The Best Lipid Fraction for the Prediction of the Population at Risk of Atherothrombotic Disease. William E. Feeman, Jr., M.D.
|
|
|
- Eileen Page
- 6 years ago
- Views:
Transcription
1 The Best Lipid Fraction for the Prediction of the Population at Risk of Atherothrombotic Disease William E. Feeman, Jr., M.D. 640 South Wintergarden Road Bowling Green, Ohio Phone Fax BGS No conflict of Interest No publication elsewhere No financial contracts No sources of support No Disclosures Word Count: 2525
2 Introduction Dyslipidemia is an important cause of atherothrombotic disease (ATD, or atherosclerotic disease with emphasis on the thrombosis that so often precipitates the acute clinical event, such as acute myocardial infarction, acute cerebral infarction, abdominal aortic aneurysm, etc.) (1-6) Four lipid fractions are widely available for screening: total serum cholesterol (CT), low-density lipoprotein (LDL) cholesterol, a ratio between CT and high-density lipoprotein (HDL) cholesterol (hereafter termed the Framingham Fraction, or FF), and a ratio between LDL-cholesterol and HDL-cholesterol. A newer lipid ratio between LDL-cholesterol and HDL-cholesterol, specifically the cholesterol retention fraction (CRF, or [LDL-HDL]/LDL) has been advocated (7). The CRF has been shown to be of value in predicting the population at risk of ATD (7) and in guiding therapy to maximally stabilize/regress coronary plaque angiographically (8). The purpose of this article is to compare the ability of these five lipid fractors to predict the population at risk of ATD.
3 Materials and Methods The author began his practice of family medicine in Bowling Green, the county seat of Wood County, in northwest Ohio on 4 Nov Details of the author s practice here been published elsewhere. (7, 9-10) Briefly, the author s practice, for purposes of this paper, consists of patients typically seen in family practice: members of both sexes and all age groups, from newborns to people in their tenth decade of life. During the 4 Nov Nov 2003 time frame, 6763 male and 6635 female patients (total 13,398 people) were seen in the author s office and entered into the general population data base of the Bowling Green Study (BGS) of the Primary and Secondary Prevention of Atherothrombotic Disease (ATD). These patients were mainly European-Americans, with Mexican-Americans being the chief minority. Asian-Americans and African- Americans were present only in small numbers. Bowling Green is a small city in the midst of the farmlands of Northwest Ohio. It numbers about 16,000 people, but is also the home of Bowling Green State University, which adds an additional 12,000 individuals to the populace. The University is also the city s chief employer. Multiple small industries are also present, but in the environs of Bowling Green, agriculture is the chief form of employment. Wood County, of which Bowling Green is the county seat, has an overall population of about 110,000 people. Many of these people seek their medical care in Bowling Green. The populations of Bowling Green and Wood County in general do not differ much. All of the author s patients have been entered into an age-sex database. Thus, blood pressures are known for 6579 male and 6620 female patients. Body mass index
4 determinations are known for 6688 male and 6631 female patients. Cigarette smoking status was not routinely until 1984; hence this data is known only for 4136 male and 3884 female patients. Total serum cholesterol (CT) is known for 2039 male and 2202 female patients and triglycerides (TG) are known for 1881 male and 2056 female patients. Since LDL- and HDL-cholesterol data were not available in Bowling Green until 1978, complete lipid profiles are available for only 1340 male and 1482 female patients. Twohour postprandial blood glucose levels are known for 1506 male and 1646 female patients. Initially, the author s practice was incorporated into a general population database, as described above. Over time, however, a number of the author s patients (1009 patients during the 4 November November 2003 timeframe) developed ATD events. These events included all ATD events in all vascular beds, and hence included such events as acute myocardial infarction, acute cerebral infarctions, abdominal aortic aneurysm, etc. All ATD patients were subsequently incorporated into an ATD database. In discussion of this database, it must be noted that the populace of Bowling Green and its environs is a fluid population. Thus complete follow-up of all patients to ascertain ATD status is not possible. However, there is only one hospital in Wood County (Wood County Hospital) and when patients who have left the author s practice enter into the hospital, the author is often able to interview them to ascertain ATD status. Also, the author s patients know of his interest in preventive cardiology, and at times inform him of what has happened to their relatives whom he formerly treated. Finally,
5 during the study timeframe, death certificates were in the public domain and the author was able to view the death certificates of his ex-patients and determine the cause of death. A brief discussion about the Cholesterol Retention Fraction (CRF, or [LDL- HDL]/LDL) is in order. The BGS devised the CRF as a means of estimating the amount of cholesterol accumulating in the artery wall. The CRF takes into account the amount of cholesterol entering the artery wall (LDL), and the amount of cholesterol being removed from the artery wall by reverse cholesterol transport (HDL). This difference was than expressed as a fraction of the cholesterol entering the artery wall. The concept was essentially this: of the cholesterol entering the artery wall, what percentage stays there. Initially, the simple LDL:HDL ratio was used, but was abandoned because the CRF predicts ATD patients better than the LDL:HDL ratio by 5% (Feeman, unpublished data). Incidentally, inspection of the author s database indicates that if LDL levels are excessively high, then even high levels of HDL cannot prevent the accumulation of LDLcholesterol within the artery wall and the consequent onset of clinical ATD events. In the BGS, the LDL level at which HDL s protective powers begin to fail is 170 mg/dl (4.4 moles/l). Even so, the lower the CRF, the later in life is the onset of ATD. The scenario of CRF > 0.70 and/or LDL > 170 mg/dl (4.4 mmoles/l) is termed the Cholesterol Threshold (CThr). For purposes of this analysis, the four lipid predicators have been divided into sextiles. (See Table I) The LDL:HDL ratio is not included in this table because CRF is a better lipid predictor.
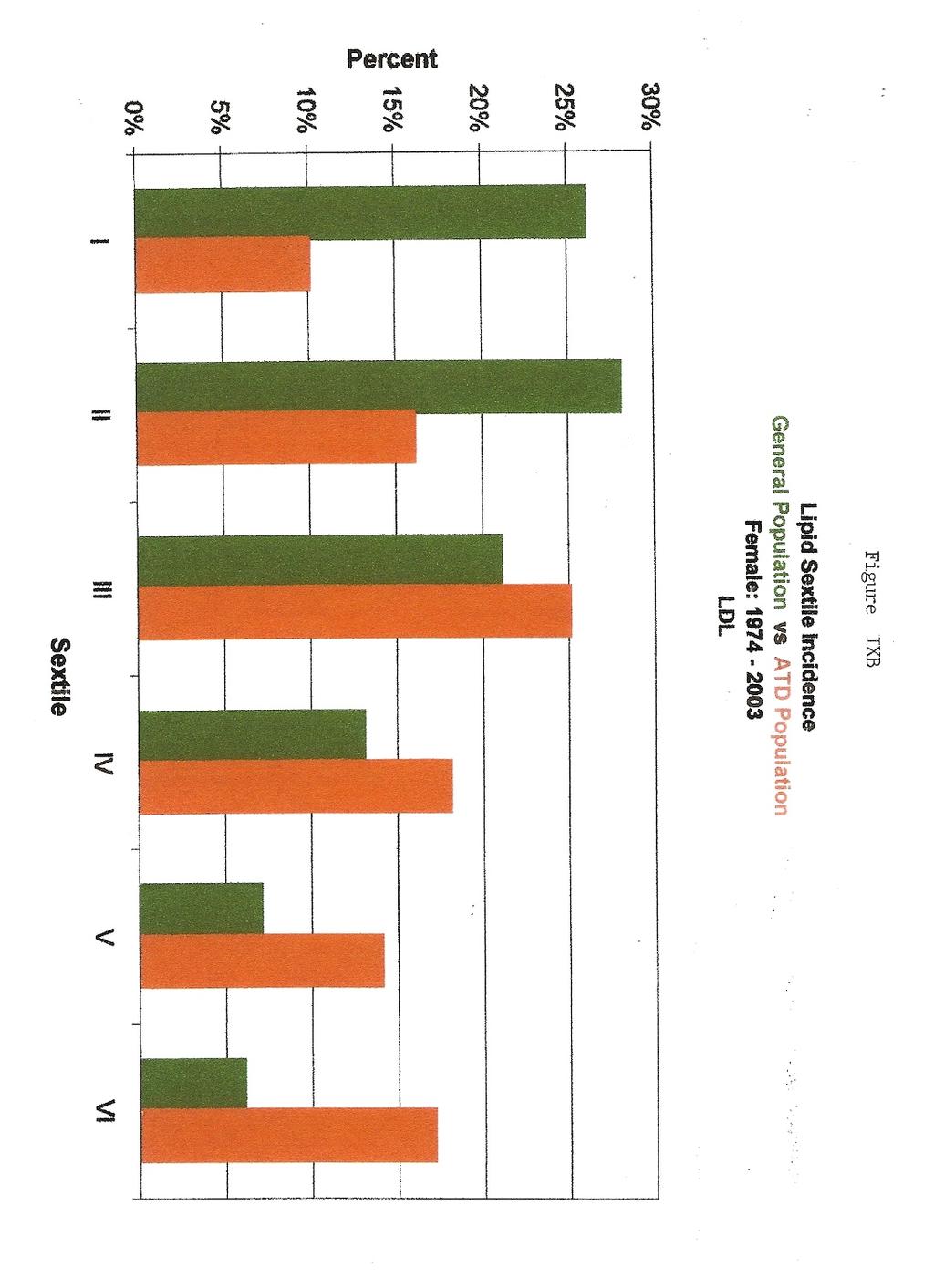
6 Results Table I gives the breakdown of each lipid predictor into sextiles. In the first analysis, the four lipid predictors have been compared with respect to the incidences of each of the sextiles in the general population (of the BGS database) and the portion of ATD patients in each sextile. See tables II-III. It will be noted that for each lipid predictor, the higher the sextile ranking, the greater the proportion of ATD patients in that sextile. (Table II) However, the FF, LDL, and CT lipid predictors have progressively fewer general population patients in the higher sextiles of the predictors. (Table III) In other words, the FF, LDL, and CT lipid predictors predict the population of ATD patients better and better in fewer and fewer patients. Only with the CRF does the number of patients rise as the sextile rank increases, such that the CRF predicts the population of ATD patients better and better in more and more patients. In the second analysis, the four lipid predictors are compared as to the frequency of each sextile in the general population and the frequency of each sextile in the ATD population. (Tables III and IV) For the FF, LDL, and CT lipid predictors, the sextiles in the general population have many more patients in the lower ranking sextiles than in the higher-ranking sextiles, and the same is true in the ATD population. Only with the CRF do numbers of ATD population patients increase as the number of general population patients increase. In the third analysis, which is limited to the ATD population, the sextiles of each lipid predictors (FF, LDL, and CT) are compared with similar sextiles of the CRF. (See Table V for LDL; Tables for FF and CT are not shown but follow the same pattern) It will be noted that, in general, at any level of each of the three lipid predictors (FF, LDL,
7 and CT) the higher the CRF, the younger is the average age of ATD onset and the lower the CRF, the older is the average age of ATD onset. The tables permit the opposite analysis and in general the age of ATD onset is less clearly demonstrated when the CRF is held constant and the values of other lipid predictors are increased or decreased.
8 Discussion Epidemiologically, to be a good lipid predictor, the predictor should do three things very well. First, it should predict the ATD incidence progressively better as its value is progressively higher, but conversely, it should also have a reasonable number of people in its upper ranges. FF, LDL, CT, and CRF all predict a greater incidence of ATD as the upper ranges of each predictor are approached. However, there are progressively fewer patients in the higher sextiles of the FF, LDL, and CT predictors. Only with the CRF do the numbers of people in the higher CRF sextiles not only not drop sharply, but also actually rise. This is clearly important since there are more people who are targets for intervention in the upper CRF sextiles than in the upper FF, LDL, and CT sextiles. This in turn implies that more ATD events can be prevented using the CRF as the prime lipid predictor. Second, the best lipid predictor should have most of its ATD patients at the higher end of its range and only a few at the lower end of its range. This is clearly true for the CRF, but the sextiles in which the most ATD events occur in the other predictors range between Sextiles II and IV. This is important because, ideally, only those people at moderate or high risk of an ATD event should be treated. Such a targeted approach prevents treatment of those not at risk for the lipid portion of the ATD risk profile, and as a result allows limited health care resources to be allocated more prudently. As a result, one would treat CRF Sextiles V and VI. (See below for comment about treatment of Sextile IV in women) and not treat lower sextiles. For LDL, one would have to treat at Sextile III and higher; for CT, one would have to treat at Sextile IV and higher. For FF, it
9 is difficult to make a treatment decision, but perhaps treatment should begin at Sextile II or III and higher. Another way to approach this matter is to advise treatment whenever the lipid predictor incidence in the ATD population exceeds that in the general population. Hence, using the CRF predictor, one would treat at Sextile V and higher in men and Sextile IV in higher in women. Using FF, one would treat at Sextile III and higher and the same is true for LDL. Using CT, one would treat at Sextile IV and higher. Sextile IV in the CRF predictor for women deserves explanation. Most women who develop ATD in this group are elderly hypertensive patients in their eight and ninth decades of life. Moreover if one separates this sextile into halves ( and ), then the risk is higher in the latter cohort than former cohort Since this group of women is at risk mainly latter in life, this author's practice is to treat the associated hypertension first and then treat the lipids if needed. Third, at any level of FF, LDL, and CT, stratification by CRF produces a gradient in ATD risk, as measured by the average age of ATD onset. The ability of the CRF to, in general, stratify ATD risk (as measured by average of ATD onset) at any given level of the other three predictors implies its superiority over the other three predictors. The findings of this study should not come as a surprise to lipidologists. CT is the sum of LDL, HDL, and very-low density lipoprotein cholesterol (VLDL). Hence, CT may be elevated if any of these components are elevated. Elevated LDL clearly constitutes a risk of ATD; however, elevated HDL does not and neither does an isolated VLDL, (11). Unfortunately an elevated CT does not tell the physician which combination of the components are elevated. For example, given a CT of 250 mg/dl (6.48 mmoles/l), is the
10 ATD risk the same if LDL=125mg/dl (3.24 mmoles/l) HDL=100mg/dl (2.59 mmoles/l), and VLDL=25 mg/dl (0.28 mmoles/l) or if LDL=170mg/dl (4.40 mmoles/l), HDL=20mg/dl (0.52 mmoles/l) and VLDL= 60 mg/dl (0.68 mmoles/l)? The former patient is at little risk of ATD, whereas the latter patient is at extremely high risk of ATD- --yet both have the same CT. A similar scenario holds for LDL. The average LDL for an ATD event in a male in the BGS is 145 mg/dl (3.78 moles/l). (Feeman unpublished data) If a lipid profile of a male discloses a LDL level of 145 mg/dl (3.78 mmoles/l), should his physician panic and prescribe a statin immediately? This author believes that a further investigation is necessary first. Suppose that patient has a HDL of 100mg/dl (2.59 mmoles/l) and a VLDL of 25 mg/dl (0.28 mmoles/l), or alternately suppose that the patient has a HDL of 20 mg/dl (0.52 mmoles/l) and a VLDL of 60 mg/dl (0.68 mmoles/l). The former patient is at little risk of an ATD event if he has never smoked cigarettes, is not hypertensive, and is not diabetic. The latter patient is at very high risk, and if he is also a cigarette smoker who is also a diabetic hypertensive, he is at extremely high risk. The former patient might well be followed on diet and exercise, whereas the latter patient requires medication at the onset and both have the same LDL level. As for FF, the ratio may be high if LDL is high, if HDL is low, or if VLDL is high. The average FF for a male with ATD in the BGS is 5.9. (Feeman, unpublished data) If a male patient has HDL=40 mg/dl (1.04 mmoles/l), LDL=60 mg/dl (1.55 mmoles/l), and VLDL=136 mg/dl (1.54 mmoles/l), or if he has HDL=80 mg/dl (2.07 mmoles/l), LDL=380 mg/dl (9.84 mmoles/l), and VLDL=10 mg/dl (0.11 mmoles/l), in either case FF=5.9, but would the treatment scenario be the same? Certainly, the therapeutic
11 regimen would be vastly different in these two men with the same FF (5.9) and certainly the goals of treatment would be different. The former patient would be treated to prevent pancreatitis, the latter to prevent ATD.
12 Conclusion The CRF is a better predictor of the lipid portion of ATD risk because as CRF sextiles increase in rank, the CRF predicts that risk better in more patients, whereas FF, LDL, and CT predict risk better in fewer patients. The CRF is a better lipid predictor, moreover because only the patients in the Sextiles V and VI need treatment, whereas with the other lipid predictors (FF, LDL, and CT) ATD risk is higher in the middle sextiles. Furthermore, CRF is a better lipid predictor because at, in general, any given Sextile of the other lipid predictors (FF, LDL, and CT), ATD risk is stratified (when measured by the average age of ATD onset) by CRF, being younger when CRF is higher, and older when the CRF is lower. Finally, the case scenarios described at the end of Discussion clearly show the ambiguities in treatment of dyslipidemia using FF, LDL, and CT. Since the CRF is purely a disorder of the cholesterol entering the artery wall and the cholesterol being removed from the artery wall, it is not subject to those ambiguities.
13 Table I Lipid Predictor Sextiles Lipid I II III IV V VI Predictor CT < 99 mg/dl mg/dl mg/dl mg/dl mg/dl > 300 mg/dl < 2.56 mmoles/l mmoles/l mmoles/l mmoles/l mmoles/l > 7.77 mmoles/l LDL < 99 mg/dl mg/dl mg/dl mg/dl mg/dl > 200 mg/dl < 2.56 mmoles/l mmoles/l mmoles/l mmoles/l mmoles/l > 5.18 mmoles/l FF < > 8.0 CRF < > 0.80 CT means total cholesterol LDL means low-density-lipoprotein cholesterol HDL means high-density-lipoprotein cholesterol FF means Framingham Fraction, or the ratio of total cholesterol to high-density-lipoprotein cholesterol (CT: HDL) CRF means Cholesterol Retention Fraction, or (LDL-HDL)/LDL
14 Table II ATD Incidence Per Lipid Sextile in General Population Sex Lipid Predictors I II III IV V VI Male No. ATD pts per sextile CRF No. pts. per sextile % 11% 15% 18% 28% 39% No. ATD pts per sextile LDL No. pts. per sextile % 14% 26% 30% 38% 42% No. ATD pts per sextile FF No. pts. per sextile % 21% 22% 34% 28% 46% No. ATD pts per sextile CT No. pts. per sextile % 3% 13% 27% 34% 44% Female No. ATD pts per sextile CRF No. pts. per sextile % 12% 11% 21% 28% 44% No. ATD pts per sextile LDL No. pts. per sextile % 10% 21% 26% 38% 54% No. ATD pts per sextile FF No. pts. per sextile % 18% 29% 34% 44% 45% No. ATD pts per sextile CT No. pts. per sextile % 3% 7% 21% 40% 51% See Table I for sextile parameters and definition of lipid predictors
15 Table III Frequency Distribution of Sextiles per Lipid Predictor in General Population Sex Lipid Predictors I II III IV V VI Male No. pts per sextile CRF Total pts. per sextile % 7% 16% 26% 32% 11% No. pts per sextile FF Total pts. per sextile % 25% 19% 12% 6% 7% No. pts per sextile LDL Total pts. per sextile % 25% 24% 17% 7% 5% No. pts per sextile CT Total pts. per sextile ~0% 11% 43% 32% 11% 3% Female No. pts per sextile CRF Total pts. per sextile % 14% 20% 24% 20% 5% No. pts per sextile FF Total pts. per sextile % 22% 14% 6% 3% 3% No. pts per sextile LDL Total pts. per sextile % 28% 21% 13% 7% 6% No. pts per sextile CT Total pts. per sextile ~0% 11% 43% 32% 11% 4% See Table I for sextile parameters and definition of lipid predictors
16 Table IV Frequency Distribution of Sextiles per Lipid Predictors in Atherothrombotic Disease Population Sex Lipid Predictors I II III IV V VI Male No. pts. per sextile CRF Total patients % 4% 10% 20% 39% 22% No. pts. per sextile FF Total patients % 21% 19% 20% 9% 16% No. pts. per sextile LDL Total patients % 18% 27% 21% 12% 9% No. pts. per sextile CT Total patients % 30% 41% 19% 6% Female No. pts. per sextile CRF Total patients % 8% 12% 30% 30% 13% No. pts. per sextile FF Total patients % 25% 22% 11% 8% 7% No. pts. per sextile LDL Total patients % 18% 25% 18% 14% 15% No. pts. per sextile CT Total patients % 22% 38% 27% 11% See Table I for sextile parameters and definition of lipid predictors
17 Table V CRF vs LDL Sextiles in Atherothrombotic Disease Population LDL Sextiles CRF Sextile 710 patients > < 0.39! > , < ! ,134 11, CRF means Cholesterol Retention Fraction ([LDL-HDL]/LDL) LDL means low density lipoprotein cholesterol
18 Table VI CRF vs FF in Atherothrombotic Disease Population: FF Sextiles CRF Sextiles 710 patients > < 0.39! > , < , ! ,134 11, CRF means Cholesterol Retention Fraction [(LDL-HDL]/LDL) FF means Framingham Fraction (CT/HDL)
19 Table VII CRF Sextiles vs CT Sextiles in Atherothrombotic Disease Population: CT Sextile CRF Sextiles 710 patients > < 0.39! > , , , < ! ,134 11, CRF means Cholesterol Retention Fraction ([LDL-HDL]/LDL) CT means total cholesterol
20 References: 1. Keys A, Aravanis C, Blackburn H, van Buchen FSP, et al. Probability of Middle- Aged Men Developing Coronary Heart Disease in Five Years. Circulation. 1972;45: Gordon T, Garcia-Palmier, Kagan A, et al. Differences in Coronary Heart Disease in Framingham, Honolulu, and Puerto Rico. J. Chron. Dis. 1974;27: The Expert Panel. Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Arch Intern Med. 1988;148: Greenland P, Knoll MD, Stamler J, et al. Major Risk Factors as Antecedents of Fatal and Nonfatal Coronary Heart Disease Events. JAMA. 2003;290: Khot UN, Khot MB, Bajzer CT, et al. Prevalence of Conventional Risk Factors in Patients with Coronary Heart Disease. JAMA. 2003;290: Nam BH, Kannel WB, D Agostino. Search for an Optimal Atherogenic Lipid Risk Profile: From the Framingham Study. Am J Cardio. 2006;97: Feeman W.E. Jr. Prediction of the Population at Risk of Atherothrombotic Disease. Experimental and Clinical Cardiology. Winter : (4); Feeman W.E. Jr. Prediction of Angiographic Stabilization/Regression of Coronary Atherosclerosis by a Risk Factor Graph. J. Cardio. Risk. 2000; 7:
21 9. Feeman W.E. Jr. The Bowling Green Study of the Primary and Secondary Prevention of Atherosclerosis: Descriptive Analysis, Findings, Applications and Conclusions. Ohio J. Sci. 92 (5): Feeman W.E. Jr. The Bowling Green Study of the Primary and Secondary Prevention of Atherosclerotic Disease: Update Ohio. J. Sci. 94 (4): Feeman W.E. Jr. Proposal for a New Lipid Disorder Classification presented at the 14 th International Symposium on Drugs Affecting Lipid Metabolism. September 2001 New York City, New York.
22 Addendum CRF vs Other Lipid Predictors Total ATD Population Average Age at ATD Onset Sextile Equivalent Line Above Line On Line Below Line FF LDL CT

23

24

25
26
27

28

29

30
31
32
33

34

35

36
37
38
39
40
41
42
43
44
45
46
47
48
49

50
51
52
53
54
55
56
Comparison of the Bowling Green Study Risk Factor Graph and the Framingham Risk Score to Predict the Population at Risk of Atherothrombotic Disease
 Comparison of the Bowling Green Study Risk Factor Graph and the Framingham Risk Score to Predict the Population at Risk of Atherothrombotic Disease Introduction Atherothrombotic Disease (ATD) is the leading
Comparison of the Bowling Green Study Risk Factor Graph and the Framingham Risk Score to Predict the Population at Risk of Atherothrombotic Disease Introduction Atherothrombotic Disease (ATD) is the leading
To the Editor, I was delighted to read the lead article (in the Autumn issue of The Lipid Spin) by Maria Luz Fernandez, PhD, concerning the use of
 by Maria Luz Fernandez, PhD, concerning the use of") To the Editor, I was delighted to read the lead article (in the Autumn issue of The Lipid Spin) by Maria Luz Fernandez, PhD, concerning the use of the LDL: HDL ratio in the prediction of the population
To the Editor, I was delighted to read the lead article (in the Autumn issue of The Lipid Spin) by Maria Luz Fernandez, PhD, concerning the use of the LDL: HDL ratio in the prediction of the population
Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients. Copyright. Not for Sale or Commercial Distribution
 CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Lipoprotein Particle Profile
 Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
HIGH LDL CHOLESTEROL IS NOT AN INDEPENDENT RISK FACTOR FOR HEART ATTACKS AND STROKES
 HIGH LDL CHOLESTEROL IS NOT AN INDEPENDENT RISK FACTOR FOR HEART ATTACKS AND STROKES A study published in the British Medical Journal shows that not only is high LDL cholesterol not a risk factor for all-caused
HIGH LDL CHOLESTEROL IS NOT AN INDEPENDENT RISK FACTOR FOR HEART ATTACKS AND STROKES A study published in the British Medical Journal shows that not only is high LDL cholesterol not a risk factor for all-caused
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
The Metabolic Syndrome Update The Metabolic Syndrome Update. Global Cardiometabolic Risk
 The Metabolic Syndrome Update 2018 Marc Cornier, M.D. Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine
The Metabolic Syndrome Update 2018 Marc Cornier, M.D. Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Statistical Fact Sheet Populations
 Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY
 MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD
 Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD 1 Preclinical? No symptoms No physical findings No diagnostic ECG findings No chest X-ray X findings No diagnostic events 2
Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD 1 Preclinical? No symptoms No physical findings No diagnostic ECG findings No chest X-ray X findings No diagnostic events 2
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
LDL cholesterol (p = 0.40). However, higher levels of HDL cholesterol (> or =1.5 mmol/l [60 mg/dl]) were associated with less progression of CAC
![LDL cholesterol (p = 0.40). However, higher levels of HDL cholesterol (> or =1.5 mmol/l [60 mg/dl]) were associated with less progression of CAC](/thumbs/88/116891773.jpg "LDL cholesterol (p = 0.40). However, higher levels of HDL cholesterol (> or =1.5 mmol/l [60 mg/dl]) were associated with less progression of CAC") Am J Cardiol (2004);94:729-32 Relation of degree of physical activity to coronary artery calcium score in asymptomatic individuals with multiple metabolic risk factors M. Y. Desai, et al. Ciccarone Preventive
Am J Cardiol (2004);94:729-32 Relation of degree of physical activity to coronary artery calcium score in asymptomatic individuals with multiple metabolic risk factors M. Y. Desai, et al. Ciccarone Preventive
Epidemiologic and clinical comparison of renal artery stenosis in black patients and white patients
 ORIGINAL ARTICLES Epidemiologic and clinical comparison of renal artery stenosis in black patients and white patients Andrew C. Novick, MD, Safwat Zald, MD, David Goldfarb, MD, and Ernest E. Hodge, MD,
ORIGINAL ARTICLES Epidemiologic and clinical comparison of renal artery stenosis in black patients and white patients Andrew C. Novick, MD, Safwat Zald, MD, David Goldfarb, MD, and Ernest E. Hodge, MD,
Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution
 and females (n=130). Box plots represent the quartiles distribution") Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution of A: total cholesterol (TC); B: low-density lipoprotein
Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution of A: total cholesterol (TC); B: low-density lipoprotein
Atherosclerotic Disease Risk Score
 Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Caduet) Reference Number: CP.CPA.237 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Caduet) Reference Number: CP.CPA.237 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
2.0 Synopsis. Choline fenofibrate capsules (ABT-335) M Clinical Study Report R&D/06/772. (For National Authority Use Only) Name of Study Drug:
 M Clinical Study Report R&D/06/772. (For National Authority Use Only) Name of Study Drug:") 2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: Choline Fenofibrate (335) Name of Active Ingredient:
2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: Choline Fenofibrate (335) Name of Active Ingredient:
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both
 Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Two articles published in the summer of 2003 (1,2) pointed
 pointed") CLNCAL CARDOLOGY Prediction of the population at risk for atheroth rom boti
CLNCAL CARDOLOGY Prediction of the population at risk for atheroth rom boti
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
A Study to Show Postprandial Hypertriglyceridemia as a Risk Factor for Macrovascular Complications in Type 2 Diabetis Mellitus
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/21 A Study to Show Postprandial Hypertriglyceridemia as a Risk Factor for Macrovascular Complications in Bingi Srinivas
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/21 A Study to Show Postprandial Hypertriglyceridemia as a Risk Factor for Macrovascular Complications in Bingi Srinivas
LIPIDS AND CHOLESTEROL - RISK FACTORS TO A POLICE UNIT FROM BRASOV
 Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 4 (53) No. 2-2011 LIPIDS AND CHOLESTEROL - RISK FACTORS TO A POLICE UNIT FROM BRASOV C. DOBRESCU 1 I. MOLEAVIN 1 Abstract:
Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 4 (53) No. 2-2011 LIPIDS AND CHOLESTEROL - RISK FACTORS TO A POLICE UNIT FROM BRASOV C. DOBRESCU 1 I. MOLEAVIN 1 Abstract:
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS
 GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
Lipoprotein (a) Disclosures 2/20/2013. Lipoprotein (a): Should We Measure? Should We Treat? Health Diagnostic Laboratory, Inc. No other disclosures
 Disclosures 2/20/2013. Lipoprotein (a): Should We Measure? Should We Treat? Health Diagnostic Laboratory, Inc. No other disclosures") Lipoprotein (a): Should We Measure? Should We Treat? Joseph P. McConnell, Ph.D. DABCC Health Diagnostic Laboratory Inc. Baptist Health South Florida Eleventh Annual Cardiovascular Disease Prevention International
Lipoprotein (a): Should We Measure? Should We Treat? Joseph P. McConnell, Ph.D. DABCC Health Diagnostic Laboratory Inc. Baptist Health South Florida Eleventh Annual Cardiovascular Disease Prevention International
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
This one thing can tell your heart s fortune and it s not what your doc has been testing you for!
 This one thing can tell your heart s fortune and it s not what your doc has been testing you for! By now, you are probably aware that there has been a lot of deception and misinformation out there about
This one thing can tell your heart s fortune and it s not what your doc has been testing you for! By now, you are probably aware that there has been a lot of deception and misinformation out there about
ΛΟΙΜΩΞΗ HIV. Ιγνάτιος Οικονομίδης,MD,FESC Β Πανεπιστημιακή Καρδιολογική
 ΛΟΙΜΩΞΗ HIV Ιγνάτιος Οικονομίδης,MD,FESC Β Πανεπιστημιακή Καρδιολογική Κλινική, Νοσοκομείο «Αττικόν» Infection Acute Myocardial Infarction p er 100,000 HIV/AIDS discharg es 800 700 600 500 400 300 200
ΛΟΙΜΩΞΗ HIV Ιγνάτιος Οικονομίδης,MD,FESC Β Πανεπιστημιακή Καρδιολογική Κλινική, Νοσοκομείο «Αττικόν» Infection Acute Myocardial Infarction p er 100,000 HIV/AIDS discharg es 800 700 600 500 400 300 200
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
STATIN UTILIZATION MANAGEMENT CRITERIA
 STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
Diabetes MAYER B. DAVIDSON, MD,* CO-EDITOR-IN-CHIEF; HENRY N. GINSBERG, MD, REVIEWER; TERRENCE F. FAGAN, MANAGING EDITOR; CHING-LING CHEN, PhD, WRITER
 Professional Postgraduate Services Release Date: March 14, 2008 Valid Through: July 14, 2008 Sponsor This educational activity is a component of the National Diabetes Education Initiative (NDEI ), sponsored
Professional Postgraduate Services Release Date: March 14, 2008 Valid Through: July 14, 2008 Sponsor This educational activity is a component of the National Diabetes Education Initiative (NDEI ), sponsored
Calculating Risk for Primary Prevention of Cardiovascular Disease (CVD)
") Calculating Risk for Primary Prevention of Cardiovascular Disease (CVD) 2. Welcome by Stacey Sheridan, MD, MPH Hello. My name is Stacey Sheridan, and I m here as your partner in Heart Health Now. The North
Calculating Risk for Primary Prevention of Cardiovascular Disease (CVD) 2. Welcome by Stacey Sheridan, MD, MPH Hello. My name is Stacey Sheridan, and I m here as your partner in Heart Health Now. The North
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Supplementary Online Content
 Supplementary Online Content Pokharel Y, Tang F, Jones PG, et al. Adoption of the 2013 American College of Cardiology/American Heart Association Cholesterol Management Guideline in cardiology practices
Supplementary Online Content Pokharel Y, Tang F, Jones PG, et al. Adoption of the 2013 American College of Cardiology/American Heart Association Cholesterol Management Guideline in cardiology practices
Non-fasting Lipid Profile Getting to the Heart of the Matter! Medimail Dec 2017
 Non-fasting Lipid Profile Getting to the Heart of the Matter! Medimail Dec 2017 Historical Basis for Fasting Lipids The initial classifications of hyperlipidemia proposed in 1967 were genetic and required
Non-fasting Lipid Profile Getting to the Heart of the Matter! Medimail Dec 2017 Historical Basis for Fasting Lipids The initial classifications of hyperlipidemia proposed in 1967 were genetic and required
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
ORIGINAL INVESTIGATION. Relation of Triglyceride Levels, Fasting and Nonfasting, to Fatal and Nonfatal Coronary Heart Disease
 ORIGINAL INVESTIGATION Relation of Triglyceride Levels, Fasting and Nonfasting, to Fatal and Nonfatal Coronary Heart Disease Lynn E. Eberly, PhD; Jeremiah Stamler, MD; James D. Neaton, PhD; for the Multiple
ORIGINAL INVESTIGATION Relation of Triglyceride Levels, Fasting and Nonfasting, to Fatal and Nonfatal Coronary Heart Disease Lynn E. Eberly, PhD; Jeremiah Stamler, MD; James D. Neaton, PhD; for the Multiple
Joshua Shepherd PA-C, MMS, MT (ASCP)
") Joshua Shepherd PA-C, MMS, MT (ASCP) None What is Cholesterol? Why cholesterol is it important? Review the National Cholesterol Education Programs guidelines (NCEP-ATPIII) Discuss New guidelines from the
Joshua Shepherd PA-C, MMS, MT (ASCP) None What is Cholesterol? Why cholesterol is it important? Review the National Cholesterol Education Programs guidelines (NCEP-ATPIII) Discuss New guidelines from the
Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care
 Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care Purpose Explore the adherence rates to cholesterol treatment targets among patients who seek care
Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care Purpose Explore the adherence rates to cholesterol treatment targets among patients who seek care
Coronary heart disease (CHD) has. Clearfield The National Cholesterol Education Program Adult Treatment Panel III guidelines
 has. Clearfield The National Cholesterol Education Program Adult Treatment Panel III guidelines") the osteopathic physician. The treatment approach involves therapeutic lifestyle changes with diet, exercise, and weight loss. It requires regular, careful monitoring of serum cholesterol levels. The new
the osteopathic physician. The treatment approach involves therapeutic lifestyle changes with diet, exercise, and weight loss. It requires regular, careful monitoring of serum cholesterol levels. The new
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Small dense low-density lipoprotein is a risk for coronary artery disease in an urban Japanese cohort: The Suita study
 Small dense low-density lipoprotein is a risk for coronary artery disease in an urban Japanese cohort: The Suita study Hidenori Arai 1, Yoshihiro Kokubo 2, Makoto Watanabe 2, Tatsuya Sawamura 3, Tomonori
Small dense low-density lipoprotein is a risk for coronary artery disease in an urban Japanese cohort: The Suita study Hidenori Arai 1, Yoshihiro Kokubo 2, Makoto Watanabe 2, Tatsuya Sawamura 3, Tomonori
Intermediate Methods in Epidemiology Exercise No. 4 - Passive smoking and atherosclerosis
 Intermediate Methods in Epidemiology 2008 Exercise No. 4 - Passive smoking and atherosclerosis The purpose of this exercise is to allow students to recapitulate issues discussed throughout the course which
Intermediate Methods in Epidemiology 2008 Exercise No. 4 - Passive smoking and atherosclerosis The purpose of this exercise is to allow students to recapitulate issues discussed throughout the course which
The investigation of serum lipids and prevalence of dyslipidemia in urban adult population of Warangal district, Andhra Pradesh, India
 eissn: 09748369, www.biolmedonline.com The investigation of serum lipids and prevalence of dyslipidemia in urban adult population of Warangal district, Andhra Pradesh, India M Estari, AS Reddy, T Bikshapathi,
eissn: 09748369, www.biolmedonline.com The investigation of serum lipids and prevalence of dyslipidemia in urban adult population of Warangal district, Andhra Pradesh, India M Estari, AS Reddy, T Bikshapathi,
Plasma fibrinogen level, BMI and lipid profile in type 2 diabetes mellitus with hypertension
 World Journal of Pharmaceutical Sciences ISSN (Print): 2321-3310; ISSN (Online): 2321-3086 Published by Atom and Cell Publishers All Rights Reserved Available online at: http://www.wjpsonline.org/ Original
World Journal of Pharmaceutical Sciences ISSN (Print): 2321-3310; ISSN (Online): 2321-3086 Published by Atom and Cell Publishers All Rights Reserved Available online at: http://www.wjpsonline.org/ Original
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Berry JD, Dyer A, Cai X, et al. Lifetime risks of cardiovascular
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Berry JD, Dyer A, Cai X, et al. Lifetime risks of cardiovascular
Nearly 62 million people in the. ... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III
 ... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III Robert L. Talbert, PharmD Abstract Coronary heart disease (CHD) is a common, costly, and undertreated
... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III Robert L. Talbert, PharmD Abstract Coronary heart disease (CHD) is a common, costly, and undertreated
Section Editor Mason W Freeman, MD
 Official reprint from UpToDate www.uptodate.com 2015 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek
Official reprint from UpToDate www.uptodate.com 2015 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek
4/14/2018 DYSLIPIDEMIA CASES. Mary Malloy, MD. I have nothing to disclose
 DYSLIPIDEMIA CASES Mary Malloy, MD I have nothing to disclose 1 Case 1 A 24 year old healthy, slender woman is referred because she has a family history of premature CAD (mother, age 59, had onset of angina
DYSLIPIDEMIA CASES Mary Malloy, MD I have nothing to disclose 1 Case 1 A 24 year old healthy, slender woman is referred because she has a family history of premature CAD (mother, age 59, had onset of angina
1. Most of your blood cholesterol is produced by: a. your kidneys b. your liver c. your pancreas d. food consumption (Your liver)
") I. TEST YOUR KNOWLEDGE OF CHOLESTEROL Choose the correct answer. 1. Most of your blood cholesterol is produced by: a. your kidneys b. your liver c. your pancreas d. food consumption (Your liver) 2. Only
I. TEST YOUR KNOWLEDGE OF CHOLESTEROL Choose the correct answer. 1. Most of your blood cholesterol is produced by: a. your kidneys b. your liver c. your pancreas d. food consumption (Your liver) 2. Only
Total risk management of Cardiovascular diseases Nobuhiro Yamada
 Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Low HDL-levels: leave it or treat it?
 Cardiology Update 2011 Davos, 14 02 2011 Low HDL-levels: leave it or treat it? Experts: J.P. Kastelein, Amsterdam and U. Landmesser, Zurich Cases: C. Besler, Zurich and I. Sudano, Zurich Mr H.B., 1960
Cardiology Update 2011 Davos, 14 02 2011 Low HDL-levels: leave it or treat it? Experts: J.P. Kastelein, Amsterdam and U. Landmesser, Zurich Cases: C. Besler, Zurich and I. Sudano, Zurich Mr H.B., 1960
Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
 ISRN Cardiology, Article ID 825461, 4 pages http://dx.doi.org/10.1155/2014/825461 Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
ISRN Cardiology, Article ID 825461, 4 pages http://dx.doi.org/10.1155/2014/825461 Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
A: Epidemiology update. Evidence that LDL-C and CRP identify different high-risk groups
 A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
The importance of both low-density lipoprotein
 Improving the Prediction of Cardiovascular Risk: Interaction Between LDL and HDL Cholesterol Steven A. Grover, 1,2,3,4 Marc Dorais, 1,3 and Louis Coupal 1,3 Background. The ratio of total cholesterol to
Improving the Prediction of Cardiovascular Risk: Interaction Between LDL and HDL Cholesterol Steven A. Grover, 1,2,3,4 Marc Dorais, 1,3 and Louis Coupal 1,3 Background. The ratio of total cholesterol to
Preventing Myocardial Infarction in the Young Adult in the First Place: How Do the National Cholesterol Education Panel III Guidelines Perform?
 Journal of the American College of Cardiology Vol. 41, No. 9, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Inc. doi:10.1016/s0735-1097(03)00187-6
Journal of the American College of Cardiology Vol. 41, No. 9, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Inc. doi:10.1016/s0735-1097(03)00187-6
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Coverage Guidelines. NMR LipoProfile and NMR LipoProfile -II Tests
 Coverage Guidelines NMR LipoProfile and NMR LipoProfile -II Tests Disclaimer: Please note that Baptist Health Plan updates Coverage Guidelines throughout the year. A printed version may not be most up
Coverage Guidelines NMR LipoProfile and NMR LipoProfile -II Tests Disclaimer: Please note that Baptist Health Plan updates Coverage Guidelines throughout the year. A printed version may not be most up
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
EXECUTIVE SUMMARY OF THE MINOR RESEARCH PROJECT Submitted to UNIVERSITY GRANTS COMMISSION
 1 A STUDY ON THE EFFECT OF DIET & LIFE STYLE ON THE INCIDENCE OF CORONARY ARTERY DISEASE IN MODERATELY DRINKING EX MILITARY MEN IN PATHANAMTHITTA DISTRICT. EXECUTIVE SUMMARY OF THE MINOR RESEARCH PROJECT
1 A STUDY ON THE EFFECT OF DIET & LIFE STYLE ON THE INCIDENCE OF CORONARY ARTERY DISEASE IN MODERATELY DRINKING EX MILITARY MEN IN PATHANAMTHITTA DISTRICT. EXECUTIVE SUMMARY OF THE MINOR RESEARCH PROJECT
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Metabolic Syndrome Update The Metabolic Syndrome: Overview. Global Cardiometabolic Risk
 Metabolic Syndrome Update 21 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes University of Colorado Denver Denver Health Medical Center The Metabolic
Metabolic Syndrome Update 21 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes University of Colorado Denver Denver Health Medical Center The Metabolic
Diabetologia 9 Springer-Verlag 1991
 Diabetologia (1991) 34:590-594 0012186X91001685 Diabetologia 9 Springer-Verlag 1991 Risk factors for macrovascular disease in mellitus: the London follow-up to the WHO Multinational Study of Vascular Disease
Diabetologia (1991) 34:590-594 0012186X91001685 Diabetologia 9 Springer-Verlag 1991 Risk factors for macrovascular disease in mellitus: the London follow-up to the WHO Multinational Study of Vascular Disease
Life Science Journal 2018;15(12)
") Multicenter observational study of risk factors profile in a sample of Egyptian Patients with Acute Coronary Syndrome (part of Egyptian Cardiovascular Risk Factors Project) Prof. Dr. Ahmed Ashraf Reda,
Multicenter observational study of risk factors profile in a sample of Egyptian Patients with Acute Coronary Syndrome (part of Egyptian Cardiovascular Risk Factors Project) Prof. Dr. Ahmed Ashraf Reda,
Clinical Approach to Achieving Treatment Targets: Case Vignette Discussion
 Clinical Approach to Achieving Treatment Targets: Case Vignette Discussion Om P. Ganda, MD; Kirit Tolia, MD, FACE Postcardiac Follow-up in a 66-Year-Old Man Slide 1. Dr. Ganda: Now we will present a case
Clinical Approach to Achieving Treatment Targets: Case Vignette Discussion Om P. Ganda, MD; Kirit Tolia, MD, FACE Postcardiac Follow-up in a 66-Year-Old Man Slide 1. Dr. Ganda: Now we will present a case
Changing lipid-lowering guidelines: whom to treat and how low to go
 European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Guidelines on cardiovascular risk assessment and management
 European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
New Features of the National Cholesterol Education Program Adult Treatment Panel III Lipid-Lowering Guidelines
 Clin. Cardiol. Vol. 26 (Suppl. III), III-19 III-24 (2003) New Features of the National Cholesterol Education Program Adult Treatment Panel III Lipid-Lowering Guidelines H. BRYAN BREWER, JR, M.D. Molecular
Clin. Cardiol. Vol. 26 (Suppl. III), III-19 III-24 (2003) New Features of the National Cholesterol Education Program Adult Treatment Panel III Lipid-Lowering Guidelines H. BRYAN BREWER, JR, M.D. Molecular
LIST OF ABBREVIATIONS
 Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
RECOGNITION OF THE METABOLIC SYNDROME
 THE METABOLIC SYNDROME IN CLINICAL PRACTICE Michael H. Davidson, MD* ABSTRACT Patients with the metabolic syndrome remain at significantly elevated risk of morbidity and mortality associated with coronary
THE METABOLIC SYNDROME IN CLINICAL PRACTICE Michael H. Davidson, MD* ABSTRACT Patients with the metabolic syndrome remain at significantly elevated risk of morbidity and mortality associated with coronary
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
ORIGINAL INVESTIGATION. C-Reactive Protein Concentration and Incident Hypertension in Young Adults
 ORIGINAL INVESTIGATION C-Reactive Protein Concentration and Incident Hypertension in Young Adults The CARDIA Study Susan G. Lakoski, MD, MS; David M. Herrington, MD, MHS; David M. Siscovick, MD, MPH; Stephen
ORIGINAL INVESTIGATION C-Reactive Protein Concentration and Incident Hypertension in Young Adults The CARDIA Study Susan G. Lakoski, MD, MS; David M. Herrington, MD, MHS; David M. Siscovick, MD, MPH; Stephen
Importance of a Patient s Personal Health History on Assessments of Future Risk of Coronary Heart Disease
 Importance of a Patient s Personal Health History on Assessments of Future Risk of Coronary Heart Disease Arch G. Mainous, III, PhD, Charles J. Everett, PhD, Marty S. Player, MD, MS, Dana E. King, MD,
Importance of a Patient s Personal Health History on Assessments of Future Risk of Coronary Heart Disease Arch G. Mainous, III, PhD, Charles J. Everett, PhD, Marty S. Player, MD, MS, Dana E. King, MD,
CARDIOVASCULAR DISEASE RISK FACTOR ESTIMATION IN GUJARATI ASIAN INDIAN POPULATION USING FRAMINGHAM RISK EQUATION
 ORIGINAL ARTICLE CARDIOVASCULAR DISEASE RISK FACTOR ESTIMATION IN GUJARATI ASIAN INDIAN POPULATION USING FRAMINGHAM RISK EQUATION Sibasis Sahoo 1, Komal Shah 2,Anand Shukla 3, Jayesh Prajapati 3, Pratik
ORIGINAL ARTICLE CARDIOVASCULAR DISEASE RISK FACTOR ESTIMATION IN GUJARATI ASIAN INDIAN POPULATION USING FRAMINGHAM RISK EQUATION Sibasis Sahoo 1, Komal Shah 2,Anand Shukla 3, Jayesh Prajapati 3, Pratik
Women and Coronary Artery Disease. Aren t Women Just Like Men?
 Women and Coronary Artery Disease Aren t Women Just Like Men? Anita Wokhlu, MD Assistant Professor of Medicine UF Shands Gainesville, FL Wed Feb 1, 2017 CP1310268-1 Disclosure Of Relationships Anita Wokhlu,
Women and Coronary Artery Disease Aren t Women Just Like Men? Anita Wokhlu, MD Assistant Professor of Medicine UF Shands Gainesville, FL Wed Feb 1, 2017 CP1310268-1 Disclosure Of Relationships Anita Wokhlu,
CARING FOR A LOVED ONE AFTER A HEART ATTACK OR STROKE
 CARING FOR A LOVED ONE AFTER A HEART ATTACK OR STROKE AFTER YOUR LOVED ONE HAS HAD A HEART ATTACK OR STROKE Heart attack and stroke affects the whole family. If your loved one has had a heart attack or
CARING FOR A LOVED ONE AFTER A HEART ATTACK OR STROKE AFTER YOUR LOVED ONE HAS HAD A HEART ATTACK OR STROKE Heart attack and stroke affects the whole family. If your loved one has had a heart attack or
HDL-C. J Jpn Coll Angiol, 2008, 48: NIPPON DATA80, MEGA study, JELIS, dyslipidemia, risk assessment chart
 Online publication March 25, 2009 48 6 2007 2007 HDL-C LDL-C HDL-C J Jpn Coll Angiol, 2008, 48: 463 470 NIPPON DATA80, MEGA study, JELIS, dyslipidemia, risk assessment chart 1987 NIPPON DATA80 Iso 10 MRFIT
Online publication March 25, 2009 48 6 2007 2007 HDL-C LDL-C HDL-C J Jpn Coll Angiol, 2008, 48: 463 470 NIPPON DATA80, MEGA study, JELIS, dyslipidemia, risk assessment chart 1987 NIPPON DATA80 Iso 10 MRFIT
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of