How to treat non-clonal polyglobulia: to bleed or not to bleed. Claire Harrison Guy s and St Thomas Hospitals London, UK
|
|
|
- Linette Nicholson
- 5 years ago
- Views:
Transcription



1 How to treat non-clonal polyglobulia: to bleed or not to bleed Claire Harrison Guy s and St Thomas Hospitals London, UK
2 Disclosures Institutional research support: Novartis and Shire Pharmaceuticals Speaker: Novartis, Sanofi Avensis, Shire, CTI, Prime oncology, Medscape Consultancy work: Novartis, Sbio, YMBioscience, Cellgene, Sanofi Avensis, Gilead, CTI, NICE
3 Learning outcomes To be able to classify erythrocytosis To understand the investigation of a suspected erythrocytosis To consider possible management options for a patient with an erythrocytosis.. To venesect or not
4 Who should be investigated? A persistently raised venous haematocrit (>0.52 males, >0.48 in females for >2 months) should be investigated. A Hct above 0.60 in males and 0.56 in females can be assumed to have absolute erythrocytosis. Caution Patients with iron deficient red cell indices BCSH guidelines 2007 McMullin etal
5 RCM shows better correlation with HCT Johansson Pl et al. Br. J. Haem. 2005; 129, 701-5
6 Haemoglobin and red cell mass (males) shows less good correlation Johansson Pl et al. Br. J. Haem. 2005; 129, 701-5
7 Diagnostic criteria for Polycythemia Vera WHO 2016 Major HCT >.49 (men),.48 (women) or other evidence of increased red cell mass JAK2 mutation Bone marrow biopsy showing panmyelosis Minor Serum Epo below the normal reference range all major or Two major and one minor establishes PV
8 Erythrocytosis Apparent: Raised haematocrit Red cell mass normal Relative: Raised haematocrit Red cell mass normal and Reduced plasma volume Absolute: Red cell mass >125% of predicted value
9 Erythrocytosis Apparent: Raised haematocrit Red cell mass normal Relative: Raised haematocrit Red cell mass normal and Reduced plasma volume Absolute: Red cell mass >125% of predicted value
10 Primary erythrocytosis Congenital Acquired Polycythemia vera LNK mutations (congenital and acquired) Secondary erythrocytosis Congenital Acquired Central hypoxic process Local hypoxia Pathologic EPO production Exogenous EPO Idiopathic erythrocytosis
11 Congenital erythrocytosis: Primary EPO receptor mutations Secondary Oxygen sensing pathway mutations VHL gene mutations PHD2 mutations HIF -2a mutations Bisphosphoglycerate mutase deficiency High oxygen-affinity haemoglobin Methaemoglobinaemia Hereditary ATP increase And many others now being

12 Diagnostic pathway Persistence History and examination EPO level +/- JAK2 mutation test CarboxyHaemoglobin

13 Diagnostic pathway History and examination Symptoms of hyperviscosity Predisposing factors Drugs including recreational Lifestyle Family history: Vascular disease & Erythrocytosis
14 Investigations Repeat confirmatory FBC Erythropoietin level, Carboxyhaemoglobin, JAK2 mutations Bone marrow biopsy Imaging Overnight oximetry Red Cell Mass P 50 - Oxygen dissociation curve Haemoglobin electrophoresis Sequencing of known gene mutations NGS.. Can replace p50, electrophoresis and sequencing
15 Erythrocytosis Measurement of EPO levels Primary if low/normal (10%) Secondary if normal/high Defect intrinsic to erythroid cell Erythropoietin driven
16 Investigations Repeat confirmatory FBC Erythropoietin level, Carboxyhaemoglobin, JAK2 mutations Bone marrow biopsy Imaging Overnight oximetry Red Cell Mass P 50 - Oxygen dissociation curve Haemoglobin electrophoresis Sequencing of known gene mutations As directed by history, examination and clinical findings NGS.. Can replace P 50, electrophoresis and gene sequencing

17


18 Acquired secondary erythrocytosis
19 Acquired: EPO mediated: Hypoxia driven Central hypoxic process Chronic lung disease Right-to-left cardiopulmonary vascular shunts Carbon monoxide poisoning Smoker's erythrocytosis Hypoventilation syndromes including sleep apnoea High-altitude habitat Local renal hypoxia Renal artery stenosis End stage renal disease Hydronephrosis Renal cysts (polycystic kidney disease) Post- renal transplant erythrocytosis
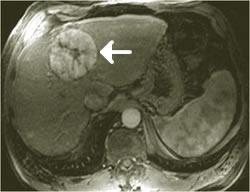
20 Acquired: Excess EPO Pathologic EPO production Cerebellar haemangioblastoma Meningioma Parathyroid carcinoma/adenomas Hepatocellular carcinoma Renal cell cancer Pheochromocytoma Uterine leiomyomas
21 Management of secondary erythrocytosis: Venesection is NOT the mainstay
22 Vascular occlusive episodes per patient - 10 years Considering PV there is clear evidence of HCT control being important >0.60 P.C.V. range Relation of PCV range to number of vascular occlusive episodes per 10 patient-years In patients with primary proliferative polycythaemia.
23 MORBIDITY STUDY 300 HIGH Hb. 15 gm % MEN gm % WOMEN 200 NOT HIGH Hb. < 15 gm % MEN < 14 gm % WOMEN But if you lower the HCT does it lower the risk? 39 0 TOTAL NON-HYPERTENSIVE (<160/95) HYPERTENSIVE (>160/95) Risk of cerebral infarction (16 year follow up) according to antecedent hemoglobin and blood pressure status. Men and women at entry: Framingham Study. KANNEL, et al, Stroke, 1972, 3,
24

25 What about primary prevention with aspirin?
26 Management of acquired secondary erythrocyosis Address the underlying cause where possible Many require non-haematological input eg sleep apnoea Standard lifestyle measures apply Only venesect if there is a very clear indication Eg very high HCT > 0.54 and symptoms or risk eg pre op NB this does NOT apply to cyanotic heart disease Aspirin only if otherwise indicated
27 Recent case from our clinical practice 34 year old man presents with episode of black out Shortly after arrival had an epileptic seizure, full recovery No relevant history, non-smoker, increasing headaches. FBC Hb 240g/L HCT 0.64 Wbc 8 x 10 9 Platelets 341 x 10 9 Advice? Persistently abnormal
28 Recent case from our clinical practice 34 year old man presents with episode of black out Shortly after arrival had an epileptic seizure, full recovery No relevant history, non-smoker, increasing headaches. FBC Hb 240g/L HCT 0.64 Wbc 8 x 10 9 Platelets 341 x 10 9 Check EPO/JAK2 etc Get urgent imaging Hydrate and perform isovolaemic venesection


29 Continue venesections target <0.5 for surgery Brain imaging Cerebellar abnormality EPO 10IU/L JAK2 mutations negative
30 Primary erythrocytosis Congenital Acquired Polycythemia vera LNK mutations (congenital and acquired) Secondary erythrocytosis Congenital Acquired Central hypoxic process Local hypoxia Pathologic EPO production Exogenous EPO Idiopathic erythrocytosis
31 Investigation of an erythrocytosis with a low EPO level EPO receptor mutations JAK2 mutations LNK mutations reported some congenital and some acquired
32 Erythropoietin Receptor EPO Signal Transduction EPO Down modulation EPO Truncated EPO R EPO Receptor Receptor Receptor JAK2 JAK2 SHP-1 JAK2 STAT5 SHP-1 SHP-1 active STAT5 dimers McMullin 2009
33 EPO receptor truncation mutation T C T T G C G T C C A T G G A C A C T G T G De novo G to A at base 6002 Stop codon at aa 439 T C T T G C G T C C A T N G A C A C T G T G Individual Hb PCV WBC Platelets EPO Level (g/dl) (x10 9 /L) x10 9 /L) (miu/ml) Teenage boy (NR ) McMullin 2009
34 Management of patients with EPO R truncation.? Lack of evidence base Consider venesection if patients are symptomatic and HCT > 0.55 Careful management of anaesthesia etc The teenage boy is now 38 years old has 2 x / year venesections

35 JAK2 Kinase -JH1 and JH2 Domains JH1 active state Interface 1 Interface 2 V617 JH2 inactive state
36 JAK2 mutation in Polycythaemia Vera Chromosome 9 exon 12 G T transversion at nucleotide 1849 Resulting V617F mutation V617F FERM SH2 JH2 Kinase Regulation of cell cycle

37 JAK2 Exon 12 mutations Scott et al 2007
 or other evidence of increased red cell mass JAK2 mutation Bone marrow biopsy showing panmyelosis Minor Serum Epo below the normal reference range Very rare JAK2 mutation negative PV cases")
38 Diagnostic criteria for Polycythemia Vera WHO 2016 Major HCT >.49 (men),.48 (women) or other evidence of increased red cell mass JAK2 mutation Bone marrow biopsy showing panmyelosis Minor Serum Epo below the normal reference range Very rare JAK2 mutation negative PV cases do exist a bone marrow biopsy if useful to detect them. Very low level JAK2 mutations may also be considered all major or Two major and one minor establishes PV
39 Primary erythrocytosis Congenital Acquired Polycythemia vera LNK mutations (congenital and acquired) Secondary erythrocytosis Congenital Acquired Central hypoxic process Local hypoxia Pathologic EPO production Exogenous EPO Idiopathic erythrocytosis
40 Investigations Repeat confirmatory FBC Erythropoietin level, Carboxyhaemoglobin, JAK2 mutations Bone marrow biopsy Imaging Overnight oximetry Red Cell Mass P 50 - Oxygen dissociation curve Haemoglobin electrophoresis Sequencing of known gene mutations As directed by history, examination and clinical findings NGS.. Can replace P 50, electrophoresis and gene sequencing
41 Investigations Repeat confirmatory FBC Erythropoietin level, Carboxyhaemoglobin, JAK2 mutations Bone marrow biopsy Imaging Overnight oximetry Red Cell Mass P 50 - Oxygen dissociation curve Haemoglobin electrophoresis Sequencing of known gene mutations As directed by history, examination and clinical findings NGS.. Can replace P 50, electrophoresis and gene sequencing
-")
42 NGS based technologies can be very helpful Roche (NimbleGen SeqCap)- SEQCAP
43 Examples of genes on the erythrocytosis NGS Candidate Gene Position No of exons VHL Chr3: EPAS1 Chr2: EGLN1 Chr1: EPOR Chr19: BPGM Chr7: HBB Chr11: SH2B3 Chr12: JAK2 Chr9: EGLN2 Ch19: HBA1 Ch16: HBA2 Ch16:
44 Management of idiopathic erythrocytosis (ie everything is negative) Venesection to HCT target of 0.54 If previous thrombosis or increased risk of thrombosis then consider a target of 0.45 Cytoreductive therapy is contraindicated
45 High Affinity Hemoglobins.. examples UPN Hb Olympia Olympia Pierre Benite Heathrow Santa Clara Age at presentation (yrs) Hemoglobin (g/dl) Hct WBC (x 10 9 /l) Pts (x10 9 /l) EPO (miu/ml) N/A N/A
46 Recommendations: management of high (oxygen) affinity haemoglobins Possible indications for Venesection include: Presence of symptoms such as dizziness, dyspnoea or angina, for which a raised Hct is considered to be a contributory factor. One or more previous thrombotic episodes. Asymptomatic individuals in whom a family member with a high oxygen affinity haemoglobin, similar haemoglobin concentration, and comparable risk factors for thrombosis has developed a thrombotic problem. McMullin 2007 BCSH recommendations
47 High oxygen affinity haemoglobins Consideration venesection should be given for individuals with a Hct >0.60 requiring major surgery Do not attempt to reduce the Hct to within the normal range. Venesection to maintain the Hct <0.60 has been recommended. When thrombosis or symptoms compatible with hyperviscosity develop at a lower Hct, a target Hct of 0.52 has been suggested. McMullin 2007 BCSH recommendations



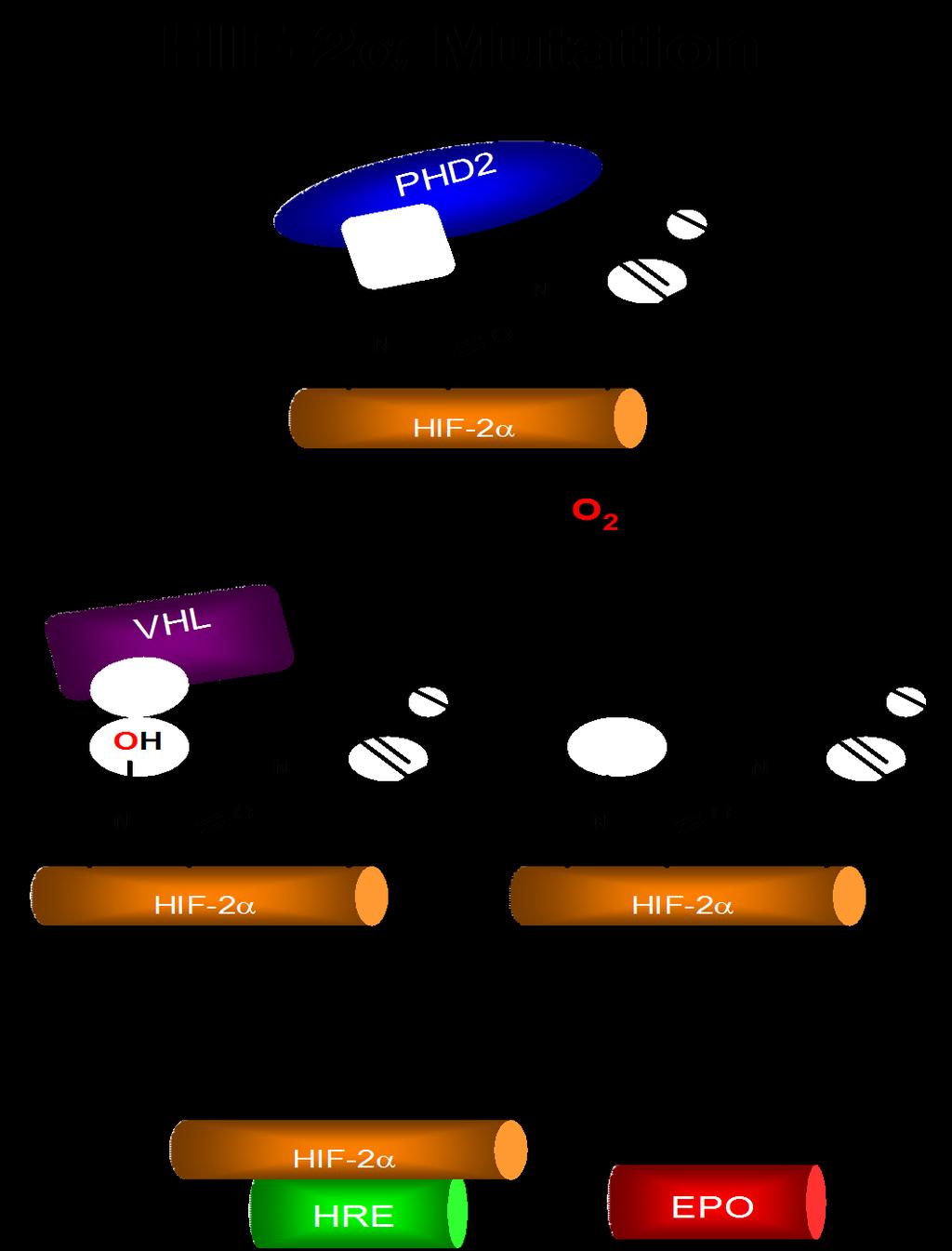
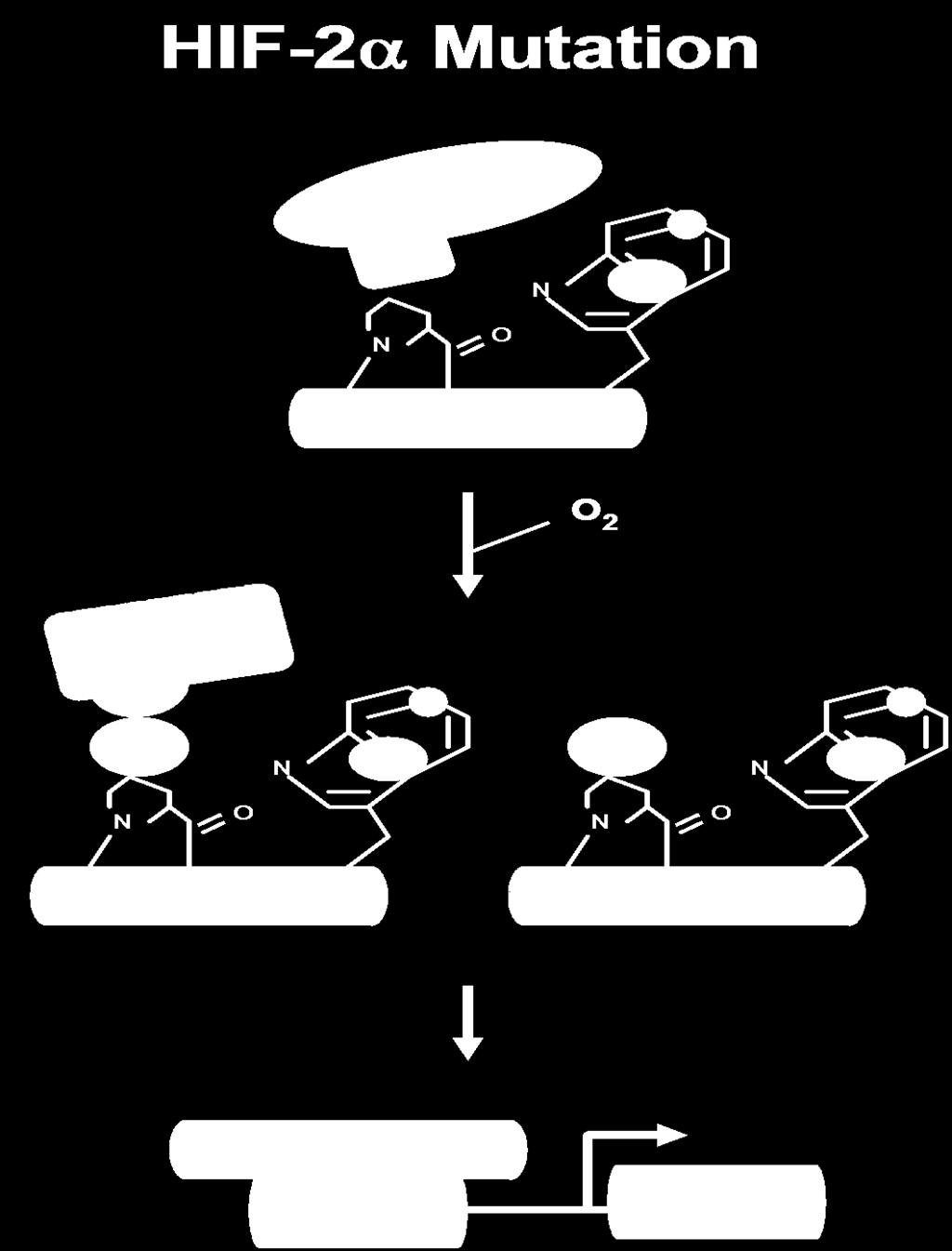
48 NORMOXIA HYPOXIA PHD2 PHD2 HIF-2a HIF-b O 2 O 2 O 2 OH HIF-2a VHL HIF-2a HIF-b EPO VEGF Transferrin etc Red Cells Degradation

49 Chuvash Pakistan Bangladesh McMullin 2009
50 VHL Mutational screen Normal >100 patients A A A G A C C T G G A G C G G C T G A C A C A G G Homozygous C598T/Arg200Trp 9 Asian families A A A G A C C T G G A G T G G C T G A C A C A G G Data suggests single founder individual McMullin 2009

51 McMullin 2009
52 Patient case: 23 year old originally from Bangladesh referred to clinic Had hypoplastic left heart, and transposition of great vessels corrected as baby, multiple operations. Good function, no exercise limitation, no hypoxia 15 months earlier suffered thrombotic CVA at that time (Hb 24 HCT 0.62)
53 Patient case 23 year old originally from Bangladesh referred to clinic Had hypoplastic left heart, and transposition of great vessels corrected as baby, multiple operations. Good function, no exercise limitation, no hypoxia 15 months earlier suffered 2 x thrombotic CVA at that time (Hb 24 HCT 0.62) EPO 15 IU/L Father attends with him and mentions that he was seen at St Thomas Hospital 18 years before and had lots of tests for Too much blood Used to have venesections, well in himself. Hb 18.8 mcv 56 HCT 0.54, EPO 20
54 Diagnosis? Father and son had a known mutation affected HIF 2A (EPAS 1 gene) Management? Father needs venesection target < 0.5 Son < 0.45 and aspirin Screen family members
55 Clinical events in erythrocytoses Homozygotes with Chuvash polycythaemia: increased mortality from cerebrovascular events and mesenteric thrombosis PHD2 and HIF2A mutations associated with thromboembolic events
56 Kaplan-Meier survival curves for Chuvash polycythemia patients and spouses or community members matched for age, sex and place of birth Gordeuk, V. R. et al. Blood 2004;103:

57 Baseline characteristics of adult Chuvash polycythemia (CP) patients and controls at time of enrollment in the case-control study. Adelina Sergueeva et al. Haematologica 2017;102:e166-e169
 over median of 8.8 years. The rate of new thrombosis was higher in CP subjects (HR 12.")
58 Multivariate Cox Proportional Hazards Model of predictors of new thrombosis during follow up in 128 CP patients. Prospective evaluation of 128 CP subjects & controls (matched by age, sex, residence) over median of 8.8 years. The rate of new thrombosis was higher in CP subjects (HR 12.7). Adelina Sergueeva et al. Haematologica 2017;102:e166-e169
59 Thrombosis and THBS1 expression in Chuvash polycythemia Adelina Sergueeva et al. Haematologica 2017;102:e166-e169
60 Chuvash polycythemia patients have different cardiovascular responses to hypoxia. Smyth,PLOS, 2005,3,e290
61 Chuvash polycythemia patients have different cardiovascular responses to hypoxia. This was also seen in PHD2 mutation proband and mimics by iron deficiency and chronic hypoxia Smyth,PLOS, 2005,3,e290

62 Chuvash polycythemia patients have different cardiovascular responses to hypoxia Implications for therapy and monitoring for complications Smyth,PLOS, 2005,3,e290

63 Paraganglioma have been reported in patients with HIF 2 a mutations Hidemi Toyoda et al. Pediatrics 2014;133:e1787-e1791

64 Management options: Congenital erythrocytosis Rare individuals may have a congenital erythrocytosis which often present at a young age and have a family history An investigation for known molecular defects should be carried out Venesection and low dose aspirin are possible management options Ruxolitinib may have efficacy in managing Chuvash polycythaemia


65 Lifestyle modification: Just as important for congenital erythrocytosis
66 Erythrocytosis & symptoms response: Ruxolitinib in Chuvash Polycythaemia Zhou et al NEJM 2016 Patient Characteristics at Baseline and Clinical Response to Ruxolitinib in Three Patients with Chuvash Polycythemia Panel A shows laboratory values, phlebotomy requirement, and symptoms for all three patients before treatment and during ruxolitinib therapy. ND denotes not determined. Panel B shows the effects of ruxolitinib on platelet-count oscillations in Patient CP-01 and the effects of ruxolitinib on hematocrit levels and phlebotomy requirements in Patients CP-02 and CP-03.
67 Management of a congenital erythrocytosis Assess individual patient Consider reduction of HCT to achievable target level? <0.5 Consider aspirin if no specific contraindication Need for long-term follow-up of treatments and outcomes? Need for global registry
68 Summary: Erythrocytosis is classified by cause measurement of EPO levels are useful way to subclassify Red cell mass is a useful test and HCT is more predictive than Hb Most cases of secondary acquired erythrocytosis are best managed by addressing the underlying cause and venesection is NOT a mainstay of therapy Congenital erythrocytosis is rare but important venesection needs to be carefully considered and long term monitoring for other late complications is important A registry for these conditions would inform future management
Department of Clinical Haematology
 Diagnosis in Primary Care and referral pathway for patients with a raised haematocrit Why implement this pathway? A raised haemoglobin or haematocrit is a common finding and can be a reason for referral.
Diagnosis in Primary Care and referral pathway for patients with a raised haematocrit Why implement this pathway? A raised haemoglobin or haematocrit is a common finding and can be a reason for referral.
CONGENITAL ERYTHROCYTOSIS. Mary Frances McMullin
 CONGENITAL ERYTHROCYTOSIS Mary Frances McMullin m.mcmullin@qub.ac.uk Disclosures No relevant disclosures Learning outcomes Describe the mechanism of red cell production following signalling from the erythropoietin
CONGENITAL ERYTHROCYTOSIS Mary Frances McMullin m.mcmullin@qub.ac.uk Disclosures No relevant disclosures Learning outcomes Describe the mechanism of red cell production following signalling from the erythropoietin
DIAGNOSIS IN PRIMARY CARE AND REFERRAL PATHWAY FOR PATIENTS WITH A RAISED HAEMATOCRIT
 DIAGNOSIS IN PRIMARY CARE AND REFERRAL PATHWAY FOR PATIENTS WITH A RAISED HAEMATOCRIT Document purpose A raised haemoglobin or haematocrit is a common finding and can be a reason for referral. This document
DIAGNOSIS IN PRIMARY CARE AND REFERRAL PATHWAY FOR PATIENTS WITH A RAISED HAEMATOCRIT Document purpose A raised haemoglobin or haematocrit is a common finding and can be a reason for referral. This document
The average adult produces red cells every
 MYELOPROLIFERATIVE DISORDERS Idiopathic erythrocytosis: a disappearing entity Mary Frances McMullin 1 1 Centre for Cancer Research and Cell Biology, Queen s University, Belfast, N. Ireland. Erythrocytosis
MYELOPROLIFERATIVE DISORDERS Idiopathic erythrocytosis: a disappearing entity Mary Frances McMullin 1 1 Centre for Cancer Research and Cell Biology, Queen s University, Belfast, N. Ireland. Erythrocytosis
Chronic Myeloproliferative Disorders
 1 Chronic Myeloproliferative Disorders 15th 9 April2015 Polycythemia vera Essential thrombocythemia Idiopathic primary myelofibrosis 2 Learning objectives To appreciate types of polycythaemia (erythrocytosis)
1 Chronic Myeloproliferative Disorders 15th 9 April2015 Polycythemia vera Essential thrombocythemia Idiopathic primary myelofibrosis 2 Learning objectives To appreciate types of polycythaemia (erythrocytosis)
Emerging diagnostic and risk stratification criteria
 PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
Characterization of blood donors with high haemoglobin concentration
 STATE OF THE ART 2A-S05-02 ISBT Science Series (2013) 8, 114 118 ISBT Science Series 2013 International Society of Blood Transfusion Characterization of blood donors with high haemoglobin concentration
STATE OF THE ART 2A-S05-02 ISBT Science Series (2013) 8, 114 118 ISBT Science Series 2013 International Society of Blood Transfusion Characterization of blood donors with high haemoglobin concentration
رناد زكريا Dr. ahmad Dr. ahmad. P a g e 1
 5 رناد زكريا Dr. ahmad Dr. ahmad P a g e 1 Before we start. -This sheet was written according to section 2 s record and reviewed according to section 1 s record by Ruba Hussien with all thanks and I referred
5 رناد زكريا Dr. ahmad Dr. ahmad P a g e 1 Before we start. -This sheet was written according to section 2 s record and reviewed according to section 1 s record by Ruba Hussien with all thanks and I referred
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease
 The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
CLINICAL CASE PRESENTATION
 European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
Is the recommended hematocrit target in polycythemia vera evidence based? Tiziano BARBUI, MD Ospedali Riuniti, Bergamo, Italy
 Is the recommended hematocrit target in polycythemia vera evidence based? Tiziano BARBUI, MD Ospedali Riuniti, Bergamo, Italy We have generated a transgenic mouse line that reaches a hematocrit concentration
Is the recommended hematocrit target in polycythemia vera evidence based? Tiziano BARBUI, MD Ospedali Riuniti, Bergamo, Italy We have generated a transgenic mouse line that reaches a hematocrit concentration
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital
 By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
COEXISTENCE OF β-thalassemia AND POLYCYTHEMIA VERA: A CHICKEN-AND-EGG DEBATE?
 COEXISTENCE OF β-thalassemia AND POLYCYTHEMIA VERA: A CHICKEN-AND-EGG DEBATE? M. DE SLOOVERE (1), L. HARLET (2), S. VAN STEENWEGHEN (3), E. MOREAU (1), D. DE SMET (1) (1) DEPARTMENT OF LABORATORY MEDICINE,
COEXISTENCE OF β-thalassemia AND POLYCYTHEMIA VERA: A CHICKEN-AND-EGG DEBATE? M. DE SLOOVERE (1), L. HARLET (2), S. VAN STEENWEGHEN (3), E. MOREAU (1), D. DE SMET (1) (1) DEPARTMENT OF LABORATORY MEDICINE,
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Latest updates in Myeloproliferative Neoplasms. Elizabeth Hexner, MD, MSTR
 Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes A critical reappraisal of anagrelide in the management of ET
 European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
HFE mutations in idiopathic erythrocytosis
 HFE mutations in idiopathic erythrocytosis Biagetti, G., Catherwood, M., Robson, N., Bertozzi, I., Cosi, E., McMullin, M. F., & Randi, M. L. (2017). HFE mutations in idiopathic erythrocytosis. British
HFE mutations in idiopathic erythrocytosis Biagetti, G., Catherwood, M., Robson, N., Bertozzi, I., Cosi, E., McMullin, M. F., & Randi, M. L. (2017). HFE mutations in idiopathic erythrocytosis. British
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Erythrocytosis due to presumed polycythemia vera
 A SELF-TEST ON A CLINICAL CASE The patient is presumed to have polycythemia vera but does she? IM BOARD REVIEW EDUCATIONAL OBJECTIVE: Readers will pursue a step-by-step approach to evaluating patients
A SELF-TEST ON A CLINICAL CASE The patient is presumed to have polycythemia vera but does she? IM BOARD REVIEW EDUCATIONAL OBJECTIVE: Readers will pursue a step-by-step approach to evaluating patients
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
HEFT Pathology Guideline. GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia
 HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination
 Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012
 Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012 Outline Case presentation Overview of PV Disease course Mechanisms of thrombosis Case Presentation
Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012 Outline Case presentation Overview of PV Disease course Mechanisms of thrombosis Case Presentation
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
WHAT IS YOUR DIAGNOSIS?
 WHAT IS YOUR DIAGNOSIS? A 12 year old, female neutered domestic shorthaired cat was presented to the R(D)SVS Feline Clinic with a 6 week history of polydipsia and polyuria, which was not quantified. The
WHAT IS YOUR DIAGNOSIS? A 12 year old, female neutered domestic shorthaired cat was presented to the R(D)SVS Feline Clinic with a 6 week history of polydipsia and polyuria, which was not quantified. The
Prognostic models in PV and ET
 Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
research paper Summary
 research paper An elevated venous haemoglobin concentration cannot be used as a surrogate marker for absolute erythrocytosis: a study of patients with polycythaemia vera and apparent polycythaemia Peter
research paper An elevated venous haemoglobin concentration cannot be used as a surrogate marker for absolute erythrocytosis: a study of patients with polycythaemia vera and apparent polycythaemia Peter
Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES)
") Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES) Author: Dr N Butt, Consultant Haematologist On behalf of the Haematology CNG Written: July 2010 Reviewed:
Guidelines for diagnosis and management of adult myeloproliferative neoplasms (PV, ET, PMF and HES) Author: Dr N Butt, Consultant Haematologist On behalf of the Haematology CNG Written: July 2010 Reviewed:
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update
 Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
JAK2 Inhibitors for Myeloproliferative Diseases
 JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
Now what do you have to learn?
 So you have this thing Now what do you have to learn? Susan J. Leclair, Ph.D, CLS(NCA) Chancellor Professor Department of Medical Laboratory Science University of Massachusetts Dartmouth Massachusetts
So you have this thing Now what do you have to learn? Susan J. Leclair, Ph.D, CLS(NCA) Chancellor Professor Department of Medical Laboratory Science University of Massachusetts Dartmouth Massachusetts
Medical Management of Adult Congenital Heart Disease
 Medical Management of Adult Congenital Heart Disease 1. Erythrocytosis 2. Pulmonary Hemorrhage 3. The Thrombosis Dilemma 4. Non-Cardiac Surgery: a) The anesthesiologist b) Bilirubin kinetics c) Post operative
Medical Management of Adult Congenital Heart Disease 1. Erythrocytosis 2. Pulmonary Hemorrhage 3. The Thrombosis Dilemma 4. Non-Cardiac Surgery: a) The anesthesiologist b) Bilirubin kinetics c) Post operative
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Myeloproliferative Neoplasms and Treatment Overview
 Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Cooperation of germ line JAK2 mutations E846D and R1063H leads to erythroid hyperplasia with megakaryocytic atypia
 Cooperation of germ line JAK2 mutations E846D and R1063H leads to erythroid hyperplasia with megakaryocytic atypia Katarina Kapralova, Ph.D. Department of Biology Faculty of Medicine and Dentistry Palacký
Cooperation of germ line JAK2 mutations E846D and R1063H leads to erythroid hyperplasia with megakaryocytic atypia Katarina Kapralova, Ph.D. Department of Biology Faculty of Medicine and Dentistry Palacký
How to monitor MPN patients
 How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
Polycythemia Vera: Aligning Real-World Practices With Current Best Practices
 Polycythemia Vera: Aligning Real-World Practices With Current Best Practices Overview Ruben A. Mesa, MD, provides practical insights into treating polycythemia vera. In addition to discussing risk stratification,
Polycythemia Vera: Aligning Real-World Practices With Current Best Practices Overview Ruben A. Mesa, MD, provides practical insights into treating polycythemia vera. In addition to discussing risk stratification,
GP Referral Guidelines. for. South Wales Cancer Network. Document Control Sheet. Specialty/Project Haematological Site Specific Group
 GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
Increased Number of Red Blood Cells (Polycythemia) Basics
 Basics") Increased Number of Red Blood Cells (Polycythemia) Basics OVERVIEW Blood consists of red blood cells (the most numerous cells normally), white blood cells, platelets, and plasma (the liquid portion of
Increased Number of Red Blood Cells (Polycythemia) Basics OVERVIEW Blood consists of red blood cells (the most numerous cells normally), white blood cells, platelets, and plasma (the liquid portion of
Sickle cell disease. Fareed Omar 10 March 2018
 Sickle cell disease Fareed Omar 10 March 2018 Physiology Haemoglobin structure HbA2: 2α and 2δ chains (2-3%) HbF: 2α and 2γ chains (
Sickle cell disease Fareed Omar 10 March 2018 Physiology Haemoglobin structure HbA2: 2α and 2δ chains (2-3%) HbF: 2α and 2γ chains (
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE
 THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms
 Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Chapter 22: Hematological Complications
 Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Erythropoietin and soluble Transferrin Receptor concentrations in high altitude residents with excessive erythrocytosis
 1 Erythropoietin and soluble Transferrin Receptor concentrations in high altitude residents with excessive erythrocytosis Guido Valverde 1 Rainer Kowoll 2, Karl A. Kirsch 2, Hanns-Christian Gunga 2 1 Universidad
1 Erythropoietin and soluble Transferrin Receptor concentrations in high altitude residents with excessive erythrocytosis Guido Valverde 1 Rainer Kowoll 2, Karl A. Kirsch 2, Hanns-Christian Gunga 2 1 Universidad
Haematology dilemma s to refer or not to refer?
 Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Retrospective Study of High Hemoglobin Levels in 56 Young Adults
 Original Article J Hematol. 2018;7(2):43-50 Retrospective Study of High Hemoglobin Levels in 56 Young Adults Alexandra Desnoyers a, Michel Pavic a, Paul-Michel Houle a, b, Jean-Francois Castilloux a, Patrice
Original Article J Hematol. 2018;7(2):43-50 Retrospective Study of High Hemoglobin Levels in 56 Young Adults Alexandra Desnoyers a, Michel Pavic a, Paul-Michel Houle a, b, Jean-Francois Castilloux a, Patrice
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016
 for Polycythemia Vera March 3, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
Polycythemia Vera and Essential Thombocythemia A Single Institution Experience
 INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Dr Marina Karakantza Consultant Haematologist, NHSBT
 Dr Marina Karakantza Consultant Haematologist, NHSBT Overview Definition of transfusion thresholds Mechanisms of adaptation to anaemia How RBC transfusion affect adaptation mechanisms to anaemia Triggers
Dr Marina Karakantza Consultant Haematologist, NHSBT Overview Definition of transfusion thresholds Mechanisms of adaptation to anaemia How RBC transfusion affect adaptation mechanisms to anaemia Triggers
EUROPEAN RCT IN MPDs
 EUROPEAN RCT IN MPDs A. Multicenter, Multinational -EORTC -ECLAP -ANHIDRET B. Multicenter, National -French PV RCTs -Italian ET RCT - PT- RCTs C. European Leukemia NET studies D. Future: JAK-2 inhibitor
EUROPEAN RCT IN MPDs A. Multicenter, Multinational -EORTC -ECLAP -ANHIDRET B. Multicenter, National -French PV RCTs -Italian ET RCT - PT- RCTs C. European Leukemia NET studies D. Future: JAK-2 inhibitor
The Irony of Anemia How to interpret the CBC
 Jaideep Shenoi MD Hematology Oncology Northwest Medical Specialities Tacoma, WA The Irony of Anemia How to interpret the CBC March 10 th, 2018 Disclosures: Advisory Board for Pharmacyclics, Janssen, Takeda,
Jaideep Shenoi MD Hematology Oncology Northwest Medical Specialities Tacoma, WA The Irony of Anemia How to interpret the CBC March 10 th, 2018 Disclosures: Advisory Board for Pharmacyclics, Janssen, Takeda,
Chi sono i candidati agli inibitori di JAK2
 Chi sono i candidati agli inibitori di JAK2 Francesco Passamon, Hematology, University Hospital Varese, Italy Ruxoli8nib (US approved in MF; EAP study and compassionate use in Italy) SAR302503 (phase 3
Chi sono i candidati agli inibitori di JAK2 Francesco Passamon, Hematology, University Hospital Varese, Italy Ruxoli8nib (US approved in MF; EAP study and compassionate use in Italy) SAR302503 (phase 3
Mechanisms of Gene Regulation and Signal! Transduction in Hypoxia!
 Mechanisms of Gene Regulation and Signal! Transduction in Hypoxia! Lorenz Poellinger! Dept. of Cell and Molecular Biology! Karolinska Institutet, Stockholm, Sweden! Normoxia - O 2 availability is in balance
Mechanisms of Gene Regulation and Signal! Transduction in Hypoxia! Lorenz Poellinger! Dept. of Cell and Molecular Biology! Karolinska Institutet, Stockholm, Sweden! Normoxia - O 2 availability is in balance
Managing ET in Tiziano Barbui MD
 Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
The frequency of JAK2 exon 12 mutations in idiopathic erythrocytosis patients with low serum erythropoietin levels
 The frequency of JAK2 exon 12 mutations in idiopathic erythrocytosis patients with low serum erythropoietin levels Melanie J. Percy, Linda M. Scott, Wendy N. Erber, Claire N. Harrison, John T. Reilly,
The frequency of JAK2 exon 12 mutations in idiopathic erythrocytosis patients with low serum erythropoietin levels Melanie J. Percy, Linda M. Scott, Wendy N. Erber, Claire N. Harrison, John T. Reilly,
Around million aged erythrocytes/hour are broken down.
 Anemia Degradation ofheme Around 100 200 million aged erythrocytes/hour are broken down. The degradation process starts in reticuloendothelial cells in the spleen, liver, and bone marrow. [1] The tetrapyrrole
Anemia Degradation ofheme Around 100 200 million aged erythrocytes/hour are broken down. The degradation process starts in reticuloendothelial cells in the spleen, liver, and bone marrow. [1] The tetrapyrrole
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms
 Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1
Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1
Which Cyanotic Patient Needs Anticoagulation?
 Which Cyanotic Patient Needs Anticoagulation? Erwin Oechslin, MD, FRCPC, FESC Director, Adult Congenital Heart Disease Program The Bitove Family Professor of ACHD Professor of Medicine, U of T Peter Munk
Which Cyanotic Patient Needs Anticoagulation? Erwin Oechslin, MD, FRCPC, FESC Director, Adult Congenital Heart Disease Program The Bitove Family Professor of ACHD Professor of Medicine, U of T Peter Munk
Swami Murugappan MD PhD Hematology Oncology Fellow University of Washington April 27, 2012
 Swami Murugappan MD PhD Hematology Oncology Fellow University of Washington April 27, 2012 Outline Clinical indications of recombinant Erythrop0ietin (EPO) Concerns about the use of EPO in chronic kidney
Swami Murugappan MD PhD Hematology Oncology Fellow University of Washington April 27, 2012 Outline Clinical indications of recombinant Erythrop0ietin (EPO) Concerns about the use of EPO in chronic kidney
No Disclosures 03/20/2019. Learning Objectives. Renal Anemia: The Basics
 Renal Anemia: The Basics Meredith Atkinson, M.D., M.H.S. Associate Professor of Pediatrics Johns Hopkins School of Medicine 16 March 2019 No Disclosures Learning Objectives At the end of this session the
Renal Anemia: The Basics Meredith Atkinson, M.D., M.H.S. Associate Professor of Pediatrics Johns Hopkins School of Medicine 16 March 2019 No Disclosures Learning Objectives At the end of this session the
Venesection Nursing Guidelines
 Venesection Nursing Guidelines Rationale Patients requiring venesection on the Day Treatment Unit (DTU) fall into 3 main categories; patients diagnosed with: Polycythemia Rubra Vera Haemachromatosis Transfusion
Venesection Nursing Guidelines Rationale Patients requiring venesection on the Day Treatment Unit (DTU) fall into 3 main categories; patients diagnosed with: Polycythemia Rubra Vera Haemachromatosis Transfusion
in people with intermediate 2 or high-risk disease, AND if the company provides ruxolitinib with the discount agreed in the patient access scheme.
 RUXOLITINIB INDICATION Licensed / NICE TA386 is recommended as an option f treating disease-related splenomegaly symptoms in adults with primary myelofibrosis (also known as chronic idiopathic myelofibrosis),
RUXOLITINIB INDICATION Licensed / NICE TA386 is recommended as an option f treating disease-related splenomegaly symptoms in adults with primary myelofibrosis (also known as chronic idiopathic myelofibrosis),
Disclosures. Dr. Scirica has also served as a consultant for Lexicon, Arena, Gilead, and Eisai.
 Disclosures Benjamin M. Scirica, MD, MPH, is employed by the TIMI Study Group, which has received research grants from Abbott, AstraZeneca, Amgen, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb,
Disclosures Benjamin M. Scirica, MD, MPH, is employed by the TIMI Study Group, which has received research grants from Abbott, AstraZeneca, Amgen, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb,
Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later
 Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later Vikas Gupta, MD, FRCP, FRCPath Associate Professor Department of Medicine Leukemia/BMT Programs Princess Margaret Cancer
Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later Vikas Gupta, MD, FRCP, FRCPath Associate Professor Department of Medicine Leukemia/BMT Programs Princess Margaret Cancer
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]
![Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]](/thumbs/87/95709298.jpg "Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]") Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations and Management
 Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2
 Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2 Alison Halliday MD Professor of Vascular Surgery University of Oxford Disclosure Statement of Financial
Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2 Alison Halliday MD Professor of Vascular Surgery University of Oxford Disclosure Statement of Financial
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
RESPONSE (NCT )
") Changes in Quality of Life and Disease-Related Symptoms in Patients With Polycythemia Vera Receiving Ruxolitinib or Best Available Therapy: RESPONSE Trial Results Abstract #709 Mesa R, Verstovsek S, Kiladjian
Changes in Quality of Life and Disease-Related Symptoms in Patients With Polycythemia Vera Receiving Ruxolitinib or Best Available Therapy: RESPONSE Trial Results Abstract #709 Mesa R, Verstovsek S, Kiladjian
Module G: Oxygen Transport. Oxygen Transport. Dissolved Oxygen. Combined Oxygen. Topics to Cover
 Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
Supplementary information. Supplementary figure 1. Flow chart of study design
 Supplementary information Supplementary figure 1. Flow chart of study design Supplementary Figure 2. Quantile-quantile plot of stage 1 results QQ plot of the observed -log10 P-values (y axis) versus the
Supplementary information Supplementary figure 1. Flow chart of study design Supplementary Figure 2. Quantile-quantile plot of stage 1 results QQ plot of the observed -log10 P-values (y axis) versus the
Investigation of patients with. polycythaemia. Polycythaemia, defined as an increased packed cell volume (haematocrit), is
, is") Postgrad Med Jt 1996; 72: 519-524 C) Te Fellowship of Postgraduate Medicine, 1996 Clinical guidelines Summary Polycythaemia may complicate or be the presenting feature of a wide variety of different pathologies.
Postgrad Med Jt 1996; 72: 519-524 C) Te Fellowship of Postgraduate Medicine, 1996 Clinical guidelines Summary Polycythaemia may complicate or be the presenting feature of a wide variety of different pathologies.
ANEMIA & HEMODIALYSIS
 ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
NCCP Chemotherapy Protocol. Ponatinib Therapy
 INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase, accelerated phase, or blast phase chronic myeloid leukaemia (CML) who are resistant to dasatinib or nilotinib; who are intolerant
INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase, accelerated phase, or blast phase chronic myeloid leukaemia (CML) who are resistant to dasatinib or nilotinib; who are intolerant
Red Cell Disorders Molecular Basis of Disease. Congenital polycythemias/erythrocytoses
 Red Cell Disorders Molecular Basis of Disease Congenital polycythemias/erythrocytoses Victor R. Gordeuk David W. Stockton Josef T. Prchal Congenital polycythemias may result from inherited defects in hypoxia
Red Cell Disorders Molecular Basis of Disease Congenital polycythemias/erythrocytoses Victor R. Gordeuk David W. Stockton Josef T. Prchal Congenital polycythemias may result from inherited defects in hypoxia
A guideline for the management of specific situations in polycythaemia vera and secondary erythrocytosis
 guideline A guideline for the management of specific situations in polycythaemia vera and secondary erythrocytosis A British Society for Haematology Mary F. F. McMullin, 1 Adam J. Mead, 2 Sahra Ali, 3
guideline A guideline for the management of specific situations in polycythaemia vera and secondary erythrocytosis A British Society for Haematology Mary F. F. McMullin, 1 Adam J. Mead, 2 Sahra Ali, 3
BONE MARROW PERIPHERAL BLOOD Erythrocyte
 None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
PRECISION: A Canadian In-practice Needs Assessment in Management of PV in Canada* Expert Consensus Recommendations
 PRECISION: A Canadian In-practice Needs Assessment in Management of PV in Canada* Expert Consensus Recommendations *This program was made possible through funding from Novartis Pharmaceuticals Canada.
PRECISION: A Canadian In-practice Needs Assessment in Management of PV in Canada* Expert Consensus Recommendations *This program was made possible through funding from Novartis Pharmaceuticals Canada.
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms Judit Demeter CML chronic myeloid leukemia Semmelweis University, I st Department of Internal Medicine PV polycythaemia vera ET essential thrombocythaemia MF myelofibrosis
Myeloproliferative Neoplasms Judit Demeter CML chronic myeloid leukemia Semmelweis University, I st Department of Internal Medicine PV polycythaemia vera ET essential thrombocythaemia MF myelofibrosis
BCH 471. Experiment (5) Hemoglobin Estimation, Erythrocyte Sedimentation Rate (ESR) and Hematocrit (HCT)
 Hemoglobin Estimation, Erythrocyte Sedimentation Rate (ESR) and Hematocrit (HCT)") BCH 471 Experiment (5) Hemoglobin Estimation, Erythrocyte Sedimentation Rate (ESR) and Hematocrit (HCT) Objectives Quantitative determination of hemoglobin in a blood sample. Determination of erythrocyte
BCH 471 Experiment (5) Hemoglobin Estimation, Erythrocyte Sedimentation Rate (ESR) and Hematocrit (HCT) Objectives Quantitative determination of hemoglobin in a blood sample. Determination of erythrocyte
Post-ASH 2015 CML - MPN
 Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Imatinib & Ponatinib. Two ends of the spectrum in 2016s reality
 Imatinib & Ponatinib Two ends of the spectrum in 2016s reality CML 2016 Benefits & risks Steve O Brien CML Horizons, May 2016 Disclosures Research funding, participation in company trial, speaker, consultant,
Imatinib & Ponatinib Two ends of the spectrum in 2016s reality CML 2016 Benefits & risks Steve O Brien CML Horizons, May 2016 Disclosures Research funding, participation in company trial, speaker, consultant,
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
Understanding Your Blood Work Results
 Understanding Your Blood Work Results Carlos Besses, MD, hd Hematology Department Hospital del Mar - IMIM, Barcelona Carlos Besses Disclosures Novartis Honorarium Speaker Shire Honorarium Speaker Galena
Understanding Your Blood Work Results Carlos Besses, MD, hd Hematology Department Hospital del Mar - IMIM, Barcelona Carlos Besses Disclosures Novartis Honorarium Speaker Shire Honorarium Speaker Galena
Permissive hypoxaemia. Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK
 Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor
 Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
Essential thrombocythemia Incidence of thrombotic complications
 ARS Medica Tomitana - 2016; 2(22): 108-112 10.1515/arsm-2016-0019 Ghinea Mihaela Maria1, Niculescu Zizi2, Niculescu C.1, Grigorian M.2 Essential thrombocythemia Incidence of thrombotic complications 1Faculty
ARS Medica Tomitana - 2016; 2(22): 108-112 10.1515/arsm-2016-0019 Ghinea Mihaela Maria1, Niculescu Zizi2, Niculescu C.1, Grigorian M.2 Essential thrombocythemia Incidence of thrombotic complications 1Faculty