol efflux and lowering of atherogenic lipoproteins Prof Dr J Wouter Jukema
 The inhibition of CETP: From simply raising HDL-c to promoting cholesterol efflux and lowering of atherogenic lipoproteins Prof Dr J Wouter Jukema Dept Cardiology, Leiden University Medical Center, Leiden,
The inhibition of CETP: From simply raising HDL-c to promoting cholesterol efflux and lowering of atherogenic lipoproteins Prof Dr J Wouter Jukema Dept Cardiology, Leiden University Medical Center, Leiden,
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Cardiovascular Controversies: Emerging Therapies for Lowering Cardiovascular Risk
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Lipoproteins Metabolism Reference: Campbell Biochemistry and Lippincott s Biochemistry
 Lipoproteins Metabolism Reference: Campbell Biochemistry and Lippincott s Biochemistry Learning Objectives 1. Define lipoproteins and explain the rationale of their formation in blood. 2. List different
Lipoproteins Metabolism Reference: Campbell Biochemistry and Lippincott s Biochemistry Learning Objectives 1. Define lipoproteins and explain the rationale of their formation in blood. 2. List different
DIAGNOSIS AND TREATMENT OF FH CHILDREN. O. GUARDAMAGNA Dipartimento di Scienze della Sanità Pubblica e Pediatriche UNIVERSITA DI TORINO
 DIAGNOSIS AND TREATMENT OF FH CHILDREN O. GUARDAMAGNA Dipartimento di Scienze della Sanità Pubblica e Pediatriche UNIVERSITA DI TORINO DISCLOSURES Kowa MSD Pfizer Astrazeneca Synageva/Alexion OUTLINE Background
DIAGNOSIS AND TREATMENT OF FH CHILDREN O. GUARDAMAGNA Dipartimento di Scienze della Sanità Pubblica e Pediatriche UNIVERSITA DI TORINO DISCLOSURES Kowa MSD Pfizer Astrazeneca Synageva/Alexion OUTLINE Background
Inflammation and and Heart Heart Disease in Women Inflammation and Heart Disease
 Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Impact of a 1- or 2-dose starting regimen of inclisiran, a novel sirna inhibitor to PCSK9 on time averaged LDL-C reductions over 1 year
 ORION-1 Impact of a 1- or 2-dose starting regimen of inclisiran, a novel sirna inhibitor to PCSK9 on time averaged LDL-C reductions over 1 year Kausik K Ray, Ulf Landmesser, Lawrence A Leiter, David Kallend,
ORION-1 Impact of a 1- or 2-dose starting regimen of inclisiran, a novel sirna inhibitor to PCSK9 on time averaged LDL-C reductions over 1 year Kausik K Ray, Ulf Landmesser, Lawrence A Leiter, David Kallend,
Cholesterol Synthesis and Absorption Markers
 The Yin and Yang of New Lipid-modifying Agents Inhibitors Are They on Life Support? PCSK9 Inhibitors Are They Potential Game Changers? Thomas Dayspring, MD, FACP, FNLA Diplomate of the American Board of
The Yin and Yang of New Lipid-modifying Agents Inhibitors Are They on Life Support? PCSK9 Inhibitors Are They Potential Game Changers? Thomas Dayspring, MD, FACP, FNLA Diplomate of the American Board of
Defining and Controlling Severe Familial Hypercholesterolemia
 Defining and Controlling Severe Familial Hypercholesterolemia Raul D. Santos MD, PhD InCor-University of Sao Paulo Hospital Israelita Albert Einstein Brazil 1 Disclosure Honoraria received for consulting,
Defining and Controlling Severe Familial Hypercholesterolemia Raul D. Santos MD, PhD InCor-University of Sao Paulo Hospital Israelita Albert Einstein Brazil 1 Disclosure Honoraria received for consulting,
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Comprehensive Treatment for Dyslipidemias. Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium
 Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Cholesterol, guidelines, targets and new medications
 Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Hypertriglyceridemia. Ara Metjian, M.D. Resident s Report 20 December 2002
 Hypertriglyceridemia Ara Metjian, M.D. Resident s Report 20 December 2002 Review of Lipids Chylomicrons (CM): Dietary lipids absorbed through the GI tract are assembled intracellularly into CM. Very Low
Hypertriglyceridemia Ara Metjian, M.D. Resident s Report 20 December 2002 Review of Lipids Chylomicrons (CM): Dietary lipids absorbed through the GI tract are assembled intracellularly into CM. Very Low
Problem patients in primary care Patient 4: Peripheral artery disease
 Problem patients in primary care Patient 4: Peripheral artery disease Dr Terry McCormack Hambleton Richmond Whitby Clinical Commissioning Group Research Lead 01/05/2014 Delivering clinical research to
Problem patients in primary care Patient 4: Peripheral artery disease Dr Terry McCormack Hambleton Richmond Whitby Clinical Commissioning Group Research Lead 01/05/2014 Delivering clinical research to
Familial hypercholesterolaemia in children and adolescents
 Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
 Glossary For TheFatNurse s For All Ages Series Adipocytes, also known as lipocytes and fat cells, are the cells that primarily compose adipose tissue, specialized in storing energy as fat. Apolipoprotein
Glossary For TheFatNurse s For All Ages Series Adipocytes, also known as lipocytes and fat cells, are the cells that primarily compose adipose tissue, specialized in storing energy as fat. Apolipoprotein
March 30, 2014, Joint ACC/JAMA Late-breaking Clinical Trials Session 402 American College of Cardiology, Washington DC
 A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
What Else Do You Need to Know? Presenter Disclosure Information. Case 1: Cardiovascular Risk Assessment in a 53-Year-Old Man. Learning Objectives
 9: 1:am Understanding Dyslipidemia Testing and Screening: Importance of Lipoprotein Particle Analysis SPEAKER Matthew Sorrentino, MD, FACC Presenter Disclosure Information The following relationships exist
9: 1:am Understanding Dyslipidemia Testing and Screening: Importance of Lipoprotein Particle Analysis SPEAKER Matthew Sorrentino, MD, FACC Presenter Disclosure Information The following relationships exist
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both
 Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
10/15/2012. Lessons Learned from Tim Russert: Investigating Residual Risk. Tim Russert: Residual CV Risk?
 Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Small Apolipoprotein(a) Size Predicts Mortality in End-Stage Renal Disease. The CHOICE Study
 Size Predicts Mortality in End-Stage Renal Disease. The CHOICE Study") Small Apolipoprotein(a) Size Predicts Mortality in End-Stage Renal Disease The CHOICE Study J. Craig Longenecker, MD, PhD; Michael J. Klag, MD, MPH; Santica M. Marcovina, PhD, DSc; Neil R. Powe, MD, MPH;
Small Apolipoprotein(a) Size Predicts Mortality in End-Stage Renal Disease The CHOICE Study J. Craig Longenecker, MD, PhD; Michael J. Klag, MD, MPH; Santica M. Marcovina, PhD, DSc; Neil R. Powe, MD, MPH;
Lipid Risk Factors (Novel) in Risk Assessment and Management of Cardiovascular Disease
 in Risk Assessment and Management of Cardiovascular Disease") Lipid Risk Factors (Novel) in Risk Assessment and Management of Cardiovascular Disease Policy Number: Original Effective Date: MM.02.013 02/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;
Lipid Risk Factors (Novel) in Risk Assessment and Management of Cardiovascular Disease Policy Number: Original Effective Date: MM.02.013 02/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;
Biomarkers (Novel) in Risk Assessment and Management of Cardiovascular Disease
 in Risk Assessment and Management of Cardiovascular Disease") Biomarkers (Novel) in Risk Assessment and Management of Cardiovascular Disease Policy Number: Original Effective Date: MM.02.013 02/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST
Biomarkers (Novel) in Risk Assessment and Management of Cardiovascular Disease Policy Number: Original Effective Date: MM.02.013 02/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST
The Target is LDL, HDL not so much
 The Target is LDL, HDL not so much HDL: A riddle wrapped in a mystery inside an enigma Jacques Genest MD Cardiovascular Research Laboratories McGill University Health Center Disclosure J. Genest MD 2013
The Target is LDL, HDL not so much HDL: A riddle wrapped in a mystery inside an enigma Jacques Genest MD Cardiovascular Research Laboratories McGill University Health Center Disclosure J. Genest MD 2013
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Lipoprotein Particle Profile
 Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
行政院國家科學委員會補助專題研究計畫成果報告
 NSC892314B002270 898 1 907 31 9010 23 1 Molecular Study of Type III Hyperlipoproteinemia in Taiwan β β ε E Abstract β Type III hyperlipoproteinemia (type III HLP; familial dysbetalipoproteinemia ) is a
NSC892314B002270 898 1 907 31 9010 23 1 Molecular Study of Type III Hyperlipoproteinemia in Taiwan β β ε E Abstract β Type III hyperlipoproteinemia (type III HLP; familial dysbetalipoproteinemia ) is a
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
USING NON -TRADITIONAL RISK MARKERS IN ASSESSING CV RISK
 USING NON -TRADITIONAL RISK MARKERS IN ASSESSING CV RISK JAMES M FALKO MD PROFESSOR OF MEDICINE UNIVERSITY OF COLORADO Adapted from: Rader D. N Engl J Med. 2000 hs-crp (mg/l) 6 5 4 3 2 1 *p
USING NON -TRADITIONAL RISK MARKERS IN ASSESSING CV RISK JAMES M FALKO MD PROFESSOR OF MEDICINE UNIVERSITY OF COLORADO Adapted from: Rader D. N Engl J Med. 2000 hs-crp (mg/l) 6 5 4 3 2 1 *p
Inclisiran lowers LDL-C and PCSK9 irrespective of diabetes status without worsening glycemia
 ORION-1 Trial Inclisiran lowers LDL-C and PCSK9 irrespective of diabetes status without worsening glycemia Lawrence A Leiter, MD, FRCPC, FACP, FACE, FAHA St Michael s Hospital, Toronto 1 Presented on behalf
ORION-1 Trial Inclisiran lowers LDL-C and PCSK9 irrespective of diabetes status without worsening glycemia Lawrence A Leiter, MD, FRCPC, FACP, FACE, FAHA St Michael s Hospital, Toronto 1 Presented on behalf
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Beyond HDL: new therapeutic targets
 Rome Cardiology Forum 2014 An ESC Update Programme in Cardiology Rome, 29-31 2014 Beyond HDL: new therapeutic targets Marcello Arca, MD Dipartimento di Medicina Interna e Specialità Mediche UOS Centro
Rome Cardiology Forum 2014 An ESC Update Programme in Cardiology Rome, 29-31 2014 Beyond HDL: new therapeutic targets Marcello Arca, MD Dipartimento di Medicina Interna e Specialità Mediche UOS Centro
Anne Carol Goldberg, MD, FACP, FAHA, FNLA Washington University, St. Louis, MO USA
 Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
Pitavastatin 4 mg vs. Pravastatin 40 mg in HIV Dyslipidemia: Post- Hoc Analysis of the INTREPID Trial Based on the Independent CHD Risk Factor for Age
 Pitavastatin 4 mg vs. Pravastatin 40 mg in HIV Dyslipidemia: Post- Hoc Analysis of the INTREPID Trial Based on the Independent CHD Risk Factor for Age Craig A. Sponseller, Masaya Tanahashi, Hideki Suganami,
Pitavastatin 4 mg vs. Pravastatin 40 mg in HIV Dyslipidemia: Post- Hoc Analysis of the INTREPID Trial Based on the Independent CHD Risk Factor for Age Craig A. Sponseller, Masaya Tanahashi, Hideki Suganami,
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a
: Results from a") Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
Defining Severe Familial Hypercholesterolemia. Raul D. Santos MD, PhD Brazil
 Defining Severe Familial Hypercholesterolemia Raul D. Santos MD, PhD Brazil 1 Disclosure Honoraria received for consulting, speaker and or researcher activities : Astra Zeneca, Akcea, Amgen, Biolab, Esperion,
Defining Severe Familial Hypercholesterolemia Raul D. Santos MD, PhD Brazil 1 Disclosure Honoraria received for consulting, speaker and or researcher activities : Astra Zeneca, Akcea, Amgen, Biolab, Esperion,