Reducing LDL-C with Non- Statin Therapies
|
|
|
- Lorraine Conley
- 6 years ago
- Views:
Transcription

1 Reducing LDL-C with Non- Statin Therapies Michael Miller, MD, FACC, FAHA, FNLA University of Maryland School of Medicine Baltimore, Maryland
2 Disclosures SPIRE (Pfizer): U.S. National Coordinator REDUCE IT (Amarin): Steering Committee DalGene (Dalcor): U.S. National Coordinator 2

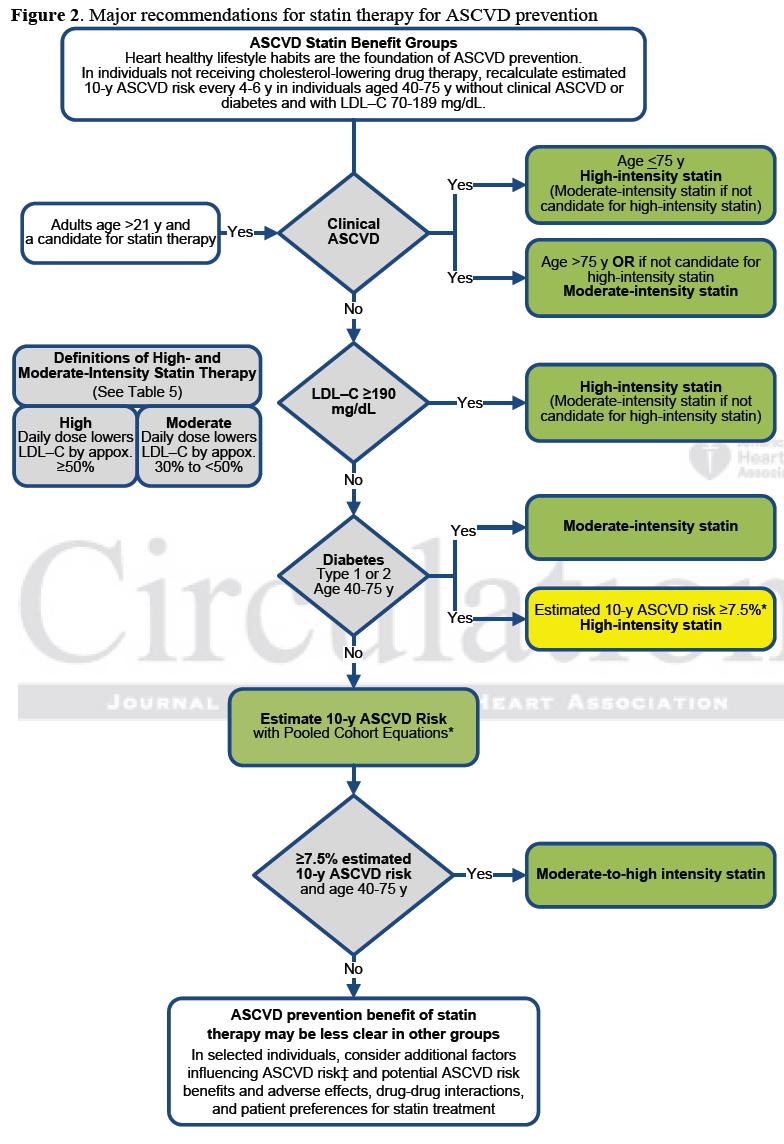
3 Stone NJ et al. Circulation. 2014;129:S1-45.
4 Non-Statin Agents with Efficacy in Reducing LDL-C Levels Drug Class Bile Acid Sequestrants (BAS) Cholesterol absorption inhibitors Fibric acids Examples of Agents Colestipol, Colesevelam, Cholestyramine Ezetimibe Fenofibric Acid* Microsomal Tg transfer protein inh Lomitapide + Nicotinic Acid Niacin* Oligonucleotide inh apo B-100 syn Mipomersen + PCSK9 Inhibitors Alirocumab, Evolocumab *In April 2016, the FDA withdrew approval of fenofibric acid delayed-release capsules and Niacin extended-release tables in combination with statins due to lack of evidence that coadministration Further reduced CV risk. +FDA-approved as an adjunct to lipid-lowering treatments and diet for people with HoFH. 4
5 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Assumptions and Definitions Thresholds for consideration of net benefit Maximally-tolerated statin therapy Achievement of 50% LDL-C reduction on highintensity statin, or 30% to <50% reduction for moderate-intensity statin May consider absolute LDL-C levels (or non-hdl-c in patients with DM) as factors in treatment decisions ( LDL-C or non-hdl-c treatment thresholds ) Writing Committee emphasizes that these are not firm triggers for adding medication but factors that may be considered within the broader context of an individual patient s clinical situation Lloyd-Jones D et al. J Am Coll Cardiol. 2016;68:
6 2016 ACC Expert Consensus Decision Pathway: Patient with Stable Clinical ASCVD without Comorbidities (one of several settings for potential use of non-statin therapies for additional LDL-C lowering) Treat with maximal tolerated statin Achieve at least 50% LDL-C reduction If this reduction is not achieved, initiate patient clinician discussion and consider non-statins: LDL-C treatment threshold 100 mg/dl Try ezetimibe first; consider BAS if TG <300 mg/dl PCSK9 inhibitor next If treatment objective achieved, follow lipids If not, reassess medication adherence and lifestyle Lloyd-Jones D et al. J Am Coll Cardiol. 2016;68:
7 Ezetimibe Lipid / lipoprotein effects LDL-C: Decrease 13-20% Non-HDL-C: Decrease 14-19% HDL-C: Increase 3-5% TG: Decrease 5-11% Jacobson T J Clin Lipidol. 8:
8 Mean LDL-C (mg/dl) IMPROVE IT Trial: Effect on LDL-C Ezetimibe (EZ) + Simvastatin vs Simvastatin Alone yr mean LDL-C TC TG HDL-C hs-crp Simvastatin EZ/Simvastatin Δ in mg/dl Simvastatin Time since randomization (months) EZ/Simvastatin QE R Median Time avg 69.5 vs 53.7 mg/dl Cannon CP et al. Am Heart J. 2008;156: Study drug is administered once daily in the evening.
9 Primary Endpoint Event Rate (%) IMPROVE IT Trial Ezetimibe + Simvastatin vs Simvastatin Alone Primary Endpoint: death from cardiovascular disease, a major coronary event, or nonfatal stroke HR CI (0.887, 0.988) P=0.016 Simvastatin 34.7% 2742 events NNT = Ezetimibe/Simvastatin 32.7% 2572 events 7-year event rates Time Since Randomization (years) 7 Cannon CP et al. N Engl J Med. 2015;371:
10 ARS Question? Major statin trials have consistently shown a direct relationship between LDL-C reduction and reduced rates of adverse clinical events. Reducing LDL-C by approximately 40% generally reduces risk of adverse events by about: 1.1) 5% 2.2) 10% 3.3) 15% 4.4) 20% 5.5) 25%
11 Reduction in Rate of Major Vascular Events (%) IMPROVE-IT: Ezetimibe vs Statin Benefit Change in LDL-C vs Clinical Benefit 0.5 (19.3) 1.0 (38.6) 1.5 (57.9) Reduction in LDL Cholesterol: mmol/l (mg/dl) 2.0 (77.2) Cannon CP et al. CTT Collaboration. Lancet. 2005;366: CCT Collaboration. Lancet. 2010;376: Cannon CP et al. N Engl J Med. 2015;372:
 Secreted serine protease Chaperones LDL-R to")


12 Background Proprotein convertase subtilisin/kexin type 9 (PCSK9) Secreted serine protease Chaperones LDL-R to destruction circulating LDL-C PCSK9 inhibitor Gain of function mutation: Higher LDL-C Loss of function mutation: Lower LDL-C Lambert et al. Atherosclerosis. 2009; 203: 1-7 Soutar AK. Curr Op 12 Lipidol. 2011;22:192-96
13 FDA-Approved PCSK9 Inhibitors (fully human monoclonal antibodies) Alirocumab: Indicated as adjunct to diet and 1) maximally tolerated statin therapy for the treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease (CVD), who require additional lowering of LDL- C. Dose: Initiate 75 mg SQ every 2 weeks (The majority of patients achieve sufficient LDL-C redution with this dosage.) If LDL-C response is inadequate may be increased to 150 mg every 2 weeks. Evolocumab: Indicated as as an adjunct to diet and: 1) Maximally tolerated statin therapy for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease, who require additional lowering of LDL-C 2) Other LDL-C-loweing therapies (e.g., statins, ezetimibe, LDL apheresis) in patients with homozygous familial hypercholesterolemia (HoFH) who require additional lowering of LDL-C Dose: ASCVD or HeFH:; 140 mg every 2 weeks or 420 mg once monthly. For HoFH: 420 hg once monthly Note: The 420 mg dose can be administered: 1) over 9 minutes by using the single-use on-body infusor with prefilled cartridge, or 2) by SQ
14 PCSK9 Inhibitors and Lipid / Lipoprotein Effects LDL-C is reduced about 50-60% with alirocumab or evolocumab Same % reduction in LDL-C is seen with appropriate dosing when added to diet alone, low and maximal dose statin or statin plus ezetimibe Patients with HeFH and nonfh respond the same HoFH patients respond about half as well, with mean reductions in LDL-C of 31% to evolocumab Other blood lipids: Decreases in Lp(a), Apo B, Non-HDL-C, Total cholesterol, triglycerides. Increase in HDL-C.
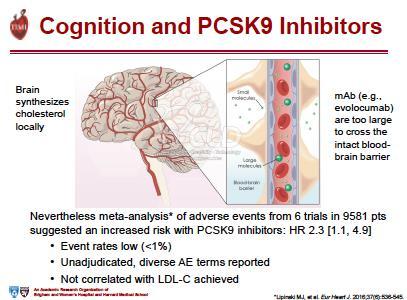
15 Safety Data from Studies Prior to FOURIER (ODYSSEY LONG TERM and OSLER 1/2) Alirocumab: Nasopharyngitis, injection site reactions, influenza Evolocumab: Nasopharyngitis, URI, influenza, back pain, and injection site reactions Self-reported neuro-cognitive AE * Alirocumab vs placebo: 1.2% vs 0.5% (Odyssey Long- Term) Evolocumab vs placebo: 0.9% vs 0.3% (OSLER 1/2) *Deliria, confusion; cognitive and attention disorders and disturbances; dementia and amnestic conditions; disturbances in thinking and perception; mental impairment disorders No diabetes signal in short-term trials. Robinson et al, NEJM 2015; Sabatine et al, NEJM, 2015; Lipinski et al, EHJ 2015; Colhoun et al. EHJ 2016
16 GLAGOV Trial Question: Does treatment with a PCSK9 inhibitor modify coronary atherosclerosis disease progression? Trial Summary: 968 patients with coronary disease treated with statins. Treated with evolocumab or placebo monthly for 76 wks and underwent IVUS determination of coronary atheroma volume. LDL-C levels reduced significantly in evolocumab group from 93 to 36 mg/dl vs from no change in placebo group. Significant reduction in percent atheroma volume with evolocumab vs placebo Significantly greater percentage of patients demonstated plaque regression Conclusion: Addition of PCSK9 inhibitor evolocumab to statin therapy produced greater LDL-C lowering and atheroma regression. Nicholls S et al. JAMA. 2016;316:
")
17 PCSK9 Inhibitors Cardiovascular Outcomes Trials Alirocumab Evolocumab Bococizumab Sponsor Sanofi/Regeneron Amgen Pfizer Trial ODYSSEY Outcomes FOURIER SPIRE I & 2 Sample Size 18,000 28,000 27,000 Patients 4-16 weeks post-acs MI, stroke, or PAD High risk of CV event Statin Evidence-based Rx Atorvastatin 20 mg or equivalent Lipid-lowering Rx LDL-C 70 mg/dl 70 mg/dl 70-99, >100 mg/dl Dosing (sc) Every 2 weeks Every 2 or Every 4 weeks Every 2 weeks Endpoint CHD death, MI, ischemic stroke, or UA hospitalization Primary: CV death, MI, stroke, UA hospitalization or coronary revascularization Key Secondary: CV death, MI, or stroke CV death, MI, stroke, or urgent revascularization Completion February 2018 November 2016 Discontinued 11/2016 Available at: Clinicaltrials.gov.
18 FOURIER Further cardiovascular OUtcomes Research with PCSK9 Inhibition in subjects with Elevated Risk MS Sabatine, RP Giugliano, AC Keech, N Honarpour, SM Wasserman, PS Sever, and TR Pedersen, for the FOURIER Steering Committee & Investigators American College of Cardiology 66 th Annual Scientific Session Late-Breaking Clinical Trial March 17, 2017 An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School
19 Trial Design 27,564 high-risk, stable patients with established CV disease (prior MI, prior stroke, or symptomatic PAD) Screening, Lipid Stabilization, and Placebo Run-in High or moderate intensity statin therapy (± ezetimibe) LDL-C 70 mg/dl or non-hdl-c 100 mg/dl Evolocumab SC 140 mg Q2W or 420 mg QM RANDOMIZED DOUBLE BLIND Placebo SC Q2W or QM Follow-up Q 12 weeks An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Sabatine MS et al. Am Heart J 2016;173:94-101
20 Baseline Characteristics Characteristic Value Age, years, mean (SD) 63 (9) Male sex (%) 75 Type of cardiovascular disease (%) Myocardial infarction 81 Stroke (non-hemorrhagic) 19 Symptomatic PAD 13 Cardiovascular risk factor (%) Hypertension 80 Diabetes mellitus 37 Current cigarette use 28 Median time from most recent event ~3 yrs An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Pooled data; no differences between treatment arms
21 Lipid Lowering Therapy & Lipid Levels at Baseline Characteristic Statin use (%)* Value High-intensity 69 Moderate-intensity 30 Ezetimibe use (%) 5 Median lipid measures (IQR) mg/dl LDL-C 92 (80-109) Total cholesterol 168 ( ) HDL-C 44 (37-53) Triglycerides 133 ( ) *Per protocol, patients were to be on atorva 20 mg/d or equivalent. 1% were on low intensity or intensity data were missing. Statin intensity defined per ACC/AHA 2013 Cholesterol Guidelines. An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Pooled data; no differences between treatment arms
22 LDL Cholesterol (mg/dl) LDL Cholesterol Placebo % mean reduction (95%CI 58-60), P< Absolute reduction: 56 mg/dl (95%CI 55-57) Evolocumab (median 30 mg/dl, IQR mg/dl) Weeks An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School
23 CV Death, MI, Stroke, Hosp for UA, or Cor Revasc Primary Endpoint 16% 14% 12% Hazard ratio % (95% CI, ) P< Placebo 12.6% 10% 8% 6% Evolocumab 4% 2% 0% Months from Randomization An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School
24 CV Death, MI, Stroke Landmark Analysis 8% 16% RRR 8% 25% RRR 6% HR 0.84 (95%CI ) P= % HR 0.75 (95%CI ) P< % 4% Placebo 2% 2% Evolocumab 0% An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School 0% Months from Randomization
25 Safety Evolocumab (N=13,769) Placebo (N=13,756) Adverse events (%) Any Serious Allergic reaction Injection-site reaction Treatment-related and led to d/c of study drug Muscle-related Cataract Diabetes (new-onset) Neurocognitive Laboratory results (%) Binding Ab 0.3 n/a Neutralizing Ab none n/a New-onset diabetes assessed in patients without diabetes at baseline; adjudicated by CEC An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School

26 Summary for Evolocumab LDL-C by 59% Consistent throughout duration of trial Median achieved LDL-C of 30 mg/dl (IQR mg/dl) CV outcomes in patients already on statin therapy 15% broad primary endpoint; 20% CV death, MI, or stroke Consistent benefit, incl. in those on high-intensity statin, low LDL-C 25% reduction in CV death, MI, or stroke after 1 st year Long-term benefits consistent w/ statins per mmol/l LDL-C Safe and well-tolerated Similar rates of AEs, incl DM & neurocog events w/ EvoMab & pbo Rates of EvoMab discontinuation low and no greater than pbo No neutralizing antibodies developed An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School
27 Confidential
28
29 Confidential
30
31
32 Available online NEJM March 17, 2017


33 Percent Reduction in LDLC The SPIRE Bococizumab Lipid Lowering Trials: Unanticipated Attenuation of LDL-C Reductions at 52 weeks 55.2 % reduction in LDLC at 12 weeks 42.5 % reduction in LDLC at 52 weeks 12 weeks, 150 mg 12 weeks, 75 mg 52 weeks, 150 mg 26 weeks, 150 mg Ridker ACC 2017
34 Cumulative proportion with MACE + UARUR The SPIRE-2 Cardiovascular Outcomes Trial: Baseline LDL-C > 100 mg/dl Primary Pre-Specified Endpoint* Placebo: 224 events Bococizumab 150 mg: 179 events (referent) HR %CI P = Baseline LDLC 133 mg/dl Placebo Event Rate 4.19 / 100-person years Median follow-up 12 months Weeks *Nonfatal myocardial infarction, nonfatal stroke, hospitalization for unstable angina requiring urgent revascularization, or cardiovascular death Ridker ACC 2017
35 Percent Change in LDLC The SPIRE Bococizumab Lipid Lowering Trials : Wide Individual Variation in Percent Change in LDLC at 52 Weeks with Bococizumab, Even Among Those Who Are Antidrug Antibody Negative* % 31% 60% 52 weeks ADA negative (N=780) No reduction Reduction<50% Reduction 50% * Analysis excludes non-compliant participants Ridker ACC 2017
36 Conclusions (1) Selection of Non-Statin Therapies: clinician-patient discussion (shared decision-making) is important CV outcome benefit with ezetimibe in addition to statin therapy (IMPROVE-IT) PCSK9 inhibitors have been evaluated in: Patients with FH Patients with high ASCVD risk and not at desirable LDL-C with maximally tolerated statin Patients intolerant to statin therapy
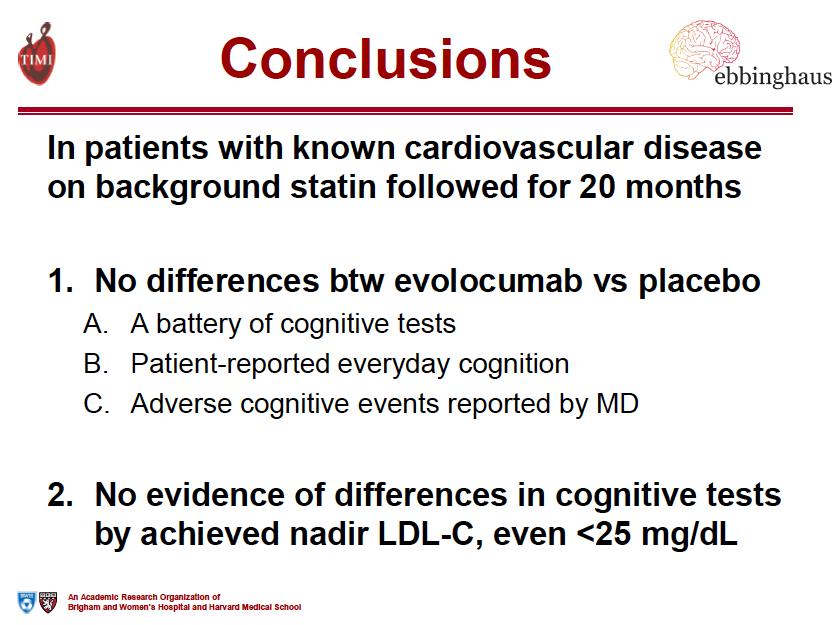
37 Conclusions (2) FOURIER / EBBINGHAUS: In pts with known CV disease: PCSK9 inhibition with evolocumab significantly & safely major CV events when added to statin therapy Benefit was achieved with lowering LDL-C well below current targets Are all agents in this class the same? No Discontinuation of bococizimab; awaiting CV outcome results with alirocumab in ODYSSEY OUTCOMES For LDL-Lowering, lower is better (lower than traditional goals)
38 In your patients with clinical ASCVD who require additional lowering of LDL- C and are on maximally tolerated statin therapy, how often WILL YOU NOW recommend adding a non-statin agent such as ezetimibe or a PCSK9 inhibitor?? 1.1) 100% of the time 2.2) 75% of the time 3.3) 50% of the time 4.4) 25% of the time 5.5) Never

39 Amazon s Top Rated Book: Heart Disease 100% of Profits to the American Heart Association
40 LDL Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: Emerging Insights Lynne T Braun, PhD, CNP, FAHA, FAANP, FPCNA, FNLA, FAAN Professor of Nursing and Medicine, Nurse Practitioner Rush University Medical Center
41 Disclosures None related to this presentation UpToDate: Author and Advisory Board 2
42 Objectives Discuss recommendations for the use of statin therapy in cholesterol guidelines. Recognize and describe patient populations who may benefit from further reductions in LDL-C despite statin therapy. Explain best practices in diagnosis and treatment of patients with familial hypercholesterolemia and statin intolerance. Describe clinical profiles of key non-statin therapies. (and emerging clinical data from ACC including FOURIER and EBBINGHAUS) Identify recommendations for the use of non-statin therapies in the ACC Expert Consensus Decision Pathway. 3
43 Age-Adjusted Death Rates for 10 Leading Causes of Death: 2014, 2015 Heart disease deaths increased in 2015 for the first time since Xu J, et al. NCHS Data Brief No December 2016

44 Cardiovascular Disease Mortality Trends Statins
45 Case Example: Mr. E.M. 75 years old PMHx CVA 1998 carotid artery disease with left ICA stent 1999 CAD with stent 2006 type 2 DM, HTN colon cancer with resection % stenosis of right ICA Retired teamster Lives with wife and 2 dogs; wife has MS Rarely drinks ETOH; smokes ppd since teenage years 6
46 Case continued Patient takes usual secondary prevention medications ASA 81 mg Atorvastatin 40 mg Valsartan, amlodipine, metoprolol Glipizide Lipid panel Total chol 131 mg/dl TG 132 mg/dl HDL 47 mg/dl LDL 48 mg/dl 7
47 ARS Question Mr. E.M. is treated according to the ACC/AHA Cholesterol Guideline for which of the following reasons? A. LDL-C is at < 100 mg/dl goal. B. LDL-C is at < 70 mg/dl goal. C. He takes a high intensity statin. D. His treatment and/or LDL-C goal is not in accordance with the ACC/AHA guideline.
48 Stone NJ et al., Circulation 2013, DOI: /01.cir a 9
49 ACC/AHA 2013 Guideline: Paradigm Shift Goal is ASCVD risk reduction rather than targeting specific LDL-C levels Statin intensity matched to ASCVD risk level, with less dependence on LDL-C levels Groups most likely to benefit from statin therapy Patients with clinical ASCVD LDL-C 190 mg/dl Diabetics age years with LDL-C mg/dl and without clinical ASCVD Non-diabetics age years with an estimated 10-year ASCVD risk of 7.5% Recommended statin intensity High intensity High intensity 7.5% 10-year ASCVD risk = high intensity <7.5% 10-year ASCVD risk = moderate intensity Moderate to high intensity if appropriate after clinician-patient discussion Finkel JB, Duffy D. Trends Cardiovasc Med. 2015;25(4): Stone NJ, et al. Circulation. 2014;129(25 Suppl 2):S1-45.
50 Use of Statins Statins have an acceptable margin of safety when used in properly selected individuals and appropriately monitored. Statin therapy recommended for secondary and primary prevention of ASCVD Based on RCTs, statins reduce morbidity and mortality associated with ASCVD Cost-effective: most statins are now generic 11
51 From Cholesterol Treatment Trialists (CTT) Collaboration. Lancet. 2015;385(9976): ; with permission. Efficacy and Safety of LDL-Lowering Therapy Meta-analysis of Individual Data from 174,000 Participants in 27 Randomized Trials Every 2 mg/dl in LDL 1% in CHD deaths
52 Managing Insufficient Response Intensity of Statin Therapy Reasonable Expectation for Treatment Response High-intensity statin therapy Average LDL-C reduction of 50% from the untreated baseline Moderate-intensity statin therapy Average LDL-C reduction of 30% to <50% from the untreated baseline Non-statin cholesterol-lowering drug(s) may be considered if the ASCVD risk-reduction benefits outweigh the potential for AEs. High-risk individuals include: Clinical ASCVD in those <75 years of age Baseline LDL 190 mg/dl Age 40 to 70 years with diabetes mellitus Preference should be given to agents shown to reduce ASCVD events in RCTs RCTs = randomized controlled trials Stone NJ, et al. Circulation. 2014;129(25 Suppl 2):S1-45.
53 Jacobson TA et al., Journal of Clinical Lipidology 2014; doi: /j.jacl
54 NLA Recommendations for Patient-Centered Management of Dyslipidemia Used evidence from more than randomized controlled trials for recommendations. Evidence that has accumulated since the 2004 update of the ATP III guidelines warrants a modest refinement of previous lipid-related risk management strategies. Importance of lifestyle therapies Jacobson TA et al., Journal of Clinical Lipidology 2014; doi: /j.jacl

55 Risk Assessment and Treatment Goals for Atherogenic Cholesterol Jacobson TA et al., Journal of Clinical Lipidology 2014; doi: /j.jacl
56 Case Example: K.C. 28 year old with FH 2014 total chol was 418 mg/dl; age mg/dl Family history: Father: age 53, hypercholesterolemia, treated with atorvastatin 80 mg, ezetimibe 10 mg; total chol mg/dl; otherwise healthy Paternal grandmother: CABG x 4, a second CABG years later Paternal uncle: died of MI at age 35 Paternal uncle: hypercholesterolemia Mother: no health problems Maternal grandmother: MI Patient s brother: normal cholesterol Patient is otherwise in good health; BMI 21.8 kg/m 2
57 Case Continued 2015 Lipid panel Total chol 455, HDL 55, TG 103, LDL > 350 mg/dl Left carotid bruit Ultrasound: no intimal thickness or plaque seen 2016 Lipid panel on atorvastatin 80 mg Total chol 187, HDL 44, TG 151, LDL 113 mg/dl Added ezetimibe 10 mg Total chol 202, HDL 46, TG 164, LDL 123 mg/dl
58 ARS Question If you were K.C. s provider, what should you do next? A. Change the statin. B. Assess adherence to lipid lowering therapies. C. Prescribe a PCSK9 inhibitor. D. Nothing the patient had an excellent response to lipid lowering therapies.
59 Familial Hypercholesterolemia Group of inherited genetic defects resulting in severely elevated cholesterol Prevalence HeFH: 1 in HoFH: 1 in a million Mutations in LDLR, ApoB, PCSK9 genes ~1600 known mutations of the LDLR gene (85-90% of FH cases) LDL-C 190 mg/dl (adults), 160 mg/dl (children and adolescents) FHx of high cholesterol and premature CHD in first degree relatives Think about FH with: Tendon xanthomas Arcus corneae in patient < 45 years Tuberous xanthomas or xanthelasma in patient < years Goldberg et al., J Clin Lipidol 2011;5:S1-S8.
60 21
61 Case Example: D.S. 54-year-old female with CAD History includes hyperlipidemia, obesity, former smoker Family history of premature CAD (mother MI at age 55) Medications: Nebivolol 5 mg daily Furosemide 20 mg daily NTG 0.4 mg SL Rosuvastatin 2.5 mg twice a week Statin intolerance: pravastatin (mental cloudiness), atorvastatin (muscle aches), pitavastatin (muscle aches), rosuvastatin (muscle/joint pain) Lipid panel: Total cholesterol 187 mg/dl Triglycerides 87 mg/dl HDL-C 49 mg/dl LDL-C 121 mg/dl
62 Case continued Evolocumab 140 mg subcutaneously every 2 weeks 6-week lipid panel: Total cholesterol 140 mg/dl Triglycerides 85 mg/dl HDL-C 53 mg/dl LDL-C 70 mg/dl Mild nasopharyngitis; fatigue for 2 days after injection
63 ARS Question Your patient reports muscle pain in her upper arms 3 months after starting atorvastatin 40 mg. Which of the following is related to statin intolerance and should be checked? A. Low serum potassium B. Low vitamin D level C. Iron deficiency anemia D. Your patient must have injured herself. Statins don t cause muscle pain.
64 Statins and Muscle Symptoms Frequency of statin-associated muscle symptoms: 1-5% in randomized controlled trials 11-29% in observational cohorts Spectrum of statin-associated muscle adverse events: Myalgia: unexplained muscle discomfort often described as flulike symptoms with normal CK level Myopathy: muscle weakness (not attributed to pain or elevated CK) Myositis: muscle inflammation Myonecrosis: muscle enzyme elevations or elevated CK Myonecrosis with myoglobinuria or acute renal failure (clinical rhabdomyolysis) CK = creatinine kinase Rosenson RS, et al. J Clin Lipidol. 2014;8(3 Suppl):S58-S71.

65 Statins and Adherence The most common non-genetic factor contributing to reduced statin response is poor medication adherence 40-70% of patients discontinue statin therapy one year after initiation The most common patient-reported reason for statin discontinuation or noncompliance is adverse effects >90% of statin-associated adverse events are musclerelated Fear of symptoms and adverse effects also contributes to non-adherence Banach M, et al. Int J Cardiol. 2016;225:
66 Statin Intolerance Definition: A clinical syndrome characterized by the inability to tolerate at least 2 statins Due to either objectionable symptoms (real or perceived) or abnormal lab determinations, which are temporally related to statin treatment Reversible upon discontinuation Reproducible by re-challenge Approximately 1 in 10 patients taking statins will report intolerance Novel non-statin agents may be appropriate in intolerant individuals Guyton JR, et al. J Clin Lipidol. 2014;8(3 Suppl):S72-S81. Jacobson TA, et al. J Clin Lipidol. 2015;9(6):S1-S122.
67 Approaches to Statin Intolerance Use a systematic approach to evaluate statin intolerance Careful history of symptoms Describe Timing Rule out other causes (hypothyroidism, vitamin D deficiency, recent exercise) Evaluate for drug-drug interactions Discontinue statin therapy and then rechallenge to verify recurrrence of muscle symptoms Rechallenge on at least 2-3 statins; use statins with different metabolic pathways and different lipophilicity 28

68 Managing Muscle Symptoms Switch to an alternate statin 92% of patients are able to tolerate a second statin after discontinuing their initial statin due to AEs 72.5% of patients who are intolerant to two statins due to myalgia can successfully tolerate a third statin Use an alternate dosing strategy Lower dose of the same statin Less-than-daily dosing Once-weekly dosing of a long-acting statin Switch to nonstatin lipid-lowering therapy in truly intolerant patients Rosenson RS, et al. J Clin Lipidol. 2014;8(3 Suppl):S58-S71.
.. What is the main reason you might miss your medication?")
69 Assess Adherence During Each Visit In the past 2 weeks, what percent of your cholesterol medicine would you say you have taken? (If less than 100%).. What is the main reason you might miss your medication? Discuss potential solutions with the patient.
70 Summary Statins are the class of medications with proven outcomes. If a patient is in a statin benefit group, several attempts should be made to find a medication regimen that is tolerated. High intensity statins are recommended for: Patients with clinical ASCVD Patients with LDL 190 mg/dl Patients with diabetes and a 10-year ASCVD risk 7.5% It s important to assess adherence in all patients but especially those who have a suboptimal response to statin therapy. Clinicians should thoroughly assess muscle symptoms in patients taking statins. Patients should be engaged in a discussion while initiating treatment and when making decisions about treatment options. 31
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial
 Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Guidelines on Lowering LDL-C Levels
 Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
REPATHA (PCSK9 INHIBITORS)
") REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
Reducing Cardiovascular Risk Through Non-Statins. Kim K. Birtcher, PharmD Joseph Saseen, PharmD
 Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia
 : 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
: 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Deep Dive into Contemporary Cholesterol Management. Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City
 Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis?
 Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
ADMINISTRATIVE POLICY AND PROCEDURE
 ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
EVOLOCUMAB Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378
 Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Educational Objectives. Disease Trajectories and CVD Risk Reduction. Hypercholesterolemia Support for LDL-C Causality
 Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Pharmacy Policy Bulletin
 Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
2017 Update in Internal Medicine: Clinical Dyslipidemia Update
 2017 Update in Internal Medicine: Clinical Dyslipidemia Update Erin E. Kershaw, M.D. Chief, Division of Endocrinology Associate Professor of Medicine Certified in Endocrinology, Diabetes, and Metabolism
2017 Update in Internal Medicine: Clinical Dyslipidemia Update Erin E. Kershaw, M.D. Chief, Division of Endocrinology Associate Professor of Medicine Certified in Endocrinology, Diabetes, and Metabolism
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Strategies for Managing Dyslipidemia Patients with Residual CVD Risk
 Strategies for Managing Dyslipidemia Patients with Residual CVD Risk Acknowledgements We acknowledge the work of Lynne T. Braun, PhD, CNP, FAHA, FPCNA, FAAN in the development of this presentation. Disclosures:
Strategies for Managing Dyslipidemia Patients with Residual CVD Risk Acknowledgements We acknowledge the work of Lynne T. Braun, PhD, CNP, FAHA, FPCNA, FAAN in the development of this presentation. Disclosures:
Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
 2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
Challenges in lipid management
 Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Cholesterol, guidelines, targets and new medications
 Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Praluent (alirocumab)
") Praluent (alirocumab) Policy Number: 5.01.600 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Praluent
Praluent (alirocumab) Policy Number: 5.01.600 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Praluent
EVIDENCE TO DATE EVOLOCUMAB (REPATHA)
") and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
Clinical Policy: Lomitapide (Juxtapid) Reference Number: ERX.SPA.170 Effective Date:
 Reference Number: ERX.SPA.170 Effective Date:") Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors
 Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Workshop. Todd Anderson MD / Jacques Genest MD
 Workshop Todd Anderson MD / Jacques Genest MD Game-Changing Trials 2017 FOURIER Evolocumab n=27,564 HR 0.80 CANTOS Canakinumab n=10,061 HR 0.85 COMPASS Rivaroxaban + ASA n=27,395 HR 0.76 Key Secondary
Workshop Todd Anderson MD / Jacques Genest MD Game-Changing Trials 2017 FOURIER Evolocumab n=27,564 HR 0.80 CANTOS Canakinumab n=10,061 HR 0.85 COMPASS Rivaroxaban + ASA n=27,395 HR 0.76 Key Secondary
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2
 Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
2/26/19. Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care. Disclosures. Faculty
 Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care Faculty v Karol E. Watson, MD, PhD Professor of Medicine/Cardiology Co-director, UCLA Program in Preventive Cardiology
Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care Faculty v Karol E. Watson, MD, PhD Professor of Medicine/Cardiology Co-director, UCLA Program in Preventive Cardiology
Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015. Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17
 Original Effective Date: 09/28/2015. Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17") Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015 Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17 Review Date(s): 5/4/2016, 4/17/2017, 7/10/2018 DISCLAIMER This Medical Policy
Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015 Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17 Review Date(s): 5/4/2016, 4/17/2017, 7/10/2018 DISCLAIMER This Medical Policy
Clinical Policy: Evolocumab (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017
 Reference Number: ERX.SPMN.184 Effective Date: 01/2017") Clinical Policy: (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Clinical Policy: (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges
 ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP
 Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Clinical Policy: Evolocumab (Repatha) Reference Number: ERX.SPA.169 Effective Date:
 Reference Number: ERX.SPA.169 Effective Date:") Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Repatha (evolocumab) Policy Number: Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019
 Policy Number: Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019") Repatha (evolocumab) Policy Number: 5.01.601 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Repatha
Repatha (evolocumab) Policy Number: 5.01.601 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Repatha
2/23/2018. Management of Hyperlipidemia Update on Guidelines and Novel Therapies. Burden of Heart Disease in U.S.
 Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
Managing Lipids and Cardiovascular Risk: Using the Data to Optimize Care
 Clinical Updates for Nurse Practitioners and Physician Assistants: 2018 Managing Lipids and Cardiovascular Risk: Using the Data to Optimize Care Faculty Robert L. Gillespie, MD, FACC, FASE, FASNC Immediate
Clinical Updates for Nurse Practitioners and Physician Assistants: 2018 Managing Lipids and Cardiovascular Risk: Using the Data to Optimize Care Faculty Robert L. Gillespie, MD, FACC, FASE, FASNC Immediate
Drug Prior Authorization Guideline PCSK9 Inhibitors -
 Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Clinical Policy: Evolocumab (Repatha) Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Juxtapid (lomitapide)
") Juxtapid (lomitapide) Policy Number: 5.01.599 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Juxtapid
Juxtapid (lomitapide) Policy Number: 5.01.599 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Juxtapid
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary
 Inhibitors Prior Authorization with Quantity Limit Program Summary") Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization
Indicações para um inibidor de PCSK9
 Indicações para um inibidor de PCSK9 Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical Research Institute Duke University Medical Center 1987 2017: 30 years since first
Indicações para um inibidor de PCSK9 Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical Research Institute Duke University Medical Center 1987 2017: 30 years since first
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University