Neuromuscular pain Clinical Assessment and Therapeutic Management. Dr Jean-Jacques LABAT Dr Jérôme RIGAUD
|
|
|
- Ashlyn Bridges
- 5 years ago
- Views:
Transcription

1 Neuromuscular pain Clinical Assessment and Therapeutic Management Dr Jean-Jacques LABAT Dr Jérôme RIGAUD
2 Chronic Post-operative operative pelvi-perineal Pain Eliminate Infection Haematoma Mesh erosion Normal standard imagery Chronic Pain > 6 months
3 Neuropathic Pain Per-operative Traumatism Direct (section ± total) Indirect (retractor, haematoma) Progressive nerve lesion Nevroma Nerve Entrapment by fibrosis
4 Somatic Neuropathic Pain Arguments Localization Troncular (or radicular) systematization Type of Pain Burning, shooting, numbness, stabbing or aching pain Superficial Hypoesthesia Allodynia Anatomo-clinic correlation +++ Which surgery for which nerve? Which nerve for which surgery? Operative report +++
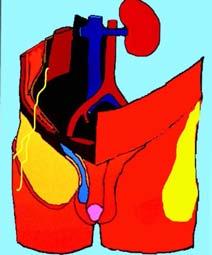
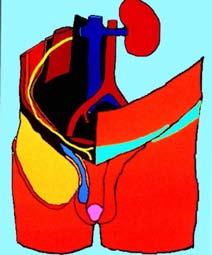
5 Ilio inguinal Génito-fémoral Obturateur Cluneal inf Pudendal
6 Mechanism Operative traumatism Immediate neurological troubles Favourable progressive evolution Fibrosis and chronic compression Progressive installation and aggravation Nevroma Paroxysmal pain Trigger point, Tinel
7 Chronology +++++
8 High-Risk Surgery Oncological surgery Abdominal wall surgery All abdominal scares (transversal or lateral) Prosthesis Mesh Incontinence surgery Sub-urethral sling Prolapse surgery Prosthesis Mesh (abdominal or vaginal approach)
9 Clinical Assessment Therapeutic Management
10 Parietal Nerves

11 Ilio-hypogastrique Ilio-inguinal Cutané latéral de la cuisse Génito-fémoral

12 Parietal Nerves High-risk Surgery Hernia repair (Aasvang et al ) 5-10% at 1 year (EVA > 5 in 2-4%) Neuropathic pain Decrease of threshold of painand cold perception Increase of threshold of tactile and warm perception Dysejaculation 2.5 % No interest of imagery (MRI)
13 Parietal Nerves High-risk Surgery All lateral abdominal incisions Open surgery Laparoscopic surgery Transversal incision 10 % caesarian Excepted Median incision
14 Parietal Nerves Clinical Assessment Exam of scares Trigger point Relative interest of EMG Infiltration loco-dolenti ++ Diagnosis Anaesthetic Therapeutic Corticoids Improvement 70% (Palumbo et al 2007)
15 Treatment Parietal Nerves Exploration of the scares with neurolysis If trigger point (Nevroma) Improvement 75% Pulsed Radiofrequency Improvement 4/5 (1-9 months) (Rozen et al2006) Improvement 1 case (Mitra et al 2007)
16 Treatment Ilio-inguinal Neurectomy Ligatured and cauterization (Zacest et al 2009) Improvement in 70 % Severe Pain, follow-up 1.5 years (loos et al2009) 50% pain free or almost pain free 25% moderate improvement 25% no benefit Selective Neurectomy + Mesh removal (Aasvang et al 2009) VAS score Parietal Nerves 27 before vs 13 after Follow-up 6 months Worsening pain in 15%
17 Pudendal Nerve
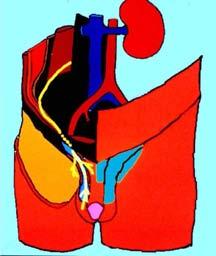
18 Ilio inguinal Génito-fémoral Obturateur Cluneal inf Pudendal
19 Pudendal Neuralgia High-Risk Surgery Not exposed Proximal lesion Prolapse surgery (Richter) Pain in 4,5% (1/3 pudendal) Distal lesion Urinary incontinence surgery Prolapse vaginal surgery (Mesh) Impotence surgery
20 Per-operative Pudendal Per-operative Pudendal neuralgia Neuralgia Pain Localization (cf anat) Subjective and objective sensory deficiency Hypoesthesia Numbness Decrease the sensation of urination and defecation Motor deficiency Urinary and anal continence troubles Sexual deficiency Erectile dysfunction Decrease sexual sensation
 (Labat JJ et al 2007) Pain in the anatomical territory of the pudendal nerve From the anus to the penis or clitoris Worsened by sitting The patient is not")
21 Pudendal neuralgia by entrapment Secondary symptomatology Apparition of real pudendal neuralgia by pudendal nerve entrapment? Diagnostic criteria (Critères de Nantes) (Labat JJ et al 2007) Pain in the anatomical territory of the pudendal nerve From the anus to the penis or clitoris Worsened by sitting The patient is not woken at night by the pain No objective sensory loss on clinical examination Positive anaesthetic pudendal nerve block
22 Post-operative operative Pudendal Neuralgia neuralgia Pre-existing asymptomatic pudendal nerve entrapment appear (decompensated) after all pelvic surgery Treatment of the entrapment Clinical Assessment MRI Compression (tumor, haematoma, ) Infiltration Nerve block (CT-Scan guidance) if entrapment Not necessary if deficiency Proximal lesion near the sacral plexus by stitch or clip, Negative diagnosis nerve block at ischial spine Positive Radicular block at S3
23 Post-operative operative Pudendal neuralgia Neurolysis According to the initial surgery Prolapse surgery (Richter) Transgluteal approach Laparoscopic approach (Possover et al 2007) Distal lesion Vaginal or perineal approach Good results, several months Interest of laparoscopic exploration (Possover et al 2009) 109 cases of pudendal pain ( ) Exploration of sacral plexus, dissection of pudendal nerve Endometriose Entrapment 43 cases 13 case Post-op lesion (fibrosis) 53 cases Improvement 62% at mean follow-up of 17 months
24 Obturator Nerve
25 Ilio inguinal Génito-fémoral Obturateur Cluneal inf Pudendal


26 Obturator Neuralgia High-risk Surgery Oncological pelvic surgery Urinary incontinence surgery Hernia repair surgery (mesh)
27 Obturator Neuralgia Pain of anterior-internal surface of the thigh Descending to the inside of the knee No pain in the lower leg Neuropathic pain Burning, paresthesia or allodynia Alleviated in the sitting or lying down position Exacerbated on walking Exacerbated by weight bearing on one leg Limping with a sidestepping gait No sensory or motor deficiency Positive infiltration test
28 Obturator Neuralgia Clinical Assessment Imagery Organic compression EMG Haematoma, tumor Discuss Denervation of adductor muscles Infiltration test ++ Posterior approach CT-Scan guidance
29 Anterior Obturator nerve block


30 Posterior Obturator nerve block
31 Posterior Approach Obturator Nerve Obturator Neuralgia Infiltration block Obturator Nerve Anterior approach Posterior Approach Anterior Approach
32 Obturator Neuralgia Treatment Per-operative section Suture Radiofrequency or cryoanalgesia Laparoscopic Neuolysis (J Rigaud et al 2008) Iatrogenic obturator neuralgia Release of the nerve + section of the scarring fibrosis or prosthetic mesh in contact TOT (3 cases), TVT (3 cases), hernia mesh (2 cases), haematoma (1 case) Idiopathic obturator neuralgia Release of the nerve + incision of 2 to 3 cm in the internal obturator muscle (obturator foramen)

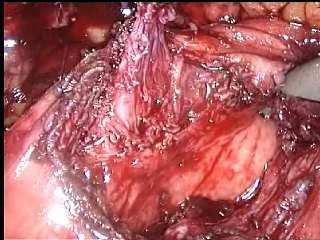
33 Normal Obturator Nerve

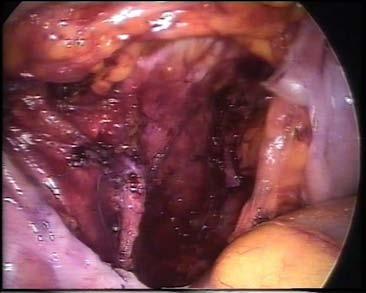
34 Iatrogenic Obturator Neuralgia (TVT)



35 Idiopathic Obturator Neuralgia
36 Our Experience (Rigaud J et al ) 2009) Total (n = 13) Iatrogenic (n = 9) Idiopathic (n = 4) Mean VAS score before surgery 7.3 ± ± ± 0 Mean VAS score after surgery 2.4 ± ± ± 2.3 VAS = 0 Decrease of VAS score > 50% Failure 54 % (n=7) 23 % (n=3) 23 % (n=3) 55 % (n=5) 11 % (n=1) 33 % (n=3) 50 % (n=2) 50 % (n=2) 0 % (n=0) Follow-up (months) % Improvement
37 Muscular Pain
38 Myo-fascial Pain Diffuse pain at palpation Endopelvic side, Buttock Fibromyalgia Muscular tension Obturator internus muscle Levator ani muscle Syndrome of the Obturator internus muscleor piriformis muscle Global pain in several nervous area

39 Example: Pain localised at perineal, perineal, buttock, buttock, inside of inside the of the knee knee and and sciatic sciatic after after a transobturator a transobturatrice tape Myofascial Syndrome of the Obturator internus muscle and piriformis muscle Buttock portion linked with sciatic nerve and posterior cutaneous nerve of the thigh Pelvic portion linked with pudendal nerve and obturator nerve Buttock and pelvic Trigger points


40 5 cms Piriformis Muscle Syndrome Obturator Internus Muscle Syndrome
41 High-Risk surgery Trans-obturator route TOT Vaginal Mesh Trans-levatori route TVT Myorrhaphy

42 TVT TOT
43 Pain after TVT/TOT Post-operative pain 15% Persistant pain 1% (> 5% -30%) Meta-analysis (Latthe et al 2007) 11 randomized, controlled studies 1261 cases: 630 TVT 631 TOT Incidence of Pain TVT 1.3% TOT 12 % (OR of 9.34)
44 Pain after TVT/TOT Treatment Cystoscopy and Imagery (MRI) Tape into the bladder (Frenkl et al 2008) Section or ablation by an endoscopic approach Tape Infiltration (Duckett et al 2005) 4/6 Improvement (not durable) Surgical Removal Few series with few patients 15 patients (Misrai et al2009)
45 TVT

46 TVT
47 TVT
48 Our Experience From November 2004 to August patients with pelvic pain after TVT/TOT 2 groups: TVT (n=17) and TOT (n=15) Delay tape placement - tape removal 37 months Associated Neuropathic Pain Pudendal: TVT (41%) vs TOT (20%) (Rigaud J et al 2010) p=0,1972 Obturator: TVT (18%) vs TOT (47%) p=0,0772
49 Tape removal Our Experience TVT group (retropubic tape) (n=17) Transperitoneal laparoscopy approach in every cases Tape in the levator ani muscle 70% (n=12) Tape in the bladder wall 23% (n=4) TOT group (transobturator tape) (n=15) Transvaginal approach (Rigaud J et al 2010) Possibly associated with a unilateral or bilateral incision in the proximal part of the thigh (8 cases)


50 TVT into the levator ani muscle


51 TVT into the bladder wall
52 Total TVT TOT n VAS Before VAS After % of Improvement 56% 55% 56% Rate of Improvement Our Experience (Rigaud J et al 2010) 0% 25% 23% 27% < 50% 6% 6% 7% > 50% 53% 59% 47% 69% 100% 16% 12% 20% Urinary Incontinence 22% 24% 20% Follow-up (months)
53 Pelvic Neural Pain Laparoscopic exploration (Possover et al 2009) 120 cases of pelvic neural pain secondary to pelvic surgery Exploration Superior hypogastric plexus Nerve decompression Sacral plexus Improvement in 65%
54 Complex Pelvic Pain
55 Post-operative Pain not systematized Myo-fascial Pain Neuropathic Pain Complex Regional Pain Syndrome Emotional context Medico-legal context Hypersensitization type fibromyalgia Visceral Hypersensitization : urinary, digestive, genital Predisposing factors Surgery = Matchstick Consequence = Blaze
56 Conclusions Post-operative Pain Direct or Indirect Neurological lesion Myofascial Pain Chronology of facts +++ (Operative report) Listen the patients Medico-legal consideration Treatment Infiltration Surgery: Neurolysis, mesh removal
Pathogenesis of Chronic Pelvic Pain
 Pathogenesis of Chronic Pelvic Pain Yong-Chul Kim Department of anesthesia and pain medicine, Seoul National University College of Medicine 1 Overview Anatomy Nerve innervation CPP by pathology CPP by
Pathogenesis of Chronic Pelvic Pain Yong-Chul Kim Department of anesthesia and pain medicine, Seoul National University College of Medicine 1 Overview Anatomy Nerve innervation CPP by pathology CPP by
Dana Alrafaiah. - Amani Nofal. - Ahmad Alsalman. 1 P a g e
 - 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
- 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
Pelvic and perineal truncular and radicular neuropathic pain. R ROBERT Anatomist- Neurosurgeon Nantes FRANCE
 Pelvic and perineal truncular and radicular neuropathic pain R ROBERT Anatomist- Neurosurgeon Nantes FRANCE Anatomical facts 1 perineal muscles 2 fibrous central perineal nucleus 3 external anal sphincter
Pelvic and perineal truncular and radicular neuropathic pain R ROBERT Anatomist- Neurosurgeon Nantes FRANCE Anatomical facts 1 perineal muscles 2 fibrous central perineal nucleus 3 external anal sphincter
Lumbar Plexus. Ventral rami L1 L4 Supplies: Major nerves.. Abdominal wall External genitalia Anteromedial thigh
 Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lumbar and Sacral Plexuses. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Lumbar and Sacral Plexuses Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Structure of Spinal Nerves: Somatic Pathways dorsal root CNS interneuron spinal nerve dorsal ramus somatic sensory
Lumbar and Sacral Plexuses Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Structure of Spinal Nerves: Somatic Pathways dorsal root CNS interneuron spinal nerve dorsal ramus somatic sensory
Inferior Pelvic Border
 Pelvis + Perineum Pelvic Cavity Enclosed by bony, ligamentous and muscular wall Contains the urinary bladder, ureters, pelvic genital organs, rectum, blood vessels, lymphatics and nerves Pelvic inlet (superior
Pelvis + Perineum Pelvic Cavity Enclosed by bony, ligamentous and muscular wall Contains the urinary bladder, ureters, pelvic genital organs, rectum, blood vessels, lymphatics and nerves Pelvic inlet (superior
Dora Street, Hurstville 160 Belmore Road, Randwick
 www.orthosports.com.au 29 31 Dora Street, Hurstville 160 Belmore Road, Randwick Pudendal Nerve Entrapment Andreas Loefler Hip, Knee, and Spine Surgeon PNE Pudendal Neuralgia Alcock s Syndrome Cyclists
www.orthosports.com.au 29 31 Dora Street, Hurstville 160 Belmore Road, Randwick Pudendal Nerve Entrapment Andreas Loefler Hip, Knee, and Spine Surgeon PNE Pudendal Neuralgia Alcock s Syndrome Cyclists
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
Table 2. First Generated List of Expert Responses. Likert-Type Scale. Category or Criterion. Rationale or Comments (1) (2) (3) (4)
 (2) (3) (4)") Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Dr Hannah Blakely. Dr Ben Sharp. Ms Julee Binns. Sara Widdowson. 7:15-8:15 Breakfast Session: Oxford Women's Health
 Dr Hannah Blakely Clinical Psychologist Oxford Women's Health Ms Julee Binns Consultant Physiotherapist Oxford Women's Health, Christchurch Sara Widdowson NZ Registered Dietitian Christchurch Public Hospital
Dr Hannah Blakely Clinical Psychologist Oxford Women's Health Ms Julee Binns Consultant Physiotherapist Oxford Women's Health, Christchurch Sara Widdowson NZ Registered Dietitian Christchurch Public Hospital
24-May-16. Pelvic and Perineal Pain: Beyond Endometriosis and Pregnancy. Jason Chow. Heartsink! Background
 Heartsink! Pelvic and Perineal Pain: Beyond Endometriosis and Pregnancy Jason Chow 1 2 Background 4 1 Surgery More 20% no response to surgery 32% placebo response 1 st surgery 2 nd surgery 83% reduction
Heartsink! Pelvic and Perineal Pain: Beyond Endometriosis and Pregnancy Jason Chow 1 2 Background 4 1 Surgery More 20% no response to surgery 32% placebo response 1 st surgery 2 nd surgery 83% reduction
Evaluation of Posterior Hip Pain
 Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Taking the Myths Out of Pudendal Nerve Entrapment Surgery
 Taking the Myths Out of Pudendal Nerve Entrapment Surgery (Sequel to Taking the Shame Out of Pudendal Neuralgia) 1 By Violet Matthews, RN, BSN, Secretary, Health Organization for Pudendal Education www.pudendalhope.org
Taking the Myths Out of Pudendal Nerve Entrapment Surgery (Sequel to Taking the Shame Out of Pudendal Neuralgia) 1 By Violet Matthews, RN, BSN, Secretary, Health Organization for Pudendal Education www.pudendalhope.org
REPRODUCTIVE SYSTEM By Dr.Ahmed Salman
 The University Of Jordan Faculty Of Medicine Anatomy Department REPRODUCTIVE SYSTEM By Dr.Ahmed Salman Assistant Professor of Anatomy &embryology Perineum It is the diamond-shaped lower end of the trunk
The University Of Jordan Faculty Of Medicine Anatomy Department REPRODUCTIVE SYSTEM By Dr.Ahmed Salman Assistant Professor of Anatomy &embryology Perineum It is the diamond-shaped lower end of the trunk
2. List the 8 pelvic spaces: list one procedure or dissection which involves entering that space.
 Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Interventional Treatments for Pelvic Pain
 Interventional Treatments for Pelvic Pain Ameet Nagpal, MD, MS, MEd Clinical Assistant Professor, Department of Anesthesiology University of Texas Health Science Center at San Antonio No relevant financial
Interventional Treatments for Pelvic Pain Ameet Nagpal, MD, MS, MEd Clinical Assistant Professor, Department of Anesthesiology University of Texas Health Science Center at San Antonio No relevant financial
Neuromodulation and the pudendal nerve
 Neuromodulation and the pudendal nerve Stefan De Wachter, MD, PhD, FEBU Professor of Urology University of Antwerpen, Belgium Chairman dept of Urology, UZA Disclosures Consultant speaker: Astellas, Medtronic,
Neuromodulation and the pudendal nerve Stefan De Wachter, MD, PhD, FEBU Professor of Urology University of Antwerpen, Belgium Chairman dept of Urology, UZA Disclosures Consultant speaker: Astellas, Medtronic,
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566
 Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology
 Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Prevention of Surgical Injuries in Gynecology
 in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
PITA Pain In The A** And Other Pains You May Not Have Heard Of. Allan S. Gordon MD Neurologist and Director Wasser PMC/ MSH
 PITA Pain In The A** And Other Pains You May Not Have Heard Of Allan S. Gordon MD Neurologist and Director Wasser PMC/ MSH Wasser Pain Management Centre Clinical care, education and research in chronic
PITA Pain In The A** And Other Pains You May Not Have Heard Of Allan S. Gordon MD Neurologist and Director Wasser PMC/ MSH Wasser Pain Management Centre Clinical care, education and research in chronic
Surgical treatment of urinary stress incontinence with tension free vaginal tape
 Surgical treatment of urinary stress incontinence with tension free vaginal tape Gynaecology department 01935 384 385 yeovilhospital.nhs.uk Many surgical operations are available for the treatment of
Surgical treatment of urinary stress incontinence with tension free vaginal tape Gynaecology department 01935 384 385 yeovilhospital.nhs.uk Many surgical operations are available for the treatment of
Desara and Desara Blue
 Desara and Desara Blue Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc.
Desara and Desara Blue Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc.
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics.
 NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal mesh background of, 84 85 Age as factor in PFDs, 8 Anal plugs in FI management in women, 107 Anterior compartment native tissue
Index Note: Page numbers of article titles are in boldface type. A Abdominal mesh background of, 84 85 Age as factor in PFDs, 8 Anal plugs in FI management in women, 107 Anterior compartment native tissue
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
25-Feb-16. Pelvic and Perineal Pain: Beyond Endometriosis and Pregnancy. Jason Chow. Heartsink! Background
 Heartsink! Pelvic and Perineal Pain: Beyond Endometriosis and Pregnancy Jason Chow 1 2 Background 4 1 Surgery More 20% no response to surgery 32% placebo response 1 st surgery 2 nd surgery 83% reduction
Heartsink! Pelvic and Perineal Pain: Beyond Endometriosis and Pregnancy Jason Chow 1 2 Background 4 1 Surgery More 20% no response to surgery 32% placebo response 1 st surgery 2 nd surgery 83% reduction
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015
 Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
10/15/2012. Pelvic Pain and Dysfunction
 Pain and Holly Bommersbach PT, MPT Angela De La Cruz PT, MPT Pain which occurs in the perineal and/or anal areas Pain in the lower abdomen, low back and/or pelvic girdle Pain may often affect other areas,
Pain and Holly Bommersbach PT, MPT Angela De La Cruz PT, MPT Pain which occurs in the perineal and/or anal areas Pain in the lower abdomen, low back and/or pelvic girdle Pain may often affect other areas,
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Perineum. done by : zaid al-ghnaneem
 Perineum done by : zaid al-ghnaneem Hello everyone, this sheet will talk about 2 nd Lecture which is Perineum but there are some slides and info from 1 st Lecture. Everything included Slides + Pics Let
Perineum done by : zaid al-ghnaneem Hello everyone, this sheet will talk about 2 nd Lecture which is Perineum but there are some slides and info from 1 st Lecture. Everything included Slides + Pics Let
Desara Blue OV D I. Sling for Female Stress Urinary Incontinence. Instructions For Use
 Desara Blue OV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc. 5171 Clareton
Desara Blue OV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc. 5171 Clareton
Dear Patient, Sincerely, The Pelvic Health and Rehabilitation Center
 Dear Patient, Welcome to the Pelvic Health and Rehabilitation Center! We specialize in physical therapy management of numerous pelvic pain disorders. We believe in a multidisciplinary collaborative approach
Dear Patient, Welcome to the Pelvic Health and Rehabilitation Center! We specialize in physical therapy management of numerous pelvic pain disorders. We believe in a multidisciplinary collaborative approach
Pelvis MCQs. Block 1. B. Reproductive organs. C. The liver. D. Urinary bladder. 1. The pelvic diaphragm includes the following muscles: E.
 Pelvis MCQs Block 1 1. The pelvic diaphragm includes the following muscles: A. The obturator internus B. The levator ani C. The coccygeus D. The external urethral sphincter E. The internal urethral sphincter
Pelvis MCQs Block 1 1. The pelvic diaphragm includes the following muscles: A. The obturator internus B. The levator ani C. The coccygeus D. The external urethral sphincter E. The internal urethral sphincter
Ali Yaghi. Omar Eyad. Ahmad Salman. 1 P a g e
 5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL
 ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL The Pelvis is just about as complicated as head and neck and considerably more mysterious. You have to be able to visualize (imagine) the underlying
ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL The Pelvis is just about as complicated as head and neck and considerably more mysterious. You have to be able to visualize (imagine) the underlying
Lower Extremity Ultrasound-Guided Regional Anesthesia. Stephanie Duffy, CRNA Regional Anesthesia Faculty Acute Pain Service NMCSD
 Lower Extremity Ultrasound-Guided Regional Anesthesia Stephanie Duffy, CRNA Regional Anesthesia Faculty Acute Pain Service NMCSD Objectives Review anatomy of lumbosacral plexus Lumbar plexus blocks Psoas
Lower Extremity Ultrasound-Guided Regional Anesthesia Stephanie Duffy, CRNA Regional Anesthesia Faculty Acute Pain Service NMCSD Objectives Review anatomy of lumbosacral plexus Lumbar plexus blocks Psoas
ARTIFICIAL MESH REPAIR FOR TREATMENT OF PELVIC ORGAN PROLAPSE
 Pelvic Floor Unit / Department of Gynaecology Ward 17, Singleton Hospital, Sketty, Swansea, SA2 8QA 01792 205666 Secretary Direct Line: 01792 285688. Fax: 01792 285874 ARTIFICIAL MESH REPAIR FOR TREATMENT
Pelvic Floor Unit / Department of Gynaecology Ward 17, Singleton Hospital, Sketty, Swansea, SA2 8QA 01792 205666 Secretary Direct Line: 01792 285688. Fax: 01792 285874 ARTIFICIAL MESH REPAIR FOR TREATMENT
Neurologic complications - whom to blame? Benno Rehberg Médecin adjoint agrégé Unité d anesthésiologie gynéco-obstétricale, HUG
 Neurologic complications - whom to blame? Benno Rehberg Médecin adjoint agrégé Unité d anesthésiologie gynéco-obstétricale, HUG SAOA spring meeting 2015 The simple surgical answer: outline Epidemiology
Neurologic complications - whom to blame? Benno Rehberg Médecin adjoint agrégé Unité d anesthésiologie gynéco-obstétricale, HUG SAOA spring meeting 2015 The simple surgical answer: outline Epidemiology
Pudendal Neuralgia Due to Pudendal Nerve Entrapment: Warning Signs Observed in Two Cases and Review of the Literature
 2150-1149 Case Report Pudendal Neuralgia Due to Pudendal Nerve Entrapment: Warning Signs Observed in Two Cases and Review of the Literature Stéphane Ploteau, MD 1,2, Claire Cardaillac, MSc 2, Marie-Aimée
2150-1149 Case Report Pudendal Neuralgia Due to Pudendal Nerve Entrapment: Warning Signs Observed in Two Cases and Review of the Literature Stéphane Ploteau, MD 1,2, Claire Cardaillac, MSc 2, Marie-Aimée
CHERRY BAKER AND TRACEY GJERTSEN BSC MCSP HCPC INTRODUCTION TO DIAMOND TRAINING REHAB AND PERFORMANCE FOR PELVIC POWER
 CHERRY BAKER AND TRACEY GJERTSEN BSC MCSP HCPC INTRODUCTION TO DIAMOND TRAINING REHAB AND PERFORMANCE FOR PELVIC POWER What is it? Where is it? Breathing Graded relaxation Incontinence Stress Incontinence
CHERRY BAKER AND TRACEY GJERTSEN BSC MCSP HCPC INTRODUCTION TO DIAMOND TRAINING REHAB AND PERFORMANCE FOR PELVIC POWER What is it? Where is it? Breathing Graded relaxation Incontinence Stress Incontinence
Pain Management Clinic ISIC
 Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
Doc, I've done my groin. Groin Pain. Peter Brukner. Doc, I've done my groin 1. acute chronic
 Doc, I've done my groin Peter Brukner Associate Professor in Sports Medicine Centre for Sports Medicine Research and Education School of Physiotherapy 9/22/2006 The University of Melbourne Groin Pain acute
Doc, I've done my groin Peter Brukner Associate Professor in Sports Medicine Centre for Sports Medicine Research and Education School of Physiotherapy 9/22/2006 The University of Melbourne Groin Pain acute
The University Of Jordan Faculty Of Medicine THE LOWER LIMB. Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan
 The University Of Jordan Faculty Of Medicine THE LOWER LIMB Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Gluteal Region Cutaneous nerve supply of (Gluteal region) 1. Lateral cutaneous
The University Of Jordan Faculty Of Medicine THE LOWER LIMB Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Gluteal Region Cutaneous nerve supply of (Gluteal region) 1. Lateral cutaneous
I-STOP TOMS Transobturator Male Sling
 I-STOP TOMS Transobturator Male Sling The CL Medical I-STOP TOMS sling for male stress urinary incontinence was developed in France where it is widely used and is the market leader. It is constructed with
I-STOP TOMS Transobturator Male Sling The CL Medical I-STOP TOMS sling for male stress urinary incontinence was developed in France where it is widely used and is the market leader. It is constructed with
Sacral, ilioinguinal, and vasal nerve stimulation for treatment of pelvic, sacral, inguinal and testicular Pain.
 Chapter 14 Sacral, ilioinguinal, and vasal nerve stimulation for treatment of pelvic, sacral, inguinal and testicular Pain. Introduction Sacral nerve root stimulation has been recognized as a treatment
Chapter 14 Sacral, ilioinguinal, and vasal nerve stimulation for treatment of pelvic, sacral, inguinal and testicular Pain. Introduction Sacral nerve root stimulation has been recognized as a treatment
Support Information Advocacy Education Research CHRONIC PELVIC PAIN. w w w. p e l v i c p a i n. o r g. u k. w w w. p e l v i c p a i n. o r g.
 Support Information Advocacy Education Research The Pelvic Pain Support Network would be pleased to hear from clinicians and researchers with an interest in this field. For further information please contact:
Support Information Advocacy Education Research The Pelvic Pain Support Network would be pleased to hear from clinicians and researchers with an interest in this field. For further information please contact:
1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:
 What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:") Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Inguinal and Femoral Hernias. August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center
 Inguinal and Femoral Hernias August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center Background Approximately 20 million groin hernias are repaired each
Inguinal and Femoral Hernias August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center Background Approximately 20 million groin hernias are repaired each
Technologies and architectures" Stimulator, electrodes, system flexibility, reliability, security, etc."
 March 2011 Introduction" Basic principle (Depolarization, hyper polarization, etc.." Stimulation types (Magnetic and electrical)" Main stimulation parameters (Current, voltage, etc )" Characteristics (Muscular
March 2011 Introduction" Basic principle (Depolarization, hyper polarization, etc.." Stimulation types (Magnetic and electrical)" Main stimulation parameters (Current, voltage, etc )" Characteristics (Muscular
Yes, cranially with ovarian, caudally with vaginal. Yes, with uterine artery (collateral circulation between abdominal +pelvic source)
") Blood supply to internal female genitalia: uterine Internal iliac Sup. large branch: uterus, inf. Small branch: cervix+ sup. Vagina Yes, cranially with ovarian, caudally with vaginal Medially in base of
Blood supply to internal female genitalia: uterine Internal iliac Sup. large branch: uterus, inf. Small branch: cervix+ sup. Vagina Yes, cranially with ovarian, caudally with vaginal Medially in base of
Paravaginal Repair: A Laparoscopic Approach
 44 Paravaginal Repair: A Laparoscopic Approach John R. Miklos and Robert Moore Atlanta Urogynecology Associates, Atlanta, Georgia, U.S.A. Neeraj Kohli Harvard University, Boston, Massachusetts, U.S.A.
44 Paravaginal Repair: A Laparoscopic Approach John R. Miklos and Robert Moore Atlanta Urogynecology Associates, Atlanta, Georgia, U.S.A. Neeraj Kohli Harvard University, Boston, Massachusetts, U.S.A.
Visceral and Urogenital pain. Natasha Curran FRCA FFPMRCA University College London Hospitals 28 th January 2010 Royal College of Anaesthetists
 Visceral and Urogenital pain Natasha Curran FRCA FFPMRCA University College London Hospitals 28 th January 2010 Royal College of Anaesthetists Outline Visceral pain The chronic pelvic pain syndromes Patient
Visceral and Urogenital pain Natasha Curran FRCA FFPMRCA University College London Hospitals 28 th January 2010 Royal College of Anaesthetists Outline Visceral pain The chronic pelvic pain syndromes Patient
Laparoscopic management of pudendal pain different endopelvic etiologies in 134
 Laparoscopic management of pudendal pain different endopelvic etiologies in 134 consecutive patients Univ.-Prof. Prof. Dr. Med. Marc Possover, MD, PhD Introduction Perianal and perineal pain is a frequent
Laparoscopic management of pudendal pain different endopelvic etiologies in 134 consecutive patients Univ.-Prof. Prof. Dr. Med. Marc Possover, MD, PhD Introduction Perianal and perineal pain is a frequent
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Neuroanatomy, Neurophysiology and Clinical Presentation of Visceral Urological Pain
 Neuroanatomy, Neurophysiology and Clinical Presentation of Visceral Urological Pain Prof Dr K. Everaert Functional urology Department of Urology Ghent University Hospital Gent, Belgium Chronic pelvic pain
Neuroanatomy, Neurophysiology and Clinical Presentation of Visceral Urological Pain Prof Dr K. Everaert Functional urology Department of Urology Ghent University Hospital Gent, Belgium Chronic pelvic pain
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
Electrostimulation Part 3: Bladder dysfunctions
 GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
Scottish Clinical Coding Standards
 Scottish Clinical Coding Standards Number 16 October 2017 Scottish Clinical Coding Standards ICD-10 Sepsis Sepsis is a serious condition which must always be coded when documented in the medical record.
Scottish Clinical Coding Standards Number 16 October 2017 Scottish Clinical Coding Standards ICD-10 Sepsis Sepsis is a serious condition which must always be coded when documented in the medical record.
URINARY INCONTINENCE
 Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Mr. LBP: Case Presentation
 CLINICAL CASES Case: Mr. LBP Mr. LBP: Case Presentation Mr. LBP is a 35-year-old male He fell down while participating in a recreational sports activity He subsequently developed low back pain Upon arrival
CLINICAL CASES Case: Mr. LBP Mr. LBP: Case Presentation Mr. LBP is a 35-year-old male He fell down while participating in a recreational sports activity He subsequently developed low back pain Upon arrival
GBM8320 Dispositifs Médicaux Intelligents. Electrostimulation. Part 3: Bladder dysfunctions
 GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia
 Disclosure & Acknowledgment Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia Disclosures - None Acknowledgements Dr. Andrea Furlan Dr. Julia Alleyne Dr. Hamilton Hall
Disclosure & Acknowledgment Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia Disclosures - None Acknowledgements Dr. Andrea Furlan Dr. Julia Alleyne Dr. Hamilton Hall
MATERIALS AND METHODS
 Pelvic nerve injury following gynecologic surgery: a prospective cohort study Justin C. Bohrer, MD; Mark D. Walters, MD; Amy Park, MD; David Polston, MD; Matthew D. Barber, MD, MHS OBJECTIVE: The purpose
Pelvic nerve injury following gynecologic surgery: a prospective cohort study Justin C. Bohrer, MD; Mark D. Walters, MD; Amy Park, MD; David Polston, MD; Matthew D. Barber, MD, MHS OBJECTIVE: The purpose
Injection of Urethral Bulking Agents
 Injection of Urethral Bulking Agents Department of Gynaecology Patient Information What are urethral bulking agents? Urethral bulking agents are substances that are injected to support the bladder neck.
Injection of Urethral Bulking Agents Department of Gynaecology Patient Information What are urethral bulking agents? Urethral bulking agents are substances that are injected to support the bladder neck.
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Urinary incontinence: the management of urinary incontinence in women
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
HERNIAS .(A) .(B) 5. .(A) 7..( (Lumbar hernia),
 .(B) 5. .(A) 7..( (Lumbar hernia),") HERNIAS ysms91@wonju.yonsei.ac.kr 1..(B) 2..(B) 3..(A) 4. (Hesselbach's striangle).(b) 5.,.(A) 6. (Sliding hernia).(a) 7..( (Lumbar hernia), (Obturator hernia), (Sciatica hernia)).(b) Hernia = rupture
HERNIAS ysms91@wonju.yonsei.ac.kr 1..(B) 2..(B) 3..(A) 4. (Hesselbach's striangle).(b) 5.,.(A) 6. (Sliding hernia).(a) 7..( (Lumbar hernia), (Obturator hernia), (Sciatica hernia)).(b) Hernia = rupture
Sacral Neuromodulation Beyond Pelvic Pain!!!
 Sacral Neuromodulation Beyond Pelvic Pain!!! Dr. Hirachand S Mutagi. Senior Consultant Pain Physician. Head -Sakra World Hospital. Director ReLeaf Pain Services. Rapid advances in neurostimulation therapy
Sacral Neuromodulation Beyond Pelvic Pain!!! Dr. Hirachand S Mutagi. Senior Consultant Pain Physician. Head -Sakra World Hospital. Director ReLeaf Pain Services. Rapid advances in neurostimulation therapy
Management of Neuropathic pain
 Management of Neuropathic pain Ravi Parekodi Consultant in Anaesthetics and Pain Management 08/04/2014 Ref: BJA July2013, Map of Medicine2013, Pain Physician 2007, IASP 2012, Nice guideline 2013 Aims Highlight
Management of Neuropathic pain Ravi Parekodi Consultant in Anaesthetics and Pain Management 08/04/2014 Ref: BJA July2013, Map of Medicine2013, Pain Physician 2007, IASP 2012, Nice guideline 2013 Aims Highlight
Efficacy and Adverse Effects of Monarc Versus Tension-free Vaginal Tape Obturator: a Retrospective One-year Follow-up Study
 Efficacy and Adverse Effects of Monarc Versus Tension-free Vaginal Tape Obturator: a Retrospective One-year Follow-up Study Yvonne KY CHENG MBChB, MRCOG William WK TO MBBS, M Phil, FRCOG, FHKAM (O&G) HX
Efficacy and Adverse Effects of Monarc Versus Tension-free Vaginal Tape Obturator: a Retrospective One-year Follow-up Study Yvonne KY CHENG MBChB, MRCOG William WK TO MBBS, M Phil, FRCOG, FHKAM (O&G) HX
CERVICAL SPINE TIPS A
 CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
nerve blocks in the diagnosis and therapy of visceral disease
 Visceral Pain nerve blocks in the diagnosis and therapy of visceral disease Guy Hans, MD, PhD Dept. of Anesthesiology, Multidisciplinary Pain Center Visceral Pain? Type of nociceptive pain (although often
Visceral Pain nerve blocks in the diagnosis and therapy of visceral disease Guy Hans, MD, PhD Dept. of Anesthesiology, Multidisciplinary Pain Center Visceral Pain? Type of nociceptive pain (although often
Physiologic Anatomy and Nervous Connections of the Bladder
 Micturition Objectives: 1. Review the anatomical organization of the urinary system from a physiological point of view. 2. Describe the micturition reflex. 3. Predict the lines of treatment of renal failure.
Micturition Objectives: 1. Review the anatomical organization of the urinary system from a physiological point of view. 2. Describe the micturition reflex. 3. Predict the lines of treatment of renal failure.
Gluteal region DR. GITANJALI KHORWAL
 Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Bony ypelvis. Composition: formed by coccyx, and their articulations Two portions
 Pelvis Bony ypelvis Composition: formed by paired hip bones, sacrum, coccyx, and their articulations Two portions Greater pelvis Lesser pelvis Terminal line ( pelvic inlet): formed by promontory of sacrum,
Pelvis Bony ypelvis Composition: formed by paired hip bones, sacrum, coccyx, and their articulations Two portions Greater pelvis Lesser pelvis Terminal line ( pelvic inlet): formed by promontory of sacrum,
One Slim Needle One Incision. One Simple Solution for Stress Urinary Incontinence. The Difference is in the Data
 CONTINENCE SOLUTIONS One Slim Needle One Incision ordering information Description US International Order Number Order Number One Simple Solution for Stress Urinary Incontinence MiniArc Single-Incision
CONTINENCE SOLUTIONS One Slim Needle One Incision ordering information Description US International Order Number Order Number One Simple Solution for Stress Urinary Incontinence MiniArc Single-Incision
UNCORRECTED PROOF ABSTRACT CASE REPORT. Harold M. Olson, DC, CCSP, Andrew J. Zetocha, DC, and Courtney A. Olson, DPT
 JCM-00370; No of Pages 4 1 Chiropractic Management of a Patient 2 With Perineal Numbness After 3 Arthroscopic Hip Surgery: A Case Report Q34Q2 Harold M. Olson, DC, CCSP, Andrew J. Zetocha, DC, and Courtney
JCM-00370; No of Pages 4 1 Chiropractic Management of a Patient 2 With Perineal Numbness After 3 Arthroscopic Hip Surgery: A Case Report Q34Q2 Harold M. Olson, DC, CCSP, Andrew J. Zetocha, DC, and Courtney
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Neuropelveological assessment of neuropathic pelvic pain
 Gynecol Surg (2014) 11:139 144 DOI 10.1007/s10397-014-0838-4 ORIGINAL ARTICLE Neuropelveological assessment of neuropathic pelvic pain M. Possover & A. Forman Received: 11 July 2013 /Accepted: 5 March
Gynecol Surg (2014) 11:139 144 DOI 10.1007/s10397-014-0838-4 ORIGINAL ARTICLE Neuropelveological assessment of neuropathic pelvic pain M. Possover & A. Forman Received: 11 July 2013 /Accepted: 5 March
Trans-Vaginal Mesh Revision: A Comprehensive Review on Etiologies and Management Strategies with Emphasis on Postoperative Pain Outcomes
 LUTS (2014) 6, 69 75 REVIEW ARTICLE Trans-Vaginal Mesh Revision: A Comprehensive Review on Etiologies and Management Strategies with Emphasis on Postoperative Pain Outcomes Stephen MOCK, William S. REYNOLDS,
LUTS (2014) 6, 69 75 REVIEW ARTICLE Trans-Vaginal Mesh Revision: A Comprehensive Review on Etiologies and Management Strategies with Emphasis on Postoperative Pain Outcomes Stephen MOCK, William S. REYNOLDS,
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
The Lower Limb. Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa
 The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
Patient Information Leaflet
 Patient Information Leaflet MID-URETHRAL SLING OPERATION TENSION-FREE VAGINAL TAPE (TVT) TRANSOBTURATOR TAPE (TOT, TVT-O) This information leaflet has been developed to help your understanding of what
Patient Information Leaflet MID-URETHRAL SLING OPERATION TENSION-FREE VAGINAL TAPE (TVT) TRANSOBTURATOR TAPE (TOT, TVT-O) This information leaflet has been developed to help your understanding of what
Basic Body Structure
 Basic Body Structure The Cell All life consists of microscopic living structures called cells. They perform various functions throughout the body. All cells are similar in structure, but not identical.
Basic Body Structure The Cell All life consists of microscopic living structures called cells. They perform various functions throughout the body. All cells are similar in structure, but not identical.
Muscles of Gluteal Region
 1 The Gluteal Region In the gluteal region the skin is tough with many layers underneath. Directly under it is the superficial fascia followed by the deep fascia then the muscles and the bones of the thigh.
1 The Gluteal Region In the gluteal region the skin is tough with many layers underneath. Directly under it is the superficial fascia followed by the deep fascia then the muscles and the bones of the thigh.
Slide Read the tables it is about the difference between male & female pelvis.
 I didn t include the slides, this is only what the doctor read or said because he skipped a lot of things because we took it previously, very important to go back to the slides (*there is an edited version)
I didn t include the slides, this is only what the doctor read or said because he skipped a lot of things because we took it previously, very important to go back to the slides (*there is an edited version)
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy
 Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Physical Therapy Treatment for Pelvic Floor Disorders: Interventions and Home Programs
 Physical Therapy Treatment for Pelvic Floor Disorders: Interventions and Home Programs T INA M A LLEN, PT PRPC BCB - PMD U N I V E R S I T Y O F W A S H I N G T O N M E D I C A L C E N T E R H E R M A
Physical Therapy Treatment for Pelvic Floor Disorders: Interventions and Home Programs T INA M A LLEN, PT PRPC BCB - PMD U N I V E R S I T Y O F W A S H I N G T O N M E D I C A L C E N T E R H E R M A
VENOUS DRAINAGE OF THE LOWER LIMB
 Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Pudendal Neuropathy One of the Main Defects in Perineology
 Pudendal Neuropathy One of the Main Defects in Perineology Jacques Beco M.D. Groupement Européen de Périnéologie Liège University, CHU Sart-Tilman, B-4 Liege, Belgium CHC Clinique Saint Elisabeth, B-48
Pudendal Neuropathy One of the Main Defects in Perineology Jacques Beco M.D. Groupement Européen de Périnéologie Liège University, CHU Sart-Tilman, B-4 Liege, Belgium CHC Clinique Saint Elisabeth, B-48
Lectures of Human Anatomy
 Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Stress Incontinence. Susannah Elvy Urogynaecology CNS
 Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
CHRONIC PELVIC PAIN AS WE UNDERSTAND IT TODAY. Dr. Sonia Wartan Consultant in Pain Medicine
 CHRONIC PELVIC PAIN AS WE UNDERSTAND IT TODAY Dr. Sonia Wartan Consultant in Pain Medicine Clinical Lead of Chronic Pain Services Chronic Pelvic MDT Clinic Royal Gwent Hospital Acute Pain Specific disease/injury
CHRONIC PELVIC PAIN AS WE UNDERSTAND IT TODAY Dr. Sonia Wartan Consultant in Pain Medicine Clinical Lead of Chronic Pain Services Chronic Pelvic MDT Clinic Royal Gwent Hospital Acute Pain Specific disease/injury
Mohammad Ashraf. Abdulrahman Al-Hanbali. Ahmad Salman. 1 P a g e
 - 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
- 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial