PISA Physicians. Background. Kenneth B. Gossler M.D.
|
|
|
- Magnus Peter Carroll
- 5 years ago
- Views:
Transcription

1

2 PISA Physicians Kenneth B. Gossler M.D. Background M.D. University of Arizona 1992 Alpha Omega Alpha Anesthesiology Residency at University of Arizona 1996 Pain Management Fellowship Mayo Clinic 1997 Board Certified Anesthesiology and Pain Practicing Interventional Pain Management in Tucson since 1997
3 Evidence Based Pain Management Epidural Steroid Injections Lumbar and Cervical Facet Pain Chronic Opioid Therapy for Non- Malignant Pain
4 Evidence Based Criteria LEVEL I: Evidence obtained from at least one properly randomized controlled trial. LEVEL II: Evidence obtained from well designed controlled trials without randomization. LEVEL II-2: Evidence obtained from well designed cohort or case control analytic studies. LEVEL II-3: Evidence obtained from multiple time series with or without the interventions. LEVEL III: Opinions of respected authorities based on clinical experience case reports and experts.
5 Epidural Steroid Injections Fluoroscopically Guided Cervical, Thoracic, Lumbar and Caudal Levels Interlaminar vs. Transforaminal
6 Indications for Epidural Steroids Cervical and Lumbar Herniated Discs Cervical and Lumbar Spinal Stenosis Cervical and Lumbar Neuroforaminal Stenosis Post Laminectomy Syndrome Discogenic Low Back Pain
7 Epidural Steroids Mechanism of Action Interrupts nociceptive input Decreases the self-sustaining activity of the neuron pools in the Dorsal Horn and CNS Prolonged suppression of Neuronal Discharge Suppress sensitization of Dorsal Horn Neurons Inhibit inflammation especially in Herniated Discs
8 Interlaminar Lumbar and Transforaminal Epidural


9 Caudal and Cervical Epidural
10 Epidural Steroid Risks Post Dural Puncture Headache Epidural Hematoma Epidural Abscess Steroid Side Effects Paralysis: Spinal Cord Infarction Nerve Damage
11 Epidural Steroid Results Lumbar Herniated Disc : 74-86% Success Cervical Herniated Disc: 74% Success Spinal Stenosis with Leg Symptoms : 70% Success Discogenic Low Back Pain: 60% Post Laminectomy Syndrome: 60%
12 Evidence Based Pain Management Lumbar Transforaminal: Level II-2 for long term relief Caudal Epidurals: Level I for long term Blind Lumbar Epidurals: Level II-2 for short term relief for Lumbar HNP, Level III for spinal stenosis, discogenic LBP, Blind Cervical Epidurals Level II-1 (Strong recommendation) Pain Physician 2009; 12: E123-E198
13 Case Study 50 year old Male History 9 yrs of low back and right leg pain all the way to the ankle. Pain at 8 out of 10 Past Med Hx: Anxiety and Depression Medications: Methadone 50 mg tid & Ibuprofen 800mg tid Baclofen 10 mg 2 at bedtime Venlafaxine & Risperidone Clonazepam 1 mg trazodone
14 Case Study cont. Pt reports pain is unchanged despite 150mg of methadone per day. Primary care physician prescribed only enough methadone to get him to today s visit Family reports patient sleeps all day and his mood is depressed since starting methadone Prior treatment at another pain clinic included epidural steroids without relief. Pain clinic refuses to prescribe narcotics to any patients. Pt offered SCS trial.
15 Physical Exam Mental Status: Slurred Speech, Somnolent Normal Neuro ROM of lumbar spine essentially absent Exaggerated Pain Behaviors Motor Strength: Uncooperative Poor Effort MRI: DDD L5/S1, No stenosis, No HNP
16 What to Do?
17 Outcome Admit to inpatient Detox again and reassess Found to be exquisitely tender over L4/L5 and L5/S1 facets and that reproduces pain all the way down the leg Performed diagnostic medial branch blocks had 80% relief for 4+ hours Performed lumbar facet medial branch Rhizotomy. Pt reports at 6 wk f/u 80% relief. Taking no pain meds.
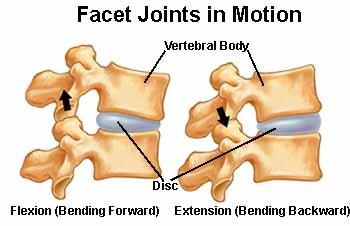
18 Facet Joint Pain (zygapophysial) Anatomy: formed by the superior and inferior articular processes of successive vertebrae. P.E. reveals tenderness in the paraspinal region with decreased R.O.M. Radiographs not very helpful for diagnosis
19

20 Facet Joint Pain Referral Pattern Primarily low back but with radiation. Described as achy difficult to localize. Worse with extension and rotation. No neurologic deficit.
21 Facet Joint Pain Chronic LBP due to Facet 30-40% of the time. Facet joint pain is Bilateral 60-79% of the time. Facet joint pain is usually two joints, but may involve three joints in 21-37% of the patients.
22 Lumbar Facet Arthropathy Cannot diagnose by radiographs P.E. and Clinical History somewhat helpful 40% of Persistent LBP is Facet Arthropathy Diagnostic Lumbar Medial Branch Blocks currently the test of choice. A positive DLMBB must have dramatic relief for the duration of local anesthetic or longer. False positives: Myofascial pain, DDD
23 Diagnostic Medial Branch Block Involve anesthetizing the lumbar medial branch of the dorsal rami that innervate the presumptive symptomatic joint. Two injections one week apart Patient then reports pain relief doing provocative maneuvers A patient obtaining >80% relief for the duration of the anesthetic indicates a successful block. EVIDENCE: Level I
24 Evidence for Diagnostic Facet Blocks Level I for diagnosing Facet Pain Level II-1 or II-2 for short and long term relief 82% of patients have >50% relief for 4-6 months with 3 injections.

25 Radio frequency Neurolysis of Lumbar Facets Involves placing RF probes on the DMB of the lumbar nerve root. RF needles heat tissue to 80 degrees killing the nerve.

26 Radio Frequency Generator


27 Lumbar Facet RF Neurolysis
28 Cervical Facet Pain symptoms Neck Pain Sub occipital HA s Shoulder and Supraclavicular Pain Crepitus/ Pain on Flexion to Ipsilateral Side Tenderness Over Cervical Facet Joints

29 Cervical Facet Pain Referral Pattern

30 Cervical Medial Branch Block

31 Cervical Radiofrequency

32 Cervical RF lateral
33 Facet RF Rhizotomy Lumbar Facet RF: Level II % of Patients received 60% or more relief, 60% had 90% relief at 12 months Cervical Facet RF Level II /28 had obtained complete relief for 3 mo or more, median duration 421 days Pain Physician 2009; 12: E123-E198
34 Chronic Opioid Therapy (COT) Evidence for Chronic Narcotic Therapy Brisk Review of Opioid Pharmacology Arizona Board of Medicine Guidelines Opioid Contracts Urine Drug Screens Dismissing Patients How we manage COT
35 Chronic Pain Prevalence of Chronic Pain: 9-20% of the population has moderate to severe chronic pain. More than 20% of patients in an average primary care practice have chronic pain Cost to treat chronic pain exceeds the combined cost of treating patients with coronary artery disease, cancer and AIDS.
36 Evidence Supporting Chronic Opioids Opioids moderately effective for pain relief Slightly effective for functional outcomes Pain relief is in the 30% range Very little evidence supporting use beyond 12 weeks Half of patients discontinue opioids There is no evidence supporting doses higher than 200mg/day morphine equivalents
37 Evidence Supporting Chronic Opioids Transdermal Fentanyl and Sustained Release Morphine evidence for improving functional status and pain is Level II-2 Oxycodone sustained release evidence is Level II-3 Hydrocodone and Methadone evidence is Level III Oxymorphone studied for 6 and 12 months found that it provided effective pain relief. Tramadol effective for pain and in one large study was abused 50% less than hydrocodone
38 Pharma Pain Studies week 1 week 2 week 3 week 4-12 Placebo Opioid
39 Sustained Release Opioids Morphine Oxycodone Transdermal Fentanyl Oxymorphone Transdermal Buprenorphine Tapentadol Methadone Tramadol Hydromorphone
40 Opioid Conversion Charts Opioid Morphine Oxycodone Hydrocodone Oxymorphone Tapentadol Hydromorphone Fentanyl Methadone Oral Equivalents 30 mg mg mg 10 mg mg mg ug/hr (transdermal) IMPOSSIBLE
41 ArizonaMedical Board Guidelines Evaluation of Chronic Pain Patient: Diagnosis Treatment Plan Informed Consent (can be verbal) Agreement for Treatment (can be verbal) Periodic Review Consultation with Specialist if Warranted Medical Records Termination From Medical Practice
42 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential.
43 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders
44 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent
45 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement (Written or Verbal)
46 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement (Written or Verbal) 5. Pre and Post-Intervention Assessment of Pain Level and Function
47 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement (Written or Verbal) 5. Pre and Post-Intervention Assessment of Pain Level and Function 6. Appropriate Trial of Opioids, Consider Adjuvants
48 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement (Written or Verbal) 5. Pre and Post-Intervention Assessment of Pain Level and Function 6. Appropriate Trial of Opioids, Consider Adjuvants 7. Reassessment of Pain and Function
49 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement (Written or Verbal) 5. Pre and Post-Intervention Assessment of Pain Level and Function 6. Appropriate Trial of Opioids, Consider Adjuvants 7. Reassessment of Pain and Function 8. Regularly Assess the Four A s
50 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement (Written or Verbal) 5. Pre and Post-Intervention Assessment of Pain Level and Function 6. Appropriate Trial of Opioids, Consider Adjuvants 7. Reassessment of Pain and Function 8. Regularly Assess the Four A s 9. Review Pain Diagnosis, Co morbid Conditions, Addictive Disorders
51 Ten Steps for Good Medical Practice 1. Make a Diagnosis with Appropriate Differential. 2. Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement (Written or Verbal) 5. Pre and Post-Intervention Assessment of Pain Level and Function 6. Appropriate Trial of Opioids, Consider Adjuvants 7. Reassessment of Pain and Function 8. Regularly Assess the Four A s 9. Review Pain Diagnosis, Co morbid Conditions, Addictive Disorders 10. Documentation Universal Precautions in Pain Medicine, Pain Medicine 2005, Vol 6, #2
52 Arizona Pharmacy Website Controlled Substances Prescription Monitoring Program Need to Register by mail: NOTORIZED Access website by DEA number and password Enter Patient s Name and Birth Date Only can review patients you are seeing or will be seeing Database is NOT all-inclusive.
53 Chronic Pain Patients Sir William Osler It is much more important to know what sort of a patient has a disease than what sort of disease a patient has.
54 Risk Factors for Prescription Drug Abuse Smokers 5 times the rate of abuse, 40% rate of monthly binge drinking. 1 Alcohol Abuse : 31% also abuse prescription drugs Chronic Pain Psychiatric Issues Low socioeconomic Status, Medicaid, Age less than 26, unemployed, male. Appearance, Behavior, Speech Pattern: Not Studied 1. Rural Kentucky
55 Opioid Agreement Written agreement to outline patient responsibilities Informed Consent: Addiction, Dependence, Tolerance, Overdose, Side effects, Pregnancy Only Obtain Opioids From one Physician, one Pharmacy Cannot Share medications No Early Refills, Called in Medications Will not replace lost, stolen or damaged medications Random Pill Counts and UDS
56 Urine Drug Screen Prescreen to look for drugs of abuse, and compliance with current therapy Continued Random Drug Screen: Used to encourage compliance and detect illicit drug use. Quantitative Urine Drug Screens used to measure compliance and detect possible diversion.
57 Urine Drug Screen dipstick In Office Point of Care Testing Test for Drugs of Abuse plus usual chronic Must get confirmatory testing for all positives before making clinical decisions. High Rate of False positives
58 Interpreting UDS Codeine Metabolized to Morphine Morphine can be metabolized to Hydromorphone Hydrocodone Metabolized to Hydromorphone Oxycodone metabolized to oxymorphone Methamphetamines false positives with cold medications Will dismiss patients for illicit drug use
59 Dismissing Patients Must give 30 days continued care. Not obligated to prescribe opioids if unsafe Can prescribe a tapering dose Medications to ameliorate withdrawal symptoms Some patients will go through withdrawal. Provide a list of other providers Referral for Detox
60 What we do: Starting COT History and Physical, Diagnosis, Prior records. Consider P.T. Interventional Procedures, Surgery Establish Medical Necessity No Narcotics on first visit, No Self Referral Urine Drug Screen on first visit and q 3mo, random Narcotic Agreement Risk Assessment Review Pharmacy Website
61 What we do: Follow Up Visit Analgesia Activities of Daily Living Adverse Effects Aberrant medication- Related Behaviors Pill Count Pharmacy Website UDS every 3 months, or random Once stable return to primary care.
62 Case Study 1 Problem: Patient on MS Contin 50mg one tab q 8hrs great pain relief, but getting nausea. Solution :Opioid rotation, Change to Oxycontin. Used company Supplied Conversion Ratio. 150mg Morphine= 100 mg Oxycontin Prescribed Oxycontin 40mg q 8hrs Result: Patient in E.D. Obtunded on Ventilator WHAT WENT WRONG?
63 Telephone Consult Homeless with chronic pain. On COT Sustained Release Morphine 60mg q 8 hr Four out the last 6 months his medications have been stolen.
64 Opioid Case Study 2 Patient recently moved to Tucson, was given a 2 month supply of Methadone, and ran out on schedule a month ago. Referred by primary care who is willing to take over prescribing after the pain medicine specialist re-establishes narcotic therapy. Pain Specialist restarts Methadone at the patients usual dose of 20mg q 8hrs.
65 Bibliography Manchikanti L, et. al, Comprehensive Review of Therapeutic Interventions in Managing Chronic Spinal Pain, Pain Physician, 2009; 12:E123-E198. Chou R, et. al., Clinical Guidelines for the Use of Chronic Opioid Therapy in Chronic Noncancer Pain, The Journal of Pain, 2009; 109:2, Trescot, Andrea M., et al, Opioids in the Management of Chronic Non-Cancer Pain: An Update of ASIPP Guidelines, Pain Physician, 2008; 11: S5-S62. Gourlay, Douglas L., Heit, Howard A., Almahrezi, A., Universal Precautions in Pain Medicine: A Rational Approach to the Treatment of Chronic Pain, Pain Medicine, 2005 Volume 6, Number 2, Vallejo, Ricardo, Barkin, Robert L., Wang Victor C., Pharmacology of Opioids in the Treatment of Chronic Pain Syndromes. Pain Physician 2011;14 E343- E360
66 Bibliography Manchikanti, L, et.al. Effectiveness of Caudal Epidural Steroid Injections in Discogram Positive and Negative Chronic Low Back Pain, Pain Physician, Volume 5, number 1, pp18-29, Manchikanti,L, Cash K.A, et. al. Preliminary Results of a Randomized, Double Blind, Controlled Trial of Fluoroscopic Lumbar Interlaminar Epidural Injections in Managing Chronic Lumbar Discogenic Pain Without Disc Herniation or Radiculitis, Pain Physician 2010, Number 13, E279-E292 Manchikanti, L., et. al., Evaluation of the Effectiveness of Lumbar Interlaminar Epidural Injections in Managing Chronic Pain of Lumbar Disc Herniation or Radiculitis, Double Blind, Controlled Trial, Pain Physician 2010, 13: Manchikanti, L., et al., One Year Results of a Randomized, Double Blind, Active Controlled Trial of Fluoroscopic Caudal Epidural Injections With or Without Steroids in Managing Chronic Discogenic Low Back Pain Without Disc Herniation or Radiculitis, Pain Physician 2011, 14:25-36.
Objectives. When to Refer. PISA Physicians 1/25/17. Financial Disclosures: None. PISA & THMEP January 28, 2017 Kenneth B. Gossler M.D.
 1/25/17 PISA & THMEP January 28, 2017 Kenneth B. Gossler M.D. PISA Physicians Kenneth B. Gossler M.D. Education University of Arizona Med School 1992. THMEP Intern 1993 Anesthesiology Residency at Financial
1/25/17 PISA & THMEP January 28, 2017 Kenneth B. Gossler M.D. PISA Physicians Kenneth B. Gossler M.D. Education University of Arizona Med School 1992. THMEP Intern 1993 Anesthesiology Residency at Financial
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Vijay Singh, M.D Roosevelt Rd., Niagara, WI 54151
 Publications and Book Chapters Vijay Singh, M.D. 1601 Roosevelt Rd., Niagara, WI 54151 PUBLICATIONS Jul-Aug 2012 Jul-Aug 2012 Jul-Aug 2012 Jul-Aug 2012 Jul-Aug 2012 July 2012 July 2012 May-Jun 2012 May-Jun
Publications and Book Chapters Vijay Singh, M.D. 1601 Roosevelt Rd., Niagara, WI 54151 PUBLICATIONS Jul-Aug 2012 Jul-Aug 2012 Jul-Aug 2012 Jul-Aug 2012 Jul-Aug 2012 July 2012 July 2012 May-Jun 2012 May-Jun
Discussion Points 10/17/16. Spine Pain is Ubiquitous. Interventional Pain Management
 Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
To: Manuel Suarez, M.D. Medical Director Neighborhood Health Plan Management Department 5757 Plaza Dr. Cyprus, CA Mailstop: CA
 To: Manuel Suarez, M.D. Medical Director Neighborhood Health Plan Management Department 5757 Plaza Dr. Cyprus, CA 30630 Mailstop: CA124-01290 Subject: Denial of Cervical Spinal Injection Procedures Dear
To: Manuel Suarez, M.D. Medical Director Neighborhood Health Plan Management Department 5757 Plaza Dr. Cyprus, CA 30630 Mailstop: CA124-01290 Subject: Denial of Cervical Spinal Injection Procedures Dear
Interventional Pain. Judith Dunipace MD Board certified in Anesthesiology, Pain Management and Hospice and Palliative Care
 Interventional Pain Judith Dunipace MD Board certified in Anesthesiology, Pain Management and Hospice and Palliative Care IASP Definition of Pain Pain is an unpleasant sensory or emotional experience associated
Interventional Pain Judith Dunipace MD Board certified in Anesthesiology, Pain Management and Hospice and Palliative Care IASP Definition of Pain Pain is an unpleasant sensory or emotional experience associated
MEDICAL HISTORY CHIRO PHYSICAL
 Overview of Spinal Injection Procedures Blake A. Johnson, MD, FACR 1 PATIENT MANAGEMENT EVALUATION TREATMENT P.T. MEDICAL CHIRO S SURGICAL Effective treatment requires a precise diagnosis! HISTORY PHYSICAL
Overview of Spinal Injection Procedures Blake A. Johnson, MD, FACR 1 PATIENT MANAGEMENT EVALUATION TREATMENT P.T. MEDICAL CHIRO S SURGICAL Effective treatment requires a precise diagnosis! HISTORY PHYSICAL
PROVIDER BULLETIN. Published by Wyoming Workers Compensation Medical Case Management Unit October 21, 2015
 Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
This evidence-informed guideline is for non-specific, non-malignant low back pain in adults only
 A Summary of the Guideline for the Evidence-Informed Primary Care Management of Low Back Pain This evidence-informed guideline is for non-specific, non-malignant low back pain in adults only Red Flags
A Summary of the Guideline for the Evidence-Informed Primary Care Management of Low Back Pain This evidence-informed guideline is for non-specific, non-malignant low back pain in adults only Red Flags
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Nonsurgical Interventional Treatments for Spinal Pain Management
 Nonsurgical Interventional Treatments for Spinal Pain Management I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain
Nonsurgical Interventional Treatments for Spinal Pain Management I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Neck Pain. Frank Thomas BSc(Hons) MBChB FANZCA FFPMANZCA
 MBChB FANZCA FFPMANZCA") Neck Pain Frank Thomas BSc(Hons) MBChB FANZCA FFPMANZCA Assessing Neck Pain Obtained detailed pain history Assess for red flags Assess range of neck movements Perform a neurological exam Identify psychosocial
Neck Pain Frank Thomas BSc(Hons) MBChB FANZCA FFPMANZCA Assessing Neck Pain Obtained detailed pain history Assess for red flags Assess range of neck movements Perform a neurological exam Identify psychosocial
Spinal and Trigger Point Injections
 Spinal and Trigger Point Injections I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain when determined to be medically
Spinal and Trigger Point Injections I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain when determined to be medically
Follow this and additional works at: Part of the Musculoskeletal Diseases Commons
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2016 Do Epidural Injections With Local Anesthetic
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2016 Do Epidural Injections With Local Anesthetic
An unpleasant sensory and emotional experience associated with actual or potential tissue damage.
 An unpleasant sensory and emotional experience associated with actual or potential tissue damage. Acute Pain results from disease, inflammation or injury to tissues; generally comes on suddenly and may
An unpleasant sensory and emotional experience associated with actual or potential tissue damage. Acute Pain results from disease, inflammation or injury to tissues; generally comes on suddenly and may
Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Disclosures. Management of Chronic Pain for Cancer Survivors. University of Kentucky HealthCare, Lexington, KY
 Management of Chronic Pain for Cancer Survivors Paul A. Sloan, M.D. Professor and Vice Chair for Research Associate Program Director, Pain Medicine Fellowship Department of Anesthesiology University of
Management of Chronic Pain for Cancer Survivors Paul A. Sloan, M.D. Professor and Vice Chair for Research Associate Program Director, Pain Medicine Fellowship Department of Anesthesiology University of
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
PACIFICSOURCE COMMUNITY SOLUTIONS AND GORGE COORDINATED CARE ORGANIZATION. Chronic Pain and Opiate Management Initiatives
 PACIFICSOURCE COMMUNITY SOLUTIONS AND GORGE COORDINATED CARE ORGANIZATION Chronic Pain and Opiate Management Initiatives Objectives To enhance understanding of current concepts, guidelines and risks of
PACIFICSOURCE COMMUNITY SOLUTIONS AND GORGE COORDINATED CARE ORGANIZATION Chronic Pain and Opiate Management Initiatives Objectives To enhance understanding of current concepts, guidelines and risks of
Interventional Pain Management
 Spinal Injections Can be beneficial for both chronic and acute pain depending on pathology Contraindications: Patient refusal Active infection Platelets less than 75 or inability to stop anticoagulation
Spinal Injections Can be beneficial for both chronic and acute pain depending on pathology Contraindications: Patient refusal Active infection Platelets less than 75 or inability to stop anticoagulation
Tennessee. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Ultrasound and Fluoroscopic Paravertebral Facet Joint Injections
 Policy Number FAC06222011RP Ultrasound and Fluoroscopic Approved By UnitedHealthcare Medicare Committee Current Approval Date 06/25/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable
Policy Number FAC06222011RP Ultrasound and Fluoroscopic Approved By UnitedHealthcare Medicare Committee Current Approval Date 06/25/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
CLINICAL POLICY DEPARTMENT: Medical
 IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
PERCUTANEOUS FACET JOINT DENERVATION
 Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-95 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-95 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Approaches to Responsible Opioid Prescribing. The Opioid Naïve Patient
 Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Conservative options to treat spine problems
 Conservative options to treat spine problems Low back pain is the most common disease in the United States. Neck pain is also extremely common. While most spine pain is caused by muscle spasms and can
Conservative options to treat spine problems Low back pain is the most common disease in the United States. Neck pain is also extremely common. While most spine pain is caused by muscle spasms and can
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
2011 Index by Key Words
 Pain Physician 2011; 14: 586-590 ISSN 1533-3159 2011 Index by Key Words A aberrant behavior... 383 abuse... 123, 175, 259 accelerometry... 407 acquired immune deficiency syndrome... E505 adaptive stimulation...
Pain Physician 2011; 14: 586-590 ISSN 1533-3159 2011 Index by Key Words A aberrant behavior... 383 abuse... 123, 175, 259 accelerometry... 407 acquired immune deficiency syndrome... E505 adaptive stimulation...
Pain Management Wrap-Up Chronic Care. David Tauben, MD Medicine Anesthesia & Pain Medicine
 Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Clinical Policy: Opioid Analgesics Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid
 Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
ESI - Utilization Review Case Presentation
 ESI - Utilization Review Case Presentation Request for ESI Hx & PE 31 y/o F parts warehouse stocker DOI: 2008 MOI: felt tightness in legs and shoulders reaching into a shelf to move a product from one
ESI - Utilization Review Case Presentation Request for ESI Hx & PE 31 y/o F parts warehouse stocker DOI: 2008 MOI: felt tightness in legs and shoulders reaching into a shelf to move a product from one
Medication Management
 Marina Treglia, AGPCNP BC April 4, 2019 Medication Management Identify patient criteria for risk mitigation in a medication management program at a multidisciplinary pain clinic Discuss opioid discontinuation
Marina Treglia, AGPCNP BC April 4, 2019 Medication Management Identify patient criteria for risk mitigation in a medication management program at a multidisciplinary pain clinic Discuss opioid discontinuation
A Patient s Guide to Pain Management: Epidural Steroid Injections
 A Patient s Guide to Pain Management: Epidural Steroid Injections 2778 N. Webb Rd. Wichita, KS 67226 Phone: (316) 631-1600 Fax: (316) 631-1617 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Pain Management: Epidural Steroid Injections 2778 N. Webb Rd. Wichita, KS 67226 Phone: (316) 631-1600 Fax: (316) 631-1617 DISCLAIMER: The information in this booklet is compiled from
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Medical Affairs Policy
 Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
MEDICAL POLICY EFFECTIVE DATE: 08/15/13 REVISED DATE: 07/17/14 SUBJECT: SPINAL INJECTIONS (EPIDURAL AND FACET INJECTIONS) FOR PAIN MANAGEMENT
 FOR PAIN MANAGEMENT") MEDICAL POLICY SUBJECT: SPINAL INJECTIONS (EPIDURAL AND PAGE: 1 OF: 7 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases,
MEDICAL POLICY SUBJECT: SPINAL INJECTIONS (EPIDURAL AND PAGE: 1 OF: 7 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases,
IEHP UM Subcommittee Approved Authorization Guidelines Referrals to Pain Management Specialists
 IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
Basic Standards for. Fellowship Training in. Acute and Chronic Pain Management. in Anesthesiology
 Basic Standards for Fellowship Training in Acute and Chronic Pain Management in Anesthesiology American Osteopathic Association and American Osteopathic College of Anesthesiologists BOT, 7/1995 BOT, 11/2002
Basic Standards for Fellowship Training in Acute and Chronic Pain Management in Anesthesiology American Osteopathic Association and American Osteopathic College of Anesthesiologists BOT, 7/1995 BOT, 11/2002
Shining a Light on MEDs Understanding morphine equivalent dose
 Shining a Light on MEDs Understanding morphine equivalent dose In the workers compensation industry, 60.2 percent of claimants utilize opioid analgesics for the treatment of pain caused by a workplace
Shining a Light on MEDs Understanding morphine equivalent dose In the workers compensation industry, 60.2 percent of claimants utilize opioid analgesics for the treatment of pain caused by a workplace
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
Outcome Measures: Numeric Rating Scale (NRS) pain scale, the Oswestry Disability Index 2.0 (ODI), employment status, and opioid intake.
 pain scale, the Oswestry Disability Index 2.0 (ODI), employment status, and opioid intake.") Pain Physician 2007; 10:425-440 ISSN 1533-3159 Randomized Trial Evaluation of Lumbar Facet Joint Nerve Blocks in the Management of Chronic Low Back Pain: Preliminary Report of A Randomized, Double-Blind
Pain Physician 2007; 10:425-440 ISSN 1533-3159 Randomized Trial Evaluation of Lumbar Facet Joint Nerve Blocks in the Management of Chronic Low Back Pain: Preliminary Report of A Randomized, Double-Blind
Kevin S. Ladin, M.D. Board Certified in Physical Medicine & Rehabilitation ABMS Subspecialty Board Certified in Pain Medicine
 Kevin S. Ladin, M.D. Board Certified in Physical Medicine & Rehabilitation ABMS Subspecialty Board Certified in Pain Medicine kslmd@cox.net EBM in Pain Medicine Evidence-based medicine (EBM) is a form
Kevin S. Ladin, M.D. Board Certified in Physical Medicine & Rehabilitation ABMS Subspecialty Board Certified in Pain Medicine kslmd@cox.net EBM in Pain Medicine Evidence-based medicine (EBM) is a form
Guideline Number: NIA_CG_301 Last Revised Date: March 2018 Responsible Department: Clinical Operations
 Magellan Healthcare Clinical guidelines PARAVERTEBRAL FACET JOINT INJECTIONS OR BLOCKS (no U/S) CPT Codes: Cervical Thoracic Region: 64490 (+ 64491, +64492) Lumbar Sacral Region: 64493 (+64494, +64495)
Magellan Healthcare Clinical guidelines PARAVERTEBRAL FACET JOINT INJECTIONS OR BLOCKS (no U/S) CPT Codes: Cervical Thoracic Region: 64490 (+ 64491, +64492) Lumbar Sacral Region: 64493 (+64494, +64495)
Vermont. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
IEHP UM Subcommittee Approved Authorization Guidelines Referrals to Pain Management Specialists
 IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
PRECISE DIAGNOSIS AND TREATMENT OF NECK AND BACK PAIN
 PRECISE DIAGNOSIS AND TREATMENT OF NECK AND BACK PAIN MEDICAL DIRECTOR Elgin, Itasca, Lake Barrington, McHenry, Libertyville, Huntley, Elmhurst John V. Prunskis M.D. FIPP JOHN V. PRUNSKIS Illinois M.D.
PRECISE DIAGNOSIS AND TREATMENT OF NECK AND BACK PAIN MEDICAL DIRECTOR Elgin, Itasca, Lake Barrington, McHenry, Libertyville, Huntley, Elmhurst John V. Prunskis M.D. FIPP JOHN V. PRUNSKIS Illinois M.D.
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Corporate Medical Policy
 Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Legal Issues in Opioid Prescribing
 Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
Prescription Drug Monitor Programs (PMDP): Combating prescription drug misuse and abuse. A physician s perspective.
: Combating prescription drug misuse and abuse. A physician s perspective.") Prescription Drug Monitor Programs (PMDP): Combating prescription drug misuse and abuse. A physician s perspective. Jeremy Johnson, MD UAB-Huntsville Family Medicine, Huntsville, AL Johnson Medical, LLC
Prescription Drug Monitor Programs (PMDP): Combating prescription drug misuse and abuse. A physician s perspective. Jeremy Johnson, MD UAB-Huntsville Family Medicine, Huntsville, AL Johnson Medical, LLC
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Phillip Weidner, DO, DABA, BCPM May 20th, 2014
 Phillip Weidner, DO, DABA, BCPM May 20th, 2014 Introduction Comprehensive Pain Management Center Interventional therapies Epidural steroid injections Sacroiliac interventions Facet joint disease Who to
Phillip Weidner, DO, DABA, BCPM May 20th, 2014 Introduction Comprehensive Pain Management Center Interventional therapies Epidural steroid injections Sacroiliac interventions Facet joint disease Who to
UCSD DEPARTMENT OF ANESTHESIOLOGY
 UCSD DEPARTMENT OF ANESTHESIOLOGY LEARNING OBJECTIVES FOR ADVANCED PAIN MEDICINE ROTATION, UCSD MEDICAL CENTER Competencies Objective Learning Environment Instructional Method Assessment Tool Patient Care:
UCSD DEPARTMENT OF ANESTHESIOLOGY LEARNING OBJECTIVES FOR ADVANCED PAIN MEDICINE ROTATION, UCSD MEDICAL CENTER Competencies Objective Learning Environment Instructional Method Assessment Tool Patient Care:
John Murphy DO, MS Lynx Healthcare
 Addiction to Pain Medication and Treatment John Murphy DO, MS Lynx Healthcare No Disclosures Objectives 1 Understand basic neurobiology and learning theory around opioid addiction 2 Identify aberrant behavior
Addiction to Pain Medication and Treatment John Murphy DO, MS Lynx Healthcare No Disclosures Objectives 1 Understand basic neurobiology and learning theory around opioid addiction 2 Identify aberrant behavior
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
A Patient s Guide to Pain Management: Epidural Steroid Injections
 A Patient s Guide to Pain Management: Epidural Steroid Injections 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is
A Patient s Guide to Pain Management: Epidural Steroid Injections 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is
INJECTION PROCEDURES
 INJECTION PROCEDURES GENERAL CONSIDERATIONS AND PREPARATION FOR THE INJECTION In general, injection procedures for the spine and some other parts of the body entail the use of live x- ray known as flouroscopy
INJECTION PROCEDURES GENERAL CONSIDERATIONS AND PREPARATION FOR THE INJECTION In general, injection procedures for the spine and some other parts of the body entail the use of live x- ray known as flouroscopy
Agenda. Case Discussions. Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT. Daniel Alford, MD Disclosures
 in Patients on MAT. Daniel Alford, MD Disclosures") Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 %
 Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Ahsan U. Rashid, M.D., F.A.C.P.
 Ahsan U. Rashid, M.D., F.A.C.P. OPIOID MAINTENANCE AND CONSENT Instructions: Review this document before signing. This document will help both the patient and caregivers in establishing a medical program
Ahsan U. Rashid, M.D., F.A.C.P. OPIOID MAINTENANCE AND CONSENT Instructions: Review this document before signing. This document will help both the patient and caregivers in establishing a medical program
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Safe and Competent Opioid Prescribing
 MILITARY Military Safe and Competent Opioid Prescribing Education (M-SCOPE) Program Safe and Competent Opioid Prescribing For Providers Working with Veterans and Military Service Personnel Daniel P. Alford,
MILITARY Military Safe and Competent Opioid Prescribing Education (M-SCOPE) Program Safe and Competent Opioid Prescribing For Providers Working with Veterans and Military Service Personnel Daniel P. Alford,
Opioids: Use and Misuse/Steven Feinberg, MD; Scott Levy, MD, MPH, FACOEM
 Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Oklahoma. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization
 AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine
 D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
Pain Management: Epidural Steroid Injections
 A Patient s Guide to Pain Management: Epidural Steroid Injections 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Pain Management: Epidural Steroid Injections 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from
Opioid Pain Contracts: A Resident Driven Quality Improvement Project
 Opioid Pain Contracts: A Resident Driven Quality Improvement Project A Response to the Opioid Epidemic Dr. Phillip Knouse Dr. Victoria Montgomery Disclosure None Objectives Discuss the current Opioid Epidemic
Opioid Pain Contracts: A Resident Driven Quality Improvement Project A Response to the Opioid Epidemic Dr. Phillip Knouse Dr. Victoria Montgomery Disclosure None Objectives Discuss the current Opioid Epidemic
Effective Date: 1/1/2019 Section: MED Policy No: 391 Medical Policy Committee Approved Date: 6/17; 12/18
 Effective Date: 1/1/2019 Section: MED Policy No: 391 Medical Policy Committee Approved Date: 6/17; 12/18 1/1/2019 Medical Officer Date APPLIES TO: Medicare Only See Policy CPT/HCPCS CODE section below
Effective Date: 1/1/2019 Section: MED Policy No: 391 Medical Policy Committee Approved Date: 6/17; 12/18 1/1/2019 Medical Officer Date APPLIES TO: Medicare Only See Policy CPT/HCPCS CODE section below
A Patient s Guide to Pain Management: Radiofrequency Ablation
 A Patient s Guide to Pain Management: Radiofrequency Ablation 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Pain Management: Radiofrequency Ablation 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
Prior Authorization Guideline
 Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline
 Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Approaches to Low Back Pain
 Approaches to Low Back Pain NECOM/MaAOHN Annual Conference December 4, 2014 Moderator: John W. Burress, MD, MPH, FACOEM Panelists: Mark Crislip, MD Kathryn Mueller, MD, MPH, FACOEM Tony Tannoury, MD Donald
Approaches to Low Back Pain NECOM/MaAOHN Annual Conference December 4, 2014 Moderator: John W. Burress, MD, MPH, FACOEM Panelists: Mark Crislip, MD Kathryn Mueller, MD, MPH, FACOEM Tony Tannoury, MD Donald
BAYLOR SCOTT & WHITE TEXAS SPINE & JOINT HOSPITAL
 BAYLOR SCOTT & WHITE TEXAS SPINE & JOINT HOSPITAL NAME: Initial Appointment / Reappointment / Update (Circle One) REQUESTED PRIVILEGE PAIN BLOCKS Blood Patch Hardware Block Epidurogram Fluoroscopy Intradural/Intrathecal
BAYLOR SCOTT & WHITE TEXAS SPINE & JOINT HOSPITAL NAME: Initial Appointment / Reappointment / Update (Circle One) REQUESTED PRIVILEGE PAIN BLOCKS Blood Patch Hardware Block Epidurogram Fluoroscopy Intradural/Intrathecal
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Karachi Spine - Pain and Minimally Invasive Spine Surgery Workshop. Lumbar Injections For Diagnosis and Treatment. Pain Management
 Lumbar Injections For Diagnosis and Treatment Pain Management Ovidiu Nicolae Palea Centrul de Diagnostic si Tratament ProVita Anesthesiology and Intensive Care 2009 decided to focus on Pain Management
Lumbar Injections For Diagnosis and Treatment Pain Management Ovidiu Nicolae Palea Centrul de Diagnostic si Tratament ProVita Anesthesiology and Intensive Care 2009 decided to focus on Pain Management
Chronic Pain Management in the Primary Care Setting
 Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
West Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile West Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile West Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prior Authorization for Opioid Products Indicated for Pain Management
 Kansas Medical Assistance Program PA Phone 800-933-6593 PA Fax 800-913-2229 Amerigroup PA Pharmacy Phone 855-201-7170 PA Pharmacy Fax 800-601-4829 Sunflower PA Pharmacy Phone 877-397-9526 PA Pharmacy Fax
Kansas Medical Assistance Program PA Phone 800-933-6593 PA Fax 800-913-2229 Amerigroup PA Pharmacy Phone 855-201-7170 PA Pharmacy Fax 800-601-4829 Sunflower PA Pharmacy Phone 877-397-9526 PA Pharmacy Fax
Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities
 Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities Svetla Slavova, PhD Sara LaMantia, MS Terry Bunn, PhD Tracey Corey, MD 2016 Safe States Annual Meeting April 13, 2016, Albuquerque,
Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities Svetla Slavova, PhD Sara LaMantia, MS Terry Bunn, PhD Tracey Corey, MD 2016 Safe States Annual Meeting April 13, 2016, Albuquerque,
Morphine er to oxycontin conversion
 Morphine er to oxycontin conversion The Borg System is 100 % Morphine er to oxycontin conversion 17-4-2011 Conversion dose from Oxycontin 40mg 3x a day to morphine sulfate 15 mg?. Oxycontin vs morphine
Morphine er to oxycontin conversion The Borg System is 100 % Morphine er to oxycontin conversion 17-4-2011 Conversion dose from Oxycontin 40mg 3x a day to morphine sulfate 15 mg?. Oxycontin vs morphine
Rhode Island. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Rhode Island Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Rhode Island Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Hydrocodone 10mg vs oxycodone 10 mg. What is the difference between oxycontin and oxycodone hcl 1 acetaminophen with oxycodone and roxicodone 5mg
 TE Te Hydrocodone 10mg vs oxycodone 10 mg What is the difference between oxycontin and oxycodone hcl 1 acetaminophen with oxycodone and roxicodone 5mg Manufacturer of oxycodone hcl 15 mg tablet side effects
TE Te Hydrocodone 10mg vs oxycodone 10 mg What is the difference between oxycontin and oxycodone hcl 1 acetaminophen with oxycodone and roxicodone 5mg Manufacturer of oxycodone hcl 15 mg tablet side effects
Pain Management Clinic ISIC
 Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
NASS Diagnosis and Treatment of Low-Back Pain Guideline Draft Clinical Question Protocol
 NASS Diagnosis and Treatment of Low-Back Pain Draft Clinical Questions Public Comment period: June 16-July 14, 2015 Comments should be sent to guidelines@spine.org Background The North American Spine Society
NASS Diagnosis and Treatment of Low-Back Pain Draft Clinical Questions Public Comment period: June 16-July 14, 2015 Comments should be sent to guidelines@spine.org Background The North American Spine Society
National Imaging Associates, Inc. Clinical guidelines FACET JOINT INJECTIONS, MEDIAL BRANCH BLOCKS, AND FACET JOINT RADIOFREQUENCY NEUROTOMY
 National Imaging Associates, Inc. Clinical guidelines FACET JOINT INJECTIONS, MEDIAL BRANCH BLOCKS, AND FACET JOINT RADIOFREQUENCY NEUROTOMY CPT Codes: Refer to pages 5 and 6 LCD ID Number: L35936 J K
National Imaging Associates, Inc. Clinical guidelines FACET JOINT INJECTIONS, MEDIAL BRANCH BLOCKS, AND FACET JOINT RADIOFREQUENCY NEUROTOMY CPT Codes: Refer to pages 5 and 6 LCD ID Number: L35936 J K
Mri with baclofen pump
 Mri with baclofen pump 830 South Main St Suite 2 Orrville, OH 44667. 1207 W. State St. Suite N Alliance, OH 44601. NeuroCare Orrville Hours: W & TH 7AM-4:30PM (subject to change). var r = [99, 104, 101,
Mri with baclofen pump 830 South Main St Suite 2 Orrville, OH 44667. 1207 W. State St. Suite N Alliance, OH 44601. NeuroCare Orrville Hours: W & TH 7AM-4:30PM (subject to change). var r = [99, 104, 101,
Thoracic Cooled-RF Training Presentation
 Thoracic Cooled-RF Training Presentation Patient Selection Anatomy Overview Neuroanatomy Lesion targets Technique Diagnostic Block Cooled-RF Precautions Summary Appendix AGENDA Patient Selection Thoracic
Thoracic Cooled-RF Training Presentation Patient Selection Anatomy Overview Neuroanatomy Lesion targets Technique Diagnostic Block Cooled-RF Precautions Summary Appendix AGENDA Patient Selection Thoracic